
Walking activities beyond gait training: Priorities in everyday life for parents and adolescents in pediatric neurorehabilitation
Abstract
PURPOSE:
This study aimed to gain knowledge about which walking-related everyday life activities and situations are relevant for parents of children with a neuromotor disorder and adolescents undergoing inpatient neurorehabilitation.
METHODS:
Two focus group interviews with purposive samples were performed, one with seven parents of children with acquired or congenital neuromotor disorders, and one with four adolescents undergoing inpatient neurorehabilitation. Data were analyzed with a qualitative descriptive research approach.
RESULTS:
Parents identified 120 activities that they considered as relevant in their everyday life and the adolescents identified 113 activities. Based on these activities, ten different categories that have a direct relation to walking in everyday life were identified. “Dealing with obstacles,” “moving in public areas,” “moving in a group,” and “walking in general” were perceived as the highest priority categories by the focus group participants.
CONCLUSION:
Activities incorporating walking tasks related to moving in a group or public areas and dealing with obstacles are perceived as meaningful by adolescents and parents in their everyday life. Addressing these categories in the goal setting process with families could facilitate the definition of walking-related goals aimed at increasing children’s and adolescents’ independence in daily life.
1Introduction
Mobility in general and walking short or long distances are priorities when defining family-centered rehabilitation goals in children undergoing neurorehabilitation [1–3]. Accordingly, therapies targeting gait function are often a focus in pediatric neurorehabilitation and include a wide variety of therapeutic approaches [4, 5]. Thereby, an emphasis is placed on bringing a child’s gait pattern as close as possible to that of typically developing children, in order to reduce their energy expenditure when walking and avoid secondary damages [6]. Parents value walking, especially “correct” walking, as a key component of their children’s wellbeing [7, 8]. Thus, studies evaluating the effectiveness of gait therapy interventions in children predominantly assess body function or capacity measures according to the International Classification of Functioning, Disability and Health (ICF) [4, 5, 9].
However, the field of childhood disability has experienced a paradigm shift in the last few decades from trying to fix the underlying biomedical impairments to promoting activities and participation meaningful to the child and their family [10, 11]. For example, children and adolescents with CP undergoing robot-assisted gait training did not express the wish of being able to walk in the same way as their non-disabled peers [12]. They used “normal walking” to refer to the way they walked themselves [12]. Both parents of children with CP and adults with CP emphasized that during childhood, therapy should not focus on the effort to normalize physical function in people with disabilities. Instead, it should be more directed to help them learn how to manage their bodies as efficiently as possible to participate in activities that are meaningful to them and, thus, experience success [8, 13].
Family-centered therapy services that meet parents’ and children’s needs have been shown to improve a child’s participation in family and recreational activities [14]. To be effective, current evidence suggests that therapy should be activity-based and focus on real-life tasks the child wants to learn to perform [15]. Therefore, the focus should initially not be on how nicely an activity can be performed, but on practicing the activities themselves and in turn promoting the acquisition of relevant skills and functional independence [11].
Young people with CP have expressed that safe and efficient mobility that allows them to participate in daily activities with as little assistance as possible was of utmost importance [16]. However, formulating SMART (specific, measurable, attainable, reasonable and time-bound) therapy goals concerning walking activities or participation in daily life remains a challenge [1]. To facilitate gait rehabilitation according to the current evidence and standards, it is important to know which activities in children’s and young people’s natural environment are meaningful for them and their families, and which potential barriers exist that might impede or complicate their ability to perform these activities. Therefore, the goal of this study was to investigate which walking-related everyday life activities are relevant for parents of children with neuromotor disorders and adolescents undergoing inpatient neurorehabilitation. This knowledge could assist in the family-centered definition of therapy goals and help to increase or maintain youths’ therapy motivation.
2Methods
2.1Study design and setting
Using a qualitative descriptive research design with a constructivist viewpoint, two focus group interviews (FGI) were performed, one with parents (FGI-P) and the second with adolescents (FGI-A). The qualitative descriptive approach entails a low-inference interpretation of the findings by staying close to the facts and events and presenting participants’ accounts in everyday language without interpretation [17]. Both FGIs took place in a spacious meeting room at the Swiss Children’s Rehab (SCR) of the University Children’s Hospital Zurich.
A clarification of responsibility by the ethics committee of the Canton Zurich confirmed that authorization was not needed (Req-2019-00385). All participants as well as the parents of the participating adolescents gave their written informed consent. For the reporting, Standards for Reporting Qualitative Research requirements were followed [18].
2.2Participant recruitment and sampling
For the FGI-P, the first author contacted potential parents directly or by telephone. The eligible participants had to be fluent in the German language and their children had to be: current or former inpatients at the SCR with a neuromotor disorder, aged four to fourteen years, and one of their therapy focuses had to involve gait function. For the FGI-A, adolescents were asked in-person by the first author to participate in a group discussion. They were eligible if they were between 12 and 20 years of age, were fluent in the German language, were currently undergoing inpatient rehabilitation at the SCR, and had a diagnosis of an acquired or congenital neuromotor disorder affecting their gait function. FGIs with both parents and adolescents were performed to gain comprehensive insight into family needs and expectations, covering the whole age range of potential inpatients at the relevant rehabilitation center. Participants were purposively sampled to ensure maximal variation regarding children’s and adolescents’ age, diagnosis (acquired or congenital), and gender. Parents and adolescents were chosen who the authors thought would be able to reflect on and communicate their experiences and who might engage actively in a group discussion. There was no family connection between the participants of the FGI-P and the FGI-A, or within the FGIs.
2.3Data collection
The FGI-team consisted of two members: CA facilitated the focus groups and JG assisted with the discussion and took field notes. Both are physical therapists. The second author is a pediatric therapy specialist, but was conducting research and not involved in patient care at the time. A semi-structured interview guide (Table 1) containing open questions and providing discussion topics, but without specifying an order, was used for the FGIs, which were audio-recorded. This interview guide aimed to elicit as many walking-related activities in the activity performance domain of the ICF as possible that the group participants considered relevant to their children’s (FGI-P) or their own (FGI-A) everyday lives. The sessions were structured by going through the participants’ typical daily routine and providing visual prompts of illustrative pictures as a source of inspiration and for further discussion. Probes were used to clarify responses, generate additional meaningful activities, and identify potential barriers and facilitators for the different activities. The FGIs were held as group discussions, so some questions were not commented upon by every participant. However, the FGI team asked those who had not yet answered if they had anything to add. The minute-taker noted all mentioned walking-related activities in an anonymized way. From the list of all compiled activities, each participant was then asked to select and write down those three that seemed most relevant to them for their child’s (FGI-P) or their own (FGI-A) functional abilities in everyday life. Each of the FGIs lasted a maximum of two hours, with short breaks when needed.
Table 1
Interview questions
| What tasks or activities in your daily life with your child come to your mind that involve walking? |
| We would like to go together through a typical day of your child step by step and collect all activities related to walking. Think about a typical day that includes kindergarten/school/work, as well as free time, time with family, and normal day-to-day routines, and consider what activities such a typical day would call for that involve walking. To structure the course of the day and assist you in this process, we show you some pictures as examples. |
| Compared to these exemplary pictures, what is the specific situation at your home? |
| What makes the respective situations more difficult; what makes it easier for you or your child? |
| Of all the everyday walking activities that were mentioned in today’s discussion, which three are most important to you personally that you would you like to see your child master or practice in therapy? Please go through the list with all the compiled activities and write down the three activities most important to you. |
2.4Analysis
All mentioned walking-related activities from the audio recordings were transcribed and added to the already existing FGI activity lists that had been compiled during the FGIs. Each activity was then printed on a small card. Using these cards, the potential commonalities of the identified activities were discussed in terms of content, activity area, environment, or requirements to define a set of categories. Finally, each activity was assigned to one category, and these categories were visualized with mind-maps [19]. To determine the categories of highest priority for the parents and adolescents, comparisons were made based on the frequency with which participants mentioned a category when asked to select which three were most relevant to them.
2.5Trustworthiness
Using a qualitative descriptive approach, the least interpretative of all existing qualitative analysis approaches was applied without interpreting the meaning of participants’ responses [17]. Categories were formulated, discussed, and rearranged by the first and second author together until agreement was reached. Further, member checks were applied by sending the created mind-maps by e-mail (FGI-P) or presenting them in person (FGI-A) and asking the participants for feedback.
3Results
Seven parents participated in the FGI-P, three were parenting a child with an acquired neuromotor disorder, and four had children with congenital neuromotor disorders. When the FGI-P interviews were conducted, five children were inpatients –two for their first rehabilitation, three for a repeated rehabilitation stay. The FGI-A was attended by four adolescents, all inpatients at the SCR. Two were undergoing their first rehabilitation stay because of a recently acquired neuromotor disorder. The other two, both with a diagnosis of cerebral palsy, had already completed several rehabilitation stays in the past. All four adolescents were living with their families. The two male participants attended school, while the female participants were already either employed or in vocational training. Further participant characteristics are listed in Table 2.
Table 2
Characteristics of the focus group interview participants
| Parents | |||||
| ID | Gender | Age (years) | Child: sex, age (years) | Child’s diagnosis | Siblings |
| P1 | Male | 42.9 | male, 13.9 | Traumatic brain injury (5 months ago) a | 1 sister |
| P2 | Female | 38.6 | male, 5.0 | Encephalopathy (4 months ago) a | 2 brothers |
| P3 | Female | 46.5 | female, 9.8 | Stroke (4.5 years ago) | 4 sisters, 2 brothers |
| P4 | Female | 45.4 | female, 6.9 | Bilateral cerebral palsy, GMFCS II | 2 sisters, 2 brothers |
| P5 | Female | 46.8 | male, 13.4 | Bilateral cerebral palsy, GMFCS III a | – |
| P6 | Female | 43.8 | male, 9.1 | Bilateral cerebral palsy, GMFCS III a | 1 sister |
| P7 | Female | 41.4 | male, 7.6 | Congenital ataxia a | 1 sister |
| Adolescents | |||||
| ID | Gender | Age (years) | Diagnosis | Siblings | |
| A1 | Female | 16.4 | Multiple sclerosis (diagnosed 2 months ago)a | 2 brothers | |
| A2 | Male | 15.8 | Stroke (4 months ago)a | 2 brothers | |
| A3 | Male | 12.3 | Bilateral cerebral palsy, GMFCS IIa | – | |
| A4 | Female | 19.3 | Bilateral cerebral palsy, GMFCS IIa | 2 brothers | |
ainpatient stay at the moment of the focus group interview.
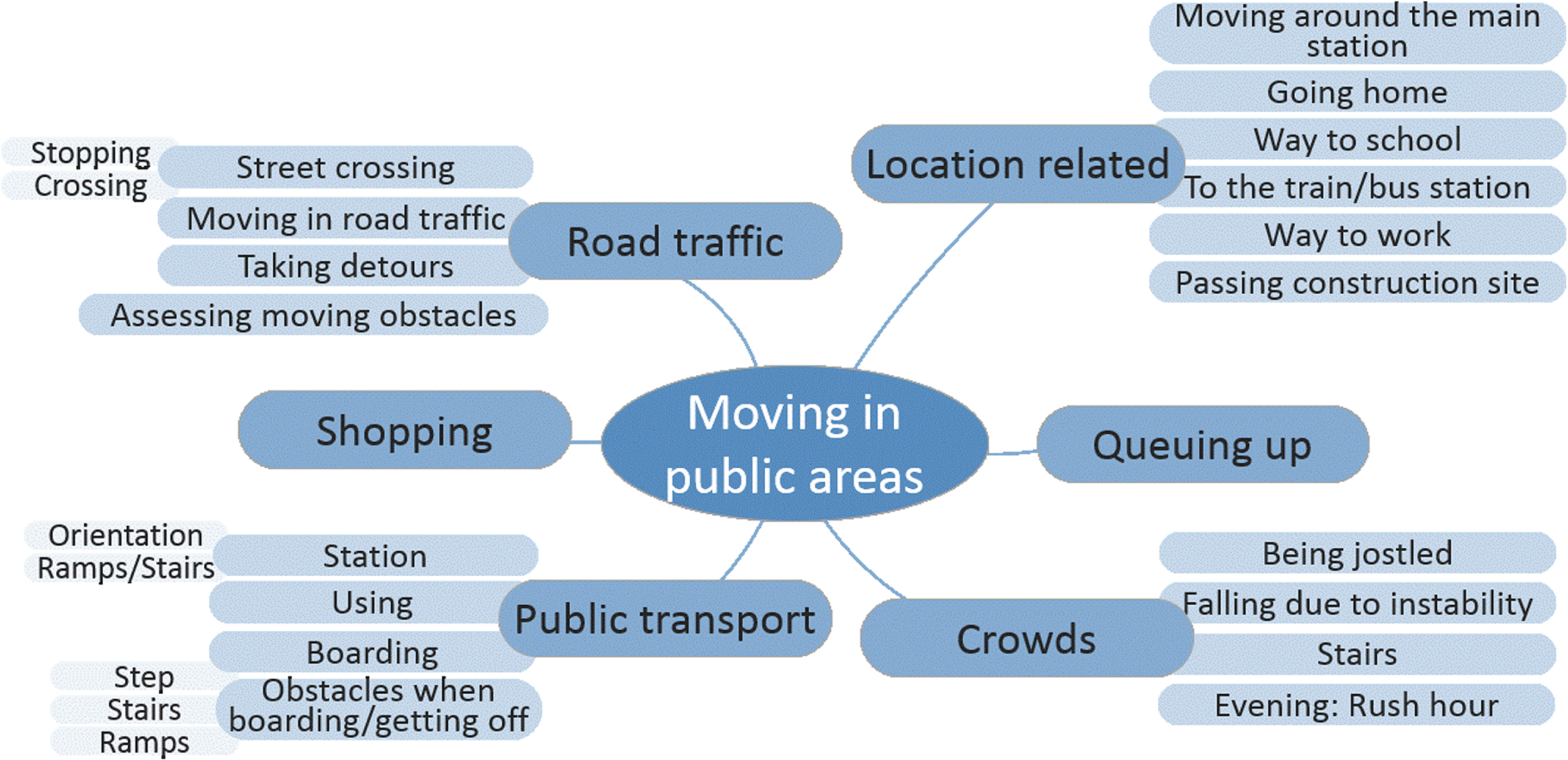
After listening to the audio recordings and removing duplicates, the FGI-P and FGI-A lists consisted of 120 and 113 different activities (Table SI). For the FGI-P, ten categories with a direct link to walking emerged from 83 of these activities. Regarding the FGI-A, 82 activities could be allocated to seven walking-related categories that had already emerged based on the FGI-P activities. (Table 3). Due to the feedbacks from the member checks, two more activities were added, neither part of this manuscript’s topic, as they were not related to walking activities. Otherwise, the participants found the mind-maps to be a complete synthesis of what they had discussed in the FGIs. Based on the number of activities per category, ‘mastering obstacles’ and ‘moving in public’ were the categories with the most mentioned activities (Table 3). Figs. 1 and 2 present all activities mentioned related to these two categories.
Table 3
Number [N] of mentioned walking-related activities in everyday life grouped by categories, and their number of priority nominations [N] by parents and adolescents
| Activity categories | Activities [N] | Priority nominations [N] | ||
| Parents | Adolescents | Parents | Adolescents | |
| Dealing with obstacles | 22 | 12 | 4 | – |
| Moving in public areas | 12 | 25 | 1 | 4 |
| Walking and carrying | 10 | 10 | 2 | – |
| Moving in a group | 9 | – | 4 | – |
| Walking with additional requirements | 8 | 14 | – | – |
| Walking on different surfaces | 8 | 9 | – | – |
| Sensory issues during walking | 5 | 2 | – | – |
| Playing | 5 | – | – | – |
| Walking with visual challenges | 3 | – | 1 | – |
| Walking in general | 1 | 10 | 2 | 6 |
| Categories not directly related to walking in everyday life | ||||
| Sports/leisure activities | 18 | 19 | 1 | – |
| Transfer | 9 | 1 | 2 | – |
| Self-care | 4 | 1 | 4 | 1 |
| Standing | 4 | 6 | – | – |
| Crawling/moving on the ground | 2 | – | – | – |
| Therapeutic context | – | 4 | – | 1 |
Fig. 1
Mind-map of activities mentioned by the parents and adolescents related to mastering obstacles.
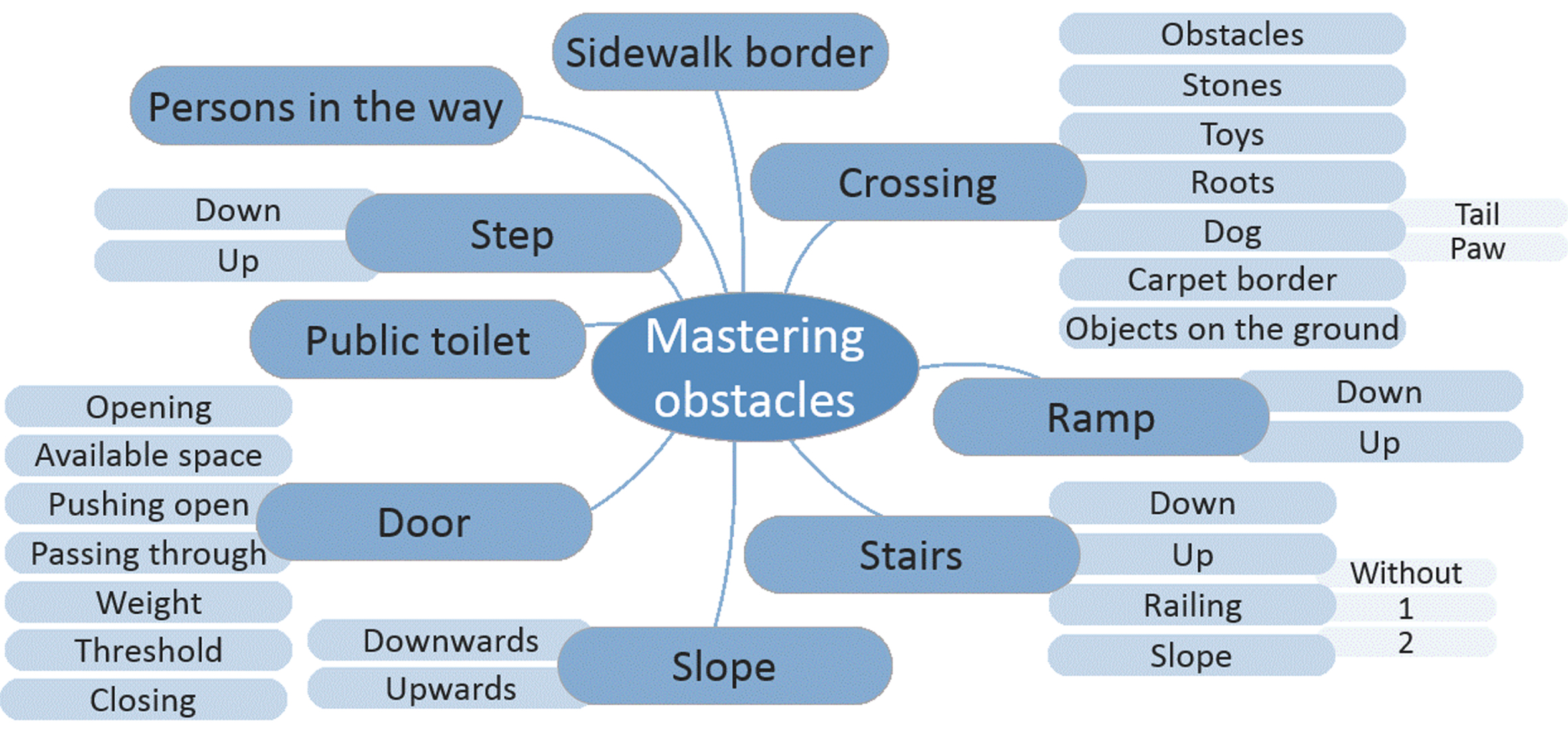
Fig. 2
Mind-map of activities mentioned by the parents and adolescents related to moving in public areas.
When asked which three were the most important activities (last question in Table 1), there were various activity nominations. The parents selected 16 different walking-related activities as the most relevant ones regarding their children’s everyday life. Walking in general, climbing stairs, walking with other children in a group, being with the other children during school breaks, and showering were each mentioned twice. The adolescents came up with ten different activities, and walking in their working environment, walking to the toilet, and crossing a threshold/gap when using public transports were each mentioned twice.
However, when looking at the activity nominations on the category level, trends emerged. Parents’ priorities mainly focused on moving in a group and their child’s ability to deal with obstacles. In contrast, the adolescents selected general walking activities or prioritized activities related to moving in public areas. All numbers regarding the walking-related activities by category and the priority nominations are listed in Table 3.
“Moving in public areas” was mentioned most often across both groups and was clearly a priority for the adolescents. Many activities reported by the adolescents referred to particular aspects of using public transportation (crossing the gap when boarding public transport, climbing downstairs in a train under time pressure, and moving around the central station in the evening). In contrast, the activities mentioned by the parents within this category were more general (using public transportation and moving safely in road traffic).
Parents prioritized activities belonging to the category “moving in a group,” reflecting their concern regarding their children’s function in the school environment. School was a major topic throughout the FGI-P, and its associated activities included walking to the gym in a group, moving in the schoolyard together with other children, or walking in the school hallway when many children are walking around. A further aspect within this category was the parents’ desire for their children to be part of a peer group and the difficulties encountered in this context. Related activities mentioned were moving together with peers, keeping the pace of the other children in the group, or being together with other children during school breaks. Difficulties reported in this context related to their child’s distraction because of the other kids, exhaustion because of the pace set by the group, or challenge to retain stability when other children jostle them.
Activities belonging to the category “dealing with obstacles,” which was another priority for the parents, did not show major differences between the adolescents and parents. Named activities included navigating obstacles in a broad sense - encountered when at home or outdoors and ranged from climbing stairs to opening doors, stepping over roots, or mastering ramps. Table 4 presents examples of participants’ accounts referring to the prioritized categories.
Table 4
Quotes of the parents (P) and adolescents (A) grouped by activity category
| Activity categories | Quotes by parents | Quotes by adolescents |
| Dealing with obstacles | P4: Into the forest, that is certainly a topic, over the roots, so now, in the school where she will go to, they will go into the forest once a week, there will be a need for support. | A1: So, carpet or something, because sometimes I still have a little trouble lifting my legs nicely and so, and then when the carpet suddenly goes up, you can fall down, yes, or slip somehow or something [...] you always have to be a little careful when there are things on the floor like that [...] carpets and such. |
| Moving in public areas | P7: It is often the case that you have to cover enormous distances as a person with a walking disability, because you don’t have the closest route, it’s not just there is the ramp or there is a lift, you are anywhere. And I think that’s a challenge just generally for (laughs) someone who has a walking disability [...]. | A1: Yeah, so... so... you have to be really careful with so many people, because they push you around and stuff, and then you fall down, because you’re not as stable as the others. |
| Walking and carrying | P6: It’s difficult when he doesn’t have enough balance, stability, he can just, ok, then you can serve cups [...] it is possible that he will fall, dropping everything, then you really have to, certain things, you can serve that, that’s for the sister [...] you can maybe only take one thing at a time, and not several things [...]. | A2: When I go to the fridge, take out a yoghurt, or such. |
| Moving in a group | P4: And I think, also the way to the gym, now for her, she also needs a vehicle to go there, because she can’t walk with the speed the others walk. | NA |
| Walking with additional requirements | P7: For us, another point where we had to rethink a bit as a family is hiking. My husband and I love to hike, and now we’re reaching our limits. In the past you used to carry him, now we are thinking a bit about whether we should somehow convert the bicycle trailer so that we can pull him, so that he can walk a certain distance being held by the hand, but for us, in our free time, as a family activity, that is a severe restriction [...]. | A1: No, you have to take them [textbooks] with you and sometimes also change the school building. |
| Walking on different surfaces | P7: Wet is deadly, so indoor swimming is actually, if I can’t take the wheelchair in, I can just walk out again because it’s just too dangerous. | A4: [...] that the floor in the kitchen is not slippery [...] we [who work] in the kitchen [have] extra shoes with good profile. |
| Sensory issues during walking | P6: And then there’s the sensitivity [...] that doesn’t like the wet, in the open-air swimming pool, on the meadow (laughter), then there’s the whole CP spasticity and then it doesn’t work anymore [...] but as soon as something is a bit hard, a bit wet, a bit cold, a bit stinging, then it doesn’t work anymore, although it might normally work [...]. | A3: When I walk barefoot, I sometimes...er...hit my foot on the wall. |
| Playing | P6: Yes, what playing outside is also about, you go outside often [...] to play with other children and then it goes on for five minutes and then they already have a problem because the children are doing something where he can’t join in, then they sit, stand there and think hm. | NA |
| Walking with visual challenges | P6: [Darkness, no light] Is generally when you walk, if you become insecure, then the tone comes back in more and then everything becomes more difficult. | NA |
| Walking in general | P1: Like I said, I’m just happy already that he can walk. | A4: I go to the wardrobe, take out my clothes, sit on the bed, get dressed, get up again, go to the breakfast table [...]. |
| Categories not directly related to walking in everyday life | ||
| Sports/leisure activities | P5: Sport in general, any sport... be it basketball, ice hockey, whatever, football [...] So now with our son, the issue is, because he really can’t walk freely, that he always needs an aid to walk, we fought so that he could participate in sport, so they wanted to suspend him from it and we then said no, that’s the social aspect, he needs that [...]. | A2: In my free time I skateboard, play basketball, ride my bike [...] I think walking is needed to do sports and just keep your mobility back in rhythm. |
| Transfer | P7: [...] then of course I have to help him, simply give him assistance, for getting on the chair, depending on how fit he is, he can get up himself and hold himself at the table and sit down. | A4: We sit up, put on ... walk to the wardrobe [...]. |
| Self-care | P6: Yes, going to the toilet is ... our son also had the possibility to go to the toilet himself, he could walk alone, but also crawled a lot on the floor, either with or without orthoses, but could really sit on the toilet himself, we had a ring, from which he did not immediately fall down [...]. | A1: So, you don’t have to walk during the shower, but you have to be able to stand. |
| Standing | P7: He does that [stand and put school books in school bag], but I just have to hold him. So, we always just have a little bit of a choice, or, well, either I just hold him by the hips and then he handles it, or then I do it. But ... something all by himself, that’s not possible. | A4: So, I stand for about eight hours a day. |
| Crawling/moving on ground | P7: [...] because he moves around at home on the floor, not in a wheelchair, because it’s too tiring for him. So, on the floor means he crawls? He doesn’t really crawl, he rather slides on his bottom or jumps. But crawling is already a problem for him, he’s much too slow. He’s developed his own technique when he was about 2 years old, or something, and he still gets on with it and it doesn’t bother him at home. | NA |
| Therapeutic context | NA | A3: Physio [...] I don’t have any other hobby that has to do with walking. |
Both groups also mentioned activities that did not fit into the category of walking-related everyday life activities. Most of these referred to sports and leisure activities, transfer, self-care, and standing (see Table 3).
4Discussion
Two FGIs were conducted to explore relevant walking-related everyday life activities in a population typical for the rehabilitation center where the authors work. Through discussion with parents and adolescents, a more comprehensive and holistic view regarding relevant walking activities and priorities in everyday life over the whole age span of childhood emerged. While the parents –due to the age of their own children - mainly discussed activities that are important for children at the age of attending kindergarten or school, the adolescents discussed topics significant for their stage of life.
“Moving in public” was such a relevant mobility-related topic in adolescents’ daily lives, with the most activities per category mentioned and four priority nominations in the FGI-A. This fact became evident in their vivid and detailed accounts of potential difficulties and challenges when being out in public. In contrast to the adolescents, most children of the FGI-P parents were at an age when they were not yet traveling independently or using public transport on their own. Thus, it was difficult for the parents to visualize their children’s potential challenges in such situations in detail. Problems with physical access to public transportation were also identified as a barrier to participation by parents of children with CP in northeast England [20]. Gaps between the train and platform, narrow aisles, or lack of space, time, steps, stairs, or lifts, which those parents mentioned, are all examples that also emerged in the “moving in public” activities in the FGIs of this study.
A major area of parental concern focused on their children’s functioning in the school environment. Besides the activities that refer to “moving in a group,” walking-related activities also included the category “walking and carrying” (carrying a school bag, bringing school supplies into the classroom, or changing school rooms). These activities often hampered or interfered with the child’s independent functioning in school. In contrast to the current findings, parents of children with CP in another study did not recognize the school as a domain of importance when asked which things they found most important to consider when they evaluated the effect of an intervention for their child [21]. A possible reason those parents did not mention school might be that the question reflected more on the medical context while the current questions focused on everyday life. Besides their child’s functioning in school, the parents in this FGI often articulated aspects that involved the wish or hope that their children might belong to a peer group and their fears or difficulties encountered in this context. This finding aligns with prior research that stated that their child being accepted by others and “being in the world that others are in” was a meaningful therapy goal for parents of children with disabilities [13]. Contrary to the adults, adolescents did not report any activities related to “moving in a group.” This fact is surprising, as peer groups are often of high significance at this stage of life [22], and youths with CP emphasized the importance of feeling included and accepted, especially among peers at school [23]. However, children with CP reported that they did not see themselves as different from other children [24], which might explain why they did not perceive a relevant connection between walking-related activities and being with their peers. On the other hand, parents reported being concerned about their child’s future [23]. Also, they may have been more aware of or apprehensive about problems like social exclusion or bullying that might arise because of their child’s disability [25]. This might explain why they considered it a priority that their child keeps up with the group as best as possible.
“Mastering obstacles” was another priority for the parents in this FGI. Barriers in the natural or manmade physical environment and a lack of accessibility were perceived as restricting factors regarding mobility and participation by other parents of children with a disability [20]. Many of the reported barriers by those parents reflect the walking activities that emerged in the FGIs in this study, ranging from dealing with steps, slopes, or doors that are difficult to open to lack of space or poorly accessible walking paths [20, 26].
Unlike the parents, adolescents gave brief answers during the FGI and required considerably more probing questions. Although the number of activities were comparable in the two FGIs, activities specified by the adolescents more often referred to “walking in general.” This included walking to get to a specific location (like walking to the toilet or the wardrobe). Interestingly, according to the findings of Gibson et al., children with CP seem to view walking primarily as exercise and rarely perceive it consciously as a means of mobility [3].
Three walking-related categories that evolved in the FGI-P were not an issue for the adolescents. While “playing” is not a major part of adolescents’ daily routines, “walking with visual challenges” probably reflected specific challenges that children of the FGI-P participants were dealing with.
The authors would like to address some of the activities that did not fit into the walking-related everyday life categories. Although they were not an original subject of the FGIs, they provide insight into families’ priorities, perspectives, and struggles in daily life. Such knowledge about the families’ considerations and challenges is of value for health professionals working in pediatric neurorehabilitation as it can inform the goal-setting process and improve treatment planning. The majority of those activities was related to “sports,” both club and school sports. While adolescents referred mainly to sports as a leisure activity, parents mentioned specific aspects such as the limited sports facilities for children with disabilities, reduced availability, increased time expenditure, and relatively high costs. Furthermore, parents discussed their views regarding the inclusion of their children in school sports and the growing gap they might experience between their abilities and those of typically developing children.
Additionally, the parents mentioned many other issues regarding their child’s disability and the resulting restrictions or difficulties in everyday life where they would be grateful for guidance or support. For example, a widely discussed theme was the perceived dilemma between therapy requirements and enabling as normal a childhood as possible; a concern that had also been raised by other parents of children with disabilities [13]. Related to this dilemma was the parents’ desire to get the most out of existing treatment options rather than enabling their children to spend their leisure time as they preferred. They also mentioned that sometimes therapists had an expectation that they would organize everyday situations at home in a therapy-oriented way whereas the parents longed to let their child experience a more ordinary and self-determined everyday life. A further challenge mentioned concerned enabling and promoting the greatest possible independence given the existing time constraints. Within this context, several activities that were categorized as “transfer” and “self-care” were mentioned.
Another topic that was not an activity but was closely related to mobility was the suboptimal supply of walking aids, wheelchairs, and orthoses, and the fight for cost coverage for this equipment as well as for therapeutic services. The difficulties in meeting the demands of all family members, especially of the siblings, was also an issue that worried many parents. Addressing such questions and discussing possible solutions with the parents during their child’s rehabilitation stay could potentially ease the families’ burden considerably.
4.1Limitations
The authors would like to acknowledge some limitations of this research. As standard for a qualitative approach, participants were not randomly selected but purposive sampling was used instead for the FGIs. In doing so, the authors tried to account for characteristics that are typical for the patient population of their rehabilitation center. Participant accounts, priorities, and difficulties are always colored by their personal circumstances and challenges. Differences in the adolescents’ age, disability, living situation, and family environment had a major impact on the activities they perceived as significant. This was even more true for the parents. Aiming for maximal variation, parents of children undergoing their first rehabilitation because of a recently acquired brain injury were included. However, it became apparent how difficult it was for them to contribute to the discussion because of limited everyday experiences with their child after the incident.
The FGI-members are not representative of a group as a whole, but rather possess their own experiences and perspectives. Nonetheless, the findings of this study can be valuable and provide access to new perspectives for many others working with children and young people in the field of gait rehabilitation. Additionally, the listed activities can help to guide the parents during the goal-setting process of identifying relevant and attainable therapy goals for their children, as some parents may feel overwhelmed or unable to define realistic goals [13]. Unfortunately, the parent perspective was represented by only one male compared to six female participants. This gender imbalance reflects the authors’ experience that mothers act more often as the primary contact for the questions of the rehabilitation team. It would have been preferable to also give younger children a voice in the FGI-A to convey their perspective first hand (the youngest participant was 12 years old). However, the eligible children seemed uncomfortable with the idea of discussing personal issues and declined to participate. Due to logistical reasons, only two FGIs were performed with a total of eleven participants. Although this sample size was too small to reach saturation, the authors are optimistic that the most prevalent topics could have been identified, as more than 80% of all themes are assumed to be mentioned within two or three focus groups [27]. One might argue that a survey with scores of respondents would yield results that are more robust. However, this approach would bias the family perspective, as the researchers would have to predefine the activities. An interesting future research approach might look at children and parents as a dyad and compare their priorities, especially given that an earlier study revealed that rehabilitation goals and priorities differed considerably between adolescents with a physical disability and their parents [28].
5Conclusions
This study provided insight into various domains and activities that are of importance for children and young people with a neuromotor disorder affecting gait as well as their parents. This knowledge can help when defining family-centered goals for gait rehabilitation with the rehabilitation team and the family. Previously, most goals address body function and task-oriented activities on the capacity level [1] and rarely consider specific walking-related activities in families’ everyday life. Although there is a relationship between changes in motor capacity and performance [29], it seems to be lower in children with less severe CP compared to those classified as GMFCS level III to V [30].
Incorporating treatment approaches with implications on all domains of the ICF would also acknowledge the fact that youth with CP and their parents endorse wide-ranging domains of impact for therapeutic interventions [21]. Activities related to dealing with obstacles, moving in public, and moving in groups seem to be particularly relevant for the families in addition to walking in general. Mastering obstacles is already a regular feature of conventional therapy as many everyday obstacles can be easily accessed during a therapy lesson. However, this is not the case for walking activities in a group or in public. Here, modern technologies like virtual reality or other innovative approaches might help develop new treatment plans and therapy contents that address the families’ priorities in everyday life. Many of the activities mentioned by the FGI participants in this study reflect themes that evolved when adolescents with CP described how they experience mobility in their daily lives: self-sufficiency, making choices, safety and efficiency, adapting to situations, constantly planning ahead, and dissatisfaction with public transportation [16]. By involving families in designing treatment plans and incorporating meaningful, everyday life-relevant goals, rehabilitation services can take a further step towards the empowerment of children, young people, and their families [31].
Acknowledgments
We thank all adolescents and parents who shared their thoughts and time with us for this project.
This project was supported by the J&K Wonderland Foundation, Steinhausen, Switzerland as part of a research project dealing with the possibilities of gait therapy in a virtual environment.
We also acknowledge the Children’s Research Center of the University Children’s Hospital, Zurich, Switzerland.
Role of the funding source: The funders were at no time involved in designing, conducting, or reporting of this study.
Conflict of interest
The authors have no conflict of interest to report.
Ethical considerations
Ethical authorization was not needed as confirmed by the ethics committee of the Canton Zurich. All participants gave their written informed consent. Trial registration number: DRKS00017439.
References
[1] | Rast FM , Labruyère R . ICF mobility and self-care goals of children in inpatient rehabilitation. Dev Med Child Neurol. (2020) ;62: (4):483–488. doi: 10.1111/dmcn.14471 |
[2] | Chiarello LA , Palisano RJ , Maggs JM , Orlin MN , Almasri N , Kang L-J , et al. Family Priorities for Activity and Participation of Children and Youth with Cerebral Palsy. Phys Ther. (2010) ;90: (9):1254–64. doi: 10.2522/ptj.20090388 |
[3] | Gibson BE , Teachman G , Wright V , Fehlings D , Young NL , McKeever P . Children’s and parents’ beliefs regarding the value of walking: Rehabilitation implications for children with cerebral palsy. Child Care Health Dev. (2012) ;38: (1):61–9. doi: 10.1111/j.1365-2214.2011.01271.x |
[4] | Booth ATC , Buizer AI , Meyns P , Oude Lansink ILB , Steenbrink F , van der Krogt MM . The efficacy of functional gait training in children and young adults with cerebral palsy: a systematic review and meta-analysis. Dev Med Child Neurol. (2018) ;60: (9):866–883. doi: 10.1111/dmcn.13708 |
[5] | Lefmann S , Russo R , Hillier S . The effectiveness of robotic-assisted gait training for paediatric gait disorders: systematic review. J Neuroeng Rehabil. (2017) ;14: (1):1. doi: 10.1186/s12984-016-0214-x |
[6] | Aboutorabi A , Arazpour M , Ahmadi Bani M , Saeedi H , Head JS . Efficacy of ankle foot orthoses types on walking in children with cerebral palsy: A systematic review. Ann Phys Rehabil Med. (2017) ;60: (6):393–402. doi: 10.1016/j.rehab.2017.05.004 |
[7] | Beveridge B , Feltracco D , Struyf J , Strauss E , Dang S , Phelan S , et al. “You gotta try it all”: Parents’ Experiences with Robotic Gait Training for their Children with Cerebral Palsy. Phys Occup Ther Pediatr. (2015) ;35: (4):327–41. doi: 10.3109/01942638.2014.990547 |
[8] | Moll LR , Cott CA . The paradox of normalization through rehabilitation: Growing up and growing older with cerebral palsy. Disabil Rehabil. (2013) ;35: (15):1276–83. doi: 10.3109/09638288.2012.726689 |
[9] | World Health Organisation. International Classification of Functioning, Disability and Health: children & youth version: ICF-CY. Geneva: World Health Organization; (2007) . |
[10] | Law M , Darrah J . Emerging therapy approaches: An emphasis on function. J Child Neurol. (2014) ;29: (8):1101–7. doi: 10.1177/0883073814533151 |
[11] | Rosenbaum P , Gorter JW . The “F-words” in childhood disability: I swear this is how we should think. Child Care Health Dev. (2012) ;38: (4):457–63. doi: 10.1111/j.1365-2214.2011.01338.x |
[12] | Phelan SK , Gibson BE , Wright FV . What is it like to walk with the help of a robot? Children’s perspectives on robotic gait training technology. Disabil Rehabil. (2015) ;37: (24):2272–81. doi: 10.3109/09638288.2015.1019648 |
[13] | Wiart L , Ray L , Darrah J , Magill-Evans J . Parents’ perspectives on occupational therapy and physical therapy goals for children with cerebral palsy. Disabil Rehabil. (2010) ;32: (3):248–58. doi: 10.3109/09638280903095890 |
[14] | McCoy SW , Palisano R , Avery L , Jeffries L , Laforme Fiss A , Chiarello L , et al. Physical, occupational, and speech therapy for children with cerebral palsy. Dev Med Child Neurol. (2020) ;62: (1):140–146. doi: 10.1111/dmcn.14325 |
[15] | Novak I , Morgan C , Fahey M , Finch-Edmondson M , Galea C , Hines A , et al. State of the Evidence Traffic Lights Systematic Review of Interventions for Preventing and Treating Children with Cerebral Palsy. Curr Neurol Neurosci Rep. (2020) ;20: (2):3. doi: 10.1007/s11910-020-1022-z |
[16] | Palisano RJ , Shimmell LJ , Stewart D , Lawless JJ , Rosenbaum PL , Russell DJ . Mobility Experiences of Adolescents with Cerebral Palsy. Phys Occup Ther Pediatr. (2009) ;29: (2):133–53. doi: 10.1080/01942630902784746 |
[17] | Sandelowski M . Whatever happened to qualitative des-cription? Res Nurs Health. (2000) ;23: (4):334–40. doi: 10.1002/1098-240x(200008)23:4<334::aid-nur9>3.0.co;2-g |
[18] | O’Brien BC , Harris IB , Beckman TJ , Reed DA , Cook DA . Standards for reporting qualitative research: A synthesis of recommendations. Acad Med. (2014) ;89: (9):1245–51. doi: 10.1097/ACM.0000000000000388 |
[19] | Vaismoradi M , Snelgrove S . Theme in qualitative content analysis and thematic analysis. Forum Qualitative Sozialforschung. (2019) ;20: (3). doi: 10.17169/fqs-20.3.3376 |
[20] | Lawlor K , Mihaylov S , Welsh B , Jarvis S , Colver A . A qualitative study of the physical, social and attitudinal environments influencing the participation of children with cerebral palsy in northeast England. Pediatr Rehabil. (2006) ;9: (3):219–28. doi: 10.1080/13638490500235649 |
[21] | Vargus-Adams JN , Martin LK . Domains of importance for parents, medical professionals and youth with cerebral palsy considering treatment outcomes. Child Care Health Dev. (2011) ;37: (2):276–81. doi: 10.1111/j.1365-2214.2010.01121.x |
[22] | Sussman S , Pokhrel P , Ashmore RD , Brown BB . Adolescent peer group identification and characteristics: A review of the literature. Addict Behav. (2007) ;32: (8):1602–27. doi: 10.1016/j.addbeh.2006.11.018 |
[23] | Lindsay S . Child and youth experiences and perspectives of cerebral palsy: a qualitative systematic review. Child Care Health Dev. (2016) ;42: (2):153–75. doi: 10.1111/cch.12309 |
[24] | Schiariti V , Sauve K , Klassen AF , O’Donnell M , Cieza A , Mâsse LC . ‘He does not see himself as being different’: the perspectives of children and caregivers on relevant areas of functioning in cerebral palsy. Dev Med Child Neurol. (2014) ;56: (9):853–61. doi: 10.1111/dmcn.12472 |
[25] | Lindsay S , McPherson AC . Experiences of social exclusion and bullying at school among children and youth with cerebral palsy. Disabil Rehabil. (2012) ;34: (2):101–9. doi: 10.3109/09638288.2011.587086 |
[26] | Piškur B , Beurskens AJ , Jongmans MJ , Ketelaar M , Norton M , Frings CA , et al. Parents’ actions, challenges, and needs while enabling participation of children with a physical disability: a scoping review. BMC Pediatr. (2012) ;12: :177. doi: 10.1186/1471-2431-12-177 |
[27] | Guest G , Namey E , McKenna K . How Many Focus Groups Are Enough? Building an Evidence Base for Nonprobability Sample Sizes. Field Methods. (2017) ;29: (1):3–22. doi: 10.1177/1525822X16639015 |
[28] | McGavin H . Planning rehabilitation. Phys Occup Ther Pediatr. (1998) ;18: (1):69–82. doi: 10.1080/J006v18n01_05 |
[29] | Halma E , Bussmann JBJ , van den Berg-Emons HJG , Sneekes EM , Pangalila R , Schasfoort FC . Relationship between changes in motor capacity and objectively measured motor performance in ambulatory children with spastic cerebral palsy. Child Care Health Dev. (2020) ;46: (1):66–73. doi: 10.1111/cch.12719 |
[30] | Smits D-W , Gorter JW , Ketelaar M , Van Schie PE , Dallmeijer AJ , Lindeman E , et al. Relationship between gross motor capacity and daily-life mobility in children with cerebral palsy. Dev Med Child Neurol. (2010) ;52: (3):e60–6. doi: 10.1111/j.1469-8749.2009.03525.x |
[31] | Dan B . Disability and empowerment. Dev Med Child Neurol. (2020) ;62: (5):536. doi: 10.1111/dmcn.14511 |


