
Efficacy of serial casting protocols in idiopathic toe-walking
Abstract
OBJECTIVE:
Idiopathic toe-walking (ITW) is a diagnosis of exclusion. A relationship between ITW and decreased range of motion (ROM) is postulated. Treatments focus on increasing ankle dorsiflexion including serial casting. There is no consensus for duration of serial casting. This study aimed to determine ROM changes with cast change intervals of one vs. two weeks, and the rate of ITW recurrence.
METHODS:
This was a retrospective study of 86 patients, ages 0–9 years with ITW undergoing weekly casting (N = 29) and two-week casting (N = 57) at a children’s hospital from 2014–2020. ROM at baseline, two weeks, four weeks, and final cast removal were collected. Statistical analyses included chi-squared tests, two-sample t-tests, and linear mixed regression. Outcome distributions were assessed for normality. P-values < 0.05 were considered statistically significant.
RESULTS:
After adjusting for baseline ROM, the mean change in ROM from baseline to two weeks was 10.6∘ vs 7.5∘ in the one-week vs. two-week casting interval, respectively (p < 0.001). The baseline to final measurement was 13.4∘ vs 9.8∘ in the one-week vs. two-week casting interval, respectively (p < 0.001). The rate of recurrence of ITW was similar between the two groups.
CONCLUSION:
This study suggests greater improvement in ROM in the one-week vs. two-week casting interval group.
1Introduction
Idiopathic toe-walking (ITW) is a common reason for referral to outpatient pediatric rehabilitation medicine (PRM) clinics. It is defined as the inability to generate a heel strike during the initial contact phase of the gait cycle and the absence of full contact during the entire standing phase [1, 2]. This is a gait pattern that can be observed in healthy typically developing children less than two years old who are learning to walk [1–3].
ITW is a diagnosis of exclusion with a prevalence of 5% within the healthy childhood population [1, 4, 5]. These children will typically have a history of normal birth, normal development, normal neurological and orthopedic status, and no prominent neuropsychiatric disorders [1]. Other diagnoses that can manifest toe-walking as a symptom include, but are not limited to, cerebral palsy, traumatic brain injury, tethered spinal cord, and autism/pervasive development disorder (PDD) [5, 6]. These diagnoses are important to rule out.
It has been postulated that there is a relationship between ITW and decreased range of motion (ROM) at the ankle [1]. Left untreated, this can cause difficulties such as inefficient gait, falling, pain, and foot deformities [1, 5]. Due to the apparent relationship between ITW and reduced ankle ROM, treatments have focused on increasing available ankle dorsiflexion with the aim of encouraging heel contact during gait [1, 7]. These treatments have included watchful waiting, stretching, serial casting, botulinum toxin A injections, orthoses, motor control strategies, or surgery [1, 4, 8, 9].
One of the most common and popular treatments available for ITW is a course of serial casting with studies showing improvement in dorsiflexion range [1, 5, 9]. However, at this time, there is no clear consensus guideline for duration of serial casting or appropriate cast-change intervals for maximum benefit. Currently at the authors’ institution, cast changes are either weekly or every two weeks for a duration of 2–6 weeks. The purpose of this study was to determine if there is greater ROM improvement based on casting intervals of one vs. two weeks in idiopathic toe-walkers. The researchers hypothesized that changing casts with a weekly interval would result in more rapid improvement in ROM at the ankle when compared to patients who had their casts changed every two weeks. The study also evaluated the rate of recurrence of toe-walking between the groups.
2Methods
This was a retrospective study of children, ages 0–9, who underwent treatment for ITW at a single tertiary pediatric hospital from 2014–2020. Institutional review board (IRB) approval was obtained for this study. Upon IRB approval, a list of all children ages 0 –9 years who presented to the PRM clinic from January 1, 2014, to December 31, 2020, with a chief complaint of toe-walking was generated using the electronic medical record. This list was sent to the hospital’s Research Administration who determined which patients had opted out of the use of their records in research. Those who had opted out were excluded from this study.
The patients included in this study met the following criteria: children ages 0–9 years who presented to the PRM clinic from January 2014–December 31, 2020, with a chief complaint of idiopathic toe-walking who were independent ambulators by 18 months of age and underwent a course of serial casting at the ankle to improve ROM. The diagnosis was confirmed by a thorough history and physical examination by the pediatric physiatrist. If there was any uncertainty about the diagnosis, a referral was made to pediatric neurology and additional diagnostic testing was undertaken as indicated including MRI and/or genetic testing.
Casts were short leg, fiberglass (hard) casts applied by experienced cast technicians. The cast technicians received training on lower extremity casting and worked on bringing the foot to a subtalar neutral position prior to trying to correct equinus. Casts remained in place until return to clinic when they were removed, skin inspected, and new casts applied as deemed appropriate by the provider. Patients were excluded if they met any of the following exclusion criteria: known neurological or psychological diagnosis including cerebral palsy, spina bifida, neuropathy/myopathy, autism/PDD, attention deficit hyperactivity disorder, arthrogryposis, acquired brain injury, or tethered or borderline tethered cord. A history of bone issues including excessive femoral anteversion, internal tibial torsion, external tibial torsion, or fibular hemimelia was also an exclusion criterion. Patients who had previous treatments including botulinum toxin injections or serial casting paired with botulinum toxin injections were also excluded. Finally, patients were excluded if they did not have their ROM collected at the specific study timepoints or present for their cast changes within three days of their weekly or every two-week cast changes.
A systematic electronic chart review was completed. The data extracted from the chart included the following: age, sex, date of birth, diagnosis, ankle ROM with knee extended (baseline, intervals, and final), duration of casting, casting interval, previous treatments, family history of toe-walking, orthotic prescription, subjective pain report complaint, percentage of time toe-walking, and recurrence of toe-walking after treatment. Recurrence of toe-walking was defined as the patient being up on their toes for ambulation greater than 25% of the time as estimated by family/caregiver.
There were two groups in this study. Both groups had ROM documented at baseline, at the time of each cast change, and at the time of final cast removal. The first group included participants who had cast changes in weekly intervals for a maximum duration of four weeks, The second group included participants who had cast changes every two weeks for up to six weeks. Frequency of cast change and when to terminate serial casting was determined by the treating pediatric physiatrist. Termination of casting was due to either sufficient ROM being obtained or a lack of response to casting.
2.1Statistical analysis
Participant demographics and characteristics were summarized using descriptive statistics (means and standard deviations for continuous variables and counts and proportions for categorical variables). Comparisons in demographics and baseline characteristics between the weekly casting interval group vs. every two weeks casting interval group were performed using chi-squared tests for categorical data and two-sample t-tests for continuous data. Baseline characteristics that were statistically different between the two groups were adjusted using regression models. The length of time that each participant was casted was analyzed in order to understand the variation in the timing of the final time point. Wide variations in the length of time for final time point were normalized by using the percent of total length of treatment instead of the number of weeks of treatment. Histograms and Q-Q plots were used to determine normality of the sample data sets. Nonparametric methods were considered if the outcome was not normally distributed. Three linear regression models were built to evaluate changes in ankle ROM for each group over three intervals: (1) baseline to two weeks, (2) two weeks to four weeks, and (3) baseline to each participant’s final measurement. All models included fixed effects for week, group, and group * week and a random intercept for ankle and a nested random intercept for ankle within participant. All models were adjusted to account for intergroup differences in baseline ROM. For each model, the average ROM (mean and standard deviation) at each time point and the change in ROM between time points, separated by study group, is reported. Additionally, to investigate the effect of time while holding the number of cast changes constant, comparison was made of the ROM improvement at two weeks for the group who had casting intervals of one week vs. the ROM improvement at four weeks for the group who had casting intervals of two weeks using a linear mixed regression model with a random intercept for participant. Also, the rate of recurrence of toe-walking between the groups was analyzed. SAS v.9.4 (SAS Institute Inc., Cary NC) was used for analysis. P-values<0.05 were considered statistically significant.
3Results
A total of 86 patients (169 ankles) who met inclusion criteria were included in this study. Patients were categorized into two groups based on their treatment: 29 patients (55 ankles as three patients had unilateral contractures) in the one-week casting interval group, and 57 (114 ankles) patients in the two-week casting interval group.
Table 1 presents the patients’ demographic data and baseline characteristics. The mean age was similar between the groups. The baseline ROM was more contracted in the one-week interval group (–5.4∘) compared to the two-week interval group (1.4∘). Baseline pain levels, family history of toe-walking, percentage of time toe-walking, previous casting, orthotics, and physical therapy were similar in both groups.
Table 1
Patients’ demographics and baseline characteristics
| One-week casting interval (n = 29 participants; 55 ankles) | Two-week casting interval (n = 57 participants; 114 ankles) | p-value | |||
| Mean | SD | Mean | SD | 0.213 | |
| Age | 5.07 | 2.12 | 5.63 | 1.89 | |
| Initial range of motion per ankle (degrees) | –5.4 | 1.1* | 1.4 | 0.8* | <.001** |
| Gender | n | % | n | % | 0.879 |
| Male | 11 | 37.93 | 24 | 42.11 | |
| Female | 18 | 62.07 | 32 | 56.14 | |
| Non-binary | 0 | 0.00 | 1 | 1.75 | |
| Pain complaint | |||||
| Yes | 13 | 50.00 | 18 | 33.96 | 0.260 |
| No | 13 | 50.00 | 35 | 66.04 | |
| Family history of toe-walking | |||||
| Yes | 13 | 50.00 | 23 | 40.35 | 0.559 |
| No | 13 | 50.00 | 34 | 59.65 | |
| Percentage of time toe-walking | |||||
| 0–24% | 0 | 0.00 | 1 | 2.38 | 0.760 |
| 25–49% | 0 | 0.00 | 2 | 4.76 | |
| 50–74% | 3 | 15.00 | 8 | 19.05 | |
| 75–100% | 17 | 85.00 | 31 | 73.81 | |
| Previous casting per participant | 1 | 3.45* | 5 | 8.77* | 0.659 |
| Previous orthotics per participant | 1 | 3.45* | 9 | 15.79* | 0.154 |
| Previous PT per participant | 12 | 41.38* | 11 | 19.30* | 0.054 |
*Standard Error; **p-value from generalized linear mixed model with a random intercept for participant. PT = Physical therapy; SD = Standard deviation.
Table 2 presents the changes in the ROM between the one-week casting and two-week casting groups at three intervals. The average ROM increased across time in both groups. The amount of ROM improvement from two weeks to four weeks was the same between the two groups (approximately 5∘); however, the ROM improvement was higher in the one-week casting interval group from baseline to two weeks (p = 0.001) and baseline to final measurement (p < 0.001). This remained true after adjusting for the baseline ROM (Fig. 1).
Table 2
Degrees of range of motion (ROM) improvement by group after adjusting for baseline ROM
| Start point | End point | Change | p-value change* | p-value group* | |||||
| Group | Mean | SD | Mean | SD | Mean | SD | |||
| Model one (baseline to two weeks) | Weekly cast change | –2.0 | 0.6 | 8.7 | 0.6 | 10.6 | 0.8 | <0.001 | 0.001 |
| Every other week cast change | –0.4 | 0.4 | 7.1 | 0.4 | 7.5 | 0.5 | <0.001 | ||
| Model two (two weeks to four weeks) | Weekly cast change | 6.6 | 0.8 | 12.0 | 1.2 | 5.5 | 1.2 | <0.001 | 0.766 |
| Every other week cast change | 7.5 | 0.5 | 12.5 | 0.9 | 5.0 | 0.9 | <0.001 | ||
| Model three (baseline to final measurement) | Weekly cast change | –2.6 | 0.6 | 10.8 | 0.6 | 13.4 | 0.8 | <0.001 | <0.001 |
| Every other week cast change | –0.1 | 0.4 | 9.7 | 0.4 | 9.8 | 0.5 | <0.001 | ||
*p-values are from generalized linear mixed models with a random intercept for ankle as well as a nested random intercept for ankles within participants [ankle, ankle(participant)]. SD = Standard deviation.
Fig. 1
Degrees of range of motion (ROM) improvement by group after adjusting for baseline ROM.
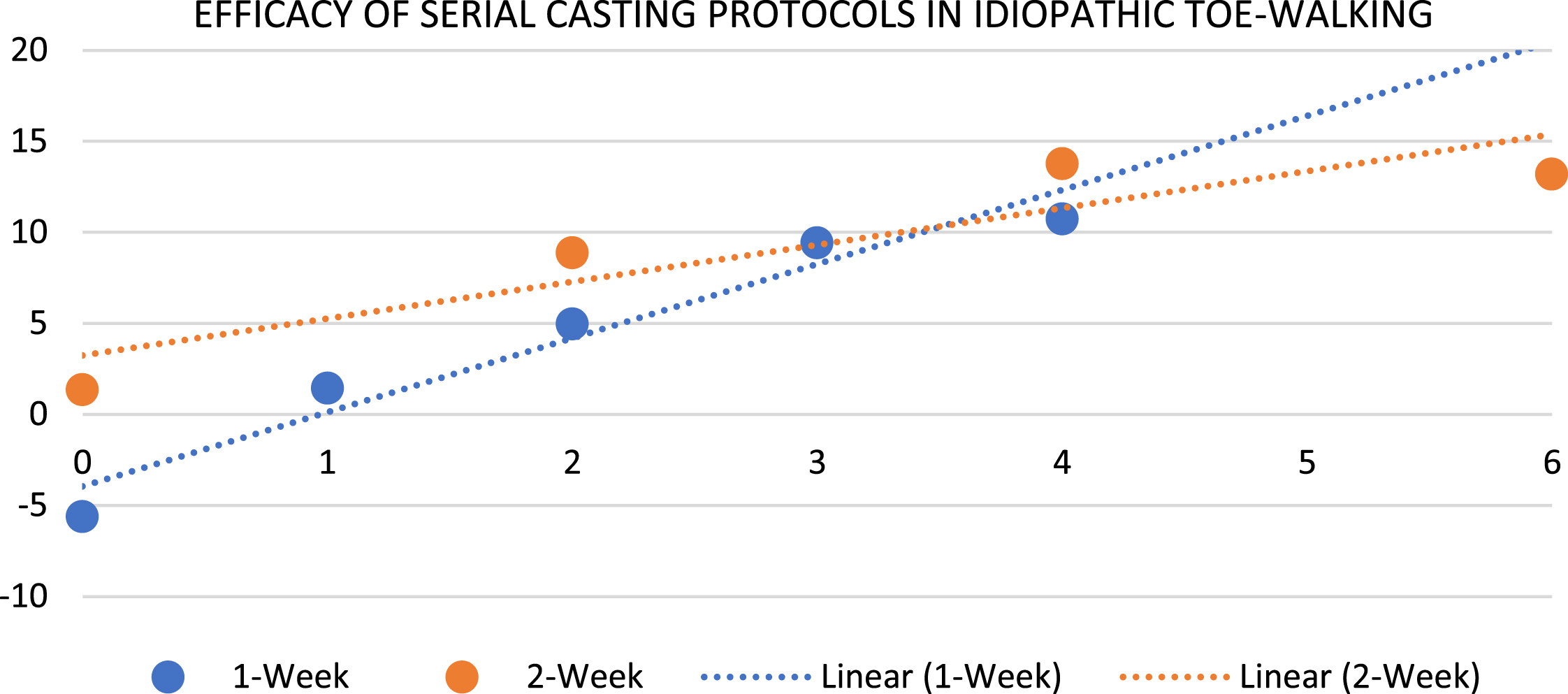
Table 3 presents the rate of recurrence of toe-walking between the groups. The rate of recurrence was 33% in the one-week casting group and 29% in the two-week casting group, respectively (p = 0.909). Time to recurrence was variable, as short as two months and as long as two years. Eight participants in each group were lost to follow-up (did not return after final cast removal).
4Discussion
This study evaluated the efficacy of different serial casting regimens on increasing ROM in children with equinus contractures due to ITW. Historically, numerous treatment modalities have been utilized, including stretching, botulinum toxin injections, physical therapy, serial casting, or surgeries [1, 4, 8, 9].
This study focused on serial casting with either weekly cast changes or cast changes every two weeks. The weekly cast change group had greater improvement in their available range at both initial to two weeks (10.6∘ vs 7.5∘) and initial to final measurements (13.4∘ vs 9.8∘). There was no significant difference in the two-week to four-week time period, approximately 5∘ for both regimens. While the one-week interval casting group did start with a greater limitation to ROM when compared to the two-week interval group, when adjusting for initial ROM, the difference was maintained.
There are no other studies at this time comparing serial casting regimens; therefore, results are difficult to compare.
Table 3
Rate of recurrence
| One-week casting interval | Two-week casting interval | p-value | |||
| (n = 21 participants+) | (n = 49 participants+) | ||||
| n | % | n | % | 0.909 | |
| Rate of recurrence | 7 | 33.33 | 14 | 28.57 | |
+Missing, n = 8 in each group.
While demographics between the two groups were similar, participants in the one-week interval casting group did start with a more limited ROM than their counterparts in the two-week interval casting group. The greater contractures may have predisposed clinicians to a more frequent cast change regimen than for their counterparts. The one-week interval group also had more potential ROM to gain due to the worsened contractures.
There are several limitations in this study. Overall, there was a small one-week interval casting group, and both groups had a small two-to-four-week follow-up population, which reduced the power of the study. As the study was retrospective, missing documentation, particularly ROM assessments, hampered data collection and was a limitation. Also, assessments were performed by a variety of providers, increasing risks for error. Likewise, there was not a standard serial casting protocol and decisions were made based on the clinical judgement of the various treating pediatric physiatrists. Eight participants in each of the groups did not return for follow-up. This could have been due to either satisfaction or dissatisfaction with casting outcome. Use of a standardized protocol, such as that described by Zapata et al. [10], and a prospective approach would strengthen this type of study.
In conclusion, this study validated that serial casting improves ROM at the ankle in ITW, regardless of serial casting regimen. Further, greater and faster ROM improvements were seen in a weekly cast change regimen as compared to cast changes every two weeks, but only for the first two weeks.
Acknowledgments
This study was supported by Gillette Children’s Foundation. A special thank you to Mark Jankowski for his assistance with data quality checks.
Declaration of interest
The authors have no conflicts of interest to report.
Ethical considerations
IRB approval with a waiver of informed consent was obtained from the University of Minnesota IRB (ID: STUDY00013192).
References
[1] | van Kuijk AA , Kosters R , Vugts M , Geurts AC . Treatment for idiopathic toe walking: a systematic review of the literature. J Rehabil Med. (2014) ;46: (10):945–57. doi: 10.2340/16501977-1881. |
[2] | Brouwer B , Davidson LK , Olney SJ . Serial casting in idiopathic toe-walkers and children with spastic cerebral palsy. J Pediatr Ortho. (2000) ;20: (2), 221–225. |
[3] | Herrin K , Geil M . A comparison of orthoses in the treatment of idiopathic toe walking: A randomized controlled trial. Prosthet Orthot Int. (2016) ;40: (2):262–269. doi: 10.1177/0309364614564023. |
[4] | Williams CM , Gray K , Davies N , et al.Exploring health professionals’ understanding of evidence-based treatment for idiopathic toe walking. Child Care Health Dev. (2020) ;46: (3):310–319. doi: 10.1111/cch.12745. |
[5] | Caserta AJ , Pacey V , Fahey M , Gray K , Engelbert RH , Williams CM Interventions for idiopathic toe walking. Cochrane Database Syst Rev. (2019) ;10: (10):CD012363.doi: 10.1002/14651858.CD012363.pub2. |
[6] | Hicks R , Durinick N , Gage JR. Differentiation of idiopathic toe-walking and cerebral palsy. J Pediatr Ortho((1988) ;8: (2), 160–163. |
[7] | Michalitsis J , Murphy AT , Rawicki B , Haines TP , Williams C . Full length foot orthoses have an immediate treatment effect and modify gait of children with idiopathic toe walking. Gait Posture. (2019) ;68: 227–231. doi: 10.1016/j.gaitpost.2018.11.022. |
[8] | Davies K , Black A , Hunt M , Holsti L . Long-term gait outcomes following conservative management of idiopathic toe walking. Gait Posture. (2018) ;62: 214–219. doi: 10.1016/j.gaitpost.2018.02.014. |
[9] | Thielemann F , Rockstroh G , Mehrholz J , Druschel C . Serial ankle casts for patients with idiopathic toe walking: effects on functional gait parameters. J Child Ortho. (2019) ;13: (2):147–154. doi: 10.1302/1863-2548.13.180183. |
[10] | Zapata KA , Trevino ME , Reyes FI , Jo CH , Sharmas C . Adherence to serial casting protocols for idiopathic toe walking: A quality improvement project. J Pediatr Rehabil Med. (2022) ;15: (3):469–476. doi: 10.3233/PRM-210054. |


