
Diagnosis of Menière’s disease according to the criteria of 2015: Characteristics and challenges in 96 patients
Abstract
BACKGROUND:
The diagnosis of Menière’s disease (MD) is made according to diagnostic criteria, the last revision of which was in 2015. For diagnosis, symptoms are weighted with audiometric findings and this can be challenging in individual patients.
OBJECTIVE:
To analyze patient’s characteristics and symptoms in a real-life cohort of 96 patients with diagnosed MD regarding sociodemographic parameters, clinical specifics, and audiometry.
METHODS:
Prospective clinical patient registry containing demographic and socioeconomic parameters, symptoms, as well as pure-tone audiometry data.
RESULTS:
31 patients with definite MD, and 36 with probable MD were identified. 29 patients showed typical clinical signs of MD, but did not meet the full diagnostic criteria, and were considered separately. Mean duration of symptoms prior to presentation was 3.9±4.6 years. Significant differences between categories were found regarding aural fullness, tinnitus, and fluctuating hearing. If multiple audiograms were available, 28.6 % (6/21) documented fluctuating hearing.
CONCLUSIONS:
Current diagnostic criteria probably do not represent patients with monosymptomatic presentation or an early stage very well. Long-term follow-up with repeated audiometry is advisable.
1Introduction
Menière’s Disease (MD) was described by Prosper Menière as a characteristic triad of vertigo episodes, fluctuating hearing loss, and tinnitus, which he as-cribed to episodic malfunction of the inner ear [3]. In clinical practice, presentation of symptoms can be very diverse and diagnosis of MD might be challenging in some cases of early stage or monosymptomatic MD [27]. Beginning with the mere presentation of vertigo, patients report of spinning sensation, swaying vertigo, gait disorders, or dizziness with diverging length. Concerning aural symptoms, patients report of aural fullness, tinnitus and hearing loss, sometimes of fluctuating nature. Some cases even suffer from drop attacks, so called tumarkin crises. In addition to consolidating the broad symptomatic pattern of MD, the delineation to vestibular migraine plays a major role [28, 30].
Given the broad presentation of MD, expert associations have been trying to assist in diagnosing MD. The Equilibrium Committee of the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) had their first guidelines published in 1972 fittingly stating that “Meniere’s disease is capricious both in its behavior and its response to treatment.” [36]. Other than the AAO-HNS, the Japan Society for Equilibrium Research (JSER) did not publish their criteria for diagnosing MD, but discussed them extensively [9]. Then, in 1985, the AAO-HNS revised their diagnostic criteria along with a recommendation of reporting results and treatment related to MD [24]. They defined MD as an idiopathic disease of the inner ear exhibiting low-frequency fluctuating sensorineural hearing loss (SNHL) associated with tinnitus and spontaneous vertigo attacks lasting for minutes to hours. Another revision followed 10 years later, after several recommendations for improvement [21]. In this revision, the authors wanted to establish a distinction between the recording of results and analysis or interpretation of the results, as well as generate more compatible data for improved computer-based analysis. MD was categorized in 4 groups: possible MD, which included patients with both episodic Menière-type vertigo episodes without a documented hearing loss, or fluctuated/fixed SNHL with disequilibrium, but without definite vertigo episodes; probable MD, which included patients with one definitive episode of vertigo, audiometrically documented SNHL on at least 1 occasion, and tinnitus/aural fullness in the respective ear; definite MD, which included patients with two or more definitive vertigo episodes (20 minutes or longer), audiometrically documented SNHL on at least 1 occasion, and tinnitus/aural fullness in the respective ear; certain MD, which included patients, who fulfilled the criteria for a definite MD plus histopathologic confirmation of an hydrops.
It took 20 years for a joint effort of the Classification Committee for an International Classification of Vestibular Disorders (ICVD), a union of the Classification Committee of the Bárány Society, the Japan Society for Equilibrium Research, the European Academy of Otology and Neurotology (EAONO), the Equilibrium Committee of the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) and the Korean Balance Society, to revise the diagnostic criteria in an international consensus (Lopez-Escamez et al, 2015; Goebel, 2016). After excluding other causes for the symptoms, e. g. vestibular migraine or vestibular paroxysmia, patients are designated to either definite MD or probable MD. Definite MD is characterized by: two or more spontaneous episodes of vertigo, lasting 20 minutes to 12 hours; audiometrically documented low- to medium-frequency sensorineural hearing loss (below 2 kHz) in one ear, which defines the affected ear on at least one occasion before, during or after one of the episode of vertigo; fluctuating aural symptoms (hearing, tinnitus or aural fullness) in the affected ear. Probable MD is defined by two or more episodes of vertigo or dizziness lasting 20 minutes to 24 hours and fluctuating aural symptoms (hearing, tinnitus or aural fullness) in the affected ear.
In order to evaluate the value of the current diagnostic criteria in a clinical setting, we applied the criteria on our cohort of patients with MD over a time span of 3 years from a large dizziness registry and described the patients’ characteristics, symptoms, and audiometric results.
2Patients and Methods
2.1Adherence to ethical standards and study design
An analysis was performed from the prospective clinical patient registry DizzyReg, a single-center database of patients with vertigo or dizziness [10]. All patients were diagnosed and treated at the interdisciplinary outpatient vertigo clinic of the German Center of Vertigo and Balance Disorders of LMU Klinikum [5]. The registry was approved by the responsible institutional review board (Ethikkommission bei der Medizinischen Fakultät der LMU München) on August 26th, 2015 with the reference number 414–15.
2.2Patient selection and data collection
We included patients, aged 18 and above, which had given informed consent, were eligible to complete the questionnaires in terms of knowledge of the German language, and adequate cognitive state. Patients had to be diagnosed with MD with the inclusion of pure tone audiometry. Data collection was carried out by health professionals trained in data collection.
Clinical data was collected and managed by using the REDCap electronic data capture tools hosted at LMU Klinikum. REDCap (Research Electronic Data Capture, www.projectredcap.org) is a secure, web-based software platform designed to support data collection for research studies, providing 1) an intuitive interface for validated data capture; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for data integration and interoperability with external sources [12, 13]. Data analysis was performed from all 96 patients who entered the DizzyReg with the clinical diagnosis MD from 2015 to 2018.
Audiological data was collected using the proprietary prospective database ENTstatistics (Innoforce Est., Ruggell, Liechtenstein). The database was customized to the clinical and research workflow at the study center.
Patients were only included into this analysis when MD was diagnosed by expert consensus aided by current diagnostic criteria [18]. Patients with other proven vestibular disorders additionally to or instead of MD (e. g. vestibular migraine, cerebellopontine lesion, autoimmune disease, stable but uncompen-sated unilateral vestibulopathia without auditory symptoms e. g. as a single event in the past) were not considered.
2.3Sociodemography
Data on sociodemographic information, working and living situation, sports and exercises, falls, sleeping problems, smoking and alcohol consumption was collected using a purpose-made questionnaire. Further questions on self-reported symptoms, triggers of vertigo, as well as health care consultation prior to referral to the clinic were covered by this questionnaire.
2.4Diagnostic approach
All patients received an extensive vestibular wor-kup in line with the current diagnostic criteria inc-luding but not limited to criteria for MD [18, 21] and diagnosis was determined by consensus of senior clinical experts for neurotology at the DSGZ. Decision making always involved one consultant-/ attending-level senior physician in neurology as well as otorhinolaryngology each. This is in line with the guiding principles of the interdisciplinary outpatient vertigo clinic of the DSGZ [5]. Clinical workup included a detailed case history, neurological, otological, and neurotological clinical examination, as well as caloric testing, video head impulse test, orthoptic examination, and pure tone audiometry. Dependent on the history and differential diagnosis, vestibular evoked myogenic potentials were performed. All patients received magnetic resonance imaging with sequences targeted for the brainstem, cerebellopontine angle, and internal auditory meatus, with no unusual findings as it is standard protocol in Germany.
2.5Audiometric testing
Standard audiometric tests were performed in anechoic chambers by specialized and experienced technical staff. In brief, pure tone audiometry was conducted at 0.5, 1, 1.5, 2, 3, 4, 6, and 8 kHz for air (AC) and bone conduction thresholds (BC) between -10 dB and 120 dB hearing level (dB HL) for each ear separately. Thresholds exceeding 120 dB HL were recorded as 130 dB HL for statistical purposes.
For better description of low- to medium-frequ-ency sensorineural hearing loss (SNHL) often enco-untered in MD, several low frequency pure tone average (PTA) values were analyzed such as AC-PTA4 (0.25, 0.5, 1, 2 kHz), BC-PTA4 (0.25, 0.5, 1, 2 kHz), AC-PTA3 (0.25, 0.5, 1), BC-PTA3 (0.25, 0.5, 1), and the average of the worst frequency below 2 kHz with its worst neighbor value (PTA2). Since there is currently a debate whether current diagnostic criteria [18] do or should include the frequency 2 kHz into the definition of low- to medium-frequency, PTA2 was calculated twice, either including or not including 2 kHz.
WHO grades of hearing impairment were applied in order to classify hearing loss along an average threshold at 500 kHz, 1 kHz, 2 kHz and 4 kHz. Mild hearing loss is considered from 26–40 dB, moderate from 41–60 dB HL, severe from 61–80 dB, and profound above 81 dB HL.
Staging of MD was performed as defined in earlier diagnostic criteria [21]. This is based on an average of the thresholds at 500 Hz, 1 kHz, 2 kHz and 3 kHz and categorizes into stage 1 (≤25 dB HL), stage 2 (26–40 dB HL), stage 3 (41–70 dB HL), and stage 4 (>71 dB HL).
Fluctuating hearing loss describes the phenome-non that hearing function can repeatedly deteriorate and improve in conjunction with other vestibular symptoms. This can be assessed by pure tone audiometry. In the present study, fluctuating hearing loss was described along a PTA4 (0.5; 1; 2; 3 kHz) to allow for comparison of disease stages according to Monsell [21].
2.6Statistical analyses
Data was statistically analyzed with the program R version 3.3.2 (R Foundation for Statistical Computing, Vienna, Austria). Prior to group comparison, the Kolmogorov-Smirnov goodness-for-fitness test assessed no normal distribution. Levene's test was performed in order to investigate for equality of variances. Regarding comparing analysis, the chi-square test and the Wilcoxon-Mann-Whitney U-test was applied. Differences were considered significant at p-values of less than 0.05. Figures were created with Microsoft Excel version 1906.
3Results
3.1Patient’s characteristics and sociodemography
In the registry, 96 patients met the inclusion criteria with a mean age of 52.2±14.0 years (range: 25 to 78 years). According to current criteria [18], they were classified in three categories as either definite MD (dMD) (31 patients) or probable MD (pMD) (36 patients). 29 patients did not meet those canonical diagnostic categories, although MD was the most likely diagnosis due to exclusion of other vestibular or related neurologic disorders by expert consensus after extensive diagnostic workup at the study center. Those patients were included into the present analysis as the additional category “Meniere’s characteristics” (MC).
The share of patients diagnosed before the age of 50 years was 48% (n = 46), 7% (n = 7) were diagnosed before the age of 30 years. There was no significant difference between the three groups in respect to gender, age, side, or duration of symptoms. Most patients in each group (dMD 61%, n = 19; pMD 62%, n = 22; MC 66%, n = 19) attended elementary school with apprenticeship or middle school. A subset of 17% (n = 16) of all patients were smokers. On average, patients slept more than 7 hours (7.6±1.3 hours). No significant difference could be found regarding sleep onset insomnia (“almost never” in dMD 52%, pMD 25%, MC 31%; p = 0.053). More than half of the patients were physically active on a regular basis (55%, n = 51). Demographic characteristics and of all 96 patients are shown in Table 1 and Supplemental Table 1.
Table 1
Sociodemographic Characteristics
| dMD | pMD | MC | total | p-value | |
| Gender [n (%)] | 0.376 | ||||
| female | 15 (48%) | 22 (61%) | 13 (45%) | 50 (52%) | |
| male | 16 (52%) | 14 (39%) | 16 (55%) | 46 (48%) | |
| Age [yrs±SD] | 53.4±12.9 | 49±13.5 | 52.45±15.5 | 51.5±14.0 | 0.385 |
| Age group [n (%)] | 0.504 | ||||
| ≤30 yrs | 1 (3%) | 3 (8%) | 3 (10%) | 7 (7%) | |
| 30–40 yrs | 7 (23%) | 7 (19%) | 1 (3%) | 15 (16%) | |
| 40–50 yrs | 5 (16%) | 9 (25%) | 10 (34%) | 24 (25%) | |
| 50–60 yrs | 9 (29%) | 8 (22%) | 5 (17%) | 22 (23%) | |
| 60–70 yrs | 6 (19%) | 7 (19%) | 6 (21%) | 19 (20%) | |
| 70–80 yrs | 3 (10%) | 2 (6%) | 4 (14%) | 9 (9%) | |
| Side [n (%)] | 0.275 | ||||
| right | 10 (32%) | 19 (53%) | 13 (45%) | 42 (44%) | |
| left | 19 (61%) | 13 (36%) | 11 (38%) | 43 (45%) | |
| both | 2 (6%) | 4 (11%) | 4 (14%) | 10 (10%) | |
| localization not possible | 0 (0%) | 0 (0%) | 1 (3%) | 1 (1%) | |
| Schooling [n (%)] | 0.840 | ||||
| no graduation | 0 (0%) | 1 (3%) | 0 (0%) | 1 (1%) | |
| elementary school without apprenticeship | 1 (3%) | 1 (3%) | 3 (10%) | 5 (2%) | |
| elementary school with apprenticeship | |||||
| o-level/middle school/a-level/vocational | 9 (29%) | 11 (31%) | 11 (38%) | 31 (32%) | |
| baccalaureate diploma/university of applied sciences entrance qualification | |||||
| college/university of applied science/university | 10 (32%) | 11 (31%) | 8 (28%) | 29 (30%) | |
| other degree | |||||
| 3 (10%) | 4 (11%) | 3 (10%) | 10 (10%) | ||
| 8 (26%) | 7 (19%) | 3 (10%) | 18 (19%) | ||
| 0 (0%) | 1 (3%) | 1 (3%) | 2 (2%) | ||
| Alcohol consumption [n (%)] | 11 (35%) | 17 (47%) | 15 (52%) | 43 (45%) | 0.420 |
| Nicotine consumption [n (%), n = 95] | 8 (26%) | 3 (8%) | 5 (18%) | 16 (17%) | 0.160 |
| Sleep hours [h] | 7.8±1.5 | 7.4±1.1 | 7.8±1.3 | 7.6±1.3 | 0.414 |
| Sleep onset insomnia [n (%)] | 0.053 | ||||
| almost never | 16 (52%) | 9 (25%) | 16 (55%) | 41 (43%) | |
| sometimes | 13 (42%) | 20 (56%) | 8 (28%) | 41 (43%) | |
| often | 2 (6%) | 7 (19%) | 5 (17%) | 14 (15%) | |
| Sleep maintenance insomnia [n (%)] | 0.988 | ||||
| almost never | 9 (29%) | 11 (31%) | 9 (31%) | 29 (30%) | |
| sometimes | 12 (39%) | 13 (36%) | 12 (41%) | 37 (39%) | |
| often | 10 (32%) | 12 (33%) | 8 (28%) | 30 (31%) | |
| Physical activity [n (%), n = 93] | 20 (65%) | 16 (46%) | 15 (56%) | 51 (55%) | 0.308 |
| Total [n] | 31 | 36 | 29 | 96 |
dMD = definite Menière’s disease; pMD = probable Menière’s disease; MC = Menière’s characteristics; yrs = years; SD = standard deviation; n = number.
The mean prevalence of migraine was 11% (n = 11). Various patients reported inflammatory or immunological diseases in their medical history. Thereof, allergic rhinitis (26 of 96 patients, 27%) and asthma (13 of 96, 14 %) were most frequent. Overall, the most common comorbidity was high blood pressure. There was no significant difference between diagnostic categories regarding the occurrence of any comorbidity to MD (Table 2).
Table 2
Comorbidities
| dMD | pMD | MC | total | p-value | |
| Migraine [n (%)] | 2 (6%) | 4 (11%) | 5 (17%) | 11 (11%) | 0.453 |
| Inflammatory/immunological diseases [n (%)] | |||||
| asthma | 2 (6%) | 7 (19%) | 4 (14%) | 13 (14%) | 0.301 |
| chronic obstructive pulmonary disease (COPD) | 0 (0%) | 1 (3%) | 0 (0%) | 1 (1%) | 0.431 |
| chronic bronchitis | 2 (6%) | 1 (3%) | 0 (0%) | 3 (3%) | 0.353 |
| allergic rhinitis | 6 (19%) | 8 (22%) | 12 (41%) | 26 (27%) | 0.113 |
| inflammatory joint disease | 1 (3%) | 3 (8%) | 3 (10%) | 7 (7%) | 0.545 |
| Cardiovascular Diseases [n (%)] | |||||
| heart failure/cardiac insufficiency | 0 (0%) | 1 (3%) | 1 (3%) | 2 (2%) | 0.604 |
| cardiac rhythm disorder | 1 (3%) | 5 (14%) | 3 (10%) | 9 (9%) | 0.321 |
| other heart disorder | 1 (3%) | 0 (0%) | 0 (0%) | 1 (1%) | 0.347 |
| high blood pressure | 11 (35%) | 8 (22%) | 12 (41%) | 31 (32%) | 0.234 |
| Other comorbidities [n (%)] | |||||
| other neurological disease | 0 (0%) | 2 (6%) | 1 (3%) | 3 (3%) | 0.425 |
| liver disease | 1 (3%) | 0 (0%) | 1 (3%) | 2 (2%) | 0.541 |
| kidney disease | 1 (3%) | 2 (6%) | 1 (3%) | 4 (4%) | 0.869 |
| Total [n] | 31 | 36 | 29 | 96 |
dMD = definite Menière’s disease; pMD = probable Menière’s disease; MC = Menière’s characteristics; n = number.
3.2Symptoms and disease characteristics
An overview of symptom distribution according to current diagnostic criteria is given in Fig. 1. The diagnostic category MC was heterogenous. 52% (n = 15) reported of aural symptoms alone without vertigo. 8 patients (27%) with MC suffered from audiometrically documented low- to medium-frequency SNHL, 4 (14%) reported of vertigo without cochlear symptoms.
Fig. 1
Distribution of symptoms along current diagnostic criteria [18] in 96 patients evaluated for Menière’s Disease (MD). (#) 31 patients categorized as definite Menière’s Disease (dMD). (†) 36 patients categorized as probable Menière’s disease (pMD).
![Distribution of symptoms along current diagnostic criteria [18] in 96 patients evaluated for Menière’s Disease (MD). (#) 31 patients categorized as definite Menière’s Disease (dMD). (†) 36 patients categorized as probable Menière’s disease (pMD).](https://ip.ios.semcs.net:443/media/ves/2022/32-3/ves-32-3-ves201634/ves-32-ves201634-g001.jpg)
There was a wide variance between diagnostic categories regarding episodes of vertigo and aural symptoms. A highly significant difference was found for aural fullness. This was mainly due to widely varying proportions in the occurrence of aural fullness between dMD and MC (p = 0.003) as well as between pMD and MC (p < 0.001), while dMD and pMD did not differ significantly (p = 0.333). Comparable differences were found between fluctuating hearing, and tinnitus. Again, those symptoms differentiated dMD and pMD on one side and MC on the other side, but no significant differences were found between the categories dMD and pMD.
Most patients reported the presence of symptoms for multiple years with an average duration of 2.9±4.6 years. A variety of additional vestibular symptoms was stated with potential relation to fluctuating peripheral vestibular dysfunction. Nausea, gait disturbance, emesis and unsteadiness were mentioned by most patients with 74/96 (77 %), 70/96 (73 %), 68/96 (71 %) and 58/96 (60 %), respectively. There were no significant differences between diagnostic categories for those parameters (Table 3, Supplemental Table 2).
Table 3
Symptoms
| dMD | pMD | MC | total | p-value | |
| Duration of symptoms [yrs±SD (n)] | 3.0±3.7 (29) | 2.6±5.7 (36) | 3.1±4.0 (28) | 2.9±4.6 (93) | 0.917 |
| Episodes of vertigo [n (%)] | < 0.001** | ||||
| vertigo 20 min –12 h | 31 (100%) | 24 (67%) | 7 (24%) | 62 (65%) | |
| vertigo or dizziness 20 min –24 h | 0 (0%) | 12 (33%) | 3 (10%) | 15 (16%) | |
| other | 0 (0%) | 0 (0%) | 19 (66%) | 19 (20%) | |
| Aural symptoms [n (%)] | |||||
| any aural symptom | 31 (100%) | 36 (100%) | 16 (55%) | 83 (86%) | < 0.001** |
| fluctuating hearing | 20 (65%) | 22 (61%) | 10 (34%) | 52 (54%) | 0.038* |
| tinnitus | 23 (74%) | 27 (75%) | 13 (45%) | 63 (66%) | 0.019* |
| aural fullness | 16 (52%) | 25 (69%) | 5 (17%) | 46 (48%) | < 0.001** |
| Other vestibular symptoms [n (%)] | |||||
| oscillopsia | 5 (14%) | 5 (17%) | 15 (16%) | 0.930 | |
| emesis | 5 (16%) | 23 (64%) | 19 (66%) | 68 (71%) | 0.151 |
| double vision | 3 (8%) | 1 (3%) | 6 (6%) | 0.720 | |
| unsteadiness | 26 (84%) | 22 (61%) | 17 (59%) | 58 (60%) | 0.972 |
| nystagmus | 2 (6%) | 10 (28%) | 12 (41%) | 33 (34%) | 0.511 |
| nausea | 19 (61%) | 30 (83%) | 21 (72%) | 74 (77%) | 0.522 |
| gait disturbance | 11 (35%) | 27 (75%) | 20 (69%) | 70 (73%) | 0.846 |
| impaired vision | 23 (74%) | 8 (22%) | 7 (24%) | 24 (25%) | 0.807 |
| blurred vision | 23 (74%) | 12 (33%) | 5 (17%) | 28 (29%) | 0.235 |
| 9 (29%) | |||||
| 11 (35%) | |||||
| Total [n] | 31 | 36 | 29 | 96 |
*p < 0.05; **: p < 0.01 dMD = definite Menière’s disease; pMD = probable Menière’s disease; MC = Menière’s characteristics; yrs = years; h = hours; min = minutes; SD = standard deviation; n = number.
3.3Hearing and audiometry
Audiometrically documented hearing impairment differed markedly between diagnostic categories, again in part explained by audiometry being a diagnostic criterion. Asymmetric SNHL was found in the vast majority of patients, in particular in the diagnostic categories dMD and MC. Interestingly, patients in the category dMD showed an average air-bone-gap of 22.1±15.1 dB HL at 250 Hz and 15.1±14.7 dB HL at 500 Hz. Average air-bone-gap was lower than 10 dB HL in every other frequency in this category and in every frequency in the other two categories. Figure 2 gives an overview of the affected and unaffected sides for each group.
Fig. 2
Mean pure tone audiograms of all 96 patients. solid lines: air conduction thresholds, dashed lines: bone conduction thresholds. A, C, E: affected sides; B, D, F: contralateral sides. A, B: 31 patients with dMD; C, D: 36 patients with pMD; E, F: 29 patients with MC. Data shown as mean values±standard deviation dMD, definite Menière’s Disease; MC, Menière’s characteristics; pMD, probable Menière’s Disease
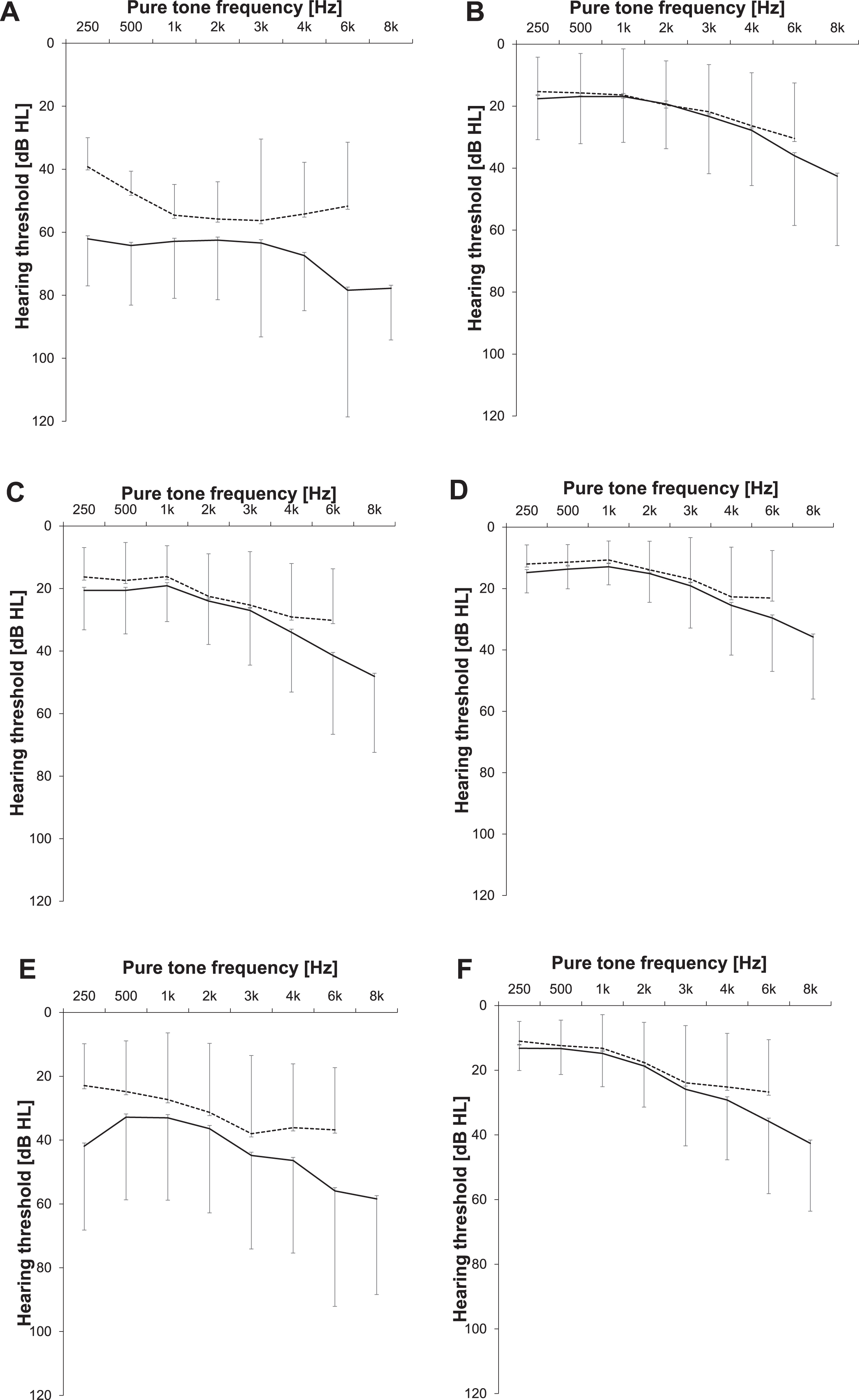
Categorial audiometric parameters showed significant differences between diagnostic categories. WHO grades of hearing impairment were asymmetric in most patients and hearing loss was more advanced on the affected side in dMD compared to MC and pMD. Additionally, there was a statistically significant difference between the diagnostic categories in the grade of hearing impairment, also on the contralateral side, again with dMD-patients showing the worst findings (41% of severe or worse impairment in dMD, 0% pMD, 20% MC).
Disease stage was significantly more advanced in the categories dMD and MC than in pMD. A significant difference between diagnostic categories could also be found for all forms of pure tone average values adapted to MD, from 2, 3 or 4 frequencies as well as air and bone conduction. In all instances, dMD-patients showed the worst, and pMD-patients the best results with MC in between (Fig. 3). Mean thresholds at low frequencies of the affected side, stage of MD, and the grade of hearing loss are reported in Table 4, while pairwise comparisons between groups are given in Supplemental Table 3.
Fig. 3
Overview of pure tone average values according to diagnostic categories. Yellow, definite Menière’s disease (dMD); red, probable Menière’s disease (pMD); green, Menière’s characteristics (MC). Horizontal bar, median value; box, interqartile range (IQR, 25th to 75th percentile); whiskers, maximum or minimum within 1.5*IQR; circles, outliers.
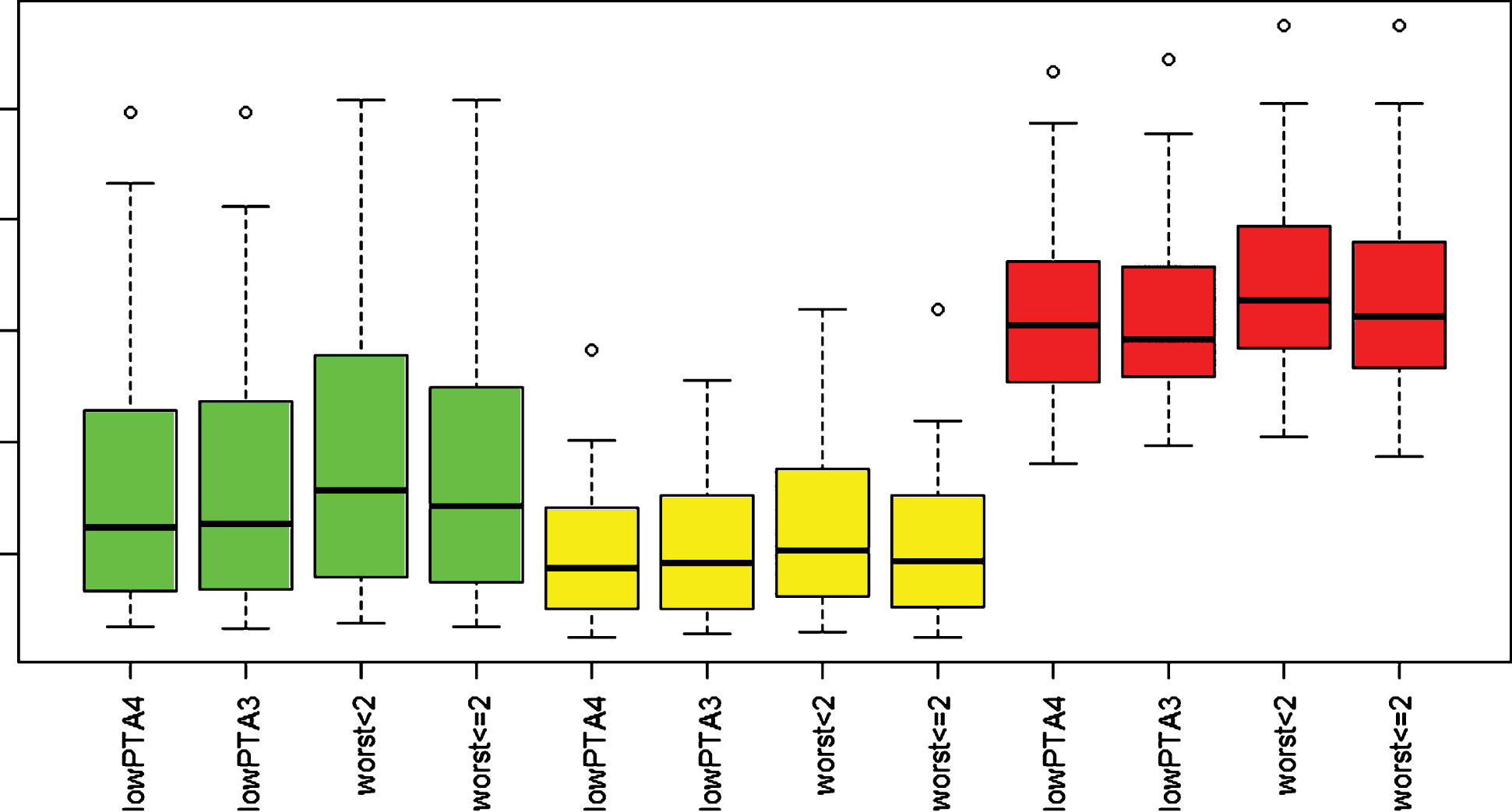
Table 4
Audiometry
| dMD | pMD | MC | Total | p-value | |
| WHO grade of hearing loss affected side [n (%)] | < 0.001** | ||||
| no impairment | 0 (0%) | 20 (56%) | 12 (41%) | 32 (33%) | |
| slight impairment | 1 (3%) | 12 (33%) | 6 (21%) | 19 (20%) | |
| moderate impairment | 14 (45%) | 4 (11%) | 5 (17%) | 23 (24%) | |
| severe impairment | 11 (35%) | 0 (0%) | 5 (17%) | 16 (17%) | |
| profound impairment or deafness | 5 (16%) | 0 (0%) | 1 (3%) | 6 (6%) | |
| WHO grade of hearing loss contralateral side [n (%)] | < 0.001** | ||||
| no impairment | 23 (74%) | 29 (81%) | 22(76%) | 74 (77%) | |
| slight impairment | 4 (13%) | 7 (19%) | 6 (21%) | 17 (18%) | |
| moderate impairment | 3 (10%) | 0 (0%) | 1 (3%) | 4 (4%) | |
| severe impairment | 1 (3%) | 0 (0%) | 0 (0%) | 1 (1%) | |
| profound impairment or deafness | 0 (0%) | 0 (0%) | 0 (0%) | 0 (0%) | |
| Staging [n]# | < 0.001** | ||||
| stage 1 | 0 (0%) | 21 (58%) | 12 (41%) | 34 (35%) | |
| stage 2 | 2 (6%) | 11 (31%) | 7 (24%) | 19 (20%) | |
| stage 3 | 20 (65%) | 4 (11%) | 6 (21%) | 30 (31%) | |
| stage 4 | 9 (29%) | 0 (0%) | 4 (14%) | 13 (14%) | |
| Summary of AC-PTA parameters [dB] | |||||
| low frequency PTA4 (0.25; 0.5; 1; 2 kHz) | 62.9±16.8 | 20.9±11.7 | 40.3±25.3 | 38.8±25.3 | < 0.001** |
| low frequency PTA3 (0.25; 0.5; 1 kHz) | 63.1±17.3 | 20±12.14 | 39.8±25.9 | 38.3±26 | < 0.001** |
| worst two contiguous low frequencies < 2 PTA2 | 65.4±18.1 | 21.8±13.5 | 41.8±26.6 | 40.3±26.8 | < 0.001** |
| worst two contiguous low frequencies≤2 PTA2 | 67.7±16.8 | 24.7±14.3 | 44.6±27.0 | 43.3±26.6 | < 0.001** |
| Summary of BC-PTA parameters [dB] | < 0.001** | ||||
| low frequency PTA4 (0.5; 1; 2; 3 kHz) | 53.5±7.9 | 20.3±11.5 | 28.8±19.4 | 33.4±19.5 | |
| low frequency PTA3 (0.25; 0.5; 1 kHz) | 47.2±6.2 | 16.7±9.9 | 25.2±16.7 | 28.9±17.3 | |
| worst two contiguous low frequencies < 2 PTA2 | 51.0±7.7 | 16.9±10.6 | 25.7±18.0 | 30.3±19.2 | |
| worst two contiguous low frequencies≤2 PTA2 | 53.5±8.7 | 19.9±11.7 | 29.7±20.1 | 34.4±20.9 | |
| audiometrically documented hearing loss | |||||
| low- to medium-frequency SNHL | 31 (100%) | 0 (0%) | 8 (28%) | 39 (41%) | < 0.001** |
| any other hearing loss | 0 (0%) | 14 (39%) | 8 (28%) | 22 (23%) | 0.001** |
| only one audiogram | 20 (65%) | 32 (89%) | 23 (79%) | 75 (78%) | |
| multiple audiograms | 0.344 | ||||
| multiple audiograms, never pathologic | 0 (0%) | 2 (56%) | 2 (7%) | 4 (4 %) | |
| multiple pathologic audiograms, never recovery | 7 (22%) | 1 (3%) | 3 (10%) | 11 (11%) | |
| multiple pathologic audiograms, recovery > 10 dB | 4 (13%) | 1 (3%) | 1 (3%) | 6 (6%) | |
| thereof recovery with change of stage† | 2 (6%) | 1 (3%) | 1 (3%) | 4 (4 %) | |
| Total [n] | 31 | 36 | 29 | 96 |
**p < 0.01 #: according to [22] dMD = definite Menière’s disease; pMD = probable Menière’s disease; MC = Menière’s characteristics; AC = air conduction; BC = bone conduction; PTA = pure tone average; SNHL = sensorineural hearing loss; SD = standard deviation; n = number.
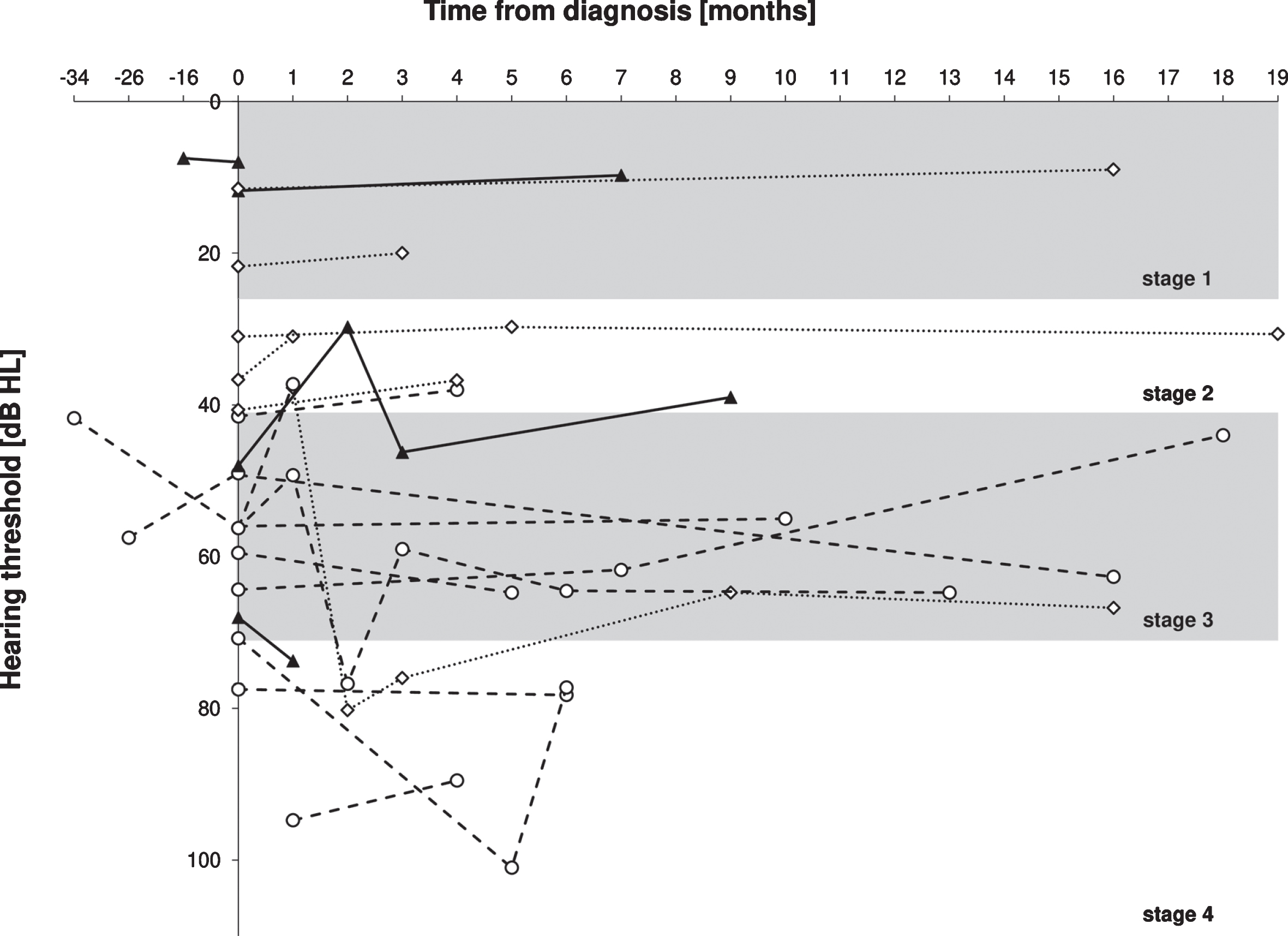
All patients with dMD had audiometrically documented low- to medium-frequency SNHL in the affected ear. This did also occur in 8/29 (28%) of MC cases but in no patients with pMD. Other forms of hearing loss were only prevalent in pMD and MC. These findings constituted significant differences between diagnostic categories. Audiometrically documented fluctuating hearing loss is a major aspect that helps to differentiate MD from other forms of asymmetric SNHL. However, it is only possible to detect this if multiple audiograms from distinct timepoints are available. This is a relevant obstacle in a specialized dizziness unit like the study center, since patients are often seen once for referral only. In the present study, a subset of 21,9% (n = 21) of all 96 patients received more than one audiometric testing. For 6 patients, even 3 or more audiograms were available with a maximum of 7. Fluctuating hearing loss was a finding in a considerable share of patients with multiple audiograms. A recovery of 10 dB or more in PTA4 (0.5; 1; 2; 3 kHz) over the previous audiogram was seen in 4/11 (36%) patients with dMD, 1/4 (25 %) with pMD and 1/6 (17 %) with MC. The extent of fluctuation towards hearing improvement was up to 23.7 dB within less than 1 month. 4 patients (2 dMD, 1 pMD and 1 MC) even improved in disease stage, two cases from 3 to 2, one from 4 to 2 and one from 4 to 3 (Table 4). Hearing fluctuation by PTA4 is visualized in Fig. 4.
Fig. 4
Changes in average hearing threshold (PTA4 : 0.5 kHz; 1 kHz;2 kHz; 3 kHz) of 21patients in the affected ear before and after diagnosis of Menière’s disease. Dashed lines: 11 patients with dMD; dotted lines: 6 patients with pMD; solid lines 4 patients with MC.
4Discussion
In this study, a relevant share of patients with Menière-like symptoms (29 of 96 patients, 30.2 %) did not fit into current diagnostic categories although MD is the only plausible explanation for their symptoms. Those patients are evaluated as an additional category (MC) here. Sociodemographic characteristics were balanced in all three categories dMD, pMD, and MC. In comparison, we found significant differences between the diagnostic categories with respect to hearing loss and other aural symptoms. The presence of aural symptoms differentiated between the canonic categories dMD and pMD, and the newly identified category MC. Whereas, analysis of hearing loss showed differences between dMD and pMD with MC lying in the middle; along the diagnostic criteria patients who were categorized dMD showed most advanced hearing loss. An asset of the study is the availability of multiple audiograms at different time points in multiple cases.
This is the first study to our knowledge that categorized patient groups with MD according to the current guidelines from 2015 [18]. Many previous studies even from a recent date rely on the 1995 version [1, 34, 35]. Analyzed parameters were confined to patients’ characteristics, reported symptoms, and audiometric results. The report and analysis of results from vestibular testing were outside the scope of this work.
This study does not include magnetic resonance inner ear imaging of the endolymph space. The vis-ualization of endolymphatic hydrops is currently inv-estigated as a marker for MD but shows conflicting evidence and a variety of protocols exists with preference still unclear [19]. Since this imaging modality is not part of current diagnostic criteria [18] or recommendations for management [4, 25], it is not yet included into routine clinical practice at the study center. Therefore, inner ear imaging was only available for few patients and could therefore not be meaningfully included into the present analysis. Clearly, a clinically well characterized patient cohort with uniform inner ear imaging would be of additional value and should be aimed for in future studies.
Average age at initial presentation was on the lower range in comparison to other studies that reported a mean of 53 to 70 years [7, 29]. While others reported a higher prevalence of MD among females [2, 11, 29], we observed a balanced occurrence by gender.
A subset of around 10% of the patients in our study also reported migraine, which is in line with other studies observing a correlation between MD and migraine. Other reports on MD found a higher share of migraine or vestibular migraine from 17,5 % [8] to 46.6% [34] of cases. The low percentage found in our sample probably reflects a more precise discrimination of diagnoses in an interdisciplinary setting inc-luding both neurological and otorhinolaryngological expertise in every patient. We did not find a significant difference between diagnostic categories regarding inflammatory or immunological diseases within our patients. Allergic rhinits was the most frequently reported issue in this regard with 27 % of all patients in our study. In the literature, a prevalence of 31.5 % to 59.2 % is given for allergies in MD [6, 14]. Since autoimmune diseases are more frequent in familial MD than in sporadic cases [14], this could be a sign for less hereditary etiology in our dataset. However, structured data on the family history is lacking in our sample and we are therefore not able to draw a conclusion in this regard.
Our investigations found a lower level of education in the majority of patients. This findings are in line with earlier studies which also associated MD with lower school level [33]. Almost a fifth of our patients were smokers. Smoking has been reported to be associated with MD before [32]. However, stress was described in a large share of patients to be involved in the progression of disease [31]. The group around Simo reported a prevalence of MD with higher household income [29], while other reports indicate deprivation as a risk factor [32]. The mean duration of the symptoms of 2.9±4.6 years before initial presentation to the study center is in line with 3.9±4.6 years reported elsewhere [26].
A considerable fraction of patients in our study, thereof almost all patients with MC (15/16), reported of aural symptoms alone, without any vertigo. The group around Zhang et al. found half of their cohort to initially present with isolated cochlear symptoms, as well as other patients with isolated vertigo without cochlear symptoms [35]. Presentation of cochlear symptoms alone, such as hearing loss and aural fullness without true vertigo or even tinnitus is an established finding in early stage MD [27]. In another study, 55% of patients reported of aural fulness as one of the first symptoms [17]. Characteristically for MD and a possible explanation of the patients investigated within the MC category is the known long interval between first symptoms and the full clinical picture of MD. A significant delay has been reported earlier with even 20% of patients taking more than five years between the initial presentation of symptoms and the development of pMD [26].
Based on disease stage, in the present study most patients with dMD suffered from stage 3 SNHL. Audiometric data from other studies showed that around half of the patients with dMD had stage 3 SNHL [8, 35]. Regarding patients with MC, a significant hearing impairment (stage 3 and 4) was found in more than one third of our cohort, of which a subset presented low- to medium frequency SNHL. A low-frequency air-bone-gap as noted in patients with dMD here was also reported before and is assumed to be a result of conductive dampening in the inner ear by endolymphatic hydrops [16, 23].
Fluctuating hearing loss has been acknowledged as a major supportive diagnostic criterion for MD [15, 18]. Though, we observed fluctuating hearing only in a fraction of even clinically certain cases (dMD), in line with an earlier study of Hoa and collaborators [15]. However, this conclusion is limited by unavailability of multiple audiograms in the majority of our patients, stressing the need for longer follow-up and regular audiometric assessment in patients with suspected MD. Dependent on the definition of fluctuation, Hoa and coworkers found audiometrically documented improvement in pure tone hearing over the time course of follow-up in 9–21% of 344 patients with definite MD according to the 1995 diagnostic criteria [15]. Another study, however, described an improvement of low-frequency hearing loss in up to 43.9% of their patients after 2 months [31]. Furthermore, hearing loss was reported to progress with the duration of the disease [1]. In our study, audiometrically documented fluctuating low- to medium-frequency SNHL was found in each category with some patients reporting permanent hearing impairment.
Major limitations of the present study are a small sample size and the lack of familial history. Clinical data from 337 [16], 488 [15] and even 1290 patients [26] has been published in recent years. While a more ambitious clinical work-up often limits sample size, large, and comprehensively characterized patient cohorts, ideally in a multicentric approach, are essential for further progress. A genetic contribution has been described in a subgroup of Menière cases [20]. Therefore, the omission of a structured evaluation of familial clustering is a drawback of our data and should also be addressed in subsequent analyses.
Following the observations of the present study, the current diagnostic criteria for MD allow to describe a high share of patients with MD. Still, a subset of patients presenting with a variation of menière-like symptoms and the exclusion of other causes remain without an adequate diagnosis. Therefore, review and development of the current understanding of the disease is required to account for the potentially heterogenic clinical picture of MD particularly in early stages.
5Conclusion
In this study we have investigated the sociodemography, disease characteristics, and audiologic data of patients with MD. This demonstrated the complexity of the disease and the differences between diagnostic categories. According to current diagnostic criteria for MD, many patients could be assigned to the canonic categories of dMD or pMD. A relevant share of patients, however, showed disease characteristics that were attributed to MD but did not meet current diagnostic criteria. Following our observations, a further development of the current diagnostic criteria is desirable. From a practical point of view, cautious follow-up, and repetitive audiometric testing aids diagnostic accuracy.
Acknowledgments
The authors are thankful to Thomas Brandt, Andreas Zwergal and coworkers for the establishment of the German Center of Vertigo and Dizziness. The meticulous work of technical and medical staff in routine patient care at the German Center of Vertigo and Dizziness, the Department of Neurology and the Department of Otorhinolaryngology is also highly appreciated. We are grateful to Joy Grimberg for assistance in statistical analyses.
Authorship contribution statements
FI designed analyses, analyzed data, and wrote the manuscript. IS acquired data, analyzed data, and wrote parts of the manuscript. JLS analyzed data, wrote parts of the manuscript, and provided critical review of the manuscript. DP and JM provided essential infrastructure, analyzed audiologic data, and provided critical review of the manuscript. RS performed statistical analysis, analyzed data, and provided critical review of the manuscript. EG provided essential infrastructure, designed experiments, and provided critical review of the manuscript.
Conflicts of interest and source of funding
This work was funded by grants to FI and EG by the German Federal Ministry of Education and Health (BMBF) in the context of the foundation of the German Center for Vertigo and Balance Disorders (DSGZ) (grant number 01 EO 0901). The authors declare no conflict of interest.
Supplementary material
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/VES-201634.
References
[1] | Albera R. , Canale A. , Cassandro C. , Albera A. , Sammartano A.M. and Dagna F. , Relationship between hearing threshold at the affected and unaffected ear in unilateral Meniere’s disease, European Archives of Oto-Rhino-Laryngology 273: (1) ((2016) ), 51–56. DOI:https://doi.org/10.1007/s00405-014-3466-8 |
[2] | Alexander T.H. and Harris J.P. , Current Epidemiology of Meniere’s Syndrome, Otolaryngologic Clinics of North America 43: (5) ((2010) ), 965–970. DOI: https://doi.org/10.1016/j.otc.2010.05.001 |
[3] | Atkinson M. , The Famous Four and the Critical Commentary,(Jan, Acta Oto-Laryngologica 53: (sup 162) (Jan. (1961) ), 14–65. DOI: https://doi.org/10.3109/00016486109121791 |
[4] | Basura G.J. , et al., Clinical Practice Guideline: Ménière’s Disease, Otolaryngology - Head and Neck Surgery (United States) 162: (2_suppl) ((2020) ), S1–S55. DOI: https://doi.org/10.1177/0194599820909438 |
[5] | Brandt T. , Zwergal A. , Jahn K. and Strupp M. , [Integrated Center for Research and Treatment of Vertigo, Balance and Ocular Motor Disorders], Nervenarzt 2009. |
[6] | Derebery M.J. and Berliner K.I. , Prevalence of Allergy in Meniere’s Disease, Otolaryngology–Head and Neck Surgery 123: (1) (Jul. (2000) ), 69–75. DOI: https://doi.org/10.1067/mhn.2000.105715 |
[7] | Van Esch B.F. , Van Benthem P.P.G. , Van Der Zaag-Loonen H.J. and Bruintjes T.J.D. , Jahn K. , Jahn K. , Jahn K. , Age of onset of Ménière’s disease in the Netherlands: Data from a specialised dizziness clinic, Journal of Laryngology and Otology 130: (7) ((2016) ), 624–627. DOI: https://doi.org/10.1017/S0022215116007982 |
[8] | Frejo L. , et al., Extended phenotype and clinical subgroups in unilateral Meniere disease: A cross-sectional study with cluster analysis, Clinical Otolaryngology 42: (6) ((2017) ), 1172–1180. DOI: https://doi.org/10.1111/coa.12844 |
[9] | Goebel J.A. , 2015 Equilibrium Committee amendment to the AAO-HNS guidelines for the definition of Méni-ère’s disease, Otolaryngology - Head and Neck Surgery (United States) 154: (3) ((2016) ), 403–404. DOI: https://doi.org/10.1177/0194599816628524 |
[10] | Grill E. , Müller T. , Becker-Bense S. , Gürkov R. , Heinen F. , Huppert D. , Zwergal A. and Strobl R. , DizzyReg: the prospective patient registry of the German Center for Vertigo and Balance Disorders, Journal of Neurology 264: (S1) (Oct. (2017) ), 34–36. DOI: https://doi.org/10.1007/s00415-017-8438-7 |
[11] | Harris J.P. and Alexander T.H. , Current-day prevalence of ménière’s syndrome, Audiology and Neurotology 15: (5) ((2010) ), 318–322. DOI: https://doi.org/10.1159/000286213 |
[12] | Harris P.A. , Taylor R. , Minor B.L. , Elliott V. , Fernandez M. , O’Neal L. , McLeod L. , Delacqua G. , Delacqua F. , Kirby J. and Duda S.N. , The REDCap consortium: Building an international community of software platform partners, Journal of Biomedical Informatics 95: (December 2018) ((2019) ), 103208. DOI: https://doi.org/10.1016/j.jbi.2019.103208 |
[13] | Harris P.A. , Taylor R. , Thielke R. , Payne J. , Gonza-lez N. and Conde J.G. , Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support,(Apr, Journal of Biomedical Informatics 42: (2) ((2009) ), 377–381. DOI: https://doi.org/10.1016/j.jbi.2008.08.010 |
[14] | Hietikko E. , Sorri M. , Männikkö M. and Kotimäki J. , Higher Prevalence of Autoimmune Diseases and Longer Spells of Vertigo in Patients Affected With Familial Ménière’s Disease: A Clinical Comparison of Familial and Sporadic Ménière’s Disease, American Journal of Audiology 23: (2) (Jun. (2014) ), 232–237. DOI: https://doi.org/10.1044/2014_AJA-13-0060 |
[15] | Hoa M. , Friedman R.A. , Fisher L.M. and Derebery M.J. , Prognostic implications of and audiometric evidence for hearing fluctuation in Meniere’s disease, Laryngoscope 125: December ((2015) ), S1–S12. DOI: https://doi.org/10.1002/lary.25579 |
[16] | Lee H.J. , Jeon J.H. , Park S. , Kim B.G. , Lee W.S. and Kim S.H. , Prevalence and clinical significance of spontaneous low-frequency air-bone gaps in Ménière’s disease, Otology and Neurotology 35: (3) ((2014) ), 489–494. DOI: https://doi.org/10.1097/MAO.0000000000000256 |
[17] | Levo H. , Kentala E. , Rasku J. and Pyykkö I. , Aural fullness in Ménière’s disease, neuro-otology 19: (6) ((2014) ), 395–399. DOI: https://doi.org/10.1159/000363211 |
[18] | Lopez-Escamez J.A. , et al. Diagnostic criteria for Menière’s disease,(Jan, Journal of Vestibular Research: Equilibrium and Orientation 25: (1) ((2015) ), 1–7. DOI: https://doi.org/10.3233/VES-150549 |
[19] | Lopez-Escamez J.A. and Attyé A. , Systematic review of magnetic resonance imaging for diagnosis of Meniere disease, Journal of Vestibular Research 29: (2–3) ((2018) ), 121–129. DOI: https://doi.org/10.3233/ves-180646 |
[20] | Lopez-Escamez J.A. , Batuecas-Caletrio A. and Bisdorff A. , Towards personalized medicine in Ménière’s disease,(Aug, F1000Research 7: (1295) ((2018) ), 1295. DOI: https://doi.org/10.12688/f1000research.14417.1 |
[21] | Monsell E.M. , Balkany T. , Gates G. , Goldenberg R. , Meyerhoff W.L. and House J.W. , Committee on Hearing and Equilibrium guidelines for the diagnosis and evaluation of therapy in Menière’s disease. American Academy of Otolaryngology-Head and Neck Foundation, Inc, Otolaryngology–head and neck surgery: official journal of American Academy of Otolaryngology-Head and Neck Surgery 113: (3) (Sep. (1995) ), 181–185. DOI: https://doi.org/10.1016/S0194-5998(95)70102-8 |
[22] | Monsell E.M. , Balkany T. , Gates G. , Goldenberg R. , Meyerhoff W.L. and House J.W. , Committee on Hearing and Equilibrium Guidelines for the Diagnosis and Evaluation of Therapy in Meniere’s Disease, Otolaryngology –Head and Neck Surgery 113: (3) (Sep. (1995) ), 181–185. DOI: https://doi.org/10.1016/S0194-5998(95)70102-8 |
[23] | Muchnik C. , Hildesheimer M. , Rubinstein M. and Arenberg I.K. , Low frequency air-bone gap in Meniere’s disease without middle ear pathology. A preliminary report, American Journal of Otology 1989. |
[24] | Pearson B.W. and Brackmann D.E. , Committee on Hearing and Equilibrium guidelines for reporting treatment results in Meniere’s disease, Otolaryngology–head and neck surgery: official journal of American Academy of Otolaryngology-Head and Neck Surgery 93: (5) ((1985) ), 579–581. DOI: https://doi.org/10.1177/019459988509300501 |
[25] | Perez-Carpena P. and Lopez-Escamez J.A. , Current Understanding and Clinical Management of Meniere’s Disease: A Systematic Review, Seminars in Neurology 40: (1) ((2020) ), 138–150. DOI: https://doi.org/10.1055/s-0039-3402065 |
[26] | Pyykkö I. , Nakashima T. , Yoshida T. , Zou J. and Nag-anawa S. , Ménière’s disease: a reappraisal supported by a var-iable latency of symptoms and the MRI visualisation of endolymphatic hydrops, BMJ Open 3: (2) (Feb. (2013) ), e001555. DOI: https://doi.org/10.1136/bmjopen-2012-001555 |
[27] | Sajjadi H. and Paparella M.M. , 2008. Meniere’s, disease, The Lancet. |
[28] | Shepard N.T. , Differentiation of Ménière’s disease and migraine-associated dizziness: A review, Journal of the American Academy of Audiology 17: (1) ((2006) ), 69–80. DOI: https://doi.org/10.3766/jaaa.17.1.7 |
[29] | Simo H. , Yang S. , Qu W. , Preis M. , Nazzal M. and Baugh R. , Meniere’s disease: importance of socioeconomic and environmental factors, American Journal of Otolaryngology 36: (3) (May(2015) ), 393–398. DOI: https://doi.org/10.1016/j.amjoto.2015.01.009 |
[30] | Tabet P. and Saliba I. , Meniere’s Disease and Vestibular Migraine: Updates and Review of the Literature, Journal of Clinical Medicine Research 9: (9) ((2017) ), 733–744. DOI: https://doi.org/10.14740/jocmr3126w |
[31] | Takahashi M. , Odagiri K. , Sato R. , Wada R. and Onuki J. , Personal Factors Involved in Onset or Progression of Ménière’s Disease and Low-Tone Sensorineural Hearing Loss, ORL 67: (5) ((2005) ), 300–304. DOI: https://doi.org/10.1159/000089412 |
[32] | Tyrrell J.S. , Taylor M.S. , Whinney D. and Osborne N.J. , Associations of Leg Length, Trunk Length, and Total Adult Height With Ménière’s, Ear and Hearing 36: (3) ((2015) ), e122–e128. DOI: https://doi.org/10.1097/AUD.0000000000000132 |
[33] | Tyrrell J.S. , Whinney D.J.D. , Ukoumunne O.C. , Fleming L.E. and Osborne N.J. , Prevalence, Associated Factors, and Comorbid Conditions for Ménière’s Disease, Ear and Hearing 35: (4) ((2014) ), e162–e169.DOI: https://doi.org/10.1097/AUD.0000000000000041 |
[34] | Wang Y. , Diao T. , Zhao Y. and Yu L. , The clinical characteristics and audiogram in 103 Meniere’s disease patients with and without vestibular migraine, Clinical Otolaryngology (2018) . |
[35] | Zhang Y. , Liu B. , Wang R. , Jia R. and Gu X. , Characteristics of the cochlear symptoms and functions in Meniere’s disease, Chinese Medical Journal 129: (20) ((2016) ), 2445–2450. DOI: https://doi.org/10.4103/0366-6999.191767 |
[36] | 1972. Committee on Hearing and Equilibrium. Report of Subcommittee on Equilibrium and its Measurement. Meniere’s disease: criteria for diagnosis and evaluation of therapy for reporting, Transactions - American Academy of Ophthalmology and Otolaryngology. American Academy of Ophthalmology and Otolaryngology 76: (6) ((1972) ), 1462–1464. |

