
Non-immersive virtual reality based treatment for children with unilateral cerebral palsy: Preliminary results
Abstract
PURPOSE:
Unilateral cerebral palsy (UCP) represents about 30–40% of overall cerebral palsy diagnoses. Upper limb impairment has a significant negative impact on activities of daily living (ADL), and recent studies have shown that the use of virtual reality (VR) can increase motivation and promote an improvement in ADL. This preliminary study was aimed at exploring the acceptability and usability of a VR rehabilitation treatment, using the VITAMIN Platform, for children with UCP. A secondary goal of the study was to compare the results of usual standardized clinical scales and questionnaires with kinematic results as well as with the quantitative measures acquired by the VITAMIN platform in each exercise of the rehabilitation sessions.
METHODS:
Six children with UCP (aged 7–15) were recruited for a preliminary investigation in using a non-immersive VR system. The treatment was composed of 10 weekly sessions of 45 minutes. Each child played five types of exergames, using the impaired upper limb to hit virtual objects projected on a wide screen. Standardized clinical scales, kinematic analysis, and questionnaires were used to extensively assess upper limb function before and at the end of treatment. Five typically-developing children provided a reference for the instrumented kinematic assessment.
RESULTS:
At the end of the treatment, Melbourne Assessment 2 (MA2) scores increased for all the participants (mean increase in range of movement (ROM) + 19.1%, accuracy + 4.6%, dexterity + 13.1%, fluency + 10.3%). Shoulder flexion-extension ROM also improved (mean increase + 10.5°), and according to the kinematic analysis, shoulder movements became more similar to reference profiles. These results were confirmed by a general improvement in performing ADL, assessed by the ABILHAND-Kids questionnaire. Finally, a general agreement among the different measures and indexes emerged from the acquired data.
CONCLUSION:
The results show that VR treatment with the VITAMIN platform could be engaging and functional for rehabilitation of children with UCP. The good agreement among the qualitative and quantitative measures and indexes confirms the potential of such novel treatment. However, due to the limited sample size and small number of sessions, further and larger investigations are required to evaluate the effectiveness and to generalize the results.
1Introduction
Cerebral palsy (CP) is one of the most common causes of childhood disability in high-income countries, with a prevalence around 0.2% per live births in the USA [1] and around 0.16% in Europe [2]. The unilateral forms (unilateral cerebral palsy –UCP), with exclusive or prevalent impairment of one side of the body, represent about 30–40% of the overall population with CP [3]. In UCP, upper limbs are typically more affected, and the resulting impairment has high negative impacts on activities of daily living (ADL) and thus on overall quality of life [4, 5].
CP rehabilitation treatments aim at promoting adaptive strategies through the enhancement of motor, psychomotor, and cognitive functions. Being repetitive, motor rehabilitation exercises may be perceived as boring, especially by children, with the possible consequence of reduced adherence to treatment [6]. Emotional involvement plays a key role in promoting participation in rehabilitation activities. The presence of auditory and visual stimuli and especially the design of games can increase motivation and engagement [7–9]. Motivation in particular is crucial as a functional neuroplasticity modulator [10–12]. Neural reorganization occurs at the cortical level and depends upon different factors such as development, degree of damage, treatments, and the environment.
In order to maximize patients’ compliance during an entire rehabilitation session, recent studies have highlighted the importance of motivation, participation, and active involvement through better engagement and innovative playful activities, like exergames [13].
The need to enrich motor rehabilitation with motivating proposals through the use of augmented or virtual reality (VR) has also been widely discussed in the most recent literature [14]. Motivation appears to be a critical factor in motor learning [15], and it is considered the only individual characteristic not related to health conditions that may influence motor changes and functional outcomes. On the contrary, the lack of motivation could limit children’s learning and maximum functional potential [16]. Novel computer-based technologies, like active videogames or VR, may help to increase motivation [17]. In recent years, clinicians and therapists have increasingly used VR as a rehabilitation method to improve motor, neuromotor, and cognitive performance in children with CP [16, 18].
Some studies have already investigated the use of off-the-shelf gaming consoles, especially the Nintendo Wii platform, providing some evidence about improvements in upper limb movements and in ADL in children with UCP [19, 20].
The use of interactive video games associated with VR has shown promising results in the improvement of motor control of the upper limbs [21]. A case report has described a cortical reorganization at the level of the primary motor cortex with an activation of different cortical areas before and after treatment; this case used a custom semi-immersive VR tool (IREX-VR) on a large screen in a hospital setting for the rehabilitation of a child with CP [22]. Other studies, investigating the effectiveness of VR in children with CP, have shown some improvements in ambulation, postural control, and arm function. At the same time, further research is mandatory to fully understand the potential and limitations of treatments based on this technology [9, 23–27].
Custom-made VR systems may lead to better results than off-the-shelf videogame consoles, for two main reasons. Firstly, they could be carefully adapted to a child’s specific capabilities and rehabilitation goals [12]. Secondly, quantitative measures gathered while performing the rehabilitation activities can be used to assess the rehabilitation process. Moreover, these are quantitative subject-specific data which are usually more objective than typical clinical evaluations that may be affected by the operator’s biases.
For these reasons, a non-immersive VR system was designed and developed at the Child Neuropsychiatry and Rehabilitation unit of the S.M. Nascente center, in Milano (Italy). The system consists of a software platform (Virtual realITy plAtform for Motor and cognItive rehabilitatioN - VITAMIN) and a lab for technologically-assisted rehabilitation, called CARE (Computer Assisted REhabilitation) Laboratory [28] (Fig. 1). During the design phase of the lab, the team took into account the importance of an interactive and engaging environment, as well as the importance of avoiding two negative effects: cyber sickness [29] and potential detachment from the real world and the therapist due to immersive VR experiences (i.e., head mounted devices –HMD). Thus, a non-immersive VR approach was preferred. Hence in the lab, a large screen covers a good amount of the child’s visual field, with suitable panels on the remaining walls painted with the same graphical elements used by the software platform (Fig. 1).
Fig. 1
Pictures of CARE Lab (left) and of a child playing the Bubble 1 game (right).

The main aim of this study was to explore the acceptability and usability of a novel rehabilitation treatment of UCP, based on the use of a previously developed VR software platform (VITAMIN). Moreover, the quantitative measures collected during the rehabilitation sessions by VITAMIN were compared to clinical and instrumental assessments. Clinical scales and questionnaires were carefully selected in order to measure body functions, capacity, and performance in the child’s typical environment, as suggested by the current International Classification of Functioning, Disability and Health framework [30].
2Materials and methods
2.1Participants
Participants were selected among patients with UCP who were receiving conventional neuromotor rehabilitation treatments at the Child Neuropsychiatry and Rehabilitation Unit of the S.M. Nascente center, Fondazione Don Carlo Gnocchi (Milano, Italy). The inclusion criteria were UCP diagnosis and age between five and 18 years, while exclusion criteria were cognitive impairment, signs of severe hypoacusia or hypovision, and botulinum neurotoxin (BoNT) injections or surgical treatments in the previous six months. All participants’ caregivers gave their informed consent for the study.
Six children with UCP, five males and one female, aged between seven and 15 years (Table 1), were enrolled in the treatment group. All children were classified Level I according to the Gross Motor Function Classification System [31]; according to the Manual Ability Classification System, two children were assessed Level II and four Level III [32].
Table 1
Demographic information about the children involved in the present study.
| Participant ID | 1 | 2 | 8 | 3 | 11 | 6 |
| Sex | M | M | F | M | M | M |
| Age in years | 11 | 10 | 8 | 11 | 15 | 10 |
| Side of motor impairment | Left | Right | Left | Right | Right | Right |
| GMFCS | I | I | I | I | I | I |
| MACS | II | III | III | II | III | III |
F = female; GMFCS = Gross Motor Function Classification System; M = male; MACS = Manual Ability Classification System.
2.2Clinical assessment
The clinical assessment included the following evaluations.
Melbourne Assessment 2 (MA2) scale: The MA2 is a widely used and reliable tool [33] for evaluating the quality of upper limb function. Another index called the MA2 Incremental Percentage Index (MA2-IPI) was derived from the MA2 scale results, to help compare the changes in MA2 scores among different patients, expressed in percentage over the reachable maximum. MA2-IPI was thus calculated as the percentage of the actual increment in the MA2 score at T1 (post-training) with respect to the score at T0 (baseline), over the greatest possible score increment. As an example, if the score at T0 is 65% for a given MA2 item and at T1 it is 84%, the difference in MA2 scores would be 19% (84% –65%), while the MA2-IPI score would be 54.3% ((84% –65%) / (100% –65%)). This index allowed for a comparison of differences in MA2 percentages that better assessed the actual improvement with respect to the maximum possible one (100%).
Modified Ashworth Scale (MAS): The MAS is a clinical scale designed to evaluate spasticity. During administration, the examiner passively moves the joint being tested and rates the perceived level of resistance in the muscle groups opposing the movement. This scale consists of a single-item measure, ranging from zero to four, where zero indicates no increase in muscle tone and four indicates that the affected part is rigid in flexion or extension [34].
Passive and active joint range of motion (PROM – AROM): A manual goniometer was used to evaluate the PROM-AROM of the arm.
ABILHAND-Kids scale: Caregivers were requested to complete the ABILHAND-Kids scale, which consists of qualitative evaluations regarding a set of bimanual daily activities that may or may not be performed by the child, scoring 0 if the action is impossible, 1 if it is difficult, and 2 if it is simple to perform [35].
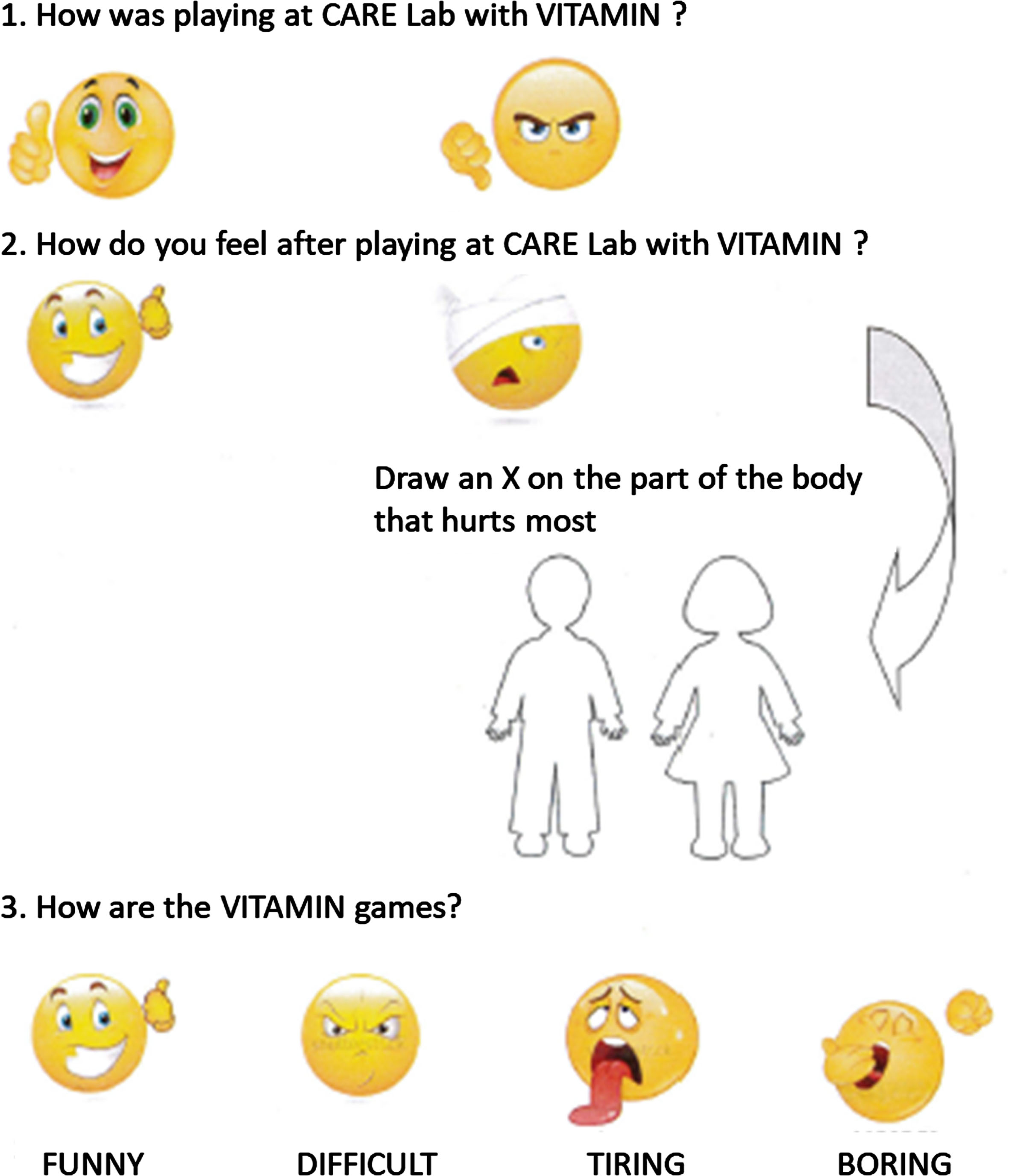
Patient satisfaction questionnaire: At the end of each VR session, each child was asked to fill in a satisfaction questionnaire (Fig. 2). This consisted of three main questions (“How was playing at CARE Lab with VITAMIN ?”, “How do you feel after playing at CARE Lab with VITAMIN ?”, “How are the VITAMIN games?”). Children could choose among simplified answers by drawing a sign on the corresponding “emoticon” (Fig. 2), and multiple choices were allowed. Alongside the second question, the questionnaire presented a simplified sketch of a human body, which participants could use to indicate part(s) of the body where they experienced any discomfort or pain. These graphical elements (the emoticons and the simplified sketch of the body) also allowed those children who could not read or write to express their opinions about the session.
Fig. 2
The satisfaction questionnaire used to collect feedback from children after each session. Please note that the figure reports the English translation of the original Italian version that was actually administered.
All the measures and the results of the scales were stored, analyzed, and plotted using Excel (Microsoft Corp., Redmond, WA, USA).
2.3Instrumental assessment
Upper limb kinematics were acquired in the Movement Analysis Laboratory in the S.M. Nascente center using a nine-camera optoelectronic system (SMART-DX, BTS, Italy) with a sampling frequency of 200 Hz, as it is the most common method used for motor function assessment in cerebral palsy [36]. The system measured the three-dimensional (3D) coordinates of nine spherical markers (15 mm diameter) placed on the following body landmarks: C7, manubrium, right and left acromion, lateral humeral condyle, mid-arm, ulnar and radial styloid processes, and hand of the tested limb. The markers’ 3D coordinates were low-pass filtered at 6 Hz and then used to compute shoulder and elbow angles according to the joint coordinate system method [37]. Articular range of motion (ROM) of the flexion-extension of the elbow, of the adduction and abduction on the frontal plane of the shoulder, and of the flexion-extension of the shoulder were hence calculated. All participants were asked to perform activities according to two items of the MA2 scale (Item 1: “Reach forward” and Item 10: “Reach to Brush from Forehead to Back of Neck”), repeating the actions five times. The average trajectory was then taken into consideration. These items relate to ADL and have different degrees of difficulty: low for item 1, and high for item 10. The entire procedure was repeated at T1 to assess the effects of VITAMIN-based rehabilitation on functional tasks.
A sample of five typically-developing children (four males and one female aged between six and 15 years), without musculoskeletal or neurological disorder, provided reference data related to joint kinematics. They performed the same MA2 scale items and were considered the control group for the instrumental kinematic assessment. From this control group, a reference set of measures was derived regarding the articular joints’ range and the motor strategies performed.
Pearson coefficients between the MA2 scores of each item and the similarity indexes between children with CP and those with typical development was calculated with MATLAB (The MathWorks Inc., Natick, MA, USA).
A correlation analysis was also performed to assess the relationship between the kinematic analysis and the MA2 scale and ABILHAND-Kids scores.
After analyzing the data of each child, the mean values of the elbow (flexion / extension) and shoulder (flexion / extension and abduction / adduction) curves were calculated for the two items considered (MA2 Item 1 and Item 10).
2.4VITAMIN measures
VITAMIN is a medical grade software, designed and built by Fondazione Don Carlo Gnocchi. It is composed of three software modules (Sensor Interface, Control Hub and Game Engine) developed in C#.NET, Python, and 3D graphical engines (Unreal Engine and Unity 3D) for the three modules respectively. For more details about the platform and the lab, see Olivieri et al. [28].
One of the advantages of computer-based rehabilitation activities is the intrinsic availability of quantitative data about the movements performed by the patient during the proposed exercises. As an example, the continuous recording of the virtual hand’s position during each game allows for both the reconstruction of the whole trajectory and the derivation of specific quantitative indexes. Among the several measures acquired by VITAMIN, this study focused on the virtual hand’s two-dimensional (2D) trajectory length (in pixels), describing the movements performed by the child during the 10 sessions.
An “efficiency index” related to the trajectory of the hand in each game was also calculated. The sum of the distances between the subsequent targets hit (i.e., the shortest path the user could follow to reach all the targets; T) was divided by the overall length of the trajectory (i.e., the sum of the distances between two subsequent points on the screen; l), thus T/l. Given that N equaled the number of targets hit and M the number of points of the sampled trajectory on the screen, the efficiency was calculated according to the following formula:
As an example, looking at Fig. 3, the efficiency can be calculated as
Fig. 3
A simple example of the efficiency index.
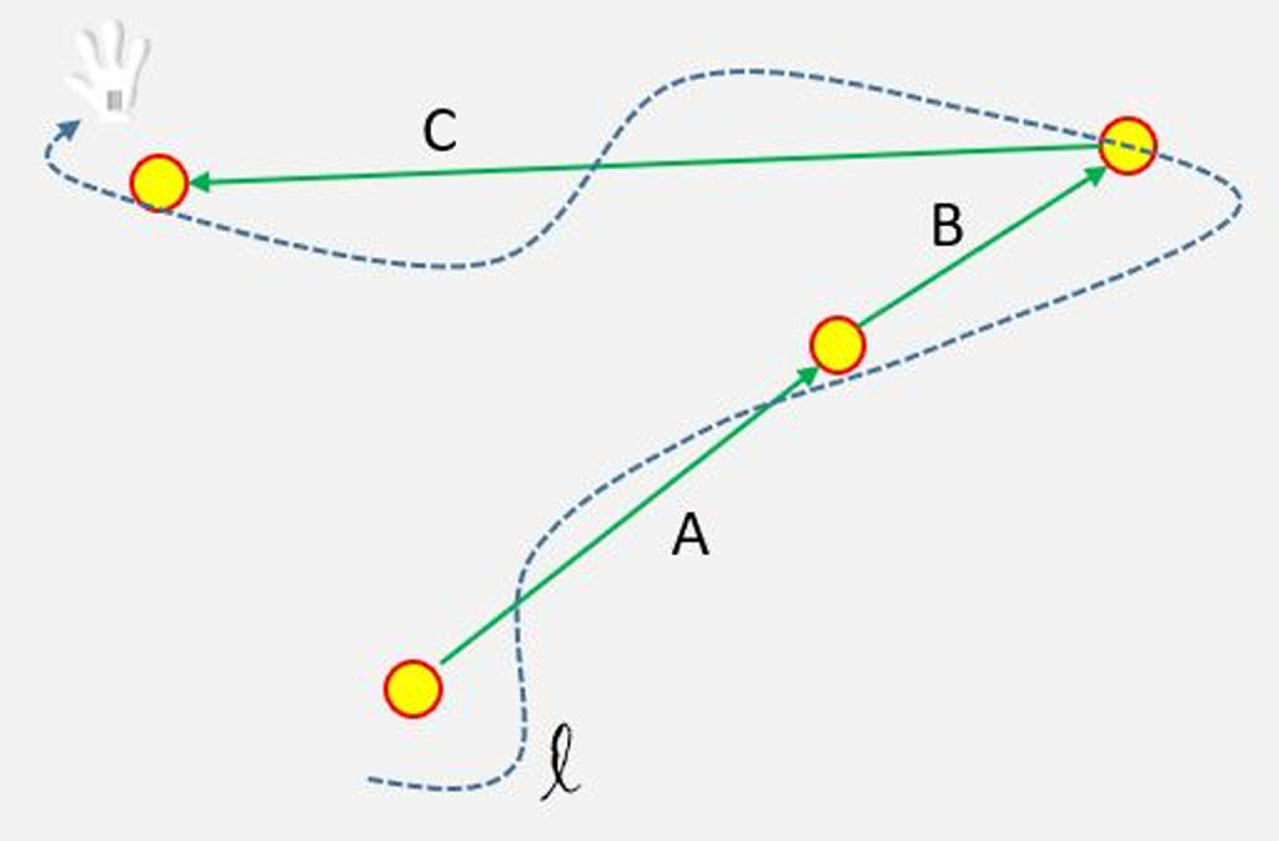
This index is close to 1.0 when the trajectory of the virtual hand gets closer to the shortest path T (i.e., when the patient’s movements are better aimed at hitting the sequence of targets without wandering). Otherwise, the more the trajectory l differs from the shortest path T (i.e., the patient’s movements are less oriented to hitting the sequence of targets), the closer it is to 0.0.
2.5Equipment
Within CARE Lab, VITAMIN ran on a high performance workstation Lenovo P500 ThinkStation equipped with an Intel Xeon E5-1660 v3 processor, 32 GB RAM, and a dedicated NVIDIA GTX 980 with 4 GB VRAM graphic card. The workstation was located in a separate room, and the Microsoft Kinect v2.0 used to acquire limb position was connected to the workstation through an Icron Spectra 3001-15 USB 3.0 cable, to ensure a smooth acquisition. The workstation was oversized on purpose, to ensure that all the data processing could be performed in real time without affecting the user experience (e.g., with long processing delays or discontinuous movements). This was mandatory for the games to be fluent and responsive, which is fundamental for a satisfactory and engaging user experience for the children. With the given hardware, the current version of VITAMIN, using Microsoft Kinect v2 as input device, usually has a load of less than 20% of the processor and less than 20% of RAM.
The images of the games were projected on a screen 4 m (width) x 2.75 m (height), by a laser projector Sony VPL-FHZ55 equipped with a short-throw lens Sony VPLL-Z2009 (throw ratio 0.85–1.0 : 1). A couple of standard Sony VPL-EX235 projectors were used to project some cue images on the ground (in particular, the position where the child should stand during the activities). The audio for the games was produced by an internal sound board (Asus Essence STX II 7.1), a high-end Yamaha RX-A3030 amplifier, and a 7.1 loudspeaker system based on seven M&K Sound LCR950 speakers and an M&K Sound V8 subwoofer.
2.6Treatment
The rehabilitation sessions took place in CARE Lab and consisted of five games (Bubbles levels 1, 2 and 3 as well as Balloons levels 1 and 2) involving upper limb movements using VITAMIN [28].
For the Bubbles game, transparent bubbles were considered normal targets, yellow were bonus, and red “malus,” hence to be avoided. For the Balloons game, neutral or happy faces were considered normal targets, while sad faces were considered “malus,” and hence to be avoided. In each game, targets spawned from the bottom of the screen and moved toward the top. The trajectories of the targets consisted of a constant velocity movement with a small sinusoidal perturbation perpendicular to the main movement. The games were classified into three levels based on their difficulty. Level 1 games required the patient to hit every target that appeared on the screen. Level II and III games required the user to discriminate between targets to be hit (normal or “bonus”) and targets to be avoided (“malus”) based on different shapes and/or color (Fig. 4). The “hit” event was triggered in-game when the virtual cursor (hand) partially overlapped the target.
Fig. 4
Pictures of the screen taken during each of the five games used in the rehabilitation sessions.

Participants controlled the virtual hand on the screen by moving the hand of their paretic limb. The movements were captured by means of a Microsoft Kinect 2.0 (Microsoft, Redmond, WA, USA), which provided the 3D real-world coordinates of the end effector to VITAMIN [28]. Once acquired, the 3D coordinates were then transformed into suitable 2D screen coordinates of the virtual hand according to the mandatory calibration parameters. It is important to underline the crucial role of the calibration procedure, which was performed by the child under the supervision of a skilled therapist. By acquiring the maximum extension of the children’s limbs, the system could map their movement on the entire screen, hence allowing each of them to play on the whole projected area of the game, independent of their specific motion and coordination capabilities and arm length.
The treatment consisted of 10 weekly sessions of approximately 45 minutes each. At the beginning of the session, a calibration procedure of around three minutes was performed. Then, each child played a two-minute game that was repeated once after around one minute of rest. After each game, the child had two minutes of rest before starting the next one, according to the sequence previously described. This fragmented sequence was designed to avoid any potential cybersickness effect [29]. Secondly, it was needed to limit fatigue due to the high attention level required for each game; some of the questionnaires filled in at the end of each session (during the remaining 4 minutes) reported that children were tired, despite the overall sum of around 20 minutes of real activities performed. However, it is important to underline that the actual amount of time for each child and each session varied slightly according to the child’s conditions and compliance, which required careful attention by the therapist.
3Results
Comparing the pre- and post-treatment evaluations, there were clear improvements in most of the measures and scores. Table 2 reports the increase in MA2 scores (Fig. 5), as well as the percentage of the values at T1 with respect to T0. All the participants showed an increase in MA2 scores, indicating a general improvement in performances.
Table 2
Melbourne Assessment 2 (MA2) Scores at T0 and T1 (left and central panels), described per single element of movement quality assessed (Range of movement –ROM; Accuracy of reach and placement; Dexterity of grasp, release and manipulation; Fluency of movement). The right panel gives the percentage of the actual increase between MA2 T1 scores over T0 scores with respect to the maximum possible increase for each child (MA2-IPI)
| MA2 Scores (T0) | MA2 Scores (T1) | MA2-IPI Scores | ||||||||||
| Participant ID | ROM | Accuracy | Dexterity | Fluency | ROM | Accuracy | Dexterity | Fluency | ROM | Accuracy | Dexterity | Fluency |
| 1 | 66.7% | 96.0% | 52.6% | 61.9% | 85.2% | 100.0% | 73.7% | 76.2% | 55.6% | 100.0% | 44.4% | 37.5% |
| 2 | 37.0% | 92.0% | 47.4% | 52.4% | 66.7% | 96.0% | 52.6% | 52.4% | 47.1% | 50.0% | 10.0% | 0.0% |
| 8 | 59.3% | 92.0% | 52.6% | 42.9% | 77.8% | 96.0% | 68.4% | 57.1% | 45.5% | 50.0% | 33.3% | 25.0% |
| 3 | 63.0% | 88.0% | 68.4% | 52.4% | 85.2% | 100.0% | 89.5% | 66.7% | 60.0% | 100.0% | 66.7% | 30.0% |
| 11 | 59.3% | 92.0% | 52.6% | 61.9% | 63.0% | 96.0% | 52.6% | 71.4% | 9.1% | 50.0% | 0.0% | 25.0% |
| 6 | 66.7% | 96.0% | 47.4% | 42.9% | 88.9% | 96.0% | 63.2% | 52.4% | 66.7% | 0.0% | 30.0% | 16.7% |
| Mean | 47.3% | 58.3% | 30.7% | 22.4% | ||||||||
Fig. 5
Mean Melbourne Assessment 2 (MA2) scores (average of all four items) for each participant.
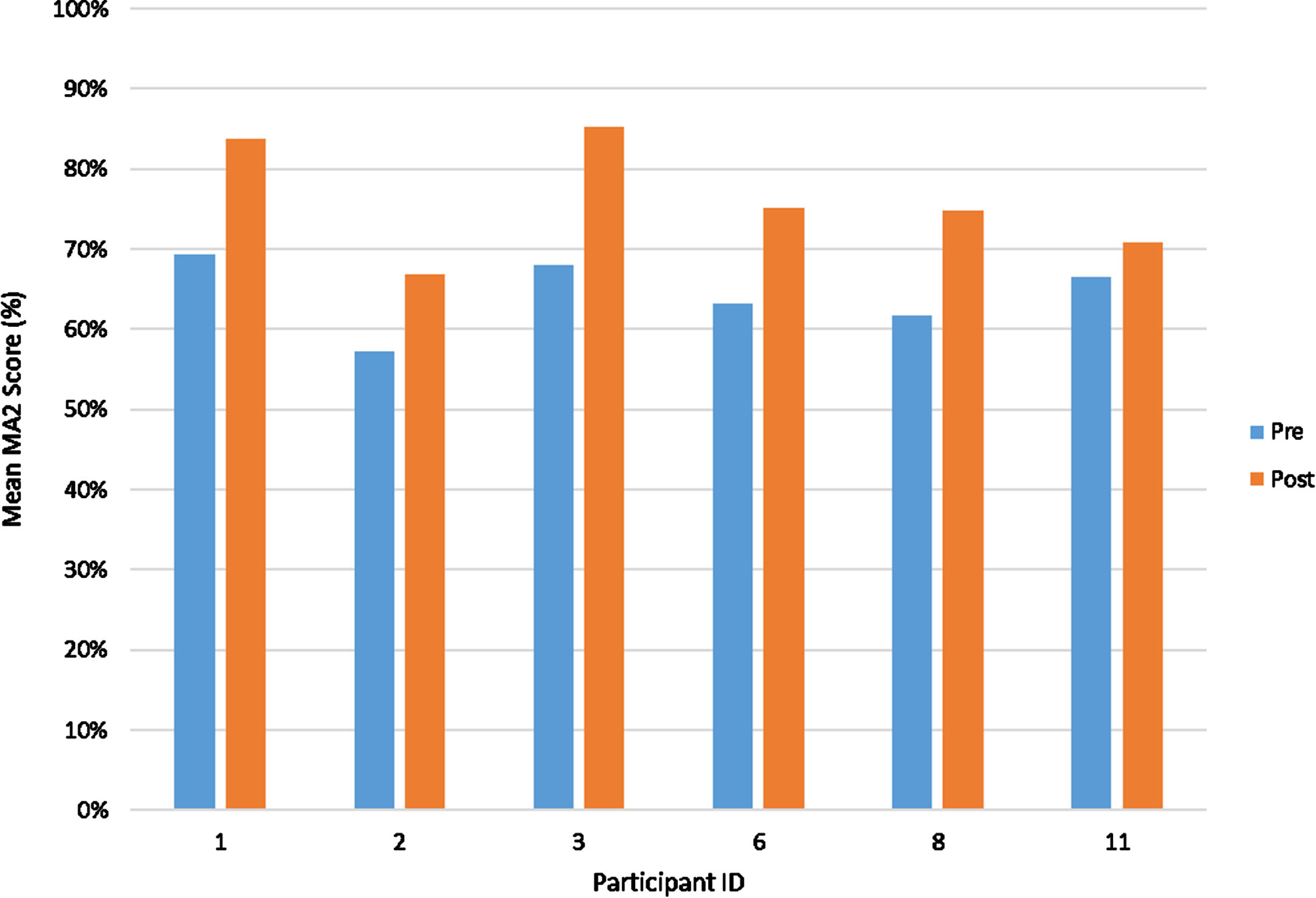
Table 4 reports some relevant differences in pre- and post-measures. There was an increase in flexion and extension in shoulder joint ROM after treatment.
The MAS did not present any changes between T0 and T1, and hence Table 4 reports the values assessed for each child in the MAS subsection.
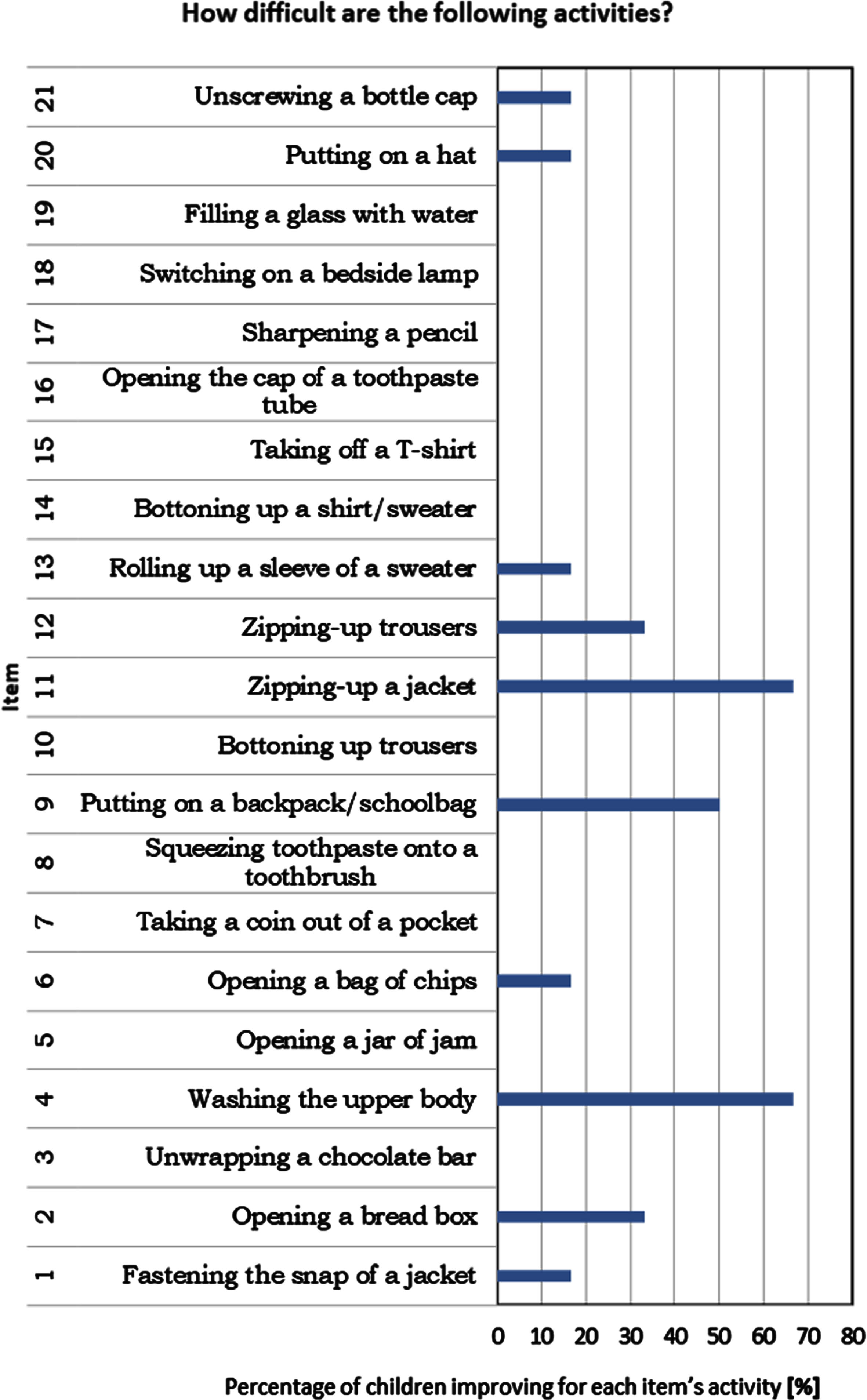
Considering ADL, Fig. 6 shows the resulting differences in the ABILHAND-Kids questionnaire.
Fig. 6
Histogram reporting the items in the ABILHAND-Kids with a performance improvement.
The satisfaction questionnaires were collected in only 36 out of 60 treatments; all participants filled out at least one satisfaction questionnaire. The VR treatment was positively accepted by all participants: 100% of answers to question 1 (“How was playing at CARE Lab with VITAMIN?”) were “good.” Regarding question 2 (“How do you feel after playing at CARE Lab with VITAMIN?”), four children always reported feeling well after the treatments, one (ID = 6) reported only once feeling “well and tired,” and one (ID = 1) always reported to be “tired.” The answer was “well” in 30 out of 36 (83.3%) questionnaires, and “tired” in 7 out of 36 (19.4%).
Despite this, in 20 out of 36 (52.8%) questionnaires, children reported some kind of discomfort or pain on the impaired side.
According to question 3 (“How are the VITAMIN games?”), VITAMIN activities were judged to be “funny” in 67% of the treatments and “boring” in 33%; 17% of the questionnaires reported the games to be “difficult” and 19% “tiring.” Children who indicated the “difficult” attribute always also marked the “funny” one too, while the “tiring” attribute was always associated with the “boring” one.
3.1Instrumental kinematic analysis
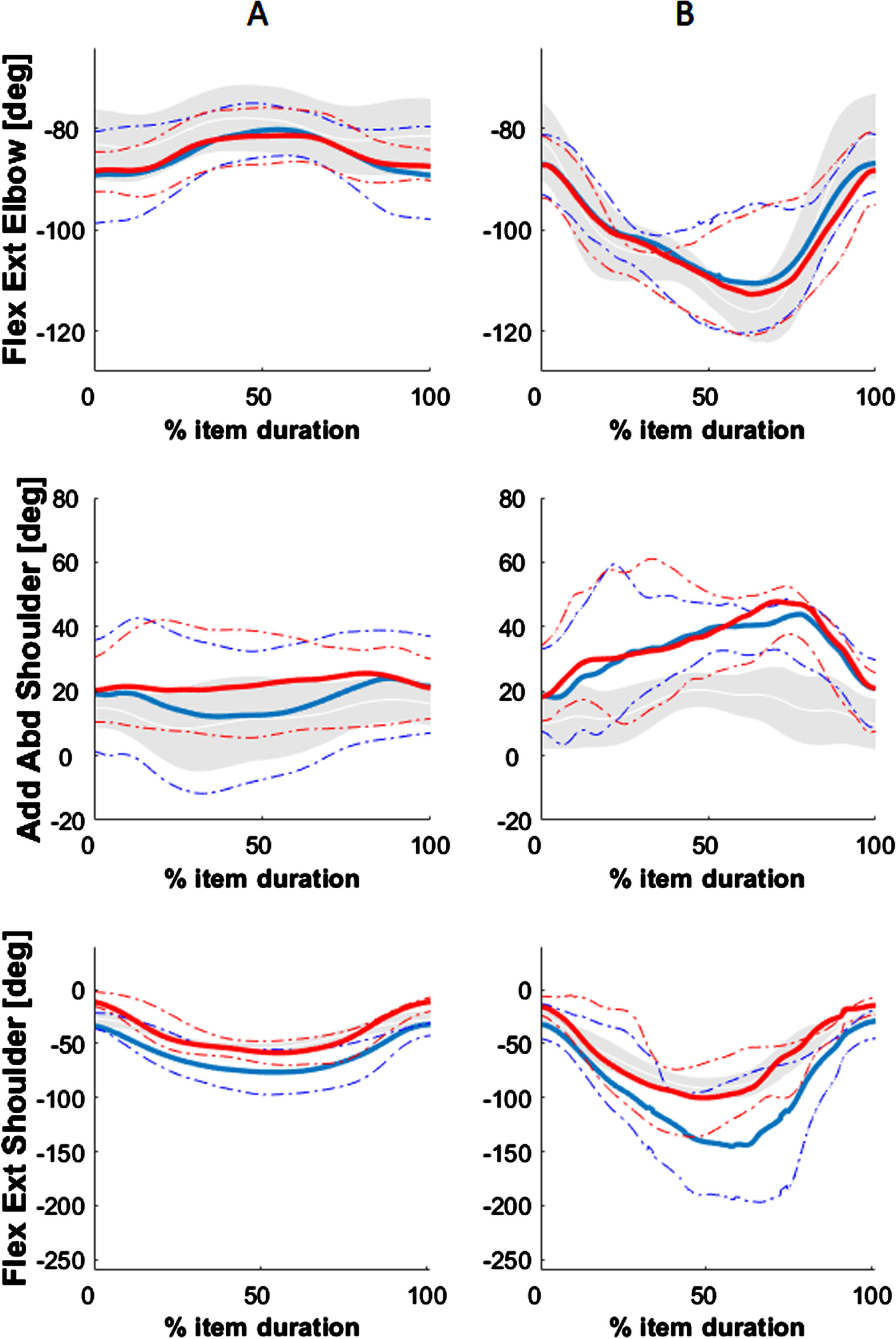
Figure 7 shows the overall average progression of the children. The solid blue line represents the mean trend of the group of children with hemiplegia at T0 (before treatment) and red at T1 (after treatment). The gray area reports the behavior of the control group, and the dotted lines represent the standard deviations of pre- (T0, in blue) and post-treatments (T1, in red).
Fig. 7
Mean trend of range of movement (ROM) of shoulder and elbow during two items of the Melbourne Assessment 2 (MA2), respectively at T0 (blue lines) and T1 (red lines), while the gray areas represent the control group reference. Column A = Reach forward (MA2 Item 1); Column B = Reach to brush from forehead to back of neck (MA2 Item 10).
Similarity indexes (SI; Pearson’s correlation, R2 –the coefficient of determination) for the children’s paretic upper limb were also calculated with respect to the typically-developing children’s reference measurements (TD) for the following: the kinematic profiles of flexion-extension (Flex / Ext) and adduction and abduction (Add. / Abd.) of the shoulder joint and the flexion-extension (Flex / Ext) of the elbow joint (Table 3). The SI values ranged from -1.0 (opposite of TD) to 1.0 (similar to TD), indicating the degree of deviation from the reference. SI absolute values in the range from 0.0 to 0.3 represented a low similarity between the curves, values in the range 0.3 to 0.7 represented a modest similarity, and values > 0.7 a strong similarity. Table 3 reports the SI as well as the Pearson correlation coefficients between MA2 measures and SI values.
Table 3
Similarity indexes and Pearson’s correlation between Melbourne Assessment 2 (MA2) scores and similarity index. The highest values of Pearson’s correlation between MA2 and Similarity Index are highlighted in yellow
| PARAMETER | MA2 ITEM 1 | MA2 ITEM 2 | MA2 ITEM 3 | MA2 ITEM 10 | MA2 ITEM 13 |
| MA2 Score | 7.8 (0.8) | 7.2 (1.3) | 2.2 (0.8) | 2.8 (1.2) | 6.0 (2.0) |
| SIMILARITY INDEXES | |||||
| SIML. FLEX/EXT ELBOW | 0.65 (0.40) | 0.53 (0.27) | 0.34 (0.55) | 0.96 (0.03) | 0.96 (0.01) |
| SIML. ADD/ABD SHOULDER | 0.59 (0.44) | 0.89 (0.08) | -0.08 (0.81) | 0.87 (0.12) | 0.57 (0.38) |
| SIML. FLEX/EXT SHOULDER | 0.93 (0.02) | 0.62 (0.51) | 0.91 (0.05) | 0.84 (0.14) | 0.91 (0.05) |
| PEARSON’S CORRELATION BETWEEN MA2 AND SIMILARITY INDEX | |||||
| FLEX/EXT ELBOW | 0.83 | 0.23 | 0.88 | 0.19 | 0.48 |
| ADD/ABD SHOULDER | 0.47 | 0.31 | 0.12 | 0.38 | 0.94 |
| FLEX/EXT SHOULDER | 0.03 | 0.76 | 0.09 | 0.27 | 0.81 |
SIML = Similarity Index; Flex = Flexion; Ext = Extension; Add = Adduction; Abd = Abduction.
Table 4
Summary of the results for all the participants. In the MAS section, the “1-” values represent the assessment of those children who were close but could not completely reach level “1” of the scale.
| Participant ID | 1 | 2 | 8 | 3 | 11 | 6 | |||||||
| PROM (°) | T0 | T1 | T0 | T1 | T0 | T1 | T0 | T1 | T0 | T1 | T0 | T1 | |
| Shoulder | flexion | 150° | 160° | 145° | 155° | 25° | 35° | 147° | 155° | 155° | 165° | 150° | 165° |
| abduction | 110° | 115° | 120° | 125° | 130° | 130° | 125° | 130° | 130° | 135° | 110° | 110° | |
| Elbow | flexion | 135° | 135° | 135° | 135° | 135° | 135° | 140° | 140° | 140° | 150° | 140° | 140° |
| extension | 180° | 180° | 170° | 170° | 180° | 180° | 175° | 175° | 170° | 175° | 180° | 180° | |
| Wrist | flexion | 85° | 90° | 90° | 90° | 90° | 90° | 75° | 75° | 90° | 90° | 10° | 10° |
| extension | 45° | 45° | 45° | 50° | 30° | 30° | 45° | 45° | 30° | 30° | 55° | 60° | |
| MAS | |||||||||||||
| Shoulder | 1 | 1 | 0 | 0 | 1 | 1 | |||||||
| Elbow | 2 | 2 | 1- | 1- | 1- | 1 | |||||||
| Wrist | 2 | 1 | 2 | 1 | 3 | 2 | |||||||
| Mean MA2 (%) | 69.3 | 83.75 | 57.2 | 67 | 61.69 | 74.75 | 67.94 | 85.25 | 66.45 | 70.75 | 63.22 | 75 | |
| ABILHAND-Kids | 10/42 | 12/42 | 23/42 | 26/42 | 13/42 | 17/42 | 33/42 | 34/42 | 21/42 | 23/42 | 19/42 | 24/42 |
(PROM = Proximal Range of Motion; MAS = Modified Ashworth Scale).
3.2VITAMIN data analysis
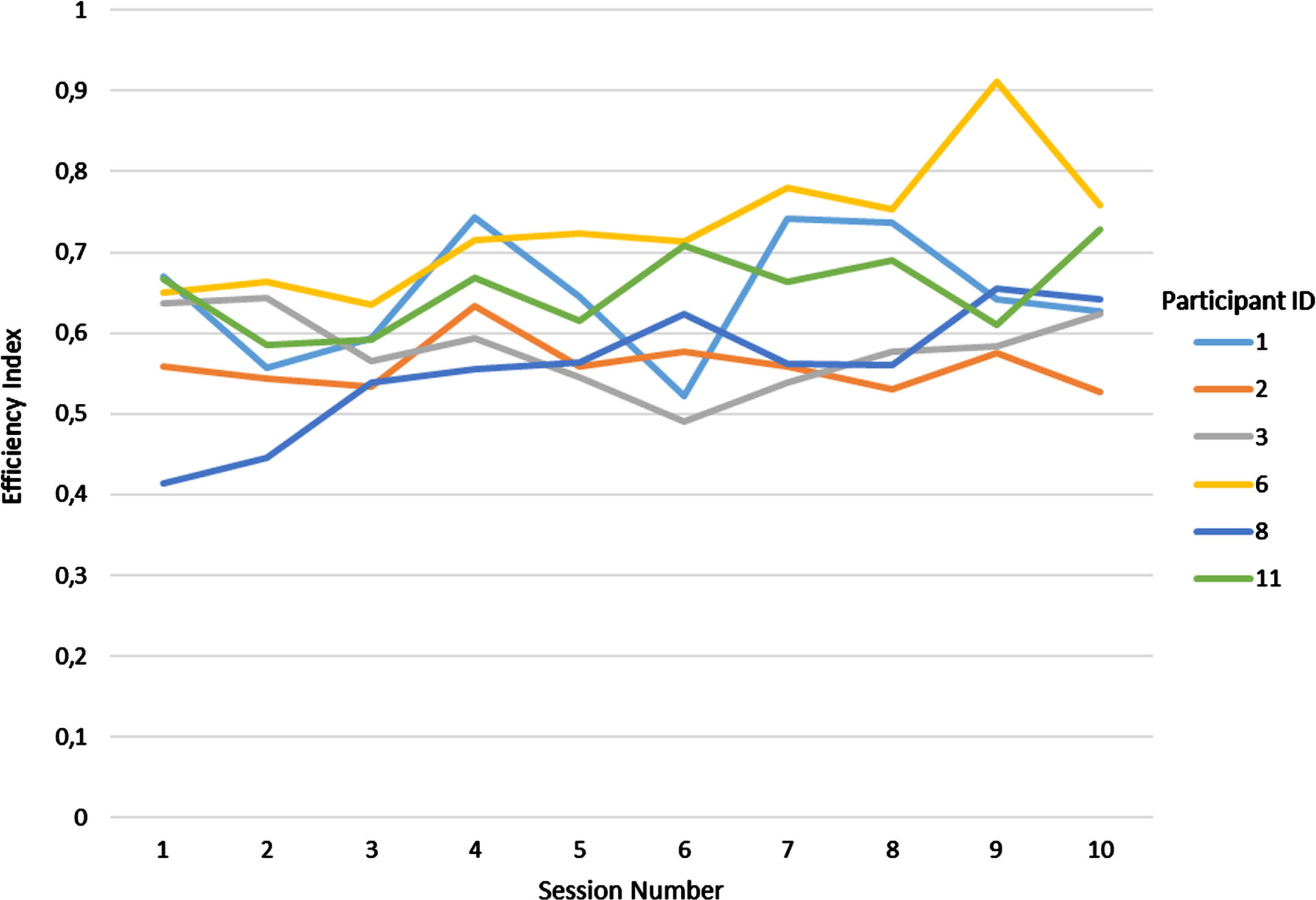
The graph in Fig. 8 shows a reduction in the trajectory length for all patients except one (participant 2). Figure 9 shows some samples of the overall 2D trajectories for two different participants (2 and 6) in the first and last sessions. The sequence of coordinates of the virtual hand is plotted in black, while the yellow circles represent the positions of the targets hit on the screen. The final trajectory for participant 6 appeared more compact and concentrated on the lower part of the screen (from where the targets were generated) with respect to the initial one (in agreement with Fig. 7). Participant 2 instead seemed to have a more dispersed trajectory in the final session with respect to the initial one. The increased dispersion of participant 2’s trajectory for the last session in Fig. 9 is also related to the results in Fig. 8. In Fig. 10, the efficiency index of six participants throughout the 10 sessions for one of the exercises (game 4) is reported.
Fig. 8
Graph on the overall two-dimensional (2D) length of the trajectories, for each participant in each session [1–10].
![Graph on the overall two-dimensional (2D) length of the trajectories, for each participant in each session [1–10].](https://ip.ios.semcs.net:443/media/prm/2024/17-1/prm-17-1-prm230028/prm-17-prm230028-g008.jpg)
Fig. 9
Movements of the hand in a given game. Black lines represent the trajectory of the hand; yellow circles represent the position of the target hit.
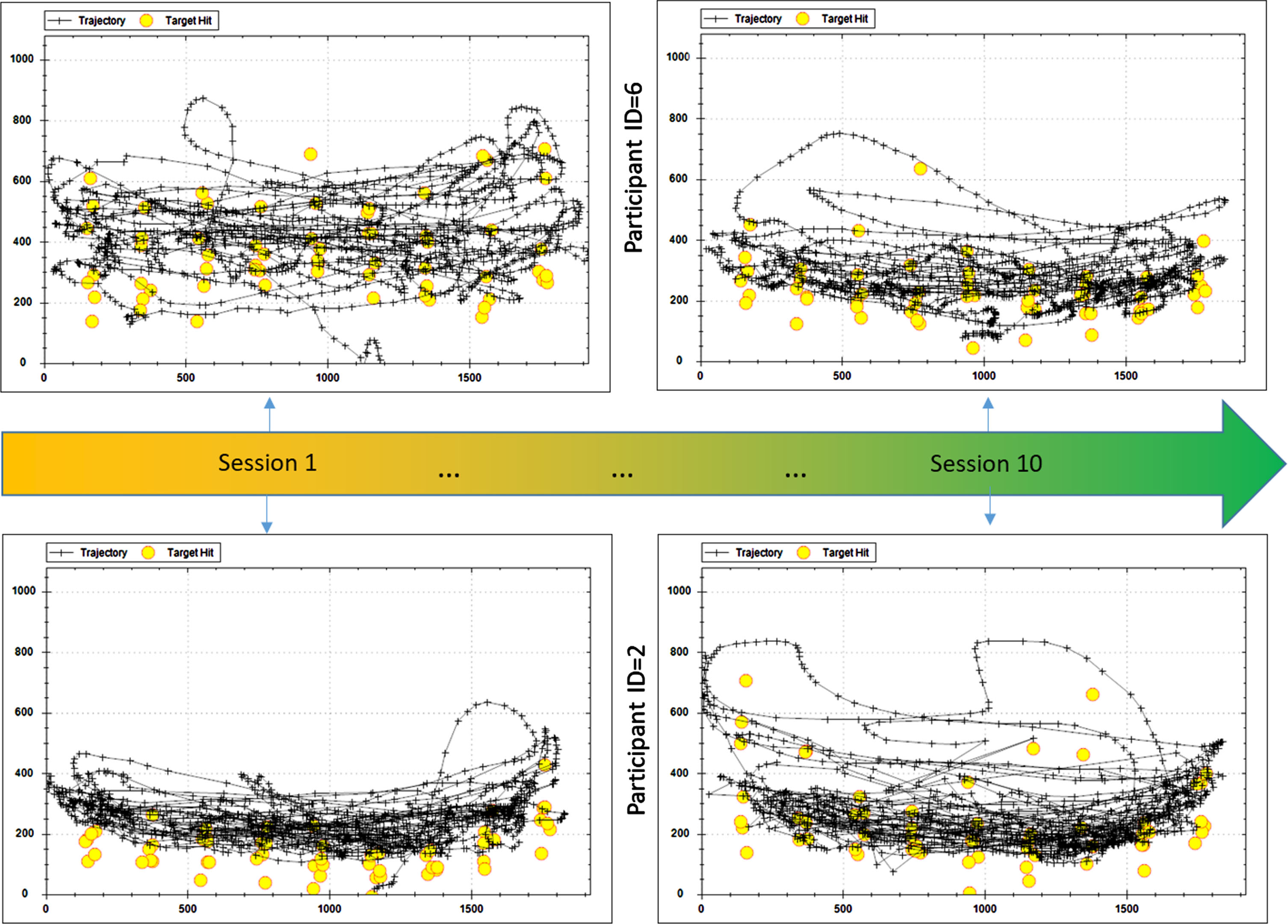
Fig. 10
Efficiency index in Game 4 for each child according to the different sessions.
4Discussion
The main aim of this study was to explore the acceptability and usability of a novel rehabilitation treatment of UCP. Recent studies investigating the effect of VR in developmental rehabilitation are still too heterogeneous and therefore difficult to compare, as confirmed by a recent meta-analysis [38]. In most cases, the studies reported in this meta-analysis investigated the effect of VR through outcome measures involving functions and body structure and documented a general positive effect of the treatments. In line with previous works, the current study used similar outcome measures in order to assess motor capacity. The results suggested a general improvement of the participants’ motor capacities at the end of the treatments, and some considerations can be derived. First, the differences between the MA2 scale scores showed an improvement between T0 and T1. It is important to underline that such improvement was more evident in the “range of movement,” which was the index with the greatest increase. In addition, “dexterity” and “fluency” showed a substantial improvement, while the slighter increase in the “accuracy” items (compared to the others) may be explained because the values at T0 were already very high.
Considering shoulder, elbow, and hand ROMs, a clear improvement was observed in both passive and active movement of flexion and extension for all children. VITAMIN games promoted relevant use of the affected arm with large flexion and extension of the shoulder while trying to hit the virtual targets that appeared on the screen. These game activities were specifically designed to disguise the repetition of movements while sustaining attention and motivation to promote motor learning [39]. This could explain the improvement in the range of motion as assessed through goniometers and also detected by the Melbourne scale in performing standardized tasks.
The Ashworth scale did not change between T0 and T1. This outcome was expected as functional activities or motor exercises may rarely produce meaningful effects on the limb’s spasticity without pharmacological treatment [40].
The ultimate goal of rehabilitation is to increase autonomy and participation in daily life, as highlighted in the meta-analysis previously cited [38]. For this reason, a specific questionnaire was used to test whether the eventual change in motor capacity could also translate into an improvement in motor capabilities. In fact, the analysis of the ABILHAND-Kids scale showed an improvement in the use of the paretic upper limb during ADL like washing the upper part of the body or pulling up the zipper of a jacket. This result may also be the effect of an improvement of the shoulder joint ROM and a better proximal control of the upper limb (the shoulder), also affecting the distal movements (the wrist and the hand).
The results of the satisfaction questionnaire administered at the end of each session confirmed the acceptability of the proposed activities by all children. Furthermore, the feedback about some degree of discomfort or fatigue in the hemiplegic upper limb at the end of each session (52.8% of the questionnaires) may have represented a positive result: it could have meant that children had used the impaired limb much more than usual. The importance of this result is also underlined by the 67% of questionnaires that described the treatment as “funny.” This general positive attitude toward the treatment was also supported by the 83.3% of children who answered “well” to question 2 (“How do you feel after playing at CARE Lab with VITAMIN?”). Only one child (ID = 1) always reported being “tired” after each session, but there was no relationship with Manual Ability Classification System (MACS) level or age, nor with performances (as measured by MA2 score). Rather, since the answers of this child to question 3 (“How are the VITAMIN games?”) were always “boring and tiring,” there may have been a negative bias in this child’s approach to the activities that influenced the final opinion.
In looking toward future studies, further evaluation of the overall percentage of sessions judged to be “difficult” and “tiring” would be of interest, as these terms may positively indicate that the proposed activities were challenging enough to have children working in their “zone of proximal development” [41]. In any case, the 33% of feedback labeling the activities as “boring” still needs to be carefully considered, to improve the playability and participant motivation in using VITAMIN. This result may mean that the difficulty level of the proposed activities was not considered challenging enough by some children (especially given the videogames they usually play), and hence it should be increased.
Considering the instrumental kinematic assessment, an outcome measure widely used also in other studies [42], Fig. 7 shows a general improvement trend in the paretic limb’s kinematics after the treatment. The T1 average curve was more similar to those of typically-developing children, possibly indicating a recovery of the physiological motor strategy. It is important to underline the progress in shoulder flexion-extension between pre- (T0, in blue) and post- treatment (T1, in red), suggested by the reduced distance of the post-treatment curve from the reference range reported in gray. The ADL improvements reported by the ABILHAND-Kids could be related to better control in shoulder flexo-extension, as it appears in Fig. 8.
The analysis of the data acquired by the VITAMIN platform, although somewhat limited and not yet generalizable, showed interesting results. Different behaviors of hand trajectory appeared among the participants (Fig. 8). For three children, the length of the trajectory decreased along the sessions, and this could have been due to the use of more efficient strategies to reach the targets. On the other hand, the length of the trajectory increased for two children, which could mean there was an increase in the working volume explored by the hand’s movements. Only one child did not show relevant variations in the length of the trajectory over the ten sessions; this could be possibly related to the enjoyment of that participant in playing the game differently than others, by using the entire screen space and not necessarily aiming directly at targets as they appeared on the screen. This behavior could also mean the game was not challenging enough for that participant. Further studies involving indexes of different natures (e.g., complexity, fractal dimension) are of course required to fully clarify these somewhat contradictory results.
It is important to highlight the need to further analyze the kinematic data acquired by the system (i.e., the 3D positions of the hand or other parts of the body relevant for the rehabilitation process). Although objective measures, the single values have low meaning in the rehabilitation process because the movement performed by the children during these activities was non-structured. Hence, their relevance increased when compared to the presence of targets, and further processing will be required to extract novel indexes that may appear meaningful for clinicians and therapists. This is a non-trivial process, currently ongoing, with the aim of establishing robust relationships among measures, sampled trajectories, and the related indexes, clinical scales, and subjective assessments performed by operators. For this reason, it was not possible to have a small “reference” group as in the kinematic instrumented assessment; in addition, VITAMIN exercises included free types of movement compared to the repetitive and structured nature of the kinematic assessment.
Finally, the efficiency index (Fig. 10) showed an increasing trend during all the sessions for four children (ID = 1, 6, 8, and 11), while for one child (ID = 3) the positive trend appeared only in the second half of the sessions. This may be related to an increasingly efficient motion strategy to reach the targets on the screen. However, another child (ID = 2) appeared to have a counterintuitive behavior (increasing trajectory length and decreasing efficiency index). As previously described, further investigations are required to fully explain these findings.
From this preliminary investigation, there were three relevant findings. The first and most important was the acceptability and usability of a rehabilitation protocol based on VITAMIN non-immersive VR treatment (especially regarding motivation) and the related assessments. This finding importantly highlights the positive effects of an engaging and pleasant treatment, which can be tailored to the child.
Secondly, the good level of agreement in upper limb performances (in particular shoulder movements) between quantitative measures, clinical scales, and the quali-quantitative results of the ABILHAND-Kids represents an encouraging finding in the perspective of future studies with a larger number of participants. Moreover, such agreement represents a key step towards an increased quantitative approach in rehabilitation: besides the usual pre- and post-treatment assessments (usually consisting of clinical scales) and the fundamental role of therapists, measuring the performances continuously during the exercises may enable each exercise to be fine-tuned in each rehabilitation session. This careful adaptation may lead to a more efficient and consistent rehabilitation process and, ultimately, to better results compared to the traditional approach to pediatric rehabilitation. These results appear to be aligned with a recent review of VR-based treatments of UCP [12], which underlined higher effectiveness in treatments that have better personalization and adaptation capabilities compared to the common off-the-shelf exergames consoles (like Nintendo Wii, etc.).
The third finding, which was possibly the most interesting, regarded the evidence that such an interactive treatment may lead to objective improvements in ADL, as underlined by the ABILHAND-Kids results and consistent reductions in the gap between the children with UCP and the reference measurements used in the pre- and post-kinematic assessment. This finding could be relevant, since it addresses the key expectation of a rehabilitation process (in light of the current biopsychosocial model underlying the ICF framework): an enhancement in participation. This last finding should be fostered in other studies to fully understand the effectiveness and the efficacy of customizable VR-based treatments, such as the one presented in this paper.
A relevant consideration regarded the usability of the system by the operators and patients: given the limited amount of time for each rehabilitation session (usually 45 minutes), it was important to reduce the burden of a complex setup procedure, while providing a simple and usable tool. Although no formal measure was collected from the therapists, the experience was anecdotally noted to be highly positive: the operators reported that the system was fast to start (there was no need to attach an instrument to the child) and easy to control through the tablet, and that there was almost no downtime.
Given the exploratory nature of this study, it is fundamental to clearly state its limitations. In addition to the small number of children involved, data validity and reliability were not formally verified; this deserves to be adequately considered in future studies.
Additionally, larger controlled studies are required to fully assess the contradictory results in the data gathered and indexes derived by VITAMIN, as previously introduced (Figs. 8 vs. 10). This issue may be crucial, because clarifying the relationships between the raw data and indexes and their clinical/rehabilitation meaning could lead to a continuous tailoring of the rehabilitation process based on the actual needs and competence of each child for each exercise in each session. To better understand the effects of the rehabilitation treatment, it would be important to collect feedback from almost all the sessions. Moreover, the satisfaction questionnaire may also be improved by adding more items to better understand the whole user experience and to possibly estimate the level of engagement, while preserving its simplicity.
Furthermore, a second questionnaire, focused on the therapists’ feedback after each session, should also be considered for a more completed view of the activities proposed and performed.
Another limitation was the lack of follow-up evaluations that could have further clarified the effects of the rehabilitation process. However, given the developmental age of the children, this would have required a larger and longer controlled study.
Finally, no formal measurements on feasibility and sustainability were performed; these should be part of larger controlled studies to thoroughly assess the impact of this novel treatment in daily clinical practice.
5Conclusions
In this study, an innovative rehabilitation protocol based on a recently developed non-immersive VR platform (VITAMIN) was presented. The protocol was initially applied to a small sample of children with UCP in order to explore its acceptability and, to some extent, its usability, as well as to start investigating the possible beneficial effects on upper limb function.
Despite the very limited sample size, good compliance, engagement, and enjoyment in the proposed activities were reported by the participants. The resulting increased performance levels, assessed (with a good level of agreement) by clinical scales, instrumental measures, and the ADL questionnaire, suggested that this new rehabilitation approach may lead to improvement in function and capabilities of paretic upper limbs.
Further investigations are required to foster the relationship between the pre- and post-treatment assessments and the measures continuously acquired during the rehabilitation sessions by the system. Possibly, these investigations may also lead to modification of the indexes or to the introduction of new ones, that may offer clinicians and therapists a synthetic view of the actual performances expressed by the child during each exercise.
This study is therefore to be considered the first step for other clinical investigations to assess the feasibility and efficacy of VITAMIN-based treatments in pediatric UCP rehabilitation. It will be also crucial to provide suitable follow-up measurements, to fully assess the real long-term effects of these VR-based activities in ADL. Of course, understanding the long-term effects will be challenging, given the developmental age of the children who are the target population for the VITAMIN platform.
Data presented in this work are limited and preliminary. Although further and larger controlled studies are required to fully address the potential and the limitations of novel technological solutions like VITAMIN, its personalized, engaging, interactive, and quantitative approach seems to be valuable and promising.
Acknowledgments
This study was partially supported and funded by the Italian Ministry of Health –“Ricerca Corrente 2023.” The authors would also like to acknowledge the Associazione Zorzi per le Neuroscienze and Fondazione Pajan Parola, which have funded most of CARE Lab and VITAMIN design and development.
Ethical considerations
Patient recruitment and data collection were performed within the framework of the usual clinical practice of Fondazione Don Carlo Gnocchi, according to the ethical standards of the responsible committee on human experimentation and the Helsinki Declaration. All participants’ caregivers provided signed informed consent to participate in the study and to let their data to be analyzed and presented in anonymous format for research purposes. The present study, being a preliminary investigation carried out as a final thesis research and given the informed consent signed by all the caregivers, was not requested to be submitted to our ethical committee.
Conflict of interest
The authors have no conflict of interest to report.
References
[1] | Durkin MS , Benedict RE , Christensen D , et al. Prevalence of Cerebral Palsy among 8-Year-Old Children in and Preliminary Evidence of Trends in Its Relationship to Low Birthweight. Paediatr Perinat Epidemiol. (2016) :30: (5):496–510. doi: 10.1111/ppe.12299 |
[2] | Arnaud C , Ehlinger V , Perraud A , et al. Public health indicators for cerebral palsy: A European collaborative study of the Surveillance of Cerebral Palsy in Europe network. Paediatr Perinat Epidemiol. (2023) :37: (5):404–12. doi: 10.1111/ppe.12950 |
[3] | Himmelmann K , Uvebrant P . The panorama of cerebral palsy in Sweden part XII shows that patterns changed in the birth years 2007–2010. Acta Paediatr. (2018) :107: (3):462–8. doi: 10.1111/apa.14147 |
[4] | Brown R , Pearse JE , Nappey T , et al. Wrist-Worn devices to encourage affected upper limb movement in unilateral cerebral palsy: Participatory design workshops. Front Rehabil Sci . (2022) :3: :1021760. doi: 10.3389/fresc.2022.1021760 |
[5] | Park H , Choi JY , Yi S-H , et al. Relationship between the more-affected upper limb function and daily activity performance in children with cerebral palsy: a cross-sectional study. BMC Pediatrics. (2021) :21: (1):459. doi: 10.1186/s12887-021-02927-2 |
[6] | Radomski MV . More than good intentions: advancing adherence to therapy recommendations. Am J Occup Ther. (2011) :65: (4):471–7. doi: 10.5014/ajot.2011.000885 |
[7] | Levin MF . Can virtual reality offer enriched environments for rehabilitation? Expert Rev Neurother. (2011) :11: (2):153–5. doi: 10.1586/ern.10.201 |
[8] | Miller S , Reid D . Doing play: competency, control, and expression. Cyberpsychol Behav. (2003) :6: (6):623–23. doi: 10.1097/PEP.0000000000000046 |
[9] | Chen YP , Lee SY , Howard AM . Effect of virtual reality on upper extremity function in children with cerebral palsy: a meta-analysis. Pediatr Phys Ther. (2014) :26: (3):289–300. doi: 10.1097/PEP.0000000000000046 |
[10] | Cramer SC , Sur M , Dobkin BH , et al. Harnessing neuroplasticity for clinical applications. Brain. (2011) :134: (Pt 6):1591–609. doi: 10.1093/brain/awr039 |
[11] | Han Y , Park S . Effectiveness of virtual reality on activities of daily living in children with cerebral palsy: a systematic review and meta-analysis. PeerJ. (2023) :11: :e15964. doi: 10.7717/peerj.15964 |
[12] | Chen Y , Fanchiang HD , Howard A . Effectiveness of Virtual Reality in Children With Cerebral Palsy: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phys Ther. (2018) :98: (1):63–77. doi: 10.1093/ptj/pzx107 |
[13] | Benzing V , Schmidt M . Exergaming for Children and Adolescents: Strengths, Weaknesses, Opportunities and Threats. J Clin Med. (2018) ;7: (11). doi: 10.3390/jcm7110422 |
[14] | Rodrigues JC , Menezes P , Restivo MT . An augmented reality interface to control a collaborative robot in rehab: A preliminary usability evaluation. Front Digit Health. (2023) :5: :1078511.. doi: 10.3389/fdgth.2023.1078511 |
[15] | Meyns P , Roman de Mettelinge T , van der Spank J , Coussens M , Van Waelvelde H . Motivation in pediatric motor rehabilitation: A systematic search of the literature using the self-determination theory as a conceptual framework. Dev Neurorehabil. (2018) :21: (6):371–90. doi: 10.1080/17518423.2017.1295286 |
[16] | Parsons TD , Rizzo AA , Rogers S , York P . Virtual reality in paediatric rehabilitation: a review. Dev Neurorehabil. (2009) :12: (4):224–38. doi: 10.1080/17518420902991719 |
[17] | Guadagnoli MA , Lee TD . Challenge point: a framework for conceptualizing the effects of various practice conditions in motor learning. J Mot Behav. (2004) :36: (2):212–24. doi: 10.3200/jmbr.36.2.212-224 |
[18] | Snider L , Majnemer A , Darsaklis V . Virtual reality as a therapeutic modality for children with cerebral palsy. Dev Neurorehabil. (2010) :13: (2):120–8. doi: 10.3109/17518420903357753 |
[19] | Winkels DG , Kottink AI , Temmink RA , Nijlant JM , Buurke JH . Wii-habilitation of upper extremity function in children with cerebral palsy. An explorative study. Dev Neurorehabil. (2013) :16: (1):44–51. doi: 10.3109/17518423.2012.713401 |
[20] | Chiu H-C , Ada L , Lee H-M . Upper limb training usingWii Sports Resort™ for children with hemiplegic cerebral palsy: a randomized, single-blind trial. Clin Rehabil. (2014) :28: (10):1015–24. doi: 10.1177/0269215514533709 |
[21] | Sandlund M , Domellof E , Grip H , Ronnqvist L , Hager CK . Training of goal directed arm movements with motion interactive video games in children with cerebral palsy –A kinematic evaluation. Dev Neurorehabil. (2014) :17: (5):318–26. doi: 10.3109/17518423.2013.776124 |
[22] | You SH , Jang SH , Kim YH , Kwon YH , Barrow I , Hallett M . Cortical reorganization induced by virtual reality therapy in a child with hemiparetic cerebral palsy. Dev Med Child Neurol. (2005) :47: (9), 628–35. |
[23] | Chen YP , Kang LJ , Chuang TY , et al. Use of virtual reality to improve upper-extremity control in children with cerebral palsy: a single-subject design. Phys Ther. (2007) :87: (11):1441–57. doi: 10.2522/ptj.20060062 |
[24] | Wang M , Reid D . Virtual reality in pediatric neurorehabilitation: attention deficit hyperactivity disorder, autism and cerebral palsy. Neuroepidemiology. (2011) :36: (1):2–18. doi: 10.1159/000320847 |
[25] | Dewar R , Love S , Johnston LM . Exercise interventions improve postural control in children with cerebral palsy: a systematic review. Dev Med Child Neurol. (2015) :57: (6):504–20. doi: 10.1111/dmcn.12660 |
[26] | Bonnechere B , Jansen B , Omelina L , et al. Can serious games be incorporated with conventional treatment of children with cerebral palsy? A review. Res Dev Disabil. (2014) :35: (8):1899–913. doi: 10.1016/j.ridd.2014.04.016 |
[27] | Rathinam C , Mohan V , Peirson J , Skinner J , Nethaji KS , Kuhn I . Effectiveness of virtual reality in the treatment of hand function in children with cerebral palsy: A systematic review. J Hand Ther. (2019) :32: (4):426–34.el. doi: 10.1016/j.jht.2018.01.006 |
[28] | Olivieri I , Meriggi P , Fedeli C , et al. Computer Assisted REhabilitation (CARE) Lab: A novel approach towards Pediatric Rehabilitation 2.0. J Pediatr Rehabil Med. (2018) :11: (1):43–51. doi: 10.3233/PRM-160436 |
[29] | Martirosov S , Bures M , Zítka T . Cyber sickness in low-immersive, semi-immersive, and fully immersive virtual reality. Virtual Real. (2022) :26: (1):15–32. doi: 10.1007/s10055-021-00507-4 |
[30] | Klingels K , Jaspers E , Van de Winckel A , De Cock P , Molenaers G , Feys H . A systematic review of arm activity measures for children with hemiplegic cerebral palsy. Clin Rehabil. (2010) :24: (10):887–900. doi: 10.1177/0269215510367994 |
[31] | Palisano R , Rosenbaum P , Walter S , Russell D , Wood E , Galuppi B . Development and reliability of a system to classify gross motor function in children with cerebral palsy. Dev Med Child Neurol. (1997) :39: (4):214–23. doi: 10.1111/j.1469-8749.1997.tb07414.x |
[32] | Eliasson AC , Krumlinde-Sundholm L , Rosblad B , et al. The Manual Ability Classification System (MACS) for children with cerebral palsy: scale development and evidence of validity and reliability. Dev Med Child Neurol. (2006) :48: (7):549–54. doi: 10.1017/S0012162206001162 |
[33] | Wang TN , Liang KJ , Liu YC , Shieh JY , Chen HL . Psychometric and Clinimetric Properties of the Melbourne Assessment 2 in Children With Cerebral Palsy. Arch Phys Med Rehabil. (2017) :98: (9):1836–41. doi: 10.1016/j.apmr.2017.01.024 |
[34] | Harb A , Kishner S . Modified Ashworth Scale. Treasure Island, FL: StatPearls; 2022. |
[35] | Arnould C , Penta M , Renders A , Thonnard JL . ABILHAND-Kids: a measure of manual ability in children with cerebral palsy. Neurology. (2004) :63: (6):1045–52. doi: 10.1212/01.wnl.0000138423.77640.37 |
[36] | Francisco-Martinez C , Prado-Olivarez J , Padilla-Medina JA , et al. Upper Limb Movement Measurement Systems for Cerebral Palsy: A Systematic Literature Review. Sensors (Basel). (2021) :21: (23):7884. doi: 10.3390/s21237884 |
[37] | Rabuffetti M , Marzegan A , Crippa A , et al. The LAMB gait analysis protocol: Definition and experimental assessment of operator-related variability. Proc Inst Mech Eng H. (2019) :233: (3):342–53. doi: 10.1177/0954411919827033 |
[38] | Voinescu A , Sui J , Stanton Fraser D . Virtual Reality in Neurorehabilitation: An Umbrella Review of Meta-Analyses. J Clin Med. (2021) :10: (7):1478. doi: 10.3390/jcm10071478 |
[39] | Levac D , Rivard L , Missiuna C . Defining the active ingredients of interactive computer play interventions for children with neuromotor impairments: a scoping review. Res Dev Disabil. (2012) :33: (1):214–23. doi: 10.1016/j.ridd.2011.09.007 |
[40] | Novak I , McIntyre S , Morgan C , et al. A systematic review of interventions for children with cerebral palsy: state of the evidence. Dev Med Child Neurol. (2013) :55: (10):885–910. doi: 10.1111/dmcn.12246 |
[41] | Podolskiy AI . Zone of Proximal Development. In: Seel NM, editor. Encyclopedia of the Sciences of Learning. Boston, MA: Springer US; 2012. p. 3485–7. |
[42] | Franco De Moura RC , Almeida CS , Dumont AJL , et al. Kinematic upper limb evaluation of children and adolescents with cerebral palsy: a systematic review of the literature. J Phys Ther Sci. (2016) :28: (2):695–700. doi: 10.1589/jpts.28.695 |


