
First-Line Immuno-Oncology Combinations for Metastatic Clear Cell Renal Cell Carcinoma (mRCC): A Systematic Review of Phase III Clinical Trials
Abstract
BACKGROUND:
The introduction of immune checkpoint inhibitors rapidly changed treatment for patients with metastatic clear cell renal cell carcinoma (mRCC). First-line treatment now includes multiple immuno-oncology (IO) combinations that were approved over a short time period and were not directly compared in randomized clinical trials. Thus, clinicians face a challenge in individualizing first-line treatment to optimize clinical outcomes.
OBJECTIVE:
We sought to systematically review clinical outcomes for first-line IO combinations for patients with mRCC.
METHODS:
Literature reporting outcomes from phase III clinical trials that evaluated first-line IO combination therapies was identified through a search of the PubMed electronic database following PRISMA guidelines. Abstracts were screened to identify manuscripts that fit the search criteria, and then, a descriptive review was performed.
RESULTS:
Our literature search identified 2,229 abstracts that met the initial search criteria, and then, it was narrowed to 431 abstracts using filters for “clinical trial” and a “ten year” time window. After review of the abstracts, six manuscripts were selected for data extraction and subsequent review.
CONCLUSION:
When compared to sunitinib, four IO combinations improved overall survival as first-line treatment, and five improved progression free survival for patients with mRCC. These IO combination therapies have unique characteristics, so clinicians should take into account patient and cancer factors to individualize treatment recommendations.
INTRODUCTION
First-line treatment of metastatic clear cell renal cell carcinoma (mRCC) has drastically changed over the past two decades, yet the conceptual framework behind novel therapeutics has remained remarkably consistent, with a focus on targeting angiogenesis and modulating the tumor microenvironment. From the 1990s until 2005, treatment of mRCC was limited to non-specific immune modulators, interferon-alpha (IFN-α) and high-dose interleukin 2 (HD IL-2), that produced meaningful responses in a minority of patients and had severe toxicities [1, 2]. During the “cytokine era”, Motzer and colleagues identified five clinical factors, low Karnofsky performance status (KPS), elevated lactate dehydrogenase (LDH), anemia, hypercalcemia, and absence of prior nephrectomy, associated with shorter survival in patients with mRCC, termed the Memorial Sloan-Kettering Cancer Center (MSKCC) risk score [3]. From 2005 until 2012, three therapies targeting angiogenesis: sunitinib, pazopanib, and bevacizumab, and one inhibitor of mammalian target of rapamycin (mTOR), temsirolimus, were added as first-line therapies for mRCC [4–9]. Most patients during this era were treated initially with a small molecule tyrosine kinase inhibitor (TKI), such as sunitinib or pazopanib, to avoid the side effects with the bevacizumab plus IFN-α. During this era of targeted therapies, Heng and colleagues developed a new prognostic model for patients with mRCC, the International mRCC Database Consortium (IMDC) risk score, which modified the MSKCC risk score by removing elevated LDH and adding thrombocytosis and neutrophilia [10, 11]. In 2018, we entered the era of first-line immuno-oncology (IO) combination therapies for patients with mRCC, and the MSKCC and/or IMDC risk scores now play a greater role in optimizing treatment selection and sequencing for individual patients.
For patients with mRCC, IO combinations currently refer to any regimen that contains a programmed cell death protein 1 (PD-1), programmed cell death-ligand 1 (PD-L1), or cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) checkpoint inhibitor. CTLA-4 is an inhibitory checkpoint expressed by T cells, and when activated, CTLA-4 out competes CD28, the second signal required for T cell activation [12]. Ipilimumab is an inhibitor of CTLA-4 that prolongs the antitumor response by T cells [13]. PD-1 is another inhibitory checkpoint expressed on T cells that diminishes T-cell activation, when engaged by PD-L1 or PD-L2, by inhibiting IL-2 production and T-cell proliferation [14]. When the interaction between PD-1 and PD-L1/PD-L2 is inhibited by drugs such as nivolumab, pembrolizumab, or avelumab, the exhausted phenotype of CD8 T cells may be reverted and anti-tumor responses may occur [15]. After the initial success of nivolumab in mRCC, investigators sought to identify therapies that can augment IO agents by reverting the immunosuppressive tumor microenvironment [16]. Angiogenesis-targeted therapies, particularly multi-target tyrosine kinase inhibitors (TKIs), are speculated to favorably modify the tumor microenvironment by increasing immune cell infiltration, inhibiting pro-inflammatory cytokines, myeloid-derived suppressor cells, and favorably shifting the phenotype of macrophages [17]. Thus, combinations of IO agents and angiogenesis-targeted therapies were evaluated in multiple phase III clinical trials.
Herein, we perform a systematic review to identify phase III clinical trials of first-line IO combinations for patients with mRCC and describe the key characteristics and findings from each trial identified. Then, we provide a case-based discussion to highlight how patient characteristics help individualize selection of a first-line IO combination for patients with mRCC.
METHODS
Search strategy and eligibility criteria
We performed a systematic review of the PubMed database on April 29, 2021, following the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines [18]. The search terms used were the following: (renal cell carcinoma OR renal cell cancer OR kidney carcinoma OR kidney cancer) AND (metastatic OR advanced) AND (randomized). Studies were included if they evaluated first-line treatment with an IO combination verse sunitinib in a phase III randomized clinical trial for patients with mRCC. IO combinations were defined as any therapeutic combination that included a PD-1/PD-L1, such as nivolumab, pembrolizumab, atezolizumab, or avelumab, or CTLA-4 checkpoint inhibitor, such as ipilimumab. We excluded observational studies, reviews, editorials, case reports, and articles not published in the English language. If multiple publications existed for a clinical trial, we used the most recent publication that included the outcomes of interest.
Outcome measures
Efficacy measures of interest were progression-free survival (PFS), overall survival (OS), and objective response rate (ORR). Efficacy measures were reported for the intention-to-treat (ITT) population, irrespective of the primary endpoint population. Toxicity measures of interest were ≥grade 3 treatment-related adverse events, treatment discontinuation rate, dose reduction rate, and the use of high-dose corticosteroids. OS and PFS were reported as hazard ratios (HR) with 95% confidence intervals (95% CI) for more objective comparisons.
Data collection
Initially, AWH screened the title and abstract of identified works for eligibility, and eligible articles were reviewed in detail to confirm they fit the eligibility criteria. For each clinical trial identified, we extracted design, patient characteristics, OS, PFS, ORR, toxicity data described above, and information on subsequent lines of therapy.
Data synthesis
Collected data are summarized in the results section.
RESULTS
The initial search criteria identified 2,229 records in the PubMed database (Fig. 1). After applying filters for clinical trials and publication within the past 10 years, 431 records were identified. The titles and abstracts of these 431 records were reviewed, and 426 records were excluded because they did not fit the exclusion criteria. Six studies were included in the systematic review, and the design and characteristics of these studies are described in Table 1. [19–24].
Fig. 1
Preferred reporting items for systematic reviews and meta-analysis (PRISMA) flow diagram.
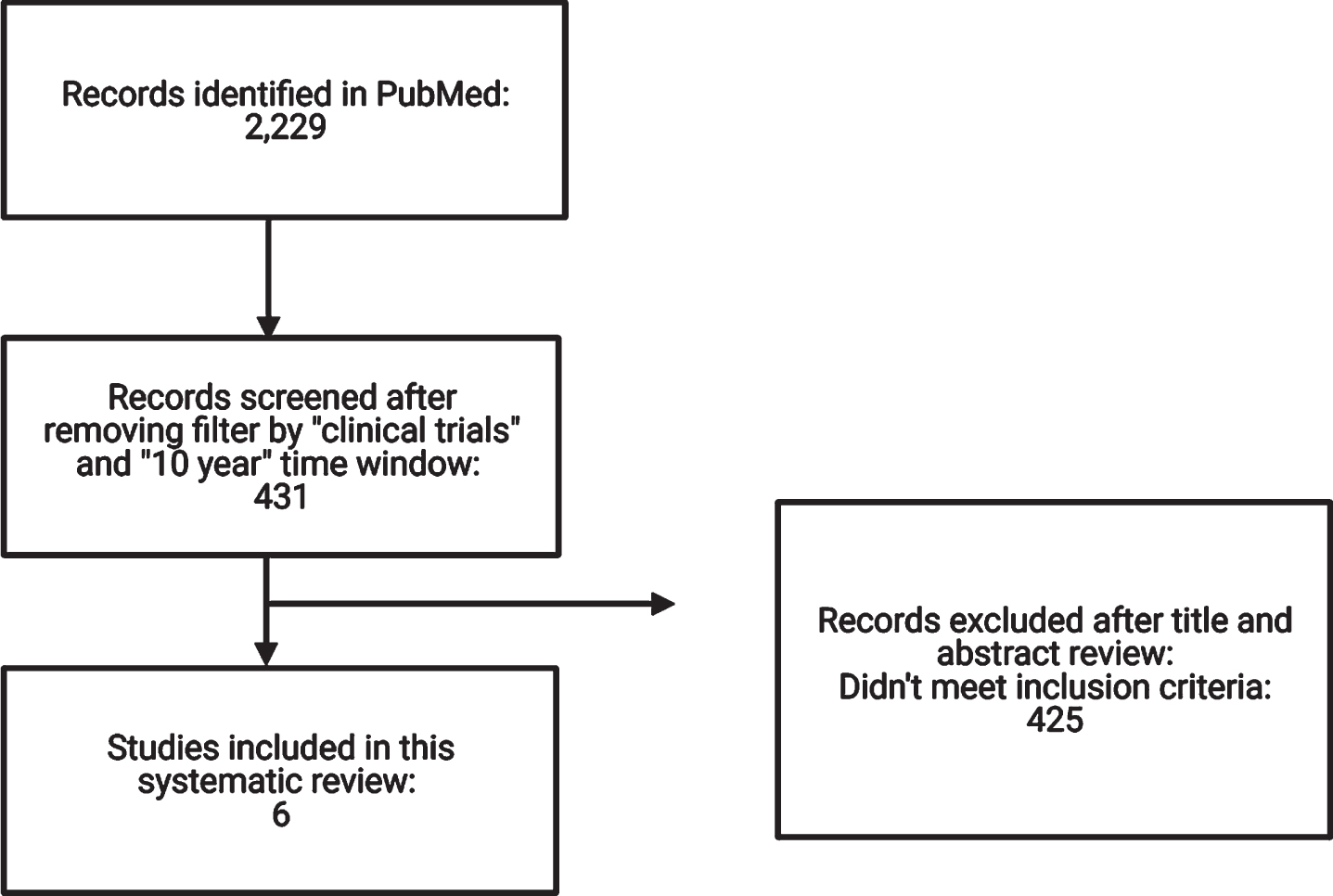
Table 1
Design and characteristics of identified studies
| CM 214 | KN-426 | IM151 | JAVELIN Renal 101 | CM 9ER | CLEAR | ||||||||
| Therapies | Nivo/ipi | Sun | Pembro/axi | Sun | Atezo/bev | Sun | Avelumab/axi | Sun | Nivo/cabo | Sun | Len/pembro | Len/Eve | Sun |
| n = 550 | n = 546 | n = 432 | n = 429 | n = 454 | n = 461 | n = 442 | n = 444 | n = 323 | n = 328 | n = 355 | n = 357 | n = 357 | |
| 1° endpoint | OS, PFS Int./Poor | OS, PFS ITT | PFS PD-L1 (+), OS ITT | OS, PFS PD-L1 (+) | PFS ITT | PFS ITT | |||||||
| Median follow-up (m) | 55 | 30.6 | 16 | 19.3 | 18.1 | 26.6 | |||||||
| Risk groups | |||||||||||||
| Fav. | 23% | 23% | 32% | 31% | 20% | 20% | 21% | 22% | 23% | 22% | 27% | 28% | 27% |
| Int. | 61% | 61% | 55% | 57% | 69% | 69% | 61% | 62% | 58% | 57% | 64% | 64% | 64% |
| Poor | 17% | 16% | 13% | 12% | 12% | 12% | 16% | 16% | 19% | 21% | 9% | 9% | 9% |
| Geography | |||||||||||||
| US | 28% | 28% | 24.1% | 24.0% | 21% | 18% | 29.0% | 29.3% | 48.9% | 49.1% | 55.8% | 56.0% | 55.7% |
| Canada/Europe* | 37% | 36% | 24.5% | 24.2% | 43% | 48% | 29.0% | 28.8% | N/A | N/A | N/A | N/A | N/A |
| Rest world | 35% | 36% | 51.4% | 51.7% | 26% | 34% | 42.1% | 41.9% | 51.1% | 50.9% | 44.3% | 44.0% | 44.3% |
| Metastatic sites | |||||||||||||
| Lung | 69% | 68% | 72.2% | 72.0% | 75% | 71% | N/A | N/A | 73.7% | 75.9% | 70.1% | 68.6% | 66.9% |
| Lymph nodes | 45% | 49% | 46.1% | 45.9% | 47% | 47% | 40.2% | 39.9% | 47.9% | 45.7% | 44.5% | ||
| Bones | 20% | 22% | 23.8% | 24.0% | 20% | 20% | 24.1% | 22.0% | 23.9% | 24.1% | 27.2% | ||
| Liver | 18% | 20% | 15.3% | 16.6% | 17% | 18% | 22.6% | 16.2% | 16.9% | 17.4% | 17.1% | ||
| Subsequent tx | |||||||||||||
| Yes | 53.5% | 66.5% | 54% | 69% | 43% | 52% | 31.2% | 51.% | 25.4% | 39.9% | 54.9% | 68.2% | 71.0% |
CM = CheckMate, KN = KEYNOTE, IM151 = IMmotion151, nivo = nivolumab, ipi = ipilimumab, sun = sunitinib, pembro = pembrolizumab, axi = axitinib, atezo = atezolizumab, bev = bevacizumab, cabo = cabozantinib, len = lenvatinib, eve = everolimus, n = total number of patients, m = months, fav.=favorable, int.=intermediate, tx = treatment, OS = overall survival, PFS = progression-free survival, ITT = intention to treat, PD-L1 = programmed death-ligand 1. *: CM 214 was Canada/Europe; KN-426 was North America, Western Europe, Rest; IM151 was North America, Western Europe and Australia, rest; JAVELIN Renal 101 was US, Canada + Western Europe, and Rest; CM 9ER defines as US/Europe vs Rest; CLEAR defines as US/Western Europe vs Rest.
CheckMate 214
CheckMate 214 was the first phase III clinical trial of an IO combination reported and demonstrated the promise of IO combinations for patients with treatment-naïve mRCC. CheckMate 214 was an international, open-label, phase III clinical trial that randomized 1096 patients to nivolumab 3 milligrams/kilogram (mg/kg) plus ipilimumab 1 mg/kg every 3 weeks for 4 cycles followed by maintenance nivolumab at 480 mg every 4 weeks or sunitinib 50 mg daily for 4 weeks of a 6 week cycle [25]. The co-primary endpoints were OS, PFS, and ORR in patients with IMDC intermediate or poor-risk disease, yet all IMDC risk groups were eligible. This primary population is unique from the other first-line IO combination trials reported in this systematic review, so we will focus on the ITT population to facilitate discussion. Detailed information regarding IMDC risk group, geographic regions, sites of metastases, and subsequent therapies are provided in Table 1.
At a median follow-up of 55 months, nivolumab plus ipilimumab significantly improved median OS compared to sunitinib in the ITT population [not reached (NR) vs. 38.4 months (m), HR 0.69, 95% CI 0.59–0.81, Table 2] [19]. Median PFS was similar between nivolumab plus ipilimumab and sunitinib (12.2 vs. 12.3 m, HR 0.89, 95% CI 0.76–1.05). By independent radiology review, ORR numerically favored nivolumab plus ipilimumab (39.1% vs. 32.4%), and 10.7% of patients achieved a complete response (CR) with nivolumab plus ipilimumab. In regards to safety and tolerability, nivolumab plus ipilimumab produced grade 3 or higher treatment-related adverse events (TRAE) in 48% of patients, while sunitinib produced grade 3 or higher TRAE in 64% (Table 3). However, dual checkpoint inhibition produced unique immune-mediated adverse events, and 29.1% of patients required high-dose corticosteroids to manage these adverse events. According to patient-reported outcomes (PRO), nivolumab plus ipilimumab improved health-related quality of life (HRQOL) compared to sunitinib across multiple PRO questionnaires [26].
Table 2
Summary of efficacy outcomes for first-line immuno-oncology combinations
| CM 21419 | KN-42620 | IM15121 | JAVELIN Renal 10122 | CM 9ER23 | CLEAR24 | ||||||||
| Therapies | Nivo/ipi | Sun | Pembro/axi | Sun | Atezo/bev | Sun | Avelumab/axi | Sun | Nivo/cabo | Sun | Len/pembro | Len/Eve | Sun |
| Median OS (m) | NR | 38.4 | NR | 35.7 | 33.6 | 34.9 | NR | NR | NR | NR | NR | NR | NR |
| OS HR | 0.69 | 0.68 | 0.93 | 0.80 | 0.60 | 0.66 | 1.15 | ||||||
| (95% CI) | 0.59–0.81 | 0.55–0.85 | 0.76–1.14 | 0.62–1.03 | 0.40–0.89 | 0.49–0.88 | 0.88–1.50 | ||||||
| Median PFS (m) | 12.2 | 12.3 | 15.4 | 11.1 | 11.2 | 8.4 | 13.3 | 8.0 | 16.6 | 8.3 | 23.9 | 14.7 | 9.2 |
| PFS HR | 0.89 | 0.71 | 0.83 | 0.69 | 0.51 | 0.39 | 0.65 | ||||||
| (95% CI) | 0.76–1.05 | 0.60–0.84 | 0.70–0.97 | 0.58–0.83 | 0.41–0.64 | 0.32–0.49 | 0.53–0.80 | ||||||
| ORR | 39.1% | 32.4% | 60% | 40% | 37% | 33% | 52.5% | 27.3% | 55.7% | 27.1% | 71.0% | 53.5% | 36.1% |
| CR | 10.7% | 2.6% | 9% | 3% | 5% | 2% | 3.8% | 2.0% | 8.0% | 4.6% | 16.1% | 9.8% | 4.2% |
| PR | 28.4% | 29.9% | 51% | 37% | 31% | 31% | 48.6% | 25.2% | 47.7% | 22.6% | 54.9% | 43.7% | 31.9% |
| PD | 17.6% | 14.1% | 11% | 17% | 18% | 19% | 12.4% | 19.4% | 5.6% | 13.7% | 5.4% | 7.3% | 14.0% |
| DOR (m) | NR | 23.7 | 23.5 | 15.9 | 16.6 | 14.2 | 18.5 | NR | 20.2 | 11.5 | 25.8 | 16.6 | 14.6 |
CM = CheckMate, KN = KEYNOTE, IM151 = IMmotion151, nivo = nivolumab, ipi = ipilimumab, sun = sunitinib, pembro = pembrolizumab, axi = axitinib, atezo = atezolizumab, bev = bevacizumab, cabo = cabozantinib, len = lenvatinib, eve = everolimus, OS = overall survival, PFS = progression-free survival, m = months, NR = not reached, HR = hazard ratio, CI = confidence interval, ORR = objective response rate, CR = complete response, PR = partial response, PD = progressive disease, DOR = duration of response.
Table 3
Summary of adverse events for first-line immuno-oncology combinations
| CM 214 | KN-426 | IM151 | JAVELIN Renal 101 | CM 9ER | CLEAR | ||||||||
| Therapies | Nivo/ipi | Sun | Pembro/ | Sun | Atezo/bev | Sun | Avelumab/axi | Sun | Nivo/cabo | Sun | Len/pembro | Len/Eve | Sun |
| ≥G3 TRAE (%) | 48% | 64% | 67% | 62% | 40% | 54% | 57% | 56% | 61% | 51% | 72% | 73% | 59% |
| % discontinue tx, 1st/2nd drug/both | 22.7% | 13.1% | 21/20/7% | 12% | 2/5/5% | 8% | NA/NA/8% | 13% | 6.6/7.5/5.6% | 16.9% | 22/25/19% | 22/25/19% | 14% |
| % dose reduction | N/A | N/A | N/A | N/A | N/A | N/A | 42.2% | 42.6% | 56.3% | 51.6% | 69% | 73% | 50% |
| % high-dose CS | 29.1% | N/A | N/A | N/A | 16% | N/A | 11.1% | N/A | 19.1% | N/A | N/A | N/A | N/A |
CM = CheckMate, KN = KEYNOTE, IM151 = IMmotion151, nivo = nivolumab, ipi = ipilimumab, sun = sunitinib, pembro = pembrolizumab, axi = axitinib, atezo = atezolizumab, bev = bevacizumab, cabo = cabozantinib, len = lenvatinib, eve = everolimus, G3 = grade 3, TRAE =treatment-related adverse events, % = percent, tx = treatment, CS = corticosteroids, N/A = not available.
KEYNOTE-426
Pembrolizumab plus axitinib was the first combination of a PD-1 checkpoint inhibitor and an angiogenesis-targeted therapy approved by the United States (US) Food and Drug Administration (FDA) as first-line treatment of mRCC. KEYNOTE-426 was an international, open-label, phase III clinical trial that randomized 861 patients to pembrolizumab 200 mg every 3 weeks plus axitinib 5 mg twice daily or sunitinib 50 mg daily for the first 4 weeks of each 6-week cycle [27]. The co-primary endpoints were OS and PFS in the ITT population. In the pembrolizumab plus axitinib arm, 32% of patients had IMDC favorable-risk, 55% had intermediate-risk, and 13% had poor-risk disease at trial enrollment. Table 1 provides more detailed information regarding sites of metastases, the geographic region patients were enrolled from, and subsequent lines of therapy.
At a median follow-up of 30.6 months, pembrolizumab plus axitinib met its primary endpoints by significantly improving OS (NR vs. 35.7 m, HR 0.68, 95% CI 0.55–0.85) and PFS (15.4 vs. 11.1 m, HR 0.71, 95% CI 0.60–0.84, Table 2) compared to sunitinib [20]. By independent radiology review, pembrolizumab plus axitinib produced an ORR of 60% with 9% of patients achieving a CR and 11% experiencing progressive disease (PD) as their best response to treatment. Pembrolizumab plus axitinib produced more grade 3 or higher TRAE than nivolumab plus ipilimumab (67% vs. 48%, Table 3), yet the frequency was similar to the sunitinib arm (62%). The investigators did not report the frequency of high-dose corticosteroid use to manage immune-mediated adverse events. Twenty percent of patients discontinued either pembrolizumab or axitinib due to adverse events, and 7% discontinued the combination due to adverse events. The influence of pembrolizumab plus axitinib on HRQOL has not been published.
IMmotion151
The combination of atezolizumab, a PD-L1 checkpoint inhibitor, and bevacizumab, a monoclonal antibody against VEGF, was studied in the IMmotion151 trial [21]. This trial was an international, open-label, phase III clinical trial that randomized 915 treatment-naïve patients to atezolizumab 1200 mg plus bevacizumab 15 mg/kg every 3 weeks or sunitinib 50 mg daily for the first 4 weeks of a 6-week cycle. The co-primary endpoints were PFS in the PD-L1 positive population, defined as ≥1% on tumor-infiltrating immune cells, and OS in the ITT population. For consistency, the outcomes we report from this trial will all focus on the ITT population, and detailed information on the PD-L1 positive population are in the original manuscript. In the atezolizumab plus bevacizumab arm, 20% of patients had MSKCC favorable-risk, 69% had intermediate-risk, and 12% had poor-risk disease at trial enrollment. Table 1 provides more detailed information regarding sites of metastases, the geographic region patients were enrolled from, and subsequent lines of therapy.
At a median follow-up of 16 months, atezolizumab plus bevacizumab significantly improved PFS in the ITT population (11.2 vs. 8.4 m, HR 0.83, 95% CI 0.70–0.97), but OS was similar between the combination and sunitinib (33.6 vs. 34.9 m, HR 0.93, 95% CI 0.76–1.14, Table 2). Additionally, the ORR was similar between atezolizumab plus bevacizumab and sunitinib (37% vs. 33%), and the combination produced a CR in 5% of patients and PD as best response in 18% of patients. Based on these findings, Roche did not seek US FDA approval for atezolizumab plus bevacizumab in patients with treatment-naïve mRCC. Atezolizumab plus bevacizumab was well tolerated with less grade 3 TRAE than sunitinib (40% vs. 54%, Table 3), a low treatment discontinuation rate, and low corticosteroid use for immune-mediated adverse events (16%). Atezolizumab plus bevacizumab improved many PRO compared to sunitinib, and time to deterioration for symptoms related to RCC was significantly prolonged (HR 0.45, 95% CI 0.37–0.55) [28].
JAVELIN renal 101
The FDA approved avelumab, a PD-L1 checkpoint inhibitor, plus axitinib for treatment-naïve mRCC based on the JAVELIN Renal 101 trial. This trial was an international, open-label, phase III clinical trial that randomized 886 patients with treatment-naïve mRCC to avelumab 10 mg/kg every 2 weeks plus axitinib 5 mg twice daily or sunitinib 50 mg daily for 4 weeks of every 6-week cycle [29]. The co-primary endpoints were OS and PFS in the PD-L1 positive population, defined as ≥1% of immune cells within the tumor area of the specimen. For this systematic review, we report outcomes for the ITT population. In the avelumab plus axitinib arm, 21% of patients had IMDC favorable-risk, 61% had IMDC intermediate-risk, and 16% had IMDC poor-risk disease. Table 1 provides more detailed information regarding the geographic region patients were enrolled from and subsequent lines of therapy received.
At a median follow-up of 19.3 months, avelumab plus axitinib significantly improved median PFS versus sunitinib in the ITT population (13.3 vs. 8.0 m, HR 0.69, 95% 0.58–0.83, Table 2) [22]. At this time, median OS remains immature with a trend favoring avelumab plus axitinib, yet it is inconclusive and does not reject the null hypothesis (NR vs. NR, HR 0.80, 95% CI 0.62–1.03). Avelumab plus axitinib produced a higher ORR than sunitinib (52.5% vs. 27.3%), but the CR rate was lower than other IO combination therapies at 3.8%. The rate of grade 3 or higher TRAE was similar between avelumab plus axitinib and sunitinib (57% vs. 56%, Table 3). Eight percent of patients discontinued the combination of avelumab plus axitinib due to adverse events, and only 11% of patients required high-dose corticosteroids to treat immune-mediated adverse events. Patient-reported outcomes for JAVELIN Renal 101 are not published.
CheckMate 9ER
CheckMate 9ER ushered a new era of IO combination therapies for mRCC where multi-target TKIs that inhibit a broader spectrum of receptor tyrosine kinases, such as cabozantinib, are combined with PD-1 checkpoint inhibition. This trial was an international, open-label, phase III clinical trial that randomized 651 patients with treatment-naïve mRCC to nivolumab 240 mg every 2 weeks plus cabozantinib 40 mg daily or sunitinib 50 mg daily for 4 weeks of every 6-week cycle [23]. The primary endpoint was PFS in the ITT population. In the nivolumab plus cabozantinib arm, 23% of patients had IMDC favorable-risk, 58% had intermediate-risk, and 19% had poor-risk disease at trial enrollment. In patients who discontinued study drug, 11.1% of patients in the nivolumab plus cabozantinib arm and 27.7% in the sunitinib arm received a subsequent systemic therapy. Table 1 provides more detailed information regarding the geographic region patients were enrolled and the sites of metastatic disease.
Nivolumab plus cabozantinib significantly improved median OS (NR vs. NR, HR 0.60, 95% CI 0.40–0.89) and PFS (13.3 vs. 8.0 m, HR 0.69, 95% CI 0.58–0.83, Table 2) compared to sunitinib. Additionally, nivolumab plus cabozantinib produced an ORR of 52.5% with 8% of patients experiencing a CR and only 5.6% experiencing PD as their best response to therapy. Based on these findings, nivolumab plus cabozantinib was approved by US FDA as first-line treatment for mRCC. Nivolumab plus cabozantinib produced a grade 3 or higher TRAE in 61% of patients compared to 51% in patients who received sunitinib (Table 3). Seven percent of patients discontinued either nivolumab or cabozantinib due to adverse events, and 19% of patients required high-dose corticosteroids to manage immune-mediated adverse events. Patients who received nivolumab plus cabozantinib had significantly better HRQOL than patients who received sunitinib.
CLEAR
The CLEAR trial evaluated the combination of lenvatinib, a multitarget TKI, plus pembrolizumab in patients with treatment-naïve mRCC. This trial was an international, open-label, phase III clinical trial that randomized 1069 patients to lenvatinib 20 mg daily plus pembrolizumab 200 mg every 3 weeks, lenvatinib 18 mg plus everolimus 5 mg daily, or sunitinib daily for 4 weeks of every 6-week cycle [24]. The primary endpoint was PFS in the ITT population. In the lenvatinib plus pembrolizumab arm, 27% of patients had IMDC favorable-risk, 64% had intermediate-risk, and only 9% had poor-risk disease. Table 1 provides more detailed information regarding sites of metastases, the geographic region patients were enrolled from, and subsequent lines of therapy.
Compared to sunitinib, lenvatinib plus pembrolizumab convincingly improved OS (NR vs. NR, HR 0.66, 95% CI 0.49–0.88) and PFS (23.9 vs. 9.2 m, HR 0.39, 95% CI 0.32–0.49, Table 2). Lenvatinib plus pembrolizumab also produced a remarkably high ORR at 71% with 16% of patients achieving a CR and only 5.6% of patients having PD as their best response to treatment, overall survival remains immature at this time. Similarly, the combination of lenvatinib plus everolimus significantly improved PFS compared to sunitinib (14.7 vs. 9.2, HR 0.65, 95% CI 0.53–0.80), but OS was immature at this analysis (NR vs. NR, HR 1.15, 95% CI 0.88–1.50, Table 2). Among IO combination therapies in this systematic review, lenvatinib plus pembrolizumab produced the highest incidence of grade 3 or higher TRAE at 69% (Table 3). A meaningful fraction of patients had to discontinue either lenvatinib (22%), pembrolizumab (25%), or both (19%) due to adverse events. The frequency of high-dose corticosteroids utilization was not reported, nor were patient-reported outcomes. The United States FDA has not approved lenvatinib plus pembrolizumab for patients with treatment-naïve mRCC, but it is anticipated to receive approval in the near future.
DISCUSSION
First-line IO combination therapies consistently improve overall survival by a relative risk reduction of 30–40% for patients with mRCC, and now, we have a relative abundance of combination therapies to select for patients in our clinics. The clinical trials evaluating first-line IO combination therapies were reported across a relatively short period, so direct head-to-head comparisons are not available to create a “one-size-fits-all” recommendation for first-line treatment of mRCC. Significant differences between studies emerge when considering the proportion of patients enrolled in various geographic regions, proportions of patients with IMDC favorable, intermediate, and poor risk prognostic groupings, and the percentage of patients with unfavorable sites of metastasis including bone and liver. Fortunately, the comparator arm, sunitinib, was constant across the phase III trials discussed, and the patient populations were broadly similar across studies (Table 1) with consistent treatment effects observed across most patient subgroups. Despite the serious caveats of cross-trial comparisons, these facts make it inevitable that clinicians will compare findings across trials in order to optimize treatment selection for individual patients. In this discussion, we will utilize clinical scenarios to highlight decision points that we believe are important in selecting a first-line treatment for patients with mRCC. Included are consideration of insurance status in the United States as this remains a crucial factor in therapy selection.
The favorable risk conundrum
Scenario 1: 48-year-old male with no co-morbidities was diagnosed with pT3aN0 clear cell RCC at the age of 46 and underwent radical nephrectomy. Two years later, he has developed a contralateral adrenal metastasis and 2 pulmonary metastases, which are biopsy proven. He is married with three children, has commercial insurance through his employer, and wishes to be as aggressive as possible in treating his cancer.
Scenario 2: A 72-year-old male with morbid obesity, metabolic syndrome, and history of coronary artery disease with coronary stents was diagnosed with a pT2NX clear cell renal cell carcinoma at the age of 66. At this time, he has a 1.5 centimeter (cm) recurrence in the head of his pancreas, biopsy proven to be RCC with no other sites of disease. The patient is a widow and lives alone in a small rural town three hours away from a city with a tertiary care hospital. He has one son who lives across the country. He has traditional Medicare A/B with no supplementary insurance.
Scenario 3: A 78-year-old female with no medical co-morbidities was diagnosed with pT3aNX clear cell renal cell carcinoma 14 months ago and has been found now to have three pulmonary metastasis and a liver metastasis, biopsy proven. She is married, has four children, 10 grandchildren, and is a retired teacher. She has traditional Medicare A/B with a supplementary drug coverage plan. She is interested in pursuing therapy, but wishes to maximize quality over quantity of life after caring for her father during his battle with leukemia.
Patients with favorable risk disease have incredible heterogeneity in both presentation and therapeutic approaches. From the MSKCC to the IMDC eras, the median survival of patients with favorable risk extended from 33 to 44 months. From the subgroups of patients with favorable risk on the combination studies, it is clear that median OS is continuing to increase for this patient population. Active surveillance, local therapies including metastasectomy, stereotactic radiosurgery or ablative techniques, single agent treatment with sunitinib or pazopanib, and combination strategies must be measured in terms of risk and benefit with the patient and caregivers. In scenario 1, the patient is young, fit, and wishes to be aggressive. His commercial insurance allows for any approach with less concern for financial toxicity related to substantial co-payments for oral targeted therapy that remain problematic for the Medicare population. In this setting, we favor nivolumab plus ipilimumab. Our rationale includes the small, but real potential that the patient may be able to achieve a deep remission and not require additional therapies. Classically, these patients were ideal candidates for HD IL-2. In scenario 2, the patient’s co-morbidities give pause for an aggressive surgical approach for his oligometastatic recurrence given the substantial morbidity and mortality risk associated with a Whipple operation. His Medicare A/B only status, limited support network, and distance from tertiary care centers must be considered. In this scenario, we would elect active surveillance to monitor the pace of his cancer. Given his co-morbidities, TKI therapy has the potential for major harm, and severe immunotherapy toxicity could be devastating. In scenario 3, we highlight a patient with favorable risk disease, but with a more aggressive presentation given the liver metastasis, and would favor a systemic treatment approach. Given her desire to prioritize quality of life, we would discuss the following options: TKI therapy with dose titration to maximize HRQOL, nivolumab plus cabozantinib given the observed HRQOL and safety profile in CheckMate 9-ER, and nivolumab plus ipilimumab with discussion about risk for serious immune-mediated adverse events. After the discussion, her preference would guide treatment selection.
Intermediate risk disease
Scenario 1: A 72 year-old male with a history of ulcerative colitis (UC) on long-standing mesalamine, without recent flares, is diagnosed with a large left renal primary tumor and multiple lung metastasis, biopsy proven to be clear cell RCC. He is otherwise healthy, retired, married, and has no children. He has Medicare A/B with supplementary insurance. He is interested in being aggressive with treatment and is willing to consider surgical options. His gastroenterologist is a UC expert and willing to help manage any flares of UC.
Scenario 2: A 62 year-old female with no co-morbidities was diagnosed with clear cell RCC four years ago and has been diagnosed with an oligometastatic recurrence in her left lung, biopsy proven. She has mild anemia. She is a physician, married, is commercially insured, and hopes to continue her medical practice for as long as possible.
Scenario 3: A 68 year-old male who has poorly controlled hypertension on three anti-hypertensives and atrial fibrillation with a history of stroke is diagnosed with a left-sided renal tumor with lung and mediastinal lymph node metastases. He is married, lives in a major city, and has four children that are heavily involved in his care. He wishes to start therapy for his mRCC. He has Medicare A/B with a supplement.
In scenario 1, the patient would have been excluded from the clinical trials discussed in this review. However, data has emerged that immune checkpoint inhibitors can be provided to patients with well controlled autoimmune conditions without substantially increasing the risk of autoimmune events, as compared to the general population [30, 31]. However, we would be hesitant recommending nivolumab plus ipilimumab given the relatively high rates of immune mediated diarrhea and colitis associated with this regimen. This scenario favors consideration of avelumab plus axitinib given its low rate of serious adverse events requiring high-dose corticosteroids (Table 3). If the patient tolerated therapy and had evidence of disease response or stability, we would consider a delayed cytoreductive nephrectomy for this patient. In scenario 2, the patient qualifies as intermediate risk based on her mild anemia, but her disease characteristics are more consistent with the favorable risk population. We would consider metastasectomy because it provides a small chance of cure (10–15%) and could delay the need to begin systemic treatment [32]. In scenario 3, this patient has co-morbidities that directly compete with RCC in terms of mortality risk. If possible, we favor avoiding TKI therapy and considering nivolumab plus ipilimumab or single agent immunotherapy, with either nivolumab or pembrolizumab, in an off-label approach.
Poor risk disease
Scenario 1: A 52 year-old male is admitted to the hospital with spinal cord compression, extensive liver metastasis, and a large right-sided primary tumor. He undergoes a decompressive spinal surgery and has clear cell RCC. He is employed and is insured through his company. He has limited co-morbidities, is married with children, and wishes to be aggressive with treatment.
Scenario 2: A 72 year-old female is diagnosed with a large right-sided renal primary tumor with adrenal and retroperitoneal lymphadenopathy. She undergoes initial nephrectomy, which finds evidence of clear cell RCC with sarcomatoid de-differentiation. On restaging two months after surgery, she has liver and lung metastases with anemia and neutrophilia. She is married, lives in a large urban environment, and has traditional Medicare A/B with an excellent supplement program.
In scenario 1, we favor starting nivolumab plus cabozantinib or pembrolizumab plus lenvatinib as soon as possible. Cabozantinib has demonstrated substantial activity as a single agent in the front line and second line setting [33, 34]. To date, it remains the only single-agent TKI that has shown an improvement in OS in the second-line setting. We favor aggressive first-line IO combination therapy for this patient due to the acuity of presentation and concern that the patient will not be fit enough to receive second-line treatment at the time of disease progression. In scenario 2, we favor nivolumab plus ipilimumab given the high potential for durable complete response in patients with sarcomatoid de-differentiation [35].
Impact on first line treatment decision on subsequent therapy
During the targeted therapy era, the median number of treatment lines for patients with mRCC was two and was consistent across the IMDC dataset and high-volume French and American academic centers [36–38]. It is unknown whether contemporary patients are more likely to receive additional therapeutic lines given the activity of cabozantinib and lenvatinib plus everolimus after progression on TKI [34, 39]. Lenvatinib plus everolimus is active as an earlier line of treatment; however, lenvatinib plus everolimus appears to have less activity after progression on cabozantinib [40]. The mechanisms of resistance after progression on cabozantinib or lenvatinib are unknown at this time, and it is unlikely that earlier generations of TKI therapy (pazopanib, sunitinib, axitinib, etc.) for mRCC will produce meaningful clinical benefit in this setting.
Initial treatment with IO agents does not diminish TKI activity. In a pooled analysis of patients treated with front line IO at MDACC and MSKCC, single-agent TKI therapy retained activity with a median PFS of over 11 months [41]. In contrast, ipilimumab has limited activity as later-line therapy with multiple studies showing an objective response rate less than 15% with no complete responses [42, 43]. In theory, patients who receive initial treatment with nivolumab plus ipilimumab have up to four potential active, sequential lines of therapy: nivolumab plus ipilimumab, axitinib, cabozantinib, and lenvatinib plus everolimus. Patients who receive pembrolizumab plus axitinib have three potential active lines of treatment: pembrolizumab plus axitinib, cabozantinib, lenvatinib plus everolimus. Furthermore, patients who receive first-line lenvatinib plus pembrolizumab likely only have subsequent cabozantinib, and those who receive nivolumab plus cabozantinib likely only have subsequent lenvatinib plus everolimus. Clearly, therapy is undergoing an impressive evolution and the high rates of disease control and the long progression free survivals witnessed with nivolumab plus cabozantinib and lenvatinib plus pembrolizumab, as compared to sunitinib, still make these appealing choices for initial treatment of mRCC.
Emerging data from prospective studies and real world data have begun to explore the role of IO combination therapy in the subsequent treatment setting. In a phase II clinical trial, lenvatinib plus pembrolizumab produced a median PFS of 11.7 months as second- or third-line treatment after progression on a PD-1 or PD-L1 agent [44]. Our group has also found that sitravatinib plus nivolumab has significant activity after progression on TKI, and the combination is now being studied after progression on PD-1 or PD-L1 therapies [45]. In our real world experience, we found that patients treated with off-label TKI + IO resulted in high rates of disease control and a PFS of 11.5 months [46]. With these findings, crucial ongoing studies, such as CONTACT-03 (NCT04338269), a randomized study of cabozantinib versus cabozantinib plus atezolizumab in patients who have previously received PD-1 or PDL-1 treatment, are needed to establish the role of continued immunotherapy after initial immunotherapy failure.
CONCLUSION
In conclusion, five IO combinations have received United States Food and Drug Administration approval for the front-line treatment of mRCC. Each of these IO combination therapies have unique therapeutic profiles and contain both inherent risks and benefits that can be used to differentiate between regimens. It remains paramount that clinicians should consider the patient holistically in his or her office and individualize first-line treatment recommendations for patients with mRCC, as no one-size-fits-all approach exists.
ACKNOWLEDGMENTS
We would like to acknowledge the patients, caregivers, research teams, investigators, and companies that have contributed to the improvement of therapy for patients with kidney cancer.
FUNDING
The authors report no funding.
AUTHOR CONTRIBUTIONS
All authors made substantial contributions to the work. AWH and MTC were involved with project inception, design, and development of the literature search. AWH performed the main literature search. AWH and MTC performed the literature analysis, synthesis of results, and first draft of the manuscript. AWH, AYS, and MTC were all involved with writing this manuscript and approve the final version for publication.
ETHICAL CONSIDERATIONS
This study, as a literature review, is exempt from any requirements for Institutional Review Board approval. No human or animal research was involved in the elaboration of this manuscript.
CONFLICTS OF INTEREST
AWH- None.
AYS- Consulting/Advisory Role: Exelixis and Pfizer. Institutional Research Grants: Bristol-Myers Squibb, Eisai, and EMD Serono.
MTC- Consulting/Advisory Role: AstraZeneca, Astellas, Eisai, EMD Serono, Exelixis, Genentech, Pfizer, Seattle Genetics, Consulting: AXDev, Exelixis, and Pfizer. Institutional Research grants: ApricityHealth, Aravive, EMD Serono, Exelixis, Janssen, and Pfizer. Non-continuing medical education: Bristol Myers Squibb, Merck, Roche, and Pfizer.
REFERENCES
[1] | Jonasch E , Haluska FG . Interferon in oncological practice: review of interferon biology, clinical applications, and toxicities. The Oncologist. (2001) ;6: :34–55. |
[2] | McDermott DF , Regan MM , Clark JI , et al. Randomized phase III trial of high-dose interleukin-2 versus subcutaneous interleukin-2 and interferon in patients with metastatic renal cell carcinoma. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. (2005) ;23: :133–41. |
[3] | Motzer RJ , Mazumdar M , Bacik J , Berg W , Amsterdam A , Ferrara J . Survival and prognostic stratification of 670 patients with advanced renal cell carcinoma. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. (1999) ;17: :2530–40. |
[4] | Motzer RJ , Hutson TE , Tomczak P , et al. Sunitinib versus interferon alfa in metastatic renal-cell carcinoma. N Engl J Med. (2007) ;356: :115–24. |
[5] | Sternberg CN , Davis ID , Mardiak J , et al. Pazopanib in locally advanced or metastatic renal cell carcinoma: results of a randomized phase III trial. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. (2010) ;28: :1061–8. |
[6] | Rini BI , Escudier B , Tomczak P , et al. Comparative effectiveness of axitinib versus sorafenib in advanced renal cell carcinoma (AXIS): a randomised phase 3 trial. Lancet. (2011) ;378: :1931–9. |
[7] | Escudier B , Eisen T , Stadler WM , et al. Sorafenib in advanced clear-cell renal-cell carcinoma. N Engl J Med. (2007) ;356: :125–34. |
[8] | Escudier B , Pluzanska A , Koralewski P , et al. Bevacizumab plus interferon alfa-2a for treatment of metastatic renal cell carcinoma: a randomised, double-blind phase III trial. Lancet. (2007) ;370: :2103–11. |
[9] | Hudes G , Carducci M , Tomczak P , et al. Temsirolimus, interferon alfa, or both for advanced renal-cell carcinoma. N Engl J Med. (2007) ;356: :2271–81. |
[10] | Heng DY , Xie W , Regan MM , et al. Prognostic factors for overall survival in patients with metastatic renal cell carcinoma treated with vascular endothelial growth factor-targeted agents: results from a large, multicenter study. Journal of clinical oncology: official journal of the American Society of Clinical Oncology. (2009) ;27: :5794–9. |
[11] | Heng DY , Xie W , Regan MM , et al. External validation and comparison with other models of the International Metastatic Renal-Cell Carcinoma Database Consortium prognostic model: a population-based study. The Lancet Oncology. (2013) ;14: :141–8. |
[12] | Alegre ML , Noel PJ , Eisfelder BJ , et al. Regulation of surface and intracellular expression of CTLA4 on mouse T cells. Journal of immunology (Baltimore, Md: 1950). (1996) ;157: :4762–70. |
[13] | Leach DR , Krummel MF , Allison JP . Enhancement of antitumor immunity by CTLA-4 blockade. Science. (1996) ;271: :1734–6. |
[14] | Okazaki T , Honjo T . PD-1 and PD-1 ligands: from discovery to clinical application. International Immunology. (2007) ;19: :813–24. |
[15] | Sharma P , Siddiqui BA , Anandhan S , et al. The Next Decade of Immune Checkpoint Therapy. Cancer Discov. (2021) ;11: :838–57. |
[16] | Motzer RJ , Escudier B , McDermott DF , et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med. (2015) ;373: :1803–13. |
[17] | Msaouel P , Genovese G , Gao J , Sen S , Tannir NM . TAM kinase inhibition and immune checkpoint blockade- a winning combination in cancer treatment? Expert Opinion on Therapeutic Targets. (2021) ;25: :141–51. |
[18] | Page MJ , McKenzie JE , Bossuyt PM , et al. The PRISMA statement: An updated guideline for reporting systematic reviews. International Journal of Surgery (London, England). (2021) ;88: :105906. |
[19] | Albiges L , Tannir NM , Burotto M , et al. Nivolumab plus ipilimumab versus sunitinib for first-line treatment of advanced renal cell carcinoma: extended 4-year follow-up of the phase III CheckMate 214 trial. ESMO Open. (2020) ;5: :e001079. |
[20] | Powles T , Plimack ER , Soulières D , et al. Pembrolizumab plus axitinib versus sunitinib monotherapy as first-line treatment of advanced renal cell carcinoma (KEYNOTE-426): extended follow-up from a randomised, open-label, phase 3 trial. The Lancet Oncology. (2020) ;21: :1563–73. |
[21] | Rini BI , Powles T , Atkins MB , et al. Atezolizumab plus bevacizumab versus sunitinib in patients with previously untreated metastatic renal cell carcinoma (IMmotion151): a multicentre, open-label, phase 3, randomised controlled trial. Lancet. (2019) ;393: :2404–15. |
[22] | Choueiri TK , Motzer RJ , Rini BI , et al. Updated efficacy results from the JAVELIN Renal 101 trial: first-line avelumab plus axitinib versus sunitinib in patients with advanced renal cell carcinoma. Annals of oncology: official journal of the European Society for Medical Oncology. (2020) ;31: :1030–9. |
[23] | Choueiri TK , Powles T , Burotto M , et al. Nivolumab plus Cabozantinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2021) ;384: :829–41. |
[24] | Motzer R , Alekseev B , Rha SY , et al. Lenvatinib plus Pembrolizumab or Everolimus for Advanced Renal Cell Carcinoma. N Engl J Med. 2021. |
[25] | Motzer RJ , Tannir NM , McDermott DF , et al. Nivolumab plus Ipilimumab versus Sunitinib in Advanced Renal-Cell Carcinoma. N Engl J Med. (2018) ;378: :1277–90. |
[26] | Cella D , Grünwald V , Escudier B , et al. Patient-reported outcomes of patients with advanced renal cell carcinoma treated with nivolumab plus ipilimumab versus sunitinib (CheckMate 214): a randomised, phase 3 trial. The Lancet Oncology. (2019) ;20: :297–310. |
[27] | Rini BI , Plimack ER , Stus V , et al. Pembrolizumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. New England Journal of Medicine. (2019) ;380: :1116–27. |
[28] | Atkins MB , Rini BI , Motzer RJ , et al. Patient-Reported Outcomes from the Phase III Randomized IMmotion151 Trial: Atezolizumab+Bevacizumab versus Sunitinib in Treatment-Naïve Metastatic Renal Cell Carcinoma. Clin Cancer Res. (2020) ;26: :2506–14. |
[29] | Motzer RJ , Penkov K , Haanen J , et al. Avelumab plus Axitinib versus Sunitinib for Advanced Renal-Cell Carcinoma. N Engl J Med. (2019) ;380: :1103–15. |
[30] | Johnson DB , Sullivan RJ , Ott PA , et al. Ipilimumab Therapy in Patients With Advanced Melanoma and Preexisting Autoimmune Disorders. JAMA Oncology. (2016) ;2: :234–40. |
[31] | Leonardi GC , Gainor JF , Altan M , et al. Safety of Programmed Death-1 Pathway Inhibitors Among Patients With Non-Small-Cell Lung Cancer and Preexisting Autoimmune Disorders. Journal of clinical oncology: official journal of the American Society of Clinical Oncology.. (2018) ;36: :1905–12. |
[32] | Ouzaid I , Capitanio U , Staehler M , et al. Surgical Metastasectomy in Renal Cell Carcinoma: A Systematic Review. European Urology Oncology. (2019) ;2: :141–9. |
[33] | Choueiri TK , Hessel C , Halabi S , et al. Cabozantinib versus sunitinib as initial therapy for metastatic renal cell carcinoma of intermediate or poor risk (Alliance A03 CABOSUN randomised trial): Progression-free survival by independent review and overall survival update. European Journal of Cancer (Oxford, England:. (2018) ;94: :115–25. |
[34] | Choueiri TK , Escudier B , Powles T , et al. Cabozantinib versus everolimus in advanced renal cell carcinoma (METEOR): final results from a randomised, open-label, phase 3 trial. The Lancet Oncology. (2016) ;17: :917–27. |
[35] | Tannir NM , Signoretti S , Choueiri TK , et al. Efficacy and Safety of Nivolumab Plus Ipilimumab versus Sunitinib in First-line Treatment of Patients with Advanced Sarcomatoid Renal Cell Carcinoma. Clin Cancer Res. (2021) ;27: :78–86. |
[36] | Levy A , Menard J , Albiges L , et al. Second line treatment of metastatic renal cell carcinoma: The Institut Gustave Roussy experience with targeted therapies in 251 consecutive patients. European journal of cancer (Oxford, England: 1990). (2013) ;49: :1898–904. |
[37] | Wells JC , Stukalin I , Norton C , et al. Third-line Targeted Therapy in Metastatic Renal Cell Carcinoma: Results from the International Metastatic Renal Cell Carcinoma Database Consortium. European Urology. (2017) ;71: :204–9. |
[38] | Chen VJ , Hernandez-Meza G , Agrawal P , et al. Time on Therapy for at Least Three Months Correlates with Overall Survival in Metastatic Renal Cell Carcinoma. Cancers. 2019;11. |
[39] | Motzer RJ , Hutson TE , Glen H , et al. Lenvatinib, everolimus, and the combination in patients with metastatic renal cell carcinoma: a randomised, phase 2, open-label, multicentre trial. The Lancet Oncology. (2015) ;16: :1473–82. |
[40] | Wiele A , Ross J , Chahoud J , et al. Lenvatinib alone or in combination with everolimus in heavily pretreated patients with metastatic renal cell carcinoma immune checkpoint inhibitors. Annals of Oncology. 2019;30. |
[41] | Shah AY , Kotecha RR , Lemke EA , et al. Outcomes of patients with metastatic clear-cell renal cell carcinoma treated with second-line VEGFR-TKI after first-line immune checkpoint inhibitors. European journal of cancer (Oxford, England : 1990). (2019) ;114: :67–75. |
[42] | Grimm MO , Schmidinger M , Duran Martinez I , et al. Tailored immunotherapy approach with nivolumab in advanced renal cell carcinoma (TITAN-RCC). Annals of Oncology. 2019;30. |
[43] | Atkins MB , Jegede O , Haas NB , et al. Phase II study of nivolumab and salvage nivolumab+ipilimumab in treatment-naïve patients (pts) with advanced renal cell carcinoma (RCC) (HCRN GU16-260). Journal of Clinical Oncology. (2020) ;38: :5006. |
[44] | Lee C , Shah AY , Makker V , et al. Phase 2 study of lenvatinib plus pembrolizumab for disease progression after PD-1/PD-L1 immune checkpoint inhibitor in metastatic clear cell renal cell carcinoma. Annals of Oncology. 2019;30. |
[45] | Msaouel P , Gao J , Yuan Y , et al. Phase I/IB trial of sitravatinib (Sitra)+nivolumab (Nivo)+ipilimumab (Ipi) in patients (pts) with advanced clear cell renal cell carcinoma (accRCC) or other solid malignancies. J Clin Oncol. (2021) ;39: :AbstrTPS365. |
[46] | LaccettiAL, GarmezyB, XiaoL, et al. Combination antiangiogenic thyrosine kinase inhibition and anti-PD1 immunotherapy in metastatic renal cell carcinoma: A retrospective analysis of safety, tolerance, and clinical outcomes. (2021) ;10: (7):2341–9. |


