
Visual rehabilitation indicating neuroplasticity in an esotropic adult patient with diplopia after sudden visual acuity loss in the non-amblyopic eye: A case report
Abstract
BACKGROUND:
The aim of this case report is to present the successful management of both diplopia and amblyopia in a specific clinical situation, demonstrating neuroplasticity of the visual system in an adult patient. Causes of diplopia include eye pathologies in monocular diplopia and ischemic ocular motor nerve palsies, sudden life-threatening and chronic conditions in central nervous system in binocular diplopia. Strabismic amblyopia and nonarteritic anterior ischemic optic neuropathy are quite often ophthalmic conditions, first one is caused by suppression during developmental period and the latter one by ischemia of the optic nerve in adults. Coexistence of aforementioned conditions may cause unusual clinical situation in which ability of nervous system to functional reorganization could be demonstrated.
CASE PRESENTATION:
In our adult patient, diplopia was incited by the loss of suppression of the strabismic amblyopic eye, which was the consequence of a sudden decrease of the visual acuity in the previously better eye in the course of nonarteritic anterior ischemic optic neuropathy. This led to impairment in daily activities.
RESULTS:
Visual training rehabilitation improved distance and near visual acuity in the amblyopic eye over three months, and prescribing two pairs of glasses with prisms enabled the patient to return to daily activities.
CONCLUSION:
The discussed patient lost the suppression of the strabismic amblyopic eye. Management of amblyopia is usually undertaken in children, however considering neuroplasticity we successfully attempted to improve visual functioning of our patient, despite lower intensity of neuroplasticity functions in an adult brain.
1Introduction
Diplopia refers to the symptom of seeing two images of a single object at the same time. In case where diplopia persists when the one eye is closed, we classify this condition as monocular diplopia, unlike the situation characteristic of binocular diplopia, when closing one eye causes the disappearance of double vision. Monocular diplopia is typically caused by pathologies of eye structures (e.g., corneal irregularities, dislocated lens or lens implant, cataract, iris defects, macular disease), whereas many neurological disorders such as ischemic ocular motor nerve palsies may produce binocular diplopia. However, other life-threatening conditions should also be considered, such as aneurysms, brain tumors, stroke, or giant cell arteritis. Diplopia could also exists in cerebral degenerative disease, myasthenia, decompensated phoria, or loss of cortical suppression (Pane et al., 2018). The cortical suppression phenomenon is a sensory adaptation to avoid double vision and is characterized by a reduced sensitivity to visual information from one eye under binocular conditions. In case of strabismus, long-term suppression of one eye can result in strabismic amblyopia, which is the most frequent amblyopia type caused by abnormal visual development early in life. Approximately half of all amblyopia cases in children are a strabismic category (de Zarate and Tejedor, 2007, Williams et al., 2008). Early detection and patching/penalization not suppressed eye to force the brain to use suppressed eye is gold standard treatment for amblyopia in children (Wallace DK et al., 2006). This management is most effective in young patients due to critical period of cortical plasticity, nevertheless successful treatment is possible outside this period (Gaier ED et al., 2017, Levi DM, 2011). As well as penalization of better eye in management of amblyopia, reduction of visual acuity in better eye may occur in the course of ophthalmic diseases e.g. nonarteritic anterior ischemic optic neuropathy (NAION). NAION is the most common clinical form of acute optic neuropathy in patients over 50 years of age (Hattenhauer et al., 1997). The reported incidence rate ranges from 2.3 to 10.2 per 100 000 people aged over 50 years (Hattenhauer et al., 1997; Johnson and Arnold, 1994). Patients suffer from painless visual acuity (VA) decrease and visual field loss in the form of altitudinal defects. Typically NAION manifests with optic disc edema without temporal artery tenderness and arteritis. The mean VA (visual acuity) of the affected eye is equal to 20/200 (range from 20/20 to light perception) (Hattenhauer et al., 1997). Typically VA worsens in the first two weeks and then is stable. Studies have demonstrated 3 lines or more improvement in VA in 13 to 42.7% of cases. So far, no report on effective medical or surgical treatment of NAION has been published. Similarly, there is no approach for preventing fellow eye involvement that occurs in 17–40% of cases (Atkins et al., 2010).
Here we present a case of female adult patient presenting with diplopia due to strike suppression in amblyopic eye in the course of NAION in non-amblyopic eye. Furthermore we present a successful management of simultaneous occurrence both amblyopia and diplopia using visual rehabilitation and optical solutions leading to increase of VA in amblyopic eye and decrease of esotropia. Aforementioned management was undertaken to prove neuroplasticity of visual system in an adult patient. Neuroplasticity is ability of the nervous system to change its activity in response to a stimulus by reorganizing its functions, structure, and connections (Mateos-Aparicio and Rodríguez-Moreno, 2019).
2Case presentation
A 71-year-old woman came for an optometric and ophthalmological examination because of her sudden onset of double vision. She reported two hospital stays in 2019 because of the optic disc edema in anamnesis. The patient reported that she was diagnosed with strabismus at the age of 6 (esotropia of left eye (LE)); however, she had neither operation nor visual training (VT) rehabilitation. Because of LE deprivation, her vision worsened with increasing age.
Optometric examination showed objective refraction: right eye (RE): sph + 4.00 cyl – 0.50/106° and LE: sph + 5.75 cyl – 1.25 /120° (Topcon RM– 8900). Subjective refraction at far showed for RE sph + 3.50 and LE sph + 4.25 cyl – 0.75/140°; at near for RE sph + 6.00 and LE sph + 6.75 cyl – 0.75/140°.
The best-corrected distance visual acuity (BCVA) was 0.7 RE and 1.0 LE (logMAR value). Corrected near visual acuity was 0.5 RE and 0.8 LE. The unilateral cover test at the distance result was 20-PD constant esotropia of the LE. At 40 cm, the cover test showed 30-PD constant esotropia of the LE. Red Lens Test in the nine diagnostic positions of gaze revealed esotropia of the LE.
The patient reported seeing five lights on the Worth 4-dot Test at 40 cm and 6 m in the dark and light examination room, indicating the LE’s constant esotropia in the primary gaze. Bagolini Striated Glasses Test showed normal retinal correspondence. Randot Stereogram testing could not be completed because of diplopia at a distance and near. Ocular motility testing found that the movements were not in full range and smooth in the RE and LE, and the patient had a problem with abduction in the LE. Pupils were equal, round, and reactive to light. Visuoscopy revealed central fixation in the RE and unsteady central fixation in the LE. The minimum amount of relieving prism that allowed for stable sensory fusion at far viewing distances was 12Δ base-out (BO), split equally between the eyes. For near vision, the amount was 20Δ base-out (BO), split equally between the eyes similarly. The patient got two pairs of glasses with prisms: far-distance prism lenses and near 3M Press-On Fresnel prisms. She reported difficulties with near-vision work due to blurry vision. We recommend using eye patching for near work.
The ocular findings were similar at the beginning and the end of visual training rehabilitation. Anterior segment examination of RE/LE revealed dry eye syndrome signs (LIPCOF 3), clear cornea, anterior chamber 3,0 mm deep, free, iris unremarkable, and incipient nuclear cataract. IOP for RE/LE was 18/19 mmHg, central corneal thickness RE/LE = 552/546μm. Posterior segment examination of RE showed a white optic disc with a sharp margin, C/D 0,4; macular drusen, sclerotic arteries and attached peripheral retina. Posterior segment examination of LE showed pale optic disc with sharp margin C/D 0,2; macular drusen, sclerotic arteries and attached peripheral retina attached, arteries were sclerotic. OCT of the macula and optic disc was performed. Central retinal thickness was 233 and 286μm for RE and LE, respectively. OCT of RE and LE: macular drusen – material under the retinal pigment epithelium (RPE), causing irregularities from RPE to the external limiting membrane (ELM). The RNFL imaging revealed global nerve fibers loss in the RE and LE (LE except for the inferotemporal sector), GCC complex was also severely impaired in both eyes, whereas changes were more prominent in RE.
We obtained MRI (signs of leukoaraiosis; multiple, small, ischemic changes; no other pathological focal changes), echocardiography (atherosclerosis plaques in the aorta; no other pathological findings), and carotid ultrasound (atherosclerosis plaques in ICA without hemodynamic influence). Laboratory tests (CBC, creatinine, GFR, CRP, Na, K, HDL within normal limits; LDL, cholesterol, and TG levels slightly elevated), neurological consultation (without pathological neurological symptoms, LE squint). The final diagnosis was NAION in the RE, and amblyopia, and squint in the LE. As neuroprotection, carbonic anhydrase inhibitors topically and vitamin B12 orally were recommended. Additionally, we suggested using artificial tears and nutritional supplements for AMD prophylaxis.
2.1Management and outcome
Based on the patient’s complaints and our clinical findings, a treatment program of three months of office and home VT rehabilitation was recommended to improve the LE’s visual acuity (VA), fusional ranges, and stabilization of fixation and extraocular motility. She was educated that the treatment goal was to reduce her symptoms by increasing the ability to compensate for esodeviation. The training involved: monocular therapy for the LE using Ann Arbor letter tracking, letter tracking, circle tracking, large Van Order Star; pursuit eye movements for LE and RE using Marsden ball, flashlight tracking, Visual Tracing Worksheet, pencils, Russell Ring; saccades for LE and RE using Hart Chart – column jumps, pencils; eye fixation monocular training using: Russel Ring with Yoked Prism and red filter. The aim of this type of training was to build steady central fixation, accurate pursuit and saccadic eye movements, and improving VA. Patient VT rehabilitation was conducted in-office with the therapist twice a week for an hour supplemented with procedures done at home three to four times a week between office visits. Ann Arbor letter tracking, letter tracking, circle tracking and Van Order Star was designed by using the appropriate threshold target size. The basic task was to find and circle a key sequence of letters and numbers. Fixation is more unstable in amblyopic so patient is taught to use the peak area of the amblyopic eye by searching and identifying threshold letters or targets. After two weeks patient was doing VT rehabilitation monocular with Yoked Prism, where the bases of the prisms were set in the four directions: left, right, up or down and using red filter. The following techniques are particularly suited also for home VT rehabilitation. Pursuit training was performed to increase motility for LE and RE. Several studies have shown that accurate smooth pursuit can improve the perception of spatial detail (Schütz AC et al., 2009), motion (Spering M et al., 2011) and color (Schütz AC et al., 2008). Marsden Ball was suspended from the ceiling and set in a swinging motion. The patient was looking at the target at the eye level for horizontal pursuit or from below by lying supine for circular pursuits. In flashlight techniques the patient’s task was to follow the therapists spot and to try to superimpose both spots of light. Visual Tracing techniques included series of intersecting lines on a piece of paper, each of this line was connected to a letter on one end and a number on the other. The purpose of this VT training was to match the number with the appropriate letter as the amblyopic eye sights along the line. The pencil and Russel Ring vision training was based on following the moving object in various directions by patient but in Russel ring the patient had to pointed in the circle. Saccadic eye movements were performed monocular and after each eye is shown to perform equally well, the VT rehabilitation may proceed to binocular training.
After three months of treatment (office and home sessions), visual parameters were improved. The patient subjectively noted that visual acuity was improved, and she could perform daily activities better. BCVA was 0.7 RE and 0.5 LE, whereas corrected near visual acuity was 0.5 RE and 0.6 LE. The unilateral cover test at a distance showed a 16-PD constant esotropia of the LE. At 40 cm, the cover test showed 20-PD constant esotropia of the LE. Ocular motility was much better in the LE. The minimum amount of relieving prism that allowed for stable sensory fusion at far viewing distances was 10Δ base-out (BO), split equally between the eyes. Improvement was noted also for near vision because we could prescribe 8Δ base-out (BO), split equally between the eyes. The patient got two pairs of glasses with prisms. An additional VT was implemented to focus on monocular therapy for the LE, red-green filters (anti-suppression Reading Bars, cards, TV-trainer), and fusional vergence ranges (Eccentric Circles – created especially for our patient). Antisuppression training has the effect of building sensory and motor fusion. The patients got different red – green tasks that were designed by using the appropriate threshold target size. Eccentric Circles were used to performed fixation training and increase fusional demand. The VT was performed in prescribe prisms glasses.
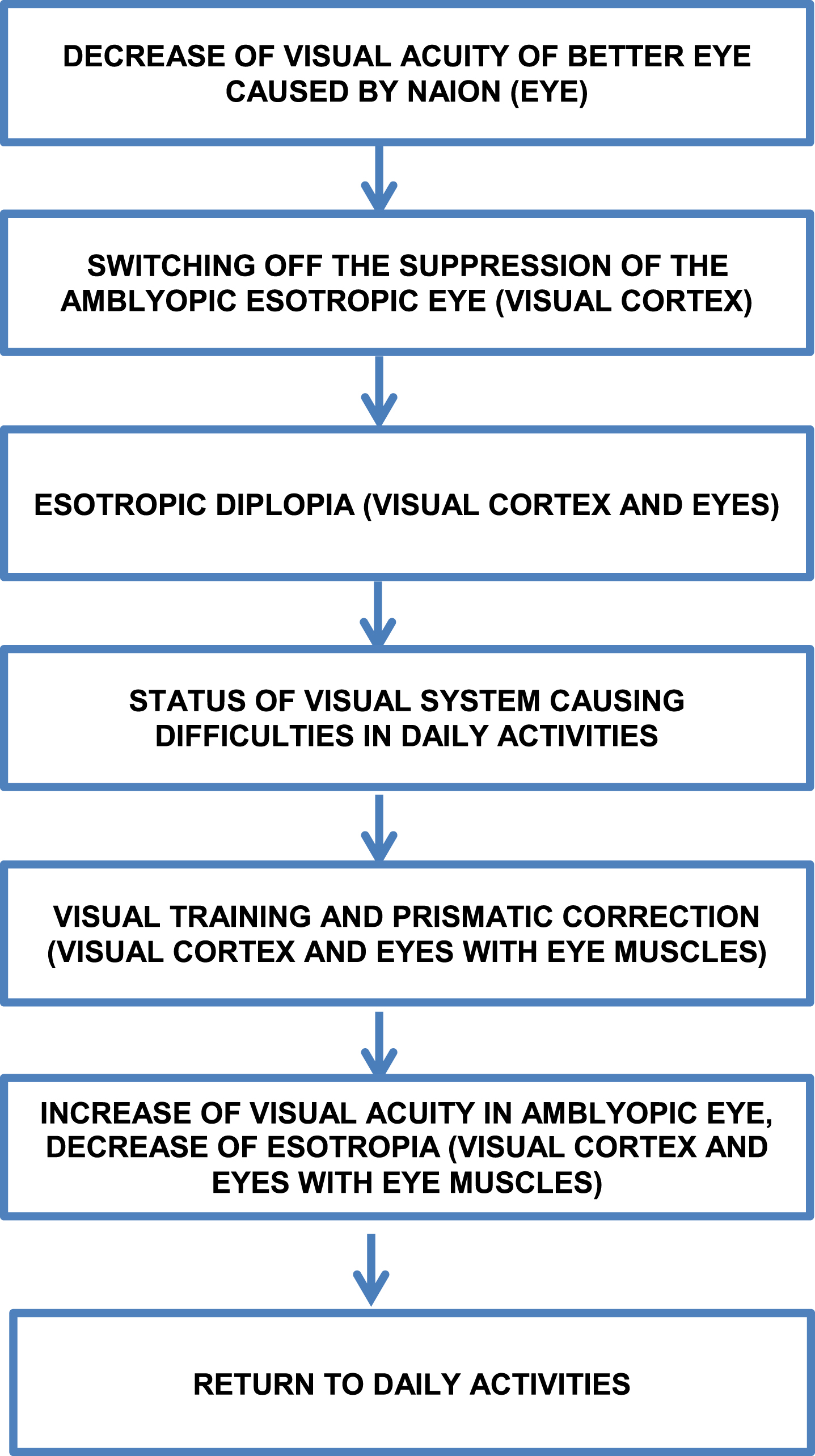
Changes in visual system status and daily performance of presented patient are summarized in Figure 1.
Fig. 1
Graphical summary of changes in visual system status and daily performance of our patient (Visual system part involved – in brackets).
3Discussion
Based on anamnesis and our clinical examination, we found that the patient lost the suppression of the strabismic amblyopic eye.
Amblyopia can be considered as the result of a lack of normal plasticity. Visual cortical dominance by the better eye leads to correspondent visual deprivation of the representations related to the eye with worse acuity. Different factors such as stroke, ocular, orbital, brain tumors, thyroid orbitopathy, myasthenia gravis, cranial nerve palsies, a sudden change in the angle of strabismus (e. g. postoperative), or prescription of new spectacle power can cause the elimination of suppression in the amblyopic eye and consequently decompensation of binocular vision (Pane et al., 2018).
In our patient, diplopia was caused by switching off the suppression of previously amblyopic and esotropic eye secondary to a tremendous decrease of BCVA in the previously better eye in the course of NAION. This phenomenon resulted from adaptation processes involving the visual cortex in our opinion. Because of diplopia, our patient had to patch the RE before attending to visual training. Notwithstanding single eye use (LE) she had problems in all daily activities, also with basic ones e.g., pouring water into a glass, caused by improper eye and hand coordination. After 3 months of monocular and binocular training she noticed improvement in her vision performance.
One of the standard therapy for amblyopia is occluding the dominant eye (de Buffon, 2005). Alotaibi group showed that near activities while patching in the treatment of anisometropic, strabismic, or combined amblyopia improves visual acuity more than patching alone (Alotaibi et al., 2012). Recently it has been suggested that patients with amblyopia have binocular cortical mechanisms for both thresholds that involve improving monocularly nondominant eye and binocularly training therapy. This theory shows that amblyopia and suppression are interconnected (Baker et al., 2008; Birch, 2013; Ding et al., 2013). Chen et al. revealed that decreased suppression from the fixating eye might not result from occlusion therapy (Chen et al., 2020). Hess et al. showed that reducing suppression and improving binocular fusion improves the visual acuity of the amblyopic eye (Hess et al., 2010).
Treatment for amblyopia is usually undertaken in young children; however, some studies show improvement in vision in adults (Levi and Polat, 1996; Hess et al., 2010). In our case, we showed that it is possible to improve visual functions in an adult patient with amblyopia. Amblyopia is a neural disorder that results from abnormal brain stimulation during visual development, and it is essential to understand the neural mechanisms of amblyopia to provide better treatment strategies for patients. Wong reviewed concepts of brain plasticity and their implications for novel therapeutic strategies that include binocular therapy and perceptual learning. This approach can be beneficial for children and adults with amblyopia (Wong, 2012).
Neuroplasticity covers all permanent functional and structural changes to the neurons, and could be divided in: developmental in children, compensatory in adults, induced by increased stimulus, related to learning, in the course of addiction and pathological. Neuroplasticity functions in an adult brain, however with lower intensity than during developmental period (Kossut, 2019). Draganski et al. proved that cortical plasticity is associated with anatomical changes in brain, examining areas processing complex visual motion after juggle training (Draganski et al., 2004). Lunghi et al. demonstrated long term visual function improvement of an amblyopic eye after inverse occlusion combined with physical exercise – cycling on a stationary bike (Lunghi et al., 2019).
Plasticity of the visual system – visual cortex allowed to achieve a successful outcome in an adult with amblyopia. Neural plasticity might permit visual recalibration and readaptation. Our observation is consistent with the reports of amblyopic patients whose VA increased over a period of time due to macular degeneration in non-amblyopic eye (El Mallah MK et al., 2000). The amblyopic visual system is an excellent model for testing recovery of visual function and provide evidence for neural plasticity in the adults (Levi DM, 2011).
Visual training is a non-surgical approach to modify factors affecting visual system functioning. Our patient was unable to perform most of the routine activities before the VT, which forced her to patch the RE. The goal of the presented approach was to improve the visual process, binocularity, and spatial organization. All of the above elements allowed the patient to improve balance and mobility and return to daily activities (Padula et al., 2007).
4Conclusion
Our results are consistent with the aforementioned. We demonstrated the usefulness of visual training rehabilitation in adult esotropic patients in managing diplopia and amblyopia after sudden visual acuity loss in the non-amblyopic eye. This indicates the neuroplasticity of the visual system, leading to improvement in visual acuity of the previously amblyopic eye.
Conflict of interest
None to report.
References
1 | Alotaibi, A. G. , Fawazi, S. M. , Alenazy, B. R. , Abu-Amero, K. K. ((2012) ). Outcomes of 3 hours part-time occlusion treatment combined with near activities among children with unilateral amblyopia. Saudi Medical Journal, 33: , 395–398. |
2 | Atkins, E. J. , Bruce, B. B. , Newman, N. J. , Biousse, V. ((2010) ). Treatment of nonarteritic anterior ischemic optic neuropathy. Surv Ophthalmol, 55: , 47–63. doi: 10.1016/j.survophthal.2009.06.008. |
3 | Baker, D. H. , Meese, T. S. , Hess, R. F. ((2008) ). Contrast masking in strabismic amblyopia: attenuation, noise, interocular suppression and binocular summation. Vision Res, 48: , 1625–1640. doi: 10.1016/j.visres.2008.04.017. |
4 | Birch, E. E. ((2013) ). Amblyopia and binocular vision. Prog Retin Eye Res, 33: , 67–84. doi: 10.1016/j.preteyeres.2012.11.001. |
5 | Chen, Y. , He, Z. , Mao, Y. , Chen, H. , Zhou, J. , Hess, R.F. ((2020) ). Patching and Suppression in Amblyopia: One Mechanism or Two? Front Neurosci, 13: , 1364. doi: 10.3389/fnins.2019.01364. |
6 | de Buffon, M. ((2005) ). Dissertation on the cause of strabismus or squint. Translated from: “Dissertation sur la cause du strabismus ou des yeux louches”. Mem Acad Roy Sci (Paris), 19 June 1743. Strabismus, 13: (4), 205–212. https://doi.org/10.1080/09273970590934319 |
7 | de Zárate, B. R. , Tejedor, J. ((2007) ). Current concepts in the management of amblyopia. Clinical Ophthalmology (Auckland, N.Z.), 1: (4), 403–414. |
8 | Ding, J. , Klein, S. A. , Levi, D. M. ((2013) ). Binocular combination in abnormal binocular vision. J Vis, 13: , 14. doi: 10.1167/13.2.14. |
9 | Draganski, B. , Gaser, C. , Busch, V. , Schuierer, G. , Bogdahn, U. , May, A. ((2004) ). Neuroplasticity: changes in grey matter induced by training. Nature, 427: (6972), 311–312. doi: 10.1038/427311a. PMID: 14737157. |
10 | El Mallah, M. K. , Chakravarthy, U. , Hart, P.M. ((2000) ). Amblyopia: is visual loss permanent? Br J Ophthalmol, 84: (9), 952–956. doi: 10.1136/bjo.84.9.952. PMID: 10966943; PMCID: PMC1723664. |
11 | Gaier, E. D. , Hunter, D. G. ((2017) ). Advances in amblyopia treatment: paradigm shifts and future directions. {Int Ophthalmol Clin, 57: (4), 117–128. |
12 | Hattenhauer, M. G. , Leavitt, J. A. , Hodge, D. O. , Grill, R. , Gray, D. T. ((1997) ). Incidence of nonarteritic anterior ischemic optic neuropathy/ American Journal of Ophthalmology, 123: (1), 103–107. https://doi.org/10.1016/s0002-9394(14)70999-7 |
13 | Hess, R.F. , Mansouri, B. , Thompson, B. ((2010) ). A binocular approach to treating amblyopia: antisuppression therapy. Optom Vis Sci, 87: , 697–704. doi: 10.1097/OPX.0b013e3181ea18e9. |
14 | Hess, R.F. , Mansouri, B. , Thompson, B. ((2010) ). A new binocular approach to the treatment of amblyopia in adults well beyond the critical period of visual development. Restor Neurol Neurosci, 28: , 793–802. doi: 10.3233/RNN-2010-0550. |
15 | Johnson, L. N. , Arnold, A. C. ((1994) ). Incidence of nonarteritic and arteritic anterior ischemic optic neuropathy. Population-based study in the state of Missouri and Los Angeles County, California. Journal of Neuro-Ophthalmology: the Official Journal of the North American Neuro-Ophthalmology Society, 14: (1), 38–44. |
16 | Kossut, M. ((2019) ). Basic mechanism of neuroplasticity. Neuropsychiatria i Neuropsychologia/Neuropsychiatry and Neuropsychology, 14: (1), 1–8. https://doi.org/10.5114/nan.2019.87727 (article in polish). |
17 | Levi, D. M. ((2012) ). Prentice award lecture 2011: removing the brakes on plasticity in the amblyopic brain. Optom Vis Sci, 89: (6), 827–38. doi: 10.1097/OPX.0b013e318257a187. PMID: 22581119; PMCID: PMC3369432. |
18 | Levi, D.M. , Polat, U. ((1996) ). Neural plasticity in adults with amblyopia. Proc Natl Acad Sci U S A, 93: , 6830–6834. doi: 10.1073/pnas.93.13.6830. |
19 | Lunghi, C. , Sframeli, A.T. , Lepri, A. , Lepri, M. , Lisi, D. , Sale, A. , Morrone, M.C. ((2019) ). A new counterintuitive training for adult amblyopia. Ann Clin Transl Neurol, 6: , 274–284. https://doi.org/10.1002/acn3.698 |
20 | Mateos-Aparicio, P. , Rodríguez-Moreno, A. ((2019) ). The Impact of Studying Brain Plasticity. Front Cell Neurosci, 13: , 66. doi: 10.3389/fncel.2019.00066. PMID: 30873009; PMCID: PMC6400842. |
21 | Padula, W. V. , Wu, L. , Vicci, V. , Thomas, J. , Nelson, C. , Gottlieb, D. , et al. ((2007) ). Evaluating and Treating Visual Dysfunction. in Brain Injury Medicine. Principles and Practice, ed. N.D. Zasler, D.I. Katz, R.D. Zafonte (Demos, NY, USA), 525–526. |
22 | Pane, A. , Miller, N. R. , Burdon, M. ((2018) ). The neuro-ophthalmology survival guide. New York. Elsevier. |
23 | Schütz, A. C. , Braun, D. I. , Gegenfurtner, K. R. ((2009) ). Object recognition during foveating eye movements. Vision Res, 49: (18), 2241–2253. |
24 | Schütz, A. C. , Braun, D. I. , Kerzel, D. , Gegenfurtner, K. R. ((2008) ). Improved visual sensitivity during smooth pursuit eye movements. Nat Neurosci, 11: (10), 1211–1216. |
25 | Spering, M. , Schütz, A. C. , Braun, D. I. , Gegenfurtner, K. R. ((2011) ). Keep your eyes on the ball: smooth pursuit eye movements enhance prediction of visual motion. J Neurophysiol, 105: (4), 1756–1767. |
26 | Wallace, D. K. , Edwards, A. R. , Cotter, S. A. , Beck, R. W. , Arnold, R. W. , Astle, W. F. , et al. ((2006) ). Pediatric Eye Disease Investigator Group. A randomized trial to evaluate 2 hours of daily patching for strabismic and anisometropic amblyopia in children. Ophthalmology, 113: (6), 904–912. |
27 | Williams, C. , Northstone, K. , Howard, M. , Harvey, I. , Harrad R. A. , Sparrow, J. M. ((2008) ). Prevalence and risk factors for common vision problems in children: Data from the ALSPAC study. Br J Ophthalmol, 92: (7), 959–964. doi: 10.1136/bjo.2007.134700. Epub 2008 May 14. PMID: 18480306. |
28 | Wong, A. M. ((2012) ). New concepts concerning the neural mechanisms of amblyopia and their clinical implications. Can J Ophthalmol, 47: (5), 399–409. doi: 10.1016/j.jcjo.2012.05.002. Epub 2012 Jun 29. PMID: 23036539. |


