
Patient Selection for Active Surveillance for Small Renal Masses: A Systematic Review of the Literature
Abstract
BACKGROUND:
The role of active surveillance (AS) has been recognized as a management strategy for localized small renal masses (SRMs). The EAU guidelines suggest AS can be offered to frail and/or comorbid patients diagnosed with SRM due to the low cancer-specific-mortality (CSM) and higher competing-cause mortality. As specific cut-offs defining the characteristics of frail and comorbid patients who may benefit from AS remain less clear, our objective is to conduct a systematic review aiming to identify potential characteristics that could assist physicians in shared decision-making.
METHODS:
The systematic literature review was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. Two authors independently screened the literature according to the PICOs criteria previously outlined in our registered review protocol (via Pubmed, Embase, and the Cochrane Central Register of Controlled Trials), extracted data, and assessed the risk of bias, using Newcastle-Ottawa Scale. Studies that analyzed differences in patient’s tumor-related and molecular characteristics associated with any differences in growth rate (GR), overall survival (OS), cancer-specific survival (CSS), and metastasis-free survival (MFS), were considered eligible.
RESULTS:
Nineteen studies comprising a total of 5105 patients were analyzed. Patient-specific factors such as age and cardiovascular index, which demonstrated a predominant impact on OS, exhibited a high degree of consistency across the analyzed studies. Less concordance was found when exploring GR, with the main predictors being ethnicity, age, sex, comorbidity, symptoms, and eGFR. The analysis of tumor-related characteristics, such as tumor size, nephrometry score, and mass histology, among others, yielded contradictory outcomes concerning their impact on GR and CSS.
CONCLUSION:
Age, cardiovascular index, and chronic kidney disease have shown to be reliable predictors of OS. Nonetheless, significant debates persist regarding tumor characteristics or molecular markers that may influence survival and GR.
Further research is awaited to shed light on the potential to identify prognostic factors. This would aid in pinpointing the subgroup of patients who could experience additional benefits from AS, potentially leading to a reduced risk of progression.
It is imperative to standardize approaches to AS and reporting of results, as this will be pivotal for future quantitative analyses.
INTRODUCTION
Small renal masses (SRMs) are defined as localized renal tumors with a maximal diameter of ≤4 cm [1] and up to 40% are benign [2, 3]. Moreover, a considerable amount of malignant SRMs have indolent behavior with a low risk of metastatic progression [4, 5]. Nevertheless, metastases have been reported to occur in 0–2% of patients with SRMs during surveillance [6, 7], and the challenge is in successful patient selection.
Active surveillance (AS) has gained traction in clinical practice in recent years. It is currently considered a safe option for managing SRM in terms of cancer-specific survival (CSS) and cost-effectiveness [8–10] in selected cases. This strategy can safely reduce the number of unnecessary interventions [11, 12].
Identifying patient and tumor-related characteristics that can predict metastatic progression is paramount. The guidelines of the American Urological Association (AUA) and the European Association of Urology (EAU) recommend AS in selected patients. These include elderly patients, those with reduced life expectancy, individuals not fit for surgery, and patients with SRMs exhibiting specific radiologic characteristics such as non-infiltrative, low complexity, or predominantly cystic features [13, 14].
Despite including AS as a safe strategy in the guidelines, no unique and validated protocol has been proposed, and uncertainty about survival outcomes still exists, as it demonstrated that even SRMs have metastatic potential [15, 16]. To address this, we conducted this systematic review to analyze the existing literature that examined tumor and patient-related characteristics, assessing the statistical correlation with survival outcomes or growth rate, as the latter demonstrated to be correlated with survival outcomes [17].
METHODS
Data sources and searches
After obtaining registration of review protocol on PROSPERO (ID: CRD42023471417), we searched PubMed, Embase, and the Cochrane Central Register of Controlled Trials from January 1, 1997 through July 1, 2023. The start date of the search was selected as the year cT1a tumor was defined according to the Union for International Cancer Control (UICC)/American Joint Committee on Cancer (AJCC) TNM scheme as a renal mass with a maximal diameter ≤4 cm.
The systematic review was conducted according to the principles highlighted by the EAU Guidelines Office and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [18, 19]. Searches were not restricted by language. We screened the databases using medical subject headings (MeSH) and free-text protocols.
The search terms used for the different databases are specified in the Supplementary material, Table 1. We manually searched the bibliographies of the included studies and previous reviews related to the topic to identify additional eligible articles.
Inclusion and exclusion criteria
A specific population (P), intervention (I), comparator (C), outcome (O), and study design (S) (PICOS) framework was specified to assess study eligibility. The following framework was applied: (P): Newly diagnosed adults with solid or cystic renal masses with a solid component ≤4 cm, (I) AS with monitoring of the tumor and metastasis by CT scan or MRI or CEUS (possible variations in protocols may arise due to the current lack of validation for different approaches), with or without delayed intervention; (C) Comparisons were made among various groups: patients who developed metastasis, patients who passed away during the follow-up period (due to both cancer-related and unrelated causes), patients exhibiting a rapid growth rate (with the definition of a slow growth rate varies depending on the specific studies), and patients who did not experience progression throughout the follow-up period of the studies; (O) Outcomes: metastasis-free rate, growth rate, overall survival, cancer-specific survival; (S) type of study: controlled studies (randomized controlled trials, non-randomized controlled trials, and comparative cohort studies) and uncontrolled studies (single cohort studies): Data from uncontrolled studies that addressed active surveillance are described in the report. Excluded all the studies including only specific groups of patients: patients diagnosed with syndromes related to RCC, as well as studies focusing exclusively on patients with benign renal masses such as oncocytoma, oncocytic neoplasms, angiomyolipoma, or cystic masses, were not included in the study. Moreover, thesis, case reports, and dissertations were excluded.
Study selection, data extraction, and quality assessment
Articles were screened by two authors (A.D. and C.M.), who determined eligibility based on the abovementioned criteria. Records were reviewed using Rayyan software (available at https://rayyan.qcri.org/reviews).
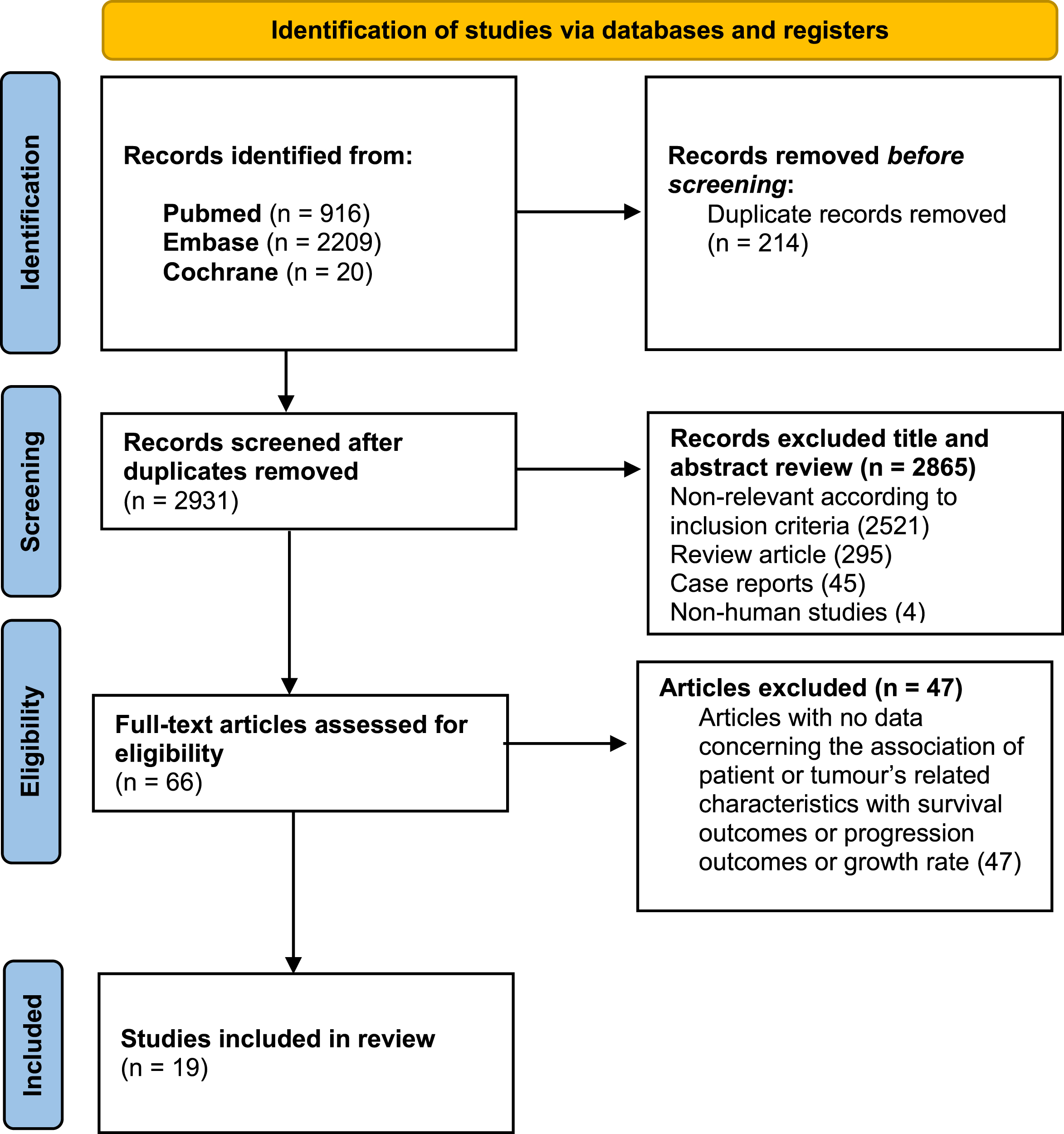
After an initial selection of articles, studies that did not meet the criteria specified by PICOS were excluded. The two authors retrieved full paper articles and thoroughly assessed them for eligibility. In case of any disagreements, a consensus was reached through discussion. Ultimately, 19 articles were suitable for the final analysis (Fig. 1). The Newcastle-Ottawa Scale was used to assess the risk of bias (Supplementary Material, Table 2 and Table 3) [20].
Fig. 1
Flow diagram for studies retrieval.
A single investigator reviewed each study to extract patient and tumor characteristics, and additional investigators verified the accuracy of the findings. Extracted data included selection criteria for AS, patient demographics (number of patients, average/median/range of age, comorbidity score), tumor-related characteristics (average/range of maximal tumor diameter, and solid/cystic features), growth rate, metastasis-free survival (MFS), cancer-specific survival (CSS) and overall survival (OS); factors associated with either one or more outcomes (OS, CSS, MFS, GR).
RESULTS
Our systematic literature review revealed 19 studies comprising 5105 patients [6, 7, 21–37] (Tables 1 and 2). Five of the 19 studies had a small sample size (<50 patients) [23, 25, 26, 33, 36]. Most articles reported results from single-center retrospective databases. Six papers were prospective: three from the DISSRM registry [7, 27, 28], one from RC4 (Renal Cell Carcinoma Consortium of Canada) [6], one reported a pooled analysis of RC4 cohort and a single center retrospective data [34], and one from a single center cohort [33].
Table 1
Studies characteristics
| Growth rate (>0.5 cm/year) | Cancer-specific survival | Metastasis-free survival | Overall survival | ||||||||
| Author, Year | Study design | N of Patients | Follow-up, Months | Events | Rate | Events | Rate | Events | Rate | Events | Rate |
| Pierorazio, 2015 | Prospective, Multicenter (DISSRM) | 223 | 25.2 | 34 | 15.2% | 0 | 100% | 0 | 100% | 13 | 94.2% |
| Jewett, 2011 | Prospective, Multicenter (RC4) | 178 | >12 | 12 | 6.7% | 2 | 98.9% | 2 | 98.9% | 10 | 94.9% |
| Leonard, 2013 | Retrospective, Population-based database | 133 | 27.9 | 7 | 5.26% | NR | NR | 1 | 99.2% | NR | NR |
| Bazan, 2021 | Retrospective, single-center | 89 | 55 | 3 | 3.4% | 0 | 100% | 0 | 100% | 6 | 93% |
| Finelli, 2020 | Retrospective and prospective cohort (pooled analysis), Multicenter | 136 | >5y (patients who remained in AS) | 49 | 36% | 3 | 97.8% | 6 | 95.6% | 29 | 78.7% |
| Zalimas, 2022 | Prospective, single center | 39 | 33 | 11 | 33.3% | NR | NR | 0 | 100% | NR | NR |
| Ajami, 2021 | Retrospective, single-center | 73 | 33 | 14 | 19.2% | NR | NR | 0 | 100% | NR | NR |
| Tang, 2022 | Retrospective, multicenter (SEER database) | 2776 | 51 | NS | NS | NS | NS | NS | NS | NS | NS |
| Patel, 2014 | Retrospective, multicenter (SEER database) | 754 | 56 | NS | NS | 67 | 91% | NS | NS | 253 | 60.6% |
| McIntosh, 2018 | Retrospective, single-center | 457 (69 > 4 cm separate analysis) | 67 | 114 | 24.9 | 5 | 98.9 | 8 | 98.3 | 73 | 84.0% |
| Schiavina, 2015 | Retrospective, single-center | 70 | 92.7 | 15 | 21.4% | 2 | 97.2 | 2 | 97.2% | 19 | 72.8% |
| Alam, 2023 | Prospective, multicenter (DISSRM) | 485 | 34 | 43 | 8.8% | 1 | 99.8% | 1 | 99.8% | 80 | 83.5% |
| Rasmussen, 2022 | Retrospective, single-center | 339 | 14.4 | 45 | 13.2% | 0 | 100% | 2 | 99.4% | 18 | 94.3% |
| Paterson, 2017 | Retrospective, multicenter | 226 | 19.5 | NS | NS | 9 | 96.0% | 7 | 97.0% | 42 | 81.4% |
| Uzosike, 2018 | Prospective, multicenter (DISSRM) | 271 | 22 | 46 | 17% | 0 | 100% | 0 | 100% | 28 | 89.7% |
| Youssif, 2007 | Retrospective, single-center | 35 | 47.6 | NS | NS | 1 | 97.1 | 2 | 94.1 | 4 | 88–6 |
| Brunocilla, 2014 | Retrospective, single center | 62 | 91.5 | 13 | 20.9% | 2 | 96.8 | NR | NR | 18 | 71% |
| Kato, 2004 | Retrospective, single-center | 18 | 22.5 | NS | NS | NR | NR | NR | NR | NR | NR |
| Sugimoto, 2013 | Retrospective, single-center | 34 | 26.6 | 8 | 23.5% | 1 | 87.5% | 1 | 96.2% | 3 | 72.6% |
Patients analyzed in the included studies had an age that ranges from 29 to 96 years. The maximal tumor diameter (MTD) range was 0.4 - 4 cm. Of the total cohort, the percentage range of patients for whom a fast growth rate was observed (which was in all studies a selection criterion for delayed intervention) was 3.4% to 36%.
Lastly, CSS, MFS, and OS were ranges were 87.5%–100%, 94.1%–100%, and 60.6%–94.9% respectively. The follow-up period ranged from 12 to 92.7 months. All results are reported in Table 4, Supplementary materials.
The heterogeneity in study design and the variation in the presentation of outcomes have limited the ability to conduct a meta-analysis of the abovementioned outcomes in a meaningful and accurate manner.
Patient-specific factors
Since AS is often reserved for elderly and co-morbid patients, mortality reported in included studies was largely driven by competing comorbidities, rather than the natural history of untreated SRM.
The most analyzed features were the one associated with frailty and comorbidity, most frequently age, Charlson comorbidity index (CCI), ECOG score and cardiovascular index (CVI).
Comorbidities and causes of death were well evaluated in Patel et al. series from the Surveillance, Epidemiology, and End-Results (SEER) who underwent deferred therapy [38]. The strongest association with decreased OS, with the most significant hazard ratio (HR) was found for chronic heart failure (CHF) and chronic kidney disease (CKD). The latter was found to be significantly associated even with GR in the Paterson et al. cohort [22], where baseline eGFR of less than 60/min/1.73 m2 and the presence of concurrent comorbidity were statistically associated with growth, while Schiavina et al. [29] did not find patient comorbidity, as measured by CCI and BMI, to predict GR in the analyzed population (even if a smaller population was analyzed). However, male sex and symptomatic presentation were significant predictors of tumor GR.
In Patel et al. cohort, with the aim of risk stratification for survival, CVI was compared with CCI by assessing 5-year survival probabilities for OS and CSS. The CVI provided better survival risk stratification.
The findings of Patel et al. are consistent with those of Pierorazio et al. [7]. In the prospective multicentric DISSM registry analysis, Pierorazio’s group observed a CSS rate of 100% for AS. However, they noted that the AS arm’s 5-year OS rate was 75%. In univariate analysis, the group identified age and CVI as the only predictors of all-cause mortality. The group found age also to be associated with lower OS and dimensional progression, which was defined by the author as GR > 0.5 cm/year or greatest tumor diameter > 4.0 cm. 15% of their cohort experienced a GR > 0.5 cm/y during AS and only 2 progressed over 4.0 cm. Another factor predictive of dimensional progression while on AS included also ECOG score≥2.
The DISSRM registry cohort was also examined by Uzosike et al. [27]. and Alam et al. [28]. Uzosike et al. found no significant patient characteristics associated with GR when analyzed as a binary variable (≥0.5 or < 0.5 cm per year). The group of Alam et al., on the other hand, assessed age as a continuous variable and found no statistically significant association with growth rate. Notably, Afro-American patients exhibited a lower GRi (GR from the initial image) than Caucasian patients, had a younger age of onset (69.6 vs. 71.2 yr), and presented with larger tumors at the initial scan (2.1 vs. 1.8 cm). When considering age thresholds, only ages 65 and 70 were respectively associated with increased GRi and GRp (GR from the previous image).
Tumor-specific factors
Tang et al. [31] utilized the SEER database to investigate the importance of maximal tumor diameter. Their focus was on overall mortality over ten years, revealing rates of 52.1% in the ≤1 cm group, 76.8% in the > 3–4 cm group, and 10-year cancer specific mortality (CSM) of 12.8% in the ≤1 cm group to 31.3% in the > 3–4 cm group. Thus all-cause mortality and cancer-specific mortality increased with larger tumor size.
In contrast, an analysis of the DISSM registry by Pierorazio et al. [7] did not find MTD, ECOG score, or RENAL nephrometry score to predict OS. The nephrometry score failed to achieve significance even in predicting GR in the Schiavina et al. group [29]. However, within the cohort studied by Paterson et al. [22], central tumor location emerged as a statistically significant predictor of growth.
Differences between solid and cystic masses were analyzed by McIntosh et al. who found a significantly improved OS for patients with a cystic mass compared to patients with solid ones [30].
Concerning histological information, Finelli et al. group focused on two biopsy-proven pooled cohorts (one retrospective and one prospective cohort) [34]. Among 136 lesions, only lesions of clear-cell subtype showed metastatic potential. Clear cell histology was also a predictor of GR, which was the most analyzed criterion by the included studies. Schiavina et al. [29] found a slightly greater tendency in faster growth rates was observed among histologically proven renal cancers compared with unknown tumors, even though this result did not reach statistical significance.
Sugimoto et al. [26] found no significant difference in time to tumor doubling according to histopathological grade and subtype. In a study with a larger sample size than that of Sugimoto et al., Paterson et al. [22] did not establish any significant differences in GR between histologically confirmed benign and malignant masses.
In the DISSM registry cohort [7], six abovementioned patients experienced a GR > 0.5 cm/y underwent delayed intervention, finding no correlation with tumor histology, grade, or stage. Strikingly, the fastest-growing tumor was an oncocytoma (1.7 cm/y). These results are concordant with those obtained by Jewett et al. [6], who found that GR between RMB-proven low and high-grade lesions did not appear to be different.
Initial MTD was a criterion well evaluated through the studies as a possible predictor of GR, with six studies finding no correlation with subsequent GR [23, 24, 29, 30, 32, 35].
Radiologic characteristics were also analyzed. Ajami et al. [32] found no statistical differences regarding the initial size, tumor heterogeneity, intratumoral vessels, irregular edge, intratumoral calcification, ratio of small/long axis, ratio of cortical/tumor density in unenhanced and enhanced (portal phase) CT, and angular interface, in the GR subgroups. When analyzing renal mass images, Rasmussen et al. [21] applied to their cohort of patients the clear cell likelihood score (ccLS), obtaining that GR of ccLS 4–5 SRMs grew faster than ccLS 1–2 and ccLS 3 SRMs by diameter andvolume.
Immunohistochemical and molecular characteristics
Specific immunohistochemical and molecular characteristics that may predict clinical outcomes of patients with SRMs also have been explored, albeit in few studies. Kato et al.[25] looked into the Ki-67 index, and found that it did not correlate with tumor GR. No significant difference in GR was observed between grade 1 and grade 2 tumors. Instead TUNEL positive ratio, which detects DNA fragmentation due to apoptosis, correlated with GR and grade 3 tumors were found to have a higher GR compared to that of grade 2 tumors. Zalimas et al. [33] analyzed urine molecular biomarkers for detection and follow-up of SRMs, finding a lower level of methylation on urines of the biomarker TFA2B.
DISCUSSION
In daily practice, the challenge for clinicians is how to select patients best suitable for such strategy. Currently, the EAU guidelines do not provide precise algorithms, and recommend AS for frail and comorbid patients only [39]. This is also because there has been a lack of high quality data supporting that analyzes factors associated with the growth rate of diagnosed lesions and the survival in patients with SRMs.
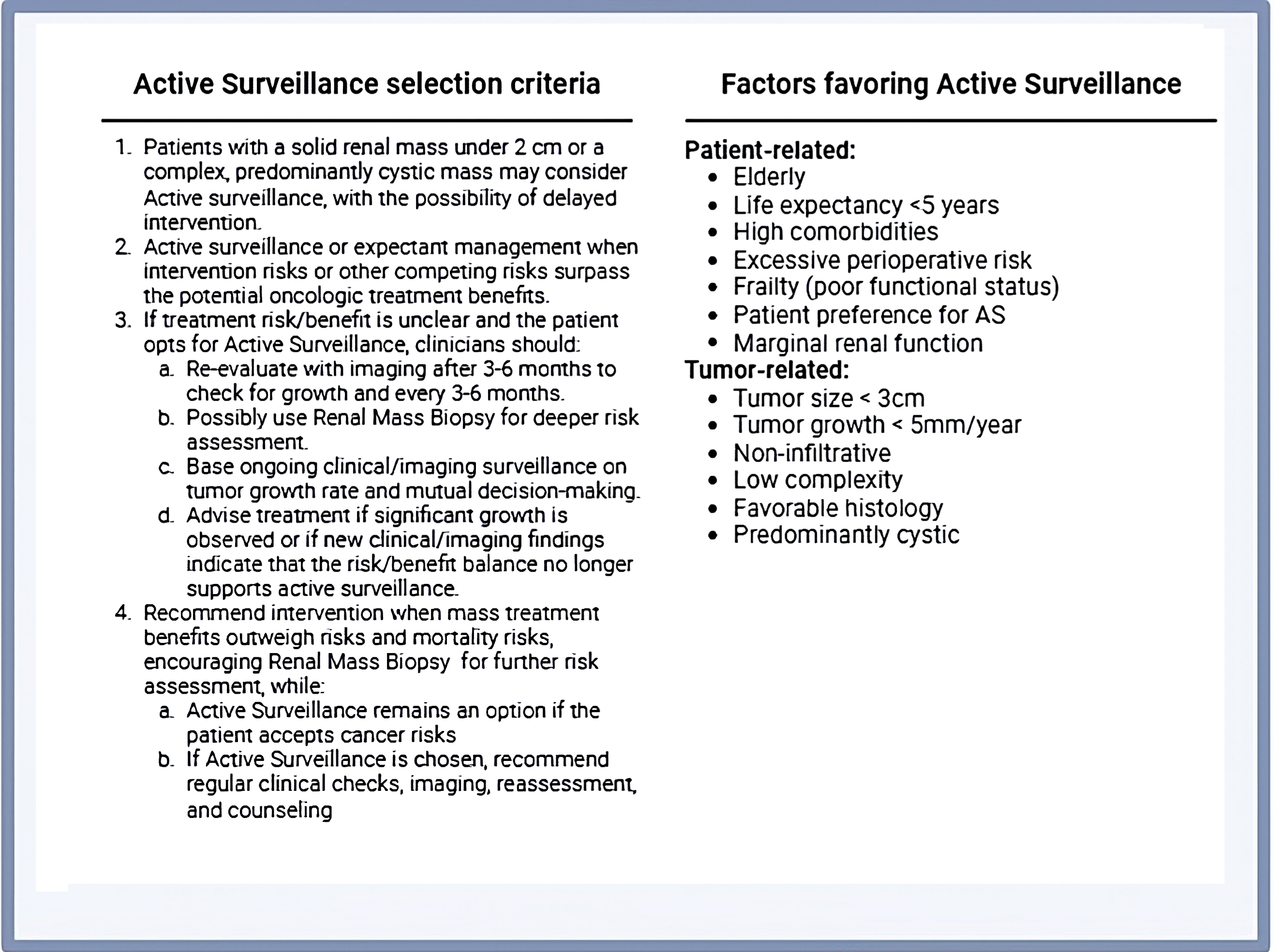
The AUA guidelines are more guiding towards AS, in particular in elderly and comorbid patients, those with high perioperative risk and/or marginal renal function, and tumors with a diameter ≤3 cm. Additionally, they recommend AS for non-invasive, low-complexity masses with favorable histology, and predominantly cystic characteristics (summarizing table adapted from AUA guidelines on Box 1) [13]. The difference between the two guidelines, despite their emphasis on evidence-based medicine through a similar approach, likely reflects a lack of strong evidence on the matter.
Box 1
Algorithm for AS in SRM: adapted from AUA guidelines.
To this end, this systematic review investigated all literature that examined tumor and patient-related characteristics and molecular factors impacting the endpoints of GR, MFS, CSS, and OS.
Given its correlation with more aggressive behavior, we have opted to include GR as an additional criterion alongside survival-based criteria [16]. Among the studies in this cohort, a significant number defined as a fast GR an increase of 0.5 cm per year or more. However, it is worth noting that this specific cut-off was not universally utilized in all studies, which presents a potential limitation. We believe further studies focusing on this aspect should report mean/median growth rate and the proportion of tumors that have grown more than 0.5 cm/yr to facilitate further quantitative analysis.
Additionally, many studies defined a GR criterion of greater than 0.5 cm per year about the previous imaging based on the assumption that the growth of SRMs may not follow a linear trajectory over time. Therefore, a sudden change in growth speed could potentially serve as a trigger for intervention. Only one study [28] employed two references for assessing GR, namely the GR calculated from the initial image and the GR based on the prior image. Higher GR potentially reflects more aggressiveness, and a GR ≥0.5 cm/year can be an arbitrary cut-off of a continuous variable. However, more research is warranted in this area to establish the exact significance of these measures in forecasting the clinical course, metastatic progression, and CSS.
Furthermore, the utilization of AS in the management of SRMs should also need to be revised more individualized with the recent 5th Edition of WHO 2022 Renal Tumor Pathology Nomenclature as because some novel genetically and molecularly defined subtypes in WHO 2022 have more aggressive potential regardless of their size [40].
There is consensus in the literature to regard age as a prognostic factor associated with increased overall mortality in patients with SRMs. This consensus makes advanced age a reliable factor when opting for AS. However, evidence also links advanced age to a higher risk of dimensional and metastatic progression, as highlighted in some selected studies [7, 28, 36]. Regarding comorbidities, numerous pieces of evidence have indicated that CVI, CCI, and ECOG scores can predict lower OS [7, 38], and some evidence even shows a certain predictive value for GR [7, 22]. A potential limitation of the study lies in the fact that we analyzed factors that are solely associated with dimensional progression or cancer-specific survival. For instance, factors such as age and frailty, the RENAL score, or renal function may be linked to a higher likelihood of progression, but ultimately making surgery a less feasible option, making the clinical management a dilemma.
Another potential limitation of the study is that our PICOS criteria only included studies focused on renal masses of ≤4 cm as maximum tumor diameter, which excludes a significant body of literature covering exclusively ≤2 cm lesions specifically. Notably, growing evidence supports AS as a viable initial management strategy for patients with masses ≤2 cm, irrespective of age and comorbidities [41]. It’s worth mentioning that some of the included studies analyzed maximum tumor diameter as a discreet variable and reached similar conclusions [31]. Furthermore, the current guidelines from AUA recommend consider a tumor size of 3 cm or smaller as a favorable criterion for selecting Active Surveillance among tumor-related factors. The European guidelines may also consider adopting this threshold in the future. Our main contention is that the analyzed patients’ characteristics, namely age and comorbidities, can serve as an essential knowledge base when determining the treatment strategy for patients with SRM up to 4 cm.
Currently most AS series do not have information on histology (i.e. patients are “treated” with AS without a biopsy). Therefore, patients may be followed-up for benign masses, and we know that the smaller the mass the higher the probability of benign histology [42, 43]. Our findings have yielded conflicting results concerning the impact of tumor histological characteristics on treatment decision-making for SRMs. Further studies are required to gain a better understanding of the precise role of RMB in guiding the management of SRMs based on tumor biology. The ongoing European Active Surveillance of Renal Cell Carcinoma (EASE RCC) study is actively enrolling participants from across Europe [11]. The study’s primary goal is to evaluate the survival outcomes of patients diagnosed with SRMs who undergo AS. An essential aspect of this trial is the requirement for histological confirmation through biopsy, aiming to pinpoint clinical and pathological factors that influence the growth rate and progression of SRMs. The integration of RMB in AS trials is anticipated to reduce the inclusion of patients without histologically confirmed RCC and add additional precious information to the findings of Finelli et al. [34].
Another limitation of the study is the inclusion of a heterogeneous cohort of patients and variations in the quality of the included studies. In particular, survival outcomes strictly depends on the study design, patient selection, and criteria for deferred treatment triggers. Standardization of AS protocols and deferred treatment triggers will be vital for future quality evidence.
We believe that the described clinical, radiological, and molecular characteristics that are correlated to the clinical outcome of these patients may feed specific artificial intelligence algorithms in the future, as their value has already been demonstrated in RCC diagnosis, treatment, and prognosis prediction [44, 45].
It will be interesting in the next future, beyond clinical and radiological factors, to identify biomarkers that could help in predicting the risk of micrometastatic spread and therefore guide towards a more interventionist approach. As known, RCC represents a tumor typically considered low shedding, and therefore with low levels of circulating tumor DNA (ctDNA), whose detection this is even more difficult in the early-stages. Plasma cell-free DNA (cfDNA) test represents a promising approach for multi-cancer early detection through a genome-wide DNA methylation enrichment platform also for early-stage cancer types, including RCC [44].
CONCLUSIONS
This review outlined how the current scientific literature is in agreement regarding age, CVI, and CKD as factors associated with decreased OS in patients with SRMs. Cystic masses appear to present a lower risk during surveillance compared to solid masses. However, there is still ongoing debate regarding the reliability of histology on renal mass biopsy as a predictor of GR and/or survival. Concerning size, at present, there is insufficient evidence to establish a specific cut-off for the safety of AS, as findings vary among the largest patient cohorts. In the realm of Immunohistochemical and molecular characteristics as predictors, conclusive evidence remains elusive, necessitating further studies. Prospective series, conducted with standardized AS protocols, methodologies, and results reports are crucial for future quantitative analyses.
ACKNOWLEDGMENTS
Dr. Hannah Warren who significantly contributed to the enhancement of the manuscript’s quality.
Her expertise and thoughtful guidance have been instrumental in shaping the final version of this work.
FUNDING
The authors report no funding.
AUTHOR CONTRIBUTIONS
All authors read and approved the final version of the manuscript.
CONFLICT OF INTEREST
Peter F.A. Mulders is a Co-Editor-in-Chief of this journal, but was not involved in the peer-review process of this paper, nor had access to any information regarding its peer-review.
Alfredo Distante, Riccardo Bertolo, Riccardo Campi, Selcuk Erdem, Anna Calio, Carlotta Palumbo, Nicola Pavan, Chiara Ciccarese, Umberto Carbonara, Michele Marchioni, Eduard Roussel, Zhenjie Wu, Peter F.A. Mulders and Constantijn H.J. Muselaers certify that there is no conflict of interest with any financial organization regarding the material discussed in the manuscript.
DATA AVAILABILITY
This article is a systematic review, and as such, it does not contain any new data generated by our research team. The findings are based on published studies that are publicly available. The references for all studies included in this review are provided in the reference list. Any additional data supporting the analysis and conclusions of this review, such as search strategies and selection criteria, are included within the article and its supplementarymaterials.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/KCA-230025.
REFERENCES
[1] | Finelli A , Ismaila N , Bro B , Durack J , Eggener S , Evans A , et al. Management of small renal masses: American society of clinical oncology clinical practice guideline. Journal of Clinical Oncology. (2017) ;35: :668–80. https://doi.org/10.1200/JCO.2016.69.9645. |
[2] | Kurban LAS , Vosough A , Jacob P , Prasad D , Lam T , Scott N , et al. Pathological nature of renal tumors – does size matter? Urol Ann. (2017) ;9: :330. https://doi.org/10.4103/UA.UA_17_17. |
[3] | Johnson DC , Vukina J , Smith AB , Meyer AM , Wheeler SB , Kuo TM , et al. Preoperatively misclassified, surgically removed benign renal masses: a systematic review of surgical series and United States population level burden estimate. J Urol. (2015) ;193: :30–5. https://doi.org/10.1016/J.JURO.2014.07.102. |
[4] | Rothman J , Egleston B , Wong YN , Iffrig K , Lebovitch S , Uzzo RG . Histopathological characteristics of localized renal cell carcinoma correlate with tumor size: a SEER analysis. J Urol. (2009) ;181: :29–34. https://doi.org/10.1016/J.JURO.2008.09.009. |
[5] | Monda SM , Lui HT , Pratsinis MA , Chandrasekar T , Evans CP , Dall’era MA , et al. The Metastatic Risk of Renal Cell Carcinoma by PrimaryTumor Size and Subtype. (2023) . https://doi.org/10.1016/j.euros.2023.04.015. |
[6] | Jewett MAS , Mattar K , Basiuk J , Morash CG , Pautler SE , Siemens DR , et al. Active Surveillance of Small Renal Masses: Progression Patterns of Early Stage Kidney Cancer. Eur Urol. (2011) ;60: :39–44. https://doi.org/10.1016/J.EURURO.2011.03.030. |
[7] | Pierorazio PM , Johnson MH , Ball MW , Gorin MA , Trock BJ , Chang P , et al. Five-year Analysis of a Multi-institutional Prospective Clinical Trial of Delayed Intervention and Surveillance for Small Renal Masses: The DISSRM Registry. Eur Urol. (2015) ;68: :408–15. https://doi.org/10.1016/J.EURURO.2015.02.001. |
[8] | Sanchez A , Feldman AS , Ari Hakimi A . Current Management of Small Renal Masses, Including Patient Selection, Renal Tumor Biopsy, Active Surveillance, and Thermal Ablation. Journal of Clinical Oncology. (2018) ;36: :3591. https://doi.org/10.1200/JCO.2018.79.2341. |
[9] | Su ZT , Patel HD , Huang MM , Alam R , Cheaib JG , Pavlovich CP , et al. Active Surveillance versus Immediate Intervention for Small Renal Masses: A Cost-Effectiveness and Clinical Decision Analysis. J Urol. (2022) ;208: :794–802. https://doi.org/10.1097/JU.0000000000002812. |
[10] | Klatte T , Berni A , Serni S , Campi R . Intermediate- and long-term oncological outcomes of active surveillance for localized renal masses: a systematic review and quantitative analysis. BJU Int. (2021) ;128: :131–43. https://doi.org/10.1111/BJU.15435. |
[11] | Mir MC , Capitanio U , Bertolo R , Ouzaid I , Salagierski M , Kriegmair M , et al. Role of Active Surveillance for Localized Small Renal Masses. Eur Urol Oncol. (2018) ;1: :177–87. https://doi.org/10.1016/J.EUO.2018.05.001. |
[12] | Campi R , Sessa F , Corti F , Carrion DM , Mari A , Amparore D , et al. Triggers for delayed intervention in patients with small renal masses undergoing active surveillance: a systematic review. Minerva Urol Nefrol. (2020) ;72: :389–407. https://doi.org/10.23736/S0393-2249.20.03870-9. |
[13] | Campbell SC , Uzzo RG , Karam JA , Chang SS , Clark PE , Souter L . Renal Mass and Localized Renal Cancer: Evaluation, Management, and Follow-up: AUA Guideline: Part II. J Urol. (2021) ;206: :209–18. https://doi.org/10.1097/JU.0000000000001912. |
[14] | Ljungberg B , Albiges L , Abu-Ghanem Y , Bedke J , Capitanio U , Dabestani S , et al. European Association of Urology Guidelines on Renal Cell Carcinoma: The 2022 Update. Eur Urol. (2022) ;82: :399–410. https://doi.org/10.1016/J.EURURO.2022.03.006. |
[15] | Tan YG , Khalid MF Bin , Villanueva A , Huang HH , Chen K , Sim ASP . Are small renal masses all the same? Int J Urol. (2020) ;27: :439–47. https://doi.org/10.1111/IJU.14219. |
[16] | Smaldone MC , Kutikov A , Egleston BL , Canter DJ , Viterbo R , Chen DYT , et al. Small renal masses progressing to metastases under active surveillance: a systematic review and pooled analysis. Cancer. (2012) ;118: :997–1006. https://doi.org/10.1002/CNCR.26369. |
[17] | Park SW , Lee SS , Lee DH , Nam JK , Chung MK . Growth kinetics of small renal mass: Initial analysis of active surveillance registry. Investig Clin Urol. (2017) ;58: :429. https://doi.org/10.4111/ICU.2017.58.6.429. |
[18] | Liberati A , Altman DG , Tetzlaff J , Mulrow C , Gøtzsche PC , Ioannidis JPA , et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) ;62: :e1–34. https://doi.org/10.1016/J.JCLINEPI.2009.06.006. |
[19] | Knoll T , Omar MI , Maclennan S , Hernández V , Canfield S , Yuan Y , et al. Key Steps in Conducting Systematic Reviews for Underpinning Clinical Practice Guidelines: Methodology of the European Association of Urology. Eur Urol. (2018) ;73: :290–300. https://doi.org/10.1016/J.EURURO.2017.08.016. |
[20] | Wells G , Wells G , Shea B , Shea B , O’Connell D , Peterson J , et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality ofNonrandomised Studies in Meta-Analyses. (2014) . |
[21] | Rasmussen RG , Xi Y , 3rd SRC , Lee CJ , Cadeddu JA , Pedrosa I . Association of Clear Cell Likelihood Score on MRI and Growth Kinetics of Small Solid Renal Masses on Active Surveillance. AJR Am J Roentgenol. (2022) ;218: :101–10. https://doi.org/10.2214/AJR.21.25979. |
[22] | Paterson C , Yew-Fung C , Sweeney C , Szewczyk-Bieda M , Lang S , Nabi G . Predictors of growth kinetics and outcomes in small renal masses(SRM≤4cm in size): Tayside Active Surveillance Cohort (TASC)Study. Eur J Surg Oncol. (2017) ;43: :1589–97. https://doi.org/10.1016/j.ejso.2017.03.006. |
[23] | Youssif TA , Kassouf W , Steinberg J , Aprikian AG , Laplante MP , Tanguay S . Active surveillance for selected patients with renal masses: updated results with long-term follow-up. Cancer. (2007) ;110: :1010–4. https://doi.org/10.1002/CNCR.22871. |
[24] | Brunocilla E , Borghesi M , Schiavina R , Della Mora L , Dababneh H , La Manna G , et al. Small renal masses initially managed using active surveillance: results from a retrospective study with long-term follow-up. Clin Genitourin Cancer. (2014) ;12: :178–81. https://doi.org/10.1016/J.CLGC.2013.11.011. |
[25] | Kato M , Suzuki T , Suzuki Y , Terasawa Y , Sasano H , Arai Y . Natural history of small renal cell carcinoma: evaluation of growth rate, histological grade, cell proliferation and apoptosis. J Urol. (2004) ;172: :863–6. https://doi.org/10.1097/01.JU.0000136315.80057.99. |
[26] | Sugimoto K , Shimizu N , Oki T , Nose K , Nishioka T , Adomi S , et al. Clinical outcome of incidentally discovered small renal cell carcinoma after delayed surgery. Cancer Manag Res. (2013) ;5: :85–9. https://doi.org/10.2147/CMAR.S44221. |
[27] | Uzosike AC , Patel HD , Alam R , Schwen ZR , Gupta M , Gorin MA , et al. Growth Kinetics of Small Renal Masses on Active Surveillance: Variability and Results from the DISSRM Registry. J Urol. (2018) ;199: :641–8. https://doi.org/10.1016/j.juro.2017.09.087. |
[28] | Alam R , Yerrapragada A , Wlajnitz T , Watts E , Pallauf M , Enikeev D , et al. Evaluation of Growth Rates for Small Renal Masses in Elderly Patients Undergoing Active Surveillance. Eur Urol Open Sci. (2023) ;50: :78–84. https://doi.org/10.1016/j.euros.2023.02.004. |
[29] | Schiavina R , Borghesi M , Dababneh H , Bianchi L , Longhi B , Diazzi D , et al. Small renal masses managed with active surveillance: predictors of tumor growth rate after long-term follow-up. Clin Genitourin Cancer. (2015) ;13: :e87–92. https://doi.org/10.1016/j.clgc.2014.08.006. |
[30] | McIntosh AG , Ristau BT , Ruth K , Jennings R , Ross E , Smaldone MC , et al. Active Surveillance for Localized Renal Masses: Tumor Growth, Delayed Intervention Rates, and>5-yr Clinical Outcomes. Eur Urol. (2018) ;74: :157–64. https://doi.org/10.1016/j.eururo.2018.03.011. |
[31] | Tang Y , Liu F , Mao X , Li P , Mumin MA , Li J , et al. The impact of tumor size on the survival of patients with small renal masses: A population-based study. Cancer Med. (2022) ;11: :2377–85. https://doi.org/10.1002/cam4.4595. |
[32] | Ajami T , Sebastia C , Corominas D , Ribal MJ , Nicolau C , Alcaraz A , et al. Clinical and radiological findings for small renal masses under active surveillance. Urol Oncol. (2021) ;39: :499.e9–499.e14. https://doi.org/10.1016/j.urolonc.2021.04.010. |
[33] | Žalimas A , Kubiliūtė R , Žukauskaitė K Sabaliauskaitė R Trakymas M Letautienė S, et al. Urine Molecular Biomarkers for Detection and Follow-Up of Small Renal Masses. Int J Mol Sci. (2022) ;23. https://doi.org/10.3390/ijms232416110. |
[34] | Finelli A , Cheung DC , Al-Matar A , Evans AJ , Morash CG , Pautler SE , et al. Small Renal Mass Surveillance: Histology-specific Growth Rates in a Biopsy-characterized Cohort. Eur Urol. (2020) ;78: :460–7. https://doi.org/10.1016/j.eururo.2020.06.053. |
[35] | Leonard M , Tait CD , Gillan AS , Rai BP , Byrne DJ , Nabi G . Impact of multiple deprivations on detection, progression and interventions in small renal masses (less than 4cm) in a population based study. European Journal of Surgical Oncology (EJSO). (2013) ;39: :1157–63. https://doi.org/10.1016/J.EJSO.2013.06.014. |
[36] | Tan YG , Khalid MF Bin , Villanueva A , Huang HH , Chen K , Sim ASP . Aresmall renal masses all the same? Int J Urol. (2020) ;27: :439–47. https://doi.org/10.1111/IJU.14219. |
[37] | Bazan A , Carrion D , Rivas J , Quesada-Olarte J , Quintana L , Alvarez-Maestro M , et al. Active surveillance in renal tumors:Clinical and oncological outcomes. J Cancer Res Ther. (2021) ;17: :414–9. https://doi.org/10.4103/JCRT.JCRT_562_18. |
[38] | Patel HD , Kates M , Pierorazio PM , Gorin MA , Jayram G , Ball MW , et al. Comorbidities and causes of death in the management of localized T1a kidney cancer. Int J Urol. (2014) ;21: :1086–92. https://doi.org/10.1111/IJU.12527. |
[39] | Campi R , Berni A , Amparore D , Bertolo R , Capitanio U , Carbonara U , et al. Impact of frailty on perioperative and oncologic outcomes in patients undergoing surgery or ablation for renal cancer: a systematic review. Minerva Urology and Nephrology. (2022) ;74: :146–60. https://doi.org/10.23736/S2724-6051.21.04583-3. |
[40] | Moch H , Amin MB , Berney DM , Compérat EM , Gill AJ , Hartmann A , etal. The World Health Organization Classification of Tumours ofthe Urinary System and Male Genital Organs-Part A: Renal, Penile,and Testicular Tumours. Eur Urol. (2022) ;82: :458–68. https://doi.org/10.1016/J.EURURO.2022.06.016. |
[41] | Pecoraro A , Rosiello G , Luzzago S , Deuker M , Stolzenbach F , Tian Z , et al. Small Renal Masses With Tumor Size 0 to 2 cm: A SEER-Based Study and Validation of NCCN Guidelines. J Natl Compr Canc Netw. (2020) ;18: :1340–7. https://doi.org/10.6004/JNCCN.2020.7577. |
[42] | Thompson RH , Kurta JM , Kaag M , Tickoo SK , Kundu S , Katz D , et al. Tumor size is associated with malignant potential in renal cell carcinoma cases. J Urol. (2009) ;181: :2033–6. https://doi.org/10.1016/J.JURO.2009.01.027. |
[43] | Frank I , Blute ML , Cheville JC , Lohse CM , Weaver AL , Zincke H . Solid renal tumors: an analysis of pathological features related to tumor size. J Urol. (2003) ;170: :2217–20. https://doi.org/10.1097/01.JU.0000095475.12515.5E. |
[44] | Distante A , Marandino L , Bertolo R , Ingels A , Pavan N , Pecoraro A , et al. Artificial Intelligence in Renal Cell Carcinoma Histopathology: Current Applications and Future Perspectives. Diagnostics (Basel). (2023) ;13. https://doi.org/10.3390/DIAGNOSTICS13132294. |
[45] | Roussel E , Capitanio U , Kutikov A , Oosterwijk E , Pedrosa I , Rowe SP , et al. Novel Imaging Methods for Renal Mass Characterization: A Collaborative Review. Eur Urol. (2022) ;81: :476–88. https://doi.org/10.1016/J.EURURO.2022.01.040. |


