
Diagnosis value of multi-slice spiral CT in renal trauma
Abstract
Computed tomography (CT) is most commonly used as a noninvasive approach in diagnosis of internal organ injures. Use of multi-slice spiral CT becomes more popular in diagnosis of trauma because of its ability to generate 3D volumetric information. This study evaluated the diagnostic value of multi-slice spiral computed tomography (MSCT) with enhanced scanning in renal trauma. In total, 126 patients with kidney injury underwent MSCT scanning from a single hospital in the southern of China between January 2012 and February 2016. According to kidney injury grading standards of American Association for the Surgery of Trauma (AAST), 30 were diagnosed and classified in level I, 26 in level II, 42 in level III, 17 in level IV, 11 in level V. The outcomes of MSCT enhanced scanning achieve a 100% diagnostic accuracy rate, which was confirmed by surgical findings. We concluded that the enhanced MSCT scan permits reliable detection of renal trauma and the associated organ or tissue injuries, providing important clinical value for the diagnosis and classification of renal trauma or internal organ injures.
1Introduction
The incidences of internal organs are significantly rising with increasing numbers of patients injured due to motor vehicles and falling down during building construction in the urban development in Shenzhen, a city in the southern of China [1]. Renal injury is the third most common solid organ injury in blunt abdominal trauma, accounting for 14.1% of cases of abdominal injuries, in which blunt trauma accounts for up to 70% [2]. Renal injuries from blunt trauma usually occur as a consequence of a direct blow to the flank or from rapid deceleration. A direct blow crushes the kidney, causing a laceration or lacerations of the renal parenchyma and resulting in a subcapsular, intrarenal or perinephric haematoma. A deceleration injury causes an acute tension on the renal pedicle, resulting in the laceration of the renal vein or artery, an intimal tear in the vessel causing thrombosis or laceration, or an avulsion of the ureteropelvic junction (UPJ) [3].
Several image examinations have been often used in diagnosis of internal organs, including renal injury (Table 1). As one of simple approaches, ultrasound is helpful in indentation of the degree of renal injury, urine extravasation and the progress of the renal diseases, such as the kidney shrink with fibrosis formation at the late of stage after trauma. However, ultrasound image is limited in the accuracy of diagnosis and clinical grading assessments [4–6]. Although intravenous pyelography (IVP) is commonly used in the investigation of diseases in urinary tract system, it has been often not selected in detecting of renal trauma because IVP fails to detect blunt lesions and accurately stage some types of renal injuries [7]. Magnetic Resonance Imaging (MRI) has high accuracy but expensive and time-consuming, particularly, the patients who are rescued by medical equipment with metal materials are restricted. As an invasive - renal angiography is valuable in the diagnosis of renal vascular injury and renal pelvis injury [8]. Used in the evaluation of blunt renal injury, CT provides the exact delineation and staging of the extent of the renal injuries, which is superior to other methods of diagnosis image [3, 9]. The indications for renal imaging in trauma patients include gross haematuria, microscopic haematuria with shock (systolic blood pressure [SBP]<90 mmHg), microscopic haematuria with flank bruising, lower rib and lumbar spine transverse process fractures, penetrating trauma [10, 11]. The preferred treatment of blunt kidney injury varies according to grade of severity.
Multi-slice spiral computed tomography (MSCT) technology offers further advantages in detect of internal organ injures because it can acquire different thicknesses of image from the same acquisition data set. Moreover, MSCT with increased speed, thin collimation, large volume, and extreme flexibility provides additional superiority over single slice helical CT. High-quality interactive multiplanar and three-dimensional (3D) image reconstructions require the generation of almost isotropic voxels achieved by the increase in spatial resolution along the z-axis. The speed of MSCT allows imaging of organs in clearly defined perfusion phases [12]. High-spatial resolution of MSCT is able to gain more detail information of injured organ or tissue, which leads to an improvement in the detection and characterization of blunt lesions within kidney tissue. In this study, we retrospectively analyzed diagnostic and grading of qualitative value of MSCT scans in renal trauma.
2Patients and methods
In total, 126 patients (95 male and 31 female) were studied. The average age of patients was 32.6 years (age range 14∼61 years). Among total patients, 43 cases (34.1%) were due to traffic accident, 31 cases (24.6%) due to falls from heights, 22 cases (17.5%) blunt injury, 13 cases (10.3%) penetrating injuries, 17 cases (13.5%) other injuries (such as pathological renal injury and renal crush injury). The clinical manifestations included low back pain, hematuria, abdominal mass, or shock. All patients accepted MSCT scanning diagnosis and treated definitely, including 98 cases of conservative treatment, 4 cases of interventional therapy (renal artery embolization), 24 cases of surgical treatment. Unstable vital signs (i.e. instant changes in pulse rate, respiration rate and blood pressure) were often considered as an indicator for surgical exploration.
Light Speed VCT multislice CT (GE in USA) was used to performe scan or Denhanced scan. Non-ionic contrast agent (ioversol) at 350 mg/ml (80∼100 ml) was intravenously administrated, at the flow rate was 3.5 ml /s before CT scan. Patients were maintained in the supine position when scanning and the scanning range was from diaphragmatic dome to pubic symphysis. The scanning time was 30-second (s)in cortical phase, 60 s in substantive phase, 180 s in excretory phase. Delay time was 10∼20 min according to the image state displayed with contrast in the patients. Thickness of scanning slice was 5 mm with a thick layer of reconstruction to 2.5 mm, while reconstruction interval was 1.2 mm.A serial of CT images were sent to GE Advantage Workstation Workstation for 3D reconstruction, using multi-plane reorganization methods (i.e. multi planar reconstructions, maximum density projection and Maximum intensity projection).
3Results
CT findings in renal traumas included renal contusion, subcapsular haematoma, renal cortical laceration, fractured kidney, shattered kidney, traumatic renal artery occlusion, and traumatic vein thrombosis (Table 2). All 126 patients accepted MSCT scanning, including 104 cases with enhanced scan, and 45 cases with individually-scanned for the delayed phase. According to standard-based grading of American Association of Trauma Surgery (AAST) 1996 Organ Damage Grading System (OISI), renal traumas in all patients were listed in Table 2 for the grading of kidney injury severity [11, 13]. In Grade I injury, amoung 30 cases, 13 cases with simple subcapsular, and hematoma, had renal curved edge or fusiform in shape with slightly high density in CT imagines; 11 cases of simple renal contusion had the delayed renal parenchyma small sheet or strip weak enhancement or without enhancement area, but not involve the envelope in the images; 6 cases had both image features at the same time. In Grade II injury, 26 cases had low density shadow (less than or equal to 10 mm) in renal parenchyma, even enhancement by the contrast administration in renal parenchyma, and also had low density gaps within the perirenal fascia due to subcapsular or perirenal hematoma (Fig. 1) In Grade III injury, 42 cases had low density (>10 mm) in renal parenchyma but not involve the collection system, and irregular or curved high density after enhanced by contrast injection. In Grade IV injury, 17 cases had contrast agent leakage in the collection system due to renal vascular tear, patchy renal infarction, giant perirenal hematoma or retroperitoneal hematoma. Grade V injury, 11 cases had multiple renal parenchymal laceration giant perirenal hematoma or extended retroperitoneal hematoma, renal pedicle injury or amputation (Fig. 2).
In the treatment of renal trauma in Group I to III, one case with multiple knife stabbed with left pneumothorax, right renal laceration, hemorrhagic shock had emergency left thoracic cavity closed drainage and right renal surgical exploration and then underwent MSCT plain scan; the remaining 97 cases were non operative treatment. In Grade IV, four patients were treated with selective renal artery embolization, and other 13 cases had surgery. Eleven cases in Grade V had surgical treatment, including a renal repair, nephrectomy, renal pelvis and ureter anastomosis, ureteroscopy stent drainage, 1 case died after 15 hours later after operation due to severe multiple organ injuries.
4Discussion
The kidneys are paired retroperitoneal structures lying against the psoas muscles, cushioned by perinephric fat, and surrounded by Gerota’s fascia. The superior aspect of the kidney is protected by the lower ribs. However, the lower poles of the kidneys are inferior to the 12th ribs and therefore, more susceptible to trauma. Incidence of the kidney injury is about 5/10 million population per year, about 72% are young adults aged 16 to 44 years old and the ratio of male and female is about 3 : 1 [14]. The hematuria, back pain and low blood pressure after injury are clinical indicators of kidney trauma. However, severity of hematuria and degree of kidney damage are not correlated. Sometime, renal injury presents no hematuria in renal artery laceration or avulsion. About 24% patients with embolization of renal artery and renal pelvis injury did not have hematuria [15]. Therefore, image diagnosis is critical to evaluate the status of renal injury.
All cases in this study with blunt and penetrating renal injuries are classified based on American Association for Surgery of Trauma (AAST). This classification enables a standardization of various renal trauma and a choice of a proper therapy and a prediction [16]. Medical management depends on the grades of renal trauma. Recent studies showed that majority of low grade of renal trauma can be conservatively treated while high grade injure often needs surgery [17]. Up to 88% of patients with grade III and 78% of grade IV had conservative treatment; while 91% of grade V injuries needed the surgical management. Nephrectomy rates were: 13% in grade III, 17% in grade IV, and 9% in grade V; surgery exploration rate with an overall is 7% for all blunt renal trauma [18]. Indications for laparotomy are persistent life-threatening hemorrhage renal pedicle injury, an expanding or pulsatile retroperitoneal hematoma, indicating a renal artery rupture.
Treatment of renal trauma usually is based on accuracy of the image diagnosis in CT images. As a safe, noninvasive and fast diagnosis tool, MSCT scan can precisely evaluate each degree of injury of kidney, determine whether urine extravasation, perirenal hemorrhage and the conditions of adjacent organ [19]. Contrast-enhanced CT could quickly determine the condition of the renal parenchymal damage both in arterial phase and venous phase, and clearly show the range and the degree of renal injury [20], renal pedicle vessels. The enhanced CT provides directly accuracy transformed into 3D images, providing the kidney injury more accurate and intuitive images (Fig. 4). In addition, CT angiography (CTA) renal vascular reconstruction technique not only can provide most of the detections of renal arteriography, but also can provide the accuracy information of hemodynamics stability and vascular interventional therapy [21, 22].
In this study, medical enhancement scanning and surgical findings in 104 cases presents in line with the rate of 100%. However, one patient in critical condition was surgically explored due to right kidney bleeding displayed on MSCT scan (Fig. 3a). The right intact kidney was isolated due to lumbar artery rupture, which was found in surgery (Fig. 3b). On MSCT images, contrast overflowing out of the renal collection system indicates renal pelvis laceration. A delay scan can be used in the patients with renal damage degree to determine whether the collection system is damaged or not. In this study, damage of the renal pelvis and ureter was found in 6 of 37 patients who had delay scan. All of the 6 patients were recovered well after a timely appropriate treatment.
5Conclusions
An appropriate management of renal trauma greatly depends on accurate diagnosis and qualitative classification of kidney injury. A 3D image reconstruction is conducted through the volume of data collected which can clear the kidney injury more intuitively and accurately. MSCT provides detailed images of abdominal and retroperitoneal structures in the investigation of renal trauma. As imaging modality of choice, enhanced MSCT has advantage of fast scanning speed, covering a wide range, high resolution image for the acute stage injury. However, diagnostic value of MCST in renal function and structures years after trauma needs further study.
References
[1] | Dongyun L. , Wei G. , Daping W. Diagnosis value of spiral CT closed renal trauma. HEBEI Medicine (06) ((2015) ), 937–939. |
[2] | McAninch J.W. , Santucci R.A. Renal and ureteral injuries, In: Gillenwater JY, Grayhack JT, Howards SS, Mitchell ME, eds Adult andediatric Urology Philadelphia: Lippincott Williams & Wilkins, ((2002) ), 479–506. |
[3] | Razali M.R. , Azian A.A. , Amran A.R. et al., Computed tomography of blunt renal trauma[J], Singapore Med J 51: (6) ((2010) ), 468–473; quiz 474. |
[4] | Aragona F. , Pepe P. , Patane D. et al., Management of severe blunt renal trauma in adult patients: A 10-year retrospective review from an emergency hospital[J]. BJU Int 110: (5) ((2012) ), 744–748. |
[5] | Baverstock R. , Simons R. , Mcloughlin M. Severe blunt renal trauma: A 7-year retrospective review from a provincial trauma centre[J]. Can J Urol 8: (5) ((2001) ), 1372–1376. |
[6] | Zabkowski T. , Skiba R. , Saracyn M. et al., Analysis of renal trauma in adult patients: A 6-year own experiences of trauma center[J]. Urol J 12: (4) ((2015) ), 2276–2279. |
[7] | Thall E.H. , Stone N.N. , Cheng D.L. et al., Conservative management of penetrating and blunt Type III renal injuries[J]. Br J Urol 77: (4) ((1996) ), 512–517. |
[8] | Bent C. , Iyngkaran T. , Power N. et al., Urological injuries following trauma. Clin Radiol 63: (12) ((2008) ), 1361–1371. |
[9] | Fleischmann D. Multiple detector-row CT angiography of the renal and mesenteric vessels[J]. Eur J Radiol 45: (Suppl 1) ((2003) ), S79–S87. |
[10] | Carpio F. , Morey A.F. Radiographic staging of renal injuries[J]. World J Urol 17: (2) ((1999) ), 66–70. |
[11] | Federle M.P. , Kaiser J.A. , Mcaninch J.W. et al., The role of computed tomography in renal trauma[J]. Radiology 141: (2) ((1981) ), 455–460. |
[12] | Tinkoff G. , Esposito T.J. , Reed J. et al., American Association for the Surgery of Trauma Organ Injury Scale I: Spleen, liver, and kidney, validation based on the National Trauma Data Bank[J]. J Am Coll Surg 207: (5) ((2008) ), 646–655. |
[13] | Lin W.C. , Lin C.H. , Chen J.H. et al., Computed tomographic imaging in determining the need of embolization for high-grade blunt renal injury. J Trauma Acute Care Surg 74: (1) ((2013) ), 230–235. |
[14] | Moore E.E. , Shackford S.R. , Pachter H.L. et al., Organ injury scaling: Spleen, liver, and kidney[J]. J Trauma 29: (12) ((1989) ), 1664–1666. |
[15] | Alonso R.C. , Nacenta S.B. , Martinez P.D. et al., Kidney in danger: CT findings of blunt and penetrating renal trauma[J]. Radiographics 29: (7) ((2009) ), 2033–2053. |
[16] | Buckley J.C. , Mcaninch J.W. Revision of current American Association for the Surgery of Trauma Renal Injury grading system[J]. J Trauma 70: (1) ((2011) ), 35–37. |
[17] | Santucci R.A. , McAninch J.M. Grade IV renal injuries: Evaluation, treatment, and outcome. World J Surg 25: (12) ((2001) ), 1565–1572. |
[18] | Ashebu S.D. , Dahniya M.H. , Aduh P. et al., Rupture of the renal pelvis of a ureteropelvic junction hydronephrosis after blunt abdominal trauma[J]. Australas Radiol 48: (2) ((2004) ), 256–258. |
[19] | Onwubiko C. , Mooney D.P. The value of official reinterpretation of trauma computed tomography scans from referring hospitals[J]. J Pediatr Surg 51: (3) ((2016) ), 486–489. |
[20] | Fraser J.D. , Aguayo P. , Ostlie D.J. et al., Review of the evidence on the management of blunt renal trauma in pediatric patients[J]. Pediatr Surg Int 25: (2) ((2009) ), 125–132. |
[21] | Smithson L. , Morrell J. , Kowalik U. et al., Correlation of computed tomographic signs of hypoperfusion and clinical hypoperfusion in adult blunt trauma patients[J]. J Trauma Acute Care Surg 78: (6) ((2015) ), 1162–1167. |
[22] | Puig S. , Schaefer-Prokop C. , Mang T. et al., Single- and multi-slice spiral computed tomography of the paediatric kidney[J]. Eur J Radiol 43: (2) ((2002) ), 139–145. |
Figures and Tables
Fig.1
Left kidney stab wound.
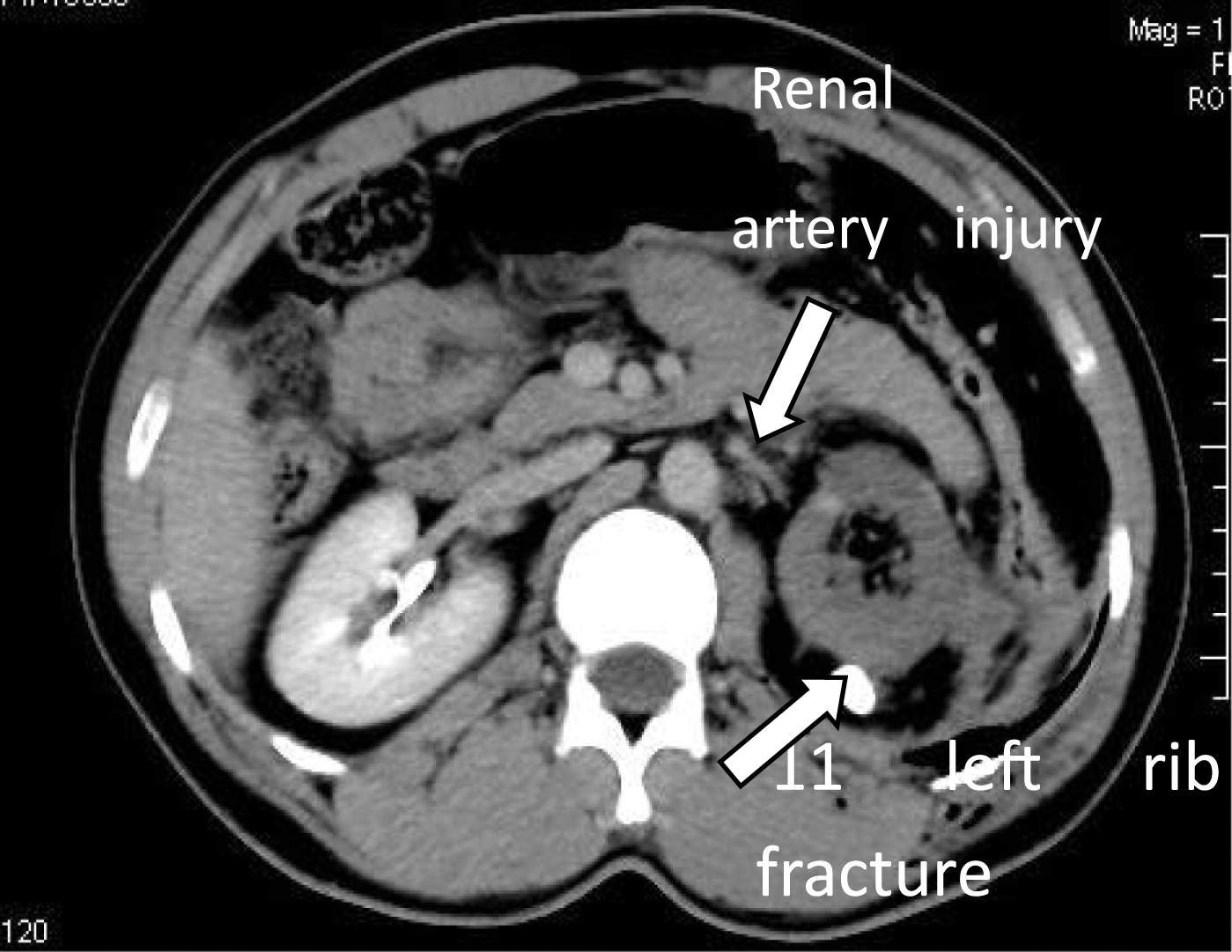
Fig.2
Left 11th rib fracture and the left renal pedicle de-vascularization.

Fig.3
(a) Right kidney enlarges due to injury. (b) Surgical exploration showed a complete right kidney (Lunbarartery hemorrhage).
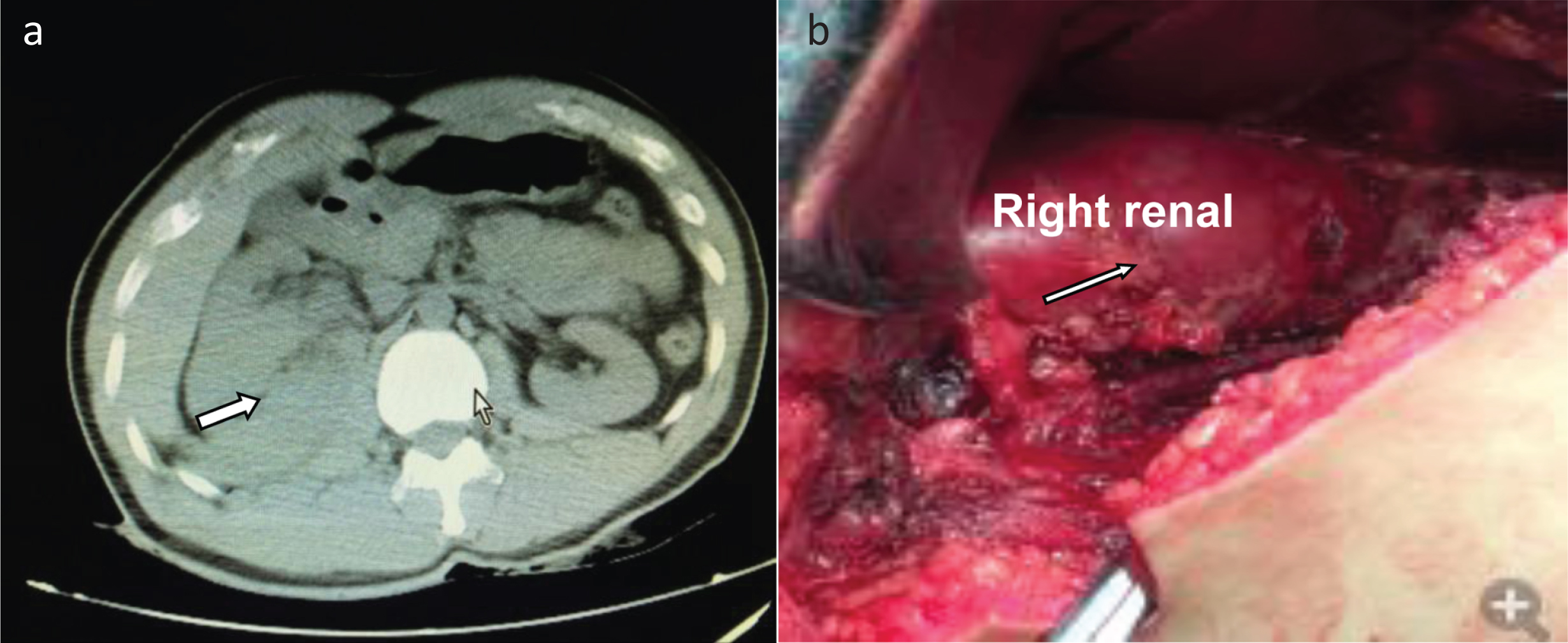
Table 1
Comparison of different examination methods for renal injury
| Advantage | Disadvantage | |
| Ultrasound | Simple, non-invasive, cheaper, | Limitation in accuracy |
| Intravenous pyelography (IVP) | Accuracy is relatively high | Sensitivity and specificity is not strong |
| Magnetic Resonance Imaging (MRI) | High accuracy | Expensive, time-consuming |
| Renal Angiography | High specificity, accuracy, | Invasive examination, time consuming, |
| Computed Tomography (CT) | High sensitivity and specificity | Relatively expensive, multi slider images |
| 3D reconstruction CT | 3D, entire images, easier to identify the lesions | Need the soft program to reconstruct 3D rotated system |
Table 2
Kidney trauma scale in Multi-slice spiral CT examination
| Grade of renal trauma | Number of cases | Symptoms and features of multi-slice spiral CT |
| I. Contusion Hematoma | 30 | Microscopic or gross hematuria, sub-capsular, |
| non-expanding without parenchymal laceration | ||
| II. Hematoma Laceration | 26 | Non-expanding peri-renal hematoma confined to renal retro-peritoneum <1 cm parenchymal depth of renal cortex without urinary extravasation |
| III. Laceration | 42 | >1 cm parenchymal depth of renal cortex without collecting system rupture or urinary extravasation |
| IV. Laceration Vascular | 17 | Parenchymal laceration extending through the renal cortex, medulla, collecting system; Main renal artery or vein injury with contained hemorrhage |
| V. Laceration Vascular | 11 | Completely shattered kidney, avulsion of renal hilum which de-vascularizes kidney |
Advance one grade for multiple or bilateral injuries up to grade III.


