
Utilizing combination intrathecal baclofen and analgesic medication to manage spasticity and pain in patients with pediatric-onset disability: Case series
Abstract
PURPOSE:
The use of intrathecal medications for the management of spasticity and various pain syndromes in the adult population has been previously reported. However, no evidence-based guidelines currently exist in the pediatric population. This case series presents patients (n = 8) with pediatric-onset disability who underwent placement of intrathecal baclofen pumps initially for management of severe spasticity. Despite titration of dose and use of oral analgesia, their uncontrolled pain persisted. Each patient was transitioned to a combination of baclofen and analgesic intrathecal therapy. The outcome in pain improvement and quality of life, as reported by patients and/or caregivers, were retrospectively reviewed.
METHODS:
Retrospective review of the background and decision-making process regarding transition to combination intrathecal therapy identified patient selection characteristics. Each patient and/or their caregivers completed a survey regarding improvements in pain, spasticity, function, and quality of life following initiation of combination intrathecal medications.
RESULTS:
Survey results revealed improvements in functional and pain assessments after initiation of combination baclofen and analgesic intrathecal medication. Patients and caregivers reported decreases in pain and oral spasticity medications.
CONCLUSION:
Use of pumps with antispasmodic and analgesic medication for combination intrathecal medication delivery should be considered in the management of patients with childhood-onset disabilities who have both severe spasticity and pain.
1Introduction
Intrathecal (IT) drug delivery is utilized for the treatment and management of chronic pain and spasticity when other options have proven unsuccessful [1–4]. IT medications offer patients an alternative to other administration routes, allowing for better symptom control with lower dose requirements and fewer systemic side effects [1, 5]. When considering the use of intrathecal baclofen (ITB) for chronic spasticity in adult and pediatric patients, therapeutic effects can be accomplished with doses up to 100 times lower than oral baclofen [5]. Approximately 7,000 adults and 1,500 children had an intrathecal baclofen pump placed between the years of 2011–2014 [6].
Optimal maintenance dosage is highly individualized and is based on many variables, including patient diagnosis and functional goals [7]. Following optimization of intrathecal baclofen therapy, patients and their caregivers have reported reduction of spasticity and pain leading to improvements in patient communication, sleep, ease of care, and performance of daily activities, as well as other measures of quality of life [8–12]. Although IT monotherapy has been successful for many patients with spasticity or chronic pain, others have not seen significant changes in their symptoms, function, or quality of life after initiation of IT monotherapy. Patients who receive ITB with refractory spasticity and chronic pain after maximizing oral pharmacotherapy may benefit from a second IT agent [2–4].
ITB has been combined with morphine, clonidine, bupivacaine, and ziconotide to improve function and quality of life in adult patients. For example, combination IT therapy with baclofen and morphine has demonstrated decreased pain associated with spasticity and spinal cord injury, and this combination has been shown to reduce neuropathic pain and lower back pain [3, 4, 13, 14]. ITB and morphine has also been successful for a patient with a below-knee amputation who thereafter experienced improved neuropathic pain, higher function in activities of daily living, improved sleep, and increased physical activity [14]. ITB and clonidine or bupivacaine has been used to reduce lower limb pain and neuropathic pain [15–17]. A poly-analgesic combination of ITB, morphine, and clonidine has also reduced severe spasticity-related pain [18]. Combination IT therapy doses in the literature have ranged from 5–1700 mcg of baclofen per day, 12–33 mcg of clonidine per day, 800-2500 mcg of morphine per day, and 1.7–14.4 mcg of ziconotide per day [14, 15, 17, 19, 20].
Few side effects and adverse events have been reported for combination IT therapy, and those that were reported were common for individual pharmacotherapies rather than an effect of the combination of medications. For example, three patients receiving ITB and morphine in a study by Saulino (2012) reported subjective cognitive dysfunction and sedation that caused them to return to strictly using ITB, and eight patients reported constipation, nausea, and fatigue related to the morphine in their pumps but were able to tolerate combination therapy for at least one year [4].
Research on combination medication pump therapy for the management of spasticity and pain syndromes exists primarily in the adult population. However, no evidence-based guidelines are available for the pediatric population. The aim of this study was to evaluate the use of combination IT medication delivery on function, pain, and quality of life for patients with pediatric-onset disabilities.
2Methods
Patients in an outpatient pediatric rehabilitation clinic were included in this case series if they experienced spasticity and pain that were managed with a combination of ITB and IT analgesia. Fifty patients in the clinic had ITB pumps. A total of nine patients with combination IT medication were identified; however, only eight were included in this case series as one pump was explanted due to infection which did not allow sufficient time to assess effectiveness of combination medication. IT bupivacaine was selected as the first-line analgesic medication to use in all patients due to lowest risk of respiratory depression, cognitive dysfunction, sedation, or respiratory depression. IT morphine was selected as an analgesic medication in those patients who did not achieve adequate pain control with bupivacaine. IT clonidine was selected as an analgesic medication in those patients experiencing pain when there was a concern for respiratory complications with morphine or in attempts to target neuropathic pain. The authors conducted a retrospective review of these patient’s electronic medical records, followed by a phone survey with each patient and their family/caregiver. Per electronic medical record review, documentation of primary movement disorder type was noted, along with patient and/or caregiver subjectively-reported significance of effect on function, activities of daily living, and severity of symptoms.
A four-question telephone survey was conducted to gather information from the families/caregivers of the eight patients regarding improvements in pain, spasticity, function, and quality of life after the initiation of combination IT medication therapy. The families were called once by staff to alert them that a survey was going to be conducted via telephone, and a second call was conducted by a resident physician for completion of the survey. Informed consent was obtained for all participants. This study was approved by the Institutional Review Board.
3Results
The age range of included patients was 5–27 years of age (median age of 21 years). Of the eight patients included in this case series, six carried a diagnosis of cerebral palsy, and one each with Leigh syndrome and stroke. For the six patients with available Gross Motor Function Classification System (GMFCS) and Manual Ability Classification System (MACS) classification, all were GMFCS V and MACS 4–5. Table 1 shows the type of movement disorder pattern noted among patients.
Table 1
Summary of patient characteristics
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | Case 8 | |
| GMFCS | V | V | V | V | N/A | V | N/A | V |
| MACS | 4 | 4 | 5 | 5 | N/A | 5 | N/A | 4 |
| Diagnosis | CP spastic tetraplegia | CP spastic tetraplegia | CP spastic tetraplegia | CP spastic tetraplegia, seronegative myasthenia gravis | Leigh syndrome, ADEM | CP spastic-athetoid tetraplegia | Left frontoparietal hemorrhagic stroke, bilateral medullary strokes, Guillain-Barre, sickle cell disease, focal epilepsy | CP spastic tetraplegia |
| Dystonia | No | No | No | No | Yes | Yes | Yes | No |
| Spasticity | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Choreoathetosis | No | No | No | No | No | Yes | No | No |
| Pain | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Initial Pain Location | Left hip/buttocks | Right foot, left hip subluxation | Right hip/anterior thigh | Bilateral hips, neck | Sensitivity in arms and legs | Low back, headaches | Left hip | Lower extremities |
| Age at Insertion | 16 y/o | 8 y/o | 18 y/o | 6 y/o | 4 y/o | 8 y/o | 12 y/o | 18 y/o |
| Age at Transition | 19 y/o | 17 y/o | 20 y/o | 18 y/o | 4 y/o | 20 y/o | 19 y/o | 25 y/o |
| Current Age | 21 y/o | 20 y/o | 20 y/o | 22 y/o | 6 y/o | 22 y/o | 22 y/o | 27 y/o |
| ITB Pump Mode | Simple continuous | Simple continuous | Simple continuous | Flex ->simple continuous | Simple continuous | Flex | Simple continuous | Flex |
| Baclofen Dose before Transition | 1035.9 mcg/day | 1032.9 mcg | 605.1 mcg/day | 900.2 mcg/day | 425 mcg/day | 1076.4 mcg/day | 1140 mcg/day | 630.6 mcg/day |
| Combination Therapy | Baclofen 1035.9 mcg/day, Bupivacaine 4.1435 mg/day | Baclofen 1250.7 mcg/day, Bupivacaine 10.006 mg/day, Clonidine 93.80 mcg/day | Baclofen 605.1 mcg/day, Bupivacaine 3.328 mg/day | Baclofen 1155.2 mcg/day, Bupivacaine 2.3103 mg/day | Baclofen 424.6 mcg/day, Bupivacaine 2.123 mg/day, Morphine 0.064 mg/day | Baclofen 1106.2 mcg/day, Bupivacaine 2.7655 mg/day | Baclofen 1050.5 mcg/day, Bupivacaine 6.828 mg/day, Clonidine 84.08 mcg/day | Baclofen 631 mcg/day, Bupivacaine 1.4198 mg/day |
| Oral Medications Prior to Transition | Diazepam 2 mg qHS, Tizanidine 2 mg TID, Baclofen 30 mg TID | Baclofen 15/10/15 mg, Hydrocodone/acetaminophen 5–325 mg q4, Toradol PRN, Gabapentin 300/300/600 mg, Amitriptyline 25 mg qHS, Diazepam 5 mg q6 | Baclofen 30 mg TID, Acetaminophen 325 q4 PRN | Clonazepam 0.5 mg qHS, Tizanidine 4/2/4 mg, Gabapentin 300/300/600 mg, Amitriptyline 25 mg qHS | Cyproheptadine 0.5 mg qHS, Clonazepam 1 mg TID, Clonidine 0.1 mg qHS, Diazepam 8 mg QID PRN, Gabapentin 600 mg TID, Morphine 7.5 mg TID, Trihexyphenidyl 2 mg TID, Carbidopa 25-Levodopa 100, Tizanidine 2 mg TID, Nortriptyline 20 mg qHS | Baclofen 20 mg TID, Trihexyphenidyl 5 mg TID, Clonazepam 0. 5 mg daily | Ibuprofen 600 QID PRN, Baclofen 60 mg TID, Hydromorphone 4 mg q4, Naproxen 500 mg BID PRN | Tizanidine 4 mg qHS, Risperidone 3 mg qHS |
| Current Oral Medications | Diazepam 5 mg qHS, Ibuprofen PRN | Hydrocodone/acetaminophen 5–325 mg q4 PRN, Amitriptyline 50 qHS, Diazepam 5 mg QID | None | Diazepam 5 mg BID, Dantrolene 50 mg BID | Carbidopa 25-Levodopa 100 2 tabs BID, Clonidine 0.2 mg qHS, Diazepam 8 mg QID PRN, Gabapentin 600 mg TID, Nortriptyline 30 mg qHS | Diazepam 5 mg qHS PRN, Trihexyphenidyl 7.5 mg BID | Gabapentin 250 mg q6 | Risperidone 3 mg qHS |
| Injections Prior to Transition | Botox 600 units - Biceps brachii 75 units - Brachioradialis 50 units - Flexor digitorum superficialis 50 units - Medial and lateral hamstrings 125 units | Botox - Quadriceps - Hamstrings - Triceps - Biceps brachii | Botox 500 units - Hip adductors - Hamstrings | Botox 400 units - Medial hamstrings 150 units - Biceps brachii 50 units - Flexor carpi ulnaris 25 units - Flexor carpi radialis 25 units Lidocaine to right trapezius | Botox 500 units - Soleus - Left flexor carpi radialis | Botox 500 - Hip adductors - Quadriceps | Dysport - Trapezius - Biceps brachii - Bilateral medial and lateral hamstrings - Left quadriceps - Left posterior tibialis | None |
| Current Injections | None | None | Botox 600 units - Hip adductors - Quadriceps - Hamstrings | Botox 200 units q6 months - Neck, right forearm | None | None | Botox 400 units q6 months - Right trapezius, right splenius capitus, right semispinalis capitis, obliquus capitis inferior, levator scapulae, biceps, pronator teres, flexor digitorum superficialis, opponens pollicis | None |
| Attempted Serial Casting | Yes, failed due to spasticity | Yes | No | No | No | No | No | No |
| Spinal Bracing Used | TLSO | TLSO | TLSO | TLSO | None | TLSO | Didn’t tolerate TLSO due to discomfort and breathing difficulty | None |
| Location of Intractable Pain | Left hip, buttocks | Back, left hip, right lower extremity | Back, right hip | Neck, right trapezius, back, right hip, bilateral lower extremities | Extremities, buttocks, back | Back, bilateral lower extremities | Neck, bilateral hips | Bilateral hips |
Footnote: ADEM = acute disseminated encephalomyelitis. BID = twice a day. CP = cerebral palsy. GMFCS = Gross Motor Function Classification System. ITB = intrathecal baclofen. MACS = Manual Ability Classification System. mg = milligrams. mcg = micrograms. PRN = as needed. q4 = every four hours. q6 = every six hours. qHS = at night. QID = four times a day. TID = three times a day. TLSO = thoracic-lumbar-sacral orthosis. y/o = years old.
All of the patients were transitioned to a combination IT medication due to pain that remained uncontrolled despite maximization of ITB dosing in combination with conservative measures and oral opioids. Significant variability in duration of management of spasticity with ITB was noted prior to this transition. All eight patients were initiated with a combination of ITB and bupivacaine. Four patients required a third medication for symptomatic control of pain. Following the initiation of the combination IT medication therapy, 87.5% (n = 7) of patients noted significant improvement in spasticity, 75% (n = 6) noted significant improvement in pain, and 75% (n = 6) reported improvement in function. The most notable finding was that 87.5 % (n = 7) of patients reported an improvement in their quality of life with their pump after initiation of multiple IT medications. The complete survey results are shown in.
Table 2
Survey responses after pump initiation with combination baclofen and analgesia
| Survey Item | % (n) | ||
| Significantly | Somewhat | Not At All | |
| Has your spasticity improved since initiation of the combination pump? | 50% (4) | 37.5% (3) | 12.5% (1) |
| Has your pain improved since initiation of the combination pump? | 25% (2) | 50% (4) | 25% (2) |
| Has the combination pump improved your function? | 50% (4) | 25% (2) | 25% (2) |
| Has the combination pump improved your quality of life? | 62.5% (5) | 25% (2) | 12.5% (1) |
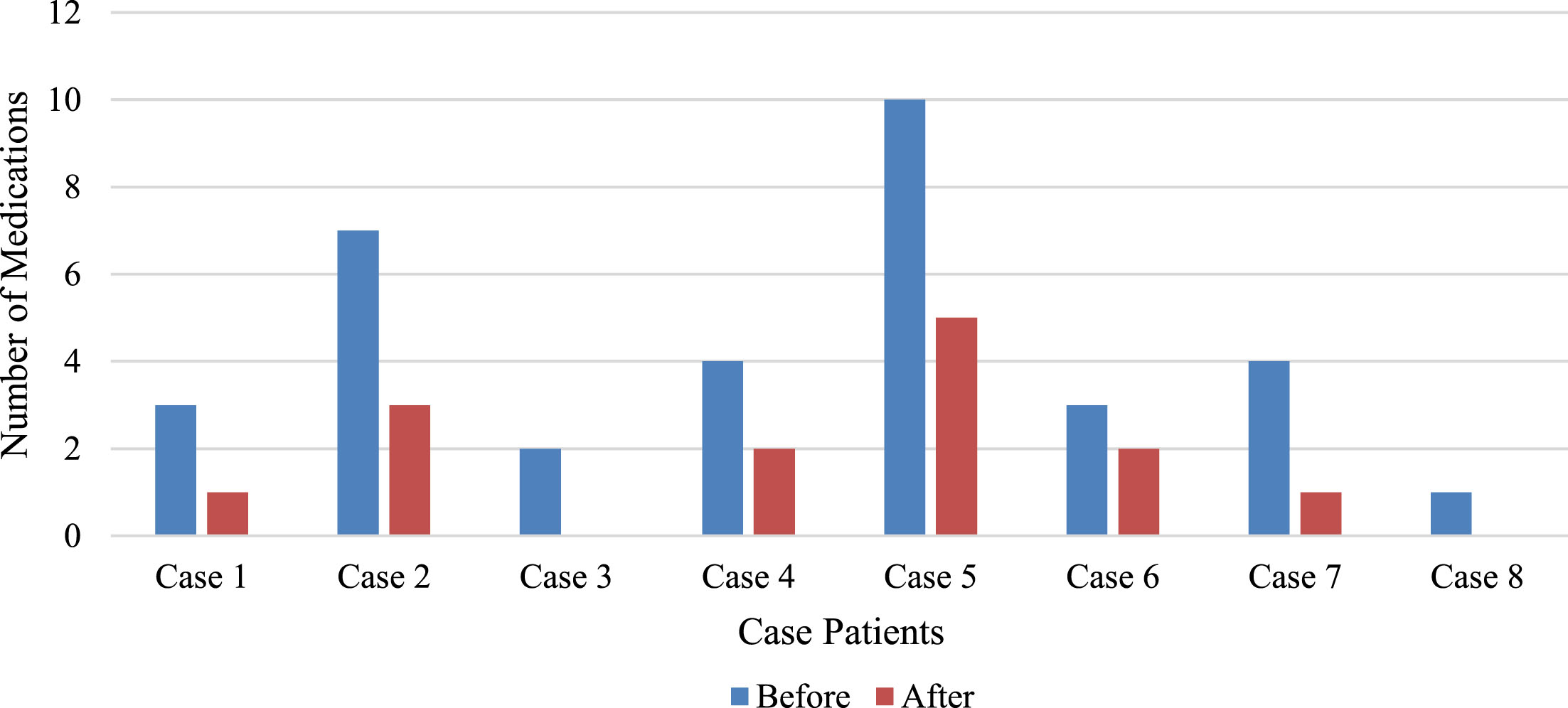
Seven of the eight patients (87.5%) had a history of receiving a combination of toxin injections, bracing, and serial casting in addition to their ITB pump for management of spasticity prior to transitioning to a combination IT therapy. Only three of the patients (37.5%) with combination IT therapy required these interventions at the time of the survey. All eight patients reduced utilization of daily oral anti-spasticity and analgesic medications after initiation of their combination IT pump. The average number of daily oral anti-spasticity and analgesic medications decreased from 4.25 medications to 1.88 medications after initiation of their combination IT medication as seen in Figure 1.
Fig. 1
Number of oral medications before and after combination intrathecal medication therapy.
ITB dosing remained relatively stable prior to and after initiation of the combination IT medication. The mode of IT delivery included flex dosing mode (n = 3), simple continuous (n = 4), and simple continuous with patient-initiated self-bolus dosing (n = 1), as shown in Table 1. Prior to initiation of combination IT medication, all patients were trialed with varied dosing patterns in an attempt to maximize the benefit of IT monotherapy. Ultimate dosing modes were selected based on the patient needs to optimize function and manage symptoms. One patient required the use of self-bolus dosing to control symptoms due to need for boluses at varied times during the day in order to maximize the effectiveness of IT therapy without worsening symptoms of concurrent medical conditions. Dosing patterns were unchanged with the addition of a third IT medication and not dependent on the IT combination medications selected. Prior to initiation of combination IT therapy, malfunction of pumps and catheter were thoroughly assessed and ruled out. Complications remained consistent with those described for ITB monotherapy, and no additional complications were experienced.
4Case presentations
4.1Case 1
A 21-year-old male with spastic tetraplegic cerebral palsy, GMFCS V, MACS 4, and a history of left hip dislocation experienced significant spasticity, with a Modified Ashworth Score of 3 in bilateral lower extremities, particularly in hip flexors resulting in severe hip and buttock pain. An ITB pump was placed at age 16 and titrated to 1035.9 mcg/day. Additionally, he was taking oral diazepam at night, tizanidine four times a day, and baclofen three times per day, as well as receiving toxin injections every three months. He was initiated on combination ITB and bupivacaine at age 19. His IT dose was titrated to effectiveness at baclofen 1035.9 mcg/day and bupivacaine 4.14 mg/day. After successful initiation, he was weaned off the majority of his oral medications and currently remains only on diazepam at night and ibuprofen as needed. He has not required any additional toxin injections since starting combination IT medication.
4.2Case 2
A 20-year-old female with spastic tetraplegic cerebral palsy, GMFCS V, MACS 4 had significant hip flexor and adductor spasticity and a painful left hip subluxation status post total hip arthroplasty. At age 8, she had an IT pump placed and baclofen dosing was titrated to 1032 mcg/day. She was started on multiple oral medications for persistent hip pain including gabapentin and baclofen three times a day, diazepam four times a day, and opioids including hydrocodone/acetaminophen every four hours. Additionally, she was receiving toxin injections every three months with the goal of pain relief. She was initiated at age 17 on combination ITB and bupivacaine, and the dose was titrated. She underwent several additional operative interventions for her hip pain. One year later, with her pain still not controlled, clonidine was added to her IT combination. After titration, her IT dosing has been baclofen 1250 mcg/day, bupivacaine 10.01 mg/day, and clonidine 93.80 mcg/day. Her oral regimen has decreased to amitriptyline at night, diazepam as needed, and hydrocodone/acetaminophen every four hours as needed. She no longer requires toxin injections.
4.3Case 3
A 20-year-old male with a history of spastic tetraplegic cerebral palsy, GMFCS V, MACS 5 experienced significant spasticity resulting in right hip dislocation and severe neuromuscular scoliosis. He was initiated on ITB therapy at age 18, and the dose was titrated to 605.1 mcg/day. In addition to his ITB pump, he required toxin injections into iliopsoas, adductor, and hamstring muscles every three months, as well as oral baclofen three times a day. IT combination of baclofen and bupivacaine was initiated at age 20 for persistent hip pain, and his dose was titrated to baclofen 605.1 mcg/day and bupivacaine 3.33 mg/day. He was weaned off all oral medications and now receives toxin injections intermittently.
4.4Case 4
A 22-year-old female with spastic tetraplegic cerebral palsy, GMFCS V, MACS 4 with severe spasticity in all extremities and cervical dystonia was initiated on ITB pump therapy at age seven and titrated to 900.2 mcg/day. Concurrently, she was receiving clonazepam, gabapentin, and tizanidine three times per day, amitriptyline at night, and toxin injections to her neck and all extremities every three months. She underwent multiple soft tissue releases and lengthening procedures. Her pump was revised, and a catheter was replaced due to the end of battery life. She developed worsened neck and hip pain that was no longer relieved with her regimen. Combination ITB and bupivacaine was initiated at age 18 but did not adequately alleviate her pain. A trial of ITB and hydromorphone was trialed due to an allergy to morphine but resulted in nausea and was discontinued. Combination ITB and ziconotide was placed but did not alleviate her pain. This combination was then replaced, and the programming was adjusted to flex dosing; she reported relief during bolus periods. Thus, the concentrations of both IT medications were decreased in order to increase the drip rate into the cerebral spinal fluid from the pump. A diagnosis of autoimmune seronegative myasthenia gravis was made, and treatment started. Presently, she is being treated with combination IT medications with baclofen at 1155.2 mcg/day and bupivacaine at 2.3103 mg/day. She remains on clonazepam at night, dantrolene as needed, and toxin injections no more than twice per year for spasticity affecting positioning or function.
4.5Case 5
A 6-year-old male with Leigh Syndrome and severe dystonia and spasticity as well as allodynia in extremities initiated ITB pump therapy at age 4 after toxin injections and ten medications failed to control his movement disorder. During titration of IT dosing, he had a paradoxical reaction once his baclofen dose exceeded 600 mcg/day. The dose was lowered, and he was started on combination IT medications at age 4 with dosing titrated to baclofen 425 mcg/day and bupivacaine 2.123 mg/day. His spasticity and dystonia improved but his pain remained uncontrolled. Clonidine was added to his IT combination but resulted in increased irritability and agitation. He was returned to the previous combination with toxin injections that failed. Due to increased requirements of opioids for pain control, IT morphine was added to the baclofen and bupivacaine combination. Now at age 6, his IT medications are baclofen 423.7 mcg/day, bupivacaine 2.12 mg/day, and morphine 0.064 mg/day. He has weaned off oral opioids and toxin injections, and his oral spasticity/dystonia regimen has decreased from ten to five medications. This patient was able to discontinue cyproheptadine, clonazepam, morphine, trihexyphenidyl, and tizanidine. He remains on carbidopa-levodopa and clonidine at original dose and frequency and uses diazepam, gabapentin, and nortriptyline at reduced dose or frequency.
4.6Case 6
A 22-year-old male with mixed tetraplegic cerebral palsy, GMFCS V, MACS 4, with severe spasticity, dystonia, and choreoathetosis initiated ITB pump therapy at age eight. Single-event multilevel surgery was performed at age 14. Despite these interventions, he was requiring oral baclofen and trihexyphenidyl three times a day and toxin injections every three months to control his movement disorder. At age 20, his pain remained poorly controlled, and he was started on combination ITB and bupivacaine titrated to baclofen 1106 mcg/day and bupivacaine 2.77 mg/day. Now age 22, he remains on diazepam at night and trihexyphenidyl twice daily. He no longer requires toxin injections.
4.7Case 7
A 22-year-old male with a history of sickle cell disease suffered bilateral medullary stroke and left frontoparietal stroke with hemorrhagic conversion at age 11. He has resultant severe spastic tetraplegia, cervical dystonia, and chronic pain from sickle cell disease and neuropathy from his multiple strokes. ITB therapy was initiated at age 12. His pain remained uncontrolled after developing avascular necrosis of bilateral femoral heads due to recurrent bone infarcts. At age 19, he was started on combination IT therapy with baclofen and bupivacaine, which improved somatic and bone-related pain. He also suffered from Guillain-Barre syndrome after a viral infection and developed persistent neuropathic pain. As a result, clonidine was added to his IT combination. The dose was titrated to baclofen 1050.5 mcg/day, bupivacaine 6.28 mg/day, and clonidine 84.08 mcg/day. His oral medications were decreased from four medications to one scheduled and two as needed. He continues to receive toxin injection twice a year for cervical dystonia.
4.8Case 8
A 27-year-old male with spastic tetraplegic cerebral palsy, GMFCS V, MACS 4, complicated by bilateral hip dislocations, initiated ITB therapy at age 18. His hip pain progressed and was supplemented with oral baclofen. At age 25, he was started on combination IT medications of baclofen and bupivacaine titrated to baclofen 631 mcg/day and bupivacaine 1.42 mg/day. His oral baclofen was discontinued.
5Discussion
This case series represents the utility of combination medications in IT pumps for the treatment of severe spasticity and chronic pain in patients with childhood-onset disability. It demonstrates that initiation of combination IT therapy can result in improved function, pain, and quality of life, as well as a significant decrease in the need for supplemental or concurrent treatment with oral medications.
Pediatric patients with spasticity from cerebral palsy experience spasticity-related pain at rates as high as 80–85% [21]. Although irreversible procedures such as selective dorsal rhizotomy (SDR) exist for patients with intractable spasticity, they are invasive and carry high risks of neurologic injury [22]. Furthermore, ITB has demonstrated increased improvements in pain when compared to SDR [23]. Therefore, using IT medications to manage both spasticity and pain should be strongly considered by pediatric physiatrists and neurosurgeons.
There is minimal research in adult populations and no research in pediatric populations regarding the use of IT pumps for administration of multiple medications. Furthermore, little is known regarding long-term effects of spasticity and pain management using a combination of IT medications. This creates a significant need for continued longitudinal research in this population to improve outcomes for pediatric patients with spasticity and chronic pain. Future studies should also consider which types of pain (e.g., neuropathic, nociceptive) are most alleviated by IT pumps with combination therapy.
6Limitations
Limitations of this study are related to the case series design, including selection bias and lack of a control group for comparison. Furthermore, perspectives from caregivers and/or families were relied upon, as all patients were not able to answer survey questions independently due to cognitive impairment or lack of a functional communication device. Recall bias may have also influenced participant responses to the survey questions. Rather than using a validated survey, questions were created that were most unique to the patient population. In the questions related to pain, the family/caregiver was not asked to specifically characterize the type of pain. Pain in this population can often be multifactorial and can also be difficult to discern. A relatively small sample size with great heterogeneity of diagnoses makes this case series more challenging to generalize to the greater population. However, given the limited existing literature on combination IT medication pump therapy for spasticity and pain management in patients with childhood-onset disabilities, this case series contributes substantial consideration for future practice.
7Conclusion
This case series demonstrates success in using combination IT medication delivery to improve spasticity, pain, function, and quality of life in patients with pediatric-onset disabilities. This is the first case series to outline the use and effectiveness of combination IT drug therapy in this population. The results suggest safety and benefit in this patient population in areas of pain and spasticity. Additional studies are warranted to further quantify this benefit and to directly compare it to traditional ITB therapy. Given that 75% of people living with cerebral palsy experience pain, there is an indication for combination IT therapy as a treatment option for these patients [24]. The use of combination antispasmodic and analgesic IT drug therapy should be considered in the management of patients with childhood-onset disabilities who have both severe spasticity and severe chronic pain.
Acknowledgment
None.
Declaration of interest
No financial or other interests related to this manuscript.
Ethical considerations
This study was approved by the Institutional Review Board and verbal informed consent was sought and received from each participant.
References
[1] | Belverud S , Mogilner A , Schulder M . Intrathecal pumps. INeurotherapeutics. (2008) ;5: (1):114–122.doi: 10.1016/j.nurt.2007.10.070. |
[2] | Duarte R , Raphael J , Eldabe S . Intrathecal drug delivery for the management of pain and spasticity in adults: an executive summary of the British Pain Society’s recommendations for best clinical practice. IBr J Pain. (2016) ;10: (2):67–69.doi: 10.1177/2049463715587747. |
[3] | Sadiq SA , Poopatana CA . Intrathecal baclofen and morphine in multiple sclerosis patients with severe pain and spasticity. IJ Neurol. (2007) ;254: (10):1464–1465.doi: 10.1007/s00415-007-0566-z. |
[4] | Saulino M . The use of intrathecal baclofen in pain management. IPain Manag. (2012) ;2: (6):603–608.doi: 10.2217/pmt.12.60. |
[5] | Winter G , Beni-Adani L , Ben-Pazi H . Intrathecal baclofen therapy-practical approach: Clinical benefits and complication management. IJ Child Neurol. (2018) ;33: (11):734–741.doi: 10.1177/0883073818785074. |
[6] | Vender JR , Hester S , Waller JL , Rekito A , Lee MR . Identification and management of intrathecal baclofen pump complications: a comparison of pediatric and adult patients. IJ Neurosurg. (2006) ;104: (1 Suppl):9–15.doi: 10.3171/ped.2006.104.1.9. |
[7] | Boster AL , Adair RL , Gooch JL ,et al Best Practices for Intrathecal Baclofen Therapy: Dosing and Long-Term Management. INeuromodulation. (2016) ;19: (6):623–631 10.1111/ner.12388. |
[8] | Eek MN , Olsson K , Lindh K ,et al Intrathecal baclofen in dyskinetic cerebral palsy: effects on function and activity. IDev Med Child Neurol. (2018) ;60: (1):94–99.doi: 10.1111/dmcn.13625. |
[9] | Creamer M , Cloud G , Kossmehl P , et al Effect of Intrathecal Baclofen on Pain and Quality of Life in Poststroke Spasticity. IStroke. (2018) ;49: (9):2129–2137.doi: 10.1161/STROKEAHA.118.022255. |
[10] | Albright AL , Barry MJ , Shafton DH , Ferson SS . Intrathecal baclofen for generalized dystonia. IDev Med Child Neurol. (2001) ;43: (10):652–657.doi: 10.1017/s0012162201001190. |
[11] | Armstrong RW , Steinbok P , Cochrane DD , Kube SD , Fife SE , Farrell K . Intrathecally administered baclofen for treatment of children with spasticity of cerebral origin. IJ Neurosurg. (1997) ;87: (3):409–414.doi: 10.3171/jns.1997.87.3.0409. |
[12] | Hoving MA , van Raak EP , Spincemaille GH , Palmans LJ , Becher JG , Vles JS . Efficacy of intrathecal baclofen therapy in children with intractable spastic cerebral palsy: a randomised controlled trial. IEur J Paediatr Neurol. (2009) ;13: (3):240–246.doi: 10.1016/j.ejpn.2008.04.013. |
[13] | Gatscher S , Becker R , Uhle E , Bertalanffy H . Combined intrathecal baclofen and morphine infusion for the treatment of spasticity related pain and central deafferentiation pain. IActa Neurochir Suppl. (2002) ;79: 75–76.doi: 10.1007/978-3-7091-6105-0_16. |
[14] | Zuniga RE , Schlicht CR , Abram SE . Intrathecal baclofen is analgesic in patients with chronic pain. IAnesthesiology. (2000) ;92: (3):876–880.doi:10.1097/00000542-200003000-00037. |
[15] | Middleton JW , Siddall PJ , Walker S , Molloy AR , Rutkowski SB . Intrathecal clonidine and baclofen in the management of spasticity and neuropathic pain following spinal cord injury: a case study. IArch Phys Med Rehabil. (1996) ;77: (8):824–826.doi: 10.1016/s0003-9993(96)90264-6. |
[16] | Schechtmann G , Lind G , Winter J , Meyerson BA , Linderoth B . Intrathecal clonidine and baclofen enhance the pain-relieving effect of spinal cord stimulation: a comparative placebo-controlled, randomized trial. INeurosurgery. (2010) ;67: (1):173–181.doi: 10.1227/01.NEU.0000370249.41634.4F. |
[17] | Sanders JC , Gerstein N , Torgeson E , Abram S . Intrathecal baclofen for postoperative analgesia after total knee arthroplasty. IJ Clin Anesth. (2009) ;21: (7):486–492.doi: 10.1016/j.jclinane.2008.12.019. |
[18] | Anastassiou E . Combined intrathecal baclofen, morphine and clonidine infusion for complex pain syndromes due to spasticity. IReg Anesth Pain Med. (2005) ;30: (5):44.doi: 10.1016/j.rapm.2005.07.044. |
[19] | Deer TR , Prager J , Levy R ,et al PolyanalgesicConsensus Conference 2012: recommendations for the management of pain by intrathecal (intraspinal) drug delivery: report of an interdisciplinary expert panel Neuromodulation. (2012) ;15: (5):436–464.doi: 10.1111/j.1525-1403.2012.00476.x. |
[20] | Saulino M , Burton AW , Danyo DA , Frost S , Glanzer J , Solanki DR . Intrathecal ziconotide and baclofen provide pain relief in seven patients with neuropathic pain and spasticity: case reports. IEur J Phys Rehabil Med. (2009) ;45: (1), 61–67. |
[21] | Heinen F , Bonfert M , Kaňovský P , et al Spasticity-relatedpain in children/adolescents with cerebral palsy. IPart Prevalenceand clinical characteristics from a pooled analysis. J PediatrRehabil Med. (2022) ;15: (1):129–143.doi: 10.3233/PRM-220011. |
[22] | Kakodkar P , Girgis H , Nabhan P , Chee SS , Tu A . Efficacy of Selective Dorsal Rhizotomy and Intrathecal Baclofen Pump in the Management of Spasticity. IAdv Tech Stand Neurosurg. (2022) ;45: 379–403.doi: 10.1007/978-3-030-99166-1_13. |
[23] | Barney CC , Merbler AM , Stansbury J ,et al Musculoskeletal Pain Outcomes Pre- and Post Intrathecal Baclofen Pump Implant in Children With Cerebral Palsy: A Prospective Cohort Study. IArch Rehabil Res Clin Transl. (2020) ;2: (2):100049.doi: 10.1016/j.arrct.2020.100049. |
[24] | Peterson MD , Haapala H , Kamdar N , Lin P , Hurvitz EA . Pain phenotypes among adults living with cerebral palsy and spina bifida. IPain. (2021) ;162: (10):2532–2538.doi: 10.1097/j.pain.0000000000002240. |


