
Structured guideline-based physiotherapy reduces difficulties in activities of daily living in Parkinson’s disease
Abstract
BACKGROUND:
In the long term, Parkinson’s disease (PD) leads to the development of difficulties in daily functional tasks. There remains a paucity of evidence on the effectiveness of physiotherapy on patient-perceived difficulties regarding basic activities of daily living (ADL).
OBJECTIVES:
To assess an effect of a versatile physiotherapy intervention on patient-perceived difficulties in basic ADL.
METHODS:
The study sample included 24 patients (10 men and 14 women) with PD. Participants were randomly assigned into intervention (IG) and control groups (CG). Two assessments were performed with a gap of 10 weeks. Following first assessment, during an 8-week period, IG participants attended sixteen physiotherapy 60-minutes sessions in groups that were divided into five parts to address the core areas recommended by the European Physiotherapy Guideline for PD (EPGPD): gait, transfers, balance, physical capacity, and manual activities. The main assessment tool was the Modified Patients Specific Functional Scale (ModPSFS), which represents a self-assessment rating on difficulties perceived in 17 different commonly occurring activities.
RESULTS:
IG members reported a significant reduction in self-perceived difficulties as assessed by ModPSFS (effect size 1.39; 95%CI 5.1, 26.6 points, p = 0.005).
CONCLUSIONS:
2-months conventional physiotherapy with incorporated core areas recommended in EPGPD for PD reduced patient-perceived difficulties in basic ADL.
1Introduction
Parkinson’s disease (PD) is a common age-related neurodegenerative disorder and its neuropathology is characterized by a selective loss of dopaminergic neurons (Cacabelos, 2017). Clinical presentations of PD motor and non-motor symptoms, wherein tremor, rigidity, bradykinesia/akinesia, and postural instability are considered cardinal signs (Balestrino & Schapira, 2020).
PD affects various aspects of life, including an ability to transfer and ambulate, which further results in a disability (Shulman, 2010). At some point, most of the PD patients start to experience difficulties in the execution of daily functional tasks. Consequently, physiotherapy is advised with an objective to maintain the patient’s independence, to maximise his/her safety and wellbeing, and to improve his/her performance of ADL, and to reduce secondary complications (Keus et al., 2014) (Tomlinson et al., 2014).
European Physiotherapy Guideline for Parkinson‘s Disease (EPGPD) includes recommendations on specific interventions and states core areas (gait, transfers, balance, manual activities, and physical capacity) for physiotherapy intervention with PD patients (Keus et al., 2014).
For example, treadmill training is recommended by EPGPD. However, although its effectiveness is proved in increasing gait speed, stride length, and cardiovascular endurance in patients with PD (Nadeau et al., 2014), this and other recommendations (e.g. tai chi) provided by the guideline might not be applicable in clinical practice. On one hand, it could be due to possible limitations related to specific intervention settings of and intervention provider, and on the other hand, patients with PD might present a wide range of functional difficulties that cannot be addressed by merely one type of intervention. Therefore, there is a need for evidence-based studies on the implementation of guidelines into physiotherapy interventions to obtain the best results in everyday life for people with PD. A need for more structured physical therapy programmes in PD patients has also been reported in the literature (Clarke et al., 2016).
Pazzaglia et al. have also conducted a study (Pazzaglia et al., 2020), where one study group received a conventional rehabilitation programme conducted according to the physiotherapy guidelines for PD patients by Royal Dutch Society for Physical Therapy (Koninklijk Nederlands Genootschap voor Fysiotherapie, i.e. KNGF Guidelines for physical therapy in PD patients, 2004). This study aimed to assess an overall improvement in selected outcome measures after a 6-week virtual reality rehabilitation programme in comparison to a conventional rehabilitation programme in patients with PD, not to specifically analyse the aspects related to structured guideline-based conventional physiotherapy.
The effectiveness of physiotherapy interventions is generally based on measures of quality of life as a whole, motor symptoms, balance, and gait outcomes (Radder et al., 2020). Patient‘s perception of the impact of an intervention on the performance of basic ADL has often remained discarded, though physiotherapists are encouraged to deliver a patient-centred care (Stevens et al., 2017).
The main aim of the study was to assess the benefit of a 2-month of supervised conventional physiotherapy intervention that incorporates EPGPD recommended core areas. We hypothesised that two month of structured guideline-based physiotherapy reduces patients reported difficulties in activities of daily living in Parkinson’s disease.
2Materials and methods
2.1Participants
Fifty patients from the PD epidemiological database (Kadastik-Eerme et al., 2018) of Tartu University Hospital were randomly contacted by telephone and were asked for the study participation (convenience sampling). The individuals willing to participate were invited to a meeting to examine their current neurological status, including the disease stage and severity. PD stage and severity were determined according to Movement Disorders Society Unified Parkinson‘s Disease Rating Scale (MDS-UPDRS) (Goetz et al., 2008) and Hoehn & Yahr Scale (HY) (Hoehn & Yahr, 1967) respectively. Neurological assessment was carried out by two movement disorders experts during baseline assessment. In addition, the participants were interviewed for their quality of life using the Estonian version of Parkinson’s Disease Questionnaire 39 (PDQ-39) (Krikmann et al., 2008) during the baseline assessment. All the participants used antiparkinsonian medications as instructed by their neurologist.
A total of 24 patients complying with subsequent inclusion criteria were assigned into either intervention group (IG, n = 12) or control group (CG, n = 12) using randomized blocked design (to assure equal number of both female and male participants in both groups). The inclusion criteria for this study were:
(1) a confirmed diagnosis of idiopathic PD (stages 1.5–3 on HY); (2) age > 60 years and < 80 years; (3) an ability to walk without an assistive device in the home setting; (4) absence of any other medical conditions that may affect gait or postural stability; (5) no physiotherapy intervention was received during the previous year; (6) an MMSE (Mini Mental State Examination) score above 24 (see Fig. 1).
Fig. 1
Flowchart of the sample collection and study design.
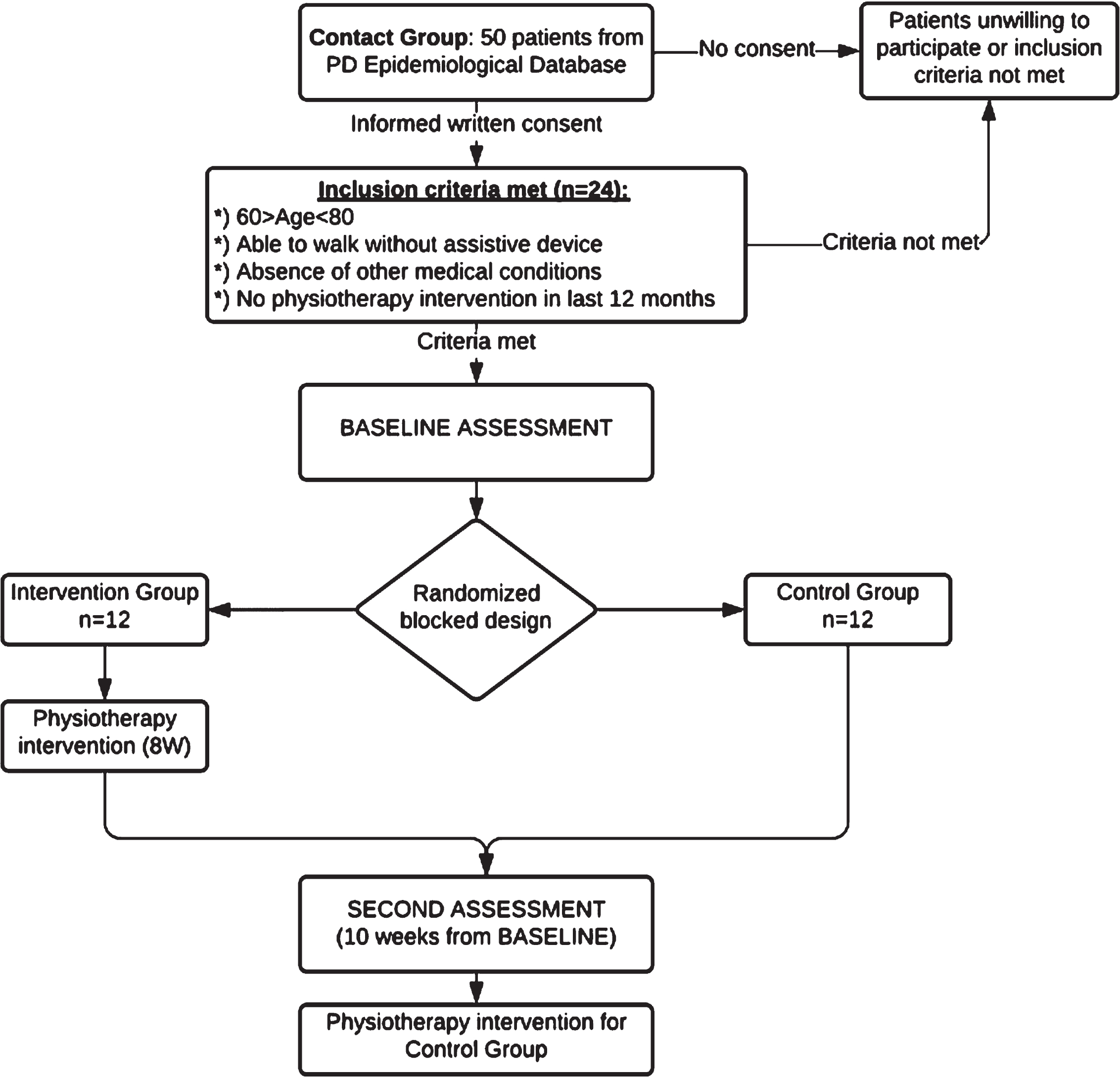
All the participants provided informed written consent and the study was carried out in compliance with the Helsinki declaration; the study protocol was approved by the Research Ethics Committee of University of Tartu and was registered on Tartu University’s Clinical Research Database (No. 12125) (ClinicalTrials.gov Identifier: NCT03568903). There were no drop-outs from the study. Table 1 illustrates the baseline characteristics of the study participants.
Table 1
Comparison of clinical and demographic characteristics of the participants at baseline
| Variable | IG (n = 12, 7F/5M) Mean (SD) | CG (n = 12, 7F/5M) Mean (SD) | p value |
| Age, years | 71.1 (4.2) | 69.9 (5.1) | 0.54 |
| Disease duration, years | 8.0 (6.9) | 7.7 (5.4) | 0.93 |
| HY stage | 2.2 (0.5) | 2.3 (0.7) | 0.93 |
| MDS-UPDRS total score | 62.2 (21.5) | 60.4 (26.7) | 0.86 |
| PDQ_Si | 25.85 (31.18) | 22.22 (12.12) | 0.67 |
| MMSE score | 28.0 (1.9) | 27.2 (1.5) | 0.24 |
| Height, cm | 165.1 (10.4) | 166.6 (10.1) | 0.72 |
| Bodyweight, kg | 72.8 (14.7) | 78.1 (14.6) | 0.39 |
IG: intervention group; CG: control group; F: female participants; M: male participants; SD: standard deviation; HY: Hoehn & Yahr Scale; MDS - UPDRS: Movement Disorders Society Unified Parkinson Disease Rating Scale; PDQ_Si: total score/single index according to Parkinson Disease Questionnaire (PDQ-39); MMSE: Mini Mental State Examination.
2.2Assessment tools
In the study, baseline and final assessments were carried out twice with a gap of 10 weeks between assessments at the Institute of Sport Sciences and Physiotherapy, University of Tartu, Estonia. Assessment time was scheduled when the PD patient was “on”-phase of PD.
The assessment began with a patient interview, preceding the rest of the examination by few days. The same researcher interviewed the same patient during both assessments. The interview included gathering information regarding medical anamnesis (the course of the disease, medications) and social anamnesis, and administration of questionnaires, including the main outcome measure of the study - Modified Patient-Specific Functional Scale (ModPSFS). A new outcome measure ModPSFS was used to maintain a patient-centred perspective of the assessment and at the same time assure direct comparison of the participants‘ functioning in different activities.
ModPSFS combines aspects of the Patient-Specific Complaint instrument (PSC) (Beurskens et al., 1999) and Patient-Specific Functional Scale (PSFS) (Stratford et al., 1995) ModPSFS includes listing aspects on which the individual with PD seeks improvement for (analogous to original PSFS). Yet, as motor presentation of PD differs substantially from person to person, then the daily activities that persons experience the most difficulties would also differ, which does not allow for comparison.
To allow generalization, in addition any 3 aspects, which the participant would want to improve, ModPSFS included 24 predefined activities (assumed to be performed regularly in a person’s daily life). The participant provided a rating of each activity on a 11-point VAS scale in terms of difficulties perceived as in original PSC (‘0’ indicates, I do not experience any problems with this activity, while, ‘10’ indicates a situation where the patient is unable to perform the activity independently).
Participants were asked to rate and make a self-check if the listed activities actually are a part of their basic ADL. self-check if the listed activities are a part of their daily function, and only activities performed by all of the subjects (17 activities, illustrated in Table 2) were encompassed in the data analysis. Latter was done to ensure that all the participants remain comparable. A total score was defined as a sum of ratings for all of these 17 items. Mean and average scores were also used. Lastly, during the second assessment all the participants were evaluated for their current health status in comparison to the baseline assessment using response options, such as “worse/deteriorated”; “same/unchanged”; “better/improved”.
Table 2
Activities included in Modified Patients Specific Functional Scale (ModPSFS)
| 1. Finding a comfortable lying position in bed | 10. Desending stairs |
| 2. Turning in bed | 11. Carrying smaller objects –eg a cup of coffee |
| 3. Getting to sitting from supine | 12. Picking an object from the floor |
| 4. Sit-to-stand | 13. Dressing lower part of the bady |
| 5. Sitting for prolonged period | 14. Dressing upper part of the body |
| 6. Standing for prolonged period | 15. Putting on shoes |
| 7. Walking in home-environment | 16. Self-hygiene |
| 8. Walking outside home-environment | 17. Eating |
| 9. Ascending stairs |
The rest of the examination involved functional assessment, which consisted of different tests, commonly used in clinical settings by physiotherapists (e.g range of motion and gait assessment). As the focus of the current paper is on patients’ perception of ADL difficulties, the impact of the intervention on functional tests is not included in this paper. An earlier article (Medijainen et al., 2019) by our research group addresses the latter aspect.
2.3Physical therapy
The intervention group (IG) underwent intervention in a group of three for 8 consecutive weeks. Altogether, IG participants attended 16 physiotherapy sessions (the participation rate was 100%), twice a week. Each session lasted for 60 minutes and included exercises to improve transfers, posture, gait, balance, and hand dexterity. The program was assembled according to EPGPD (Keus et al., 2014). Each therapy group received analogous exercises. For this, the exercises prescribed for the first group were recorded in writing and were followed by the other therapy groups (only minor adaptations were used if necessary). Please see the Appendix for a short description of the structure and contents of the physiotherapy sessions, as well as our previously published work (Medijainen et al., 2019).
During the study period, the CG received the usual care, however, all the participants in CG were offered to participate in 16 sessions of individual physiotherapy starting after the second assessment.
2.4Data analysis
Data analysis was performed using commercially available software (SPSS 20.0, IBM, Armonk, USA). Wilcoxon Signed Ranks test or Mann-Whitney U-test was used to compare differences between the baseline and post-intervention results. The significance level was set at p < 0.05. The effect size was calculated based on the coefficient of product-moment correlation (r) (T
3Results
Baseline assessment revealed no differences between the groups in any of the assessments performed (See Table 1)
During the baseline assessment IG demonstrated a little higher level of patient-perceived difficulties in basic ADL compared to CG, although this difference was not statistically significant. After 2-months of physiotherapy sessions in small groups patient-perceived difficulties in basic ADL were reduced in IG. There were significant improvements in the total score and also median and average scores of ModPSFS. Main results of the study are summarized in Table 3.
Table 3
Comparison between the intervention and control groups before and after the intervention
| Variable | Group | Before (SD) | After (SD) | ES | p value | |
| ModPSFS totalscore, points | IG | 48.71 (31.18) | 35.25 (25.67) | 1.39 | 0.005* | |
| CG | 30.84 (20.78) | 34.29 (21.30) | –0.49 | 0.248 | ||
| ModPSFS median item score, points | IG | 2.9 (0.7) | 1.8 (0.5) | 0.97 | 0.033* | |
| CG | 1.3 (0.5) | 1.7 (0.4) | –0.36 | 0.38 | ||
| ModPSFS average item score, points | IG | 3.0 (0.6) | 2.1 (0.4) | 1.39 | 0.005* | |
| CG | 1.9 (0.4) | 2.1 (0.4) | –0.49 | 0.248 | ||
| Health status: improved/same/deteriorated, number of subjects | IG | 10/0/2 | ||||
| Health status: improved/same/deteriorated, number of subjects | CG | 1/4/7 | ||||
SD: standard deviation; ES: effect size, ModPSFS: Modified Patients Specific Functional Scale; IG: intervention group; CG: control group; *: significant difference between assessments before and after intervention
Of note, when comparing the extent of change in patient-perceived difficulties in basic ADL (according to ModPSFS) at baseline and second assessment, significantly different results were evident –for example, group effect of change of ModPSFS total score was significant and large effect 1.6 (p = 0.002). Between groups, the difference in ModSPFS median score was also of the large effect of 1.04 (p = 0.024).
Post-intervention 10 of the participants in the IG group reported their health status to be improved, whereas 7 subjects from CG found it to have deteriorated. Of note, many participants failed to list the activities they find difficult and want to improve and rather expressed their concerns about poor sleep, poor vision, back pain, hand tremor, especially during the second assessment.
4Discussion
This study revealed that physiotherapy intervention that focuses briefly on different core areas as recommended by the standard guidelines, helped to reduce the patient reported difficulties of basic ADL in the PD patients.
We used a previously unused patient reported outcome measure ModPSFS, which is a combination of two standardized assessment measures, namely PSC and PSFS.
The PSC is one of the frequently used measuring instruments in Dutch community-based physiotherapy practices (Swinkels et al., 2011). Administration of PSC is also recommended by KNGF Guidelines for physical therapy in PD patients (2004), however, this instrument has hardly been used in research, especially with PD patients. During the administration of the original version of PSFS, a patient is expected to list any three (up to five) activities that are limited and for which he/she is seeking treatment. During reassessments, the patient is asked to provide a current difficulty score for the same listed activities (Beurskens et al., 1999). PSFS is claimed to be an easy-to-use valid, reliable, responsive, and efficient outcome measure applicable to a large number of clinical presentations, including in assessing physical function in community-dwelling elderly (Mathis et al., 2019). It has also been used in PD adults: The PSFS yields reliable scores when it is administered to people living with PD (Burgos-Martinez, 2011). Yet, though one part patient-centered physiotherapy is to clarify patients’ problems (Donnelly & Carswell, 2002), then measurement of physical function that is both specific to the individual and generates comparable outcome data is a fundamental need in physiotherapy examination (Mathis et al., 2019), which can be met by using ModPSFS.
Bohannon and co-authors revealed that patients with PD identified 60 different activities they were unable to do or they were experiencing difficulties as a result of their PD (Bohannon et al., 2020). Comparable outcome data is also of key importance in both research and clinical work. To compare the impact of an intervention on the basic ADL, standardized assessment, including the same specific activities, seems appropriate.
Previously used standardized assessments are the Nottingham Extended Activities of Daily Living (NEADL) Scale (Clarke et al., 2016) and Patient-Specific Index for Physiotherapy in Parkinson‘s disease (PSI-PD) (Nijkrake et al., 2009). Both include a list of pre-defined activities, analogous to ModPSFS. However, though both can be considered as good outcome measures of ADL from a patient’s perspective, they do not enable good comparisons across individuals or groups. For example, NEADL (Clarke et al., 2016) involves 22 questions on different activities which the subject is required to provide on one of four answer boxes for each keeping in mind the past week. However, it includes several activities that can remain un-executable due to other reasons not due to functional difficulties (for example gardening/driving a car because she or he does not own a garden or a car). Understandably, a valid comparison of two persons cannot be performed if one has provided one of the following ratings “with help”, “on my own with difficulty” or “on my own” for all 22 activities and another person has used the answer option “not at all” for several items.
PSI-PD (Nijkrake et al., 2009) includes an excellent predefined list of 26 aspects in which a person with PD is likely to experience limitations, however, PSI-PD also includes some items that the authors of the present study knew in advance that not all participants would perform (e.g. getting on or off a bicycle), we did not use the predefined list (though several items are included), but generated our list of 24 pre-defined activities, assumed to be performed on regular basis in person’s daily life. Participants were asked to rate and make a self-check if they perform the listed activity in their everyday life. To ensure that all the participants remain comparable, ModPSFS scoring was based only on 17 activities that each participant executed in his/her everyday life. For example, some male participants were not able to rate difficulties in food preparation as this was entirely the spouse’s responsibility in their household. Gender is likely to be one of the most evident contributors to the execution of ADL. Some gender differences in instrumental ADL in PD patients have also been reported previously (Foster, 2014).
The ModPSFS enables to obtain a perception of “the extent of the limitation/perceived difficulty” as the patient provides an answer on an 11-point VAS scale as in original PSC the severity for each complaint is scored (Beurskens et al., 1999) (‘0’ indicates, I do not experience any problems with this activity, while, ‘10’ indicates a situation where the patient is unable to perform the activity independently). PSI-PD provides an examiner with a list of limitations, assessed basically on a 2-point scale (e.g. item “turning around in bed” limited, “instability when stopping walking” –not limited), along with a ranking of “top five” activities that are limited items he or she wishes to improve. ModPSFS could be used to aid this along with a greater degree of comparison and generalization than is currently available from scientific evidence with PD patients, or a variety of other comorbidities and medical conditions. The validity and reliability of this test can hopefully be provided in near future.
In this study, 80%of the participants in the IG group reported post-intervention improvement health status, whereas nearly 60%of CG members perceived their health status to have deteriorated at the second assessment. This is a clear indication of the successful administration of patient-centred physiotherapy in PD patients.
A health status check was just a one-item question in ModPSFS. However, Rosenzveig et al. (2014) have reported that there is sufficient evidence to warrant the use of single items in clinical practice and also for long term monitoring (Rosenzveig et al., 2014). Despite that lack of time has been identified as one of the key barriers to patient-centred care (West et al., 2005), nonetheless, there should always be time to ask the patient to provide a one-item estimation on their health status, both pre- and post-intervention.
Clarke et al. (Clarke et al., 2016) reported the evidence on the usage of low-dose, patient-centred, goal-directed physiotherapy and occupational therapy in early stage PD patients to be insufficient. However, besides using NEADL as the main outcome measure (which might degrade comparison, as discussed earlier) the individualised interventions administered in Clarke et al. (Clarke et al., 2016) were for a very short period (median of four visits of 58 minutes as contact time), compared to 16 one-hour sessions in the present study.
Clarke et al. (2016) also indicated a need of more structured and intensive physical therapy programmes in PD patients. Our study, where versatile physiotherapy involving the core areas as recommended in EPGPD (Keus et al., 2014) is an example of such intervention.
Conventional rehabilitation programme claiming to be conducted according to the physiotherapy guidelines have been published earlier, e.g. a study by Pazzaglia et al. (2020) who based the intervention of one of the study groups on KNGF (2004) for PD. Interventions in Pazzaglia et al. (2020) and our study cannot be directly compared, as they differed substantially in many aspects (e.g. duration of intervention session and period). Nevertheless, Pazzaglia et al. (2020) reported that both interventions provided in their study, virtual reality therapy and conventional physiotherapy intervention, resulted in a significant improvement in arm function. Arm function improvement has a significant impact on the performance of daily activities. Though upper limb functional assessment was not included in our study, likely, incorporation of 10 minutes of manual activities into the therapy sessions has contributed for a reduction in perceived difficulties in basic ADL (by improving arm function).
Besides a 10-minute section of manual activities, the physiotherapy session included 4 other sections to address other core areas on EPGPD. Still, it is possible, that 60-minute sessions as designed in this study, may not be sufficient to focus in the best possible way on each core area recommended in EPGPD. For example, not all aspects of physical capacity, which is defined as including exercise tolerance and endurance along with joint mobility, muscle tone, power, and coordination in EPGPD (Keus et al., 2014), received the optimal attention in the present study. Specifically, the aspect of endurance and exercise tolerance was not focused extensively in this study, though a fixed period focusing strictly on this aspect of physical capacity would have been relevant. In order not to exhaust the patient during supervised sessions, the exercise tolerance aspect was diminished in the present study, as it could be more easily addressed in a form of unsupervised activities between sessions. However, other aspects of physical capacity were included. Further research should be undertaken to investigate which is the optimal length of intervention targeted to each of the core areas recommended in EPGPD. We propose that further research should take place to optimize intervention duration targeted to each core area recommended in EPGPD.
The recommendations from the EPGPD guideline were incorporated into group physiotherapy intervention instead of individualised intervention, which might somewhat influence the results. Administration of conventional physiotherapy in a group environment has been reported influential to improve attitude and foster optimism among PD patients (Park et al., 2014). We considered a group of 3–4 people to be optimal to bring out positive aspects of group therapy and at the same time to keep a necessary individualized approach for the patient to be cost-effective. Our approach of providing ‘conventional physiotherapy’ as group treatment is well supported by EPGPD (Keus et al., 2014).
The number of patients enrolled in the study is relatively small, which can limit the extrapolation of the study outcomes in the larger population. Hence, we were conservative in the interpretation of the results and while concluding.
The participants included in our study had not received any physiotherapy intervention during the previous year. One might argue that the sample was well functioning and therefore representative for a specific group of people with PD. However, in reality, a patient with PD does not always receive treatment when it is required. As was reported in a study by Keus et al. In their paper, 41%of the patients from 95 patients (of a total of 235 patients) who were identified to have serious problems within at least one of the four core areas of physiotherapy practice in PD (posture, balance, gait, transfers) and were therefore regarded as requiring referral to physiotherapy, did not receive physiotherapy (Keus et al., 2004). We are rather convinced that accessibility to physiotherapy services in Estonia is worse than in the Netherlands where the before mentioned study was conducted.
The present study approves that different evidence-based physiotherapy recommendations can be incorporated into conventional physiotherapy programme in a manner easily applicable in clinical settings, having beneficial outcomes to the patients with PD. Patient-centred care has been increasingly recognized as an essential component of quality care that has a positive effect on patients’ performance and rehabilitation (Yun & Choi, 2019). The present is a valuable contribution to increase patient-centred management care. The study convincingly showed that the participants who received a guideline-based, structured conventional physiotherapy programme perceived a positive impact on self-perceived difficulties of basic ADL. The authors propose that future research should explore the long term effect of such conventional, guideline-based and structured physiotherapy intervention and should optimize a cycle of intervention. Also, recent research reports support intermittent, short term intensive interventions (Welsby et al., 2019). Patient’s perception is necessary to consider in research and clinical practice with individuals with PD, so important issues would not be missed.
5Conclusions
The outcomes of this study revealed that 2-months of physiotherapy intervention in a group environment that was focused on all the core areas recommended in physiotherapy guideline reduced patient-perceived difficulties in basic ADL in PD patients.
Acknowledgments
The authors wish to acknowledge physiotherapists Kristi Reimann, Mari Raudmann and Kristel Ao for their contribution in the data collection. We also thank Mikk Medijainen for his insightful comments and suggestions.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding statement
This study was supported by the Grant PRG957 of the Estonian Research Council.
References
1 | Balestrino, R. , & Schapira, A. H. V. ((2020) ). Parkinson disease. European Journal of Neurology, 27: (1), 27–42. https://doi.org/10.1111/ene.14108 |
2 | Beurskens, A. J. , de Vet, H. C. , Köke, A. J. , Lindeman, E. , vander Heijden, G. J. , Regtop, W. , & Knipschild, P. G. ((1999) ). A patient-specific approach for measuring functional status in low back pain. Journal of Manipulative and Physiological Therapeutics, 22: (3), 144–148. https://doi.org/10.1016/s0161-4754(99)70127-2 |
3 | Bohannon, R. W. , Nair, P. , & Green, M. ((2020) ). Feasibility and informativeness of the Patient-Specific Functional Scale with patients with Parkinson’s disease. Physiotherapy Theory and Practice, 36: (11), 1241–1244. https://doi.org/10.1080/09593985.2019.1571134 |
4 | Borenstein, M, L. V. , Hedges, J. P. T. , & Higgins, H. R. . Rothstein. Introduction to Meta-Analysis. 2009 John Wiley & Sons, Ltd. ISBN: 978-0-470-05724-7. |
5 | Burgos-Martinez, G. (2011). THE RELIABILITY AND VALID-ITY OF THE PSFS IN PEOPLE WITH PD [Thesis]. https://macsphere.mcmaster.ca/handle/11375/11302 |
6 | Cacabelos, R. ((2017) ). Parkinson’s Disease: From Pathogenesis to Pharmacogenomics. International Journal of Molecular Sciences, 18: (3). https://doi.org/10.3390/ijms18030551 |
7 | Clarke, C. E. , Patel, S. , Ives, N , Rick, C. E. , Woolley, R. , Wheatley, K. , Walker, M. F. , Zhu, S. , Kandiyali, R. , Yao, G. , & Sackley, C. M. ((2016) ). Clinical effectiveness and cost-effectiveness of physiotherapy and occupational therapy versus no therapy in mild to moderate Parkinson’s disease: A large pragmatic randomised controlled trial (PD REHAB). Health Technology Assessment (Winchester, England), 20: (63), 1–96. https://doi.org/10.3310/hta20630 |
8 | Donnelly, C. , & Carswell, A. ((2002) ). Individualized outcome measures: A review of the literature. Canadian Journal of Occupational Therapy. Revue Canadienne D’ergotherapie, 69: (2), 84–94. https://doi.org/10.1177/00084174020690020 |
9 | Foster, E. R. ((2014) ). Instrumental activities of daily living performance among people with Parkinson’s disease without dementia. The American Journal of Occupational Therapy: Official Publication of the American Occupational Therapy Association, 68: (3), 353–362. https://doi.org/10.5014/ajot.2014.010330 |
10 | Goetz, C. G. , Tilley, B. C. , Shaftman, S. R. , Stebbins, G. T. , Fahn, S. , Martinez-Martin, P. , Poewe, W. , Sampaio, C. , Stern, M. B. , Dodel, R. , Dubois, B. , Holloway, R. , Jankovic, J. , Kulisevsky, J. , Lang, A. E. , Lees, A. , Leurgans, S. , LeWitt, P. A. , Nyenhuis, D. , ... Movement Disorder Society UPDRS Revision Task Force. ((2008) ). Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Movement Disorders: Official Journal of the Movement Disorder Society, 23: (15), 2129–2170. https://doi.org/10.1002/mds.22340 |
11 | Hoehn, M. M. , & Yahr, M. D. ((1967) ). Parkinsonism: Onset, progression, and mortality. Neurology, 17: (5), 427–442. https://doi.org/10.1212/wnl.17.5.427 |
12 | Kadastik-Eerme, L. , Taba, N. , Asser, T. , & Taba, P. ((2018) ). The increasing prevalence of Parkinson’s disease in Estonia. Acta Neurologica Scandinavica, 138: (3), 251–258. https://doi.org/10.1111/ane.12948 |
13 | Keus, S. H. J. , Bloem, B. R. , Verbaan, D. , de Jonge, P. A. , Hofman, M. , van Hilten, B. J. , & Munneke, M. ((2004) ). Physiotherapy in Parkinson’s disease: Utilisation and patient satisfaction. Journal of Neurology, 251: (6), 680–687. https://doi.org/10.1007/s00415-004-0402-7 |
14 | Keus, S. , Munneke, M. , Graziano, M. , Paltamaa, J. , Pelosin, E. , Domingos, J. , Ramaswamy, B. , Prins, J. , Struiksma, C. , Rochester, L. , Nieuwboer, A. , & Bloem, B. (2014). European Physiotherapy Guideline for Parkinson’s Disease. 191. |
15 | KNGF Guidelines for physical therapy in patients with Parkinson’s disease. (2004). Suppl Dutch J Phys Ther Parkinsons Dis. Published. |
16 | Krikmann, Ü. , Taba, P. , Lai, T. , & Asser, T. ((2008) ). Validation of an Estonian version of the Parkinson’s Disease Questionnaire (PDQ-39). Health and Quality of Life Outcomes, 6: , 23. https://doi.org/10.1186/1477-7525-6-23 |
17 | Mathis, R. A. , Taylor, J. D. , Odom, B. H. , & Lairamore, C. ((2019) ). Reliability andValidity of the Patient-Specific Functional Scale in Community-Dwelling Older Adults. Journal of Geriatric Physical Therapy (2001), 42: (3), E67–E72. https://doi.org/10.1519/JPT.0000000000000188 |
18 | Medijainen, K. , Pääsuke, M. , Lukmann, A. , & Taba, P. ((2019) ). Versatile guideline-based physiotherapy intervention in groups to improve gait speed in Parkinson’s disease patients. NeuroRehabilitation, 44: (4), 579–586. https://doi.org/10.3233/NRE-192723 |
19 | Nadeau, A. , Pourcher, E. , & Corbeil, P. ((2014) ). Effects of 24 wk of treadmill training on gait performance in Parkinson’s disease. Medicine and Science in Sports and Exercise, 46: (4), 645–655. https://doi.org/10.1249/MSS.0000000000000144 |
20 | Nijkrake, M. J. , Keus, S. H. J. , Quist-Anholts, G. W. L. , Overeem, S. , De Roode, M. H. , Lindeboom, R. , Mulleners, W. , Bloem, B. R. , & Munneke, M. ((2009) ). Evaluation of a Patient-Specific Index as an outcome measure for physiotherapy in Parkinson’s disease. European Journal of Physical and Rehabilitation Medicine, 45: (4), 507–512. |
21 | Park, A. , Zid, D. , Russell, J. , Malone, A. , Rendon, A. , Wehr, A. , & Li, X. ((2014) ). Effects of a formal exercise program on Parkinson’s disease: A pilot study using a delayed start design. Parkinsonism & Related Disorders, 20: (1), 106–111. https://doi.org/10.1016/j.parkreldis.2013.10.003 |
22 | Pazzaglia, C. , Imbimbo, I. , Tranchita, E. , Minganti, C. , Ricciardi, D. , Lo Monaco, R. , Parisi, A. , & Padua, L. ((2020) ). Comparison of virtual reality rehabilitation and conventional rehabilitation in Parkinson’s disease: A randomised controlled trial. Physiotherapy, 106: , 36–42. https://doi.org/10.1016/j.physio.2019.12.007 |
23 | Radder, D. L. M. , Lígia Silva de Lima, A. , Domingos, J. , Keus,S. H. J. , van Nimwegen, M. , Bloem, B. R. , & de Vries, N. M. ((2020) ). Physiotherapy in Parkinson’s Disease: A Meta-Analysis of Present Treatment Modalities. Neurorehabilitation and Neural Repair, 34: (10), 871–880. https://doi.org/10.1177/1545968320952799 |
24 | Rosenzveig, A. , Kuspinar, A. , Daskalopoulou, S. S. , & Mayo, N. E. ((2014) ). Toward patient-centered care: A systematic review of how to ask questions that matter to patients. Medicine, 93: (22), e120. https://doi.org/10.1097/MD.0000000000000120 |
25 | Shulman, L. M. ((2010) ). Understanding disability in Parkinson’s disease. Movement Disorders: Official Journal of the Movement Disorder Society, 25 Suppl 1: , S131–135. https://doi.org/10.1002/mds.22789 |
26 | Stevens, A. , Moser, A. , Köke, A. , van der Weijden, T. , & Beurskens, A. ((2017) ). The use and perceived usefulness of a patient-specific measurement instrument in physiotherapy goal setting. A qualitative study. Musculoskeletal Science & Practice, 27: , 23–31. https://doi.org/10.1016/j.msksp.2016.12.005 |
27 | Stratford, P. , Gill, C. , Westaway, M. , & Binkley, J. ((1995) ). Assessing Disability and Change on Individual Patients: A Report of a Patient Specific Measure. Physiotherapy Canada, 47: (4), 258–263. https://doi.org/10.3138/ptc.47.4.258 |
28 | Swinkels, R. A. , van Peppen, R. P. , Wittink, H. , Custers, J. W. , & Beurskens, A. J. ((2011) ). Current use and barriers and facilitators for implementation of standardised measures in physical therapy in the Netherlands. BMC Musculoskeletal Disorders, 12: , 106. https://doi.org/10.1186/1471-2474-12-106 |
29 | Tällez, A. , García, C. H. , & Corral-Verdugo, V. ((2015) ). Effect size, confidence intervals and statistical power in psychological research. Psychology in Russia: State of the Art, 8: (3), 27–47. https://doi.org/10.11621/pir.2015.0303 |
30 | Tomlinson, C. L. , Herd, C. P. , Clarke, C. E. , Meek, C. , Patel, S. , Stowe, R. , Deane, K. H. , Shah, L. , Sackley, C. M. , Wheatley, K. , & Ives, N. ((2014) ). Physiotherapy for Parkinson’s disease: A comparison of techniques. The Cochrane Database of Systematic Reviews, 2014(6). https://doi.org/10.1002/14651858. CD002815.pub2 |
31 | Welsby, E. , Berrigan, S. , & Laver, K. ((2019) ). Effectiveness of occupational therapy intervention for people with Parkinson’s disease: Systematic review. Australian Occupational Therapy Journal, 66: (6), 731–738. https://doi.org/10.1111/1440-1630.12615 |
32 | West, E. , Barron, D. N. , & Reeves, R. ((2005) ). Overcoming the barriers to patient-centred care: Time, tools and training. Journal of Clinical Nursing, 14: (4), 435–443. https://doi.org/10.1111/j.1365-2702.2004.01091.x |
33 | Yun, D. , & Choi, J. ((2019) ). Person-centered rehabilitation care and outcomes: A systematic literature review. International Journal of Nursing Studies, 93: , 74–83. https://doi.org/10.1016/j.ijnurstu.2019.02.012 |
Appendices
Appendix
The structure of the physiotherapy sessions: Different sections of each physiotherapy session
| Exercises in a laying position (supine, prone, and side-laying), | Exercises in a sitting position, | Exercises in a standing position (including cues where appropriate and visual feedback), | Gait training (including different cues where appropriate and visual feedback), | Exercises for hand function and manual dexterity | |
| 15 minutes | 10 minutes | 15 minutes | 10 minutes | 10 minutes | |
| Core area(s) targeted | Transfers, physical capacity | Transfers, physical capacity | Balance, physical capacity | Gait, physical capacity | Manual activities |
| Types of exercise | •in-bed transfers (e.g. rolling from supine to side-laying etc) sand transfers from laying-to-sitting and vice versa | •Transfers (sitting-to-standing and standing-to-sitting transfers and scooting movements in sitting) | •Postural correction exercises, | •Gait initiation exercises, | •Manual dexterity exercises (including different bilateral and unilateral activities with the need of using different grasp types) |
| •Range of motion exercises (e.g. spinal, neck, shoulder, hip, knee), incorporating stretching exercises (e.g. hamstrings, pectoral, neck muscles) | •Range of motion exercises (e.g spinal, shoulder, knee range of motion) | •Static balance exercises (including exercises with eyes closed) | •Gait exercises including turns (U-turn), stepping over obstacles, gait with head turns etc | •Upper limb range of motion exercises | |
| •Muscle strengthening exercises (e.g. spinal extensors, knee and hip extensors, hip and knee flexors, abductors) | •Postural correction exercises | •Gait initiation exercises and dynamic balance exercises (e.g. weight transference, stepping in different directions, practising turns in place, including clock-turn) | •Gait exercises with different cues (eg visual cues to increase step length, and gait speed etc) | •Upper limbs muscle strengthening exercises | |
| •Muscle strengthening exercises (e.g. spinal/thoracic extensors, hip flexors) | •Muscle strengthening (e.g hip abductors and extensors) |


