
The Impact of Motor, Non-Motor, and Social Aspects on the Sexual Health of Men Living with Parkinson’s Disease
Abstract
Background:
Sexual health (SH) is influenced by several biological, mental, and social factors that may be negatively impacted by Parkinson’s disease (PD). Despite its prevalence and relevance for quality of life, the factors that affect SH in men with PD (MwPD) are still poorly understood.
Objectives:
To investigate the impact of motor, non-motor, and social aspects on the SH in MwPD.
Methods:
We conducted a cross-sectional study of 80 men (mean-age 53.55±10.8) in stages 1–3 of Hoehn and Yahr classification (H&Y), who reported having an active sex life in the last six months. The following data were collected for each person: 1) Demographic and clinical features; 2) global cognitive capacity (T-MoCA); 3) Non-Motor Aspects of Experiences of Daily Living (MDS-UPDRS, part I); 4) Motor Aspects of Experiences of Daily Living (MDS-UPDRS, part II); 5) Fatigue (FSS); 6) Self-esteem (RSES); 7) Sleep disorder (PDSS); 8) Couple relationship quality (DAS); 9) Depressive signals (BDI); 10) Short-term sexual health by International Index of Erectile Function (IIFE); and 11) Long-term sexual health by Sexual Quotient-Male (SQ-M).
Results:
Our results showed that although several motor, non-motor, and social factors were correlated with SH, only motor disability levels in daily living predicted short-term SH and erectile dysfunction, while only depression predicted long-term SH in MwPD. Age, disease onset, and medication daily dosage were not correlated with SH.
Conclusions:
Our findings confirm that multidimensional factors can affect the SH of MwPD and emphasize that only a multi-professional team can offer proper care to improve SH in MwPD.
INTRODUCTION
Parkinson’s disease (PD) is an idiopathic, neurodegenerative, multisystemic, progressive, and irreversible disorder with a large spectrum of motor and non-motor signs and symptoms [1]. Its incidence increases with age and rises sharply after 65 years [2]. According to the Global Burden of Disease study, PD was the only neurological disorder with increasing age-standardized rates of deaths, prevalence, and disability-adjusted life-years between 1990 and 2015 [3].
According to the World Health Organization, sexual health (SH) is “a state of physical, emotional, mental and social well-being in relation to sexuality” [4]. SH involves many factors, including organic causes, environmental influences, and psychological factors. It is a complex phenomenon, making its study and understanding challenging [5].
Among the non-motor functions affected by PD, sexual dysfunction (SD) has a negative impact on SH [6, 7], and can significantly reduce the quality of life for patients and their sex partners [8]. Unfortunately, SD is often underreported and receives little attention from health professionals [9, 10]. Studies have shown that SD is more prevalent in people with PD (PwPD) than in healthy individuals [11–13], and may be an early symptom of PD [14]. The prevalence ranges between 42% and 79% in men with PD (MwPD) and between 36 and 87% in women with PD (WwPD) [6, 15–17]. More than 50% of PwPD reported that their sex activity was affected by the disease [18] and decreased progressively over a two-year follow-up period [19].
Regarding age, studies show different results: some show that SD is worse in older PwPD [13, 20–23] while others show that younger people report more SD [24] or that SD is age-independent [22].
Regarding disease progression and disease severity, some studies showed that SD increases with disease progression [18, 25, 26] and disease severity [15, 26–28], while others showed no correlation between disease progression [20, 24, 29, 30] or disease severity [16, 18, 21, 29, 31]. In MwPD, disease severity was associated with libido loss [15].
Frequency of intercourse, sexual arousal, subjective abnormal sexual fantasies, or sexual satisfaction deteriorated in both genders, but especially in MwPD [23]. The main SD observed in MwPD were 1) hypoactive sexual desire disorder, reported by 83% of participants [17]; 2) erectile dysfunction (ED), reported between 42.6% and 79% of MwPD [6, 15, 17, 32, 33]; 3) difficulty reaching orgasm, reported by 39.5% [6], premature ejaculation, reported between 40.6% and 79% of MwPD [6, 10, 34]; 5) anejaculation, reported by 87% [17], and 6) hypersexuality, reported by 5.2% of MwPD [35].
Several alterations in sensory, motor, mental, and autonomic functions associated with PD and social aspects can directly or indirectly affect the SH [19, 36].
Regarding motor alterations associated with PD, rigidity, tremor, postural instability, immobility in bed, incoordination in fine movements of the hands, and facial hypomimia can make it difficult for patients to experience pleasure and sexual arousal, as well as be a barrier to full participation in sexual activity [6, 34]. In fact, PwPD who reported SD showed higher motor symptom severity than those without SD [18]. In MwPD, motor symptom severity was associated with ED [20] and decreased quality of SH of the sex partner [7]. Increased motor disability level in MwPD is associated with decreased SH [9, 19, 34] and sexual satisfaction [37].
Among the non-motor alterations, depression and anxiety have been identified as the factors most correlated with SD [13, 18, 20, 34, 37]. Depression is a predictor for libido loss and decreased sexual desire in PwPD [15]. For MwPD, lower depression is associated with higher sexual activity [19]. Few studies that have investigated the impact of cognitive changes on the SH of PwPD showed no correlation between cognitive status and SD [19, 24]. Particularly in MwPD, it was found an association between cognitive decline and libido loss [15]. Urinary, autonomic dysfunction, and fatigue have also been associated with SD complaints, such as loss of libido and decreased sexual satisfaction in PwPD [13, 15].
Among the social factors, the quality of the marital relationship has been bidirectionally related to SH [38]. Brown et al. (1990) showed that couples where one of the partners had PD who reported a better marital relationship were more satisfied with their sex life and vice versa [9]. However, satisfaction with the marital relationship varied between genders: dissatisfaction with the marital relationship and the sex life of both partners was more significant when the PwPD was a man. MwPD rejected sex less often and reported higher desire and more dissatisfaction with their sex life than women [6, 7].
SH is a multifaceted issue that can be attributed to not only organic causes, but also environmental and psychological factors. SD is a prevalent and disturbing non-motor symptom of PD, mainly for men. Although several studies have investigated SD in PD, there is a lack of complete and consistent data on SH in MwPD. This study aimed to investigate the impact of motor, non-motor, and social factors on SH of MwPD who reported having an active sex life.
MATERIALS AND METHODS
Study design and participants
A cross-sectional study included 80 MwPD. The eligibility criteria were (a) man; (b) confirmed diagnosis of idiopathic PD offered by a neurologist according to the UK Parkinson’s Disease Society Brain Bank diagnostic criteria [39], age above 21 years; (c) reported sexual activity, not necessarily with penetration, within the last six months, and (d) have access to telephone or internet and agree to participate in the study. The non-eligibility criteria were (a) the presence of neurological disorders other than PD and (b) the presence of dementia, speech, and hearing disorders that could impair the remote interview.
Recruitment
Participants were recruited by a non-probability sampling method from the contacts of the AMPARO network (http://www.amparo.numec.prp.usp.br) in Brazil. At first, we checked the eligibility criteria through calls. Subsequently, information about the study procedures was passed on, and those selected were asked to consent to participate. This study was approved by the Ethics Committee of the Federal University of Amapa in Brazil (#CAAE39971420.0.0000.0003) and conducted in accordance with the Helsinki Declaration.
Study procedures
The study flow is shown in Fig. 1.
Fig. 1
The schematic study designs.
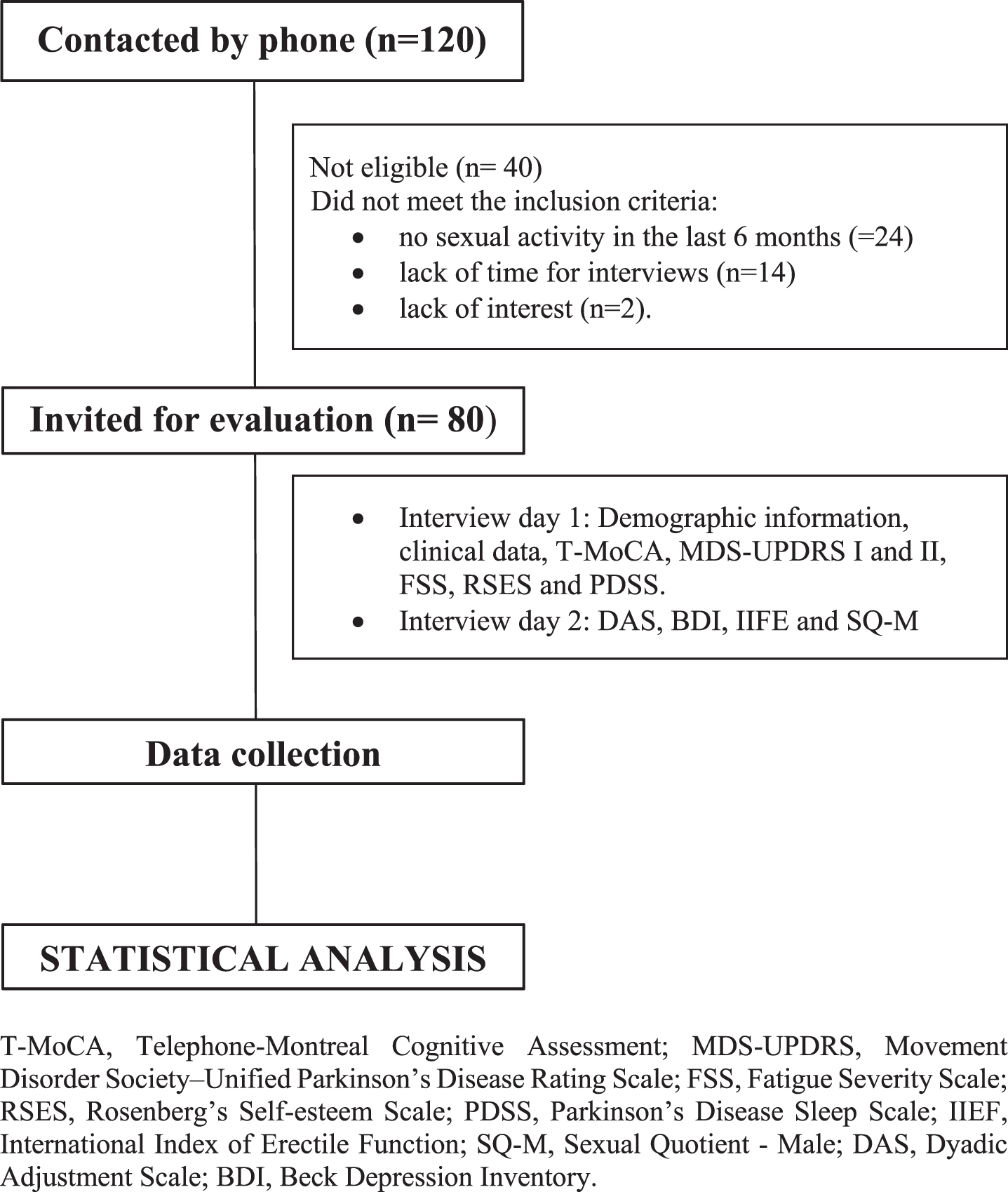
After agreeing to take part in the study, participants were requested to specify their preferred day and time for the remote interview, considering the on-period of dopaminergic medication (40–120 min post the last intake). Then, the researchers applied the questionnaire, which included general information, information associated with PD, and the structured instruments selected for the study.
The interviews for this study were conducted by the same interviewer in two separate sessions, with a gap of less than 7 days between them. Each interview lasted around 30–35 min.
Instruments
Socioeconomic condition (SEC)
The socio-economic condition (SEC) was evaluated by the Brazilian Economic Classification Criterion, which is a socioeconomic classification standard, carried out based on households, family education and income [40]. Higher scores indicate better SEC conditions.
Telephone-Montreal Cognitive Assessment (T-MoCA)
The T-MoCA is an adapted version of the MoCA 30 test administered by phone. It contains only the items that do not require the use of pencil and paper or visual stimuli, so its maximum score is 22 [41].
Movement Disorder Society-Unified Parkinson’s Disease Rating Scale (MDS-UPDRS)
The MDS-UPDRS is a tool to measure PD severity and progression based on the difficulties presented in the last seven days. In this study, only Part I (Non-motor aspects of experiences of daily living) and Part II (Motor aspects of experiences of daily living) were used [42]. Additionally, the scores obtained in item 1.6 of the MDS-UPDRS were used to assess the prevalence of dopamine dysregulation syndrome (DDS).
Fatigue Severity Scale (FSS)
The FSS is a non-specific rating scale often used in PD. This instrument contains 9 questions with answers ranging from 1 (strongly disagree) to 7 (strongly agree). The total score is the mean of the 9 questions, and higher scores indicate higher fatigue degrees [43].
Rosenberg’s Self-esteem Scale (RSES)
The RSES comprises 10 questions to assess self-esteem. Questions are answered on a Likert-type scale of how many points range from strongly agree, agree, disagree, and strongly disagree [44].
Parkinson’s Disease Sleep Scale (PDSS)
The PDSS is a specific scale for assessing sleep disorders in PD [45]. It comprises 15 questions associated with sleep disorders based on the last week. The score ranges from always (0) to never (10), except for question 1, whose scale ranges from poor (0) to excellent (10). The maximum score is 150 [46].
Dyadic Adjustment Scale (DAS)
The DAS is a self-report tool to assess the couple’s relationship quality (CRQ) based on marital adjustment. It consists of 4 subscales of dyadic satisfaction, cohesion, consensus, and affectional expression, with scores ranging from 0 to 5. The total score (sum of all questions) ranges from 0 to 151. Higher scores indicate a better relationship. A total score below 101 indicates dissatisfaction [47].
Beck Depression Inventory (BDI)
The BDI is widely used to screen for depression and to measure behavioral manifestations and severity of depression. The BDI comprises 21 questions about quality and depressive symptoms, ranging from 0–63 points (0–13 no depression, 14–19 mild depression, 20–28 moderate, 29–63 severe depression). The total score is the sum of all values. The BDI has been described as a valid instrument to assess depressive symptoms in PD [48].
International Index of Erectile Function (IIEF) –Short-term SH
The 15-question International Index of Erectile Function (IIEF) Questionnaire is a validated, multidimensional, self-administered investigation. Although it has been recommended as a primary endpoint for clinical trials of erectile dysfunction (ED) and diagnostic evaluation of ED severity [49]. The questionnaire consists of 15 questions, grouped into five domains: erectile function, orgasm, sexual desire, sexual satisfaction, and general satisfaction. Each question has a value ranging from 1 to 5, and the sum of the answers generates a final score for each domain, with low values indicating poor quality of sexual life based on the last four weeks [50]. In this study the IIFE total score was calculated by the sum of the five domains.
The ranges of scores allow classifying ED into five categories, based on the domain of erectile function, with scores ranging from 6 to 30: without ED (26–30); mild ED (22–25); mild to moderate ED (17–21); moderate ED (11–16); severe ED (6–10).
Sexual Quotient –Male (SQ-M) –Long-term SH
It was constructed and validated for the Brazilian population according to the sexual specificities of men. This quotient has 10 questions with five possible Likert-type answers: 0 (never), 1 (rarely), 2 (sometimes), 3 (approximately 50% of the time), 4 (most of the time), and 5 (always). The final score reflects the sexual performance pattern based on the last six months, which can be classified as having sexual dysfunction (<60 points) and without sexual dysfunction (≥60 points). This score is obtained by adding the numbers corresponding to each question and multiplying by 2 [51].
Statistical analyses
Descriptive statistical analysis was used for demographic and clinical data. The Spearman Rank Order Correlation was used to test correlations among age, socio-economic classification (SEC), Daily Dosage of Levodopa (DDL), Daily Dosage of Agonist of Levodopa (DDAL), DDS, disease duration, H&Y stages, T-MoCA, MDS-UPDRS I, MDS-UPDRS II, FSS, RSES, PDSS, DAS, BDI with IIEF total scores, erectile function (EF)–domain of the IIFE and SQ-M, and between EF and SQ-M.
A multiple regression model as predictor variables also included all factors that reached a significant statistical correlation with total scores of IIEF, EF domain and SQ-M (response variable).
Additionally, the scores in IIEF and SQ-M were compared by Kolmogorov-Smirnov test between participants with early onset PD (EOPD), i.e., diagnosed when aged less than 50 years and late-onset PD (LOPD), i.e., diagnosed when aged more than 50 years [52].
Differences were considered statistically significant for p < 0.05. The statistical analyses were performed using Statistica Version 13 (TIBCO Software Inc., USA).
RESULTS
The participants’ demographic and clinical characteristics are shown in Table 1.
Table 1
Demographic and clinical features of the participants
| Variable | Mean | SD |
| Age (y) | 53.55 | 10.82 |
| SEC | 33.26 | 10.89 |
| DDL (mg/day) | 566.87 | 429.52 |
| DDAL (mg/day) | 1.54 | 1.18 |
| DDS | 1.72 | 0.47 |
| Disease duration (y) | 6.62 | 6.67 |
| H&Y | 1.86 | 0.68 |
| TMOCA | 19.08 | 1.82 |
| MDS-UPDRS I | 12.81 | 8.40 |
| MDS-UPDRS II | 13.81 | 9.30 |
| FSS | 36.97 | 16.45 |
| RSES | 16.45 | 16.45 |
| PDSS | 98.31 | 25.28 |
| DAS | 110.30 | 9.44 |
| BDI | 11.93 | 8.90 |
SEC, socio-economic condition; DDL, daily dosage levodopa; DDAL, daily dosage agonist levodopa; DDS, Dopaminergic Dysregulation Syndrome; H&Y, Hoehn and Yahr Stage; T-MoCA, Telephone-Montreal Cognitive Assessment; MDS-UPDRS, Movement Disorder Society–Unified Parkinson’s Disease Rating Scale; FSS, Fatigue Severity Scale; RSES, Rosenberg’s Self-esteem Scale; PDSS, Parkinson’s Disease Sleep Scale; DAS, Dyadic Adjustment Scale; BDI, Beck Depression Inventory; SD, standard deviation.
Out of all the participants, it was found that 31% were in Stage 1, 51% were in Stage 2, and 18% were in Stage 3, according to the H&Y classification [53]. Additionally, 68% of participants were less than 60 years old, and 64% presented EOPD. There was no statistically significant difference for IIEF and SQ-M scores between participants with EOPD and LOPD.
It is important to note that although 10 of the participants reported mild to moderate DDS according to item 1.6 of the MDS-UPDRS I (6 involving compulsion for shopping, 3 for games and 1 for candies), none of them reported hypersexuality.
Short-term sexual health (STSH)
The total score in IIEF, which investigated SH in the last four weeks, was 55.98±17.8. The results for each IIFE domain can be observed in Table 2.
Table 2
IIEF domain scores
| Domain | Maximal | Mean | Standard |
| score | deviation | ||
| Erectile function | 30 | 23.10 | 8.48 |
| Intercourse sexual | 15 | 9.90 | 4.11 |
| Orgasmic function | 10 | 8.28 | 2.98 |
| Sexual desire | 10 | 7.35 | 1.92 |
| Overall satisfaction | 10 | 7.34 | 2.26 |
IIEF, Index International of Erectile Function.
The total scores obtained by the IIEF had a moderate positive statistically significant correlation (R > 0.30) with the T-MoCA and PDSS scores and a moderate negative statistically significant correlation with H&Y stages, disease duration, MDS-UPDRS I and II, RSES, FSS and BDI (Table 3). The regression model showed that MDS-UPDRS II could predict IIEF with Adjusted R2 = 0.355, F (1.78) = 44.67 and Beta = –0.60, p = 0.00001.
Table 3
Correlation between IIEF, EF, QS-M and demographic and clinical variables
| Variable | IIFE | EF | QS-M | |||
| R | p | R | p | R | p | |
| Age (y) | –0.120 | >0.05 | –0.202 | >0.05 | –0.117 | >0.05 |
| SEC | 0.215 | >0.05 | 0.143 | >0.05 | 0.198 | >0.05 |
| Disease duration (y) | –0.326 | 0.003 | –0.262 | 0.018 | –0.154 | >0.05 |
| H&Y | –0.432 | 0.001 | –0.340 | 0.001 | –0.295 | 0.007 |
| DDL (mg/day) | –0.221 | >0.05 | –0.118 | >0.05 | –0.097 | >0.05 |
| DDAL (mg/day) | –0.157 | >0.05 | –0.206 | >0.05 | –0.062 | >0.05 |
| DDS | 0.081 | >0.05 | 0.068 | >0.05 | 0.021 | >0.05 |
| TMOCA | 0.413 | 0.001 | 0.359 | 0.001 | 0.252 | 0.024 |
| MDS-UPDRS I | –0.413 | 0.001 | –0.372 | 0.000 | –0.328 | 0.002 |
| MDS-UPDRS II | –0.055 | 0.001 | –0.478 | 0.000 | –0.411 | 0.000 |
| FSS | –0.438 | 0.001 | –0.320 | 0.003 | –0.343 | 0.001 |
| PDSS | 0.444 | 0.001 | 0.379 | 0.001 | 0.333 | 0.002 |
| DAS | 0.101 | >0.05 | 0.115 | >0.05 | 0.283 | 0.023 |
| BDI | –0.385 | 0.001 | –0.233 | 0.037 | –0.290 | 0.008 |
| RSES | –0.38 | 0.001 | –0.268 | 0.016 | –0.297 | 0.007 |
IIEF, International Index of Erectile Function; EF, erectile function; QS-M, Sexual Quotient-Male; SEC, socio-economic condition; H&Y, Hoehn and Yahr Stage; DDL, daily dosage levodopa; DDAL, daily dosage agonist levodopa; DDS, Dopaminergic Dysregulation Syndrome; T-MoCA, Telephone-Montreal Cognitive Assessment; MDS-UPDRS, Movement Disorder Society–Unified Parkinson’s Disease Rating Scale; FSS, Fatigue Severity Scale; PDSS, Parkinson’s Disease Sleep Scale; DAS, Dyadic Adjustment Scale; BDI, Beck Depression Inventory; RSES, Rosemberg’s Self-esteem Scale.
The mean score in the erectile function (EF) domain was 23.10±8.48 (Table 2), below the minimal score adopted to identify erectile dysfunction (cut-off score <26).
The scores obtained by the EF domain had a moderate positive statistically significant correlation with T-MoCA and PDSS scores, a moderate negative statistically significant correlation with H&Y stages, MDS-UPDRS I and II, FSS, and a weak negative statistically significant correlation with disease duration, RSES and BDI scores (Table 3).
The variables disease duration, T-MoCA, PDSS, H&Y stages, MDS-UPDRS I and II, FSS, RSES, and BDI, were included in the multiple regression model, with only the MDS-UPDRS II remaining as a predictor variable for the EF, which presented Adjusted R2 = 0.31; F (1,78) = 12.08; Beta = –0.57, p = 0.000001.
Long-term sexual health (LTSH)
The mean score in SQ-M, which investigated SH in the last six months, was 78.02±19.2, above the score adopted to identify sexual dysfunction (cut-off score <60).
The total score obtained by SQ-M had a moderate positive statistically significant correlation with T-MoCA, PDSS and DAS scores, a moderate negative statistically significant correlation with MDS-UPDRS I and II, FSS, and a weak negative statistically significant correlation (R < .30) with H&Y stages, RSES and BDI scores (Table 3).
Furthermore, the multiple regression model included the variables T-MoCA, DAS, PDSS, MDS-UPDRS I and II, FSS, H&Y stages, RSES, BDI scores included in the multiple regression model, with only the BDI remaining in the final model as independent predictors for SQ-M with Adjusted R2 = 0.14; F (1,62) = 12.08; Beta = –0.40; p = 0.00009.
Finally, a strong positive correlation was found between IIFE and SQ-M (R = 0.78; p < 0.000001).
DISCUSSION
SH is essential for maintaining overall well-being and health. Decreased SH has consequences that extend beyond the individual and can affect families and society [54]. However, there has been a lack of research on SH in people with PD. To the best of our knowledge, the present study was the first aiming to investigate the impact of the motor, non-motor, and social aspects on the short and long-term SH in MwPD by different but complementary instruments developed to assess SH.
Our results showed that despite several motor, non-motor, and social factors had a significant role in determining SH, only motor disability level in daily living was a predictor for short-term SH and EF, while depression severity was the unique predictor for long-term SH. Interestingly, we did not find any significant association between SH and factors such as age, disease onset, DDL, DDAL and DDS. These findings suggest that addressing motor disability and mental health may be crucial in improving the overall health of MwPD.
Taken together, several considerations can be made based on the results.
In the present study, we utilized two different instruments to evaluate SH in MwPD. The first tool, IIEF, assessed overall SH and specifically evaluated EF over the past four weeks. The second tool, SQ-M, based on a qualitative approach, evaluated SH over the past six months. We found that both IIEF and SQ-M were strongly correlated with each other and with the same variables, such as disease progression, disease duration, global cognitive capacity, depression, self-esteem, motor and non-motor disability in daily living, fatigue, and sleep. However, only SQ-M was correlated with the CRQ. Most importantly, different factors predicted IIEF and SQ-M scores. While previous studies have primarily used IIEF to evaluate SH in MwPD, our findings suggest that incorporating the SQ-M questionnaire can offer additional insights into how PD affects SH.
Based on our results, many MwPDs experience ED. Specifically, our findings show that 47% of MwPD reported ED based on IIEF, with 17% experiencing moderate to severe ED. Although age did not predict SH in the present study, it is important to note that 28% of participants under the age of 60 reported ED. Of these, 13% reported moderate to severe dysfunction. These findings are in line with previous studies that have identified ED as the most prevalent SD among MwPD, with prevalence rates ranging from 42.6% to 79% [6, 15, 17, 32, 33].
Our results have demonstrated the importance of recognizing ED as a non-motor symptom in MwPD. We found that while several factors were associated with EF, it was only the motor disability in daily living that was able to predict the presence of ED and short-term SH. Previous research has also shown that individuals with PD who have more severe motor symptoms and disability tend to experience more SD [9, 18, 19, 34, 37] and ED [20], which is consistent with our findings. Although the MDS-UPDRS Part II assesses various factors that may affect sexual performance, such as bed mobility, dressing ability, and hand coordination, it is not entirely clear how motor disability specifically impacts EF. Our findings emphasize the need for clinicians to consider the impact of motor disability on sexual health in individuals with PD and highlight the demand for more studies to understand the relationship between motor disability and EF.
Our findings showed that the severity of depression plays a critical role in predicting long-term SH. This is consistent with previous research emphasizing the close link between depression and sexual dysfunction. In fact, studies conducted by Kotková and Weiss (2013) [37], Vela-Desojo et al. (2020) [13], Raciti et al. (2020) [18], Özcan et al. (2015) [20], and Jitkritsadakul et al. (2015) [34] have also reported similar results. Additionally, our study identified depression severity as a significant predictor of SD in MwPD, which is consistent with the findings of Ferrucci et al. (2016) [33], Kotková and Weiss (2013) [37], and Kummer et al. (2009) [15] that showed depression as a predictor for SD in men and women with PD. Specifically, for MwPD, higher levels of depression symptoms were associated with decreased sexual activity, as reported by Picillo et al. (2019) [19]. Since depression is a common non-motor symptom that may even be present before a diagnosis is possible, interventions to prevent or reduce depression are crucial to avoid or minimize the decreased SH in MwPD.
Interestingly, it was found that the total score of SQ-M was significantly correlated only to the quality of marital relationships. This suggests that general aspects of long-term SH are influenced by the complex aspects of marital relationship assessment by DAS. Previous studies have shown that the quality of the marital relationship is closely related to SH in both directions [9, 38, 55]. Our findings reinforce the importance of providing care not only for the patient but also for their partner.
Some previous studies have found associations between other non-motor symptoms and SD [56]. However, the MDS-UPDRS I, PDSS, and FSS, which assess general non-motor symptoms, sleep quality, and fatigue, respectively, although correlated with IIEF and SQ-M scores, had no predictive value for both in the present study. The same was observed for self-esteem: despite some features like drooling, excessive sweating, seborrhea, and hypomimia may decrease self-esteem [11], the RSES scores, although correlated with IIEF and SQ-M scores, had no predictive value for both.
Finally, although dopaminergic medication has been correlated with SD in MwPD [11], the DDL, DDAL, and DDS were not associated with SH in the present study.
The present study presents some strengths: using multidimensional generic instruments to assess SH, quality of couple relationships, depression, and cognition. Moreover, the use of disease-specific instruments that comprehensively assess motor and non-motor dysfunction in PD. The results obtained are promising and can serve as a foundation for further research in the field.
Our study has some limitations to be considered. One of the main limitations is that it was designed as cross-sectional, meaning that the information gathered was only based on data from a specific point in time. However, we tried to minimize this limitation by using different tools to assess the STSH and LTSH. Another limitation is that the sample size may not allow for large generalization to the PD population. However, we included participants from 5 different geographical areas with sizable sociocultural differences, which may have helped to minimize this limitation. Lastly, and importantly, we did not find men of advanced age and stage of PD who reported having an active sex life to be included in this study. This can be considered a study limitation. Further studies are needed to investigate SH in MwPD who are no longer sexually active.
In conclusion, various motor, non-motor, and social factors were found to be associated with SH in MwPD, regardless of their age, disease onset, and medication dosage. However, motor disability in daily living was the only factor that could predict short-term SH and ED, while the severity of depression was found to predict long-term SH. Therefore, to prevent the decline in SH, an interdisciplinary approach that addresses these factors should be made available to people with PD from the early stages of the disease.
Clinical implications
Although SH has been considered a non-motor alteration associated with PD, it has received little attention from health professionals. In the present study, although 57% of participants rated SH as a “very important issue for MwPD,” only 19% reported having ever asked a health professional (including a neurologist) about their SH, and only 5% received some orientation to deal with the problem. Participants’ comments such as: “It looks like that for doctors, sex is only a leisure activity we are no longer entitled to”; and “When I asked the doctor about vasectomy, he asked me: do you still have sex?” alert us about the importance of offering a proper evaluation of SH, considering all factors that can negatively impact it. In addition to increasing research in the field, there is a need to expand educational initiatives to improve the multidisciplinary care of SH in PD.
ACKNOWLEDGMENTS
This article was produced as part of the activities of the FAPESP Research, Innovation, and Dissemination Center for Neuromathematics (grant #2013/07699-0, S. Paulo Research Foundation).
FUNDING
ACR is partially supported by a research fellowship from CNPq (grant # 303359/2022-6).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
[1] | Bloem BR , Okun MS , Klein C ((2021) ) Parkinson’s disease. Lancet 397: , 2284–2303. |
[2] | Van Den Eeden SK , Tanner CM , Bernstein AL , Fross RD , Leimpeter A , Bloch DA , Nelson LM ((2003) ) Incidence of Parkinson’s disease: Variation by age, gender, and race/ethnicity. Am J Epidemiol 157: , 1015–1022. |
[3] | GBD 2015 Neurological Disorders Collaborator Group ((2017) ) Global, regional, and national burden of neurological disorders during 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet Neurol 16: , 877–897. |
[4] | World Health Organization (2006) Defining sexual health: Report of a technical consultation on sexual health, 28–31 January 2002, Geneva. Geneva: World Health Organization, Department of Reproductive Health and Research. Retrieved from:https://www.who.int/reproductivehealth/publications/sexual_health/defining_sexual_health.pdf?ua=1. |
[5] | Meco G , Rubino A , Caravona N , Valente M ((2008) ) Sexual dysfunction in Parkinson’s disease. Parkinsonism Relat Disord 14: , 451–456. |
[6] | Bronner G , Royter V , Korczyn AD , Giladi N ((2004) ) Sexual dysfunction in Parkinson’s disease. J Sex Marital Ther 30: , 95–105. |
[7] | Bronner G , Cohen OS , Yahalom G , Kozlova E , Orlev Y , Molshatzki N , Strauss H , Hassin-Baer S ((2014) ) Correlates of quality of sexual life in male and female patients with Parkinson disease and their partners. Parkinsonism Relat Disord 20: , 1085–1088. |
[8] | Ng YF , Chen CY , Chia GT , Tan BBJ , Chan LL , Tan EK ((2022) ) The association between Parkinson’s disease and Sexual dysfunction: Clinical correlation and therapeutic implications. Ageing Res Rev 79: , 101665. |
[9] | Brown RG , Jahanshahi M , Quinn N , Marsden CD ((1990) ) Sexual function in patients with Parkinson’s disease and their partners. J Neurol Neurosurg Psychiatry 53: , 480–486. |
[10] | Bronner G , Vodušek DB ((2011) ) Management of sexual dysfunction in Parkinson’s disease. Ther Adv Neurol Disord 4: , 375–383. |
[11] | Bhattacharyya KB , Rosa-Grilo M ((2017) ) Sexual dysfunctions in Parkinson’s disease: An underrated problem in a much-discussed disorder. Int Rev Neurobiol 134: , 859–876. |
[12] | Zhao S , Wang J , Xie Q , Luo L , Zhu Z , Liu Y , Luo J , Zhao Z ((2019) ) Parkinson’s disease is associated with risk of sexual dysfunction in men but not in women: A systematic review and meta-analysis. J Sex Med 16: , 434–446. |
[13] | Vela-Desojo L , Urso D , Kurtis-Urra M , García-Ruiz PJ , Pérez-Fernández E , Lopez-Valdes E , Posada-Rodriguez I , Ybot-Gorrin I , Lopez-Manzanares L , Mata M , Borrue C , Ruiz-Huete C , Del Valle M , Martinez-Castrillo JC ((2020) ) Sexual dysfunction in early-onset Parkinson’s disease: A cross-sectional, multicenter study. J Parkinsons Dis 10: , 1621–1629. |
[14] | Gao X , Chen H , Schwarzschild MA , Glasser DB , Logroscino G , Rimm EB , Ascherio A ((2007) ) Erectile function and risk of Parkinson’s disease. Am J Epidemiol 166: , 1446–1450. |
[15] | Kummer A , Cardoso F , Teixeira AL ((2009) ) Loss of libido in Parkinson’s disease. J Sex Med 6: , 1024–1031. |
[16] | Brown E , Brown GM , Kofman O , Quarrington B ((1978) ) Sexual function and affect in parkinsonian men treated with L-dopa. Am J Psychiatry 135: , 1552–1555. |
[17] | Sakakibara R , Shinotoh H , Uchiyama T , Sakuma M , Kashiwado M , Yoshiyama M , Hattori T ((2001) ) . Questionnaire-based assessment of pelvic organ dysfunction in Parkinson’s disease. Auton Neurosci 92: , 76–85. |
[18] | Raciti L , De Cola MC , Ortelli P , Corallo F , Lo Buono V , Morini E , Quattrini F , Filoni S , Calabrò RS ((2020) ) Sexual dysfunction in Parkinson disease: A multicenter Italian cross-sectional study on a still overlooked problem. J Sex Med 17: , 1914–1925. |
[19] | Picillo M , Palladino R , Erro R , Colosimo C , Marconi R , Antonini A , Barone P , PRIAMO study group ((2019) ) The PRIAMO study: Active sexual life is associated with better motor and non-motor outcomes in men with early Parkinson’s disease. Eur J Neurol 26: , 1327–1333. |
[20] | Özcan T , Benli E , Demir EY , Özer F , Kaya Y , Haytan CE ((2015) ) The relation of sexual dysfunction to depression and anxiety in patients with Parkinson’s disease. Acta Neuropsychiatr 27: , 33–37. |
[21] | Moore O , Gurevich T , Korczyn AD , Anca M , Shabtai H , Giladi N ((2002) ) Quality of sexual life in Parkinson’s disease. Parkinsonism Relat Disord 8: , 243–246. |
[22] | Pedro T , Sousa M , Rito M , Pereira R , Januário C , Moreira F ((2020) ) The impact of deep brain stimulation on the sexual function of patients with Parkinson’s disease. Neurologist 25: , 55–61. |
[23] | Buhmann C , Dogac S , Vettorazzi E , Hidding U , Gerloff C , Jürgens TP ((2017) ) The impact of Parkinson disease on patients’ sexuality and relationship. J Neural Transm (Vienna) 124: , 983–996. |
[24] | Hand A , Gray WK , Chandler BJ , Walker RW ((2010) ) Sexual and relationship dysfunction in people with Parkinson’s disease. Parkinsonism Relat Disord 16: , 172–176. |
[25] | Guo X , Song W , Chen K , Chen X , Zheng Z , Cao B , Huang R , Zhao B , Wu Y , Shang HF ((2013) ) Gender and onset age-related features of non-motor symptoms of patients with Parkinson’s disease–a study from Southwest China. Parkinsonism Relat Disord 19: , 961–965. |
[26] | Spica V , Pekmezović T , Svetel M , Kostić VS ((2013) ) Prevalence of non-motor symptoms in young-onset versus late-onset Parkinson’s disease. J Neurol 260: , 131–137. |
[27] | Wermuth L , Stenager E ((1995) ) Sexual problems in young patients with Parkinson’s disease. Acta Neurol Scand 91: , 453–455. |
[28] | Celikel E , Ozel-Kizil ET , Akbostanci MC , Cevik A ((2008) ) Assessment of sexual dysfunction in patients with Parkinson’s disease: A case-control study. Eur J Neurol 15: , 1168–1172. |
[29] | Varanda S , Ribeiro da Silva J , Costa AS , Amorim de Carvalho C , Alves JN , Rodrigues M , Carneiro G ((2016) ) Sexual dysfunction in women with Parkinson’s disease. Mov Disord 31: , 1685–1693. |
[30] | Welsh M , Hung L , Waters CH ((1997) ) Sexuality in women with Parkinson’s disease. Mov Disord 12: , 923–927. |
[31] | Özcan T , Benli E , Özer F , Demir EY , Kaya Y , Ayyıldız A ((2016) ) The association between symptoms of sexual dysfunction and age at onset in Parkinson’s disease. Clin Auton Res 26: , 205–209. |
[32] | Bronner G , Peleg-Nesher S , Manor Y , Rosenberg A , Naor S , Taichman T , Ezra A , Gurevich T ((2023) ) Sexual needs and sexual function of patients with Parkinson’s disease. Neurol Sci 44: , 539–546. |
[33] | Ferrucci R , Panzeri M , Ronconi L , Ardolino G , Cogiamanian F , Barbieri S , Barone P , Bertolasi L , Padovani A , Priori A ((2016) ) Abnormal sexuality in Parkinson’s disease: Fact or fancy? . J Neurol Sci 369: , 5–10. |
[34] | Jitkritsadakul O , Jagota P , Bhidayasiri R ((2015) ) Postural instability, the absence of sexual intercourse in the past month, and loss of libido are predictors of sexual dysfunction in Parkinson’s disease. Parkinsonism Relat Disord 21: , 61–67. |
[35] | Weintraub D , Koester J , Potenza MN , Siderowf AD , Stacy M , Voon V , Whetteckey J , Wunderlich GR , Lang A ((2010) ) Impulse control disorders in Parkinson disease: A cross-sectional study of 3090 patients. Arch Neurol 67: , 589–595. |
[36] | Bronner G , Korczyn AD ((2017) ) The role of sex therapy in the management of patients with Parkinson’s disease. Mov Disord Clin Pract 5: , 6–13. |
[37] | Kotková P , Weiss P ((2013) ) Psychiatric factors related to sexual functioning in patients with Parkinson’s disease. Clin Neurol Neurosurg 115: , 419–424. |
[38] | Kinateder T , Marinho D , Gruber D , Hatzler L , Ebersbach G , Gandor F ((2022) ) Sexual dysfunctions in Parkinson’s disease and their influence on partnership-data of the PRISM Study. Brain Sci 12: , 159. |
[39] | Hughes AJ , Daniel SE , Kilford L , Lees AJ ((1992) ) Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry 55: , 181–184. |
[40] | ABEP: Brazilian Market Research Association (2022)https://www.abep.org/.Accessed on January 25, 2021.. |
[41] | Katz MJ , Wang C , Nester CO , Derby CA , Zimmerman ME , Lipton RB , Sliwinski MJ , Rabin LA ((2021) ) T-MoCA: A valid phone screen for cognitive impairment in diverse community samples. Alzheimers Dement (Amst) 13: , e12144. |
[42] | Goetz CG , Tilley BC , Shaftman SR , Stebbins GT , Fahn S , Martinez-Martin P , Poewe W , Sampaio C , Stern MB , Dodel R , Dubois B , Holloway R , Jankovic J , Kulisevsky J , Lang AE , Lees A , Leurgans S , LeWitt PA , Nyenhuis D , Olanow CW , Rascol O , Schrag A , Teresi JA , van Hilten JJ , LaPelle N Movement Disorder Society UPDRS Revision Task Force ((2008) ) Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov Disord 23: , 2129–2170. |
[43] | Valderramas S , Feres AC , Melo A ((2012) ) Reliability and validity study of a Brazilian-Portuguese version of the fatigue severity scale in Parkinson’s disease patients. Arq Neuropsiquiatr 70: , 497–500. |
[44] | Hutz CS , Zanon C ((2011) ) Revisão da adaptação, validação e normatização da Escala de Autoestima de Rosenberg. Aval Psicol 10: , 41–49. |
[45] | Chaudhuri KR , Pal S , DiMarco A , Whately-Smith C , Bridgman K , Mathew R , Pezzela FR , Forbes A , Högl B , Trenkwalder C ((2002) ) The Parkinson’s disease sleep scale: A new instrument for assessing sleep and nocturnal disability in Parkinson’s disease. J Neurol Neurosurg Psychiatry 73: , 629–635. |
[46] | Margis R , Donis K , Schönwald SV , Fagondes SC , Monte T , Martín-Martínez P , Chaudhuri KR , Kapczinski F , Rieder CR ((2009) ) Psychometric properties of the Parkinson’s Disease Sleep Scale–Brazilian version. Parkinsonism Relat Disord 15: , 495–499. |
[47] | Spanier GB ((1976) ) Measuring dyadic adjustment: New scales for assessing the quality of marriage and similar dyads. J Marriage Fam 38: , 15–28. |
[48] | Gorenstein C , Andrade L ((1996) ) Validation of a Portuguese version of the Beck Depression Inventory and the State-Trait Anxiety Inventory in Brazilian subjects. Braz J Med Biol Res 29: , 453–457. |
[49] | Rosen RC , Riley A , Wagner G , Osterloh IH , Kirkpatrick J , Mishra A ((1997) ) The international index of erectile function (IIEF): A multidimensional scale for assessment of erectile dysfunction. Urology 49: , 822–830. |
[50] | Gonzáles AI , Sties SW , Wittkopf PG , Mara LS , Ulbrich AZ , Cardoso FL , Carvalho Td ((2013) ) Validation of the International Index of Erectile Function (IIFE) for use in Brazil. Arq Bras Cardiol 101: , 176–182. |
[51] | Abdo C , Helena N ((2006) ) Elaboração e validação do quociente sexual - versão masculina, uma escala para avaliar a função sexual do homem/Development and validation of the male sexual quotient - a questionnaire to assess male sexual satisfaction. RBM Rev Bras Med 63: , 42–46. |
[52] | Mehanna R , Smilowska K , Fleisher J , Post B , Hatano T , Pimentel Piemonte ME , Kumar KR , McConvey V , Zhang B , Tan EK , Savica R; International Parkinson and Movement Disorder Society Task Force on Early Onset Parkinson’s Disease ((2022) ) Age cutoff for early-onset Parkinson’s disease: Recommendations from the International Parkinson and Movement Disorder Society Task Force on Early Onset Parkinson’s Disease. Mov Disord Clin Pract 9: , 869–878. |
[53] | Hoehn MM , Yahr MD ((1967) ) Parkinsonism: Onset, progression and mortality. Neurology 17: , 427–442. |
[54] | World Health Organization (2002) Defining sexual health: Report on technical consultation on sexual health. http://www.who.int/reproductivehealth/publications/sexual_health/defining_sexual_health.pdf.Accessed on February 25, 2022. |
[55] | Wielinski CL , Varpness SC , Erickson-Davis C , Paraschos AJ , Parashos SA ((2010) ) Sexual and relationship satisfaction among persons with young-onset Parkinson’s disease. J Sex Med 7: , 1438–1444. |
[56] | Solla P , Cannas A , Ibba FC , Loi F , Corona M , Orofino G , Marrosu MG , Marrosu F ((2012) ) Gender differences in motor and non-motor symptoms among Sardinian patients with Parkinson’s disease. J Neurol Sci 323: , 33–39. |


