
Venous thromboembolism and anticoagulation in spinal cord lesion rehabilitation inpatients: A 10-year retrospective study
Abstract
BACKGROUND:
Venous thromboembolism (VTE) is a concern following the onset of spinal cord lesions (SCL).
OBJECTIVES:
To assess the current efficacy and risks of anticoagulation after SCL and consider changes in thromboprophylaxis.
METHODS:
This retrospective cohort study included individuals admitted to inpatient rehabilitation within 3 months of SCL onset. Main outcome measures were the incidence of deep vein thrombosis (DVT), pulmonary embolism (PE), bleeding, thrombocytopenia, or death, which occurred within 1 year of the SCL onset.
RESULTS:
VTE occurred in 37 of the 685 patients included in the study (5.4%, 95% CI 3.7–7.1%, 2.8% PE), and in 16 of 526 patients who received prophylactic anticoagulation at rehabilitation (3%, 95% CI 1.6–4.5%, 1.1% PE, with at least 1 fatality). Of these 526, 1.3% developed clinically significant bleeding and 0.8% thrombocytopenia. Prophylactic anticoagulation, most commonly 40 mg/day, continued until a median period of 6.4 weeks after SCL onset (25% –75% percentiles 5.8–9.7), but in 29.7%, VTE occurred more than 3 months after SCL onset.
CONCLUSION:
The VTE prophylaxis used for the present cohort contributed to a considerable but limited reduction of VTE incidence. The authors recommend conducting a prospective study to assess the efficacy and safety of an updated preventive anticoagulation regimen.
1Introduction
Deep vein thrombosis (DVT) is the formation of a blood clot in the deep veins, most commonly in the lower legs. Persons with DVT may contract a pulmonary embolism (PE) when a part of the clot reaches the lungs and blocks a pulmonary artery, which may be life-threatening. Risk factors for venous thromboembolism (VTE = DVT and/or PE) in the general population include older age, former VTE, hypercoagulability, pelvic or lower extremity fracture, cancer, tobacco use, obesity, pregnancy, immobilization, congestive heart failure, and recent major surgery (Anderson & Spencer, 2003; Galson, 2008).
VTE is an important concern in persons with traumatic spinal cord lesion (SCL), where it can occur because of alternation of blood vessels, hypercoagulability, and venous stasis due to paralysis (Hassouna, 2000; Miranda & Hassouna, 2000; Yue et al., 2017). Without adequate prophylaxis, VTE rates following traumatic SCL may range between 7% and 100% (Dhall et al., 2013; Fujii et al., 1992; Wei et al., 2023). Older age, male gender, complete paralysis, and concurrent traumatic injuries are risk factors for VTE in people with SCL. Spinal surgery, personal or family history of VTE, smoking, and diabetes are also risk factors (Piran & Schulman, 2016; Tator et al., 1987; Wei et al., 2023). Individuals with non-traumatic SCL may be similarly at risk for VTE, which can appear before or after surgery (Chung et al., 2011; Yamada et al., 2019).
Current recommendations include preventive anticoagulation following SCL, predominantly with low-molecular-weight heparin (LMWH), starting within 72 hours after lesion onset (Fehlings et al., 2018). Some studies have recommended continuing prophylaxis for at least 12 weeks after patient stabilization, at which point the risk of DVT after SCL declines considerably (Giorgi Pierfranceschi et al., 2013). Recently, a direct oral anticoagulant (DOAC) has been considered for SCL VTE prophylaxis, but satisfactory research on its safety and efficacy following SCL is lacking (Weidner et al., 2020).
The benefit of preventive anticoagulation is always weighed against the risk of bleeding, which may be a considerable side effect of anticoagulation (Eichinger et al., 2018). The assessment of relative risks and the adapted anticoagulant regimens vary between patients, spinal units, and studies (de Almida et al., 2019; Hamidi et al., 2019).
Despite efforts to reduce VTE morbidity with current anticoagulant regimens, VTE and bleeding events still occur and may be fatal, suggesting that prophylaxis is not optimal yet (Arnold et al., 2017; Bělohlávek et al., 2013; Klemen et al., 2020; Søgaard et al., 2014). We conducted the present study to evaluate the need and possibility to improve VTE prophylaxis, after assessing the effectiveness and risks of anticoagulation in adult SCL patients undergoing rehabilitation.
2Methods
2.1Patients
We retrospectively collected the data of patients admitted to the Spinal Department of a Rehabilitation Medical Center between 2010 and 2019. Inclusion criteria were age≥18 and admission up to 3 months after traumatic or non-traumatic SCL onset. For traumatic SCL, we defined the lesion onset date as the date of the event, and for non-traumatic SCL, the date on which the neurological deficit first appeared in the medical records. Exclusion criteria were being discharged from the department after less than 1 week and lack of data required for the study analyses.
2.2Procedure
The sources of participant and SCL data were the records of the Rehabilitation Medical Center and a shared hospital-community database. The data included information on clinical follow-up 1 year or more after SCL onset, and on VTE prevention and outcomes for all participants. The main outcomes were the incidence of clinically diagnosed DVT, PE, clinically significant bleeding events or thrombocytopenia related to anticoagulant treatment, and death, which occurred within 1 year after SCL onset.
The DVT and PE diagnoses were made by clinicians who cared for the participants. They screened the rehabilitation inpatients for SCL complications, including VTE, on a weekly basis. They based DVT diagnosis on clinical symptoms, including swelling, redness, warmth, pain, or tenderness of the limb. They frequently verified the diagnosis with ultrasound. They based PE diagnosis on shortness of breath, unexplained new tachycardia, chest pain, bloody sputum, and/or laboratory blood gas tests, frequently verified by pulmonary CT-angiography.
2.3Statistical analyses
Patient characteristics and outcomes are described by means and standard deviations (SD) of continuous normally distributed variables; by medians, 25% –75% percentiles, for variables not normally distributed; and by counts and percentages for categorical variables with confidence intervals (CI) for important outcomes. To assess the association of VTE with continuous variables such as age, we used independent samples T-tests with appropriate transformations for not normally distributed data. To examine relationships between VTE incidence and categorical variables, we used Chi-square analysis, the Fisher’s exact test when expected counts were less than 5, or we calculated odds ratios (OR) with 95% CI. We assessed the association between the duration of prophylactic anticoagulation (after a natural logarithm transformation) and SCL characteristics with analysis variance (ANOVA). We determined statistical significance at P < 0.05 and performed all statistical analyses with SPSS v 27 (IBM Corp., Armonk, NY, USA).
2.4Ethical consideration
The ethics committee of the Rehabilitation Medical Center approved the study (approval number 003-13-LOE) and waived the requirement to obtain informed consent from the patients because the study was retrospective and investigators anonymized the data before analysis.
3Results
3.1Participants
Of 1,298 persons admitted to the department during the 10-year study period, 221 suffered from conditions other than SCL, such as Guillain-Barré syndrome or low back pain disability, 266 were admitted to rehabilitation more than 3 months after SCL onset, and 1 was younger than 18 years. Of the remaining 810, who conformed to the inclusion/exclusion criteria, we excluded 93 because they were less than 1 week in rehabilitation, and 32 because data about the anticoagulation received or follow-up for one year after SCL onset were missing. Six hundred eighty-five men and women were included in the final analysis. Of these, 666 arrived at rehabilitation without a VTE diagnosis. Table 1 shows patient characteristics.
Table 1
Characteristics of the study population
| Characteristic | All patients (n = 685) | Admitted without VTE (n = 666) |
| Age at admission, mean (SD) | 54 (17) | 54 (17) |
| Men, n (%) | 450 (65.7) | 437 (65.6) |
| BMI>30, n (%) | 95 (19.5) (n = 486) | 91 (19.3) (n = 472) |
| SCL etiology, n (%) | ||
| Traumatic | 270 (39.4) | 259 (38.9) |
| Non-traumatic | 415(60.6) | 407 (61.1) |
| Disc herniation | 195 (28.5) | 190 (28.5) |
| Spinal stenosis | 71 (10.4) | 70 (10.5) |
| Tumor | 37 (5.4) | 37 (5.5) |
| Vascular lesion | 29 (4.2) | 29 (4.4) |
| Myelopathy UO | 30 (4.4) | 30 (4.5) |
| Infection | 27 (3.9) | 25 (3.8) |
| Multiple sclerosis | 12 (1.8) | 12 (1.8) |
| Syringomyelia | 3(0.4) | 3(0.5) |
| Other | 11(1.6) | 11(1.6) |
| Days SCL, median (25–75 percentiles) | 22(14–37) | 21 (14–36) |
| Patients after spinal surgery, n (%) | 527 (76.9) | 511 (76.7) |
| Days surgery, median (25–75% percentiles) | 16 (10–27) | 15 (10–26) |
| SCL level, n (%) | ||
| Tetraplegia | 290 (42.3) | 280 (42) |
| Paraplegia | 395 (57.7) | 386 (58) |
| Admission AIS grade, n (%) | ||
| A | 79 (11.5) | 78 (11.7) |
| B | 29 (4.2) | 28 (4.2) |
| C | 134 (19.6) | 131 (19.7) |
| D | 443 (64.7) | 429 (64.4) |
| LOS, mean (SD) | 90(55) | 90 (55) |
Abbreviations and terms: VTE, Venous thromboembolism; Admitted without VTE, Patients admitted without VTE diagnosis; BMI, Body mass index; SCL, Spinal cord lesion; Myelopathy UO, Myelopathy of unknown origin; Days SCL, Time from SCL onset to admission; AIS grade = American Spinal Injury Association impairment scale grade.
3.2VTE risk, timing, and effect on length of stay in rehabilitation (LOS)
VTE was diagnosed in 37 patients, 5.4%, of all participants (95% CI 3.7–7.1%). Eighteen patients (2.6%) had a diagnosis of DVT, 17 (2.5%) of PE, and 2 (0.3%) of both DVT and PE. Clinical DVT diagnosis was verified by ultrasound at least in 65% of the patients, and clinical PE diagnosis by pulmonary CT-angiography at least in 58%.
Of the VTE diagnoses, 19 had been made before admission to rehabilitation, 9 after admission but before discharge, and 9 after discharge but within 1 year from SCL onset. Of the 18 (2.7%) patients who contracted VTE after admission to rehabilitation, 12 patients (1.8%) had a diagnosis of DVT, 5 (0.75%) of PE, and 1 (0.15%) of both DVT and PE. Sixteen of the 18 who contracted VTE after admission to rehabilitation amounted to 3% (95% CI 1.6–4.5%) of the patients who received preventive anticoagulation during rehabilitation. Table 2 details the characteristics of persons who contracted VTE.
Table 2
Characteristics of patients with venous thromboembolism
| Characteristic | VTE at any time (n = 37) | VTE after admission (n = 18) |
| Age at admission, mean (SD) | 52 (17) | 55 (18) |
| Men, n (%) | 24 (65) | 11 (61.1) |
| BMI>30, n (%) | 6 (22.2) (n = 27) | 2 (15.4) (n = 13) |
| SCL etiology, n (%) | ||
| Trauma | 17 (46) | 6 (33.3) |
| Not trauma | 20 (54) | 12 (66.7) |
| Disc herniation | 12 (32.4) | 7 (38.9) |
| Spinal stenosis | 1 (2.7) | |
| Tumor | 2 (5.4) | 2 (11.1) |
| Vascular | 2 (5.4) | 2 (11.1) |
| Infection | 2 (5.4) | |
| Syringomyelia | 1 (2.7) | 1 (5.6) |
| SCL level, n (%) | ||
| Tetraplegia | 14 (37.8) | 5 (27.8) |
| Paraplegia | 23 (62.2) | 13 (72.2) |
| Patients after spinal surgery, n (%) | 29 (78.4) | 13 (72.2) |
| Admission AIS grade, n (%) | ||
| A | 5 (13.5) | 4 (22.2) |
| B | 3 (8.1) | 2 (11.1) |
| C | 9 (24.3) | 6 (33.3) |
| D | 20 (54.1) | 6 (33.3) |
| Personal history of VTE, n (%) | 4 (10.8) | 3 (16.7) |
| VTE Risk factors other than SCL, n (%) | 8 (21.6) | 7 (38.9) |
| Type of VTE, n (%) | ||
| Deep vein thrombosis (DVT) | 18 (48.6) | 12 (66.7) |
| Pulmonary embolism (PE) | 17(45.9) | 5 (27.8) |
| DVT+PE | 2 (5.4) | 1 (5.6) |
Abbreviations and terms: At any time, Before admission, after admission, or after discharge; Admission, Admission to rehabilitation; AIS grade, American Spinal Injury Association impairment scale grade; SCL, Spinal cord lesion; VTE, Venous thromboembolism; BMI, Body mass index; DVT, Deep vein thrombosis; PE, Pulmonary embolism.
Figure 1 shows the time from SCL onset to VTE. In 11 participants (29.7% of all the patients with VTE and 61% of those diagnosed after admission), VTE occurred 3 months or more after SCL onset (in all of them after the admission). Of them, 4 had an AIS grade A, 1 B, 3 C, and 3 D. None of them walked without aids at admission, and 1 was walking without aids 3 months after SCL onset. The SCL level was above C5 in 2 of them, T7-T12 in 8, and below L2 in 1. Eight of the 11 (73%) had risk factors other than the SCL, such as active cancer (Anderson & Spencer, 2003), severe infection (Crous-Bou et al., 2016), previous VTE (Anderson & Spencer, 2003; Piran & Schulman, 2016), chronic kidney disease (Wattanakit & Cushman, 2009), hip surgery (Anderson & Spencer, 2003; Galson, 2008), or drug abuse (Coull et al., 2021). Of the 26 patients who contracted VTE within 3 months of SCL onset, 1 had an AIS grade A, 2 B, 6 C, and 17 D. Two of them walked without aids at admission, and 5 were walking without aids 3 months after SCL onset. The SCL level was above C5 in 10 of them, C5-C8 in 2, T1-T6 in 2, T7-T12 in 2, and below L2 in 10. Only 4 of the 26 (15%) had additional risk factors (P = 0.001). Two of them had active cancer, and 2 had a previous VTE. Of the 7 patients who contracted VTE within 3 months of SCL onset but after admission, 1 (14%) had additional risk factors.
Fig. 1
Time from SCL onset to VTE diagnosis (months). Dark gray represents individuals with risk factors for VTE other than SCL. Light gray represents individuals with no documented risk factors.
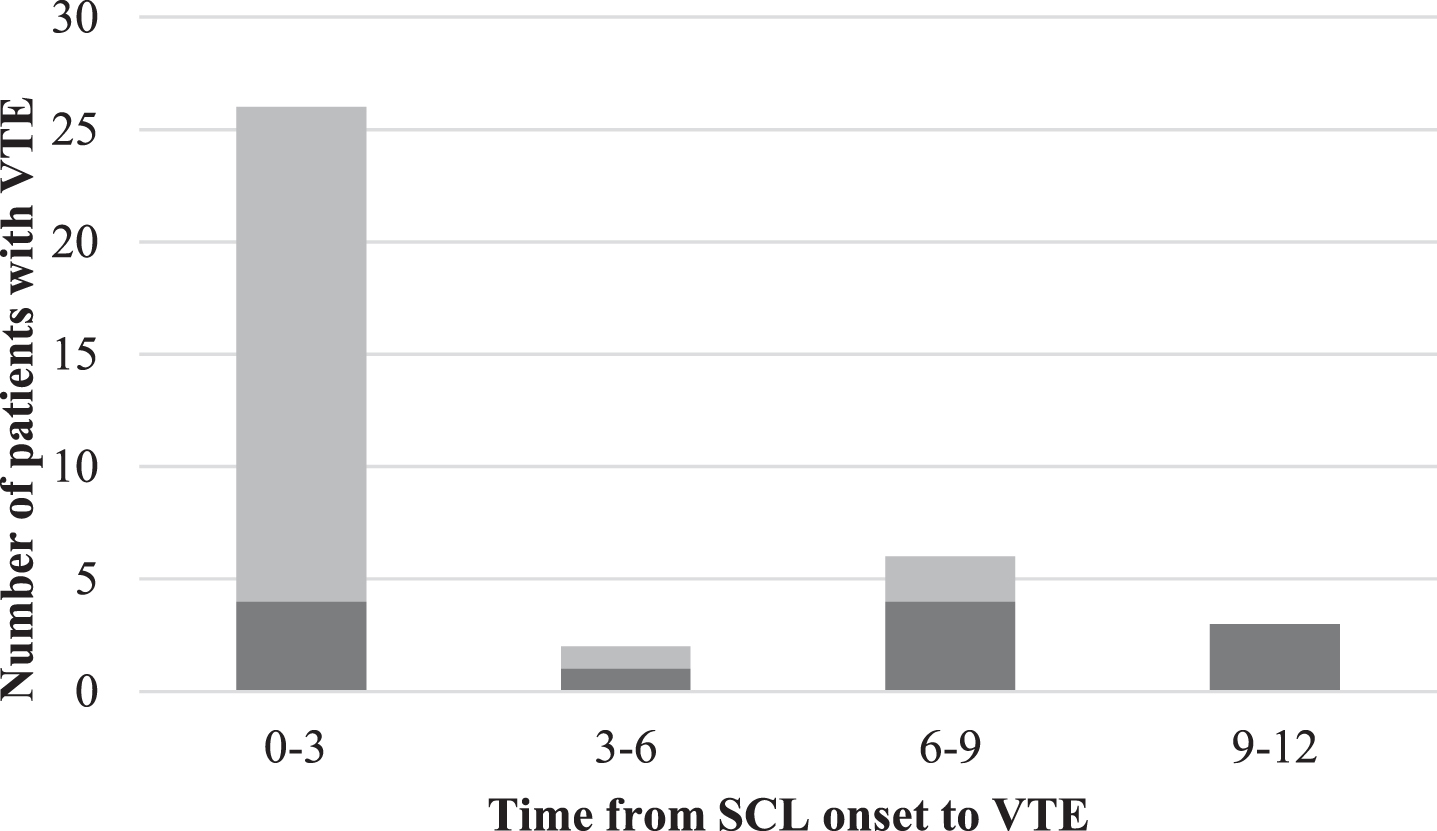
Of the 11 participants who contracted VTE 3 months or more after SCL onset, in 10 VTE occurred despite preventive anticoagulation, lasting 3.7–9.3 weeks, 35–262 days after discontinuing it, either at rehabilitation (3 patients) or after discharge. Of the 11, 8 patients received prophylactic anticoagulation with Enoxaparin 40 mg/day, 1 with Enoxaparin 60 mg/day and 1 was treated with Coumadin.
LOS was 89±55 days for the patients without a VTE diagnosis in the first year after SCL onset, compared with 103±61 days for all the patients with a VTE diagnosis after SCL onset (P > 0.1), and 118±53 days for the patients who contracted VTE after admission to rehabilitation (P < 0.04).
3.3Risk of death
Thirteen patients (1.9% of those included in the study) died within a year from SCL onset. Causes of death were infection (n = 7), cancer (n = 1), and PE (n = 1). The person who died after contracting clinically diagnosed PE was a 58-year-old woman with advanced cancer. She received preventive enoxaparin until 6.5 weeks after SCL onset, and PE occurred after discharge from rehabilitation, and 8.5 months after SCL onset. The cause of death of 4 individuals is unknown, but all of them suffered from medical problems in addition to the SCL.
3.4VTE risk factors
In the entire group of included individuals, as well as among the patients admitted to rehabilitation without a VTE diagnosis, those with former VTE were more likely to develop DVT or PE (OR = 8.6, 95% CI = 2.5–29.4; OR = 14.2, 95% CI = 3.5–57.8, respectively). Among the patients admitted to rehabilitation without a VTE diagnosis, VTE occurred in 5.1%, 7.1%, 4.6%, and 1.4%, in patients with AIS grades A, B, C, or D, respectively. The SCL level of the patients with AIS grades A–C was cervical in 35.9%, thoracic in 35.9%, and lumbar in 28.2%. In those with D, 45.4%, 15.4%, and 39.2%, respectively. The VTE risk was higher in those with AIS grades A–C than in those with grade D (OR = 3.8, 95% CI = 1.4–10.1). VTE risk was lower in patients who were walking with or without aids (OR = 0.14, 95% CI = 0.02–1.06, P = 0.026) and higher in patients with thoracic lesions (P = 0.022). However, both not-walking and thoracic level of lesion were associated with the AIS grades A–C (P < 0.001).
In all the patients, as well as in those admitted to rehabilitation without a VTE diagnosis, we found no significant relationships between VTE incidence and age, gender, BMI > 30, traumatic or non-traumatic etiology, or spinal surgery (P > 0.1, Tables 1 and 2).
3.5Prophylactic anticoagulant therapy
Of the 666 patients who arrived at rehabilitation without a VTE diagnosis, 526 (79%) received preventive anticoagulation during inpatient rehabilitation (some of them at therapeutic doses). As shown in Table 3, 480 (72%) received low-dose enoxaparin (≤60 mg/day), most commonly 40 mg/day. Enoxaparin prevention ended before discharge from inpatient rehabilitation for 97% of the patients receiving it. Enoxaparin at higher doses (≥80 mg/day), heparin, warfarin, or direct oral anticoagulants (DOACs) were prescribed for 46 patients (6.9%), 87% of whom had comorbidities such as atrial fibrillation. Ninety-four percent of the individuals treated with warfarin or DOACs were instructed to continue taking those medications after discharge, probably because of comorbidities. Of the 18 patients who contracted VTE during or after inpatient rehabilitation, 15 (83.3%) received preventive enoxaparin (most commonly 40 mg/day), 1 (5.6%) received warfarin for prevention, and 2 (11.1%) did not receive prophylactic anticoagulation, one because of good mobility at admission and the other because of relative contraindication for anticoagulation.
Table 3
Prophylactic anticoagulant therapy administered to the patients admitted to rehabilitation with no VTE diagnosis (n = 666)
| Medication | n (%) | Reasons for anticoagulation besides SCL, n |
| None | 140 (21.0) | |
| Enoxaparin≤60 mg/day | 480 (72) | |
| Enoxaparin≥80 mg/day | 6 (0.9) | Artery dissection, 3 |
| Warfarin | 9 (1.4) | Cardiac, 5Coagulation disorder, 2Spinal cord thrombosis, 1Past VTE,1 |
| UFH | 2 (0.3) | |
| DOACs | 7 (1.1) | Cardiac, 6Past VTE,1 |
| Enoxaparin+Warfarin | 10 (1.5) | Cardiac, 3Past VTE, 2Artery dissection, 2Spinal cord thrombosis, 2Coagulation disorder, 1 |
| Enoxaparin+DOACs | 8 (1.2) | Cardiac, 6Past VTE, 1 |
| Enoxaparin+UFH | 2 (0.3) | Cardiac, 1Artery dissection, 1 |
| Enoxaparin Warfarin+UFH | 1 (0.15) | Artery dissection, 1 |
| or Enoxaparin+Warfarin+DOACs | 1 (0--·15) | Cardiac, 1 |
Abbreviations and terms: UFH, Unfragmented heparin; SCL, Spinal cord lesions; DOACs, Direct Oral Anticoagulants (Dabigatran, Apixaban or Rivaroxaban); VTE, Venous thromboembolism.
In 4 of the 16 patients who received preventive anticoagulation and contracted VTE after admission, VTE occurred during anticoagulation, and in 12, 7–262 days after its discontinuation.
Table 3 also shows that 140 people with SCL (21%) did not receive preventative anticoagulation during rehabilitation. Reasons were a good level of mobility or strong muscle power (n = 92, 65.7%) more than 4–6 weeks from the onset of SCL or surgery to admission to rehabilitation (n = 34, 24.3%), medical reasons (n = 8, 5.7%), refusal of suggested treatment, (n = 3, 2.1%), and lack of contribution of the SCL to the decrease in mobility (n = 3, 2.1%). The difference in VTE incidence between the patients who received (3%) or did not receive (1.4%) preventive anticoagulation was non-significant (OR 2.2 95% CI 0.5–9.6).
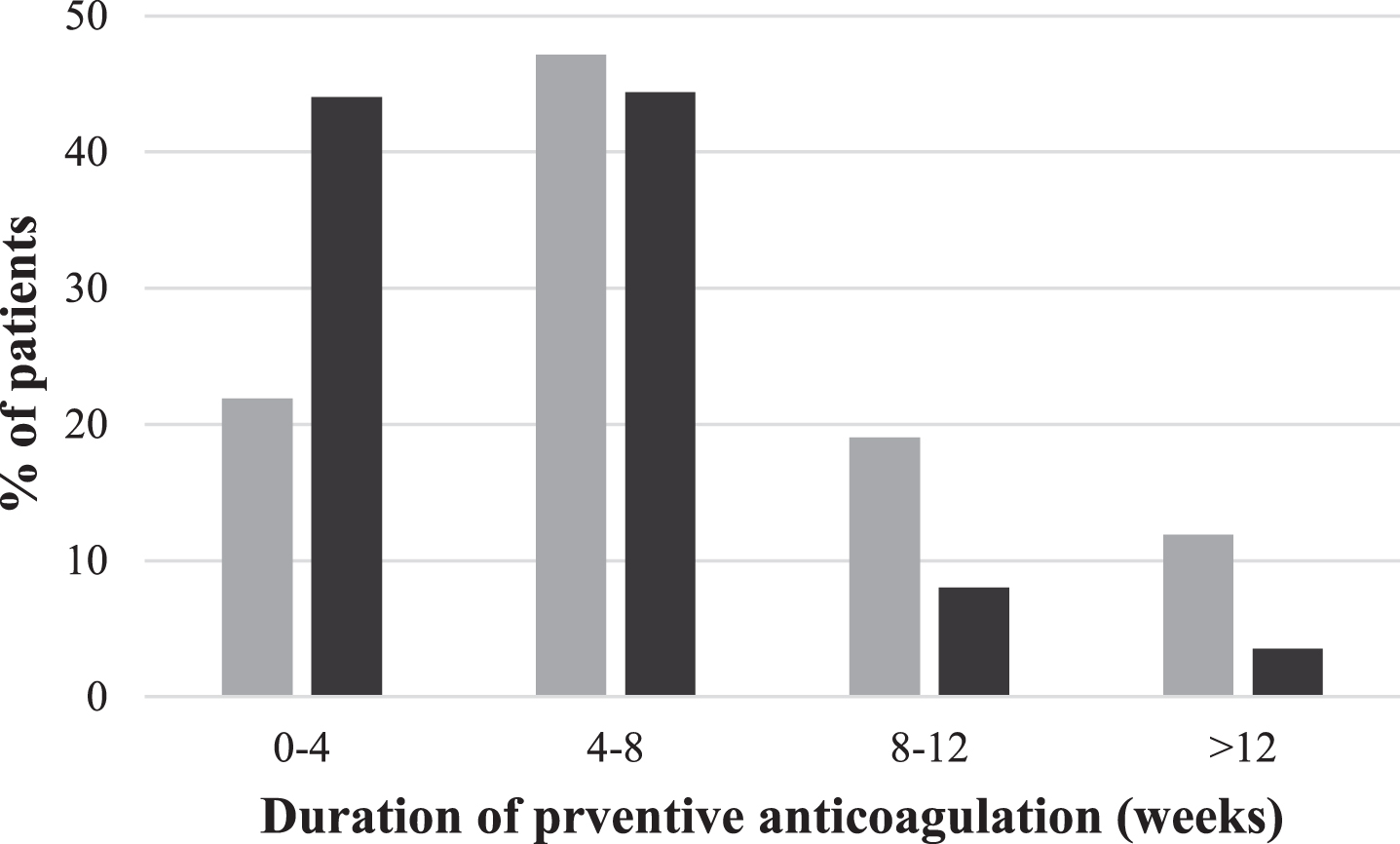
Prophylactic anticoagulation at rehabilitation started on the first day after admission in 94.7% of patients; only in 1.7% of patients it started 7–68 days after admission. The median duration of prophylactic anticoagulation during rehabilitation was 4.6 weeks (25% –75% percentiles = 3.1–6.6), and it continued until a median period of 6.4 weeks after SCL onset or spinal surgery (25% –75% percentiles = 5.8–9.7). Figure 2 demonstrates the duration of prophylactic anticoagulation during rehabilitation. Patients with AIS grades A–C received prophylaxis for 5.9 (4.1–8.6) weeks and those with grade D for 4.1 (2.7–5.3) weeks (P < 0.001) Lesion level did not affect the duration of preventive anticoagulation (P > 0.7). The average duration of preventative anticoagulation was 5 weeks for patients who contracted VTE and 5.6 weeks for those who did not (P > 0.4).
Fig. 2
Duration (weeks) of prophylactic therapy during impatient rehabilitation. Light gray bars represent patient with AIS grades A–C; dark gray bars represent patients with AIS grade D. The figure refers to patients admitted without a VTE diagnosis.
3.6Side effects of preventive anticoagulation
Side effects were recorded for 8 of the 526 patients who received preventive anticoagulation during SCL rehabilitation (1.5%, 95% CI 0.5–2.6%) as shown in Table 4. Seven patients (1.3%) had clinically significant bleeding and one (0.2%) had a diagnosis of thrombocytopenia. Of the major bleeding events and thrombocytopenia after SCL onset, 6 occurred following enoxaparin and 2 could be attributed to warfarin or DOACs, administered because of a spinal thrombus or atrial fibrillation (Table 4).
Table 4
Characteristics of patients who suffered side effects of preventive anticoagulation during SCL rehabilitation (n = 8)
| Age | Gender | SCL level | AIS grade | SE | SE timing | Anticoagulation at side effect onset |
| 72 | Male | Paraplegia | C | Bleeding (ureter) | 31 | Rivaroxaban 20 mg |
| 46 | Male | Paraplegia | B | Bleeding (hematuria) | 1 | Enox 80 mg |
| 71 | Male | Paraplegia | D | Bleeding (upper GI) | 2 | Enox 40 mg |
| 67 | Male | Paraplegia | D | Bleeding (upper GI) | 12 | Enox 40 mg |
| 77 | Male | Tetraplegia | C | Bleeding (GI) | 4 | Enox 40 mg |
| 84 | Female | Paraplegia | B | Thrombocytopenia | 8 | Enox 40 mg |
| 59 | Male | Tetraplegia | A | Bleeding (GI) | 62 | Enox 20 mg |
| 75 | Male | Tetraplegia | D | Bleeding (hematuria) | 12 | Enox 120 mg+Warfarin |
Abbreviations and terms: SCL, Spinal cord lesion; AIS, American Spinal Injury Association impatient scale grade; SE, side effect; SE timing, days from admission; Admission, Admission to rehabilitation; GI, Gastrointestinal; Enox, Enoxaparin.
4Discussion
4.1Main findings
The main findings of this study show that VTE prophylaxis in the investigated spinal rehabilitation department was effective relative to historic VTE rates without prophylaxis, but limited. In this study, VTE incidence in the patients who received preventive anticoagulation after arriving at rehabilitation was much lower than it may have been without anticoagulation, and it was not fatal in patients whose SCL was the only VTE risk factor (Dhall et al., 2013; Fujii et al., 1992; Wei et al., 2023). VTE at rehabilitation prolonged LOS, however, and the present prophylaxis was insufficient. More than 5% of all the SCL patients who arrived at rehabilitation and 3% of those who received preventive anticoagulation in rehabilitation still contracted VTE, which was fatal in a patient with an additional risk factor, despite the preventive measures.
VTE and mortality percentages presented here are, respectively, compatible with rates described previously for persons with SCL or following surgery, who received preventive anticoagulation (Arnold et al., 2017; Junqueira et al., 2017), or for patients at elevated risk of VTE, who received preventive anticoagulation and who contracted PE (Bělohlávek et al., 2013; Klemen et al., 2020; Søgaard et al.,2014).
4.2Possible shortcomings of the anticoagulation regimen used
Several possible shortcomings of the anticoagulation regimen used may have contributed to limiting the reduction in VTE rate. These include lack of prophylactic anticoagulation in certain patients, short duration, inadequate dose, and inadequate attention paid to VTE risk factors.
4.2.1No prophylactic anticoagulation for 21% of the patients
Although physicians considered that in the group of 140 patients who did not receive preventive anticoagulation during rehabilitation the risk of VTE was low because of the relatively mild SCL or the long time after SCL onset, 2 of these individuals developed VTE. The lack of significant difference in VTE rate between the patients who received prophylaxis and those who did not, shows that preventive anticoagulation decreased VTE incidence in patients considered to have a higher risk to that of patients who were presumed to be in the low-risk group. The VTE rate in both groups indicates that both groups were insufficiently anticoagulated. The data suggest that anticoagulation of all SCL patients without contra-indication during rehabilitation, regardless of SCL severity, may improve VTE prevention.
4.2.2Short duration of anticoagulation
Fewer than 20% of the patients continued prophylaxis more than 3 months after SCL onset, but in 10 of 16 patients who contracted VTE after receiving preventive anticoagulation, VTE occurred after that period, that is, after prophylaxis was discontinued. This suggests that the duration of preventive anticoagulation was too short. Yet, in 2 prospective studies, with a median VTE prophylaxis duration longer than that in our study, VTE rate was similar or higher. With preventive 40 mg enoxaparin daily for 8 weeks, starting within 5 days of SCL onset, VTE appeared in 5.4% of patients (Halim et al., 2014). With prophylactic LMWH for a median duration of 7 months, throughout rehabilitation, VTE rate was even higher (Giorgi Pierfranceschi et al., 2013). Based on these studies, it appears that prolonging anticoagulation at the standard preventive dose for the entire SCL patient group may not improve VTE prevention. Prolongation of preventive anticoagulation may be beneficial, however, for SCL patients with additional VTE risk factors, such as those who were involved in many of the late VTE events, in the present study.
4.2.3Inadequate dose of anticoagulation
Despite a standard preventive regimen of 40 mg enoxaparin daily for most SCL patients, VTE events were more frequent than those of bleeding and thrombocytopenia, and one VTE case was fatal. The risk of clinically significant bleeding was lower than that of VTE, in this study, and none of the bleeding patients died. This suggests that the customary preventive enoxaparin dose may be rather low. Yet, a retrospective study showed that an increased preventive dose of 60 mg enoxaparin daily was not more effective than the standard 40 mg dose (Hebbeler et al., 2004). Based on this study, it appears, therefore, that using a higher fixed preventive dose of anticoagulation may not improve VTE prevention either.
It is possible, however, that an adjusted dose, adapted to body weight, will improve VTE prevention. This was demonstrated in patients with burns (Cronin et al., 2019), and SCL VTE prevention guidelines recommended an adjustment of the LMWH dose for patients with low or very high body weight (Weidner et al., 2020). Such adjustment can be adapted to any body weight and may limit the risk of bleeding (Cronin et al., 2019; Martin et al., 2021; Thomas et al., 2015).
4.2.4Inadequate attention paid to VTE risk factors
Except for refraining from anticoagulation in the case of many patients with mild SCL, in the present sample anticoagulation was not adapted to the patients’ VTE risk factors. Former VTE, however, was found to be a significant VTE risk factor. Higher AIS grades increased the risk among patients admitted to rehabilitation without a VTE diagnosis. In patients who contracted VTE more than 3 months after lesion onset, the rate of additional risk factors was high. Previous studies showed that a complete lesion (AIS grades A or B) and factors such as hypercoagulability, femoral fracture, or cancer were risk factors in SCL patients (Clements et al., 2017; Wei et al., 2023). We suggest, therefore, that anticoagulation be adapted to the patients’ VTE risk factors to enhance VTE prevention after SCL.
4.3Recommendation
Based on our findings and the above discussion, we recommend conducting a prospective study aimed at assessing the efficacy and safety of:
1. Starting or continuing preventive enoxaparin for all SCL patients arriving to rehabilitation without a contra-indication for anticoagulation immediately after admission. This is the earliest start possible in rehabilitation, although it may not comply with the recommendation to start prophylaxis within 72 hours of SCL onset (Aito et al., 2002).
2. Administering a preventive enoxaparin dose of 40 mg daily for patients with AIS grade D and those with grade C who walk without aids, weigh 50 Kgs or more, and have no major VTE risk factors.
3. Administering a preventive enoxaparin dose of 0.8 mg/Kg body weight for patients who weigh less than 50 Kgs, and for patients with major VTE risk factors, or those with AIS grades A or B and those with grade C who do not walk without aids. The suggested dose is higher than that used in this study for most patients, but lower for low-weight patients. It is 40% of the recommended therapeutic dose, follows recommendations for adapting the dose to body weight after SCL, and fits the dose that showed efficacy and safety in obese patients (Smythe et al., 2016; Wang et al., 2014; Weidner et al., 2020).
4. In case of renal failure, all doses should be reduced according to current guidelines.
5. Discontinuing prophylactic anticoagulation after 6 weeks of walking without aids but not longer than 24 weeks after SCL onset, for SCL patients with no significant VTE risk factors besides the SCL. Discontinuing anticoagulation 12 weeks after SCL onset for patients who walk without aids and have significant VTE risk factors besides the SCL, and those who do not walk without aids and have no significant VTE risk factors besides the SCL. Discontinuing anticoagulation 24 weeks after onset for patients who do not walk without aids and have additional significant VTE risk factors. The suggested durations of anticoagulation are compatible with our findings and with the duration recommended in the guidelines (Weidner et al., 2020).
We expect the suggested enoxaparin regimen to reduce VTE incidence, with a limited increase in bleeding. We also expect that administering enoxaparin to all SCL patients arriving in rehabilitation without a contra-indication, with the suggested doses, timing for starting and discontinuing it, and the adjustment to VTE risk factors will improve the efficacy of prophylaxis.
In addition to seeking ways of improving LMWH VTE prevention, studies are needed to test the safety and efficacy of DOACs for preventive anticoagulation (Weidner et al., 2020 If DOACs prove at least as safe and effective for this purpose as LMWH, they may provide more convenient VTE prophylaxis.
4.4Study limitations
As a result of the retrospective nature of the study, information on VTE incidence and prophylaxis before admission to rehabilitation is missing, and in many cases, documentation of objective VTE imaging was not found. Nevertheless, there is no reason to assume that VTE incidence was lower in patients who were not referred to the studied rehabilitation department, and a rate of 3–5%, probably represents the minimal VTE incidence after SCL in the entire study population. Objective VTE imaging for PE and DVT was documented in 58% and 65% of patients, respectively, and in the patients without it, the clinical diagnosis would have been confirmed in at least an additional 14% and 21% (Line, 2001; Markel et al., 1995). This means that at least 72% and 86% of the VTE diagnoses were solid, and VTE incidence after SCL and standard anticoagulation remains considerable, higher than bleeding, and warrants the prospective study we recommend.
5Conclusions
The VTE prophylaxis used for the cohort described here contributed to a considerable but limited reduction of VTE incidence. Several possible shortcomings of the anticoagulation regimen used may have contributed to the limited reduction in VTE rate. To overcome these shortcomings, we recommend conducting a prospective study to assess the safety and efficacy of enoxaparin starting immediately after admission to rehabilitation, with a dose and duration adapted to patient VTE risk factors and contra-indications for anticoagulation. We also support conducting studies with DOACs following SCL to improve the safety and efficacy of VTE prevention.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
The work was supported by a Loewenstein Rehabilitation Medical Center fund (KM600010309).
Ethics statement
The ethics committee of Loewenstein Rehabilitation Medical Center approved the study (number 003-13-LOE) and waived the need for obtaining informed consent from patients because the study was retrospective and the investigators anonymized the data before analysis.
References
1 | Aito, S. , Pieri, A. , D’Andrea, M. , Marcelli, F. , & Cominelli, E. ((2002) ). Primary prevention of deep venous thrombosis and pulmonary embolism in acute spinal cord injured patients. Spinal Cord 40: (6), 300–303. |
2 | de Almeida, R. L. , Rodrigues, C. C. , Melo e Silva, C. A. , Beraldo, P. S. S. , & Amado, V. M. ((2019) ). Comparison of two pharmacological prophylaxis strategies for venous thromboembolism in spinal cord injury patients: a retrospective study. Spinal Cord 57: (10), 890–896. |
3 | Anderson F. A. Jr, , & Spencer, F. A. ((2003) ). Risk factors for venous thromboembolism. Circulation 107: (23_suppl_1), I-9. |
4 | Arnold, P. M. , Harrop, J. S. , Merli, G. , Tetreault, L. G. , Kwon, B. K. , Casha, S. , & Norvell, D. C. ((2017) ). Efficacy, safety, and timing of anticoagulant thromboprophylaxis for the prevention of venous thromboembolism in patients with acute spinal cord injury: a systematic review. Global Spine Journal 7: (3_suppl), 138S–150S. |
5 | Belohlávek, J. , Dytrych, V. , & Linhart, A. ((2013) ). Pulmonary embolism, part I: Epidemiology, risk factors and risk stratification, pathophysiology, clinical presentation, diagnosis and nonthrombotic pulmonary embolism. Experimental and Clinical Cardiology, 18: (2), 129–138. |
6 | Clements, R. , Churilov, L. , Wahab, A. L. A. , & Ng, L. C. ((2017) ). Exploratory analysis of factors associated with venous thromboembolism in Victorian acute traumatic spinal cord-injured patients 2010–2013. Spinal Cord 55: (1), 74–78. |
7 | Coull, A. F. , Kyle, R. G. , Hanson, C. L. , & Watterson, A. E. ((2021) ). Risk factors for leg ulceration in people who inject drugs: A cross-sectional study. Journal of Clinical Nursing 30: (11-12), 1623–1632. |
8 | Cronin, B. J. , Godat, L. N. , Berndtson, A. E. , Pham, A. , Kolan, S. , Box, K. , & Costantini, T. W. ((2019) ). Anti-Xa guided enoxaparin dose adjustment improves pharmacologic deep venous thrombosis prophylaxis in burn patients. Burns 45: (4), 818–824. |
9 | Crous-Bou, M. , Harrington, L. B. , & Kabrhel, C. ((2016) ). Environmental and genetic risk factors associated with venous thromboembolism. In Seminars in Thrombosis and Hemostasis (Vol. 42: , No. 08, pp. 808–820). Thieme Medical Publishers. |
10 | Chung, S. B. , Lee, S. H. , Kim, E. S. , & Eoh, W. ((2011) ). Incidence of deep vein thrombosis after spinal cord injury: a prospective study in 37 consecutive patients with traumatic or nontraumatic spinal cord injury treated by mechanical prophylaxis. Journal of Trauma and Acute Care Surgery 71: (4), 867–871. |
11 | Dhall, S. S. , Hadley, M. N. , Aarabi, B. , Gelb, D. E. , Hurlbert, R. J. , Rozzelle, C. J. , & Walters, B. C. ((2013) ). Deep venous thrombosis and thromboembolism in patients with cervical spinal cord injuries. Neurosurgery 72: (suppl 3), 244–254. |
12 | Eichinger, S. , Eischer, L. , Sinkovec, H. , Wittgruber, G. , Traby, L. , Kammer, M. , & Wildburger, R. ((2018) ). Risk of venous thromboembolism during rehabilitation of patients with spinal cord injury. PLoS One 13: (3), e0193735. |
13 | Fehlings, M. G. , Tetreault, L. A. , Wilson, J. R. , Kwon, B. K. , Burns, A. S. , Martin, A. R. , & Harrop, J. S. ((2017) ). A clinical practice guideline for the management of acute spinal cord injury: introduction, rationale, and scope. Global Spine Journal 7: (suppl 3), 84S–94S. |
14 | Fujii, Y. , Mammen, E. F. , Farag, A. , Muz, J. , Salciccioli, G. G. , & Weingarden, S. T. ((1992) ). Thrombosis in spinal cord injury. Thrombosis Research 68: (4-5), 357–368. |
15 | Galson S. K. ((2008) ). Prevention of deep vein thrombosis and pulmonary embolism. Public Health Reports 123: (4), 420–421. |
16 | Giorgi Pierfranceschi, M. , Donadini, M. P. , Dentali, F. , Ageno, W. , Marazzi, M. , Bocchi, R. , & Imberti, D. ((2013) ). The short- and long-term risk of venous thromboembolism in patients with acute spinal cord injury: a prospective cohort study. Thrombosis and Haemostasis 109: (1), 34–38. |
17 | Halim, T. A. , Chhabra, H. S. , Arora, M. , & Kumar, S. ((2014) ). Pharmacological prophylaxis for deep vein thrombosis in acute spinal cord injury: an Indian perspective. Spinal Cord 52: (7), 547–550. |
18 | Hamidi, M. , Zeeshan, M. , Kulvatunyou, N. , Mitra, H. S. , Hanna, K. , Tang, A. , & Joseph, B. ((2019) ). Operative spinal trauma: thromboprophylaxis with low molecular weight heparin or a direct oral anticoagulant. Journal of Thrombosis and Haemostasis 17: (6), 925–933. |
19 | Hassouna H. I. ((2000) ). Blood stasis, thrombosis and fibrinolysis. Hematology/oncology clinics of North America 14: (2), xvii–xxii. |
20 | Hebbeler, S. L. , Marciniak, C. M. , Crandall, S. , Chen, D. , Nussbaum, S. , & Mendelewski, S. ((2004) ). Daily vs twice daily enoxaparin in the prevention of venous thromboembolic disorders during rehabilitation following acute spinal cord injury. The Journal of Spinal Cord Medicine 27: (3), 236–240. |
21 | Junqueira, D. R. , Zorzela, L. M. , & Perini, E. ((2017) ). Unfractionated heparin versus low molecular weight heparins for avoiding heparin-induced thrombocytopenia in postoperative patients. Cochrane Database of Systematic Reviews, (4). |
22 | Klemen, N. D. , Feingold, P. L. , Hashimoto, B. , Wang, M. , Kleyman, S. , Brackett, A. , & Pei, K. Y. ((2020) ). Mortality risk associated with venous thromboembolism: a systematic review and Bayesian meta-analysis. The Lancet Haematology 7: (8), e583–e593. |
23 | Line, B. R. (2001). Pathophysiology and diagnosis of deep venous thrombosis. In Seminars in nuclear medicine (Vol. 31, No. 2, pp. 90-101). WB Saunders. |
24 | Markel, A. , Weich, Y. , & Gaitini, D. ((1995) ). Doppler ultrasound in the diagnosis of venous thrombosis. Angiology 46: (1), 65–73. |
25 | Martin, A. M. , Polistena, P. , Mahmud, A. , Bettridge, B. , Morling, A. , Chuah, H. , & Leahy, M. F. ((2021) ). Optimal enoxaparin dosing strategies for venous thromboembolism prophylaxis and treatment of high body weight patients. Thrombosis Research 207: , 116–122. |
26 | Miranda, A. R. , & Hassouna, H. I. ((2000) ). Mechanisms of thrombosis in spinal cord injury. Hematology/Oncology Clinics of North America 14: (2), 401–416. |
27 | Piran, S. , & Schulman, S. ((2016) ). Incidence and risk factors for venous thromboembolism in patients with acute spinal cord injury: a retrospective study. Thrombosis Research, 147: , 97–101. |
28 | Smythe, M. A. , Priziola, J. , Dobesh, P. P. , Wirth, D. , Cuker, A. , & Wittkowsky, A. K. ((2016) ). Guidance for the practical management of the heparin anticoagulants in the treatment of venous thromboembolism. Journal of Thrombosis and Thrombolysis 41: , 165–186. |
29 | Søgaard, K. K. , Schmidt, M. , Pedersen, L. , Horváth–Puhó, E. , & Sørensen, H. T. ((2014) ). 30-year mortality after venous thromboembolism: a population-based cohort study. Circulation 130: (10), 829–836. |
30 | Tator, C. H. , Duncan, E. G. , Edmonds, V. E. , Lapczak, L. I. , & Andrews, D. F. ((1987) ). Comparison of surgical and conservative management in 208 patients with acute spinal cord injury. Canadian Journal of Neurological Sciences 14: (S1), 60–69. |
31 | Thomas, O. , Lybeck, E. , Strandberg, K. , Tynngård, N. , & Schött, U. ((2015) ). Monitoring low molecular weight heparins at therapeutic levels: dose-responses of, and correlations and differences between aPTT, anti-factor Xa and thrombin generation assays. PLoS One 10: (1), e0116835. |
32 | Wang, T. F. , Milligan, P. E. , Wong, C. A. , Deal, E. N. , Thoelke, M. S. , & Gage, B. F. ((2014) ). Efficacy and safety of high-dose thromboprophylaxis in morbidly obese inpatients. Thrombosis and Haemostasis 111: (01), 88–93. |
33 | Wattanakit, K. , & Cushman, M. ((2009) ). Chronic kidney disease and venous thromboembolism: epidemiology and mechanisms. Current Opinion in Pulmonary Medicine 15: (5), 408. |
34 | Wei, B. , Zhou, H. , Liu, G. , Zheng, Y. , Zhang, Y. , Hao, C. , Wang, Y. , Kang, H. , Lu, X. , Yuan, Y. , & Meng, Q. ((2023) ). Risk factors for venous thromboembolism in patients with spinal cord injury: A systematic review and meta-analysis. The Journal of Spinal Cord Medicine 46: (2), 181–193. |
35 | Weidner, N. , Müller, O. J. , Hach-Wunderle, V. , Schwerdtfeger, K. , Krauspe, R. , Pauschert, R. , Waydhas, C. , Baumberger, M. , Göggelmann, C. , Wittgruber, G. , Wildburger, R. , & Marcus, O. ((2020) ). Prevention of thromboembolism in spinal cord injury -S1 guideline. Neurological Research and Practice 2: , 43. |
36 | Yamada, K. , Suda, K. , Matsumoto Harmon, S. , Komatsu, M. , Ushiku, C. , Takahata, M. , Minami, A. , & Iwasaki, N. ((2019) ). Rapidly progressive cervical myelopathy had a high risk of developing deep venous thrombosis: a prospective observational study in 289 cases with degenerative cervical spine disease. Spinal Cord 57: (1), 58–64. |
37 | Yue, J. K. , Winkler, E. A. , Rick, J. W. , Deng, H. , Partow, C. P. , Upadhyayula, P. S. , Birk, H. S. , Chan, A. K. , & Dhall, S. S. ((2017) ). Update on critical care for acute spinal cord injury in the setting of polytrauma. Neurosurgical Focus 43: (5), E19. |


