
Overview of randomized controlled trials of moderate to severe traumatic brain injury: A systematic review
Abstract
BACKGROUND:
Given the complexity of post-TBI medical, surgical, and rehabilitative care, research is critical to optimize interventions across the continuum of care and improve outcomes for persons with moderate to severe TBI.
OBJECTIVE:
To characterize randomized controlled trials (RCTs) of moderate to severe traumatic brain injury (TBI) in the literature.
METHOD:
Systematic searches of MEDLINE, PubMed, Scopus, CINAHL, EMBASE and PsycINFO for RCTs up to December 2022 inclusive were conducted in accordance with PRISMA guidelines.
RESULTS:
662 RCTs of 91,946 participants published from 1978 to 2022 met inclusion criteria. The number of RCTs published annually has increased steadily. The most reported indicator of TBI severity was the Glasgow Coma Scale (545 RCTs, 82.3%). 432 (65.3%) RCTs focused on medical/surgical interventions while 230 (34.7%) addressed rehabilitation. Medical/surgical RCTs had larger sample sizes compared to rehabilitation RCTs. Rehabilitation RCTs accounted for only one third of moderate to severe TBI RCTs and were primarily conducted in the chronic phase post-injury relying on smaller sample sizes.
CONCLUSION:
Further research in the subacute and chronic phases as well as increasing rehabilitation focused TBI RCTs will be important to optimizing the long-term outcomes and quality of life for persons living with TBI.
1Introduction
Traumatic brain injury (TBI) is a leading cause of death and disability worldwide, and it can be associated with devastating long-term consequences for individuals and families (World Health Organization, 2006). TBI is defined as “an alteration in brain function, or other evidence of brain pathology, caused by an external force” (Menon et al., 2010). TBI is a complex and heterogenous condition, that includes mild forms of injury such as concussion as well as severe penetrating injuries (Wang et al., 2018). TBI severity is typically categorized as mild, moderate, and severe depending on measures such as the duration of post-traumatic amnesia, duration of loss of consciousness or coma (Blennow et al., 2016), and the Glasgow Coma Scale (GCS) score (Robinson, 2021). The diagnosis of TBI is also supported by neuroimaging findings, which may reveal skull fractures, edema and/or hemorrhage; these signs of intracranial injury are present in the majority of moderate injuries and in all cases of severe injuries (Public Health Agency of Canada, 2020; World Health Organization, 2006). For individuals with moderate to severe TBI, timely and appropriate medical, surgical, and rehabilitative care is critical to improving outcomes. An estimated 69 to 74 million individuals worldwide sustain a TBI each year, presenting a serious health and economic challenge (Dewan et al., 2018). Among survivors of TBI, the majority of injuries result from road traffic accidents, falls, or violence/assault (World Health Organization, 2006). TBI is prevalent across all age groups, including children, working-age adults, and older adults.
Groups that are particularly susceptible to TBI are individuals who participate in high-impact sports (e.g., ice hockey), victims of intimate partner violence, and those who use alcohol and drugs (Public Health Agency of Canada, 2020). TBI also occurs in the context of one’s occupation; in Canada, Toccalino et al. (2021) found that individuals who work in manual labor industries, such as construction, are more likely to sustain a work-related TBI. Other high risk industries include farming, education, healthcare, and transportation (Toccalino et al., 2021). Moreover, individuals in the military who are in active duty have a higher incidence of TBI when compared to civilians (Haarbauer-Krupa et al., 2021). Some sociodemographic factors, such as race and ethnicity, may also confer increased risk of TBI and contribute to disparities experienced across the healthcare continuum for individuals who have sustained a TBI (Saadi et al., 2022).
Within the first hours, days and weeks post-injury, an individual may need interventions to prevent mortality and further neurological damage, treatments to manage body temperature, intracranial pressure, airway/ventilation, coagulopathies, and electrolytes, as well as complications of critical illness (Wiles, 2022). Subsequently, after discharge from acute care, persons with TBI often need extensive individualized rehabilitation with an expert interdisciplinary team in order to address impairments and optimize function in areas such as activities of daily living, communication, mobility, and cognition (Kreitzer et al., 2019). Given the complexity of post-TBI medical, surgical, and rehabilitative care, research is critical to optimize interventions across the continuum of care and improve outcomes for persons with TBI.
The objective of this research is to characterize randomized controlled trials (RCTs) of moderate to severe traumatic brain injury (TBI) in the literature and to analyze the number of studies, sample sizes used, and the areas of research focus.
2Methods
2.1Literature search
Systematic searches of MEDLINE, PubMed, Scopus, CINAHL, EMBASE and PsycINFO were conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The search terms were restricted to RCTs published in the English language up to and including December 2022. Key terms such as ‘brain injury’, ‘head injury’, ‘head trauma’, ‘randomized’, ‘placebo controlled’, and ‘randomized controlled trial’ were used in combination, and Medical Subject Headings (MeSH) were used in each database. Variations of these terms were employed, as appropriate, for each separate database search. The full search details can be found in the Supplementary Materials. The complete search results from each database were imported to Endnote version 8 (Camelot UK Bidco Limited (Clarivate)) and duplicates were removed. Titles and abstracts were screened against inclusion criteria by two independent reviewers and the full text of abstracts that appeared to meet inclusion criteria were reviewed by two independent reviewers; disputes were resolved by an independent third reviewer.
2.2Inclusion and exclusion criteria
Studies were included if they met the following a priori criteria: (a) human participants with a mean age ≥18 years; (b) ≥50% of the sample had moderate to severe TBI; and (c) the study design was a RCT. The following studies were excluded: (a) protocols and secondary analyses of RCTs; (b) studies not reporting the injury severity or etiology; (c) <50% of the sample had a traumatic injury etiology; and/or (e) >50% of the sample had mild TBI. In cases where the authors were unable to locate a full-text version of an article, an email was sent to the corresponding author requesting a copy. All contacted authors were given one month to respond before the article was excluded.
2.3Data extraction
Two reviewers participated in the data extraction process. Extracted data included author, year of publication, journal of publication, injury etiology (traumatic or mixed traumatic and atraumatic), time post-injury, injury severity indicators, sample size, and the specific area of research focus. If data was missing for any of the variables, it was documented as not reported (NR).
2.4Defining RCT area of research focus
For this systematic review, we divided studies into two groups: rehabilitation and medical/surgical (Med/Surg) management. We considered studies to fall into the rehabilitation category if they addressed the improvement of functional outcomes, including but not limited to speech, physical movement, cognition, emotional, behavioural, and social participation. Studies in this group did not need to take place in specific rehabilitation settings; for instance, early rehabilitation that occurs in critical care was also considered to belong to this group (Brasure et al., 2012). We considered studies to fall into the medical/surgical management category if they addressed critical care and interventions to prevent mortality and further neurological damage, including but not limited to surgery, tracheostomy, red blood cell transfusion, therapeutic cooling, temperature regulation management, and intracranial pressure management and monitoring (Wiles, 2022). While studies in the medical/surgical management group tend to address factors that occur almost exclusively in the acute phase post-injury, this was not a criterion for categorization.
2.5Defining time post-injury
We divided the RCTs according to time post-injury as follows: acute (≤1 month), subacute (>1 to <6 months), and chronic (≥6 months).
3Results
3.1Description of studies
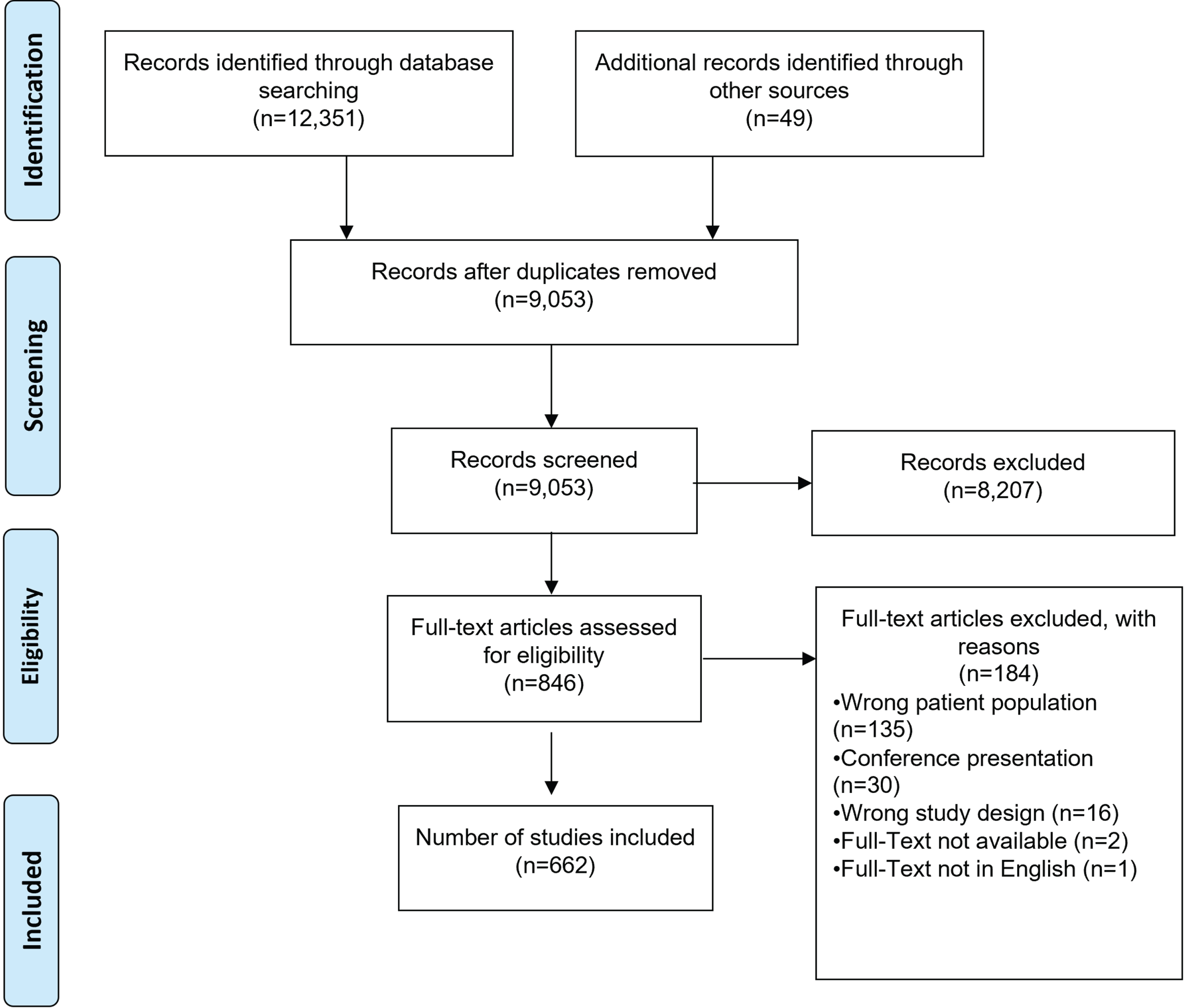
9,053 unique articles were screened for title and abstract after duplicates were removed and 846 underwent full-text review. 662 RCTs met inclusion criteria and underwent data extraction (Fig. 1). These studies represented a total of 91,946 participants; the mean sample size of all RCTs was 147.4, with sample sizes varying from 17 to 18,079 each year.
Fig. 1
PRISMA Flowchart.
3.2Temporal trends
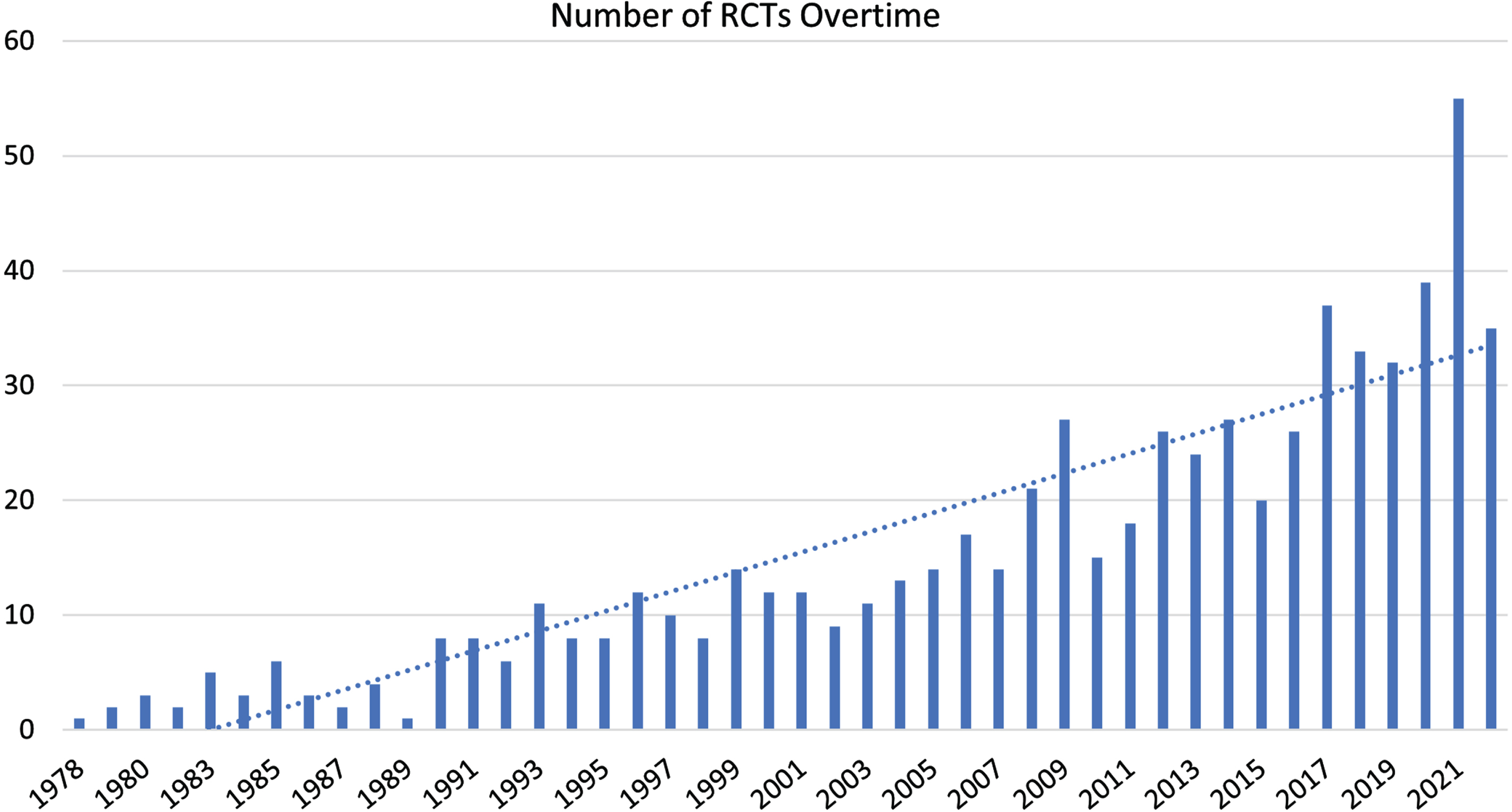
Studies were published between 1978 and 2022. The annual number of published RCTs increased steadily starting in the 1990s and accelerated into the 2010s (Fig. 2). There were 32 RCTs published between 1978 and 1989 (mean 2.7 per year), 93 RCTs from 1990 to 1999 (9.3 per year), 150 RCTs from 2000 to 2009 (25.0 per year), 258 RCTs from 2010 to 2019 (25.8 per year), and 129 RCTs from 2020 to 2022 (43.0 per year). Additional temporal trends are outlined in the subsequent sections.
Fig. 2
Number of RCTs of moderate to severe TBI published by year.
3.3Research focus: rehabilitation versus medical/surgical management
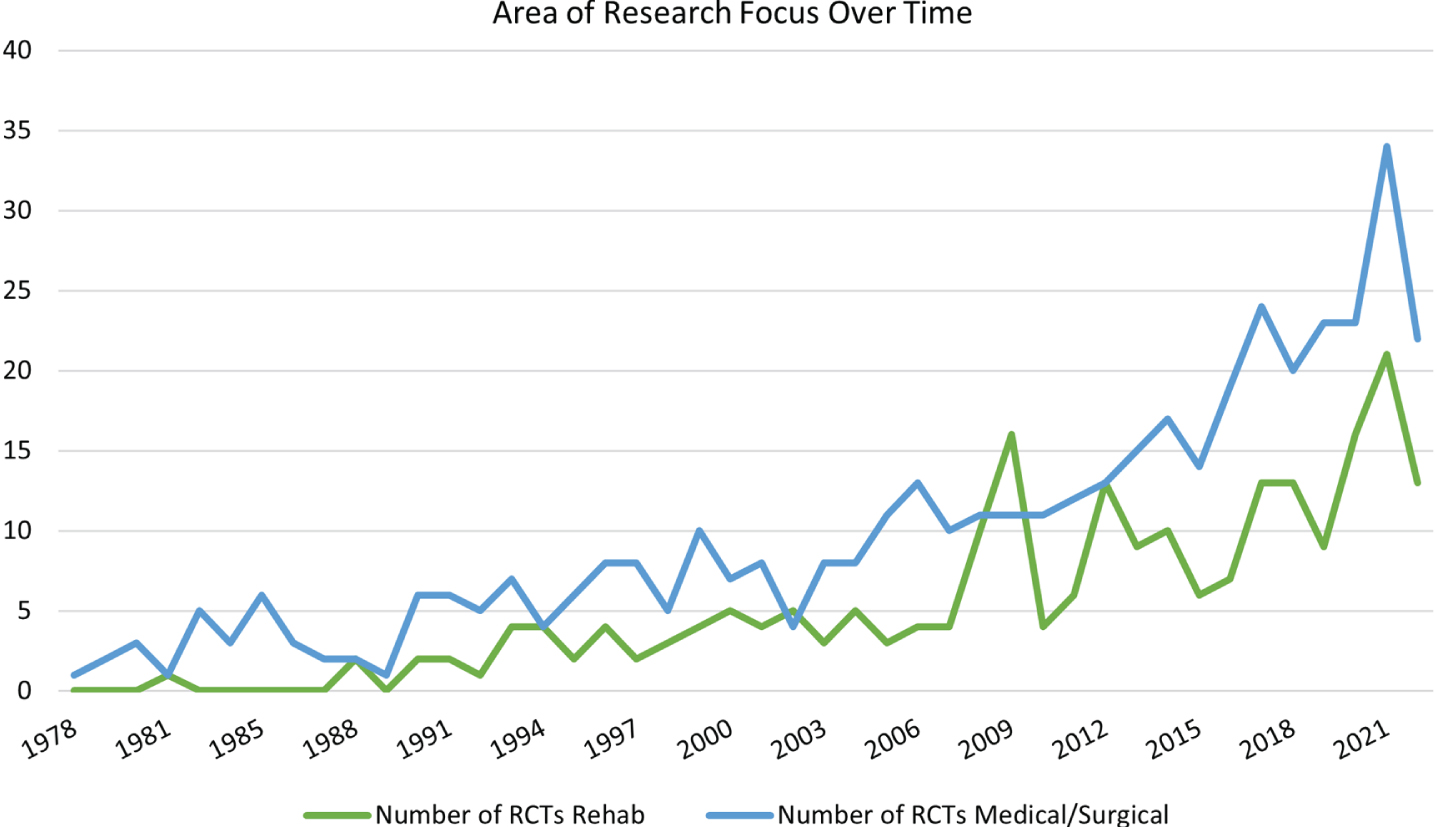
As summarized in Table 1, 65.3% of all TBI RCTs evaluated medical/surgical management, while the remainder (34.7%) evaluated rehabilitation interventions. Figure 3 demonstrates how the number of RCTs focused on the medical/surgical management of TBI have increased to a greater degree over time when compared to rehabilitation-focused RCTs.
Table 1
Area of research focus in RCTs of moderate to severe TBI
| Area of research | Number of RCTs | Percentage |
| Medical/surgical management | 432 | 65.3% |
| Rehabilitation | 230 | 34.7% |
| Total | 662 |
Fig. 3
Area of research focus of moderate to severe TBI RCTs over time.
3.4Sample size
Sample sizes ranged from 3 to 12,737 participants; the annual number of participants across all studies ranged from 17 to 18,079 each year. The majority of RCTs (507, 76.6%) had sample sizes of <100 individuals; 141 RCTs (21.3%) had sample sizes of 101–500 individuals and only 14 RCTs (2.1%) had sample sizes of >500 individuals (Table 2). All 14 of the largest studies (sample size >500) were RCTs evaluating medical/surgical management (Table 2). The mean sample size for all RCTs was 147.4 (median 52.5). Among medical/surgical RCTs, the mean sample size was 195.8 (median 62.0) compared to a mean of 56.4 (median 36) in rehabilitation RCTs. Additional data on sample size is available in the Supplementary Materials.
Table 2
Sample size of moderate to severe TBI TBI RCTs by area of research focus
| Sample size | Total RCTs | % | Rehab RCTs | % | Med/surg RCTs | % |
| <51 | 317 | 47.9% | 143 | 62.2% | 174 | 40.3% |
| 51–100 | 190 | 28.7% | 56 | 24.3% | 134 | 31.0% |
| 101–500 | 141 | 21.3% | 31 | 13.5% | 110 | 25.5% |
| >500 | 14 | 2.1% | 0 | 0.0% | 14 | 3.2% |
| Total | 662 | 230 | 432 |
3.5Time post-injury
Time post-injury was reported for 519 RCTs (78.4%) (Table 3). Nearly half of all RCTs occurred in the acute phase (n = 322, 48.6%), almost a quarter occurred in the chronic phase (n = 160, 24.2%), and the fewest RCTs occurred in the subacute phase (n = 37, 5.6%) post-injury.
Table 3
Time post-injury in RCTs of moderate to severe TBI by area of research focus
| Time post-injury | Number of RCTs | % | Number of rehabilitation RCTs | % | Number of medical/surgical management RCTs | % |
| Not reported | 143 | 21.6% | 26 | 11.3% | 117 | 27.1% |
| Acute (≤1mo) | 322 | 48.6% | 20 | 8.7% | 302 | 69.9% |
| Subacute (> 1mo to < 6mo) | 37 | 5.6% | 34 | 14.8% | 3 | 0.7% |
| Chronic (≥6mo) | 160 | 24.2% | 150 | 65.2% | 10 | 2.3% |
| Total | 662 | 230 | 432 |
Stratifying RCTs by time post-injury and area of research focus illustrates that the majority of studies focusing on medical/surgical management occurred in the acute phase post injury (n = 302; 69.9%), which rises to 95.9% (302/315) when considering only studies where time post-injury is reported. In contrast, most studies focusing on rehabilitation interventions occurred in the chronic phase post-injury (n = 150; 65.2%), which rises to 73.5% when considering only RCTs where time post-injury is reported (n = 150/204).
The mean sample size in RCTs that did not report time post-injury was 83.7, compared with a mean of 234.5 participants in the acute phase, 74.1 in subacute phase, and 46 in chronic phase RCTs. The median sample size for RCTs that did not report time-post-injury was 60, compared with a median of 62 participants in the acute phase, 40 participants in the subacute phase, and 30 participants in the chronic phase RCTs.
3.6Injury etiology
Most studies focused on populations with an exclusively traumatic injury etiology (n = 607, 91.7%) (Table 4). Those RCTs including participants with mixed traumatic and non-traumatic etiologies (n = 55, 8.3%) also included individuals with acquired brain injury such as tumors, stroke, and hypoxia.
Table 4
Injury etiology in RCTs of moderate to severe TBI by area of research focus
| Injury etiology | Number of RCTs | % | Number of rehab RCTs | % | Number of med/surg RCTs | % |
| TBI | 607 | 91.7% | 201 | 87.4% | 406 | 94.0% |
| Mixed | 55 | 8.3% | 29 | 12.6% | 26 | 6.0% |
| Total | 662 | 230 | 432 |
Stratifying by area of research focus illustrates that the majority of RCTs focused on medical/surgical management (406/432, 94%) and those focused on rehabilitation interventions (201/230, 87.4%) included exclusively individuals with traumatic etiologies.
3.7Indicators of injury severity
Across the 662 RCTs, 17 different indicators of injury severity were used (Table 5). 24 RCTs (3.6%) did not report the specific injury severity indicator(s) used. The Glasgow Coma Scale (GCS) score, alone or in combination with other indicators, was the most frequently used metric for defining the severity of injury and was used in 545 RCTs (82.3%). Other common indicators of TBI severity were duration of post-traumatic amnesia (PTA) used in 120 RCTs (18.1%), and duration of loss of consciousness or presence of a disorder of consciousness (LOC/DOC) used in 65 RCTs (9.8%). Some studies reported other metrics, including the Injury Severity Score (ISS) (18 RCTs, 2.7%) and/or the Abbreviated Injury Score (AIS) (13 RCTs, 2.0%).
Table 5
TBI Severity indicators used in RCTs of moderate to severe TBI
| Severity indicator | Number of RCTs | % |
| Glasgow coma scale (GCS) | 545 | 82.3% |
| Posttraumatic amnesia (PTA) | 120 | 18.1% |
| Loss of consciousness/disorder of consciousness (LOC/DOC) | 65 | 9.8% |
| Not reported (NR) | 24 | 3.6% |
| Injury severity score (ISS) | 18 | 2.7% |
| Abbreviated injury score (AIS) | 13 | 2.0% |
| Coma recovery scale revised (CRS-R) | 5 | 0.6% |
| Acute physiology and chronic health evaluation (APACHE II) | 3 | 0.5% |
| Traumatic coma data bank (TCDB) | 3 | 0.5% |
| Ohio state university TBI identification method (OSU TBI-ID) | 2 | 0.3% |
| Rotterdam classification | 2 | 0.3% |
| Imaging only | 2 | 0.3% |
| Marshall computed tomography (CT) score | 2 | 0.3% |
| Medical records | 1 | 0.2% |
| Department of defense score | 1 | 0.2% |
| Grady coma scale | 1 | 0.2% |
| Full outline of unresponsiveness (FOUR) | 1 | 0.2% |
| Arakis classification of head injuries | 1 | 0.2% |
Stratifying RCTs by area of research focus illustrates that the majority of medical/surgical RCTs (397/432, 91.9%) used GCS, either alone or in combination with other metrics, to define injury severity (Table 6). In contrast, only 64.3% of those RCTs focused on rehabilitation interventions (148/230) defined injury severity using GCS; these RCTs were much more likely to define injury severity using other measures, particularly PTA (116/230, 50.4%) and LOC/DOC (51/230, 22.2%).
Table 6
Top five indicators of injury severity in RCTs of moderate to severe TBI by area of research focus
| Top 5 indicators | Total RCTs | % | Rehab RCTs | % | Med/surg RCTs | % |
| GCS | 545 | 82.3% | 148 | 64.3% | 397 | 91.9% |
| PTA | 120 | 18.1% | 116 | 50.4% | 4 | 0.9% |
| LOC/DOC | 65 | 9.8% | 51 | 22.2% | 14 | 3.2% |
| ISS | 18 | 2.7% | 3 | 1.3% | 15 | 3.5% |
| AIS | 13 | 2.0% | 2 | 0.9% | 11 | 2.5% |
Abbreviations: GCS = Glasgow Coma Scale score; PTA = post-traumatic amnesia; LOC/DOC = duration of loss of consciousness or presence of disorder of consciousness; ISS = Injury Severity Score; AIS = Abbreviated Injury Score.
3.8Interventions
There were more than 200 different interventions that were used alone or in combination across 662 RCTs. Each intervention was given a unique code to determine how many RCTs had utilized that particular intervention, and 9 categories were used to group them: motor and sensory, psychosocial and behavioural, alternative medicine, electrical stimulation, technological, nutrition, acute/surgical, pharmacological, and non-pharmacological rehabilitation (Table 7). In 29.3% of RCTs, interventions were compared to ‘placebo/sham’. 35% of RCTs compared interventions to ‘standard of care’. Only 3.5% of RCTs used ‘no treatment’ as the control group. Almost half of (n = 313, 47.3%) included pharmacological interventions, with Mannitol being the most commonly used medication. Interventions were highly heterogeneous. Table 7 presents a list of interventions used in ≥5 RCTs by category.
Table 7
Interventions used in ≥5 RCTs of moderate to severe traumatic brain injury
| Interventions | |
| Motor-sensory interventions | RCTs |
| Exercise | 14 |
| Gait/balance training | 7 |
| Physical therapy | 6 |
| Casting/splinting | 6 |
| Psychosocial/behavioural interventions | RCTs |
| Psychotherapy | 22 |
| Social intervention/peer support | 10 |
| Motivational interviewing (MI) | 8 |
| Behavioural modification/management | 7 |
| Emotion recognition training | 7 |
| Alternative interventions | RCTs |
| Traditional chinese medicine | 5 |
| Electrical stimulation interventions | RCTs |
| Transcranial direct electrical stimulation (tDCS) | 6 |
| Technological interventions | RCTs |
| Telehealth intervention | 7 |
| Virtual reality | 5 |
| Nutrition interventions | RCTs |
| Enteral nutrition | 20 |
| Parenteral nutrition | 14 |
| Enhanced enteral nutrition formula | 11 |
| Combined enteral + parenteral nutrition | 5 |
| Acute/surgical interventions | RCTs |
| Hypothermia | 42 |
| Decompressive craniectomy/craniotomy | 17 |
| ICU environment/coma sensory stimulation | 15 |
| Mechanical ventilation intervention | 12 |
| Oxygen therapy/hyperoxia | 11 |
| Intracranial pressure (ICP) monitoring/management | 8 |
| Transfusion intervention (RBC/Hb) | 7 |
| Intubation intervention/monitoring | 6 |
| Tracheostomy intervention | 6 |
| Intracranial pressure/cerebral perfusion pressure (ICP/CPP) guided management | 5 |
| Pharmacological interventions | RCTs |
| Mannitol | 20 |
| Methylphenidate | 19 |
| Hypertonic saline (HTS) | 18 |
| Tranexamic acid (TXA) | 14 |
| Phenytoin/fosphenytoin | 12 |
| Propofol | 12 |
| Progesterone | 12 |
| Amantadine | 11 |
| Nimodipine | 8 |
| Dexmedetomidine | 8 |
| Erythropoietin (EPO) | 7 |
| Sufentanil | 6 |
| Intensive insulin therapy (IIT) | 6 |
| Cyclosporin | 6 |
| Midazolam | 6 |
| Fentanyl | 5 |
| Sertraline | 5 |
| Non-pharmacological/rehabilitation interventions | RCTs |
| General cognitive rehabilitation/training | 20 |
| Memory training | 20 |
| Education | 13 |
| Attention training | 11 |
| Information/discussion and writing groups | 8 |
| Music therapy | 8 |
| Communication intervention | 7 |
| Early multidisciplinary intensive rehabilitation | 6 |
NOTE: Interventions were used alone or in combination with others.
4Discussion
Our search identified 662 RCTs published from 1978 to the end of 2022, which had enrolled 91,946 participants with moderate to severe TBI. The number of TBI RCTs published each year has been increasing steadily over time. Compared to the decade after the first RCT was published (1978–1987 inclusive), the most recent decade (2013–2022 inclusive) saw a 10-fold increase in the number of published RCTs, which is in line with global trends (Vinkers et al., 2021). This marked increase in research productivity has primarily been driven by an increase in RCTs focused on medical/surgical interventions, mostly occurring in the acute phase post-injury, with a lesser contribution made by RCTs focused on rehabilitation interventions mostly occurring in the chronic phase post-injury.
322 RCTs (48.6%) took place in the acute phase post-injury, of which 302 (69.9%) focused on medical/surgical management. The proportion is even higher (95.9%) if considering only those RCTs which reported time post-injury. Only 20 RCTs in the acute phase (8.7%) focused on rehabilitation interventions. Conversely, of the 160 RCTs conducted in the chronic phase, 150 RCTs (93.8%) focused on rehabilitation and only 10 (2.3%) addressed medical/surgical interventions. This is as expected because with increasing time post-injury an individual’s medical stability is likely to improve and healthcare interventions will accordingly shift to address a greater need for and ability to participate in rehabilitative interventions. Unfortunately, 143 RCTs (21.6%) did not report on time post-injury.
Other time post-injury trends are harder to explain. For instance, remarkably few RCTs (a mere 37, 5.6%), were initiated in the subacute phase (>1 months to <6 months), 34 of which focused on rehabilitation and 3 on medical/surgical management. From what we know about critical windows of neurologic recovery from other conditions (Carroll et al., 2004; Ditunno et al., 1992; Grau et al., 2001; Steeves et al., 2011), the underrepresentation of this time interval may be a barrier to optimizing patient outcomes through intensive inpatient and/or community rehabilitation. Alternatively, those critical time windows may not be as relevant to TBI recovery. This is an important question which requires further research, especially given that this is the time period when almost all inpatient and a substantial amount of outpatient rehabilitation takes place.
Sample size varied widely across these studies (3 to 12,737). Sample size was greater for medical/surgical RCTs when compared to rehabilitation RCTs (mean 195.8 vs. 56.4 participants; median 62 vs. 36 participants). This correlates strongly with time post-injury data where sample size was greater for acute compared to chronic RCTs (mean 234.5 vs. 46.0 participants; median 62 vs. 30 participants). Other analyses of rehabilitation RCTs have also commented that small sample sizes are typical, but that this is not without concern (Boukrina et al., 2020; Gianola et al., 2019; Latif et al., 2011).
The most common indicator used to define injury severity was GCS (545 RCTs, 82.3%). The GCS was even more prevalent when looking specifically at the literature focused on medical/surgical management post-TBI (397 RCTs, 91.9%). Given that the clinical use of GCS is widely recommended in guidelines for the management of individuals in trauma situations and to define and monitor neurological responsiveness acutely, its widespread use in TBI RCTs is not surprising (Teasdale et al., 2014). Of the commonly used injury severity indicators identified in this systematic review, GCS can most easily and rapidly be determined at any time point post-injury. In comparison, duration of PTA, duration of LOC, or presence of DOC are more difficult to determine, particularly in the first month post-injury, as these often require skilled medical personnel, specific instruments, and/or specialized training (Nakase-Richardson et al., 2011; Walker et al., 2010). Moreover, the duration of PTA and/or LOC or DOC may extend indefinitely, and determination of duration at the time of study enrolment may not be possible over a short time period. In contrast, rehabilitation RCTs, which predominantly took place in the chronic (≥6 months) phase, frequently used PTA as an indicator of injury severity. PTA was used in 116 of 230 rehabilitation RCTs (50.4%) compared to only 4 of 432 medical/surgical management RCTs (0.9%). Similarly, LOC/DOC were used in 51 of 230 rehabilitation RCTs (21.7%) compared to only 14 of 432 medical/surgical RCTs (3.2%).
Acute phase and medical/surgical management research are unequivocally essential to improving patient outcomes after TBI. As this research contributes to improved outcomes such that mortality decreases and survival improves for persons who experience TBI, the importance of research on rehabilitation interventions to improve outcomes for the individual, their family, and society increases. Indeed, a growing body of literature demonstrates that rehabilitation for persons with moderate to severe TBI is cost-effective and not only improves health outcomes, hospital length of stay, level of disability, and quality of life for the individual, but also reduces health and social services dependency (Andelic et al., 2014; Howe et al., 2022; Oddy & da Silva Ramos, 2013; Turner-Stokes, 2007; Turner-Stokes et al., 2006; Worthington et al., 2006). Moreover, numerous studies have demonstrated the cost effectiveness of various forms (inpatient, outpatient, other) of TBI rehabilitation (Andelic et al., 2014; Cooney & Carroll, 2016; Oddy & da Silva Ramos, 2013; Turner-Stokes, 2008).
Studies focused on rehabilitation interventions accounted for only 34.7% of RCTs identified in this systematic review. The relative paucity of rehabilitation focused RCTs and the lower sample sizes seen in this area of research is concerning and makes a strong case for the need for dedicated research of this type. Moreover, rehabilitation research was largely confined to the chronic phase post-injury. The limited number of RCTs in the subacute phase, of which 34 (91.9%) were focused on rehabilitation, indicates that research is not taking place in the time period when intensive inpatient rehabilitation tends to take place (Hammond et al., 2015; Seel et al., 2015).
4.1Limitations
This manuscript presents data from a database of 662 RCTs on moderate to severe TBI. An initial search was conducted up to June 2021, with an updated search conducted up to and including December 2022. The generalizability of the findings of this systematic review is limited by having considered only moderate to severe TBI and not having included mild TBI.
We did not consider studies that did not report the severity of TBI or where there were mixed populations but the proportion of TBI was not reported or less than 50%. Moreover, important data for the generalizability of RCT findings was missing from a few included studies; 143 RCTs (21.6%) did not report the time post-injury of their participants, and 24 RCTs (3.6%) did not report the metrics used to define injury severity, although they classified included participants as having moderate to severe TBI.
A protocol was not registered on the International Prospective Register of Systematic Reviews before this submission. We did not perform GRADE or Cochrane risk of bias. The physicians in our team assisted with the classification of RCTs into medical/surgical management or rehabilitation. Given the heterogeneity of studies, we did not collect information on effectiveness of the trial. This review only considered adults (18 years of age and older); therefore, pediatric populations are not represented.
5Conclusions
This systematic review identified 662 RCTs published from 1978 to 2022 representing 91,946 participants with moderate to severe TBI. The majority of TBI RCTs examine medical/surgical management in the acute phase post-injury and use GCS to define injury severity. Rehabilitation RCTs accounted for only a third of moderate to severe TBI RCTs and are primarily conducted in the chronic phase with smaller sample sizes. There is a substantial gap in research in the subacute phase post-injury. As acute phase medical/surgical interventions improve mortality after TBI, increasing research in the subacute and chronic phases as well as increasing rehabilitation focused TBI RCTs will be important for the optimization of long-term outcomes and quality of life for persons living with TBI.
Acknowledgments
The authors would like to acknowledge the valuable contributions of Muskan Sait to the preparation of this manuscript.
Conflict of interest
Dr. Robert Teasell had received a grant from Abbvie (makers of Botox) for Stroke research within the last three years. The authors report there are no competing interests to declare. An abstract of the present research has been previously submitted to the World Federation for Neurorehabilitation 13th World Congress Conference.
Ethical considerations
This study, as a systematic review, is exempt from Institutional Review Board approval.
Funding
Funding was provided by the Ontario Ministry of Health and Long-Term Care through Neurotrauma Pathways and the St. Joseph’s Health Care (London) Foundation.
Transparency statement
Data presented in this article comes from a large database of 662 RCTs on moderate to severe TBI that partially overlaps with the Evidence-Based Review of Acquired Brain Injuries (ERABI) which is freely available online www.erabi.ca. Other parts of this database, including data on country of origin and sex differences, have been published elsewhere and data included in the supplementary materials may partially overlap with data presented in these publications.
Supplementary material
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/NRE-240019.
References
1 | Andelic N. , Ye J. , Tornas S. , Roe C. , Lu J. , Bautz-Holter E. , Moger T. , Sigurdardottir S. , Schanke A.-K. , Aas E. ((2014) ). Cost-effectiveness analysis of an early-initiated, continuous chain of rehabilitation after severe traumatic brain injury. Journal of neurotrauma, 31: (14), 1313–1320. |
2 | Blennow K. , Brody D.L. , Kochanek P.M. , Levin H. , McKee A. , Ribbers G.M. , Yaffe K. , Zetterberg H. ((2016) ). Traumatic brain injuries. Nature Reviews Disease Primers, 2: , 16084.https://doi.org/10.1038/nrdp.2016.84. |
3 | Boukrina O. , Kucukboyaci N.E. , Dobryakova E. ((2020) ). Considerations of power and sample size in rehabilitation research. International Journal of Psychophysiology, 154: , 6–14.https://doi.org/10.1016/j.ijpsycho.2019.08.009. |
4 | Brasure M. , Lamberty G.J. , Sayer N.A. , Nelson N.W. , MacDonald R. , Ouellette J. , Tacklind J. , Grove M. , Rutks I.R. , Butler M.E. , Kane R.L. , Wilt T.J. (2012). AHRQ Comparative Effectiveness Reviews. In Multidisciplinary Postacute Rehabilitation for Moderate to Severe Traumatic Brain Injury in Adults. Agency for Healthcare Research and Quality (US). |
5 | Carroll L.J. , Cassidy J.D. , Peloso P.M. , Borg J. , von Holst H. , Holm L. , Paniak C. , Pépin M. ((2004) ). Prognosis for mild traumatic brain injury: Results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. Journal of rehabilitation Medicine(43 Suppl), 84–105.https://doi.org/10.1080/16501960410023859. |
6 | Cooney M.T. , Carroll Á. ((2016) ). Cost effectiveness of inpatient rehabilitation in patients with brain injury. Clinical Medicine, 16: (2), 109. |
7 | Dewan M.C. , Rattani A. , Gupta S. , Baticulon R.E. , Hung Y.C. , Punchak M. , Agrawal A. , Adeleye A.O. , Shrime M.G. , Rubiano A.M. , Rosenfeld J.V. , Park K.B. ((2018) ). Estimating the global incidence of traumatic brain injury. Journal of Neurosurgery, 1–18.https://doi.org/10.3171/2017.10.Jns17352. |
8 | Ditunno J.F. , Stover S.L. , Freed M.M. , Ahn J. ((1992) ). Motor recovery of the upper extremities in traumatic quadriplegia: A multicenter study. Archives of physical medicine and rehabilitation, 73: (5), 431–436. |
9 | Gianola S. , Castellini G. , Corbetta D. , Moja L. ((2019) ) . Rehabilitation interventions in randomized controlled trials for low back pain: Proof of statistical significance often is not relevant. Health and quality of life outcomes, 17: , 1–8. |
10 | Grau A.J. , Weimar C. , Buggle F. , Heinrich A. , Goertler M. , Neumaier S. , Glahn J. , Brandt T. , Hacke W. , Diener H.C. ((2001) ). Risk factors, outcome, and treatment in subtypes of ischemic stroke: The German stroke data bank. Stroke, 32: (11), 2559–2566.https://doi.org/10.1161/hs1101.098524. |
11 | Haarbauer-Krupa J. , Pugh M.J. , Prager E.M. , Harmon N. , Wolfe J. , Yaffe K. ((2021) ). Epidemiology of Chronic Effects of Traumatic Brain Injury. Journal of neurotrauma, 38: (23), 3235–3247.https://doi.org/10.1089/neu.2021.0062. |
12 | Hammond F.M. , Horn S.D. , Smout R.J. , Beaulieu C.L. , Barrett R.S. , Ryser D.K. , Sommerfeld T. ((2015) ). Readmission to an acute care hospital during inpatient rehabilitation for traumatic brain injury. Archives of physical medicine and rehabilitation, 96: (8), S293–S303.e291. |
13 | Howe E.I. , Andelic N. , Fure S.C. , Røe C. , Søberg H.L. , Hellstrøm T. , Spjelkavik Ø. , Enehaug H. , Lu J. , Ugelstad H. ((2022) ). Cost-effectiveness analysis of combined cognitive and vocational rehabilitation in patients with mild-to-moderate TBI: Results from a randomized controlled trial. BMC Health Services Research, 22: (1), 185. |
14 | Kreitzer N. , Rath K. , Kurowski B.G. , Bakas T. , Hart K. , Lindsell C.J. , Adeoye O. ((2019) ). Rehabilitation Practices in Patients With Moderate and Severe Traumatic Brain Injury. Journal of Head Trauma Rehabilitation, 34: (5), E66–E72.https://doi.org/10.1097/htr.0000000000000477. |
15 | Latif L.A. , Amadera J.E. D. , Pimentel D. , Pimentel T. , Fregni F. ((2011) ). Sample size calculation in physical medicine and rehabilitation: A systematic review of reporting, characteristics, and results in randomized controlled trials. Archives of physical medicine and rehabilitation, 92: (2), 306–315. |
16 | Menon D.K. , Schwab K. , Wright D.W. , Maas A.I. ((2010) ). Position statement: Definition of traumatic brain injury. Archives of physical medicine and rehabilitation, 91: (11), 1637–1640.https://doi.org/10.1016/j.apmr.2010.05.017. |
17 | Nakase-Richardson R. , Sherer M. , Seel R. , Hart T. , Hanks R. , Arango-Lasprilla J. , Yablon S. , Sander A. , Barnett S. , Walker W. ((2011) ). Utility of post-traumatic amnesia in predicting 1-year productivity following traumatic brain injury: Comparison of the Russell and Mississippi PTA classification intervals. Journal of Neurology, Neurosurgery & Psychiatry, 82: (5), 494–499. |
18 | Oddy M. , da Silva Ramos S. ((2013) ). The clinical and cost-benefits of investing in neurobehavioural rehabilitation: A multi-centre study. Brain Injury, 27: (13–14), 1500–1507. |
19 | Public Health Agency of Canada. (2020). Spotlight on Traumatic Brain Injuries Across the Life Course. |
20 | Robinson C.P. ((2021) ). Moderate and Severe Traumatic Brain Injury. Continuum (Minneap Minn), 27: (5), 1278–1300.https://doi.org/10.1212/con.0000000000001036. |
21 | Saadi A. , Bannon S. , Watson E. , Vranceanu A.M. ((2022) ). Racial and Ethnic Disparities Associated with Traumatic Brain Injury Across the Continuum of Care: A Narrative Review and Directions for Future Research. Journal of Racial and Ethnic Health Disparities, 9: (3), 786–799.https://doi.org/10.1007/s40615-021-01017-4. |
22 | Seel R.T. , Barrett R.S. , Beaulieu C.L. , Ryser D.K. , Hammond F.M. , Cullen N. , Garmoe W. , Sommerfeld T. , Corrigan J.D. , Horn S.D. ((2015) ). Institutional variation in traumatic brain injury acute rehabilitation practice. Archives of physical medicine and rehabilitation, 96: (8), S197–S208. |
23 | Steeves J. , Kramer J. , Fawcett J. , Cragg J. , Lammertse D. , Blight A. , Marino R. , Ditunno J. , Coleman W. , Geisler F. ((2011) ). Extent of spontaneous motor recovery after traumatic cervical sensorimotor complete spinal cord injury. Spinal cord, 49: (2), 257–265. |
24 | Teasdale G. , Maas A. , Lecky F. , Manley G. , Stocchetti N. , Murray G. ((2014) ). The Glasgow Coma Scale at 40 years: Standing the test of time. The Lancet Neurology, 13: (8), 844–854. |
25 | Toccalino D. , Colantonio A. , Chan V. ((2021) ). Update on the epidemiology of work-related traumatic brain injury: A systematic review and meta-analysis. Occupational and Environmental Medicine, 78: (10), 769–776.https://doi.org/10.1136/oemed-2020-107005. |
26 | Turner-Stokes L. ((2007) ). Cost-efficiency of longer-stay rehabilitation programmes: Can they provide value for money? Brain Injury, 21: (10), 1015–1021.https://doi.org/10.1080/02699050701591445. |
27 | Turner-Stokes L. ((2008) ). Evidence for the effectiveness of multi-disciplinary rehabilitation following acquired brain injury: A synthesis of two systematic approaches. Journal of rehabilitation Medicine, 40: (9), 691–701. |
28 | Turner-Stokes L. , Paul S. , Williams H. ((2006) ). Efficiency of specialist rehabilitation in reducing dependency and costs of continuing care for adults with complex acquired brain injuries. Journal of Neurology, Neurosurgery & Psychiatry, 77: (5), 634–639.https://doi.org/10.1136/jnnp.2005.073411. |
29 | Vinkers C.H. , Lamberink H.J. , Tijdink J.K. , Heus P. , Bouter L. , Glasziou P. , Moher D. , Damen J.A. , Hooft L. , Otte W.M. ((2021) ). The methodological quality of 176,620 randomized controlled trials published between 1966 and 2018 reveals a positive trend but also an urgent need for improvement. PLoS Biology, 19: (4), e3001162.https://doi.org/10.1371/journal.pbio.3001162. |
30 | Walker W. , Ketchum J. , Marwitz J. , Chen T. , Hammond F. , Sherer M. , Meythaler J. ((2010) ). A multicentre study on the clinical utility of post-traumatic amnesia duration in predicting global outcome after moderate-severe traumatic brain injury. Journal of Neurology, Neurosurgery & Psychiatry, 81: (1), 87–89. |
31 | Wang K.K. , Yang Z. , Zhu T. , Shi Y. , Rubenstein R. , Tyndall J.A. , Manley G.T. ((2018) ). An update on diagnostic and prognostic biomarkers for traumatic brain injury. Expert Review of Molecular Diagnostics, 18: (2), 165–180.https://doi.org/10.1080/14737159.2018.1428089. |
32 | Wiles M.D. ((2022) ). Management of traumatic brain injury: A narrative review of current evidence. Anaesthesia, 77: (Suppl 1), 102–112.https://doi.org/10.1111/anae.15608. |
33 | World Health Organization. (2006). Neurological Disorders Public Health Challenges. |
34 | Worthington A.D. , Matthews S. , Melia Y. , Oddy M. ((2006) ). Cost-benefits associated with social outcome from neurobehavioural rehabilitation. Brain Injury, 20: (9), 947–957.https://doi.org/10.1080/02699050600888314. |


