
Association Between Parkinson’s Disease and Coronary Artery Disease: A Systematic Review and Meta-Analysis
Abstract
Background:
The relationship between Parkinson’s disease (PD) and coronary artery disease (CAD) is unclear.
Objective:
This study aims to investigate whether PD and CAD are associated through systematic review and meta-analysis of observational studies.
Methods:
Electronic database search of PubMed, EMBASE, and Web of Science for observational studies published from 1 January 2010 to 1 August 2021 was conducted using terms related to PD and CAD. Unadjusted risk ratios (RR) and odds ratios (OR) of included cohort and case-control studies respectively were used to ascertain the association between PD and CAD. Study heterogeneity was evaluated using the I2 test.
Results:
Forty-one full-text studies were initially retrieved for eligibility assessment. Five studies that satisfied the inclusion criteria, consisting of three cohort and two case-control studies, were eventually included in this meta-analysis. The five studies enrolled 35,237 PD patients and 650,866 non-PD patients. PD and CAD were found to be significantly associated in cohort studies (RR = 2.23, 95% CI = 1.08–4.59, p = 0.03; Fig. 2), which held after sensitivity analysis (RR = 1.45, 95% CI = 1.31–1.60, p < 0.001; Fig. 3). Case-control studies found a trend towards association of PD and CAD approaching significance (OR = 1.47, 95% CI = 0.84–2.56, p = 0.18; Fig. 2).
Conclusion:
Overall, this meta-analysis suggests that PD is associated with CAD. The underlying mechanisms, as well as the role of ethnicity and other comorbidities on the relationship between PD and CAD should be further explored.
INTRODUCTION
Parkinson’s disease (PD), clinically characterized by resting tremors, rigidity, and bradykinesia [1], is a common neurodegenerative disease in the elderly [2]. With increasing life expectancy, the prevalence and burden of PD have increased globally [3]. The prevalence of coronary artery disease (CAD) in the general population aged 20 and above is about 6.7% [4] and as high as 29% in the general elderly population [5]. However, the prevalence and relationship of CAD in the PD population is not well documented. Recent literature has increasingly described cardiovascular dysfunction as a non-motor manifestation in the prodromal phases of PD which worsens with disease progression [6, 7]. Moreover, PD and CAD might be linked due to shared vascular risk factors and cardiovascular dysautonomia from cardiac sympathetic denervation in PD [8]. In fact, recent studies also suggest that common risk factors for both PD and the general population such as diabetes and hypertension are prevalent conditions in both populations [9–11]. Increasing evidence seems to suggest an association between PD and CAD; however, the association between PD and CAD still remains unclear, with different studies yielding conflicting results. While some studies have shown that CAD was associated with PD [12] and that PD patients were associated with having acute myocardial infarction (AMI) [13], others have found similar [14] or even lower [15] rates of CAD among PD patients compared to controls. Previous studies [16, 17] have investigated the effects of PD on cardiovascular disease (CVD), including both CAD and cerebrovascular events, but none focusing on PD and CAD specifically.
CAD, including ischemic heart disease (IHD) and AMI, is one of the top causes of death among the elderly [18]. CAD is a preventable disease for which patients and those at high risk of developing CAD can benefit from early detection and treatment [19]. Therefore, it is imperative to clarify the relationship between PD and CAD in facilitating early identification and pre-emptive management of a debilitating disease like CAD.
In this systematic review and meta-analysis, the aim was to determine the association between PD and CAD, through the analysis of observational (cohort, case-control, cross-sectional) studies published between 1 January 2010 to 1 August 2021 that studied the frequency of CAD in PD patients compared to control groups.
METHODS
Eligibility criteria
For this systematic review and meta-analysis, all published observational studies reporting the prevalence of CAD [CAD, MI (myocardial ischemia), and/or IHD] in both PD patients and controls, with clear determination of PD and CAD based on hospital records, doctor’s diagnosis, disease identification codes, or self-reporting, were considered eligible.
Non-English articles, case reports, review articles, published abstracts, studies with duplicated study cohorts (the more recent one included), and studies where access to the full text was unavailable, were excluded. Studies with study groups which were non-representative of the general PD population, such as mortality studies, or control populations which had a natural higher predisposition to comorbidities like CAD than the general population, such as hospitalization studies, were also excluded.
Search strategy
All relevant articles published in English between 1 January 2010 to 1 August 2021 were identified by searching on PubMed, EMBASE, and Web of Science for studies that investigated the incidence and prevalence of AMI/IHD/CAD/CVD/coronary heart disease (CHD) in PD patients and non-PD controls. The search terms “coronary artery disease”, “coronary heart disease”, “heart failure”, “acute coronary syndrome”, “myocardial ischemia”, “cardiovascular disease”, “comorbidity”, “Parkinson’s disease”, “Parkinson’s”, “epidemiological studies”, “cohort studies”, “case-control studies”, and “observational studies” were used with appropriate Boolean operators for the identification of potential studies. The reference list of relevant studies was also manually examined for eligible studies that were not found using the search terms. The details of the search strategy are presented in Supplementary Material 1.
The articles were independently assessed by two authors (S.K.K.C and S.J.Y.L), to determine the eligibility to be included in the final review. Any disagreements were discussed with a third author (E.K.T) and resolved by consensus among the authors.
Data extraction
The title and abstracts were retrieved from the electronic database search for potentially relevant studies. The full reports of the potentially relevant studies were then retrieved and assessed to be included in the review based on the decided inclusion criteria.
The data extracted from the included studies were: sample size, patient and control demographics such as the mean age, gender distribution, and country where the study was conducted. Information regarding the study design, data source, outcomes of interest, and the adjustments applied to the outcome variables [risk ratio (RR), hazard ratio (HR), odds ratio (OR)] were also extracted.
The type of study was categorized into case control and cohort studies.
Outcome
The outcome of interest for this study was determined to be CAD. The terms IHD, AMI, CHD, or acute coronary syndrome (ACS) were taken to be synonymous with CAD.
The common outcome variable for comparison between all studies was chosen to be the unadjusted RR and unadjusted OR for cohort and case-control studies respectively. If adjusted RR/HR/OR was provided, unadjusted RR was calculated manually using R software [20] with the raw frequency of the outcome of interest (CAD/IHD/AMI) and sample size in PD and non-PD populations.
Initial search of the electronic databases yielded 1,365 studies, with 41 full text articles subsequently retrieved for eligibility assessment and five studies eventually selected for meta-analysis (Fig. 1). Out of the five studies, two studies provided adjusted OR [21, 22] and three studies provided adjusted HR [8, 12, 13]. One study [8] did not report the raw AMI frequencies, but instead only reported the calculated HR. Effort was made to contact the authors of the paper for the raw data, which proved unsuccessful. Hence, back-calculation using the reported HR was performed to estimate the raw frequencies and subsequently the unadjusted HR.
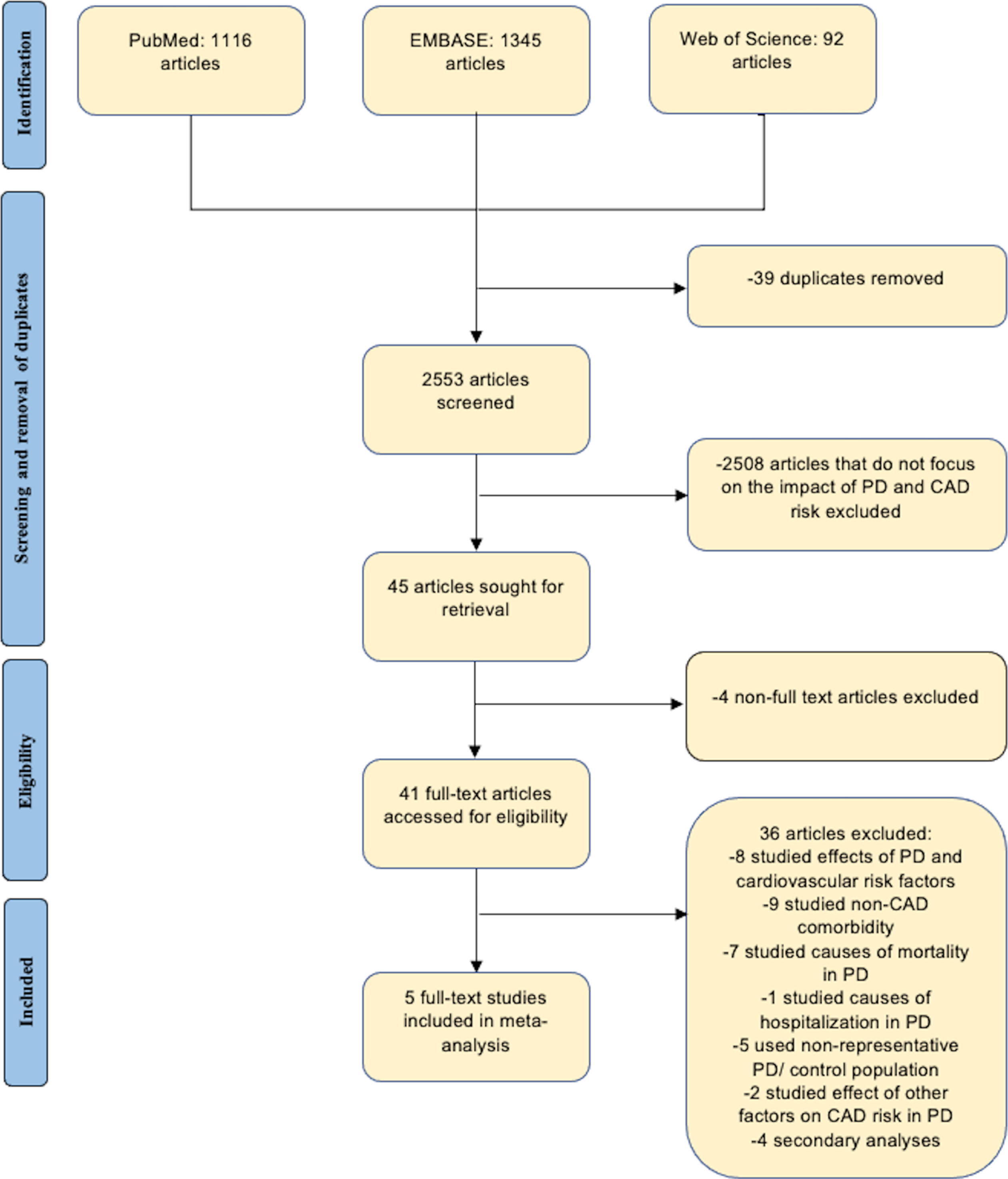
Fig. 1
PRISMA flowchart detailing database search procedure and exclusion criteria.
Finally, the unadjusted RR of the three cohort studies and OR of the two case-control studies were pooled together and compared between PD and non-PD groups to determine the association between PD and CAD.
Assessment of study quality
To assess the quality of included studies, the Newcastle-Ottawa Scale (NOS) was used to perform risk of bias (RoB) analysis. Studies were then classified as ‘Good’, ‘Fair’, or ‘Poor’ quality based on Agency for Healthcare Research and Quality (AHRQ) ratings which were derived from the NOS scores.
The details of the RoB and AHRQ framework used for study quality assessment are presented in Supplementary Material 2.
Statistical analysis
Statistical analysis was performed using R software [20]. Random effects meta-analyses via restricted maximum-likelihood estimator were performed on end points and variables due to observed estimates and sampling variability between studies. Between-study heterogeneity was presented by the I2 statistic test. p values for the I2 statistics were computed by chi-square distribution of Cochran Q test. Statistical significance was set at p < 0.05.
Sensitivity analysis
Where I2 values were high, sensitivity analysis was performed to reduce study heterogeneity in the meta-analysis. This was conducted through examination sources of heterogeneity among study cohorts and subsequently performing the meta-analysis after removing the corresponding study cohort contributing most to the study heterogeneity.
RESULTS
Included studies
Initial search of the electronic databases yielded 1,365 studies, and 41 full text articles were subsequently retrieved for eligibility assessment. Five studies were eventually selected for meta-analysis in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Fig. 1). Reasons for exclusion of studies retrieved for eligibility assessment are detailed in Supplementary Table 1.
The five studies, inclusive of three cohort studies and two case-control studies, enrolled 35,237 PD patients and 650,866 non-PD patients. Two [21, 22] studies were conducted in the United Kingdom (UK), while three [8, 12, 13] other studies were conducted in Asia, namely, Korea, China, and Taiwan respectively. Two studies [12, 13] compared AMI frequencies between PD and non-PD groups, while two studies [8, 21] and one other study [22] compared CAD and IHD frequencies respectively between PD and non-PD groups. One study, Li 2018 [8], investigated the outcomes of PD and controls between two separate populations, namely Malu and Wu Li Qiao (wlq). Hence, these studies were further split into two sub-groups, Li 2018 (malu) and Li 2018 (wlq), for analysis. Details of the five studies are summarized in Table 1.
Table 1
Summary of studies included in the meta-analysis
| No. | Author, year | Study design | Country | Sub-group | Sample size | # Male (%) | Mean age (SD) | Data source | PD diagnosis | CAD diagnostic tool | Matching | Outcome assessment | Outcome adjustment | Reported outcome (risk of CAD) | |||
| PD | Non-PD | PD | Non-PD | PD | Non-PD | ||||||||||||
| 1 | Liang, 2015 [13] | Cohort | Taiwan | Nil | 3,211 | 3,211 | 1,652 (51.4) | 1,620 (50.5) | 71.9 (9.3) | 72.0 (9.0) | National Health Insurance Claim Database | International Classification of Disease diagnosis codes | Medical information from health care database | Age, Sex | AMI | propensity score matching (based on age, sex, preexisting comorbidity, socioeconomic status) | Higher |
| 2 | Park, 2020 [12] | Cohort | Korea | Nil | 25,624 | 128,120 | 10,890 (42.5) | 54,451 (42.5) | 69 (10.2) | 69 (10.2) | National Health Insurance Service and National Rare Intractable Disease Registry Database | International Classification of Disease diagnosis codes | Medical information from health care database | Age, Sex | AMI | age, sex, lowest quartile income, diabetes mellitus, hypertension, and dyslipidemia | Higher |
| 3 | Mclean, 2017 [21] | Case-Control | UK (Scotland) | Nil | 2,640 | 507,862 | 1,459 (55.3) | 232,602 (45.8) | 76.4 (9.1) | 68.2 (9.7) | Primary Care Clinical Informatics Unit Database | Read Codes (NHS Scotland Information) | Medical information from health care database | NR | CAD | age, gender, and deprivation (carstairs) score | Higher |
| 4 | Li, 2018 [8] | Cohort | China | Malu | 63 | 4,483 | 34 (54.0) | 1,906 (42.5) | 74.9 (8.6) | 66.5 (9.4) | Door to door assessment (PD) and questionnaire (CAD) | UK Parkinson’s Disease Society Brain Bank Clinical Diagnostic Criteria | Questionnaire | NR | CAD | age, sex, smoking status, alcohol consumption, hypertension, diabetes mellitus, tea consumption, hypercholesterolemia and BMI | Higher |
| Wuliqiao (wlq) | 62 | 3,553 | 26 (41.9) | 1,134 (31.9) | 75.7 (9.5) | 69.4 (10.6) | Higher | ||||||||||
| 5 | Becker, 2010 [22] | Case-Control† | UK | Nil | 3,637 | 3,637 | 2,167 (59.6) | 2,167 (59.6) | NR | NR | General Practice Research Database | Oxford Medical Information System or Read codes | Medical information from health care database | Age, gender, general practice, PD diagnosis date, years of history in GPRD prior to PD diagnosis date | IHD | age, sex, smoking status, BMI, other comorbidities | Higher |
†Nested case-control. No., number; UK, United Kingdom; PD, Parkinson’s disease; CAD, coronary artery disease; IHD, ischemic heart disease; AMI, acute myocardial infarction; NR, not reported; BMI, body mass index; NHS, National Health Service; GPRD, General Practice Research Database.
The reporting quality of the included studies were all ‘Good’ except for Li 2018 [8] which used questionnaires and self-reporting for outcome assessment, in contrast to other studies which only used registries and databases. Details of the reporting quality of the included studies are summarized in Table 2.
Table 2A
Risk of Bias Analysis for Cohort studies
| Author | Selection | Comparability | Outcome | Total quality score | Quality rank | |||||
| Representativeness of exposed cohort | Selection of the non-exposed cohort | Ascertainment of exposure | Demonstration that outcome of interest was not present at start of study | Comparability of cohorts based on the design or analysis | Assessment of outcome | Was follow-up long enough for outcomes to occur | Adequacy of follow up of cohort | |||
| Liang, 2015 [13] | + | + | + | + | ++(age, sex, comorbidities, socioeconomic status) | +(National Health Insurance claim database) | +(from index visit to the first occurrence of AMI, death, or end of follow up) | 8 | Good | |
| Park, 2020 [12] | + | + | + | + | ++(age, sex) | +(National Health Insurance Service and National Rare Intractable Disease Registry database) | +(from 2010 to 2016) | 8 | Good | |
| Li, 2018 [8] | + | + | + | ++(age, sex, smoking status, alcohol consumption, hypertension, diabetes mellitus, tea consumption, hypercholesterolemia, and body mass index) | (Questionnaire, Self-Report) | +(from April 2013 to October 2013 for Malu, 2014 for Wuliqiao) | 6 | Poor | ||
Table 2B
Risk of Bias Analysis for Case-control studies
| Author | Selection | Comparability | Exposure | Total quality score | Quality rank | |||||
| Is the case definition adequate? | Representativeness of the cases | Selection of controls | Definition of controls | Comparability of cases and controls | Ascertainment of exposure | Same method of ascertainment for cases and controls | Non-response rate | |||
| Mclean, 2017 [21] | + | + | + | ++(age, gender, socioeconomic deprivation) | +(Primary Care Clinical Informatics Unit Database) | + | 7 | Good | ||
| Becker, 2010 [22] | + | + | + | + | ++(age, gender, calendar time) | +(General Practice Research Database) | + | 8 | Good | |
Meta-analysis
This study found that PD was associated with CAD (RR = 2.23, 95% CI = 1.08–4.59, p = 0.03; Fig. 2) for cohort studies. A greater association between PD and CAD was found among the cohort studies as compared to case-control studies (OR = 1.47, 95% CI = 0.84–2.56, p = 0.18; Fig. 2).
Fig. 2
Forest plots of cohort and case-control studies.
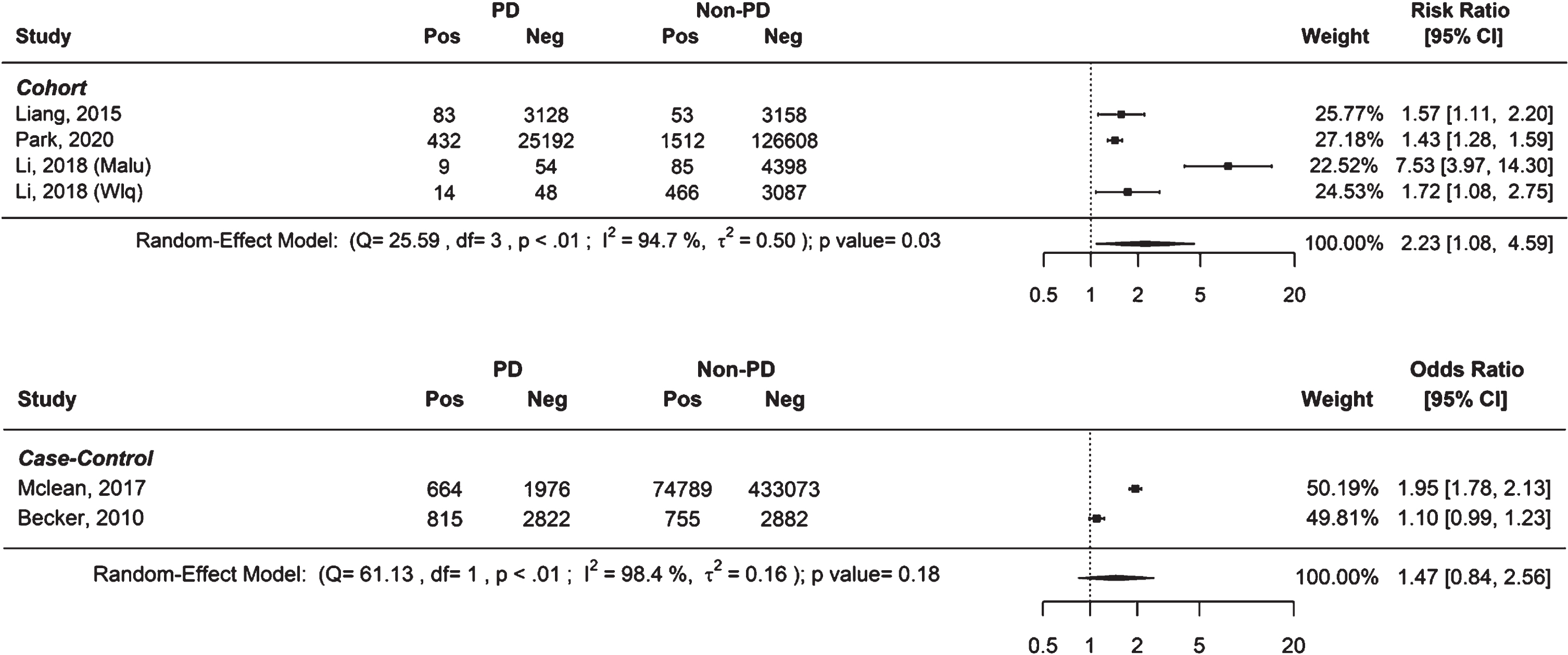
The I2 value obtained before sensitivity analysis was 94.7% and 98.4% for cohort and case-control studies respectively.
Sensitivity analysis
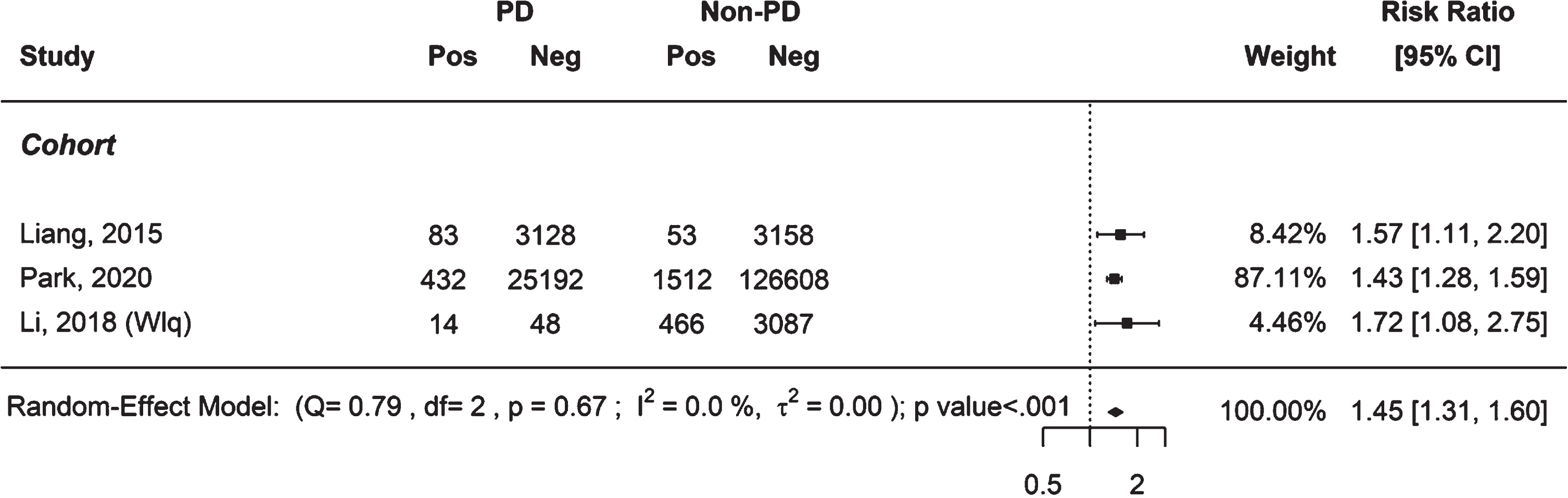
After sensitivity analysis to reduce study heterogeneity, the positive association found between PD and CAD in cohort studies held with I2 value at 0% (RR = 1.45, 95% CI = 1.31–1.60, p < 0.001; Fig. 3) after removal of one study cohort (Li 2018 (malu)) that contributed significantly to the study heterogeneity, further supporting our findings.
Fig. 3
Forest plot of cohort studies after sensitivity analysis.
DISCUSSION
Association between PD and CAD
This study found an association between PD and CAD in cohort studies, providing new evidence to address the uncertainty surrounding the relationship between the two. Several reasons have been proposed to explain this correlation.
First, while the pathophysiology of PD remains poorly understood, it has been hypothesized that the neurodegenerative disease may be caused by oxidative stress that leads to mitochondrial dysfunction and damage to the substantial nigra [23]. Moreover, neurodegeneration in PD have also been thought to be contributed by chronic central and systemic inflammation [24]. Both oxidative stress and systemic inflammation are possible underlying mechanisms in the pathogenesis of atherosclerosis [25, 26] and CAD [27–29], suggesting a possible common pathophysiology in both PD and CAD that could explain their association.
Second, autonomic dysfunction, specifically an increased sympathetic activity and decreased parasympathetic activity, in PD patients have been proposed to be a possible mechanism through which PD may predispose to vascular diseases like CAD [30]. Significantly, orthostatic hypotension (OH) is a known non-motor manifestation of PD that is thought to be caused by autonomic dysfunction in PD [31, 32]. OH has been associated with an increased risk of CAD and suggested to be a consequence of decreased myocardial perfusion leading to ischemia [33, 34]. Hence, OH is a possible mechanism for which PD could be associated with CAD. Moreover, beyond autonomic dysfunction, the concept of a “Parkinsonian heart” in recent literature further describes the cardiovascular dysfunction in PD patients not only due to sympathetic denervation, but also changes that occur at the functional, structural, and molecular level of the heart [35, 36].
Third, PD and CAD could be linked via a common molecular pathway involving matrix metalloproteinases (MMPs). MMPs are a family of proteins that are responsible for tissue remodeling and degradation of extracellular matrix (ECM) proteins. MMPs play a key role in the pathogenesis of atherosclerosis and CAD [37], and vascular endothelial cell damage from CAD can further activate MMPs through the release of free radicals and proinflammatory cytokines [38]. Activation of MMPs causes ECM degradation and Blood-Brain-Barrier leakage, which could facilitate microglial activation and dopaminergic neurodegeneration [39]. Moreover, MMPs activation could cause alteration and aggregation of α-synuclein protein, a key protein in the pathogenesis of PD [40]. Therefore, MMPs implicated in both CAD and PD could possibly mediate both pathologies.
Fourth, PD patients have a high tendency for physical inactivity [40] due to both non-motor (dementia, depression) and motor (bradykinesia, tremors, rigidity) symptoms, which is a significant risk factor for CAD [41, 42]. Regular physical activity has known cardioprotective effects [42], and PD patients have markedly reduced levels of physical activity with greater disease severity [40]. Therefore, it is plausible that as PD, a chronic progressive disease, worsens with time, the eventual loss of ability to be physically active and its cardioprotective effects could make PD patients more vulnerable to cardiovascular diseases like CAD.
Fifth, medication given for the treatment of PD such as Levodopa have been known to cause adverse cardiovascular effects through an increased serum homocysteine level which induces atherosclerosis [43, 44]. Specifically, many ergot-derived dopamine agonist have been associated with valvulopathies and fibrosis of the heart leading to cardiovascular impairment [45, 46]. Anti-psychotic medications prescribed to PD patients who develop psychosis also increases risk of cardiovascular mortality [47–49]. Therefore, pharmacological treatment commonly initiated in the management of PD patients could also be a possible pathophysiological mechanism affecting cardiovascular health in PD patients. Nonetheless, while PD treatment may be the cause of increased CAD risk rather than PD itself, a recent meta-analysis [50] found that the cardiac complication associated with PD were more related to the degenerative disease itself rather than exposure to cardiotropic drugs.
Furthermore, several PD-related genes may be potentially involved in the relationship between PD and CAD. The PARK family proteins related to PD such as α-synuclein (PARK1), Parkin (PARK2), PINK1 (PARK6), DJ-1 (PARK7), and LRRK2 (PARK8) have been proposed to play a role in the association of PD and cardiac dysfunction, including CAD [51–53]. These genes have also been thought to be found in heart tissue and implicated in oxidative damage and loss of cardioprotective effects in gene mutations or depletions [54]. Nonetheless, there are still limited data on the molecular and genetic links of PD and CAD, and more studies are needed in the future to decipher the potential links between PD and cardiovascular health.
It is also plausible that patients with PD or comorbidities such as CAD are innately more likely to visit healthcare facilities for their treatment or follow-up, putting them in a more likely position for health related problems such as PD and CAD to be presented and diagnosed by a healthcare professional. Studies have shown that the combination of PD related symptoms, as well as the associated treatment side-effects and comorbidities have led to an increase in healthcare utilization and expenditure, with increased healthcare seeking behavior in populations where there is higher prevalence and awareness of PD [55, 56]. Therefore, there could be increased health seeking behavior in populations with either PD or comorbidities which increases their chances of being diagnosed with either diseases compared to the general population.
While some previous studies have proposed a negative correlation between PD and CAD [15], comparison was made with a hospital-based control group which were subject to selection bias as hospital-based populations are more likely to have comorbidities like CAD compared to the general population. As such, these studies were not included in this review which aims to investigate the association of CAD with PD patients versus the general population.
Nonetheless, it is interesting to note that while previous studies have documented a lower prevalence of vascular risk factors such as diabetes, hypertension, and dyslipidemia and smoking rate among PD patients [23, 57], our findings suggest that PD and CAD are associated. Therefore, despite the reduced prevalence of vascular risk factors, patients with PD should still be monitored for CAD which could be mediated by various mechanisms as proposed above.
Cohort versus case-control studies
Methodological factors may have played a role in the results with cohort studies showing a more significant CAD association in PD patients compared to case-control studies. The cohort studies included predominantly Asian populations whereas the case-control studies selected a predominantly Caucasian population in the UK. Studies have shown that Asians are more predisposed to developing CAD compared to non-Asians [58, 59], suggesting that ethnic differences may have contributed to the greater association found in cohort studies.
Study heterogeneity
For cohort studies, the study cohort that contributed to significant heterogeneity within the results and subsequently removed in the sensitivity analysis was Li 2018 (malu). The study cohort could have attributed to significant study heterogeneity as it included a rural study population, in contrast to the other cohort studies that included populations from more developed areas or countries. Nonetheless, the positive association found in cohort studies held with low heterogeneity after sensitivity analysis and reanalysis of the remaining cohorts after removal of Li 2018 (malu), further supporting our findings.
For case-control studies, sensitivity analysis could not be performed as there were only two studies [21, 22]. Mclean et al. [21] found a significant positive association between PD and CAD in contrast to Becker et al. [22] which found an insignificant positive association. Study heterogeneity between the case-control studies may be attributed to differences in methodology of subject recruitment as Becker et al. [22] had gender and age (year) matched cases and controls in contrast to Mclean et al. [21] where cases and controls were matched by gender, age groups (55 to 64, 65 to 74, 75 to 84, and over 85) and socioeconomic deprivation.
Potential implications
The positive association between PD and CAD found in this study emphasizes the greater need for early screening and prevention of CAD in PD patients. Healthier lifestyle choices and more regular follow up to prevent and slow down the progression of CAD should be encouraged especially among younger PD patients. PD patients, especially those with PD onset at 50 years or younger who have a longer disease trajectory, should undergo cardiovascular risk screening at a younger age and be put under closer cardiac monitoring involving cardiac assessments such as treadmill exercise stress test and cardiac echocardiogram for early detection of any present cardiac abnormalities. Early control is then warranted for any abnormalities found in the cardiovascular screen or cardiac assessment. Furthermore, the possible involvement of MMPs and OH in the pathogenesis of PD and CAD sets up plausible new therapeutic angles that should be further investigated, where treatment inhibiting MMPs or reducing OH could reduce the risk of PD or CAD.
Study strengths
Our meta-analysis was a novel investigation of the association between PD and CAD. Two previous meta-analysis [16, 17] explored the relationship between PD and CAD. However, Hong et al. [17] investigated the effects of PD on both cerebrovascular and cardiovascular disease as one entity, and in contrast to Alves et al. [16], this study excluded studies which focused solely on specific subgroups of PD patients, such as PD mortality and hospital admission studies, hence selecting a more representative PD population. Furthermore, this study only included more recent publications in the last ten years with a more updated view on the subject matter.
Study limitations
First, inherent publication bias may be present in the selection of studies. Studies with positive findings may be more publishable and replicable, hence having a greater chance of selection by this meta-analysis. Second, while this meta-analysis included studies from a diverse population consisting of Europe and Asia, it had a small number of available studies with limited capture of all ethnic races, affecting the generalizability of this study to both the global and certain populations.
Conclusions
In this systematic review and meta-analysis, we found an association between PD and CAD. However, to prove a direct cause and effect relationship between the two conditions, more large-scale prospective studies and experimental data will be required. Future studies should also explore the contributions of ethnicity, comorbidities, and other lifestyle factors on the relationship between PD and CAD.
ACKNOWLEDGMENTS
We thank National Medical Research Council for their support (STAR 0030 and PD LCG 000207 SPARK II to TEK).
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JPD-223291.
REFERENCES
[1] | Lim EW , Tan EK ((2017) ) Genes and nonmotor symptoms in Parkinson’s disease. Int Rev Neurobiol 133: , 111–127. |
[2] | Dorsey E , Constantinescu R , Thompson J , Biglan K , Holloway R , Kieburtz K , Marshall F , Ravina B , Schifitto G , Siderowf A , Tanner C ((2006) ) Projected number of people with Parkinson disease in the most populous nations, 2005 through 2030. Neurology 68: , 384–386. |
[3] | Macerollo A , Chen J ((2016) ) Trends in the incidence of Parkinson disease. Neurol 73: , 1497–1498. |
[4] | Fryar C , Chen T , Li X ((2012) ) Prevalence of uncontrolled risk factors for cardiovascular disease: United States, 1999-2010. NCHS Data Brief 103: , 1–8. |
[5] | Gadó K , Szabo A , Markovics D , Virág A ((2022) ) Most commoncardiovascular diseases of the elderly –A review article. Dev Health Sci 4: , 27–32. |
[6] | Krämer H , Lautenschläger G , de Azevedo M , Doppler K , Schänzer A , Best C , Oertel W , Reuter I , Sommer C , Birklein F ((2019) ) Reduced central sympathetic activity in Parkinson’s disease. Brain Behav 9: , e01463. |
[7] | Lamotte G , Holmes C , Wu T , Goldstein D ((2019) ) Long-term trends in myocardial sympathetic innervation and function in synucleinopathies. Parkinsonism Relat Disord 67: , 27–33. |
[8] | Li Q , Wang C , Tang H , Chen S , Ma J ((2018) ) Stroke and coronary artery disease are associated with Parkinson’s disease. Can J Neurol Sci 45: , 559–565. |
[9] | Sun Y , Chang Y , Chen H , Su Y , Su H , Li C ((2012) ) Risk of Parkinson disease onset in patients with diabetes: A 9-year population-based cohort study with age and sex stratifications. Diabetes Care 35: , 1047–1049. |
[10] | Cereda E , Barichella M , Pedrolli C , Klersy C , Cassani E , CaccialanzaR , Pezzoli G ((2011) ) Diabetes and risk of Parkinson’s disease: Asystematic review and meta-analysis. Diabetes Care 34: , 12. |
[11] | Qiu C , Hu G , Kivipelto M , Laatikainen T , Antikainen R , Fratiglioni L , Jousilahti P , Tuomilehto J ((2011) ) Association of blood pressure and hypertension with the risk of Parkinson disease: The National FINRISK Study. Hypertension 57: , 1094–1100. |
[12] | Park J , Kim D , Park Y , Kwon D , Choi M , Jung J , Han K ((2020) ) Association of Parkinson disease with risk of cardiovascular disease and all-cause mortality. Circulation 141: , 1205–1207. |
[13] | Liang H , Huang Y , Pan S ((2015) ) Parkinson disease and risk of acute myocardial infarction: A population-based, propensity score–matched, longitudinal follow-up study. Am Heart J 169: , 508–514. |
[14] | Nataraj A , Rajput A ((2005) ) Parkinson’s disease, stroke, and related epidemiology. Mov Disord 20: , 1476–1480. |
[15] | Abugroun A , Taha A , Abdel-Rahman M , Patel P , Ali I , Klein L ((2020) ) Cardiovascular risk among patients ≥65 years of age with Parkinson’s disease (from the National Inpatient Sample). Am J Cardiol 136: , 56–61. |
[16] | Alves M , Caldeira D , Ferro J , Ferreira J ((2019) ) Does Parkinson’s disease increase the risk of cardiovascular events? A systematic review and meta-analysis. Eur J Neurol 27: , 288–296. |
[17] | Hong C , Hu H , Chan L , Bai C ((2018) ) Prevalent cerebrovascular and cardiovascular disease in people with Parkinson’s disease: A meta-analysis. Clin Epidemiol 10: , 1147–1154. |
[18] | Khan M , Hashim M , Mustafa H , Baniyas M , Suwaidi S , Alkatheeri R , Alblooshi F , Almatrooshi M , Alzaabi M , Darmaki R , Lootah S ((2020) ) Global epidemiology of ischemic heart disease: Results from the Global Burden of Disease Study. Cureus 12: , e9349. |
[19] | Arnett DK , Blumenthal RS , Albert MA , Buroker AB , Goldberger ZD , Hahn EJ , Himmelfarb CD , Khera A , Lloyd-Jones D , McEvoy JW , Michos ED , Miedema MD , Muñoz D , Smith SC Jr , Virani SS , Williams KA Sr , Yeboah J , Ziaeian B ((2019) ) 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 74: , 1376–1414. |
[20] | R Core Team (2020) R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. Available from: https://www.R-project.org/. |
[21] | McLean G , Hindle J , Guthrie B , Mercer S ((2017) ) Co-morbidity and polypharmacy in Parkinson’s disease: Insights from a large Scottish primary care database. BMC Neurol 17: , 126. |
[22] | Becker C , Jick S , Meier C ((2010) ) Risk of stroke in patients with idiopathic Parkinson disease. Parkinsonism Relat Disord 16: , 31–35. |
[23] | Scigliano G , Musicco M , Soliveri P , Piccolo I , Ronchetti G , Girotti F ((2006) ) Reduced risk factors for vascular disorders in Parkinson disease patients: A case-control study. Stroke 37: , 1184–1188. |
[24] | Collins L , Toulouse A , Connor T , Nolan Y ((2012) ) Contributions of central and systemic inflammation to the pathophysiology of Parkinson’s disease. Neuropharmacology 62: , 2154–2168. |
[25] | Harrison D , Griendling K , Landmesser U , Hornig B , Drexler H ((2003) ) Role of oxidative stress in atherosclerosis. Am J Cardiol 91: , 7–11. |
[26] | Libby P , Ridker P , Maseri A ((2002) ) Inflammation and atherosclerosis. Circulation 105: , 1135–1143. |
[27] | Heitzer T , Schlinzig T , Krohn K , Meinertz T , Münzel T ((2001) ) Endothelial dysfunction, oxidative stress, and risk of cardiovascular events in patients with coronary artery disease. Circulation 104: , 2673–2678. |
[28] | Madamanchi N , Vendrov A , Runge M ((2005) ) Oxidative stress and vascular disease. Arterioscler Thromb Vasc Biol 25: , 29–38. |
[29] | Hansson G ((2005) ) Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med 352: , 1685–1695. |
[30] | Scorza F , Fiorini A , Scorza A , Finsterer J ((2018) ) Cardiac abnormalities in Parkinson’s disease and Parkinsonism. J Clin Neurosci 53: , 1–5. |
[31] | Velseboer D , de Haan R , Wieling W , Goldstein D , Bie R ((2011) ) Prevalence of orthostatic hypotension in Parkinson’s disease: A systematic review and meta-analysis. Parkinsonism Relat Disord 17: , 724–729. |
[32] | Jain S , Goldstein D ((2012) ) Cardiovascular dysautonomia in Parkinson disease: From pathophysiology to pathogenesis. Neurobiol Dis 46: , 572–580. |
[33] | Verwoert G , Mattace-Raso F , Hofman A , Heeringa J , Stricker B , Breteler M , Witteman J ((2008) ) Orthostatic hypotension and risk of cardiovascular disease in elderly people: The Rotterdam Study. J Am Geriatr Soc 56: , 1816–1820. |
[34] | Rose K , Tyroler H , Nardo C , Arnett D , Light K , Rosamond W , Sharrett A , Szklo M ((2000) ) Orthostatic hypotension and the incidence of coronary heart disease: The atherosclerosis risk in communities study. Am J Hypertens 13: , 571–578. |
[35] | Fornai F , Ruffoli R , Soldani P , Ruggieri S , Paparelli A ((2007) ) The“Parkinsonian heart”: From novel vistas to advanced therapeuticapproaches in Parkinson’s disease. Curr Med Chem 14: , 2421–2428. |
[36] | Goldstein D , Sharabi Y ((2019) ) The heart of PD: Lewy body diseases as neurocardiologic disorders. Brain Res 1702: , 74–84. |
[37] | Mittal B , Mishra A , Srivastava A , Kumar S , Garg N ((2014) ) Matrix metalloproteinases in coronary artery disease. Adv Clin Chem 64: , 1–72. |
[38] | Lakhan S , Kirchgessner A , Tepper D , Leonard A ((2013) ) Matrix metalloproteinases and blood-brain barrier disruption in acute ischemic stroke. Front Neurol 4: , 32. |
[39] | Brkic M , Balusu S , Libert C , Vandenbroucke R ((2015) ) Friends or foes: Matrix metalloproteinases and their multifaceted roles in neurodegenerative diseases. Mediators Inflamm 2015: , 1–27. |
[40] | Nimwegen M , Speelman A , Hofman-van Rossum E , Overeem S , Deeg D , Borm G , van der Horst M , Bloem B , Munneke M ((2011) ) Physical inactivity in Parkinson’s disease. J Neurol 258: , 2214–2221. |
[41] | León-Latre M , Moreno-Franco B , Andrés-Esteban , Ledesma M , Laclaustra , Alcalde V , Peñalvo J , Ordovás J , Casasnovas J ((2014) ) Sedentary lifestyle and its relation to cardiovascular riskfactors, insulin resistance and inflammatory profile. Rev EspCardiol 67: , 449–455. |
[42] | Lavie C , Ozemek C , Carbone S , Katzmarzyk P , Blair S ((2019) ) Sedentary behavior, exercise, and cardiovascular health.. Circ Res 124: , 799–815. |
[43] | Rogers J , Sanchez-Saffon A , Frol A , Diaz-Arrastia R ((2003) ) Elevated plasma homocysteine levels in patients treated with levodopa. Arch Neurol 60: , 59. |
[44] | Temple M , Luzier A , Kazierad D ((2000) ) Homocysteine as a risk factor for atherosclerosis. Ann Pharmacother 34: , 57–65. |
[45] | Horvath J , Fross R , Kleiner-Fisman G , Lerch R , Stalder H , Liaudat S , Raskoff W , Flachsbart K , Rakowski H , Pache J , Burkhard P , Lang A ((2004) ) Severe multivalvular heart disease: A new complication of the ergot derivative dopamine agonists. Mov Disord 19: , 656–662. |
[46] | Zanettini R , Antonini A , Gatto G , Gentile R , Tesei S , Pezzoli G ((2007) ) Valvular heart disease and the use of dopamine agonists for Parkinson’s disease. N Engl J Med 356: , 39–46. |
[47] | The Parkinson Study Group ((1999) ) Low-dose clozapine for the treatment of drug-induced psychosis in Parkinson’s disease. N Engl J Med 340: , 757–763. |
[48] | Emre M , Ford P , Bilgiç B , Uç E ((2014) ) Cognitive impairment and dementia in Parkinson’s disease: Practical issues and management. Mov Disord 29: , 663–672. |
[49] | Raedler T ((2010) ) Cardiovascular aspects of antipsychotics. Curr Opin Psychiatry 23: , 574–581. |
[50] | Heranval A , Lefaucheur R , Fetter D , Rouillé A , Goff F , Maltête D ((2016) ) Drugs with potential cardiac adverse effects:Retrospective study in a large cohort of parkinsonian patients. Rev Neurol (Paris) 172: , 318–323. |
[51] | Chen Y , Dorn G ((2013) ) PINK1-phosphorylated mitofusin 2 is a Parkin receptor for culling damaged mitochondria. Science 340: , 471–475. |
[52] | Mukherjee U , Ong S , Ong S , Hausenloy D ((2015) ) Parkinson’s disease proteins: Novel mitochondrial targets for cardioprotection. Pharmacol Ther 156: , 34–43. |
[53] | Bloem B , Okun M , Klein C ((2021) ) Parkinson’s disease. Lancet 397: , 2284–2303. |
[54] | Cuenca-Bermejo L , Almela P , Navarro-Zaragoza J , Fernández E , González-Cuello A , Laorden M , Herrero M ((2021) ) Cardiac changesin Parkinson’s disease: Lessons from clinical and experimentalevidence. Int J Mol Sci 22: , 13488. |
[55] | Csoti I , Jost W , Reichmann H ((2016) ) Parkinson’s disease between internal medicine and neurology. J Neural Transm 123: , 3–17. |
[56] | Mantri S , Fullard M , Beck J , Willis W ((2019) ) State-level prevalence, health service use, and spending vary widely among Medicare beneficiaries with Parkinson disease. NPJ Parkinson’s Dis 5: , 1. |
[57] | De Michele G , Filla A , Volpe G , De Marco V , Gogliettino A , Ambrosio G , Marconi R , Castellano A , Campanella G ((1996) ) Environmental and genetic risk factors in Parkinson’s disease: A case-control study in southern Italy. Mov Disord 11: , 17–23. |
[58] | Agha A ((2019) ) Association between Asian ethnicity and premature coronary artery disease. Eurasian J Med 543: , 38. |
[59] | Zaman M , Philipson P , Chen R , Farag A , Shipley M , Marmot M , Timmis A , Hemingway H ((2013) ) South Asians and coronary disease: Is there discordance between effects on incidence and prognosis? Heart 99: , 729–736. |


