
Comparing neurodevelopmental outcomes at 30 months by presence of hydrocephalus and shunt status among children enrolled in the MOMS trial
Abstract
PURPOSE:
To evaluate for differences in neurodevelopmental outcomes at 30 months of age for children enrolled in the Management of Myelomeningocele Study (MOMS) based on the presence of hydrocephalus and cerebral shunts.
METHODS:
Children with no hydrocephalus (
RESULTS:
In unadjusted comparisons, statistically significant differences were noted between the three groups on the Peabody Gross Motor Quotient and thus the Total Motor Quotient. After adjustment, no statistically significant differences were identified. In subanalyses, children with more severe hydrocephalus fared worse on the Peabody Fine Motor Quotient (median 88 versus 94,
CONCLUSION:
No neurodevelopmental differences were noted with children enrolled in MOMS across the three hydrocephalus/shunt groups, although severity of hydrocephalus was associated with poorer outcomes.
1.Introduction
Myelomeningocele, the most common and severe variant of spina bifida, is a complex neural tube defect that occurs in approximately 1 in 1,500 births in the United States [1]. Myelomeningocele is primarily characterized by defective closure of the caudal neural tube during embryonic development, leading to a defect of the bony spine and protrusion of the meninges, spinal cord (depending on the lesion level), and spinal nerves [2]. Individuals with myelomeningocele can experience lower extremity motor and sensory dysfunction and neurogenic bowel and bladder, in addition to a host of long-term neurodevelopmental sequelae resulting from multiple brain abnormalities. These abnormalities may include a concomitant Chiari II malformation, characterized by varying degrees of hindbrain herniation and myelomeningocele-associated hydrocephalus [3, 4]. Hydrocephalus causes axonal damage and decreased cerebral perfusion pressures and is linked to delayed myelination, endocrine derangements, and a constellation of deficits in cognitive, sensory, and motor functions [5, 6, 7]. The impact of hydrocephalus is highly variable in terms of anatomic and functional consequences [8].
Historically, myelomeningocele was and is treated with surgical repair of the defect shortly after birth. Placement of a cerebrospinal fluid (CSF) shunt for hydrocephalus, if present, often occurred within the first few days of life [9, 10]. Current evidence suggests that some of the downstream sequelae of myelomeningocele can be reduced with fetal repair [11]. Theoretical benefits of prenatal repair include reduced exposure of the spinal cord to amniotic fluid and trauma during gestation and delivery and improved cerebrospinal fluid dynamics thereby reducing the degree of hindbrain herniation and hydrocephalus [3, 5, 12]. Advances in fetal surgery in the late 1990s and early 2000s were followed by the Management of Myelomeningocele Study (MOMS). Initial results published in 2011 and updated in 2015 demonstrated that patients undergoing prenatal repair fared significantly better than those undergoing standard postnatal repair as evidenced by reduced severity of hindbrain herniation, reduced rates of hydrocephalus, and improved motor outcomes [13, 14].
While shunting is a well-established treatment modality for hydrocephalus, variability exists regarding which patients receive shunts and when [15, 16, 17, 18]. An estimated 50% of shunts placed in the pediatric population fail within 2 years due to complications including malfunction and infection [16, 17, 19, 20, 21, 22]. These complications require hospitalizations and shunt revisions, posing a burden to patients, their families, and the healthcare system [15, 18, 23, 24, 25, 26]. Studies have suggested that shunt placement in patients with myelomeningocele is associated with a decrease in IQ and an increase in mortality compared to patients who were not shunted [27, 28, 29]. Whether this is due to shunting and its complications or due to the underlying severity of hydrocephalus is controversial [30, 31]. Thus, many neurosurgeons are hesitant to place shunts unless deemed absolutely necessary [9, 12, 15, 16, 17, 19, 20, 32, 33, 34, 35, 36]. Several centers have proposed stringent shunt criteria (based on signs of increased intracranial pressure, severe ventriculomegaly, presence of syringomyelia, pseudomyelomeningocele, or leakage of CSF from the repair site, etc.) in an effort to reduce rates of shunt placement [11, 15, 32, 33, 37]. These criteria have not been well studied or widely accepted. To date, there are no adequate clinical prediction rules to determine patient populations in which the benefits of shunt placement outweigh the risks. The decision to shunt or not is often based on individual experience and preference [15, 18].
In MOMS, hydrocephalus shunt criteria based on expert consensus were pre-established to decrease the influence of biases among treating neurosurgeons. Of MOMS participants who had their shunt criteria evaluated at one year of age, 71.9% of the infants in the prenatal surgery group and 97.8% of the infants in the postnatal surgery group met shunt criteria [14]. Actual rates of shunt placement in prenatal and postnatal repair groups were 44.9% and 83.7%, respectively [13]. Why treating neurosurgeons and families opted not to pursue shunt placement in the face of hydrocephalus is unknown, and may include selection bias as surgeons and families may have had a vested interest in not shunting infants who had previous prenatal repair. In addition, it may relate to hesitancy on the part of neurosurgeons to place shunts even if the predetermined hydrocephalus criteria were met because they use different criteria in their clinical practices.
The analyses presented herein utilize the differing shunting patterns of the MOMS children to evaluate neurodevelopmental outcomes at 30 months by the presence of both hydrocephalus (based on the predetermined criteria) and shunts. Three groups of children are evaluated: children with hydrocephalus and shunts (the shunted hydrocephalus group), children with hydrocephalus but without shunts (the unshunted hydrocephalus group), and children without hydrocephalus and without shunts (the no hydrocephalus group). There were two a priori hypotheses. First, that unshunted hydrocephalus would be associated with worse outcomes on the neurodevelopmental battery at 30 months compared to shunted hydrocephalus and no hydrocephalus. Second, that the no hydrocephalus group would have better neurodevelopmental outcomes than both the hydrocephalus groups (shunted and unshunted).
Table 1
MOMS criteria for the presence of hydrocephalus indicating need for shunt [13]
| Criterion 1 | At least 2 of the following:
|
|---|---|
| Criterion 2 | Presence of marked syringomyelia with ventriculomegaly |
| Criterion 3 | Ventriculomegaly with symptoms of Chiari malformation (stridor, swallowing difficulties, apnea, bradycardia) |
| Criterion 4 | Persistent CSF leakage from the myelomeningocele wound or bulging at the repair site |
2.Methods
The MOMS trial was conducted between 2003 and 2010 at three clinical sites with extensive expertise in maternal-fetal surgery (Children’s Hospital of Philadelphia, University of California San Francisco and Vanderbilt University) with George Washington University serving as the Data Coordinating Center and the Eunice Kennedy Shriver National Institute of Child Health and Human Development serving as the sponsor. Institutional Review Board approval was obtained at all sites. While the MOMS trial was enrolling participants, all other maternal-fetal surgery centers ceased performing fetal surgery for spina bifida. During enrollment, 183 maternal-fetal dyads from across the country were randomized to either standard postnatal repair or prenatal repair [14]. The inclusion criteria included fetal myelomeningocele with an upper boundary between T1-S1 with a normal karyotype in a singleton pregnancy between 19.0–25.9 weeks gestation, along with evidence of hindbrain herniation, in a mother at least 18 years of age with residency in the United States. The major exclusion criteria included maternal body mass index of 35 or higher, surgical contraindications such as prior hysterotomy, high risk of preterm birth, placental abruption, major fetal anomalies not associated with spina bifida, and severe fetal kyphosis. After randomization, mothers randomized to the prenatal repair group stayed near the study center for the duration of their pregnancy, while mothers in the standard postnatal repair group went home and returned for planned cesarean delivery and post-natal repair at the study center [14]. After delivery (and repair if in the postnatal group) families returned home for their ongoing care. The first primary outcome of the MOMS trial was a composite measure of fetal/neonatal death plus need for a cerebrospinal fluid shunt based on predetermined hydrocephalus criteria (see Table 1) [13] by 12 months of age [14]. The second primary outcome, at 30 months, was a composite of the Mental Development Index of the Bayley Scales of Infant Development II and motor function adjusted for lesion level [14]. The trial was stopped for efficacy based on the results of both primary outcomes in December of 2010 prior to the planned enrollment of 200 maternal-fetal dyads [14].
Figure 1.
Participants by hydrocephalus and shunt status.
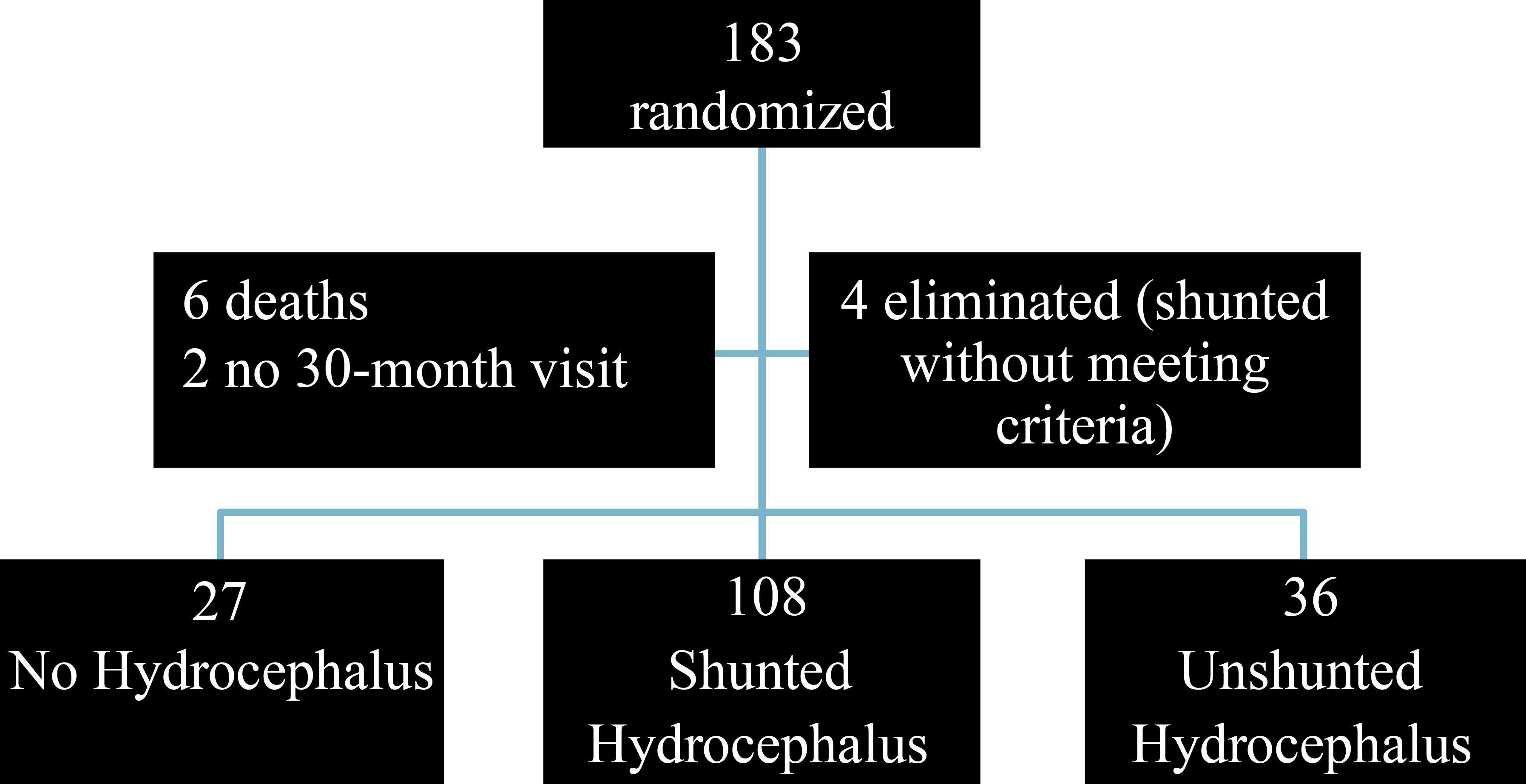
Of those 183 participants (91 in the prenatal surgery group and 92 in the postnatal surgery group), there were six deaths and two additional children who were not assessed at 30 months. See Fig. 1 for a flow chart of the participants. At the 30-month visit, 175 children were assessed for neurodevelopmental outcomes. Hydrocephalus criteria (Table 1) and shunt status were assessed by one year of age. Of those with neurodevelopmental evaluations, 106 met criteria for hydrocephalus and had a shunt placed. Two more children had third ventriculostomies, totaling 108 children with shunted hydrocephalus. Of the remaining 67 children, 36 met criteria but did not have shunts placed (unshunted hydrocephalus) and 27 did not meet hydrocephalus criteria and were not shunted (no hydrocephalus) [13]. Four children in the postnatal repair group had shunts placed without meeting hydrocephalus criteria and were excluded from the analysis. Two of these children had shunts placed at the time of the spina bifida repair by their local neurosurgeon. One had a shunt placed within a week of repair and one had a shunt placed at the age of four months [13].
Table 2
Characteristics by hydrocephalus and shunting status
| All | No hydrocephalus | Shunted hydrocephalus | Unshunted hydrocephalus | |
| Maternal education at screening – yrs | 14.9 | 15.0 | 15.0 | 0.87 |
| Prenatal repair group | 25 (92.6) | 39 (36.1) | 23 (63.9) | |
| Female child | 10 (37.0) | 59 (54.6) | 23 (63.9) | 0.10 |
| Lesion level at L3 or lower | 21 (77.8) | 84 (77.7) | 26 (72.2) | 0.78 |
| Gestational age at delivery – wks | 34.9 | 36.1 | 35.2 | 0.003 |
| Ventricle size at screening* – mm | 8.5 | 11.8 | 10.9 |
Data presented as mean
In this analysis of MOMS data, neurodevelopmental assessment results were used to evaluate differences in outcomes for the three hydrocephalus criteria/shunt groups of subjects: Bayley II Mental and Psychomotor Development Indices, the Peabody Developmental Motor Scale-2 and the Preschool Language Scale 4
In univariable analysis, continuous variables were compared using the Wilcoxon test; categorical variables were compared with the chi-square or Fisher’s exact test as appropriate. Normal order score transformations were employed for each of the outcomes as many of the scores from the evaluations are not normally distributed in this population. Kruskal-Wallis tests were used to determine differences between the three hydrocephalus criteria/shunt groups in these scores. Generalized linear models were used in a multivariable analysis adjusted for pre or postnatal repair group, maternal education and ventricular size at screening. Gestational age at birth was not included because it was highly correlated with prenatal repair status. To determine how the severity of hydrocephalus is associated with the outcomes, the same methods were employed for only the children who met hydrocephalus criteria. Those who met only one criterion were compared to those who met two or more hydrocephalus criteria. The multivariable model included adjustment for surgery group assignment, maternal education, and ventricular size at screening.
Table 3
Outcomes by hydrocephalus and shunt status
| All | No hydrocephalus | Shunted hydrocephalus | Unshunted hydrocephalus | |||||||
| Bayley Psychomotor Index | 15 (55.6) | 41 (38.0) | 15 (41.7) | 0.25 | ||||||
|
| Median | IQR |
| Median | IQR |
| Median | IQR | ||
| Bayley Mental Index | 27 | 91.0 | (13.0) | 108 | 91.5 | (20.5) | 36 | 94.0 | (9.0) | 0.43 |
| Peabody Developmental Motor Scale | ||||||||||
| Fine motor quotient | 27 | 97.0 | (18.0) | 107 | 94.0 | (12.0) | 36 | 94.0 | (15.0) | 0.15 |
| Gross motor quotient | 27 | 72.0 | (22.0) | 107 | 61.0 | (9.0) | 36 | 64.0 | (13.0) | 0.04 |
| Total motor quotient | 27 | 78.0 | (18.0) | 107 | 71.0 | (9.0) | 36 | 74.5 | (11.5) | 0.03 |
| Preschool Language Scale: | ||||||||||
| Auditory comprehension | 27 | 102.0 | (26.0) | 99 | 102.0 | (25.0) | 36 | 103.0 | (20.0) | 0.88 |
| Expressive communication | 26 | 102.0 | (17.0) | 104 | 102.0 | (23.0) | 36 | 106.0 | (13.5) | 0.83 |
| Total language score | 26 | 105.0 | (27.0) | 99 | 100.0 | (24.0) | 36 | 106.0 | (18.0) | 0.91 |
For all scores, higher indicates better score.
Table 4
Adjusted models for neurodevelopmental outcomes comparing unshunted hydrocephalus to no hydrocephalus and shunted hydrocephalus to no hydrocephalus
| All | Odds ratio | 95% confidence interval | |
| Bayley Psychomotor Index | |||
| Unshunted hydrocephalus vs. no hydrocephalus | 0.70 | (0.24–2.10) | 0.53 |
| Shunted hydrocephalus vs. no hydrocephalus | 0.74 | (0.25–2.12) | 0.57 |
| 95% confidence interval | |||
| Bayley Mental Index | |||
| Unshunted hydrocephalus vs. no hydrocephalus | 0.28 | ( | 0.28 |
| Shunted hydrocephalus vs. no hydrocephalus | 0.10 | ( | 0.70 |
| Peabody Developmental Gross Motor Scale: | |||
| Fine motor quotient | |||
| Unshunted hydrocephalus vs. no hydrocephalus | 0.11 | ( | 0.66 |
| Shunted hydrocephalus vs. no hydrocephalus | ( | 0.38 | |
| Gross motor quotient | |||
| Unshunted hydrocephalus vs. no hydrocephalus | 0.02 | ( | 0.94 |
| Shunted hydrocephalus vs. no hydrocephalus | 0.02 | ( | 0.92 |
| Total motor quotient | |||
| Unshunted hydrocephalus vs. no hydrocephalus | 0.003 | ( | 0.99 |
| Shunted hydrocephalus vs. no hydrocephalus | ( | 0.65 | |
| Preschool Language Scale: | |||
| Auditory comprehension score | |||
| Unshunted hydrocephalus vs. no hydrocephalus | 0.06 | ( | 0.82 |
| Shunted hydrocephalus vs. no hydrocephalus | 0.08 | ( | 0.74 |
| Expressive communication score | |||
| Unshunted hydrocephalus vs. no hydrocephalus | 0.11 | ( | 0.68 |
| Shunted hydrocephalus vs. no hydrocephalus | 0.03 | ( | 0.92 |
| Total language score | |||
| Unshunted hydrocephalus vs. no hydrocephalus | 0.11 | ( | 0.68 |
| Shunted hydrocephalus vs. no hydrocephalus | 0.08 | ( | 0.75 |
Adjusted for: surgery assignment (prenatal vs postnatal), ventricular size at screening and maternal education.
Table 5
Severity of hydrocephalus in those who met criteria for shunting
| Univariable | Adjusted | |||||||||
| 1 criterion met | 2 | |||||||||
|
| % |
| % | OR | 95% CI | |||||
| Bayley Psychomotor Index | 49 | (42) | 7 | (26) | 0.13 | 0.56 | (0.21–1.50) | 0.25 | ||
|
| Median | IQR |
| Median | IQR | Estimate | 95% CI | |||
| Bayley Mental Index | 117 | 94.0 | (15.0) | 27 | 83.0 | (20.0) | 0.09 | ( | 0.20 | |
| Peabody Developmental Motor Scale: | ||||||||||
| Fine motor quotient | 117 | 94.0 | (12.0) | 26 | 88.0 | (12.0) | 0.005 | ( | 0.003 | |
| Gross motor quotient | 117 | 61.0 | (13.0) | 26 | 61.0 | (9.0) | 0.44 | ( | 0.47 | |
| Total motor quotient | 117 | 73.0 | (11.0) | 26 | 70.0 | (7.0) | 0.02 | ( | 0.02 | |
| Preschool Language Scale: | ||||||||||
| Auditory comprehension | 113 | 104.0 | (25.0) | 22 | 93.0 | (17.0) | 0.02 | ( | 0.05 | |
| Expressive communication | 114 | 104.5 | (20.0) | 26 | 95.0 | (16.0) | 0.01 | ( | 0.03 | |
| Total language score | 113 | 105.0 | (22.0) | 22 | 92.0 | (17.0) | 0.004 | ( | 0.02 | |
*
3.Results
The characteristics of the three groups of subjects are provided in Table 2. There were no statistically significant differences in maternal education, fetal gender, or lesion level. As demonstrated previously [13], children in the prenatal group less frequently met shunting criteria and were less frequently shunted. Children in the prenatal group represented 92.6% of the children who did not meet shunt criteria, 63.9% of the children who met shunt criteria but who were not shunted, and 36.1% of the children who met criteria and were shunted (
Among the 108 children with shunted hydrocephalus, 91.7% met the first hydrocephalus criteria (at least 2 of the following: crossing head circumference percentiles; bulging fontanelle or split sutures or sunsetting sign; increased hydrocephalus on consecutive imaging as determined by the ratio of biventricular diameter to biparietal diameter; or head circumference greater than 95 percentile for gestational age), 5.6% met criteria 2 (presence of marked syringomyelia with ventriculomegaly), 10.2% met criteria 3 (ventriculomegaly with symptoms of Chiari malformation) and 19.4% met criteria 4 (persistent CSF leak or bulging from the repair site). The sum is more than 100% because some children met more than one criteria. In contrast, among the 36 children with unshunted hydrocephalus, 100% met the first criteria, 2.8% met the fourth criteria, while none met criterion 2 or 3.
Table 3 includes univariable comparisons between the 3 groups (no hydrocephalus, shunted hydrocephalus and unshunted hydrocephalus) for the neurodevelopmental outcomes. There were no significant differences between these groups for either of the Bayley Indices (Mental or Psychomotor) or for the Preschool Language Scale (Auditory Comprehension, Expressive Communication or Total Language score). The Peabody Gross Motor Quotient (comprised of the stationary, locomotion and object manipulation subscales) was significantly different between the hydrocephalus/shunt groups (
In order to assess the association of the severity of hydrocephalus and the outcomes for all children who met criteria for hydrocephalus, comparisons were made between those who met one criterion and those who met two or more criteria. Table 5 shows the univariate analysis which shows no differences in those who met one versus more than one criteria for the Bayley Mental or Psychomotor Indices. However, there was a difference by severity for the Peabody Fine Motor Quotient (
4.Discussion
Neurodevelopmental outcomes at 30 months of age were analyzed for 171 children participating in the MOMS trial. Children were categorized into three groups based on the presence of hydrocephalus and shunt placement to determine if the neurodevelopmental outcomes differed. In univariable analysis, differences were found on the Peabody Developmental Gross Motor and Total Motor Quotients. After adjustment, none of the comparisons were statistically different between the three groups. Children with unshunted hydrocephalus did not fare worse from a neurodevelopmental perspective as was expected. Additional analysis of only the children with hydrocephalus demonstrated that severity of the hydrocephalus, as measured by the number of hydrocephalus criteria met, was associated with poorer neurodevelopmental functioning. Children with more severe hydrocephalus had lower scores on the Fine Motor Quotient, and thus the Total Motor Quotient of the Peabody Developmental Motor Scale, and both the Auditory Comprehension and Expressive Communication sections of the Preschool School Language Scale and thus the Total Language Score.
This is the first study to evaluate neurodevelopmental outcomes for children shunted or unshunted with documented hydrocephalus based on predetermined clinical criteria compared to children without hydrocephalus. The results demonstrate relatively similar neurodevelopmental profiles between the three groups -no hydrocephalus, shunted hydrocephalus, and unshunted hydrocephalus. In contrast, other studies have found that children with spina bifida without hydrocephalus fare better than those with hydrocephalus, although different outcome measures were used [40, 42, 44, 45, 46]. We also note that in our unadjusted analysis, children without hydrocephalus seemed to fare better neurodevelopmentally for some motor outcomes. However, this difference did not persist after adjustment. This may be in part because ventricular size at screening differed statistically between the 3 groups indicating the need to control for this variable in our adjusted analysis. This difference was found to be predictive of scores on the Bayley Psychomotor Index [47]. In our analyses, children with more severe hydrocephalus fared worse on some neurodevelopmental tests likely indicating that severity is a more important driver of outcomes than whether or not a shunt was placed. Importantly, in this cohort, children with more severe hydrocephalus were more likely to have a shunt placed. This indicates the need for further research using groups of children with and without shunts who have the same severity of hydrocephalus to determine if shunting itself has an impact on neurodevelopmental outcomes.
One goal of evaluating neurodevelopmental outcomes by hydrocephalus and shunt status was to provide information that may eventually be incorporated into a clinical decision-making tool for the management of hydrocephalus in children with spina bifida. If, for example, children who met hydrocephalus criteria but were not shunted fared worse than children who met criteria and were shunted, this would indicate that not placing a shunt for a child with hydrocephalus might have long-term deleterious consequences. Or conversely, if children with shunted hydrocephalus fared worse than those with unshunted hydrocephalus, permitting some amount of ventriculomegaly instead of proceeding with a shunt would potentially be warranted. The lack of difference between these groups of children in this study does support the idea that some permissible hydrocephalus is likely a reasonable option. This is important as many neurosurgeons are actively trying to reduce shunting rates [48]. Additional research is necessary before this conclusion can be made with confidence. Furthermore, it is important to remember that in this cohort, children with more severe hydrocephalus fared worse on some outcomes and that these same children were shunted more frequently. This highlights the impact of severe hydrocephalus on neurodevelopmental outcomes.
This study has several limitations. First, number of shunt revisions which have been demonstrated to negatively impact cognitive outcomes [8], were not taken into account. Second, the timing in infancy at which the children met hydrocephalus criteria was not assessed in this analysis, which may be important because the long-term impacts of hydrocephalus may differ with age of onset. Third, although the number of study criteria for hydrocephalus that are met is known in this study, this is not a standard measure of severity. How this correlates to other measures of hydrocephalus severity is not known. Fourth, the outcomes analyzed are quite proximal and may not correlate to later childhood outcomes. Fifth, morphologic brain differences were not noted in MOMS and therefore were not included in this analysis although they could be considered in future studies [49]. Sixth, a majority of the sample had hydrocephalus and were shunted making the comparison groups unequal. The power to detect differences would have been increased with larger comparison groups. Lastly, mothers enrolled in MOMS may not be similar to other mothers with children with spina bifida, limiting the generalizability of the findings.
5.Conclusions
This analysis of 171 children enrolled in the MOMS trial evaluated neurodevelopmental outcomes at 30 months by hydrocephalus and shunt status. After controlling for multiple factors, there were no statistical differences in the outcomes when comparing children without hydrocephalus, children with shunted hydrocephalus and children with unshunted hydrocephalus. Children with more severe hydrocephalus fared worse on some neurdevelopmental assessments. Further research is warranted to evaluate neurodevelopmental outcomes by hydrocephalus severity and shunt status to help develop decision-making tools to aid neurosurgeons in the management of hydrocephalus in patients with spina bifida.
Acknowledgments
The authors are funded by the NIH NICHD U01HD0 68541 MOMS2: Follow up of the Mangement of Myelomeningocele Study. Thom and Burrows were also funded by U01-HD041665 MOMS: Management of Myelomeningocele Study.
Conflict of interest
The authors have no other financial disclosures and no conflicts of interest.
References
[1] | Parker SE, Mai CT, Canfield MA, et al. Updated National Birth Prevalence estimates for selected birth defects in the United States, 2004-2006. Birth Defects Res A Clin Mol Teratol (2010) ; 88: : 1008-16. |
[2] | Houtrow A, Dicianno B. Advances in spina bifida care: From the womb to adulthood. Current Physical Medicine and Rehabilitation Reports (2014) ; 2: : 71-8. |
[3] | McLone DG, Dias MS. The Chiari II malformation: Cause and impact. Childs Nerv Syst (2003) ; 19: : 540-50. |
[4] | McLone DG, Knepper PA. The cause of Chiari II malformation: A unified theory. Pediatric Neuroscience (1989) ; 15: : 1-12. |
[5] | Danzer E, Finkel RS, Rintoul NE, et al. Reversal of hindbrain herniation after maternal-fetal surgery for myelomeningocele subsequently impacts on brain stem function. Neuropediatrics (2008) ; 39: : 359-62. |
[6] | Burmeister R, Hannay HJ, Copeland K, Fletcher JM, Boudousquie A, Dennis M. Attention problems and executive functions in children with spina bifida and hydrocephalus. Child Neuropsychol (2005) ; 11: : 265-83. |
[7] | Del Bigio MR. Neuropathology and structural changes in hydrocephalus. Dev Disabil Res Rev (2010) ; 16: : 16-22. |
[8] | Arrington CN, Ware AL, Ahmed Y, Kulesz PA, Dennis M, Fletcher JM. Are shunt revisions associated with IQ in congenital hydrocephalus? A meta-analysis. Neuropsychol Rev (2016) ; 26: : 329-39. |
[9] | Akalan N. Myelomeningocele (open spina bifida) – surgical management. Adv Tech Stand Neurosurg (2011) ; 113-41. |
[10] | Lorber J. Results of treatment of myelomeningocele. An analysis of 524 unselected cases, with special reference to possible selection for treatment. Dev Med Child Neurol (1971) ; 13: : 279-303. |
[11] | Adzick NS. Fetal surgery for spina bifida: Past, present, future. Seminars in Pediatric Surgery (2013) ; 22: : 10-7. |
[12] | Meuli M, Moehrlen U. Fetal surgery for myelomeningocele: A critical appraisal. Eur J Pediatr Surg (2013) ; 23: : 103-9. |
[13] | Tulipan N, Wellons JC, 3rd, Thom EA, et al. Prenatal surgery for myelomeningocele and the need for cerebrospinal fluid shunt placement. J Neurosurg Pediatr (2015) ; 16: : 613-20. |
[14] | Adzick NS, Thom EA, Spong CY, et al. A Randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med (2011) . |
[15] | Houtrow A, Dicianno BE. Advances in spina bifida care: From the womb to adulthood. Curr Phys Med Rehabil Rep (2014) ; 2: : 71-8. |
[16] | Kebriaei MA, Shoja MM, Salinas SM, et al. Shunt infection in the first year of life. J Neurosurg Pediatr (2013) ; 12: : 44-8. |
[17] | Caldarelli M, Di Rocco C, La Marca F. Shunt complications in the first postoperative year in children with meningomyelocele. Childs Nerv Syst (1996) ; 12: : 748-54. |
[18] | Dias MS, Shaffer ML, Iantosca MR, Hill KL, Jr., Variability among pediatric neurosurgeons in the threshold for ventricular shunting in asymptomatic children with hydrocephalus. J Neurosurg Pediatr (2011) ; 7: : 134-42. |
[19] | Adzick NS. Fetal surgery for myelomeningocele: Trials and tribulations. Isabella Forshall Lecture. J Pediatr Surg (2012) ; 47: : 273-81. |
[20] | Radmanesh F, Nejat F, El Khashab M. Infection in myelomeningocele after VP shunt placement. Childs Nerv Syst (2011) ; 27: : 341-2, author reply 3-4. |
[21] | Radmanesh F, Nejat F, El Khashab M, Ghodsi SM, Ardebili HE. Shunt complications in children with myelomeningocele: Effect of timing of shunt placement. Clinical article. J Neurosurg Pediatr (2009) ; 3: : 516-20. |
[22] | Braga MH, Carvalho GT, Brandao RA, Lima FB, Costa BS. Early shunt complications in 46 children with hydrocephalus. Arq Neuropsiquiatr (2009) ; 67: : 273-7. |
[23] | Rocque BG, Bishop ER, Scogin MA, et al. Assessing health-related quality of life in children with spina bifida. J Neurosurg Pediatr (2015) ; 15: : 144-9. |
[24] | Wakhlu A, Ansari NA. The prediction of postoperative hydrocephalus in patients with spina bifida. Childs Nerv Syst (2004) ; 20: : 104-6. |
[25] | Tuli S, Drake J, Lamberti-Pasculli M. Long-term outcome of hydrocephalus management in myelomeningoceles. Childs Nerv Syst (2003) ; 19: : 286-91. |
[26] | Vinchon M, Dhellemmes P. Cerebrospinal fluid shunt infection: Risk factors and long-term follow-up. Childs Nerv Syst (2006) ; 22: : 692-7. |
[27] | Mapstone TB, Rekate HL, Nulsen FE, Dixon MS, Jr., Glaser N, Jaffe M. Relationship of CSF shunting and IQ in children with myelomeningocele: A retrospective analysis. Childs Brain (1984) ; 11: : 112-8. |
[28] | Davis BE, Daley CM, Shurtleff DB, et al. Long-term survival of individuals with myelomeningocele. Pediatr Neurosurg (2005) ; 41: : 186-91. |
[29] | Paulsen AH, Lundar T, Lindegaard KF. Pediatric hydrocephalus: 40-year outcomes in 128 hydrocephalic patients treated with shunts during childhood. Assessment of surgical outcome, work participation, and health-related quality of life. J Neurosurg Pediatr (2015) ; 16: : 633-41. |
[30] | McLone DG, Zebracki K. Intelligence quotient in children with meningomyeloceles. J Neurosurg (2007) ; 106: : 103-4, discussion 4-5. |
[31] | Nejat F, Kazmi SS, Habibi Z, Tajik P, Shahrivar Z. Intelligence quotient in children with meningomyeloceles: A case-control study. J Neurosurg (2007) ; 106: : 106-10. |
[32] | Adzick NS, Thom EA, Spong CY, et al. A randomized trial of prenatal versus postnatal repair of myelomeningocele. N Engl J Med (2011) ; 364: : 993-1004. |
[33] | Chakraborty A, Crimmins D, Hayward R, Thompson D. Toward reducing shunt placement rates in patients with myelomeningocele. J Neurosurg Pediatr (2008) ; 1: : 361-5. |
[34] | Liptak GS, Bolander HM, Langworthy K. Screening for ventricular shunt function in children with hydrocephalus secondary to meningomyelocele. Pediatr Neurosurg (2001) ; 34: : 281-5. |
[35] | Phillips BC, Gelsomino M, Pownall AL, et al. Predictors of the need for cerebrospinal fluid diversion in patients with myelomeningocele. J Neurosurg Pediatr (2014) ; 14: : 167-72. |
[36] | Sutton LN. Fetal surgery for neural tube defects. Best Pract Res Clin Obstet Gynaecol (2008) ; 22: : 175-88. |
[37] | Bowman RM, McLone DG. Neurosurgical management of spina bifida: research issues. Dev Disabil Res Rev (2010) ; 16: : 82-7. |
[38] | Werner EE, Bayley N. The reliability of Bayley’s revised scale of mental and motor development during the first year of life. Child Development (1966) ; 37: : 39-50. |
[39] | Palisano RJ. Concurrent and predictive validities of the Bayley Motor Scale and the Peabody Developmental Motore Scales. Phys Ther (1986) ; 66: : 1714-9. |
[40] | Johnson MP, Gerdes M, Rintoul N, et al. Maternal-fetal surgery for myelomeningocele: Neurodevelopmental outcomes at 2 years of age. Am J Obstet Gynecol (2006) ; 194: : 1145-50, discussion 50-2. |
[41] | Schoenmakers MA, Gulmans VA, Gooskens RH, Helders PJ. Spina bifida at the sacral level: More than minor gait disturbances. Clin Rehabil (2004) ; 18: : 178-85. |
[42] | Warf B, Ondoma S, Kulkarni A, et al. Neurocognitive outcome and ventricular volume in children with myelomeningocele treated for hydrocephalus in Uganda. J Neurosurg Pediatr (2009) ; 4: : 564-70. |
[43] | Zimmerman IL, Castilleja NF. The role of a language scale for infant and preschool assessment. Ment Retard Dev Disabil Res Rev (2005) ; 11: : 238-46. |
[44] | Vachha B, Adams RC. Memory and selective learning in children with spina bifida-myelomeningocele and shunted hydrocephalus: A preliminary study. Cerebrospinal Fluid Res (2005) ; 2: : 10. |
[45] | Lindquist B, Uvebrant P, Rehn E, Carlsson G. Cognitive functions in children with myelomeningocele without hydrocephalus. Childs Nerv Syst (2009) ; 25: : 969-75. |
[46] | Iddon JL, Morgan DJ, Loveday C, Sahakian BJ, Pickard JD. Neuropsychological profile of young adults with spina bifida with or without hydrocephalus. J Neurol Neurosurg Psychiatry (2004) ; 75: : 1112-8. |
[47] | Farmer DL, Thom EA, Brock JW, 3rd, et al. The management of myelomeningocele study: Full cohort 30 month pediatric outcomes. Am J Obstet Gynecol (2017) . |
[48] | Phillips BC, Gelsomino M, Pownall AL, et al. Predictors of the need for cerebrospinal fluid diversion in patiens wihth myelomeningocele. Journal of Neurosurgical Pediatrics (2014) ; 14: : 167-72. |
[49] | Mandell JG, Kulkarni AV, Warf BC, Schiff SJ. Volumetric brain analysis in neurosurgery: Part 2. Brain and CSF volumes discriminate neurocognitive outcomes in hydrocephalus. J Neurosurg Pediatr (2015) ; 15: : 125-32. |
[50] | O’Hayon BB, Drake JM, Ossip MG, Tuli S, Clarke M. Frontal and occipital horn ratio: A linear estimate of ventricular size for multiple imaging modalities in pediatric hydrocephalus. Pediatr Neurosurg (1998) ; 29: : 245-9. |


