
Recommendations for the Organization of Multidisciplinary Clinical Care Teams in Parkinson’s Disease
Abstract
Background:
Optimal management in expert centers for Parkinson’s disease (PD) usually involves pharmacological and non-pharmacological interventions, delivered by a multidisciplinary approach. However, there is no guideline specifying how this model should be organized. Consequently, the nature of multidisciplinary care varies widely.
Objective:
To optimize care delivery, we aimed to provide recommendations for the organization of multidisciplinary care in PD.
Methods:
Twenty expert centers in the field of multidisciplinary PD care participated. Their leading neurologists completed a survey covering eight themes: elements for optimal multidisciplinary care; team members; role of patients and care partners; team coordination; team meetings; inpatient versus outpatient care; telehealth; and challenges towards multidisciplinary care. During a consensus meeting, outcomes were incorporated into concept recommendations that were reviewed by each center’s multidisciplinary team. Three patient organizations rated the recommendations according to patient priorities. Based on this feedback, a final set of recommendations (essential elements for delivery of multidisciplinary care) and considerations (desirable elements) was developed.
Results:
We developed 30 recommendations and 10 considerations. The patient organizations rated the following recommendations as most important: care is organized in a patient-centered way; every newly diagnosed patient has access to a core multidisciplinary team; and each team has a coordinator. A checklist was created to further facilitate its implementation.
Conclusion:
We provide a practical tool to improve multidisciplinary care for persons with PD at the organizational level. Future studies should focus on implementing these recommendations in clinical practice, evaluating their potential applicability and effectiveness, and comparing alternative models of PD care.
INTRODUCTION
Parkinson’s disease (PD) is a complex neurodegenerative disorder associated with considerable disability [1]. Despite optimal medical management, motor- and non-motor symptoms can be relieved only partially [2]. Examples of motor symptoms that are controlled suboptimally with current medications include freezing of gait and postural instability, resulting in falls and difficulties with activities of daily living [3]. Common non-motor symptoms that present during all disease stages include autonomic dysfunction, cognitive symptoms, psychiatric disorders, fatigue and sleep disturbances [4]. These complex problems could possibly be improved by supplemental, non-pharmacological interventions. Scientific evidence for such non-pharmacological interventions is increasing, in particular for physiotherapy [5]. Other allied health approaches, e.g., occupational therapy or speech-language therapy, are also developing a role in the management of PD [6, 7], with rising referral rates [8]. Finally, there is an appreciation—now also supported by emerging evidence—that organizing different healthcare professionals into a multidisciplinary or interdisciplinary care team with shared and harmonized clinical decisions may improve the overall management of PD [9, 10].
Various guidelines recommend that all persons with PD should have access to a broad range of medical and allied health professionals [11–13]. Healthcare centers around the world have followed this recommendation and thus deliver multidisciplinary care for persons with PD, with involvement of different healthcare professionals [14]. However, there is an absence of a guideline that clarifies how such a multidisciplinary team approach should be organized [15]. An important framework for the provision of multidisciplinary care is vertical and horizontal integration at the clinical, professional, organisational and system level, supported by person-focused and population-based care as guiding principles [16]. Inspired by this, several different organizational models of multidisciplinary care have been evaluated, including inpatient rehabilitation [17, 18], community-based treatment [19, 20] and home visits by a team of healthcare professionals [21]. Furthermore, new care models are arising, such as hubs combining medical services and science [22]. However, the efficacy of these approaches has shown to be variable. Many questions remain to be answered, e.g., which healthcare disciplines should be part of the core multidisciplinary team? What is the role of telehealth in multidisciplinary care [23, 24]? How can patients and care partners be involved in their own healthcare team?
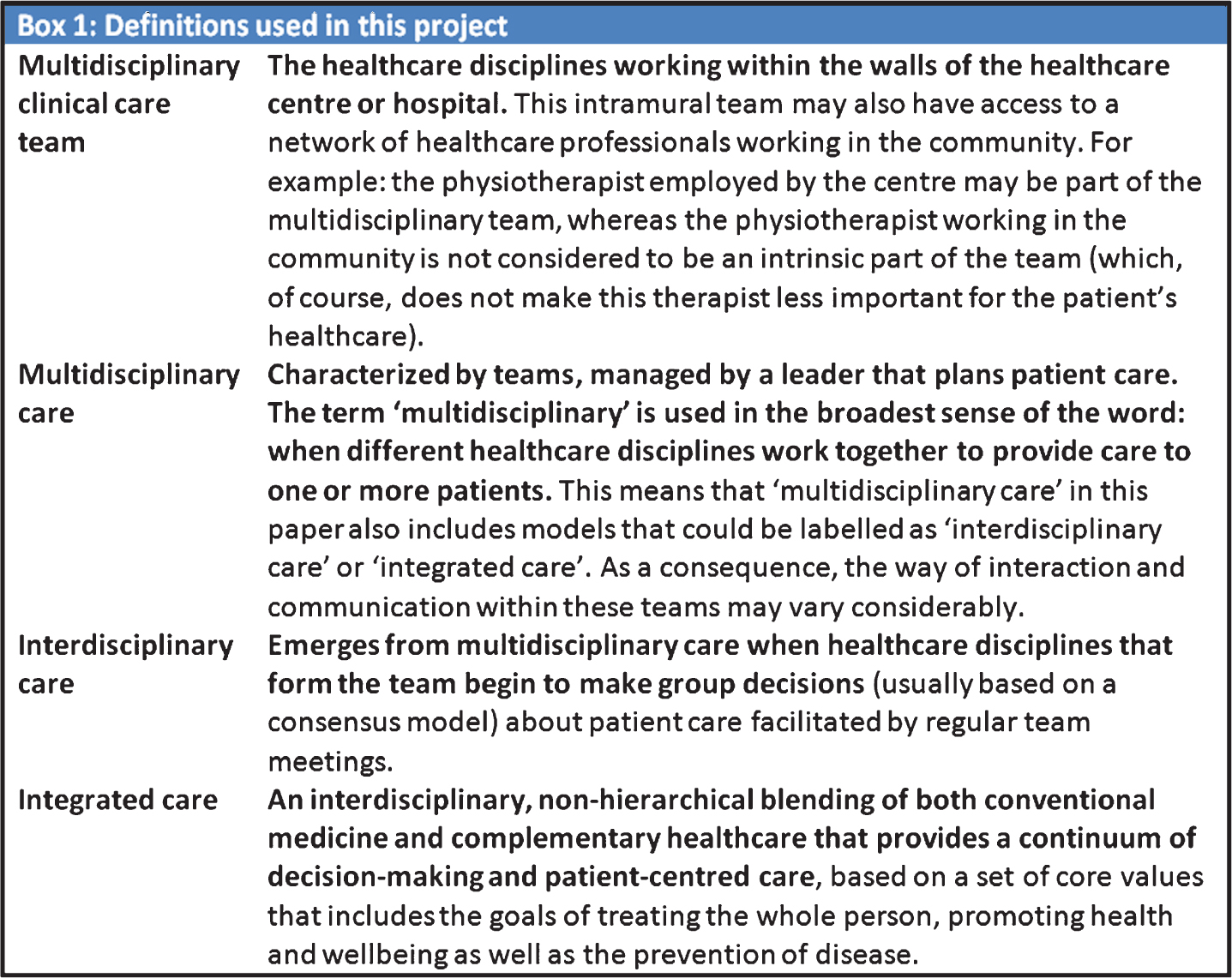
Because there is no consensus, the nature of multidisciplinary care varies widely between centers around the world [14], We therefore aimed to provide a practice-based guideline for the organization of multidisciplinary clinical care teams in PD. To develop this tool, we used the experience obtained from 20 expert centers in PD. Our goal was to provide both recommendations (essential elements for delivery of multidisciplinary care) and considerations (desirable elements). Importantly, these recommendations are designed to be aspirational guidelines, since not every healthcare center will have sufficient resources to pursue all recommendations. Box 1 describes several definitions used here, including the ‘multidisciplinary care team’, which we define as the healthcare disciplines working within the walls of the healthcare center. Importantly, in this paper we use the term ‘multidisciplinary care’ in its broadest sense and as an overarching umbrella term, namely to reflect every way of interaction and communication within a team of healthcare professionals providing PD care, including the interaction with the patient and care partner [25]. This means that ‘multidisciplinary care’ in this paper also includes models that could be labelled as ‘interdisciplinary care’ or ‘integrated care’.
Box 1
: Definitions used in this project.
METHODS
Inclusion of expert centers
A total of 17 internationally recognised centers in the field of multidisciplinary care in PD were invited to participate. These centers were chosen by the research team based on group consensus. Centers needed to have a multidisciplinary management program, they needed to be involved in scientific endeavors, and we took their geographical distribution into account. We organized a meeting with one leading neurologist of each center at The International Congress of Parkinson’s Disease and Movement Disorders (Vancouver, June 2017). A leading neurologist was defined as a person working at that center that was highly involved in the organization and execution of a PD multidisciplinary care model. Based on group consensus, three additional expert centers were invited. All participating neurologists and centers are listed in Supplementary Table 1. The practice-based guideline was developed in four phases (Fig. 1).
Fig.1
Development of the practice-based guideline.
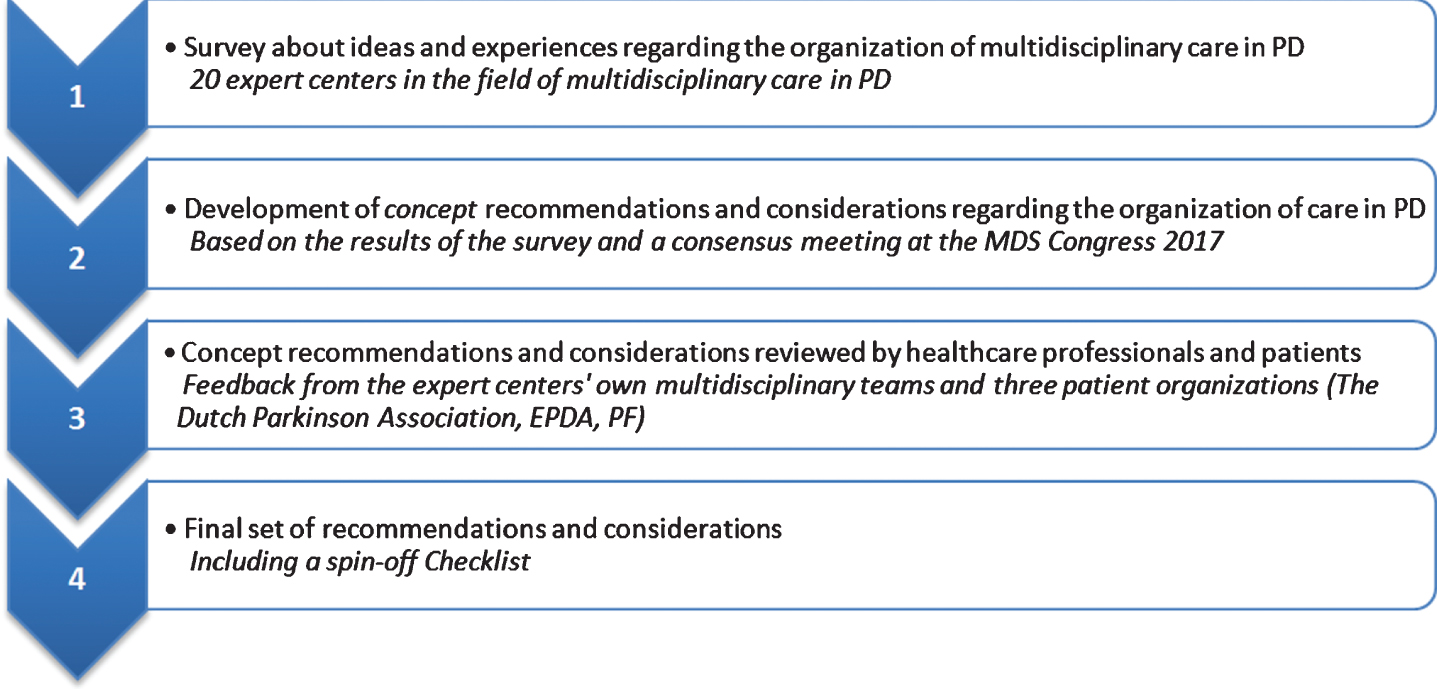
Phase 1: Survey
We developed an exploratory survey to collect ideas and experiences about how the expert centers currently organize their multidisciplinary care and how they would ideally wish to organize care. The survey consisted of 39 propositions and 12 open questions that were drafted based on pilot work, including interviews with six neurologists and one member of a patient organization, performed at a previous conference. Based on pre-formulated questions, these healthcare professionals spoke about their experiences with integrated care, about the differences with multidisciplinary care and about its strengths and possible weaknesses. The survey was organised around eight themes (Table 1). We asked the participating neurologists to rate the importance of each proposition on a scale from 1 (“not important at all”) to 10 (“most important”). Propositions did not have to be ranked, e.g., multiple propositions could be rated with a “10”.
Table 1
Themes addressed in the exploratory survey for neurologists
| Theme | |
| A | Elements for optimal multidisciplinary care |
| B | Members of the team |
| C | Role of the patient and care partner |
| D | Coordination of the team |
| E | Team meetings |
| F | Inpatient or outpatient care |
| G | Telehealth |
| H | Challenges and barriers towards multidisciplinary care |
Phase 2: Development of concept recommendations and considerations
Based on the survey results, we developed a concept set of recommendations and considerations by summing the scores of all propositions and ranking them according to degree of importance. Propositions receiving an average score of “8” or higher were considered a recommendation; propositions receiving an average score of “6” or “7” were considered a consideration; and propositions receiving an average score below 6 (so “5” or lower) were further discarded. During the consensus meeting, the concept recommendations and considerations were discussed with the participating neurologists. The aims included reaching general agreement and developing additional recommendations that were considered to be missing.
Phase 3: Review by multidisciplinary teams and patient organizations
The updated concept recommendations and considerations were then reviewed by the multidisciplinary teams of the participating centers. The teams discussed all recommendations in focus groups and reported their feedback using free text. These focus groups consisted of at least a neurologist and PD nurse. In addition, depending on the center, physiotherapists, speech- and language therapists, occupational therapists, psychologists, social workers and dieticians were included as well. To facilitate discussion, we sent a PowerPoint presentation including all recommendations and considerations to each center. Additionally, we prepared a feedback form where focus groups could indicate for each recommendation whether they did or did not agree, including room for extra comments. Finally, three patient organizations (Dutch Parkinson Association, European Parkinson’s Disease Association and Parkinson’s Foundation in the US) reviewed the recommendations as well using a specific format. They were asked to: (1) prioritize the five most important recommendations from the patient perspective; and (2) add any essential missing issues.
Phase 4: Final set of recommendations & considerations
Based on the feedback from Phase 3, the final set of recommendations and considerations was drafted. A checklist was created to facilitate their implementation into clinical practice, but the checklist was not further tested in practice (Supplementary Checklist).
RESULTS
The participating expert centers
All 20 invited centers participated. In the survey, the neurologists were asked why multidisciplinary care was considered important for persons with PD. The general consensus was: “PD is a complex, multidimensional condition with cognitive, psychological and social ramifications, as well as motor and non-motor signs. The clinical manifestations are only partially amenable to pharmacological or surgical treatment. This makes it impossible for one healthcare professional in any discipline to cover all complexities and diversities of symptoms and to deliver all management options.” With the term “healthcare professional”, we equally consider any of the healthcare professionals that are part of the multidisciplinary team, where specific expertises in healthcare delivery are paralleled by a comprehensive understanding of the abilities of other services and of the multidimensional requirements of patients.
Phase 1: Survey
The survey reached a 100% response rate. Seventeen propositions received an average score of “8” or higher and were considered recommendations. Fourteen propositions received an average score of “6” or “7” and were designated considerations. Eight propositions received a “5” or below and were discarded.
Phase 2: Development of concept recommendations and considerations
Based on the results of the survey, a set of 30 concept recommendations and 14 concept considerations was developed. The extra 13 recommendations (in addition to the 17 propositions receiving an average score of “8” or higher in the survey) were based on answers to open questions.
Phase 3: Review by multidisciplinary teams and patient organizations
The feedback from neurologists and their respective multidisciplinary teams reached a response rate of 80%. Based on their feedback, the concept recommendations and considerations were adjusted, which led to a total of 30 recommendations and 10 considerations.
Comparing the answers of the three patient organizations, they considered the following recommendations as most important:
• Care is organized in a patient-centered way, adopting patients’ and care partners’ goals of care, health and well-being.
• There is a core care team available for newly diagnosed PD patients (see Table 2 for the core team members). Members of the multidisciplinary team are available depending on individual patient needs and specific (crisis) situations.
• The patient’s care team has a team coordinator. The patient and all team members are aware of who this team coordinator is.
Table 2
Final set of recommendations and considerations. The recommendations and considerations per category are shown in random order
| Theme | Recommendations and considerations |
| A. Elements for optimal care | Recommendations |
| •There is mutual trust between team members and respect for diversity of professional roles and perspectives. | |
| •Team members believe in the benefits of multidisciplinary care and are motivated to provide it as a joint effort. | |
| •Parkinson’s disease (PD) care is broader than just for PD alone. All team members promote general health and well-being, as well as the prevention of other diseases. | |
| •There is a core care team# available for newly diagnosed PD patients. Team members are available depending on patient needs and specific situations. #Members of the team are described in section B | |
| •Follow-up consultations by neurologists are scheduled depending on patient needs and disease complexity, but at least once a year. For allied healthcare, the frequency depends on individual needs. | |
| •Patients do not have to be seen by a neurologist at every follow-up visit. Depending on their needs, they may be seen by a PD nurse specialist or another member of the core team. | |
| •Clinical care teams are transparent about which elements of good multidisciplinary care they offer. Consequently, patients know what to expect and the team knows what elements are missing and where there is room for improvement. | |
| •Healthcare providers working in nursing homes or on general hospital wards receive dedicated training in managing PD.* | |
| •Continuity of care is essential. This is defined as the first point of contact with the healthcare team, which is then harmonized by continuous communication with the other required healthcare providers.* | |
| Considerations | |
| •Care is non-hierarchical and all team members have a respected voice. The final treatment decision and liability depend on the specific problem(s) and the expertise of the disciplines involved. | |
| •All team members perform their job within their formally-defined scope of practice. They are aware of each other’s strengths to facilitate optimal collaboration and referral. | |
| B. Members of the team | Recommendations |
| •The following healthcare professionals are part of the core care team: the dietician, movement disorder neurologist, occupational therapist, Parkinson’s disease nurse specialist#, physiotherapist, psychiatrist or (neuro)psychologist, social worker and the speech and language therapist. #This may also be a nurse practitioner or registered nurse | |
| •The following healthcare professionals are available for referral: the gastroenterologist, geriatrician, neurosurgeon, nursing home physician, pain specialist (usually an anaesthesiologist) and the urologist. | |
| •Effective and efficient lines of communication between team members are essential to signal possible crises regarding patient care or context and divert them in due time. | |
| •The primary care physician has an essential role in the community, in making referrals to medical specialists and in the palliative stage of the disease. | |
| •All core team members are potentially important in all disease stages, but the contribution of each team member depends on patient needs. | |
| •All team members are flexible and have the capability to learn from each other, especially from persons with PD and their care partners.* | |
| Considerations | |
| •The following healthcare professionals can be considered for referral: the clinical geneticist, dentist, internist, neuro-ophthalmologist, pulmonologist, rehabilitation specialist and the sleep consultant. | |
| C. Role of patient and care partner | Recommendations |
| •The care partner is involved from the moment of diagnosis. | |
| •Patients and care partners are engaged in shared decision making to determine treatment approaches, i.e. by jointly prioritizing issues and problems for the treatment plan. | |
| •Care is organized in a patient-centred way, adopting patients’ and care partners’ goals of care, health and well-being. | |
| •Patients and care partners are aware of and have access to relevant and reliable educational resources to enable self-management, for example specific patient-related material. | |
| •Caregiver strain is evaluated and treated. | |
| •Patients and care partners evaluate the quality of perceived care. | |
| •Time constraint of professionals is an important limitation to allow for optimal patient participation. To improve this, sufficient consultation time is needed. | |
| Considerations | |
| •Patients and care partners are involved in their care, for example by inviting them to#: be involved in decision making about their treatment plan; (sometimes) participate in team meetings; participate in advisory boards for monitoring and developing care delivery; and/or complete questionnaires about care satisfaction and provide feedback regarding healthcare. #Examples to involve patients and care partners; this list is not exhaustive. | |
| D. Coordination of the team | Recommendations |
| •The patient’s care team has a team coordinator. The patient and team members are aware of who this is. | |
| •Care coordination is of critical importance in all disease stages. However, what it looks like varies per stage and depends on patient needs. | |
| Considerations | |
| •The team coordinator# is either the (specialized PD) nurse, or the most suitable person in the team regardless of their discipline (i.e. someone with leadership, communication and organizational skills). #The movement disorders centre determines the team coordinator assignments | |
| •Treatment related decisions are integrated into a shared treatment plan by the team coordinator. This is especially important for patients in the advanced stages. | |
| E. Team meetings | Recommendations |
| •The team gets together in face-to-face or virtual team meetings at least once a month. | |
| •Team meetings are used mainly for goal-setting in patient care, for education, to talk about organizational and communication issues and to discuss complicated patients. | |
| Considerations | |
| •During team meetings, team members discuss treatment plans and jointly make integrated group decisions, especially for patients in the advanced stages of the disease. | |
| •It is important to organize team meetings to promote team building. | |
| F. Inpatient or outpatient care | Recommendations |
| •An outpatient setting is the preferred setting to organize care for the majority of PD patients. | |
| •An inpatient setting is useful for more complicated patients with the need for frequent revision of the treatment plan, followed by consultations in the community to aid generalization. | |
| Considerations | |
| •Patients are referred to community healthcare professionals that are skilled in treating people with PD. There is at least annual follow-up in the clinical centre. | |
| •If necessary, e.g. due to regional unavailability or complex needs, patients are referred to healthcare professionals who practice within the clinical centre. | |
| G. Telehealth | Recommendations |
| •Telehealth has added value for care delivery, especially for patients living at a great distance from the clinic, patients with a job, and advanced patients who would otherwise be lost to follow-up. In addition, telehealth can support communication between healthcare disciplines. | |
| •Telehealth can be used by neurologists for follow-up consultations to enable video consultations and tele-rehabilitation, but not for establishing a diagnosis in new patients. For allied healthcare, the use of telehealth varies per discipline. |
*These recommendations were emphasized by the patient organizations.
The patient organizations emphasized that all recommendations were appropriate and important, but that they missed three key items. First, they considered it essential that healthcare providers working in nursing homes or general hospital wards receive dedicated training in managing PD. Second, they emphasized the importance of continuity of care. This was defined as the first point of contact with the healthcare team, which is then harmonized by continuous communication with the other required healthcare providers. Third, they highlighted that all team members should be flexible and have the capability to learn from each other, especially from persons with PD and their care partners.
Phase 4: Final set of recommendations and considerations
The final set of recommendations and considerations is shown in Table 2. The checklist including all recommendations and considerations can be found in the Supplementary Material. In the following sections, we elaborate further on the content of the final recommendations.
Elements for optimal multidisciplinary care
The expert centers were unanimous about the profound importance of mutual trust between team members and emphasized that respect for diversity of professional roles and perspectives is an essential element of good multidisciplinary practice. The need for team members to believe in the benefits of multidisciplinary care and their motivation to provide care as a joint effort was also considered important. Here, the need for good understanding of each other’s role in the team should be emphasized. For example, a neurologist can have a better understanding of the role of the occupational therapist in falls prevention when the therapist discusses his/her approach to addressing this specific problem in the team during case discussions. A better dissemination of this knowledge across disciplines, ensured through regular team case discussions, is an irreplaceable process that turns multidisciplinary care into more than just the sum of its components. Patients do not have to be seen by a neurologist at every follow-up visit, but, depending on their needs, may also be seen intermittently by, e.g., a PD nurse specialist. However, patients should be seen by the neurologist at least once a year, which may particularly be sufficient when there is an adequate multidisciplinary team in place that collaborates well. However, more complex patients may need to be seen more often.
Members of the team
All core clinical team members are described in Table 2. These core members are important in all disease stages (early, middle and late), but their exact contribution may vary by disease stage and may depend on individual patient needs. The primary care physician was generally not considered part of the core care team, but was felt to have an essential role in the community, e.g., in the palliative stage, for management of comorbidities and for first line interventions such as checking for infections with sudden changes in conditions. In addition, primary care physicians play an integral role in providing feedback after multidisciplinary assessments. Therefore, subsequent follow-ups should always be communicated to the primary care physician (this feedback can also assist in teaching primary care physicians about challenges related to PD). However, their role highly depended on the organization of healthcare in different countries. Importantly, healthcare centers should strive to develop relationships with the professionals recommended for frequent referral, and these physicians should develop an expertise in PD related issues within their area of specialization. On the other hand, the healthcare professionals that can be considered for referral may not need to develop an expertise in PD.
Role of patient and care partner
Here, we define “care partners” as non-professional caregivers close to the patient, such as the patient’s partner, family members and close friends. It is essential that care partners are involved in patient care from the moment of diagnosis. However, healthcare professionals should address the role of ‘care partner’ cautiously, especially in early disease stages where a role of ‘partner’ or ‘family member’ is more appropriate than a role of ‘caregiver’. When the patient does not have such a care partner, the healthcare team should try to identify a care partner or at least facilitate the conversation about the pivotal role of a care partner. In addition, patients and care partners should be engaged in shared decision making to reach personalized treatment approaches, but time constraint is an important limitation for optimal patient participation. Therefore, healthcare professionals should have sufficient consultation time for optimal delivery of patient-centered care. This concept can be aided by ‘expert patient groups’ or ‘patient and public involvement initiatives’ [26].
Coordination of the team
Care coordination is critically important in all disease stages. Each patient’s care team should therefore have a team coordinator. Importantly, all team members, as well as the patient, should be aware of who this team coordinator is. Ideally, the team coordinator is either the (specialized PD) nurse or else the most suitable person in the team, regardless of their healthcare discipline. This entails a person with demonstrable leadership, communication and organizational skills.
Multidisciplinary team meetings
The team should convene in regular face-to-face or virtual team meetings (preferably weekly, but at least once a month). Such meetings can focus both on patient care, including discussion of complex cases, and on education, e.g., by discussing recent guidelines or literature. Importantly, not every patient has to be reviewed by the team once a month. Furthermore, as mentioned in the section ‘elements for optimal multidisciplinary care’, team meetings are an essential tool to build cross-discipline understanding and cross-discipline education (e.g., of medical, surgical and rehabilitative interventions). This will make it easier for any team member to recognize an opportunity for improvement through a different discipline and initiate appropriate referrals. In addition, the distinct disciplines bring different perspectives to the table, thus providing a 360-degree view of each individual patient. Therefore, each team member may take the initiative to bring up a patient for team discussion.
Inpatient versus outpatient care
An outpatient setting is the preferred way to organize care for most persons with PD. However, an inpatient setting may be useful for more complicated patients who need frequent revision of their treatment plan or for patients that are treated with complex advanced therapies, such as deep brain stimulation or intestinal levodopa infusion. Examples of patients that may need frequent revision of their treatment plan include 1) patients with a type of advanced therapy, especially right before and after the start of these treatments; 2) patients in the advanced stage of disease who need frequent changes in their medication regime; 3) patients with PD complicated by depression, anxiety or another psychiatric disorder; and 4) patients with severe gait, balance and cognitive impairments. Such inpatient admissions should be followed by consultations in the community to facilitate implementation of the treatment advice. This can be complemented by community outreach programs that offer care provided by expert teams in the home of the patient. Additionally, close proximity of team members may improve their feeling of connectedness.
Telehealth and remote management
A total of 65% (13/20) of the included healthcare centers currently uses telehealth. They emphasized that telehealth has added value in care delivery, particularly for patients living at great distances from the clinic, for patients with a job and for advanced patients who would otherwise be lost to follow-up. Telehealth solutions are particularly useful for follow-up consultations, but they are not recommended for establishing a diagnosis in new patients. To deliver telehealth effectively, sufficient technical and nursing support should be in place. Many different technological solutions are available and none is specifically preferred, but each clinic should use one common platform to ensure continuity of care. However, future studies are needed to determine the optimal ratio between in-person encounters and telehealth consultations, which is also dependent on social and demographic factors [27].
Challenges and barriers towards multidisciplinary care
In the survey, the neurologists were asked to identify challenges and barriers in the delivery of multidisciplinary care. Lack of reimbursement was considered the greatest barrier, followed by lack of time and labour intensity. Lack of up-to-date guidelines and new scientific evidence about the delivery of multidisciplinary care were not considered major barriers.
DISCUSSION
We provide a set of recommendations and considerations for the organization of multidisciplinary clinical care teams for persons with PD and their care partners. These recommendations were developed based on practice-based evidence, by using experiences from 20 well-known expert centers with specific investments in multidisciplinary care in PD. These recommendations have not yet been tested against standard consultative care models. Importantly, we do not advocate that all recommendations should be implemented in each healthcare center, since the role of the team members that provide distinct care elements can vary between countries, and even between regions. Instead, the recommendations can be used as an indicator to verify which elements have already been implemented in a specific center and to identify unmet needs or missing services. Moreover, these recommendations provide a practical starting point to improve care in an optimal patient-centered way, tailored to the needs and local circumstances of each healthcare center. The use of transparency to display and publish which recommendations have been implemented can assist patients in identifying which elements of multidisciplinary care they can anticipate receiving from a specific center. Clinical care teams can also identify missing elements and prioritize which could be improved.
The importance of the recommendations is supported by the recent European Inventory performed by the European Parkinson’s Disease Association (EPDA) [28]. Based on interviews with persons with PD, their care partners and healthcare providers from 11 countries, the EPDA developed six recommendations to improve PD management and to offer health economic benefits for both persons with PD and for healthcare systems. Five of their recommendations somewhat mirror our recommendations. However, we have added an essential recommendation, which was also emphasized by the patient organizations, namely that the involved healthcare professionals should have sufficient knowledge and expertise to treat persons with PD. Indeed, recent work has shown that allied health professionals who received a dedicated training program to augment their PD-specific expertise achieved better outcomes, and with greater efficiency, than their peers, who had only received generic training and were sporadically involved in PD care [29]. Multiple organizations (e.g., the International Parkinson’s and Movement Disorders Society, the Parkinson’s Foundation, the Michael J. Fox Foundation, Parkinson’s UK and the Dutch ParkinsonNet) now offer dedicated training programs for, among others, medical specialists, nurses and allied health professionals. Our recommendations would support the notion that these initiatives should possibly be expanded.
Over the past years, multiple studies evaluating different organizational models of multidisciplinary care in PD have been published, with conflicting results. In a 2-month inpatient multidisciplinary program, motor impairment, balance, activities of daily living and quality of life improved, which was maintained one year after the intervention [17]. Furthermore, a 4-week inpatient multidisciplinary rehabilitation program also showed improvements in quality of life and motor function [18]. However, these inpatient programs were built over a long period of time and involved procedures that may be financially prohibitive and generally non-reimbursable in most healthcare systems, which limits the generalizability of the results. This is reflected by our recommendations, which indicate an outpatient setting as the preferred mode to organize care for most persons with PD. The IMPACT trial tested a different model of care, consisting of an individually tailored comprehensive assessment in an expert tertiary referral center with subsequent referrals sent to a regional network of allied health professionals specialized in PD [19]. The results showed only small benefits in disability and quality of life, which disappeared after correction for baseline disease severity. It is unknown why this occurred, but one possibility was that community professionals did not adequately follow up the advice of the expert center. In addition, in a 6-week multidisciplinary rehabilitation program, patients reported worse general and mental health, while caregivers had a trend towards more strain [30]. In contrast, a recent trial evaluating a 6-month integrated healthcare approach consisting of an individually tailored therapy plan and additional home visits by PD nurses showed improvement in quality of life, motor and non-motor symptoms compared to the control group [31].
These studies collectively emphasise the complexity in demonstrating the potential benefits of multidisciplinary care, which is aimed at the ultimate goal of delivering personalized care for persons with PD [32]. No strong recommendations can be drawn on how a multidisciplinary approach should be organized. Therefore, the International Parkinson and Movement Disorder Society has built a Task Force on ‘Management of Movement Disorders: Interdisciplinary and Integrated Care’ to further address this topic. Pending further evidence, we feel that care could be organized better according to the capabilities of each center within the circumstances of the national healthcare system and geared toward the needs of each individual patient.
The present project was not without shortcomings. First, our selection of centers was biased. These centers were mostly based in Western countries and there was underrepresentation of different cultures and countries. However, we aimed to define the recommendations in a broad way, so that they are flexible enough for PD specialists outside the Western world to adopt and customize for use within their cultural and political environment. Second, the initial survey in Phase 1 was completed by neurologists, which has the potential bias of producing one-sided results due to lack of involvement of other healthcare professionals. However, PD nurses and other (allied) health professionals were involved in the feedback of all multidisciplinary teams and provided essential additional comments in that phase. Third, the method used to define the recommendations and considerations was not based on unanimous consensus, but on the majority of opinions. This may be somewhat subjective and various score systems could have been used. However, we wanted to make sure that only the most valued recommendations were included. Finally, future randomized studies are needed to address whether these recommendations from expert centers invested in multidisciplinary care are superior to either standards of care or alternatively other approaches.
The recommendations presented here may serve as a practical tool for shaping multidisciplinary services. Importantly, the involved neurologists considered lack of reimbursement the greatest barrier toward delivery of optimal multidisciplinary care, followed by lack of time and labour intensity. These three concerns are reflections of the same construct: the current financial arrangements provide insufficient support for true multidisciplinary care, leaving it largely to the good will of motivated teams to squeeze optimal care into busy daily routines. This finding emphasises the need to gather more supportive and objective evidence for the cost-effectiveness of multidisciplinary care and to demonstrate that an upfront investment in an adequate team structure and in providing sufficient time to address complex problems would be offset by long-term cost savings. Such future studies should not only focus on quantitative outcomes (e.g., motor and non-motor symptoms), but also on qualitative outcomes such as Goal Attainment Scaling [33], where patients prioritize and evaluate personal goals of care, health and well-being. The Patient- Centered Questionnaire for PD (PCQ-PD) can be used to evaluate the level of patient-centeredness and the quality of care as perceived by patients and their care partners [34]. The information from this project has the potential to positively influence PD care delivery, but there remains a critical need to directly test and compare various PD care models. Supplemented with new evidence as it emerges, these practice-based recommendations should be included in updated guidelines on multidisciplinary care in PD.
CONFLICT OF INTEREST
The authors declare no competing interests.
ACKNOWLEDGMENTS
Prof. Bas Bloem and Dr. Marten Munneke were supported by a research grant from the Parkinson’s Foundation and the Gatsby Foundation. Drs. Danique Radder, Dr. Jorik Nonnekes, and Dr. Marlies van Nimwegen were supported by a research grant from AbbVie. Dr. Jori Fleisher was supported by a grant from the National Institutes of Neurological Disorders and Stroke (K23NS097615).
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-202078.
REFERENCES
[1] | Den Oudsten BL , Van Heck GL , De Vries J ((2007) ) Quality of life and related concepts in Parkinson’s disease: a systematic review. Mov Disord 2: , 1528–1537. |
[2] | Lees AJ , Hardy J , Revesz T ((2009) ) Parkinson’s disease. Lancet 373: , 2055–2066. |
[3] | LeWitt PA , Fahn S ((2016) ) Levodopa therapy for Parkinson disease: A look backward and forward. Neurology 86: (14 Suppl 1), S3–12. |
[4] | Pfeiffer RF ((2016) ) Non-motor symptoms in Parkinson’s disease. Parkinsonism Relat Disord 22: (Suppl 1), S119–122. |
[5] | Tomlinson CL , Patel S , Meek C , Clarke CE , Stowe R , Shah L , Sackley CM , Deane KH , Herd CP , Wheatley K , Ives N ((2012) ) Physiotherapy versus placebo or no intervention in Parkinson’s disease. Cochrane Database Syst Rev 7: , CD002817. |
[6] | Sturkenboom IH , Graff MJ , Hendriks JC , Veenhuizen Y , Munneke M , Bloem BR , Nijhuis-van der Sanden MW ; OTiP study group ((2014) ) Efficacy of occupational therapy for patients with Parkinson’s disease: a randomised controlled trial. Lancet Neurol 13: , 557–566. |
[7] | Herd CP , Tomlinson CL , Deane KH , Brady MC , Smith CH , Sackley CM , Clarke CE ((2012) ) Speech and language therapy versus placebo or no intervention for speech problems in Parkinson’s disease. Cochrane Database Syst Rev 8: , CD002812. |
[8] | Nijkrake MJ , Keus SH , Oostendorp RA , Overeem S , Mulleners W , Bloem BR , Munneke M ((2009) ) Allied health care in Parkinson’s disease: referral, consultation, and professional expertise. Mov Disord 24: , 282–286. |
[9] | Post B , van der Eijk M , Munneke M , Bloem BR ((2011) ) Multidisciplinary care for Parkinson’s disease: not if, but how!. Postgrad Med J 87: , 575–578. |
[10] | Qamar MA , Harington G , Trump S , Johnson J , Roberts F , Frost E ((2017) ) Multidisciplinary care in Parkinson’s disease. Int Rev Neurobiol 132: , 511–523. |
[11] | Bloem BR , van Laar T , Keus SH , de Beer H , Poot E , Buskens E , Aarden W , Munneke M , Centrale Werkgroep Multidisciplinaire richtlijn Parkinson 2006–2010 ((2010) ) Multidisciplinaire richtlijn voor de ziekte van Parkinson. van Zuiden Communications, Alphen aan de Rijn. |
[12] | |
[13] | Factor SA , Bennett A , Hohler AD , Wang D , Miyasaki JM ((2016) ) Quality improvement in neurology: Parkinson disease update quality measurement set: Executive summary. Neurology 86: , 2278–2283. |
[14] | van der Marck MA , Kalf JG , Sturkenboom IH , Nijkrake MJ , Munneke M , Bloem BR ((2009) ) Multidisciplinary care for patients with Parkinson’s disease. Parkinsonism Relat Disord 15: (Suppl 3), S219–223. |
[15] | van der Marck MA , Bloem BR ((2014) ) How to organize multispecialty care for patients with Parkinson’s disease. Parkinsonism Relat Disord 20: (Suppl 1), S167–173. |
[16] | Valentijn PP , Schepman SM , Opheij W , Bruijnzeels MA ((2013) ) Understanding integrated care: a comprehensive conceptual framework based on the integrative functions of primary care. Int J Integr Care 13: , e010. |
[17] | Monticone M , Ambrosini E , Laurini A , Rocca B , Foti C ((2015) ) In-patient multidisciplinary rehabilitation for Parkinson’s disease: A randomized controlled trial. Mov Disord 30: , 1050–1058. |
[18] | Ferrazzoli D , Ortelli P , Zivi I , Cian V , Urso E , Ghilardi MF , Maestri R , Frazzitta G ((2018) ) Efficacy of intensive multidisciplinary rehabilitation in Parkinson’s disease: a randomised controlled study. J Neurol Neurosurg Psychiatry 89: , 828–835. |
[19] | van der Marck MA , Munneke M , Mulleners W , Hoogerwaard EM , Borm GF , Overeem S , Bloem BR ; IMPACT study group ((2013) ) Integrated multidisciplinary care in Parkinson’s disease: a non-randomised, controlled trial (IMPACT). Lancet Neurol 12: , 947–956. |
[20] | Munneke M , Nijkrake MJ , Keus SH , Kwakkel G , Berendse HW , Roos RA , Borm GF , Adang EM , Overeem S , Bloem BR ; ParkinsonNet Trial Study Group ((2010) ) Efficacy of community-based physiotherapy networks for patients with Parkinson’s disease: a cluster-randomised trial. Lancet Neurol 9: , 46–54. |
[21] | Fleisher J , Barbosa W , Sweeney MM , Oyler SE , Lemen AC , Fazl A , Ko M , Meisel T , Friede N , Dacpano G , Gilbert RM , Di Rocco A , Chodosh J ((2018) ) Interdisciplinary home visits for individuals with advanced Parkinson’s disease and related disorders. J Am Geriatr Soc 66: , 1226–1232. |
[22] | Okun MS , Ramirez-Zamora A , Foote KD ((2018) ) Neuromedicine service and science hub model. JAMA Neurol 75: , 271–272. |
[23] | Dorsey ER , Venkataraman V , Grana MJ , Bull MT , George BP , Boyd CM , Beck CA , Rajan B , Seidmann A , Biglan KM ((2013) ) Randomized controlled clinical trial of “virtual house calls” for Parkinson disease. JAMA Neurol 70: , 565–570. |
[24] | Wilkinson JR , Spindler M , Wood SM , Marcus SC , Weintraub D , Morley JF , Stineman MG1 Duda JE ((2016) ) High patient satisfaction with telehealth in Parkinson disease: A randomized controlled study. Neurol Clin Pract 6: , 241–251. |
[25] | Boon H , Verhoef M , O’Hara D , Findlay B ((2004) ) From parallel practice to integrative health care: a conceptual framework. BMC Health Serv Res 4: , 15. |
[26] | Qamar MA , Rizos A , Stones L , Meachin C , Chaudhuri KR ((2016) ) Public and patient involvement (PPI) at King’s: community for research involvement and support for people with Parkinson’s (CRISP). ACNR 16: , 17–20. |
[27] | Dorsey ER , Vlaanderen FP , Engelen LJ , Kieburtz K , Zhu W , Biglan KM , Faber MJ , Bloem BR ((2016) ) Moving Parkinson care to the home. Mov Disord 31: , 1258–1262. |
[28] | |
[29] | Bloem BR , Munneke M ((2014) ) Revolutionising management of chronic disease: the ParkinsonNet approach. BMJ 348: , g1838. |
[30] | Wade DT , Gage H , Owen C , Trend P , Grossmith C , Kaye J ((2003) ) Multidisciplinary rehabilitation for people with Parkinson’s disease: a randomised controlled study. J Neurol Neurosurg Psychiatry 74: , 158–162. |
[31] | Eggers C , Dano R , Schill J , Fink GR , Hellmich M , Timmermann L ; CPN study group ((2018) ) Patient-centered integrated healthcare improves quality of life in Parkinson’s disease patients: a randomized controlled trial. J Neurol 265: , 764–773. |
[32] | Titova N , Chaudhuri KR ((2017) ) Personalized medicine and nonmotor symptoms in Parkinson’s disease. Int Rev Neurobiol 134: , 1257–1281. |
[33] | Kiresuk TJ , Sherman RE ((1968) ) Goal attainment scaling: A general method for evaluating comprehensive community mental health programs. Community Ment Health J 4: , 443–453. |
[34] | van der Eijk M , Faber MJ , Ummels I , Aarts JW , Munneke M , Bloem BR ((2012) ) Patient-centeredness in PD care: development and validation of a patient experience questionnaire. Parkinsonism Relat Disord 18: , 1011–1016. |


