
Safety of botulinum toxin injections in children less than one year old: A retrospective chart review
Abstract
PURPOSE:
Infants can have muscle hypertonia due to cerebral palsy, muscle strength imbalances due to brachial plexus palsy, refractory clubfoot, and torticollis. These muscle problems can cause significant development impairments. A child with severe sialorrhea and dysphagia from leukodystrophy can aspirate, causing respiratory problems. Botulinum toxin (BoNT) injections can improve these conditions but may lead to adverse effects from the toxin spreading to non-targeted muscles, potentially impacting breathing, swallowing, and overall strength. This is particularly concerning in infants. This study assessed the safety of BoNT injections in children less than one year of age.
METHODS:
This was a retrospective cohort study.
RESULTS:
Forty-seven patients (22 male, 25 female) received BoNT injections before one year of age (three to 12 months). Thirty-seven received one round of injections and 10 were injected on multiple occasions. Forty-five received onabotulinumtoxinA (15–100 units [U], 1.9–15.2 U/kg), one received abobotulinumtoxinA (70 U, 9.0 U/kg), and one received incobotulinumtoxinA (25 U, 3.5 U/kg). Lower extremities were treated in 15 patients, upper extremities in 38, the sternocleidomastoid in two, and the salivary glands in one. Forty-five patients had no reported complications. One experienced transient fever, vomiting, and diarrhea. The parent of another reported subjective weakness in one muscle.
CONCLUSION:
BoNT injections in children less than one year of age appear to be safe.
1Introduction
Cerebral palsy (CP) affects between two and 2.5 in 1000 children, making it the most common cause for childhood disability [1]. About 80% of children with CP have spasticity [2], which can interfere with function and development, cause discomfort, and make care difficult [3]. Spasticity is defined as increased, involuntary, velocity-dependent muscle tone that causes resistance to movement and increased stretch reflex [4, 5]. Hypertonia can be reduced with focal injections of BoNT [6].
In addition to cerebral palsy, neonatal brachial plexus injuries occur 1.5 to 2.6 times per 1000 births [7, 8]. These injuries can cause muscle strength imbalances, shoulder subluxations, and contractures [9]. Typically, these injuries result in a very weak bicep, because of C5 and C6 cervical nerve root involvement [9, 10]. Injections to the triceps can weaken the triceps enough to allow the weak biceps to contract against less opposition, thus improving the potential to develop more strength [9]. Similarly, congenital torticollis can cause muscle imbalances, which can also be seen in clubfeet. BoNT has been used in managing congenital torticollis [11], sialorrhea [12], and clubfeet [13]. BoNT partially paralyzes muscles by stopping the release of the neurotransmitter acetylcholine from the distal axon at the neuromuscular junction [4, 14, 15]. The effect of onabotulinumtoxinA typically reaches its peak two weeks after the injections and begins to decline about 10 weeks after the injections [15–17]. AbobotulinumtoxinA and incobotulinumtoxinA have similar effects. BoNT can spread outside the target muscle, potentially causing localized and systemic adverse effects [14, 18].
There have been concerns about the side effect profile of BoNT. In April of 2009, the FDA added a black box warning regarding the potential development of unwanted symptoms similar to botulism, including swallowing, breathing difficulties, and even death. They specified that these symptoms were mostly reported in children being treated for CP [19]. These concerns are heightened in infants because BoNT may spread more easily due to their smaller size. AbobotulinumtoxinA (maximum dose 30 U/kilogram [kg] bodyweight [BW] up to 1,000 U), incobotulinumtoxinA (maximum dose 16 U/kg BW up to 400 U), and onabotulinumtoxinA (maximum dose 10 U/kg BW up to 340 U) have been approved to treat pediatric spasticity in children two years and older.
Currently available studies regarding the safety profile of BoNT are inconclusive. Several studies indicated that BoNT A causes few adverse events in the treatment of spasticity in children. However, changes in dose per weight or dilution may alter the adverse event profile. A systematic review by Hernandez [20], which included 20 studies, stated that adverse events were mild in the first few months after injections, but that data was too sparse to draw any conclusions regarding long term safety. O’Flaherty et al. [21] and Langdon et al. [22] concluded that the risks associated with treating spasticity with BoNT A were low, and most likely linked to comorbidities present along with the condition being treated. Paget et al. [23] reported systemic adverse events in up to 3.6% of patients who were classified as Gross Motor Function Classification System (GMFCS) level IV and V, especially those who received higher doses and/or had a history of dysphagia, gastrostomy tube placement, or aspiration pneumonia. They found that a history of dysphagia and/or aspiration pneumonia were the two most likely factors to lead to adverse systemic events after BoNT injections. A study by Naidu et al. [14] also concluded that systemic side effects from BoNT were low, and documented a 1% possibility of urinary incontinence that resolved spontaneously within 1–6 weeks and 1.3% chance of hospital admission due to respiratory symptoms. They found this incidence to correlate with a higher GMFCS level and dose of BoNT. On the other hand, Goldstein [24] concluded it was safe to use high doses of onabotulinumtoxinA up to 22 U/kg or a total dose of 1200 U/treatment. Lee [25] reported that a dilution of 100 U of onabotulinumtoxinA per 8 ml had a higher side effect profile than a dilution of 100 U per 2 ml. Finally, a randomized control trial by Edwards et al. [26], showed no difference in side effect profile between children receiving BoNT injections as opposed to a placebo.
There are no previous studies investigating the adverse effects of BoNT A therapy in children one year of age and younger. Concerns about the unwanted side effects of this treatment are increased because of the small size of infants and the concept that the toxin could spread through the body more easily, potentially harming breathing and swallowing functions. Early intervention to lessen spasticity in children with CP, muscle strength imbalances, and other conditions can be important in helping them use their muscles more effectively, which can foster the development of motor skills [2]. Avoiding treatment with BoNT A in children one year old and younger may further delay motor development.
Clinicians are particularly reluctant to use BoNT in children less than one year of age due to safety concerns. Only one study addressing BoNT in children 11–24 months old [27] was found. In this study, BoNT was injected only into the gastrocnemius muscle, with no major side effects reported. As there have been no studies conducted about the safety of BoNT therapy in infants, this study sought to determine if treatment of children less than one year of age with BoNT is safe.
2Methods
This study was approved by the Institutional Review Board, and the patients’ parents or guardians gave consent to participate. The medical records of all children (infants) less than one year old who were treated with BoNT from 2005 to 2018 were retrospectively reviewed. One patient who was one year 13 days old was included since their age was very close to one year. Information collected included diagnosis, age in months at injection, weights at injection, muscles injected, dose and concentration of botulinum toxin, and any adverse effects reported by the parents. The total dose per kg BW and dose per kg per muscle of BoNT was calculated.
Details about the method of sedation and localization technique were also gathered.
This is a descriptive study and counts of adverse events were reported.
The follow-up data was collected from the patient’s first follow-up visit after the injections, and the timeframe varied from two to 16 weeks (mean nine weeks). All parents were asked about any problems following the injections including but not limited to weakness, swallowing, respiratory or gastrointestinal problems, fever, or any other neurological changes.
3Results
Forty-seven patients, 22 male and 25 female, who received 59 BoNT injections at or before one year 13 days of age were included. Twenty-seven were diagnosed with a brachial plexus injury, 15 with CP, three with clubfoot, one with sialorrhea, and one with congenital torticollis. Patients with CP fell mostly into two groups: quadriplegic CP (7/15) and hemiplegic CP (8/15), in whom hypertonia interfered with development. The patients with brachial plexus injuries represented the cohort of patients seen in a brachial plexus clinic. In this subset, muscle imbalances were leading to contractures and shoulder subluxation from unopposed muscle activity. The patient with sialorrhea had leukodystrophy and chronic respiratory problems from aspirating their oral secretions.
All but two of the patients received onabotulinumtoxinA. One received incobotulinumtoxinA, and another received abobotulinumtoxinA.
Thirty-seven patients received only one round of injections, and 10 patients were injected on multiple occasions before they were one year of age. In those who received multiple injections, the interval between injections varied from 39 to 169 days, with the average interval being 94.7 days.
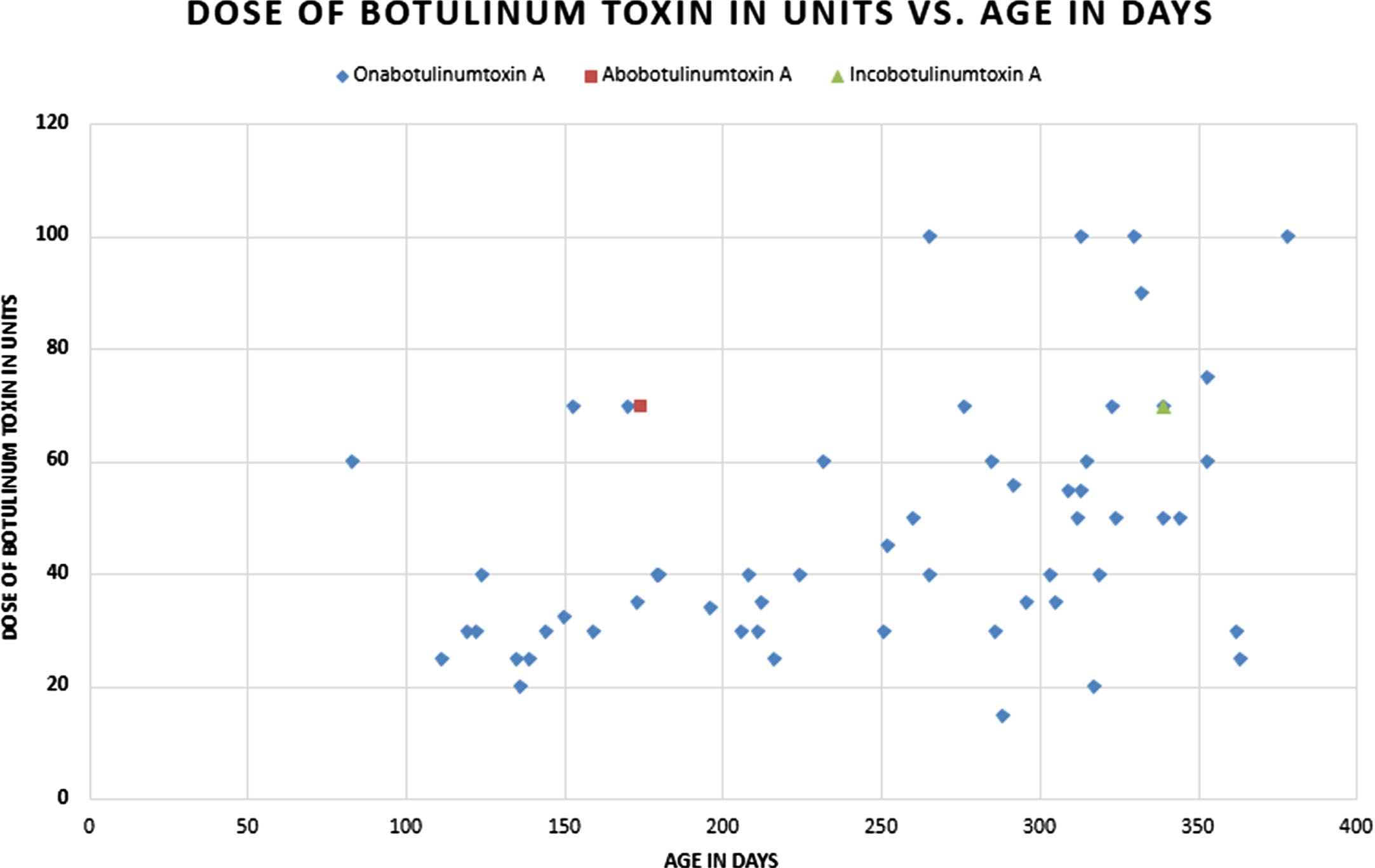
The youngest patient was 83 days old at the time of injections, and the oldest was 379 days old. At the time of injections, all patients’ BW ranged from 5.55 to 12.95 kg, with those receiving incobotulinumtoxinA weighing 7.1 kg and abobotulinumtoxinA 7.8 kg (Fig. 1).
Fig. 1
Dose of Botulinum Toxin in units vs. Age in Days.
None of the brachial plexus or congenital torticollis patients had any other significant developmental problems at the time of the injections. Two of the patients with clubfoot had no other developmental problems, and one with clubfoot had mild cognitive developmental problems from a chromosomal abnormality. Those with CP were eventually classified by the following GMFCS levels: I –4, II –3, III –2, IV –1, V –5. At the time of the injections, the patients with CP were functioning at the following levels: not rolling - 1, not sitting - 9, sitting but not crawling - 1, crawling - 1, walking with hands held - 1. The patient with sialorrhea had leukodystrophy.
Twenty-seven patients had brachial plexus injuries. The distribution of nerve root involvement is as follows: C5-6 - 15, C5-7 - 10, C5-T1 - 2.
Five patients had a single muscle injection, while the remaining patients received injections in multiple muscles. Fifteen were treated in the lower extremities (gastrocnemius-soleus - 8, hamstrings - 1, hip adductors - 2, quadriceps - 2, posterior tibialis - 3), 38 patients were treated in the upper extremities (biceps - 6, triceps - 6, pectoralis - 27, subscapularis - 24, pronator - 7, flexor digitorum profundus - 3, flexor digitorum superficialis - 4, adductor pollicis brevis - 8), two in the sternocleidomastoid, one in the trapezius, one in the suboccipital, and one in the salivary glands.
Twenty-seven patients with brachial plexus palsy (37 rounds of injections) had the following muscles injected by number of times injected: pectoralis - 27, subscapularis - 22, triceps - 3, pronator teres - 1.
Fifteen patients with cerebral palsy (17 rounds of injections) had the following muscles injected by number of times injected: gastrocnemius - 7, hamstrings - 1, hip adductors - 3, biceps - 6, pronator - 5, flexor digitorum profundus - 3, flexor digitorum superficialis - 3, adductor pollicis brevis - 7, pectoralis - 1, quadriceps - 3, and posterior tibialis - 1.
One patient with sialorrhea and leukodystrophy had their bilateral parotids and right submandibular gland injected using ultrasound guidance for a total of 20 units or 2.5 U/kg.
Three patients with clubfeet had the following muscles injected: one received 50 U (7.41 U/kg) into the posterior tibialis, one to the gastrocnemius for a total of 50 U (6.25 U/kg), and one to the gastrocnemius and posterior tibialis totaling 30 U (3.45 U/kg).
The patient with torticollis (two rounds) had the following muscles injected: sternocleidomastoid, trapezius, and suboccipital for a total dose of 60 U (6.6 U/kg).
Dosing by muscle can be found in Tables 1 and 2.
Some doses of BoNT used in this study were outside the FDA approved dosing guidelines for children older than two years. These doses should only be used as a reference regarding adverse events in this study and not as recommended or approved doses of BoNT. These patients received BoNT from various physicians, and dosing varied widely by area injected and the injectors’ clinical judgment.
The total dose of onabotulinumtoxinA used in one round of injections ranged from 15 to 100 U (mean 47.37 U). The units of onabotulinumtoxinA injected per kg BW ranged from 1.93 U/kg to 15.2 U/kg, with a mean of 5.68 U/kg and a standard deviation of 2.71 U/kg. One patient in the data set was treated with a 50 U/milliliter (mL) concentration rather than a 100 U/mL concentration of onabotulinumtoxinA. This patient was given injections into their bilateral hamstrings (40 U, 6.08 U/kg per hamstring) and left sternocleidomastoid muscle (20 U, 3.04 U/kg), for a total of 100 U or 15.2 U/kg, which was the highest in this study. One patient received abobotulinumtoxinA at a concentration of 200 U/mL with injections into their left pectoralis and subscapularis, for a total of 70 U or 8.97 U/kg. Another received incobotulinumtoxinA at a concentration of 100 U/mL with injections into the right pectoralis and subscapularis, for a total of 25 U or 3.52 U/kg. (See Table 1 and Table 2.)
Table 1
Frequency of muscle injected onabotulinum toxin, dose range and average
| Muscle injected with onabotulinumtoxinA | Number of patients (total number of muscles injected) | Dose range in units | Average dose in units | Dose range in U/kg | Average dose in U/kg |
| Gastrocnemius | 8 (12) | 5–50 | 26.25 | .59–7.28 | 3.22 |
| Hamstrings | 1 (2) | 40 | 40 | 6.08 | 6.08 |
| Hip Adductors | 2 (5) | 5–15 | 5 | .59–1.27 | 0.87 |
| Posterior Tibialis | 3 (3) | 10–50 | 21.67 | .59–7.41 | 3.05 |
| Quadriceps Femoris | 2 (5) | 17–30 | 24 | 1.85–4.00 | 2.69 |
| Biceps | 7 (9) | 5–40 | 18.33 | .59–4.82 | 2.02 |
| Triceps | 6 (9) | 7.5–30 | 19.44 | 0.83–4.54 | 2.46 |
| FDP | 3 (5) | 10–20 | 12 | 1.11–2.41 | 1.44 |
| FDS | 4 (4) | 10 | 15 | 0.85–2.07 | 1.47 |
| Pronator Teres | 7 (8) | 10–20 | 13.75 | 1.04–2.16 | 1.44 |
| Adductor Pollicis Brevis | 8 (10) | 2.5–15 | 6.51 | 0.3–1.61 | .72 |
| Subscapularis | 20 (25) | 7.5–50 | 15.96 | 0.83–4.31 | 1.82 |
| Trapezius | 1 (2) | 20–35 | 27.5 | 2.22–3.89 | 3.06 |
| Pectoralis | 25 (36) | 5–50 | 23.44 | 0.94–6.4 | 3.03 |
| Suboccipital | 1 (1) | 20 | 20 | 2.22 | 2.22 |
| Sternocleidomastroid | 2 (3) | 15–20 | 18.33 | 1.67–3.04 | 2.31 |
| Parotid glands | 1 (2) | 7–9 | 8 | 0.9–1.1 | 1 |
| Submandibular gland | 1 (1) | 4 | 2 | 0.5 | 0.5 |
| Total | 45 (158) | 15–100 (total body dose) | 16.57 | 2.3–15.2 (total body dose) | 5.82 |
U/kg: units per kilogram body weight, FDP: flexor digitorum profundus, FDS: flexor digitorum superficialis.
Table 2
Frequency of muscle injected abobotulinum toxin, and incobotulinum toxin, dose range and average
| Muscle injected with abobotulinumtoxinA | Number of patients (total number of that muscle injected) | Dose range in units | Average dose in units | Dose range in U/kg | Average dose in U/kg |
| Pectoralis | 1 (1) | 15 | 15 | 2.11 | 2.11 |
| Subscapularis | 1 (1) | 10 | 10 | 1.4 | 1.4 |
| Muscle Injected with incobotulinumtoxinA | |||||
| Pectoralis | 1 (1) | 50 | 50 | 6.41 | 6.41 |
| Subscapularis | 1 (1) | 20 | 20 | 2.56 | 2.56 |
U/kg: units per kilogram body weight.
Only two patients reported any adverse events. One received onabotulinumtoxinA into their bilateral gastrocnemii (each gastrocnemius 3.13U/kg and total body dose 6.25U/kg), and the parents reported a week of fever, vomiting, and diarrhea starting one day after the injections. However, there were no adverse events following repeat injections one year later, suggesting that the initial adverse events may have been secondary to an illness unrelated to the BoNT injections. Also, their increased size with growth may have reduced the risk of spread, or they may have increased tolerance to injections with subsequent rounds of BoNT. Another patient’s parent reported subjective weakness in their biceps after one round of onabotulinumtoxinA (right bicep 30 U, 3.1 U/kg, total body dose 70 U, 7.25 U/kg). The patient could still flex their elbow, but the severity and duration of elbow flexion weakness was not documented, and the mild weakness had resolved by their four-month follow-up appointment. This response may have been an expected, dose-related response as the recommended dose for the biceps is 2 U/kg and the dose used was 3.1 U/kg. This patient had no reported adverse events with subsequent injections. The patients who received incobotulinumtoxinA, abobotulinumtoxinA, or 50 U/mL concentration of onabotulinumtoxinA injections did not report any adverse events.
Nine patients received no sedation, 11 received midazolam, 18 nitrous oxide, 20 general anesthesia, and one propofol. Forty-four patients had no skin analgesia, 12 had lidocaine cream, and two had ethyl chloride spray. Of the patients who had no sedation, two had lidocaine skin analgesia and seven had no skin analgesia.
Two patients had palpation guidance, 24 electromyography (EMG), 30 electrical stimulation, one ultrasound, and two had a combination of EMG and electrical stimulation.
4Discussion
Possible adverse effects from BoNT injections can be classified as obligate, local, and systemic. The obligate adverse effect is excessive weakness beyond that to be expected from the treatment in the target muscle. The local adverse effect is weakness in adjacent muscle resulting from diffusion of the toxin locally, and the systemic adverse effect results in weakness in distant muscles caused by diffusion of the toxin systemically [16]. Due to the size of the BoNT A molecule, the toxin is unable to cross the blood brain barrier [15], so systemic adverse effects to the brain are very unlikely. Reported adverse events in the literature include flu-like symptoms, generalized weakness, dysphagia (leading to aspiration pneumonia), lower respiratory involvement, and bladder incontinence, all of which are transient [21, 28].
The results obtained in this retrospective chart review detail the diagnoses, age, and weight at injection, dose per weight, dose per muscle, and adverse effects of the treatment. These results indicated that no significant adverse effects were caused by doses less than 16 U/kg with onabotulinumtoxinA, 9 U/kg with abobotulinumtoxinA, or 4 U/kg with incobotulinumtoxinA injections. The patients had a variety of doses, muscles injected, and conditions treated. The child who received injections in the sternocleidomastoid at age 38 weeks, diluted to 50 U/mL, reported no adverse effects on swallowing or breathing. It seems unlikely that the adverse events seen in the one patient who reported a week of fever, vomiting, and diarrhea starting one day following the first round of injections can be attributed to the BoNT A treatment since the peak effects of the injections are seen about two weeks after injections [15, 17]. Also, this patient received an additional round of injections one year later and reported no adverse events. In the patient who reported transient weakness in their biceps after injections at 39 weeks of age, no report was made about the length of time of weakness or additional weakness in any other muscle groups injected. The weakness had resolved when the patient was seen in follow-up at four months. No further injections in the biceps were needed, but the patient did tolerate multiple rounds of injections in other upper extremity muscles.
The patients treated were a heterogeneous group with varying diagnoses, muscles injected, and doses, which limit strong conclusions. All these patients tolerated the injections well, and although caution should still be used when injecting infants with BoNT, these injections in infants seem to have a similar safety profile relative to older children.
Another weakness of this study is that it was a retrospective chart review; thus, adverse events may have been underreported.
5Conclusion
This study concludes that BoNT A injections in children less than one year of age can be a safe treatment of spasticity and muscle imbalances. No significant adverse effects at doses less than 16 U/kg for onabotulinumtoxinA and injections at least six weeks apart were noted. The numbers of patients in this study were low, and great care should be taken when treating children less than one year of age with BoNT. Further studies on the treatment of young children with BoNT are encouraged.
Acknowledgments
1. Oral platform presentation at the 2016 AAP Annual Meeting in Sacramento, CA, February 18–20, 2016.
2. Accepted for a paper presentation at AACPDM annual meeting September 23–26, 2020.
Conflict of interest
Dr. Gormley reports research and consulting support from Ipsen Pharmaceuticals and Allergan Pharmaceuticals. The other authors have no conflicts of interest to report.
References
[1] | Stavsky M , Mor O , Mastrolia SA , Greenbaum S , Than NG and Erez O . Cerebral Palsy—Trends in Epidemiology and Recent Development in Prenatal Mechanisms of Disease, Treatment, and Prevention. Front Pediatr. (2017) ;5: :21. doi: 10.3389/fped.2017.00021 |
[2] | Russman BS , Tilton A and Gormley ME . Cerebral Palsy: A Rational Approach to a Treatment Protocol and the Role of Botulinum Toxin in Treatment. Muscle Nerv Suppl. (1997) ;6: :S181–93. |
[3] | Gormley ME , O’Brien CF and Yablon SA . A clinical overview of treatment decisions in the management of spasticity. Muscle Nerve Suppl. (1997) ;6: :S14–20. |
[4] | Mayer N and Herman R . Positive Signs and Consequences of an Upper Motor Neuron Syndrome. In: Mayer NH, Brashear A, editors. Spasticity and Other Forms of Muscle Overactivity in the Upper Motor Neuron Syndrome: Etiology, Evaluation, Management, and the Role of Botulinum Toxin. WeMove; 2008. pp. 11-26. |
[5] | Pandey K . Spasticity 415 Clinical Presentation. Medscape [updated 2019 Jun 28; cited 2023 Jun 16]. Available from: https://emedicine.medscape.com/article/2207448-clinical |
[6] | Coghill J . Managing Spasticity in Children: Botulinum Toxin. ACNR. (2012) ;12: (2):26–28. |
[7] | Coroneos CJ , Voineskos SH , Christakis MK , Thoma A , Bain JR and Brouwers MC . Obstetrical brachial plexus injury (OBPI): Canada’s national clinical practice guideline. BMJ Open. (2017) ;7: (1):e014141. doi: 10.1136/bmjopen-2016-014141 |
[8] | Foad SL , Mehlman CT and Ying J . The epidemiology of neonatal brachial plexus palsy in the United States. J Bone Joint Surg Am. (2008) ;90: (6):1258–64. doi: 10.2106/JBJS.G.00853 |
[9] | Buchanan PJ , Grossman JAI , Price AE , Reddy C , Chopan M and Chim H . The use of botulinum toxin injection for brachial plexus birth injuries: a systematic review of the literature. Hand (NY). (2019) ;14: (2):150–4. doi: 10.1177/1558944718760038 |
[10] | Thatte MR and Mehta R . Obstetric brachial plexus injury. Indian J Plast Surg. (2011) ;44: (3):380–9. doi: 10.4103/0970-0358.90805 |
[11] | Joyce MB and de Chalain TMB . Treatment of recalcitrant idiopathic muscular torticollis in infants with botulinum toxin type a. J Craniofac Surg. (2005) ;16: (2):321–7. doi: 10.1097/00001665-200503000-00023 |
[12] | Alvarenga A , Campos M , Dias M , Melão L and Estevão-Costa J . BOTOX-A injection of salivary glands for drooling. J Pediatr Surg. (2017) ;52: (8):1283–6. doi: 10.1016/j.jpedsurg.2016.09.074 |
[13] | Alvarez CM , Tredwell SJ , Keenan SP , et al. Treatment of idiopathic clubfoot utilizing botulinum A toxin: a new method and its short-term outcomes. J Pediatr Orthop. (2005) ;25: (2):229–35. doi: 10.1097/01.bpo.0000149861.50400.db. |
[14] | Naidu K , Smith K , Sheedy M , Adair B , Yu X and Graham HK . Systemic adverse events following botulinum toxin A therapy in children with cerebral palsy. Dev Med Child Neurol. (2010) ;52: (2):139–44. doi: 10.1111/j.1469-8749.2009.03583.x |
[15] | Dressler D and Bigalke H . Pharmacology of botulinum toxin drugs. In: Truong D, Dressler D, Hallett M, editors. Manual of botulinum toxin therapy. 4th ed. New York: Cambridge University Press; (2012) . pp. 13–22. |
[16] | Dressler D . Pharmacology of Botulinum Toxin Drugs. In: Meyer NH, Brashear A, editors. Spasticity: Etiology, Evaluation, Management and the Role of Botulinum Toxin. We Move; 2009. pp. 155-62. |
[17] | Koman L , Smith B and Goodman A . Pharmacology and Pharmacokinetics. In: Koman LA, Smith BP, Goodman A, editors. Botulinum Toxin Type A in the Management of Cerebral Palsy. Wake Forest University Press; 2002. pp. 29-32. |
[18] | Ramirez-Castaneda J , Jankovic J , Comella C , Dashtipour K , Fernandez HH and Mari Z . Diffusion, spread, and migration of botulinum toxin. Mov Disord. (2013) ;28: (13):1775–83. doi: 10.1002/mds.25582 |
[19] | Montastruc J , Marque P , Moulis F , et al. Adverse drug reactions of botulinum neurotoxin type A in children with cerebral palsy: a pharmaco-epidemiological study in VigiBase. Dev Med Child Neurol. (2017) ;59: (3):329–34. doi: 10.1111/dmcn.13286 |
[20] | Albavera-Hernández C , Rodríguez JM and Idrovo AJ . Safety of botulinum toxin type A among children with spasticity secondary to cerebral palsy: a systematic review of randomized clinical trials. Clin Rehabil. (2009) ;23: (5):394–407. doi: 10.1177/0269215508099860 |
[21] | O’Flaherty SJ , Janakan V , Morrow AM , Scheinberg AM and Waugh M-CA . Adverse events and health status following botulinum toxin type A injections in children with cerebral palsy. Dev Med Child Neurol. (2011) ;53: (2):125–30. doi: 10.1111/j.1469-8749.2010.03814.x |
[22] | Langdon K , Blair E , Davidson S-A and Valentine J . Adverse events following botulinum toxin type A treatment in children with cerebral palsy. Developmental Medicine & Child Neurology. (2010) ;52: :972–3. doi: https://doi.org/10.1111/j.1469-8749.2010.03695.x |
[23] | Paget SP , Swinney CM , Burton KLO , Bau K and O’Flaherty SJ . Systemic adverse events after botulinum neurotoxin A injections in children with cerebral palsy. Dev Med Child Neurol. (2018) ;60: (11):1172–7. doi: 10.1111/dmcn.13995 |
[24] | Goldstein EM . Safety of high-dose botulinum toxin type A therapy for the treatment of pediatric spasticity. J Child Neurol. (2006) ;21: (3):189–92. doi: 10.2310/7010.2006.00041 |
[25] | Lee JH , Sung IY , Yoo JY , Park EH and Park SR . Effects of different dilutions of botulinum toxin type A treatment for children with cerebral palsy with spastic ankle plantarflexor: a randomized controlled trial. J Rehabil Med. (2009) ;41: (9):740–5. doi: 10.2340/16501977-0418 |
[26] | Edwards P , Sakzewski L , Copeland L , et al. Safety of botulinum toxin type A for children with nonambulatory cerebral palsy. Pediatrics. (2015) ;136: (5):895–904. doi: 10.1542/peds.2015-0749 |
[27] | Tedroff K , Löwing K , Haglund-Akerlind Y , Gutierrez-Farewik E and Forssberg H . Botulinum toxin A treatment in toddlers with cerebral palsy. Acta Paediatr. (2010) ;99: (8):1156–62. doi: 10.1111/j.1651-2227.2010.01767.x |
[28] | Paracka L , Kollewe K , Wegner F and Dressler D . Strategies to decrease injection site pain in botulinum toxin therapy. J Neural Transm (Vienna). (2017) ;124: (10):1213–6. doi: 10.1007/s00702-017-1764-1 |


