
Children’s meals at restaurants in Abu Dhabi, United Arab Emirates, have poor nutritional quality
Abstract
BACKGROUND:
Many people in the UAE eat out frequently, but there is limited knowledge about the nutritional quality of the consumed meals.
OBJECTIVE:
The aim of this study was to assess the nutritional quality of children’s meals in Abu Dhabi restaurants, considering deep-frying and food group content.
METHODS:
In this cross-sectional pilot study, popular food outlets were identified using an online customer rating application. Children menus were collected and the meal quality was assessed. A healthy meal should not be deep-fried and contain at least 2 of the following food groups: low-fat dairy/lean protein/whole grain/fruits/vegetables (criteria adapted from the “Kids Live Well Nutritional Criteria” by the National Restaurant Association, US).
RESULTS:
58 restaurants were included, of which 29 had children menus, offering a total of 209 meals. 60% of the meals had beverages included in the price: 13% being water or milk. Overall, 78.9% of the assessed meals did not meet the cut-offs for healthy meals.
CONCLUSIONS:
In this pilot study, a majority of children’s meals in Abu Dhabi’s food outlets had poor nutritional quality. The findings suggest a need for more extensive studies around meal offerings at restaurants.
1Introduction
A poor nutritional intake – with a high intake of saturated fat, sugar and sodium, and a low intake of micro nutrients – has been reported among children in the United Arab Emirates (UAE) [1, 2]. There are high rates of non-communicable diseases among children, with high prevalences of obesity, diabetes and hypertension in parallel with underweight children and micro nutrient deficiencies [3, 4]. One of the UAE’s national key performance indicators is the health of its population, with one of the goals of the UAE vision 2021 being to improve this health [5, 6]. Abu Dhabi – one of the Emirates in the UAE – released its plan on how to tackle childhood obesity in December 2016 [7]. Some of the key areas of focus are making healthier food and beverages available in sport facilities, schools and public places, as well as helping businesses create and supply healthier options to children [7].
No studies have so far been published in the UAE in regard to the quality of restaurant meals for children, but findings from elsewhere show a complex picture. Restaurant meals in the US are often high in calories and sodium and low in nutrients, regardless of whether the meals are intended for adults or children, and whether the meals are from full-service or fast food restaurants [8–12]. Children’s meals in the US and Ireland have been reported to be high in total and saturated fat while being low in other nutrients [13, 14]. Fat content has also been found to be high in other countries whereas the findings regarding micronutrients are inconsistent [15]. In countries other than the US sodium content has also been reported to be high. Scourboutakos et al. found that adult’s and children’s meals in restaurants in Canada contain on average 1455 and 790 mg of sodium respectively, a large percentage of the daily recommended sodium intake [16]. Furthermore, in Belgium the sodium density in children’s meals is high [17]. In Texas few meals include fruits and/or vegetables, sides are often unhealthy and there are limited healthy meal options on the menus for children [18]. Vegetable portions in Belgian restaurants are large, but so are the overall portion sizes [17]. In the UK the portion sizes vary widely, as do the content of fruits and vegetables in children meals [19].
A recent systematic review of eating out among both children and adults, looking at 17 countries in Europe, Asia and the Americas, showed that in most countries looked at, there is a trend that people are obtaining greater percentages of their energy by eating out than before [15]. The caloric consumption of children from food away from home has significantly increased in the US over the past few decades, from 23.4% in 1977 to 33.9% in 2006 [20]. In the Philippines the numbers are similar to those in the US, while children in China and Russia only consume a small proportion of their calories outside of their homes [21]. The UAE has been rapidly changing, evolving from a Bedouin society to a modern country in less than forty years [1, 22, 23]. The country’s financial growth means that many people can afford to eat out [22, 24]. According to the Pan Arab Research Centre, 26.1% of households in the UAE with children aged 3–18 years old eat at restaurants at least once a week, and 21.2% from the same group eat fast food at least once a week, indicating that families with children in the UAE eat out frequently [25].
Some studies have shown that a frequent consumption of food away from home has been associated with a higher body mass index (BMI) in children, and higher intake of sugar sweetened beverages (SSBs) like soft drinks, fruit squashes and savory snacks [13, 26–28]. Reducing the consumption of meals away from home has been associated with improved nutrient intake and improved BMI and body fat percentages in overweight children [29]. Different strategies have been suggested and tested to improve children’s restaurant meals, including offering more fruit and vegetables as side options, offering water instead of SSBs, using calorie labels on menus, and only allowing toys to be included in the price for healthy meals [19, 30, 31]. The “Kids Live Well Nutritional Criteria” by the National Restaurant Association in the US is one of several initiatives designed to promote healthy kid’s meals, focusing on both nutrient quality and quantity [32]. In Abu Dhabi, where a high prevalence of non-communicable disease has been reported among children and adults, the authorities are addressing the issues in several ways [33]. Standards for healthy adult meals have been developed under the name “Weqaya”, meaning prevention in Arabic [34]. Restaurants can enroll in the program, which allows them to add a Weqaya logo next to healthy meals, – promoting healthy eating among adults, but no standard exists for children meals [34].
To date, no data has been published regarding nutritional aspects of restaurant meals in Abu Dhabi. The UAE government is determined to improve the health of children, and, with a frequent consumption of meals away from home, more knowledge is needed around food offerings in restaurants available to children.
2Objective
The aim of this study was to assess the nutritional quality of children’s meals in Abu Dhabi restaurants considering deep-frying and food group content.
3Methods
In this cross-sectional pilot study, the proportion of children’s meals that were deep-fried, and the food group content of the remaining meals, at restaurants in Abu Dhabi, were examined. The selection of food outlets was performed using a free social media restaurant finder application, based on popularity. The online application was visited in spring 2016, and the 58 most popular food outlets were selected. The restaurants were geographically spread across the city of Abu Dhabi, located in both urban and suburban areas. The children menus were collected from the restaurants. When the cooking methods, sidings and ingredients could not be determined from the menu alone, this information was acquired by asking the waiters. Restaurants with no children menus were excluded as were food outlets offering “pick and mix options” due to the complexity of analyzing all possible meal combination.
As no local criteria for healthy children’s meals in restaurants exist, an adapted version of the “Kids Live Well Nutritional Criteria”, by the National Restaurant Association (NRA) in the US, was used. According to the NRA, deep-fried meals are not healthy, and in order for a meal to be healthy it has to contain at least 2 of 5 healthy food groups (lean protein, low fat diary, whole grains, fruit, vegetables). The “Kids Live Well Nutritional Criteria” also include criteria for the energy and nutrient content, but this was not taken into consideration in this pilot study [32].
3.1Statistical analysis
Each meal was analyzed in regard to deep-frying and food group content after which is was compared with the adapted NRA “Kids Live Well Nutritional Criteria”. Microsoft Excel, version 15.36, was used for data analysis.
4Results
As shown in Fig. 1, 58 restaurants were visited, of which 29 offered children menus. These 29 were a mix of independent, international full-service, fast food chain, shopping malls eateries, and hotel restaurants located in different geographic locations. The restaurant offerings included Arabic, Asian, Italian and Western cuisine meals. In total, these outlets offered 209 meals on their children menus of which all but 2 were main course meals, with an average (SD) cost of USD 7.6 (2.7).
Fig.1
Flowchart of study methodology, depicting how the proportion of children’s meals in Abu Dhabi restaurants which are healthy was determined.
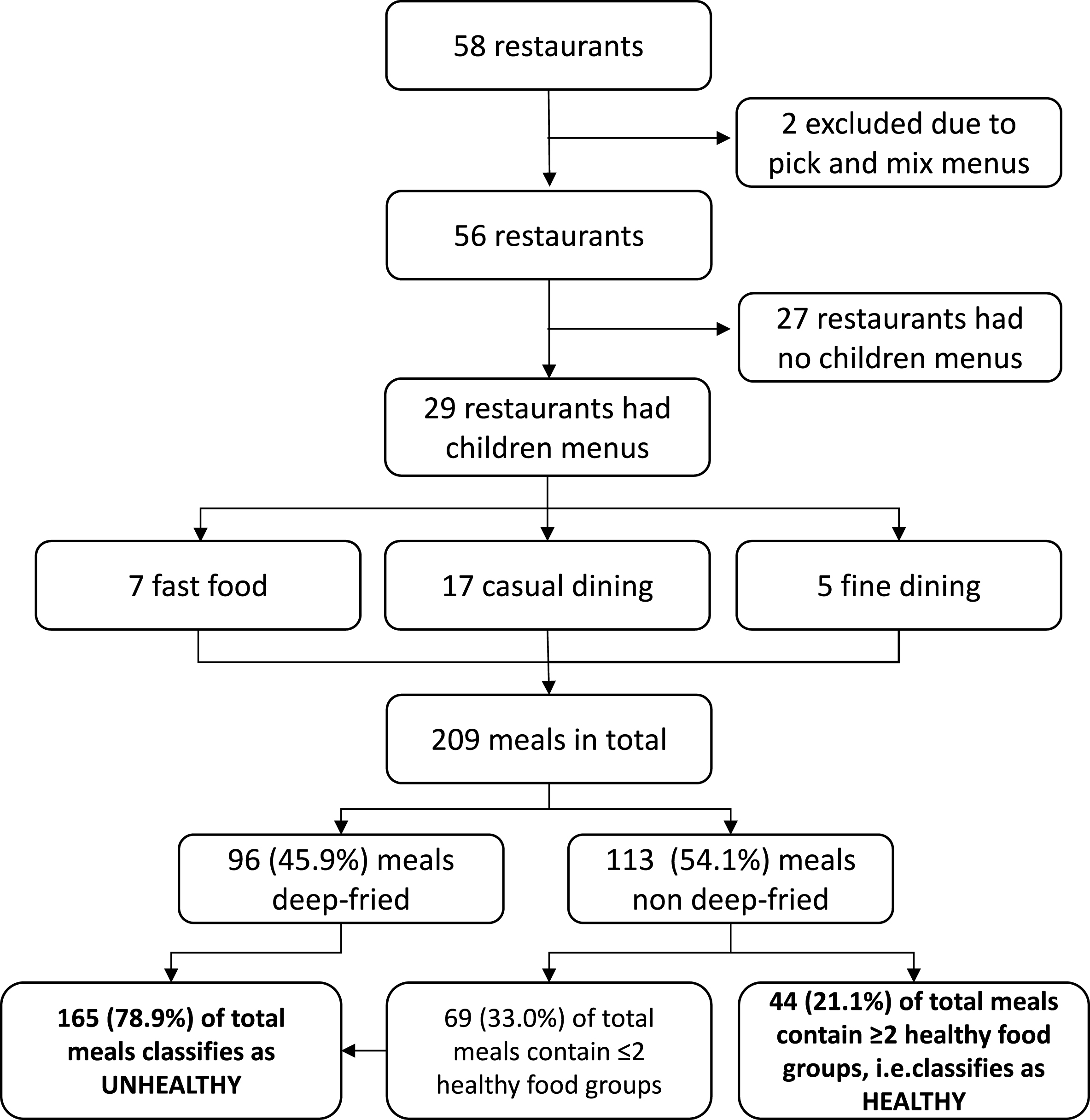
Forty-six percent of the meals (96/209) were deep-fried and were thus classified as “non-healthy” following the adopted NRA criteria. No further analysis of these meals was performed [32].
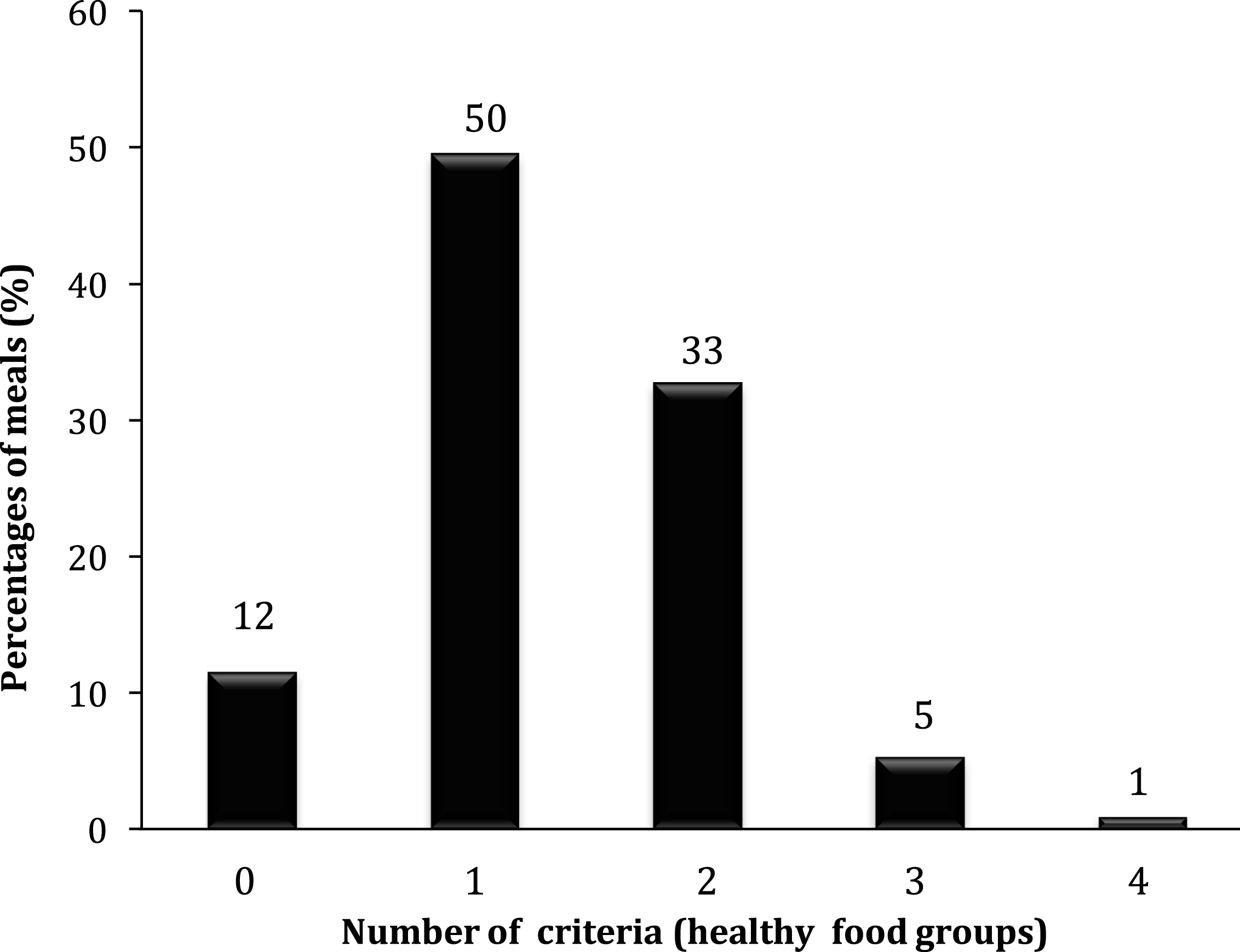
The characteristics of the remaining 113 meals are shown in Fig. 2. Most of these meals, 91%, were set by default, but in some meals, there was an option to choose between different grains (whole grain or refined grain), beverages and/or vegetables. Most meals contained refined grains and unprocessed (lean) protein. Fruits and vegetables were included less frequently, being present in 10.6% and 15% of these meals respectively. As shown in Fig. 3, 39% of the 113 meals contained 2 or more healthy food groups if the healthy options were chosen, and can thus be classified as healthy [32]. Overall, Fig. 1 shows that 21.1% of the 209 meals would meet the adapted criteria for a healthy meal, not having considered the energy and nutrient content [32].
Fig.2
Percentages of food groups in non-deep-fried children’s meals at restaurants in Abu Dhabi, UAE. Each meal can include one or more food groups. n = 113. *Vegetables were an option that could be selected. ‡Whole grain was an option that could be selected. ‡Primarily mashed potatoes.
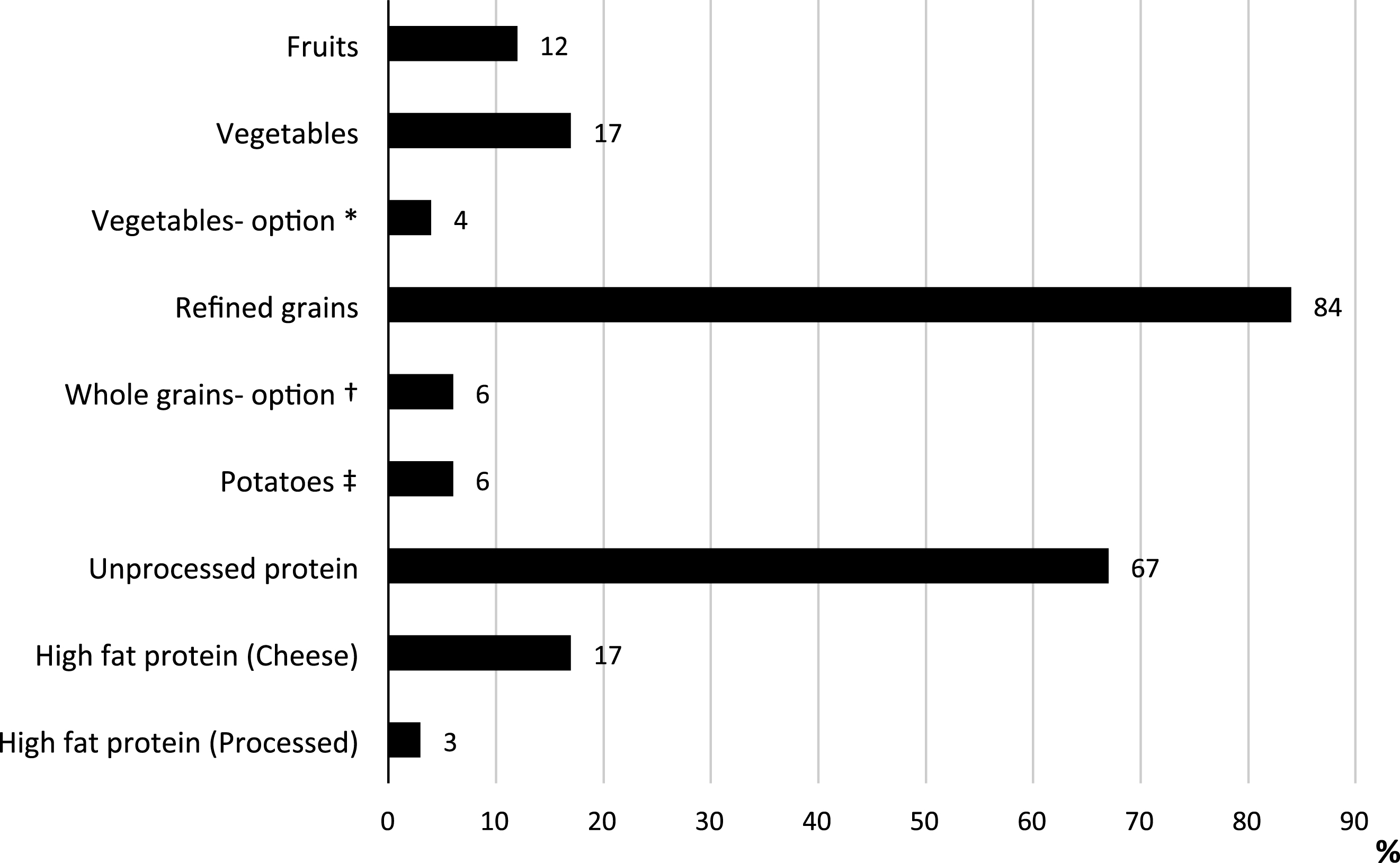
Fig.3
Number of healthy food groups per meal compared with the adapted “Kids Eat Well Nutritional Criteria”, National Restaurant Association, US in non-deep-fried children meals at restaurants in Abu Dhabi, UAE.≥2 healthy food groups were the criteria for a healthy meal. n = 113.
One hundred and twenty-five meals (60%) included beverages in their prices. A total of 247 beverage options were available for the 125 meals, of which 4% were water, 4% were milkshake, 9% were milk, 18% were fresh juices, 27% were soft drinks and 37% were other beverages (pre-packed juices/fruit cocktails and more). Beverage sizes varied between 180–390 ml.
Nine percent of the meals (19/209) included desserts in their prices of which all were discretionary calories (brownies, pastries, ice creams). For another 100 meals, there were also dessert options available on the children’s menu, offering a total of 26 different desserts of which 23% were fruits/fruit salads and the remaining ones were discretionary calories only.
5Discussion
This study revealed that most children’s meals offered at restaurants in Abu Dhabi had poor nutritional quality, a concern in a country where a high prevalence of non-communicable disease is reported as well as a high frequency of eating out [3, 4, 25, 35]. Meals often contained refined grains and a protein source, but seldom fruits and/or vegetables. Most beverage options offered as part of the meals’ prices were unhealthy.
Worryingly, almost half of the meals were deep-fried, a food preparation method that leads to high fat content and energy density, the opposite of what is recommended for a healthy meal [36]. Only a fifth of the meals would meet the amended NRA’s healthy meal criteria, supporting findings from other parts of the world that children’s meals are often unhealthy [12, 15, 16]. Even though fruits and vegetables are known to increase the intake of vitamins, minerals and fiber, and to reduce energy density, very few meals in this study included either of these food groups by default [36]. Some have reported similar findings but the results are inconclusive [15]. Many meals did contain juice, which is a source of vitamin C. However, according to the recommendations, juice consumption should be limited due to the high sugar and low fiber content, and whole fruits should be consumed instead [37]. It has been reported that serving fruit and vegetables instead of french-fries as a side item, a change that most children in the study by Anzman-Frasca et al. would think was acceptable, could result in a mean reduction of 170 kcal per meal [38].
Introducing more healthy meals onto children menu, including healthy sidings by default and not including french-fries and soft drinks in meals’ prices, has resulted in higher proportions of meals ordered that are healthy, elsewhere [32]. A significant decreased energy intake has been reported among children who accept the healthy options [31]. In the UAE, with a very high prevalence of non-communicable diseases among children, such changes could have a positive effect, especially since many families regularly consume restaurant food [25]. This study included different types of food outlets. Regardless of restaurant type, a majority of the meals were unhealthy, indicating a need for improvements across Abu Dhabi restaurants.
According to the American Pediatric Association, plain milk or water are the preferred beverage options for children [39]. In this study only 13% of the beverage options were water or milk showing a discrepancy to the guidelines for healthy beverage consumption in children [39]. On the other hand, sweet beverages, considered to be discretionary calories, were common. This poses a risk not only from an energy perspective, but also from a dental perspective. In the UAE, dental caries is common among children and a frequent consumption of sugar has been associated with higher caries prevalence in some studies [35, 40]. The beverage sizes in this study varied widely. In adults, consuming meals at full-service restaurants the replacement of SSBs with water reduced the daily energy intake by 443 kcals and lowered sugar intake by 58,2 grams [41]. It has also been shown that providing calorie labels on SSBs leads to a lower consumption due to less frequent purchases and customers buying smaller sizes [42]. Wang et al. showed that limiting sizes of SSBs could have a positive effect among overweight children and young adults [43].
Energy and nutrient contents were not considered in this study which may be seen as a limitation. However, using the deep- frying and food group content as screening criteria worked well to determine the healthiness of meals, contributing to new knowledge in this field in the UAE. Further analysis of nutrient content would likely result in the elimination of additional meals, which would result in even more concerning findings.
It would be valuable if future studies used a stratified sampling technique to get a representative sample of all restaurants in Abu Dhabi. However, in a city where there is limited statistical data available regarding restaurant types the study used an innovative way of collecting data, and since the restaurants were located in different areas of the city, and included different cuisines and categories of eateries, the findings highlight some important aspects of meals offered to children. As reported elsewhere, several initiatives promoting healthy children’s meals at food outlets show promising results [44]. While this study focused on food offerings, regional studies about children’s meal choices while eating out would be necessary in order to fully understand what impact potential policies and regulations for healthier children’s meals in restaurants could have in the UAE.
To conclude, a large majority of the assessed children meals were unhealthy. Beverages included in the price were primarily sugar containing drinks, thus contributing to a high intake of empty calories. With a goal to improve health among all children in the UAE and to decrease childhood obesity to 12% by 2021 different strategies must be considered [5, 6]. The Health Authorities in Abu Dhabi already have “Weqaya” menu labeling for adult meals. The results in this study indicate that actions need to be taken to improve the healthiness of children meals in Abu Dhabi.
References
[1] | Ng SW , Zaghloul S , Ali H , Harrison G , Yeatts K , El M , Popkin , BM . Nutrition Transition in the United Arab Emirates (UAE). Eur J Clin Nutr. (2011) ;65: (12):1328–37. http://doi.org/10.1038/ejcn.2011.1356 |
[2] | Hashim R , Williams SM , Thomson WM . Diet and caries experience among preschool children in Ajman, United Arab Emirates. Eur J Oral Sciences. (2009) ;117: (6):734–40. |
[3] | Al Junaibi A , Abdulle A , Sabri S , Hag-Ali M , Nagelkerke N . The prevalence and potential determinants of obesity among school children and adolescents in Abu Dhabi, United Arab Emirates. Int J Obes. (2013) ;37: (1):68–74. |
[4] | Hwalla N , Al Dhaheri AS , Radwan H , Alfawaz HA , Fouda MA , Al-Daghri NM , et al. The prevalence of micronutrient deficiencies and inadequacies in the middle east and approaches to interventions. Nutrients. (2017) ;9: (3). |
[5] | UAE Government. National key performance indicators. World Class Health Care. Index 3: Prevalence of obesity amongst children. (2015) . https://www.vision2021.ae/en/national-priority-areas/world-class-healthcarePre (Accessed July 2016). |
[6] | United Arab Emirates Ministry of Health and Prevention. National Program for Government Communication. Healthy children 2021. (2016) . http://healthychildren2021.ae/?lang=EN (Accessed July 10 2016). |
[7] | Health Authorities Abu Dhabi. Ending Childhood Obesity – a call to action. Abu Dhabi 2016 Report. (2016) , UAE. |
[8] | Auchincloss AH , Leonberg BL , Glanz K , Bellitz S , Ricchezza A , Jervis A . Nutritional value of meals at full-service restaurant chains. J Nutr Educ Behav. (2014) ;46: (1):75–81. |
[9] | Jarlenski MP , Wolfson JA , Bleich SN . Macronutrient composition of menu offerings in fast food restaurants in the U.S.. Am J Prev Med. (2016) ;51: (4):e91–7. |
[10] | Urban LE , Weber JL , Heyman MB , et al. Energy contents of frequently ordered restaurant meals and comparison with human energy requirements and US Department of Agriculture Database Information: A Multisite Randomized Study. J Acad Nutr Diet. (2016) ;116: (4):590–8. |
[11] | Batada A , Bruening M , Marchlewicz EH , Story M , Wootan MG . Poor nutrition on the menu: Children’s meals at America’s top chain restaurants. Child Obes. (2012) ;8: (3):251–4. |
[12] | Urban LE , Lichtenstein AH , Gary CE , et al. The energy content of restaurant foods without stated calorie information. JAMA Intern Med. (2013) ;173: :1292–9. |
[13] | Powell LM , Nguyen BT . Fast-food and full-service restaurant consumption among children and adolescents: Effect on energy, beverage, and nutrient intake. JAMA Pediatr. (2013) ;167: (1):14–20. |
[14] | Burke S , McCarthy S , O’Neill J , et al. An examination of the influence of eating location on the diets of Irish children. Pub Health Nutr. (2007) ;10: (6):599–607. |
[15] | Lachat C , Nago E , Verstraeten R , Roberfroid D , Van Camp J , Kolsteren P . Eating out of home and its association with dietary intake: A systematic review of the evidence. Obes Rev. (2012) ;13: :329–46. |
[16] | Scourboutakos MJ , L’Abbe MR . Sodium levels in Canadian fast-food and sit-down restaurants. Can J Public Health. (2013) ;104: (1):e2–8. |
[17] | Vandevijvere S , Lachat C , Kolsteren P , Van Oyen H . Eating out in Belgium: Current situation and policy implications. Br J Nutr. (2009) ;102: (6):921–8. |
[18] | Krukowski , RA , Eddings K , Smith West D . The children’s menu assessment: Development, evaluation, and relevance of a tool for evaluating children’s menus. J Am Diet Assoc. (2011) ;111: (6):884–8. |
[19] | Reeves S , Wake Y , Zick A . Nutrition labelling and portion size information on children’s menus in fast-food and table-service chain restaurants in London, UK. J Nutr Educ Behav. (2011) ;43: (6):543–7. |
[20] | Poti JM , Popkin BM . Trends in Energy Intake among US Children by Eating Location and Food Source 1977–2006, J Acad Nutr Diet ((2014) ;114: (6):908–17. |
[21] | Adair LS , Popkin BM . Are child eating patterns being transformed globally? Obes Res. ((2005) ;13: (7):1281–99. |
[22] | Mosaad AT , Younis MZ . Health policies and intervention strategies: A description of current issues and approaches to care of the public health and health care system in the United Arab Emirates. J Health Care Finance. (2014) ;40: (3):86–100. |
[23] | Worldbank.org.GDP at market prices. UAE, (2016) Available from: http://data.worldbank.org/country/united-arab-emirates (Accessed Nov. 2016). |
[24] | Katsaiti M , El Anshasy AA . What determines obesity in oil-rich United Arab Emirates? New evidence from survey data. Appl Econ Lett. (2013) ;20: (17):1574–9. |
[25] | Pan Arab Research Center. TGI. (2014) ; V3.3. Dubai, UAE. |
[26] | Bin Zaal A , Musaiger A , D’Souza R . Dietary habits associated with obesity among adolescents in Dubai, United Arab Emirates. Nutr Hos. (2009) ;24: (4):437–44. |
[27] | Thompson OM , Ballew C , Resnicow K , et al. Food purchased away from home as a predictor of change in BMI z-score among girls. Int J Obes. (2004) ;28: :282–9. |
[28] | Duffey KJ , Gordon-Larsen P , Jacobs DR , Williams OD , Popkin BM . Differential associations of fast food and restaurant food consumption with 3-y change in body mass index: The Coronary Artery Risk Development in Young Adults Study. Am J Clin Nutr. (2007) ;85: (1):201–8. |
[29] | Altman M , Holland JC , Lundeen D , et al. Reduction in food away from home is associated with improved child relative weight and body composition outcomes and this relation is mediated by changes in diet quality. J Acad Nutr Diet. (2015) ;115: (9):1400–07. |
[30] | Ayala GX , Castro IA , Pickrel JL , et al. A restaurant-based intervention to promote sales of healthy children’s menu items: The Kids’ Choice Restaurant Program cluster randomized trial. BMC Public Health. (2016) ;16: :250. |
[31] | Anzman-Frasca S , Mueller MP , Sliwa S , et al. Changes in children’s meal orders following healthy menu modifications at a regional U.S. restaurant chain. Obesity. (2015) ;23: (5):1055–62. |
[32] | National Restaurant Association (2016). Kids Live Well Nutritional Criteria. US, (2016) . Available from: http://www.healthydiningfinder.com/kids_livewell/criteria (Accessed June. 2016). |
[33] | Hajat C , Harrison O , Al Siksek Z . Weqaya: A population-wide cardiovascular screening program in Abu Dhabi, United Arab Emirates. Am J Public Health. (2012) ;102: (5):909–14. |
[34] | Health Authorities Abu Dhabi. Standards for labeling food with Weqaya logo, page 3-4. UAE, (2012) . Available from: http://www.haad.ae/HAAD/LinkClick.aspx?fileticket=VyqVIfF-KLY%3D&tabid=819 (Accessed Nov 2017). |
[35] | Hashim R , Thomson WM , Ayers KMS , Lewsey JD . Dental caries experience and use of dental services among preschool children in Ajman, UAE. Int J of Ped Dentistry. (2006) ;16: :257–62. |
[36] | U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans. 8th edition. US, 2015. Available from: http://health.gov/dietaryguidelines/2015/guidelines/ (Accessed Nov 2017). |
[37] | World Health Organization. Sugars intake for adults and children-Guideline. (2015) WHO, Geneva. |
[38] | Anzman-Frasca , S , Dawes F , Sliwa S , et al. Healthier side dishes at restaurants: An analysis of children’s perspectives, menu content, and energy impacts. Int J Behav Nutr Phys Act. (2014) ;11: :81. |
[39] | American Pediatric Association. Food and feeding. US, 2017. Available from: https://www.aaorg/en-us/advocacy-and-policy/aap-health-initiatives/HALF-Implementation-Guide/Age-Specific-Content/Pages/Preschooler-Food-and-Feeding.aspx (Accessed Nov. 2017). |
[40] | Burt BA , Pai S . Sugar consumption and caries risk: A systematic review. J Dent Ed. (2001) ;65: :1017–23. |
[41] | An R. Plain water and sugar-sweetened beverage consumption in relation to energy and nutrient intake at full-service restaurants. Nutrients. (2016) ;8: (5):263. |
[42] | Bleich SN , Wolfson JA , Jarlenski MP . Calorie changes in chain restaurant menu items: Implications for obesity and evaluations of menu labelling. Am J Prev Med. (2015) ;48: (1):70–5. |
[43] | Wang YC , Ludwig DS , Sonneville K , Gortmaker SL . Impact of change in sweetened caloric beverage consumption on energy intake among children and adolescents. Arch Pediatr Adolesc Med. (2009) ;163: (4):336–443. |
[44] | Anzman-Frasca S , Mueller MP , Lynskey VM , Harelick L , Economos CD . Orders of healthier children’s items remain high more than two years after menu changes at a regional restaurant chain. Health Aff (Millwood). (2015) ;34: (11):1885–92. |

