
Parkinson’s Disease in Sub-Saharan Africa: Pesticides as a Double-Edged Sword
Abstract
Long-term exposure to pesticides used in agriculture is increasingly being identified as a risk factor for developing Parkinson’s disease. How chronic pesticide exposure might contribute to the growth of Parkinson’s disease in the mainly agricultural communities of Sub-Saharan Africa has thus far received limited attention. There are specific concerns in this area of the world: aging of the population, in combination with chronic exposure to widely used pesticides, including those that have been restricted elsewhere in the world because of neurotoxicity and other health risks. Of interest, the prevalence of Parkinson’s disease among specific (semi)nomadic populations in Tanzania seems very low, possibly due to their lack of exposure to agricultural chemicals. But at the same time, pesticides have also brought important benefits to this part of the world. Specifically, in Sub-Saharan Africa, pesticides have been directly helpful in preventing and controlling famine and in containing major human infectious diseases. This creates a complex risk-benefit ratio to the use of pesticides within a global perspective, and urgently calls for the development and implementation of affordable alternatives for areas such as Sub-Saharan Africa, including non-neurotoxic compounds and non-chemical alternatives for the use of pesticides.
INTRODUCTION
There has been a steep increase in the worldwide prevalence of Parkinson’s disease (PD) in recent decades, making it the fastest growing neurological condition globally [1, 2]. In addition to aging and genetic factors [3], lifetime exposure to low grade risk factors such as the presence of toxins in our environment contributes to the rise of PD [1, 4, 5]. Pesticides are one example of environmental toxins that have been linked to the etiology of PD. Farmers appear to have a significantly increased risk of developing PD [1, 4] and the raised risks may also affect people living in the immediate vicinity of farmland where pesticides are used [4, 5]. Various pesticides are toxic to dopamine-producing cells in the substantia nigra, leading to parkinsonian signs in exposed animals [1].
The ‘Parkinson Pandemic’ [1] does not spare Sub-Saharan Africa (SSA) although a global survey from 2016 shows an age-adjusted PD prevalence approximately three to four times lower than Canada and the United States [2]. There is very limited information on the incidence of PD [2, 6]. The published prevalence of PD in SSA ranges from 7-67/100,000, with 30/100,000 reported in a large community-based study in Tanzania [2, 6]. The mean age of onset of PD in the latter study was 69.4 years [6], with one decade later a trend towards a lower age of onset at 62 (53–73) years [7]. A recent South African study involving 687 cases of PD in mixed race persons reported an onset age of 57.3 years. For the subgroup of 102 persons of African ancestry, the age at onset was 54.8 years [8].
These figures are difficult to compare, however, as hospital-based studies in SSA identify cases with access to hospital services, which typically includes those patients whose costs are covered by national insurance or are self-financing—they are more likely to be younger compared to the typically older patients who are more likely to resort to traditional medicine within the local community.
Contributory reasons for the reported low prevalence of PD include the relatively low life expectancy in SSA during the time of the studies, ranging from 57.5 years in 2011 to 60.24 years in 2021. When this is coupled with socioeconomic deprivation and the relative lack of access to neurologists and specialized neurological health care services, then the lower reported rates of PD are better understood. Migrant studies suggest a higher prevalence of PD in persons of African ancestry living in USA [6]. Factors which are known to influence the frequency of PD in high income countries such as genetics, lifestyle including diet, smoking, exercise, and environment remain to be studied in detail in Africa [9]. However, a possible cause in Africa which may be of much more relevance and importance is occupational and passive exposure to pesticides with the worrying possibility that the duration of exposure from early childhood may be a critical factor in later disease pathogenesis.
The lower reported prevalence of PD is not common to all neurological diseases in SSA but diseases like dementia, that similar to PD affect a mainly older age group and typically do not disable the patient immediately also tend to go under diagnosed and hence under reported. In contrast those neurological diseases that affect a mainly younger age group, such epilepsy and headache or present acutely such as stroke or paraplegia are well reported in studies in SSA. Indeed, the prevalence of stroke is reported to be higher in SSA than in high income countries [2, 7].
There is a ‘diagnosis and treatment gap’ for PD in SSA due to its low neurologist-to-population ratio. This means that the lion’s share of patients in this part of the world never see a physician or neurologist during their lifetime [6]. Presently each country in SSA has at least one neurologist, but for some countries such as Djibouti and Malawi it literally means just a single neurologist for an entire population as large as 20 million persons [9]. We can take the United Republic of Tanzania as an example, which was recently classified as a lower middle income country, and which has a population of over 60 million and a life expectancy of 67 years [10]. Tanzania has approximately one neurologist per 5 million inhabitants. In reality, this ratio may actually be even more worrisome, because of the common under recognition of PD in this part of the world, which occurs for a variety of reasons: cultural acceptance of PD as part of normal aging (and not as a disease), easier access to traditional medicine, and stigmatization [6, 11]. In the only available rural community prevalence study on PD, less than a quarter of patients were previously diagnosed and even fewer were on regular treatment [6].
SSA DEMOGRAPHY
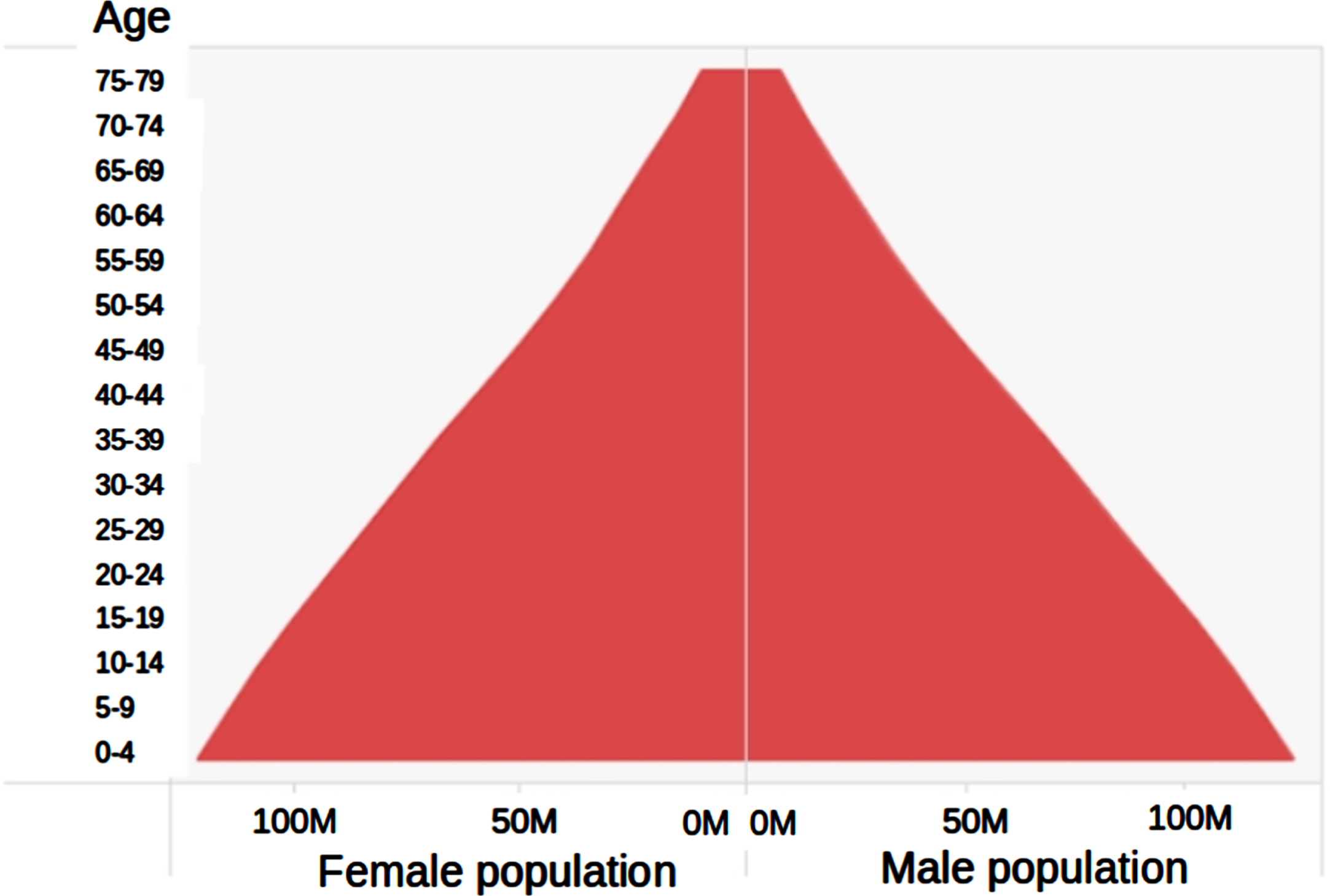
Presently over 1.2 billion people (16% of the world’s citizens and its youngest population) live in SSA, an area which is forecast to expand in population size, as opposed to the rest of the world where stagnation or decrease is expected [10]. Within a generation, life expectancy in SSA has increased by 10 years to 62 years [10]. Primary disease prevention and better healthcare and nutrition are mainly responsible for this improvement. SSA has a pyramidal age distribution (Fig. 1), skewed towards younger ages with 42% of people aged <15 years [9]. The projected population of SSA by 2050 is estimated to be 2.5 billion, or 25% of the world’s population [10]. A concurrent rise in the incidence and prevalence of PD is therefore expected in SSA. This is all the more reason why SSA has to act now on reducing the risk of developing this disease, for example by limiting the exposure to pesticides. While exposure to pesticides to the average rural SSA inhabitant is omnipresent, quantification is difficult with limited data available specifically on longer term neurotoxic effects [5, 12–14]. Factors that complicate study of the relationship between pesticides in PD include the fact that chronic exposure to pesticides may require an up to several decades long incubation prior to leading to symptoms of PD. Moreover, the same pesticide level is likely more toxic for an infant than an adult [15]. When viewed in person years, long term toxin exposure for the youth in SSA, with their much improved survival and population expansion, impacts their health and safety to an unknown extent.
Fig. 1
Pyramidal age distribution in millions population per gender projected for SSA 2050. United Nations, Department of Economic and Social Affairs, Population Division (2013). World Population Prospects: The 2012 Revision. (https://www.ageing.ox.ac.uk/population-horizons/data/gpt, Accessed October 17, 2023).
POPULATIONS WITH LITTLE TO NO PD
Where there is universal exposure, it may be difficult to assess causality. In a disease such as PD whose etiology has only been established in part, studies on ‘absence of’ may be as informative as studies on ‘presence of’ the condition. SSA still has exceptional nomadic and semi-nomadic populations such as the Hadzabe, one of the last hunter gatherer tribes in the world living around Lake Eyasi in Northern Tanzania [16]. They live largely off game shot by bow and arrow and by foraging the savannah brush for wild fruits, honey, and tubers. Hadzabe nomads migrate over large distances which could facilitate identification of anyone with impaired mobility such as by a movement disorder because they slow down the group. Although this is anecdotal evidence, to the best of our knowledge, long serving medical and research staff in the wider roaming area with experience as far back as the 1960 s have never identified a case of PD among the Hadzabe. Limited exposure to environmental chemicals could be one explanation, although it is also possible that many individuals of this tribe never live long enough to develop PD. Indeed, in the previous century the tribe comprised several tens of thousands of individuals but has declined to 1,300 individuals in 2015 with an estimated life expectancy at birth of just 33 years [16]. Life expectancy in hunter gatherer populations, however, is strongly determined by high infant and childhood mortality. Those who survive childhood may live well into their seventies, so a woman surviving to age 45 has an estimated life expectancy of another 23 years [16]. A largely similar observation applies to the at least 1 million pastoralist Maasai living across vast savannah of Northern Tanzania, with a life expectancy at birth of 45 years [17]. Over 40 years of clinical practice in the area by neurologists and doctors of Maasai origin working in the catchment area have identified just three cases of PD in Maasai individuals, all being non-pastoralists with higher education.
Apart from a non-sedentary lifestyle (which could itself be partially protective against the risk of developing PD) a common factor in both tribes is a lack of occupational exposure to pesticides. Hadzabe roam and do not grow vegetables. A traditional Maasai diet also does not contain any vegetables and the only exposure to pesticides is occasional to male Maasai pastoralists when cows require seasonal spraying with the insecticide pyrethrin. This observation may imply a lower than average risk in those people who are minimally or unexposed to pesticides. This observation needs caution due to the tribes’ shorter life expectancy and small numbers. Furthermore, they have their own traditional medicine systems and live in remote areas, so not all health conditions will present to hospital. Unknown genetic factors (e.g., risk genes selected out of nomadic populations due to impaired mobility) may also play a role. There has never been a prevalence study to try and identify people who might have PD in these populations. No other studies on PD in hunter gatherer populations are available, but the absence of other conditions in other hunter gatherers may suggest favorable environmental factors, such as the absence of acne vulgaris in the Kitavan Islanders of Papua New Guinea and the Aché Hunters of Paraguay [18]. The apparently low incidence of PD among these hunter gatherer populations is an area that is worthy of further detailed study.
RISE OF PESTICIDE USE IN SSA
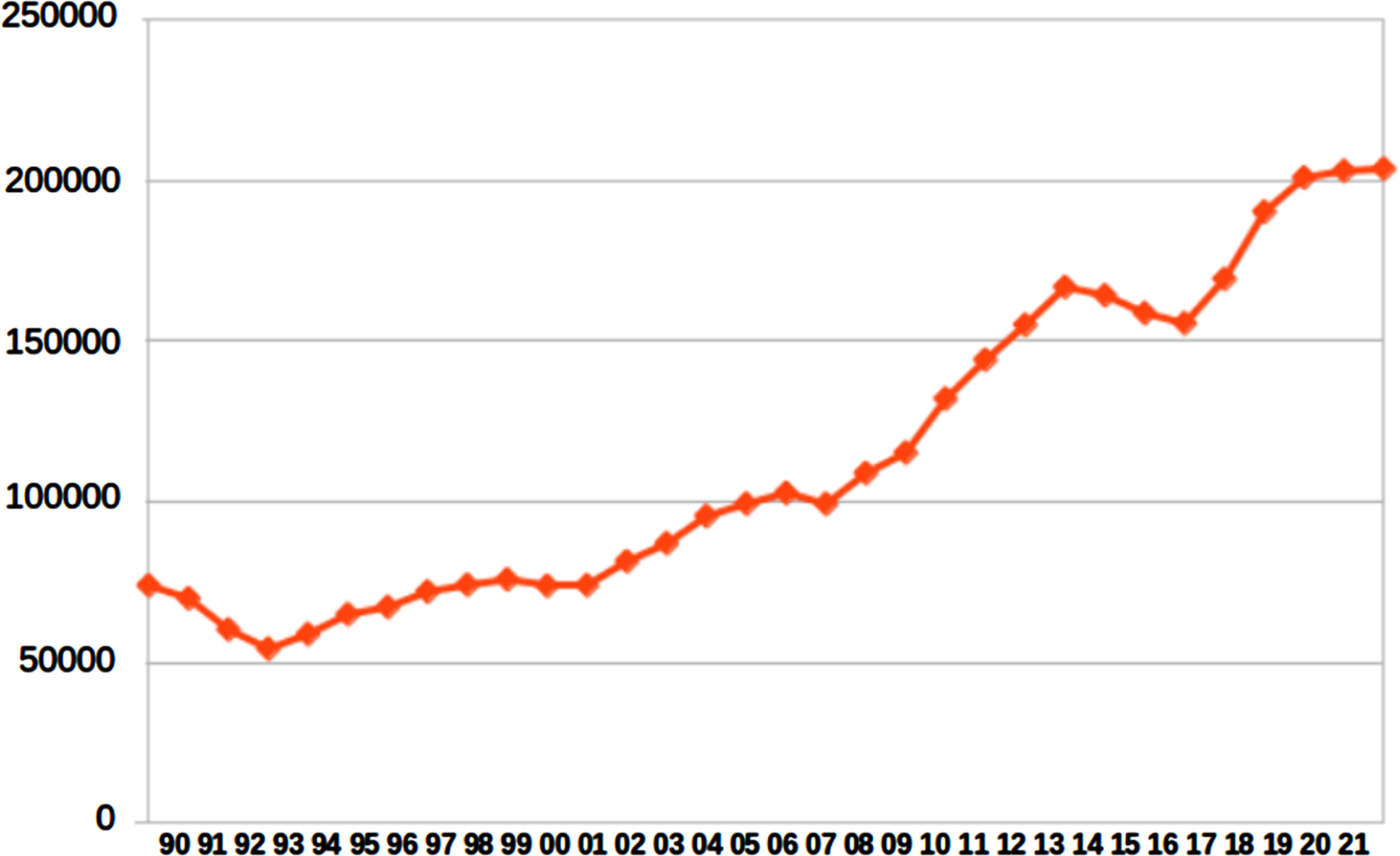
Compared with the rest of the world, Africa’s use of pesticides is lower due to its geography with less arable land, restricted resources. and smaller scale farming methods (Fig. 2). Pesticide use in SSA has tripled over the past decades (Fig. 3) making it the relatively fastest growing pesticide market [12, 13, 19]. Data on pesticide usage over time in Africa are only available for 18 of 54 African countries and mainly those situated North of SSA [12]. There are no reliable figures on the longer term use of pesticides in Africa in the more distant past. In Tanzania under a period of socialism in the 1960s-1980 s pesticides were widely used and often available for free in order to encourage people to grow their own crops and to be self sufficient.
Fig. 2
Total pesticide use by continent worldwide. Compared with the rest of the world, Africa’s use of pesticides is lower due to its geography with less arable land, restricted resources and smaller scale farming methods (https://www.fao.org/faostat/en/#data/RP, Accessed October 17, 2023).
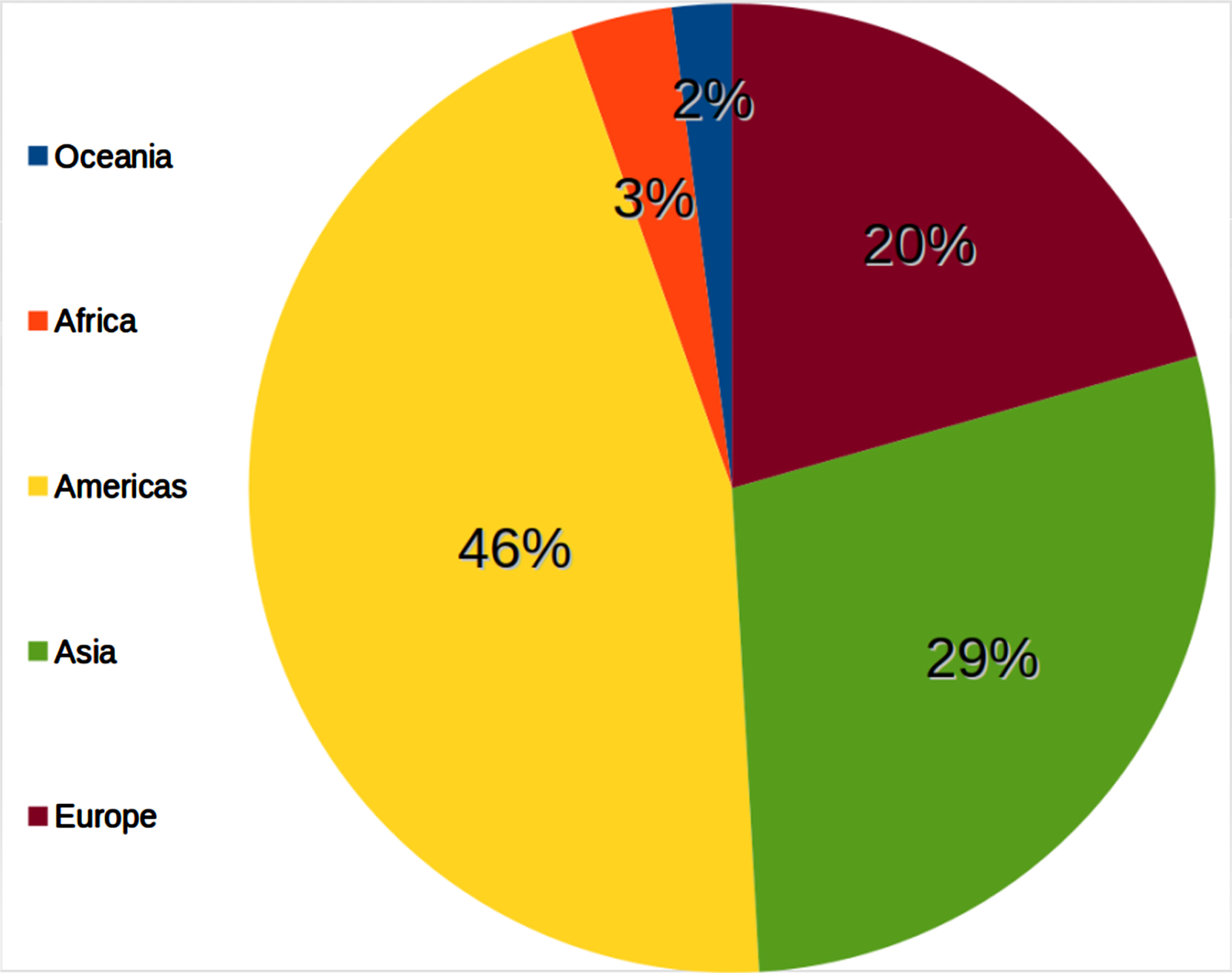
Fig. 3
Total pesticide use in tonnes in Africa 1990–2021. Pesticide use in SSA has tripled over the past decades. (https://www.fao.org/faostat/en/#data/RP, Accessed October 17, 2023).
Pesticides are reasonably affordable and available over the counter for the SSA citizen. The omnipresence of pesticides is illustrated by common hospital admissions across all ages and throughout 4 decades of neurological disorder registration in Tanzania for acute intoxications with organophosphates and paraquat, with an almost 25% mortality in 47 adult cases and a median age of 31 years ([20], WPH personal communication).
Apart from acute intoxications, chronic exposure to pesticides does not only apply to farmers but also to all consumers of pesticide-treated food. Organophosphates, for instance, are lipophilic and accumulate in brain tissue which may already start in utero following maternal exposure. Breast milk and common foods in SSA were shown to contain alarming quantities of pesticides linked to PD pathogenesis [1, 4, 5, 14, 15]. Although governmental guidelines are in place, limited training and materials are available to protect the SSA farmer [21–23]. Most are subsistence farmers and frequently manage to grow only enough crops sufficient for their own use. They may spend a lifetime of manual labor on their fields, with their hoes as the only equipment and bare-hand applied spray pesticide as their guarantee of yield (Fig. 4). Discussion of ‘pros and cons’ of pesticides in the community and education on how to mitigate risks of pesticide use is still in development and subject to non evidence based perceptions among farmers and retailers, and to restricted resources [21–23].
Fig. 4
Tanzanian farmers using pesticides (photo with permission of depicted individuals, RJ Mwezi).

In comparison to high income countries where pesticides are mainly applied to optimize crop yield, in SSA they are needed to prevent hunger and infectious disease such as malaria, which still results in 250 million cases and causes over half a million deaths annually [24]. The success of pesticides is illustrated by the example of tsetse fly transmitted trypanosomiasis, a major parasitic infection of humans and other large mammals which used to ravage African society over the previous centuries, but now largely eradicated by virtue of regular pesticide wash for cattle. Subsistence crops which have benefited in particular from better pest control in terms of better crop yield have improved the overall nutritional status of a mainly young population in SSA. They include the staple foods maize, cassava and wheat and rice. The last recorded major large scale famine in SSA was almost 40 years ago although periodic food shortages continue to occur because of local climatological changes and political conflict.
A GLOBAL RESERVOIR
Analogous to the human brain as a reservoir for lipophilic pesticides, SSA is a global chemical reservoir for phased out pharmacological and chemical compounds, with pesticides being an example. Pesticides banned in the country of manufacture may continue to be exported to global destinations such as SSA [14, 25]. Figure 5 depicts the number of banned all-purpose hazardous pesticides specified for SSA countries, showing the median position of Tanzania being a rather representative country for this region [25, 26]. Table 1 lists a number of PD-linked pesticides and their status in Tanzania [1, 5, 25–32]. Most presently known PD linked pesticides have been banned in many areas of the world, particularly in high income regions, yet some of these pesticides continue to be used in SSA. Table 1 also shows organochlorines linked to PD [5, 25] which have been banned in many countries including SSA but still being used in the United States. Despite documented adverse effects on the ecosystem and carcinogenic risks, hazardous pesticides persist in SSA for lack of affordable and safer alternatives to control famine and epidemics. Some of those banned decades ago have a sheer ineradicable presence in the ecosystem [14, 15, 21], hence SSA can be viewed as the ‘tip’ of a global chemicals chain, a reservoir for various chemical products of which pesticides are a most concerning example.
Fig. 5
Number of banned all-purpose pesticides per country (https://pan-international.org, Accessed October 1, 2023). EU, European Union; UK, United Kingdom; DRC, Democratic Republic of Congo; CAR, Central African Republic.
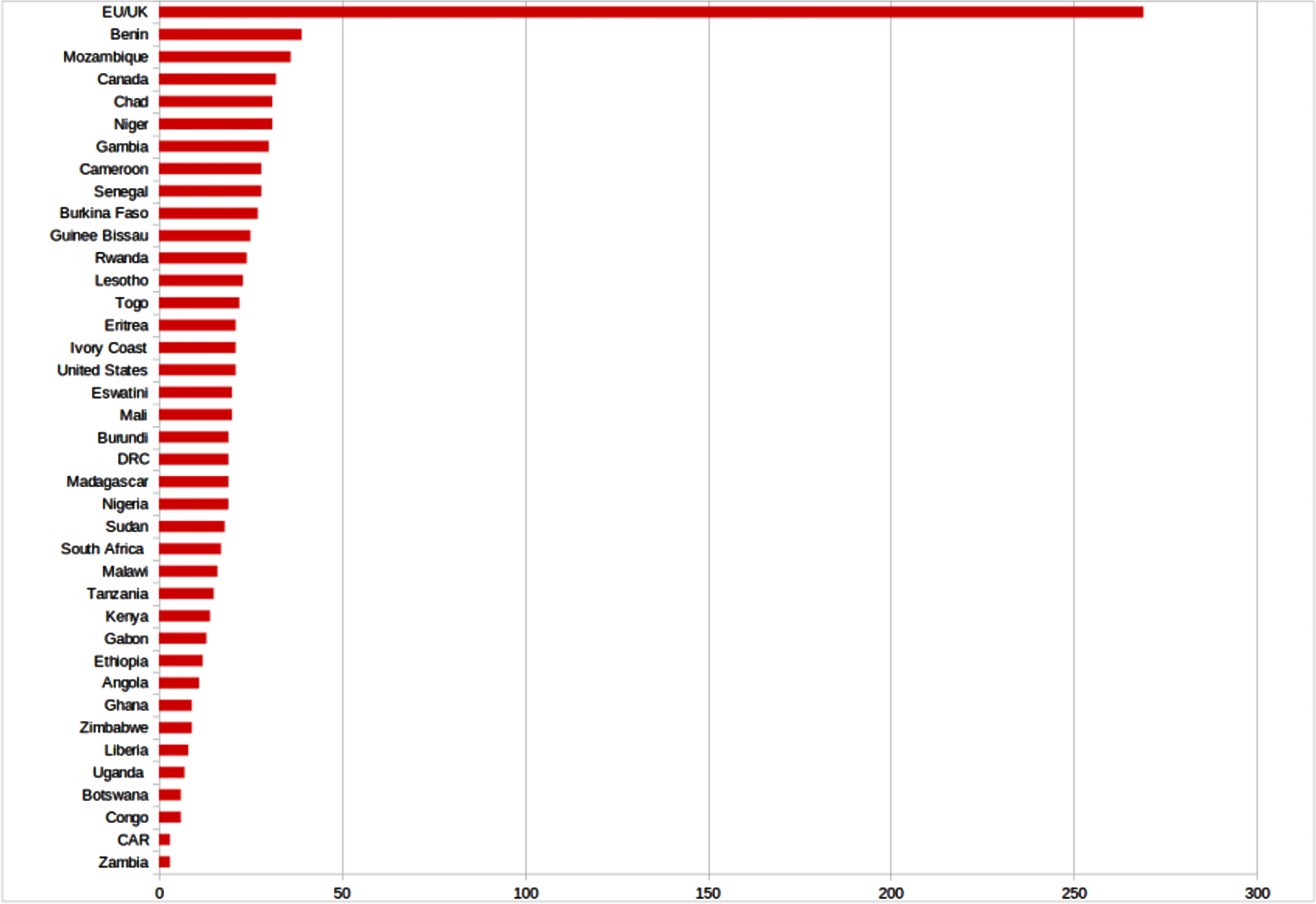
Table 1
Pesticides linked to Parkinson’s Disease globally and in Sub-Saharan Africa [1, 5, 25–33]
| Name | Pesticide type* | WHO class** | Study findings | Banned in: United States (US), Canada (C), European Union (EU) or United Kingdom (UK)*** | Registration status in United Republic of Tanzania**** | Countries of imported pesticide origin | Reference |
| Aldrin | Organochlorine | O | Widely in use in SSA in the 1980s and 1990s. Banned in most countries worldwide due to multisystem toxicity. Dieldrin is its extremely stable metabolite. | EU/UK (1991) US (1974) C (1974) | Banned | [1, 15, 25–27] | |
| Atrazine | Chlorinated triazine | 3 | Detected throughout African diet foods in SSA total diet study. | EU/UK restriction to essential use (2004) | Full | Switzerland, Kenya, China, South Africa | [14, 25–27] |
| Chlorpyrifos | Organophosphate | 2 | Most commonly sold pesticide worldwide [18–21]. One of the most important pesticides in a PD prevalence community study in Tanzania [6]. The most prevalent pesticide in a study on SSA total daily diet, with exceptionally high concentrations in smoked fish products from Western Africa [14]. Fish in smoked or salted form is an important affordable source of animal protein in many parts of Africa and is promoted to optimize children’s growth. | EU/UK: widely usedUS: ban for food production only (2021) C phase out (2021) | Full | Israel, Germany, China, Kenya | [6, 14, 25–27] |
| Copper sulphate (basic and pentahydrate) | Heavy metal | 2 | Non biodegradable but listed as organic pesticide. In use in agriculture since the 1700s. One of the most important pesticides along with chlorpyrifos in a PD prevalence community study in Tanzania [6]. Among 10 pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study [5] | EU/UK: repermitted (2009) after initial ban (2002) | Full | Norway, Italy, Germany | [5, 6, 25–27] |
| Diazinon | Organophosphate | 2 | Significantly elevated odds ratios in PD case control study [29] | EU/UK (2006)US: phase out for residential use (2004) but still available (2023) | Full | Singapore | [14, 25–27, 29] |
| Dichlorodipheny-ltrichloroethane (DDT) | Organochlorine | 2 | DDT used to be a major insecticide globally. Purpose in SSA to control malaria but increasingly banned. Breast milk study from Ethiopia showing recent metabolites which indicate illegal use and bioaccumulation through mother- infant transmission [15]. | EU/UK (1986) US: 1972 C: 1990 | Ministry of Health commissioned use in very exceptional circumstances only | [15, 25–27] | |
| Dicofol | Organochlorine | 2 | Among 10 pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study [5] | EU/UK severe restrictions (1991) | Banned | – | [5, 24–26] |
| Dieldrin | Organochlorine | O | Extremely stable metabolite of aldrin. Banned in most countries worldwide due to multisystem toxicity, in US since 1975. | EU/UK (1981) US (1974) C (1984) | Banned | – | [1, 15, 25–27] |
| Diquat dibromide | Dipyridyl | 2 | Second most potent of ten pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in heat map study [5] | EU/UK (2018) C: phase out | Full | China | [5, 25–27, 29, 31] |
| Endosulfan | Organochlorine | 2 | Among 10 pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study [5] | EU/UK (2012) US (2016) C (2018) | Banned | – | [5, 25–27] |
| Endothal-sodium | Organochlorine | 2 | Among 10 pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study [5] | US (1996) | Banned | – | [5, 25–27] |
| Folpet | Phthalimide fungicide | U | Third most potent of 10 pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study | EU/UK suspended registration (2018) | Banned | – | [5, 25–27] |
| Glyphosate | Organophosphate | 3 | Roundup® (Bayer Inc.) is most commonly used pesticide in Canada | EU/UK ban for household use (2017) otherwise widely used US phase out started (2023) C use increased but ban for household use pending | Full | Switzerland, Germany, China, India, Israel, Kenya | [25–27, 29] |
| Heptachlor | Organochlorine | O | Banned in most countries worldwide due to severe toxicity | US (1987) C (1991) EU/UK (1984) | Banned | – | [1, 25] |
| Malathion | Organophosphate | 3 | Significantly elevated odds ratios in PD case control study [29] | EU/UK partial ban and restricted use in greenhouses (1986) C (2018) | Full | Kenya | [25–27, 29] |
| Maneb | Dithiocarbamate fungicide (combination of manganese with ethylene bisdithiocarbamate) | U | Exposure to the dithiocarbamate maneb induces Parkinson’s disease-like neurotoxicity in mice. Among 10 pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study [5] Mancozeb is a related pesticide that consists of Maneb and is still registered for use being regarded as safer alternative for highly hazardous pesticides by WHO/FAO. | EU/UK (2009) US (2017) | Full registration for Mancozeb | India, China | [5, 21, 25–27, 30] |
| Naled | Organophosphate | 2 | Fourth most potent of 10 pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study | EU/UK (2005) | Banned | – | [1, 5, 25, 26] |
| Paraquat | Dipyridyl | 2 | Several studies link paraquat to risk of PD. One of two most common intoxications in a semirural Tanzanian hospital over 4 decades along with organophosphate intoxication (WH personal communication). | EU/UK (2007) C (2018) | Restricted | Switzerland, Taiwan, China, Kenya, South Africa | [1, 5, 25–29, 31] |
| Parathion | Organophosphate | 2 | Most significantly elevated odds ratios in case control study on pesticide exposure in PD [29] | EU/UK severe restriction (2003) US (1998) C (2013) | Banned | – | [25–27, 29] |
| Permethrin | Pyrethroid | 2 | Permethrin is on the World Health Organization’s List of Essential Medicines and a registered pesticide throughout East Africa. Well known chemical for mosquito net impregnation and treatment of scabies and lice and other parasites. In a SSA total daily diet study, permethrin significantly contaminated 44% of beans, and 25% of cassava [14]. Beans are a source of protein and cassava is the first staple food for the African continent before maize, preventing starvation in case of failing harvests. | Widely used EU/UK (2003) US/C restricted use | Full | Switzerland, Kenya | [14, 25–28] |
| Propargite | Organosulfite acaracide/miticide | 2 | Single most potent of all 10 pesticides studied, leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study [5] | EU/UK (2011) | Full | [5, 25–27] | |
| Rotenone | Naturally occurring isoflavone derived from certain plant roots | 2 | A pesticide known to be linked to PD for almost 4 decades | EU/UK (2009) US/C phase out except for as piscicide | Banned | – | [1, 25–27, 32] |
| Trifluralin | Trifluralin | U | Commonly used herbicide. Among 10 pesticides leading to significant cell death in vitro associated with PD occurrence and exposure in US heat map study [5] | EU/UK (2008) | Not available | [5, 25, 26] |
*Note: many pesticides can still be found in residual amounts in the soil many years after their application [1, 4, 5, 14, 15]. WHO Toxicity Class: 1a – extremely hazardous; 1b – Highly hazardous; 2 – Moderately hazardous; 3 – Slightly hazardous; U – Not Hazardous; O – believed to be obsolete. **https://www.who.int/publications/i/item/9789240005662 accessed October 1, 2023. *** https://pan-international.org accessed October 1, 2023. ****Registered pesticides for use in the United Republic of Tanzania. Tanzania Plant Health and Pesticides Agency/Tropical Pesticides Research Institute. www.kilimo.go.tz.
SAFETY AND EDUCATION ON PESTICIDE USE
Education amongst SSA farmers and retailers regarding pesticide use and its possible longer term effects is minimal [13, 19, 21–23]. While pesticide safety regulations are in place they are not strictly enforced, and farmers may apply the chemicals without formal training on their proper use. Protective equipment may not be available or not used consistently [13, 19, 21–23]. Pesticides are frequently decanted on the shop counter or field, and applied without the use of personal protection by gloves, gown, or mask [21, 22] (Fig. 5). Recent studies have in fact questioned the efficacy of protective equipment against pesticide toxicity, so more work and effort is needed to better protect those working with pesticides [1, 21, 22]. Although farmers are commonly aware of possible harmful consequences, knowledge is limited and mostly concerns acute poisoning [20]. Raising awareness and policy implementation with enforcement of regulations and process were identified as the key issues in pesticide handling [21–23]. The majority of pesticide retailers in a Tanzanian survey were young adults who had not attended secondary school education, although almost half of them had attended a dedicated pesticide training course offered by governmental or non-governmental organizations [21]. As an illustration, pesticides were commonly recommended as being effective when the user had experienced direct side effects, such as skin and eye irritation or difficulty in breathing [19, 21, 22]. Use of combined pesticide ‘potions’, which have a stronger association with PD than single pesticides [5, 21], are commonly based on a relative or neighbor’s advice rather than product label instructions [19, 21, 22].
RISK BENEFIT RATIO
The risk benefit ratio of the increasing use of insecticides in SSA highlights the vexing dilemma of their possible longer term damage versus their proven acute survival benefit. An argument that was historically very valid in SSA may now be less so. Life expectancy in SSA has improved and the burden of non-communicable diseases is increasing alarmingly, largely driven by high rates of hypertension, diabetes, and obesity, mostly secondary to changes in diet and lifestyle [33]. This a strong argument in favor of a safer approach to nutrition and in particular to safer insecticides and for a quantitative decrease in their use. The role of more specific risk factors for PD including diet, genetics, smoking and head trauma have not been studied in depth to date in SSA and will need to be assessed in future studies [9]. Such studies will have to be tailored to the specific circumstances in SSA, including the resources available to perform research. For example, recent work has started to identify specific genetic risk factors for PD that are particularly relevant for African populations [3]. Exposure studies could address continued use of certain highly toxic pesticides that have already been banned in many western countries. Registry studies using for instance medical claims databases are difficult to perform due to a need of uniform, standardized registration mechanisms which are likely to be lacking in most of SSA. Longitudinal cohort studies will likely be expensive and highly dependent on the scarcely available human resources, limiting their feasibility. But case control studies might prove an effective strategy to gather more specific evidence for this part of the world.
CONCLUSION
When the epidemiological and experimental evidence of a causal link between pesticide exposure and PD is viewed in the light of increased life expectancy, rural SSA in particular can expect a rise in the burden of PD. Increased use of pesticides and exposure to the present African population could lead to larger numbers of individuals with PD in future generations.
Pesticides in SSA underlie a societal dilemma, having sacrificed safety for production: they are critical for both food security and for control of acute human infectious disease. Affordable and less neurotoxic pesticides or non-chemical alternatives to the use of pesticides (such as biological farming) are urgently needed. As the Parkinson pandemic continues to unfold, it will inevitably shed more light on the critical role of pesticides in PD in SSA and worldwide.
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The authors have no funding to report for this contribution.
CONFLICT OF INTEREST
Dr. E.R. Dorsey has received honoraria for speaking at American Academy of Neurology, American Neurological Association, Excellus BlueCross BlueShield, International Parkinson’s and Movement Disorders Society, National Multiple Sclerosis Society, Northwestern University, Physicians Education Resource, LLC, PRIME Education, LLC, Stanford University, Texas Neurological Society, and Weill Cornell; received compensation for consulting services from Abbott, Abbvie, Acadia, Acorda, Bial-Biotech Investments, Inc., Biogen, Boehringer Ingelheim, California Pacific Medical Center, Caraway Therapeutics, Curasen Therapeutics, Denali Therapeutics, Eli Lilly, Genentech/Roche, Grand Rounds, Huntington Study Group, Informa Pharma Consulting, Karger Publications, LifeSciences Consultants, MCM Education, Mediflix, Medopad, MedRhythms, Merck, Michael J. Fox Foundation, NACCME, Neurocrine, NeuroDerm, NIH, Novartis, Origent Data Sciences, Otsuka, Physician’s Education Resource, Praxis, PRIME Education, Roche, Brown, McCarthy & Gruber, Sanofi, Seminal Healthcare, Spark, Springer Healthcare, Sunovion Pharma, Theravance, Voyager and WebMD; research support from Biogen, Biosensics, Burroughs Wellcome Fund, CuraSen, Greater Rochester Health Foundation, Huntington Study Group, Michael J. Fox Foundation, National Institutes of Health, Patient-CenteredOutcomes Research Institute, Pfizer, PhotoPharmics, Safra Foundation, and Wave Life Sciences; editorial services for Karger Publications; stock in Included Health, stock in Mediflix and ownership interests in SemCap.
Prof. B.R. Bloem currently serves as co-Editor in Chief for the Journal of Parkinson’s Disease. He serves on the editorial board of Practical Neurology and Digital Biomarkers, has received honoraria from serving on the scientific advisory board for Abbvie, Biogen and UCB, has received fees for speaking at conferences from AbbVie, Zambon, Roche, GE Healthcare and Bial, and has received research support from the Netherlands Organization for Scientific Research, the Michael J Fox Foundation, UCB, Not Impossible, the Hersenstichting Nederland, the Parkinson’s Foundation, Verily Life Sciences, Horizon 2020 and the Parkinson Vereniging (all paid to the institute). Prof. BR Bloem is an Editorial Board member of this journal, but was not involved in the peer-review process of this article nor had access to any information regarding its peer review.
For the remaining authors, there are any affiliations with or financial involvement (e.g., employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, royalties) with any organization or entity with a financial interest in or in financial competition with the subject matter or materials discussed in the manuscript.
REFERENCES
[1] | Dorsey ER , Sherer T , Okun MS , Bloem BR ((2018) ) The emerging evidence of the Parkinson pandemic. 2018. J Parkinsons Dis 8: , S3–S8. |
[2] | GBD 2016 Parkinson’s Disease Collaborators ((2018) ) Global, regional, and national burden of Parkinson’s disease, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol 17: , 939–953. |
[3] | Rizig M , Bandres-Ciga S , Makarious MB , Ojo OO , Crea PW , Abiodun OV , Levine KS , Abubakar SA , Achoru CO , Vitale D , Adeniji OA , Agabi OP , Koretsky MJ , Agulanna U , Hall DA , Akinyemi RO , Xie T , Ali MW , Shamim EA , Ani-Osheku I , Padmanaban M , Arigbodi OM , Standaert DG , Bello AH , Dean MN , Erameh CO , Elsayed I , Farombi TH , Okunoye O , Fawale MB , Billingsley KJ , Imarhiagbe FA , Jerez PA , Iwuozo EU , Baker B , Komolafe MA , Malik L , Nwani PO , Daida K , Nwazor EO , Miano-Burkhardt A , Nyandaiti YW , Fang ZH , Obiabo YO , Kluss JH , Odeniyi OA , Hernandez DG , Odiase FE , Tayebi N , Ojini FI , Sidranksy E , Onwuegbuzie GA , D’Souza AM , Osaigbovo GO , Berhe B , Osemwegie N , Reed X , Oshinaike OO , Leonard HL , Otubogun FM , Alvarado CX , Oyakhire SI , Ozomma SI , Samuel SC , Taiwo FT , Wahab KW , Zubair YA , Iwaki H , Kim JJ , Morris HR , Hardy J , Nalls MA , Heilbron K , Norcliffe-Kaufmann L ; Nigeria Parkinson Disease Research Network; International Parkinson’s Disease Genomics Consortium Africa; Black and African American Connections to Parkinson’s Disease Study Group; 23andMe Research Team; Blauwendraat C, Houlden H , Singleton A , Okubadejo NU ((2023) ) Identification of genetic risk loci and causal insights associated with Parkinson’s disease in African and African admixed populations: a genome-wide association study. Lancet Neurol 22: , 1015–1025. |
[4] | Dorsey ER , Zafara M , Lettenberger SE , Pawlik ME , Kinel D , Frissen M , Schneider RB , Kieburtz K , Tanner CM , De Miranda BR , Goldman SM , Bloem BR ((2023) ) Trichloroethylene: An invisible cause of Parkinson’s disease? J Parkinsons Dis 13: , 203–218. |
[5] | Paul KC , Krolewski RC , Moreno EL , Blank J , Holton KM , Ahfeldt T , Furlong M , Yu Y , Cockburn M , Thompson LK , Kreymerman A , Ricci-Blair EM , Li YJ , Patel HB , Lee RT , Bronstein J , Rubin LL , Khurana V , Ritz B ((2023) ) A pesticide and iPSC dopaminergic neuron screen identifies and classifies Parkinson-relevant pesticides. Nat Commun 14: , 2803. |
[6] | Dotchin C , Msuya O , Kissima J , Massawe J , Mhina A , Moshy A , Aris E , Jusabani A , Whiting D , Masuki G , Walker R ((2008) ) The prevalence of Parkinson’s disease in rural Tanzania. Mov Disord 23: , 1567–1672. |
[7] | Howlett WP , Urasa SJ , Maro VP , Walker RW , Kilonzo KG , Howlett PJ , Dekker MCJ ((2022) ) Neurological disorders in Northern Tanzania: A 6-year prospective hospital-based case series. Afri Health Sci 22: , 269–284. |
[8] | van Rensburg ZJ , Abrahams S , Chetty D , Step K , Acker D , Lombard CJ , Elbaz A , Carr J , Bardien S ((2022) ) The South African Parkinson’s Disease Study Collection. Mov Disord 37: , 230–232. |
[9] | Ben-Shlomo Y , Darweesh S , Llibre-Guerra J , Marras C , San Luciano M , Tanner C ((2024) ) The epidemiology of Parkinson’s disease. Lancet 403: , 283–292. |
[10] | https://www.gapminder.org/, Accessed September 13, 2022. |
[11] | Mshana G , Dotchin CL , Walker RW ((2011) ) We call it the shaking illness: Perceptions and experiences of Parkinson’s disease in rural northern Tanzania. BMC Publ Health 11: , 219. |
[12] | https://www.fao.org/faostat/en/#data/RP, Accessed May 1, 2023. |
[13] | Fuhrimann S , Wan C , Blouzard E , Veludo A , Holtman Z , Chetty-Mhlanga S , Dalvie MA , Atuhaire A , Kromhout H , Röösli M , Rother H-A ((2022) ) Pesticide research on environmental and human exposure and risks in Sub-Saharan Africa: A systematic literature review. Int J Environ Res Public Health 19: , 259. |
[14] | Ingenbleek L , Huc R , Lopes Pereirac L , Paineau A , Colet I , Zié Konéd A , Adegboyee A , Epiphane Hossouf S , Dembélég Y , Dada Oyedelee A , Sika K.J. Kisitoh C , Eyangoha S , Vergeri P , Leblanc J-C , Le Bizecb B ((2019) ) Sub-Saharan Africa total diet study in Benin, Cameroon, Mali and Nigeria: Pesticides occurrence in foods. Food Chem X 2: , 100034. |
[15] | Mekonen S , Ambelu A , Wondafrash M , Kolsteren P , Spanoghe P ((2021) ) Exposure of infants to organochlorine pesticides from breast milk consumption in southwestern Ethiopia. Sci Rep 11: , 22053. |
[16] | Blurton Jones N , Hawkes K , O’Connell JF ((2002) ) Antiquity of postreproductive life: Are there modern impacts on hunter-gatherer postreproductive life spans? Am J Hum Biol 14: , 184–205. |
[17] | https://maasai-association.org/maasai.html, Accessed May 1, 2023. |
[18] | Cordain L , Lindeberg S , Hurtado M , Hill M , Eaton SB , Brand-Miller J ((2002) ) Acne vulgaris. A disease of western civilization. Arch Dermatol 138: , 1584–1590. |
[19] | Snyder J , Smart JC , Goeb J , Tschirley D ((2018) ) Pesticide use in Sub-Saharan Africa: Estimates, projections, and implications in the context of food system transformation. In Agricultural & Applied Economics Association Annual Meeting, Washington, D.C., USA. August 5-7, 2018. http://ageconsearch.umn.edu16. Accessed May 1, 2023. |
[20] | Lekei EE , Ngowi AV , London L ((2016) ) Under reporting of acute pesticide poisoning in Tanzania: Modelling results from two cross-sectional studies. Environ Health 15: , 118. |
[21] | Final technical report on ‘Project on Support for Reducing Risks of Highly Hazardous Pesticides in the United Republic of Tanzania (URT)’. Capacity building related to multilateral environmental agreements in ACP countries- Phase 2. “ACP/MEAS2”-GCP/INT/153/EC”. Tropical Pesticides Research Institute (TPRI). www.tpri.or.tz, Accessed May 1, 2023. |
[22] | Lekei EE , Ngowi AV , London L ((2014) ) Pesticide retailers knowledge and handling practices in selected towns of Tanzania. Environ Health 13: , 79. |
[23] | Röösli M , Fuhrimann S , Atuhaire A , Rother HA , Dabrowski J , Eskenazi B , Jørs E , Jepson PC , London L , Naidoo S , Rohlman DS , Saunyama I , van Wendel de Joode B , Adeleye AO , Alagbo OO , Aliaj D , Azanaw J , Beerappa R , Brugger C , Chaiklieng S , Chetty-Mhlanga S , Chitra GA , Dhananjayan V , Ejomah A , Enyoh CE , Galani YJH , Hogarh JN , Ihedioha JN , Ingabire JP , Isgren E , Loko YLE , Maree L , Ernest NM , Moda HM , Mubiru E , Mwema MF , Ndagire I , Olutona GO , Otieno P , Paguirigan JM , Quansah R , Ssemugabo C , Solomon S , Sosan MB , Sulaiman MB , Teklu BM , Tongo I , Uyi O , Cueva-Vásquez H , Veludo A , Viglietti P , Dalvie MA ((2022) ) Interventions to reduce pesticide exposure from the agricultural sector in Africa: A workshop report. Int J Environ Res Public Health 19: , 8973. |
[24] | https://www.who.int/news-room/fact-sheets/detail/malaria, Accessed September 13, 2022. |
[25] | https://pan-international.org, Accessed October 1, 2023. |
[26] | The WHO Recommended Classification of Pesticides by Hazard and guidelines to classification, 2019 edition. WHO Team Chemical Safety and Health Unit. Editors. WHO. ISBN: 9789240005662. https://www.who.int/publications/i/item/9789240005662, Accessed October 1, 2023. |
[27] | Registered pesticides for use in the United Republic of Tanzania. Tanzania Plant Health and Pesticides Agency/Tropical Pesticides Research Institute. www.kilimo.go.tz, Accessed May 1, 2023. |
[28] | Dorsey ER , Sherer T , Okun MS , Bloem BR ((2020) ) The rise of Parkinson’s disease. Sci Am, www.amsci.org/magazine/issues/2020/may-june, Accessed May 1, 2023. |
[29] | Firestone JA , Smith-Weller T , Franklin G , Swanson P , Longstreth WT , Checkoway H ((2005) ) Pesticides and risk of Parkinson disease. A population-based case-control study. Arch Neurol 62: , 91–95. |
[30] | Liu C , Liu Z , Fang Y , Du Z , Yan Z , Yuan X , Dai L , Yu T , Xiong M , Tian Y , Li H , Li F , Zhang J , Meng L , Wang Z , Jiang H , Zhang Z ((2022) ) Exposure to the environmentally toxic pesticide maneb induces Parkinson’s disease-like neurotoxicity in mice: A combined proteomic and metabolomic analysis. Chemosphere 308: (Pt2), 136344. |
[31] | Sandy MS , Di Monte D , Cohen P , Smith MT ((1988) ) Role of active oxygen in paraquat and 1-methyl-4-phenyl-1,2,3,6- tetrahydropyridine (MPTP) cytotoxicity. Basic Life Sci 49: , 795–801. |
[32] | Heikkila RE , Nicklas WJ , Vyas I , Duvoisin RC ((1985) ) Dopaminergic toxicity of rotenone and the 1-methyl-4-phenylpyridinium ion after their stereotaxic administration to rats: implication for the mechanism of 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine toxicity. Neurosci Lett 62: , 389–394. |
[33] | Gouda HN , Charlson F , Sorsdahl K , Ahmadzada S , Ferrari AJ , Erskine H , Leung J , Santamauro D , Lund C , Aminde LN , Mayosi BM , Kengne AP , Harris M , Achoki T , Wiysonge CS , Stein DJ , Whiteford H ((2019) ) Burden of non-communicable diseases in sub-Saharan Africa, 1990-2017: results from the Global Burden of Disease Study 2017. Lancet Glob Health 7: , e1375–e1387. |


