
Assessing the Swallowing Function in Children with Spinal Muscular Atrophy: An Easily Accessible and Objective Multidimensional Approach
Abstract
Background:
Spinal muscular atrophy (SMA), a genetic neuromuscular disease caused by lack of survival of motor neuron (SMN) protein, is characterized by muscular atrophy and respiratory and bulbar dysfunction. While swallowing disorders are common, they remain poorly studied.
Objectives:
Our study aimed to explore 1) intraoral pressure measurements with the Iowa Oral Performance Instrument system and the reliability of a Swallowing Function Assessment Questionnaire (SFAQ) in healthy controls, and 2) evaluate their use as swallowing function biomarkers and the evolution of swallowing function over time in children with SMA.
Methods:
We recruited 53 healthy children and 27 SMA patients all treated with SMN gene modulator therapy. Participants completed the SFAQ and underwent at least one measurement of maximal oral pressures (lingual, labial, and masseter).
Results:
Mean oral normalized pressure index were lower (all sites p < 0.001) and mean SFAQ scores were higher (p < 0.001) in patients compared with healthy controls. Pressure evolution over 1 year in SMA patients for all three oral sites did not show significant differences. SFAQ scores correlated negatively with oral pressures at all three sites in patients.
Conclusions:
Both tools provided new insights on the oral and pharyngeal phase of swallowing in SMA patients. In SMA patients, muscle strength in certain crucial anatomical regions during swallowing is weaker than in healthy children.
Abbreviations
ALS | Amyotrophic Lateral Sclerosis |
HFMSE | Hammersmith Functional Motor Scale Expended |
IOPI | Iowa Oral Performance Instrument |
MANOVA | Multivariate Analysis Of Variance |
OPMD | Oculopharyngeal Muscular Dystrophy |
Pmax | pressure maximum |
SBMA | Spinal and Bulbar Muscular Atrophy |
SD | Standard Deviation |
SF | Swallowing Function |
SFAQ | Swallowing Function Assessment Questionnaire |
SMA | Spinal Muscular Atrophy |
SMN | Survival of Motor Neuron |
INTRODUCTION
Spinal muscular atrophy (SMA) is an autosomal recessive disease caused by a genetic mutation in the gene encoding the survival of motor neuron protein, SMN1. This protein is essential for motor neuron survival, its absence causing degeneration of motor neurons in the anterior horn of the spinal cord and brain stem. The consequences of this mutation are generalized muscle atrophy and progressive bulbar dysfunction [1, 2].
Several types of SMA (0 to 4) exist, which are defined by symptom onset age, highest motor function achieved without treatment, and age of death without treatment, type 0 defining the most severe form of the disease [1]. SMA is a rare disease. Approximately 50% of patients are type 1. SMA severity mostly depends on the number of SMN2 copies [2].
SMA affects a variety of different functions (swallowing, motor function, respiratory function ...), therefore SMA treatment requires a multidisciplinary symptomatic and pharmaceutical approach [3]. Since 2017, three approved SMN-enhancing medications positively impacted both patient survival and motor function. Two drugs, nusinersen (Spinraza®, Biogen) and risdiplam (Evrysdi®, Roche) modify the alternative splicing of SMN2 messenger ribonucleic acid, with an increased production of functional SMN protein via intrathecal or oral administration [3, 4]. The third one, Onasemnogene abeparvovec (Zolgensma®, Novartis) consists of a single intravenous gene therapy of an adeno-associated viral vector type 9 containing the SMN1 gene [6].
New SMA drug therapy introduction led to the appearance of new disease evolution trajectories (phenotypes) significantly differing from the disease’s natural history, thus blurring the boundaries between SMA traditional phenotypes. It is now more appropriate to define the clinical phenotype by the highest motor milestone achieved (non-sitter, sitter, or walker) and to rely on a combination of age of onset, age at treatment onset, and number of SMN2 gene copies rather than the traditional phenotypes [7].
The vital functions affected by SMA include swallowing, a complex process requiring the perfect coordination of six cranial and four cervical nerve pairs, as well as more than 30 muscle pairs, under the control of brainstem and cortical areas [8]. Studies revealed that SMA patients may experience difficulties during the different phases of swallowing: the oral phase, which includes difficulties in bringing food into the mouth and chewing, the pharyngeal phase, during which dysfunctional air way protection or residues in the epiglottic vallecula may occur [9–13], and the esophageal phase. A previous study reported that 36% of SMA patients experience feeding problems [9], which are more pronounced in SMA type 1 patients than in the other phenotypes of SMA [1, 14]. Studying feeding and swallowing in SMA patients is paramount, as these are among the most common causes of morbidity and mortality, possibly leading to malnutrition, discomfort, and an increased risk of aspiration pneumonia [9, 10]. Swallowing function (SF) can be studied via clinical and instrumental evaluations, by the means of fiberoptic endoscopic evaluation of swallowing and video fluoroscopic swallow study. Given their invasive nature, they should only be performed in complex situations [14]. More recently, the Iowa Oral Performance Instrument (IOPI) was validated as a noninvasive investigation tool in patients affected by oropharyngeal muscular dystrophy and is currently being used in patients with myotonic dystrophy (TREAT-CDM at the University of Virginia, USA; and GUP19002, grant given to vs from Telethon and the Italian Muscular Dystrophy Association) [15]. Trucco et al. (2023)’s study on patients with SMA type 2 and 3 shows that the assessment of tongue and lip strength via IOPI could well complement the other tests in both adults and children [16]. However, SF is still poorly investigated, with only scarce literature on this topic. Given the lack of growth charts and dietary guidelines specific to SMA patients [17], as well as their high complication risk and decreased quality of life, further investigations are recommended. In this exploratory study, we aimed to explore intraoral pressure measurements in both healthy and SMA children treated with gene modulator therapy, to assess SF evolution over time. In addition, we undertake to evaluate the reliability of a new swallowing questionnaire, the Swallowing Function Assessment Questionnaire (SFAQ), which has been adapted to facilitate its integration into clinical practice. Our objective is to determine the questionnaires’ reliability and its utility as a streamlined tool for assessing swallowing function in a clinical setting.
MATERIALS AND METHODS
Patients and Study Design
This prospective multicenter pilot study was conducted at two Belgian neuromuscular reference centers, including Hôpital Universitaire des Enfants Reine Fabiola in Brussels, and Universitair Ziekenhuis Gent. The study protocol was approved by the institutional Ethics Committee (HUDERF protocol P2022/191–B4062022000099) (UZ protocol P2022 / 252- B408679560085). After receiving an information leaflet, at least one parent of each child signed an informed consent form, as did the child provided he/she was old enough to understand its content. The measurements were performed between March 2021 and September 2022 on 27 SMA patients, aged 2.5 to 17 years old, with a confirmed genetic diagnosis of SMA, among whom nine were SMA type 1, 13 SMA type 2, and five SMA type 3, in addition to 53 healthy controls aged 3 to 16 years old.
All study patients were on treatment, either attending a scheduled consultation or being hospitalized for their nusinersen injection in the SMA group, while the control group was in the school setting. SMA type 1 patients were defined as those with early symptoms (before five months) who had failed to acquire independent sitting position before starting treatment SMA type 2 patients were defined as patients who had acquired sitting position before the age of two years but never walked alone, even after receiving a treatment that was administered to all of them after the age of two years. SMA type 3 patients were defined as patients who had acquired walking before treatment onset.
Experimental Protocol
The SFAQ and the IOPI system were performed on 27 SMA patients and a second IOPI measurement concerned 17 SMA (six SMA1, nine SMA2, and two SMA3) patients with an interval of one year. In the control group, the two tests were performed on 53 children. A second IOPI measurement was performed after 24 hours in 42 healthy children to assess the reproducibility of the measurements. The control of IOPI measurement was not carried out after 24 hours in the group of SMA patients because it was difficult in practice. The time to complete questionnaire and the measures (12 in total) was 15 minutes.
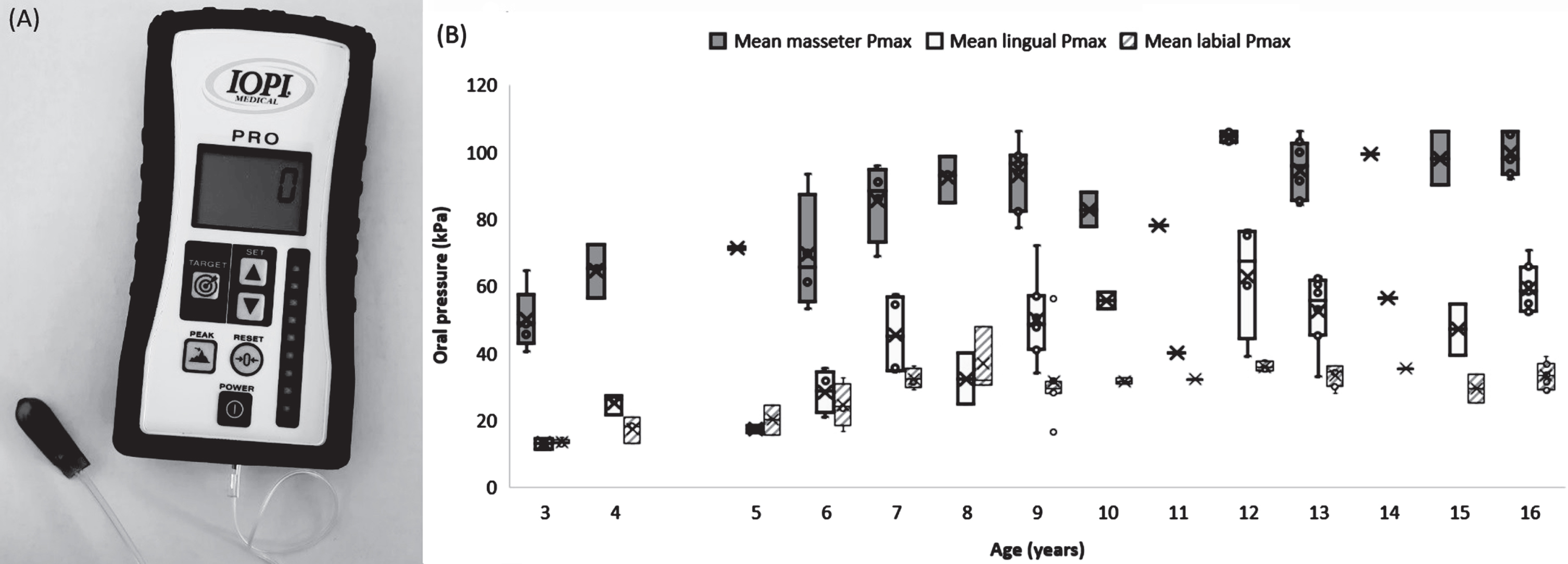
The IOPI system, as illustrated in Fig. 1 (A), provides an objective measurement of oral pressures that an individual can exert on an air-filled bulb. These pressures, measured in kiloPascal (kPa), were displayed on the screen of the device connected to the bulb. The maximum pressure (Pmax) measured by this bulb was 106kPa [19]. The device recorded the “peak” value, representing the maximum value achieved during the push. The IOPI had previously been validated in several scientific studies [20–22]. Additionally, we measured the oral Pmax values (lingual, labial, and masseter) of each child, placing the bulb between the tongue and anterior palate, between the lips on the midline, and between the posterior molars (right and left), respectively, while asking the participants to exert a Pmax on this bulb three times for each anatomical position, with the average of the three values taken as the reference for each patient and for each anatomical location.
Fig. 1
Iowa oral performance instrument (A) and boxplot representation of the maximal mean oral pressures (Pmax) as a function of age in the control group (n = 53) (B). Boxplot extremes represent the lowest and highest values of the sample. The lowest and highest part of the box represent the first and third quartiles, respectively. The crosses and bars represent the mean and median values of the samples. The age groups with only one patient are represented in the form of a “star” with 6 points.
We decided to create an index value enabling us to normalize the differences according to age group between healthy and SMA children by using the following formula:
(1)
Thus, an index < 1 means that the mean control Pmax value is higher than the SMA Pmax. An index > 1 means that the mean control Pmax value is lower than the SMA Pmax. The closer to 1, the more similar the mean control Pmax and SMA Pmax values.
The SFAQ (see Appendix) was constructed by combining two published questionnaires, namely the Swallowing Disturbance Questionnaire [18] and a questionnaire from a published article by Chen et al. (2012) [9]. The first questionnaire represents a sensitive and accurate tool for identifying patients suffering from swallowing disorders, while the second was designed to assess feeding and swallowing difficulties in SMA type 2–3 patients. Our questionnaire is a combination of these two well-known questionnaires, gathering about 80% of the questionnaire designed by Chen et al. (2012) [9] and all of the Swallowing Disturbance Questionnaire [18]. Chen’s questionnaire is specific to the SMA population, and we decided to add items with frequency elements as in the Swallowing Disturbance questionnaire. The latter was initially intended for Parkinson’s disease patients but can be used in patients with other neurological impairments. All the questions were translated in French and rephrased to be asked to the caregiver. Then, we discussed the consistency of the translation with speech therapists from our team. Of note, in most patients of our study, the questions were asked in French by a speech therapist or one of the two medical doctors (Dr. Colot and Dr. Benmechri) leading the study to the parents. Our new questionnaire is still exploratory and has never been used before.
The resulting SFAQ questionnaire consisted of 21 questions: eight assessing the oral phase and 13 others the pharyngeal phase, with 18 questions scored on a four-point scale (0 to 3), along with three yes/no questions. For these latter, “yes” was scored as 2.5 and “no” as 0.5. The minimum score obtained was 1.5, and the maximum 61.5. The higher the score, the worse the swallowing. During each interview, each parent with their child next to them was invited to answer the SFAQ, resulting in a swallowing score for each participant. We divided our patients into three categories based on the SFAQ: mild impairment if the patient had a score≤20, moderate impairment if the score obtained was between 20 and 40, and severe if the score obtained was > 40. We compared the sub-questions for the three groups qualitatively. Severity was based on frequency, that is on the frequency (defined by the number of times per week) of the occurrence of an event.
In order to correlate swallowing function with gross motor function, SMA patients underwent the Hammersmith Functional Motor Scale Expended (HFMSE). The HFMSE is a validated tool allowing for global motor skill assessment in SMA adults and children. The scale was performed annually by a trained physiotherapist during the patient’s follow-up and was often used during clinical trials to evaluate the drug’s effect on SMA patients’ global motor skills. This scale assesses physical abilities and is based on 33 items rated on a scale ranging from 0 to 2 [23].
Statistical analysis
Descriptive statistics
Continuous variables were described using the mean and the standard deviation (SD) when following a normal distribution, or the median and the interquartile range in the opposite case. Categorical variables were reported using counts and percentages.
In addition, the oral Pmax was estimated three times for each anatomical region. A mean of these estimations was computed for each region respectively.
To correct for multiple comparisons, the Sidak method was used, a p-value < 0.007 was considered statistically significant (i.e., p < 0.05/7, with 7 the number of comparisons).
Participants were considered “outliers” when they deviated from their group by more than three absolute deviations from the median for each measurement [24]. Such outliers were removed from the analyses. Analyses were performed using the Jamovi© software (The Jamovi Project, 2022) [25] and R studio (version 4.2.2).
Analysis of the SFAQ and oral pressure in healthy children
The association between the SFAQ score and gender and age were tested with a Mann-Whitney-U test, Welch test as appropriate, and a Spearman correlation test (due to non-normality of the distribution), respectively.
A multivariate analysis of variance (MANOVA) was performed on the control population to assess the impact of independent variables like age and gender on the mean oral Pmax values for the three regions.
Finally, an intra-class correlation analysis was performed to test the stability of the mean oral Pmax estimations 24 hours after the first measure in 42 healthy children.
Comparison of the SFAQ and the oral Pmax between the healthy children and the SMA group
The SFAQ scores were compared between the two groups using the Welch’s t-test due to heterogeneity of the variances between the groups.
The mean oral Pmax was compared between healthy and SMA children for each anatomical region. Student’s paired t-test was used to compare the groups (or Wilcoxon signed-rank tests when appropriate). SMA patients and healthy controls were paired based on the age which is a statistical predictor of the Pmax value.
Analysis of the SFAQ and the oral pressure in SMA patients
The SFAQ score was analyzed through different sub-groups in SMA patients. Primarily, the score was analyzed among the three types of SMA. Secondly, it was analyzed according to the highest motor milestone achieved (non-sitter, sitter, or walker). Subsequently, the difference in SFAQ score between two types of treatment (nusinersen and risdiplam) was evaluated with the Welch’s t-test due to heterogeneity of the variance between the groups.
The oral Pmax was studied through the Pmax index. The descriptive analyses were performed according to the different categorizations of SMA patients, for each anatomical region. In addition, the difference between the Pmax indexes was studied in the two treatment groups with a Wilcoxon rank sum test.
Finally, the study focused on tracking the progression of SFAQ scores and mean oral Pmax indexes over a 1-year interval within the SMA patient cohort. The signed-rank Wilcoxon test was used for the SFAQ score due to non-normality of the distribution.
Correlation between the SFAQ score, the Oral Pmax, and the HFMSE scores in SMA patients
Our aim was to establish the degree of association between the global motor skills (as assessed by the HFMSE score) and the specific swallowing performance of the child (as assessed by the SFAQ score). The analyses were performed using a Pearson test or Spearman test when appropriate. Subsequently, the link between the HFMSE and the Pmax index in the three anatomical regions was analyzed with a Pearson test (or Spearman test when appropriate). Finally, we examined the connection between the SFAQ score and the Pmax index in each region.
RESULTS
Demographic characteristics of the population
A total of 80 children were included in the analyses, comprising 27 SMA and 53 healthy control participants, ranging in age from 2 to 16 years old.
In the SMA group, we observed nine patients with SMA type 1, 13 patients with SMA type 2, and five patients with SMA type 3. In the SMA type 1 group, two patients received pre-symptomatic treatment either with onasemnogene abeparvovec or with nusinersen and achieved the ability to walk. The majority of the patients in the group had two SMN2 copies and the others had three SMN2 copies.
Children in the SMA type 2 group all had three SMN2 copies except for one patient who had a point mutation in SMN1 (heterozygous deletion) and one copy of the SMN2 gene.
Also, children in the SMA type 3 group had three SMN2 copies or more.
The SMA sample was also divided according to their best global motor skills / acquired milestone at first evaluation: walker (n = 5), sitter (n = 15), and non-sitter (n = 7). This classification seems more accurate since the arrival of new therapeutics, which changed the natural evolution of this disease.
Notably, the body mass indexes (BMIs) of SMA type 3 patients were relatively high compared to healthy children (SMA type 3 patients: 25.45±7.96 kg/m2 vs healthy children: 18.46± 4.58 kg/m2).
Finally, 30% of the children in the SMA group were receiving non-invasive respiratory support and 15% were fed via gastrostomy.
In the control group, children were in a school setting and had no comorbidities. The demographic characteristics of the SMA and control groups are presented in Table 1.
Table 1
Characteristics of the control and SMA groups. Age is presented as median (IQR) and BMI as mean± standard deviation. BMI, body mass index
| Control | Spinal Muscular Atrophy (SMA) | ||||
| SMA 1 | SMA 2 | SMA 3 | Total | ||
| Number | 53 | 9 | 13 | 5 | 27 |
| Age (years old) | 9 (7) | 4 (3) | 9 (4) | 15 (3) | 9 (7) |
| Gender (male) | 33 | 2 | 8 | 3 | 13 |
| BMI (kg/m2) | 18.46±.58 | 14.69±.59 | 16.42±86 | 25.45±.96 | 19.46±.18 |
| Treatment | |||||
| Nusinersen | / | 5 | 6 | 3 | 14 |
| Risdiplam | / | 3 | 7 | 2 | 12 |
| Onasemnogene abeparvovec | / | 1 | 0 | 0 | 1 |
| Feeding | |||||
| Oral | 53 | 4 | 10 | 5 | 19 |
| Gastrostomy | 0 | 4 | 0 | 0 | 4 |
| Unknown | 0 | 1 | 3 | 0 | 4 |
Analysis of the SFAQ and oral pressure in healthy children
The SFAQ scores was not associated with age or gender in the control group.
On the other hand, oral Pmax values increased with age, reaching a stabilized value among individuals aged 9–10 years (refer to Fig. 1 (B)). Age had a significant impact on oral Pmax values (p < 0.05), with p < 0.001 observed for lingual, labial, and masseter Pmax values in the healthy children group (lingual: F(1.47) = 9.438, p < 0.001; labial: F(1.47) = 4.091, p < 0.001; masseter: F(1.47) = 10.762, p < 0.001).
The intraclass correlation coefficient was calculated for the 53 control participants in the three zones, the concordance was significantly very high (Masseter: ICC (1) = 0.97, Lingual: ICC (1) = 0.994, and Labial: ICC (1) = 0.982).
Comparison of the SFAQ and the oral Pmax between healthy children and the SMA group
The Welch’s t-test indicated a significant difference in SFAQ score between healthy children and the SMA group. The statistic was equal to –3.455 (df = 18.221) with an associated p-value of 0.003. The SFAQ score was significantly higher in the SMA group with more variability observed between the scores (median = 9.0; IQR = 21.00) compared with the healthy group (median = 1.5, IQR = 2.0). Notably, this difference was enhanced in SMA type 1 children who had the highest scores. In the analysis, the children were not matched for age and gender, as these parameters did not impact the scores in healthy children.
The mean oral Pmax were significantly higher for healthy children compared with SMA children in each anatomical region (all p-values = < 0.003) (Table 2), showing reduced oral pressures in patients with SMA (refer to Table 3 for a descriptive summary detailing the mean oral Pmax among SMA patients and healthy children based on age groups and medication status).
Table 2
SFAQ score and mean maximal oral pressures expressed as mean± SD in the control (n = 53) and SMA groups (n = 25). Age: A (years), SFAQ: Swallowing function assessment questionnaire
| Control | Spinal Muscular Atrophy (SMA) | ||||
| SMA 1 | SMA 2 | SMA 3 | Total | ||
| n = 53 | n = 6 | n = 9 | n = 5 | n = 20 | |
| SFAQ score | A: 3–16 | A: 3.5–9 | A: 6.5–16.5 | A: 6.5–16.5 | A: 3.5–16.5 |
| 2.89±2.18 | 31.08±20.90 | 9.94±9.92 | 7.62±3.99 | 16.13±16.16 | |
| Lingual Pmax (kPa) | n = 50 | n = 7 | n = 13 | n = 5 | n = 25 |
| 44.3±16.5 | 10.75±8.14 | 28.41±10.67 | 40.80±14.32 | 27.12±14.68 | |
| Labial Pmax (kPa) | n = 53 | n = 7 | n = 11 | n = 5 | n = 23 |
| 29.2±8.94 | 7.90±5.64 | 24±12.67 | 22.40±6.35 | 20.53±11.94 | |
| Masseter Pmax (kPa) | n = 53 | n = 7 | n = 11 | n = 5 | n = 23 |
| 85.9±17.8 | 31.88±20.80 | 67.96±20.47 | 92.56±11.37 | 60.68±31.54 | |
Table 3
Individual oral Pmax indexes. SMA: spinal muscular atrophy
| Age (years) | Pmax index | |||
| Lingual | Labial | Masseter | ||
| SMA1 (n = 9) | ||||
| Nusinersen | 3 | / | 0.57 | 0.55 |
| 4 | 0.03 | 0.19 | 0.47 | |
| 4.9 | 0.36 | 0.29 | 0.29 | |
| 6.1 | 0.27 | 0.37 | 0.35 | |
| 7.2 | 0.33 | 0.54 | 0.33 | |
| 3.5 | 0.98 | 0.99 | 0.38 | |
| 3.5 | 0.47 | / | / | |
| Risdiplam | 14.3 | 0.47 | / | / |
| Onasemnogene abeparvovec | 2.5 | / | 0.99 | 0.52 |
| SMA2 (n = 13) | ||||
| Nusinersen | 8.8 | 0.65 | 1.39 | 0.83 |
| 8.8 | 0.58 | 0.12 | 0.73 | |
| 9.4 | 0.58 | 0.56 | 0.79 | |
| 12 | 0.43 | 0.75 | 0.46 | |
| 12.5 | 0.39 | / | / | |
| 16.8 | 0.16 | 0.11 | 0.27 | |
| Risdiplam | 6.7 | 1 | 1.40 | 0.88 |
| 7.3 | 0.94 | 0.87 | 1.03 | |
| 7.7 | 0.57 | 0.63 | 0.57 | |
| 9.8 | 0.37 | 0.59 | 0.98 | |
| 12 | 0.49 | 1.16 | 0.83 | |
| 16.1 | 0.62 | / | / | |
| 16.4 | 0.86 | 0.88 | 0.98 | |
| SMA3 (n = 5) | ||||
| Nusinersen | 6.5 | 0.98 | 0.72 | 1.12 |
| 12.2 | 0.63 | 0.63 | 0.93 | |
| 16.7 | 0.78 | 0.90 | 1.04 | |
| Risdiplam | 15.1 | 1.33 | 0.72 | 0.81 |
| 15.5 | 0.37 | 0.88 | 1.03 | |
For the labial region, the median score was 31.33 in the healthy group compared to 17.67 in the SMA group (U = 937.5, p < 0.001), in the lingual region, the median was 49.50 in healthy children and 26.20 in SMA children (t = 4.75, df = 68, p < 0.001). The biggest difference was observed in the masseteric region, where the difference between the medians was 29.01 (Welch test 4.19, df = 30.14, p < 0.001).
Analysis of the SFAQ and the oral pressure in SMA patients
We thoroughly analyzed the questionnaires of 20 SMA patients (SMA 1 n = 6, SMA 2 n = 9, and SMA3 n = 5), which were aged 3.5 to 16.5 years (Fig. 2). In greater details, we analyzed the average scores for each question in three groups: SMA type 1, SMA type 2, and SMA type 3 (except for question 5, 17, and 21, which have binary ‘yes/no’ answers)
Fig. 2
Scores average obtained for the different questions of the SFAQ according to the type of SMA with standard deviation (SD) in table. SFAQ: swallowing function assessment questionnaire, SMA: spinal muscular atrophy.
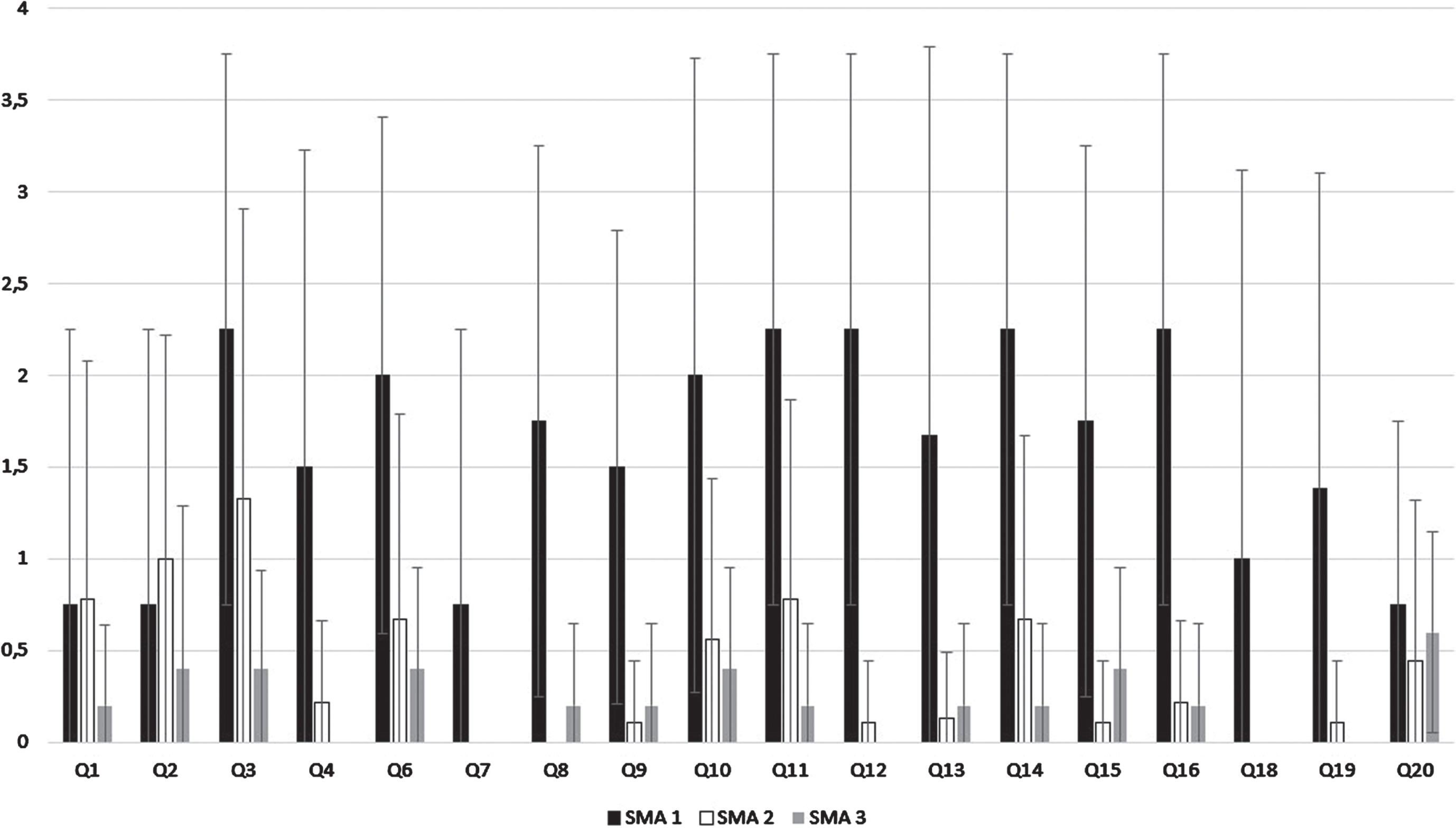
The majority of SMA type 2 (78%) and all SMA type 3 patients (walkers and no walkers) had a mild swallowing impairment (total SFAQ score≤20) the maximum average score for any single question never exceeded 1. In the SMA type 1 group, the severity of swallowing impairment ranged from moderate (>20 and≤40) to severe (>40). Except for question 2, the average scores for each question were consistently higher in the SMA type 1 group compared to the SMA type 2–3 group. This suggests more pronounced swallowing impairment in various aspects within the SMA type 1 group. Question 2 assesses the difficulty of bringing food into the mouth, reflecting more on gross motor function than the swallowing function. Certain questions (1, 2, 7, 10, 19, and 20) were rarely scored as more than mild in the SMA type 1 group. Notably, the average scores for questions 1 and 2 did not differ significantly between the two groups.
Within the “sitting” group, most patients (75%) had a mild impairment, but one patient (SMA type 1) has a severe swallowing impairment. In the “non-sitting” group, impairment was scored as mild (n = 1), moderate (n = 2) and severe (n = 1) (Table 4). Therefore, the highest SFAQ scores were found among SMA patients with SMA type 1 (median = 33.5, IQR = 26.5). Furthermore, within the non-sitter group, the median SFAQ score was 28.5 (IQR = 11.3), notably surpassing both the sitter group (median = 9.0, IQR = 15.3) and the walker group (median = 6.0, IQR = 3.9).
Table 4
Severity of the impairment of SFAQ, measured by the overall score qualified as “mildly” impaired, “moderately” impaired, or “severely” impaired, according to the global motor function (most recent record, A) and according to the type of SMA (B). SMA: spinal muscular atrophy. SFAQ: swallowing function assessment questionnaire
| A | Mild impairment (n) | Moderate impairment (n) | Severe impairment (n) |
| Walker (n = 4) | 4 | 0 | 0 |
| Sitter (n = 13) | 10 | 2 | 1 |
| Non sitter (n = 4) | 1 | 2 | 1 |
| B | Mild impairment (n) | Moderate impairment (n) | Severe impairment (n) |
| SMA 3 (n = 5) | 5 | 0 | 0 |
| SMA 2 (n = 10) | 8 | 2 | 0 |
| SMA 1 (n = 6) | 2 | 2 | 2 |
Regarding the treatment, the Welch’s t-test analysis revealed a non-statistically significant at the alpha level of 0.007, difference between the two treatments, indicating higher SFAQ scores associated with the nusinersen treatment(t = 2.522, df = 12.97, p = 0.026). Onasemnogene abeparvovec was not analyzed because only one patient received this treatment. The Pmax index was analyzed according to the SMA type (Fig. 3) and the highest motor milestone achieved, in the different oral anatomical regions.
Fig. 3
Oral anatomical sites Pmax indexes according to SMA type (A) and treatment (B). SMA: spinal muscular atrophy. Of note, the onasemnogen abeparvovec data are not shown because only one patient received this treatment. The dashed orange line represents an index of 1.
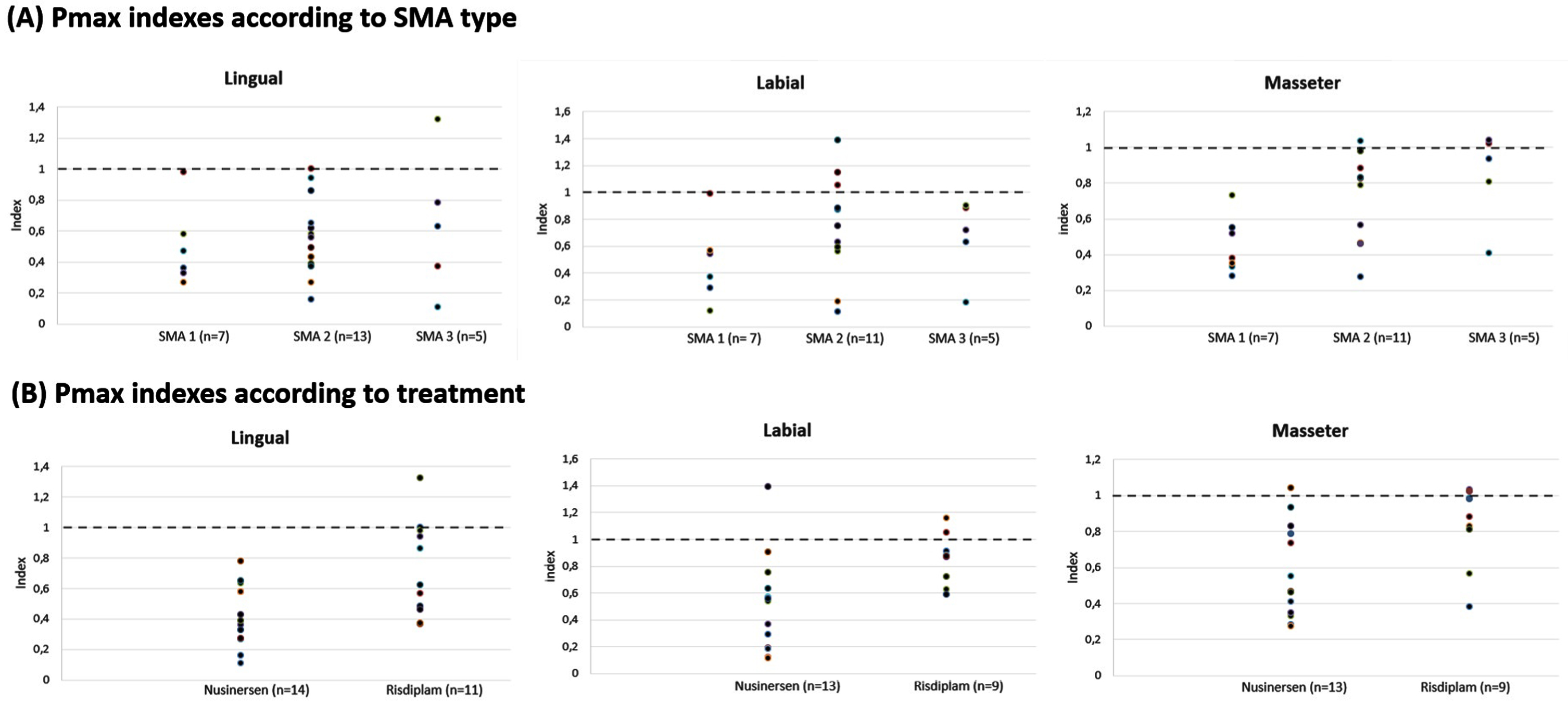
The results emphasized a globally higher Pmax index in SMA type 3 patients followed by SMA type 2 and SMA type 1 patients. In addition, non-sitter exhibited the lowest Pmax indexes (Table 5). Finally, patients treated with nusinersen presented a lower oral pressure index compared with those treated with risdiplam.
Table 5
Median values and interquartile interval of the mean oral Pmax indices in SMA patients. SMA: spinal muscular atrophy
| Anatomical region | Type 1 (n = 9) | Type 2 (n = 13) | Type 3 (n = 5) | Total (n = 27) |
| Lingual | 0.4 (0.2) | 0.6 (0.2) | 0.8 (0.4) | 0.6 (0.4) |
| Missing | 2 | 0 | 0 | 2 |
| Labial | 0.5 (0.4) | 0.8 (0.4) | 0.7 (0.2) | 0.7 (0.3) |
| Missing | 2 | 2 | 0 | 4 |
| Masseter | 0.4 (0.2) | 0.8 (0.3) | 1.0 (0.1) | 0.8 (0.5) |
| Missing | 2 | 2 | 0 | 4 |
| Non-sitter | Sitter | Walker | ||
| Lingual | 0.4 (0.2) | 0.6 (0.5) | 0.8 (0.2) | 0.6 (0.4) |
| Missing | 0 | 0 | 2 | 2 |
| Labial | 0.3 (0.3) | 0.8 (0.3) | 0.7 (0.3) | 0.7 (0.3) |
| Missing | 2 | 2 | 0 | 4 |
| Masseter | 0.5 (0.1) | 0.8 (0.5) | 0.9 (0.5) | 0.8 (0.5) |
| Missing | 2 | 2 | 0 | 4 |
Except for a trend on the masseteric location, no correlations were found between age at treatment initiation and Pmax indexes.
Finally, regarding the evolution over time, we observed no significant difference between the SFAQ scores at a 1-year interval (n1 = 19, n2 = 13, p = 13.5, p = 0.168. Similarly, no statistical difference was found between the Pmax index taken at a 1-year interval for each anatomical region, showing consistency between the assessments and performances.
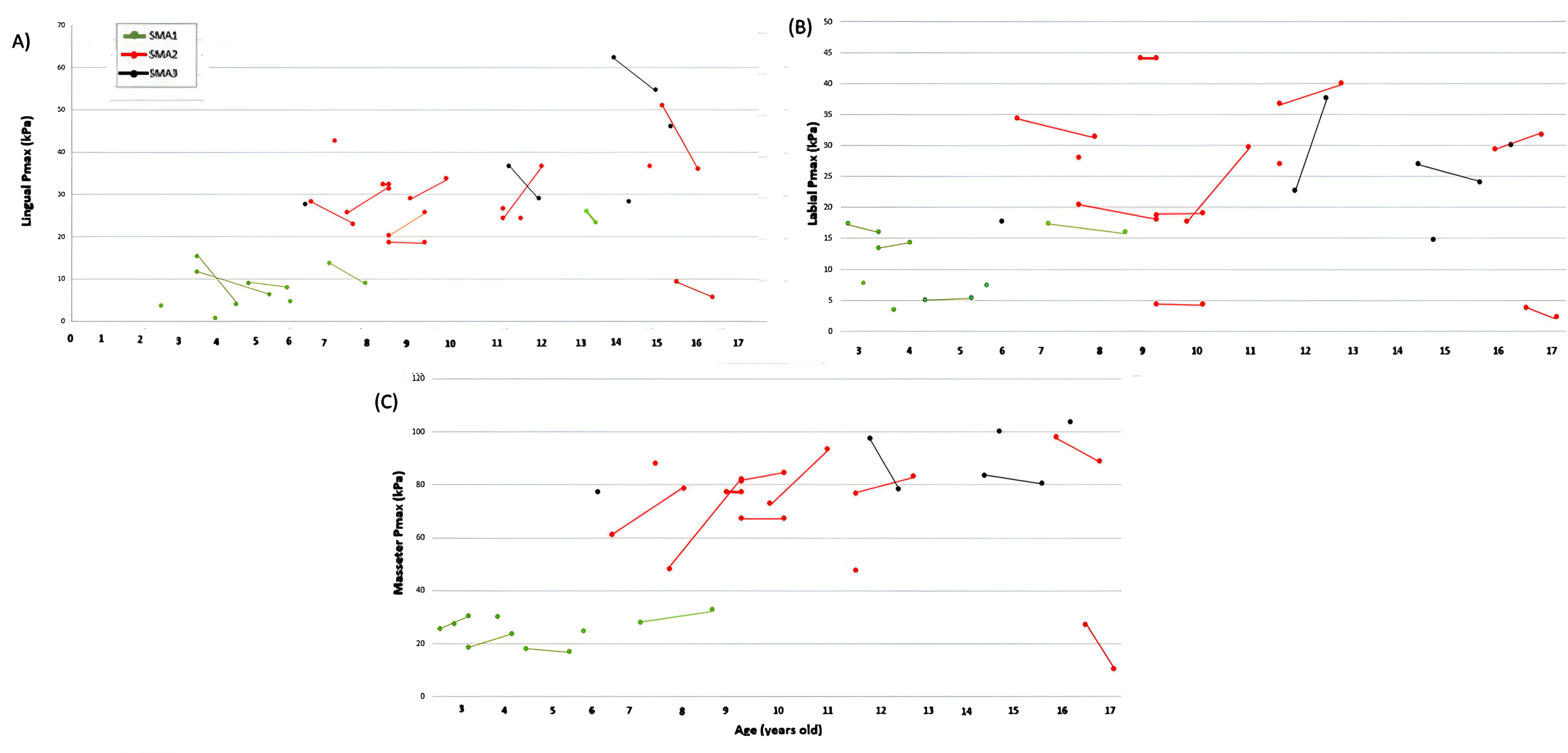
Pmax values, measured in 13 SMA patients, tended to either increase or stabilize between the first and second measurements one year apart for the different oral anatomical sites, excepting a slight decrease in lingual Pmax for SMA type 2 patients and in masseter Pmax for SMA type 3 patients, without statistically significant differences between the first and second measurements (Fig. 4).
Fig. 4
Evolution of individual lingual (A), labial (B), and masseter (C) Pmax values at a 1-year interval according to SMA type (n = 17). SMA: spinal muscular atrophy.
Correlation between the SFAQ score, the Oral Pmax, and the HFMSE scores in SMA patients
Correlation analyses revealed that low SFAQ scores correlated with high Pmax indexes (lingual: Spearman’s ρ= –0.852, p < 0.001; labial: Spearman’s ρ= –0.699, p < 0.001; masseter: Spearman’s ρ= –0.555, p < 0.017). Considering correlation analyses with the HFMSE score, no significant correlations were found with the lingual, labial, masseter regions and the Pmax index. However, a higher HFMSE score tended to be correlated with a lower SFAQ (Spearman’s ρ= –0.587, p = 0.027).
Discussion
In this prospective pilot study, we were able to confirm that the IOPI pressure measurement system, by means of retest-reliability can be easily applied in an outpatient setting involving either healthy children or SMA patients. Based on our initial results, SMA patients displayed significantly lower labial, lingual, and masseter pressures compared with age matched healthy controls, the impairment becoming more severe along the SMA spectrum (SMA type 1 > SMA type 2 >SMA type 3).
The required duration to perform these two tests was quite short, generally around 15 minutes, making them highly suitable for patient follow-up. Moreover, despite the limited number of children recruited at this stage, these two tests enabled us to obtain fairly reproducible results, not only within a population of healthy control children aged three to sixteen years old, but also within our SMA population. Indeed, our results obtained in healthy controls were quite close to those described in the literature [20]. In other published articles using the IOPI, the authors preferred to consider the maximum value, but we advocate considering the average of several measurements to mitigate the impact of variability, specifically within this pediatric study population.
In the control group, oral Pmax values increased with age, reaching a plateau around 9–10 years old, which can be by the fact that orofacial musculature, neurological maturation, and the resulting voluntary orofacial praxis develop progressively with age [26]. After the age of two, SF changes as the child develops and the aerodigestive tract moves toward a swallowing pattern that, by the age of ten, approaches that of an adult, developing only marginally more during teenage years [14].
The IOPI assesses the voluntary phases of swallowing, and the device is quite easy to use in children, except for very young patients under 4 years of age, in whom we experienced difficulties in understanding the bulb positioning and the way to apply pressure on it. This might be due to the fact that the ability to perform voluntary orofacial movements progresses with age, and that the performance of younger children is improved when the instructions are rather shown by imitation than verbally [26, 27]. Lingual pressure and IOPI had previously been studied in the context of several neurological conditions. With dysphagia being the main feature of Oculopharyngeal Muscular Dystrophy (OPMD), tongue strength measured by the IOPI was shown to reduce with a mean of 10 % over a 20 months period. Indeed, the tongue muscle is the most affected oropharyngeal muscle in patients with OPMD as shown with MRI measures. Moreover, tongue strength is easy to measure with commercially available handheld devices [15]. For instance, tongue muscle strength was likely decreased in patients with spinal and bulbar muscular atrophy (SBMA), prior to dysphagia awareness, suggesting that lingual pressure measurement could be a novel biomarker for detecting swallowing disorder in SBMA patients at an early stage [28].
Based on the oral Pmax obtained in SMA patients, and by comparing these values with those obtained in control children, we demonstrated that SMA patients displayed a decrease in the force exerted by the orofacial musculature across the three anatomical regions explored: the tongue, lips, and masseters. This is perfectly in line with the results observed in the literature showing that chewing difficulties, along with decreased tongue movements and food residues persisting within in the oral cavity are very common problems encountered by SMA type 1 and 2 patients during oral feeding [9–11]. The mean Pmax measurements revealed a lower masseteric and lingual mean Pmax in the SMA type 1 group compared with the SMA type 2 group. The max pressure index thus likely reflects the known severity in the different SMA subgroups. It is also in line with Trucco et al. (2023)’s recent publication indicating that tongue strength was below normative data in 47% of patients in a children cohort of SMA type 2–3 patients [16].
One of the particularities of our study was that the evaluated patients had been receiving SMN gene modulator therapy for 1 to 6 years, and one patient was even treated with gene therapy. Although we did not have oral IOPI measurements prior to treatment initiation, we performed exploratory analyses to investigate whether the Pmax indexes of SMA patients obtained during the first measurements correlated with several factors, including treatment received and time between first symptom onset and treatment initiation.
Although the groups were small, our analysis suggests that there was a difference between the two treatment groups (nusinersen and risdiplam) and the three tested anatomical regions. It is worth noticing that the nusinersen group included a greater number of SMA type 1 patients, namely five (62.5 %) versus three for the risdiplam (37.5 %) group.
Except for a trend on the masseteric location, no correlations were found between age at treatment initiation and Pmax indexes. Although the number of SMA patients included in the cohort was limited, this observation contrasts with several previous studies showing beneficial effects on global motor skills and survival when the treatment is started quickly after symptoms onset or even before their onset [29–32].
In contrast to healthy controls, pressure measurements in SMA children over a 1-year interval did not significantly differ, which may suggest a stabilizing effect of the SMN gene modulator therapies, although the natural evolution of oral muscle strength in untreated SMA patients is unknown.
The swallowing questionnaire, developed as a pilot to complete the pressure measurements with elements of anamnesis about swallowing allowed us to distinguish healthy controls from SMA patients, especially SMA type 1 and type 2 cases.
Regarding the sub-analysis of the SFAQ questions, the severity scores were higher in the SMA type 1 group for all questions, with the exception of question 1 and 2. In the first question, the patients’ opening limitation is examined, and in the second, the frequency of difficulties reaching the hand to the mouth is evaluated. The responses did not differ between the two groups because the frequency was probably difficult to define. These two questions would be best described by the intensity rather than by the frequency of these complaints. Other studies on swallowing in SMA patients used objective mouth opening measure and did not focus on frequency [16]. Thus, we should consider removing these two questions from the SFAQ in the future.
Despite a great score variability in SMA type 1 patients, the most severely scored items mainly concerned the pharyngeal phase, with greater severity and frequency (>50%) than in the other two SMA groups (Fig. 3). In particular, difficulty to swallow food (solid and semi-solid), a feeling of a piece of food getting stuck in the throat and coughing when swallowing solids were frequently reported. These patients also had difficulty chewing solid food. In contrast, analysis in SMA type 2 and SMA type 3 groups revealed fewer complaints related to swallowing, yet both phases of swallowing were affected. There was a higher severity for the oral phase, but only one item (question 3, difficulties chewing solid food) reached a score superior to 1 in SMA type 2 patients. In these groups, the two most problematic items were if the child had difficulty chewing solid food and had difficulty getting food into his mouth. These observations are in line with those previously published by Chen et al. (2012) [9], as the most frequently reported swallowing impairments in SMA patients were difficulties to bring food to the mouth, chewing and choking problems with solid foods, and prolonged meal duration (>30min).
Looking at the severity of swallowing impairment, as measured by the SFAQ questionnaire, according to the gross motor function or SMA type (status), all patients in the SMA type 3 group had a mild swallowing impairment, regardless of whether they were “walker” or had lost the ability to walk. The majority of SMA type 2 patients had a mild impairment (80%) and a small proportion had a moderate swallowing impairment. In the SMA type 1 group, a high variability was observed as the impairment ranged from mild to severe. Although the number of patients included in the analysis was limited, the variability may probably partly be explained by the differences in age at treatment onset. Interestingly, the patient with a severe swallowing impairment requiring gastrostomy and who received nusinersen only from the age of 14 months reached the sitting stage, suggesting that current treatments can improve gross motor function without helping swallowing [33]. In contrast, SMA type 1 patients with a mild swallowing impairment were treated early: one patient received risdiplam from the age of 4.5 months, resulting in less than 4 months between onset of symptoms and treatment initiation, and another patient was treated presymptomatically with onasemnogene abeparvovec.
Data analysis revealed that the majority of SMA patients exhibited impaired SF characterized by decreased oral Pmax values and increased SFAQ scores, despite standard medical treatment. SF impairment was more severe in SMA type 1 patients than in SMA type 2 and in SMA type 3 patients.
In our study, significant negative correlations were found between SFAQ scores and Pmax for the three studied locations, showing that high SFAQ scores are associated with reduced oral pressures in SMA patients. Regardless of the SMA type and treatment administered, lower lingual, labial, and masseter Pmax values were associated with poorer SF. However, in some SMA patients, we observed a decrease in oral Pmax compared to what is expected for their age, while their swallowing scores were close to those of healthy controls. This suggests that either the decrease in Pmax, indicating the atrophy of the orofacial musculature and bulbar dysfunction, preceded the onset of swallowing disorders perceived in SMA patients, or that this phenomenon was not well captured by the SFAQ in the early stages of the disease. Interestingly and similarly to SMA patients, tongue weakness as measured by IOPI can also be observed with or without associated dysphagia in amyotrophic lateral sclerosis (ALS) patients [34].
Concerning long-term perspectives, the improvement of global motor capacities alone is unlikely to be completely satisfactory, and the improvement of comorbidities, including bulbar dysfunction, is essential to ensure an optimal quality of life. For this reason, collecting data on all comorbidities, whether motor or non-motor complications, is paramount for assessing the impact of modulating SMN in these specific areas [17].
A number of limitations were identified in our study, and we also make some suggestions for improvement. Firstly, regarding IOPI Pmax index, only one patient was included for some age groups, potentially distorting the control’s group Pmax index representativeness for that particular age. This circumstance could account for the recorded variability in Pmax pressure index from one year to the next.
Secondly, although sensitive to detect swallowing impairment in SMA patients, the SFAQ questionnaire is not yet ready for regular use in routine follow-ups of patients in SMA clinics. In addition, some questions may not be “discriminant” (see previous discussion), the questionnaire should be used with caution in the context of very young children, as in its design questions were rephrased from previous well-known existing patient questionnaires to be asked to the caregiver. Its final validation will need additional investigation in the context of further studies.
Thirdly, the two tools for assessing SF could not be carried out within a population naive of treatment, which would have been more appropriate to approach a real situation of natural history, but impossible in the context of this study in view of the widespread access to new treatments in Belgium.
Finally, with the exception of the requirement to use a gastrostomy, we have not directly studied the correlations between our tools and typical complications attributed to swallowing disorders in daily life, such as aspiration pneumonia or poor weight gain. Consequently, more clinical data should be considered in future studies, and the different SFAQ items should be analyzed in more detail.
CONCLUSIONS
The reproducibility of the results obtained with the SFAQ and repeated oral Pmax measurements by the IOPI in healthy controls suggests that these tests could be relevant for investigating SF in children aged 4 to 17 years old in routine follow-ups. SMA patients experienced disturbed SF, compared with healthy age-matched controls. These results must be interpreted with caution given the limited number of children included. Nevertheless, they likely pave the way for larger prospective studies to better understand swallowing disorders in SMA and to assess the impact of different treatments, taking the child’s age at treatment initiation and treatment duration into account. Given the promising new therapies, investigating the motor, respiratory, and swallowing function will help refine the prognosis and improve quality of life of SMA patients.
ACKNOWLEDGMENTS
We are grateful to the patients and parents for giving us permission to run this trial.
The authors of this article are members of the ERN EURO NMD. We thank the members of the ERN EURO NMD.
CONFLICT OF INTEREST
ND received consulting fees in the context of advisory Board of Biogen, Roche, and Novartis Gene Therapy. He also received a research grant from Roche and Novartis Gene Therapies.
The other authors declare no conflicts of interest.
FUNDING
ND was supported by the FNRS (Belgium) in the context of a CDR grant (n°J.0047.20).
DECLARATION OF COMPETING INTERESTS
ND reports grants from F Hoffmann-La Roche and Novartis, and consultancy fees from F Hoffmann-La Roche, Biogen, and Novartis. He served on advisory boards for F Hoffmann-La Roche, Biogen, and Novartis. The other authors declare no conflicts of interest.
DATA STATEMENT
Data available upon reasonable request to the authors.
REFERENCES
[1] | Lunn MR , Wang CH . Spinal muscular atrophy. The Lancet. (2008) ;371: (9630):2120–33. |
[2] | Deconinck N , Goemans N , editors. Neuromuscular disorders in children: A multidisciplinary approach to management. First published. London: Mac Keith Press; 2019. pp. 452. (Clinics in developmental medicine). |
[3] | Schorling DC , Pechmann A , Kirschner J . Advances in Treatment of Spinal Muscular Atrophy – New Phenotypes, New Challenges, New Implications for Care. J Neuromuscul Dis. (2020) ;7: (1):1–13. |
[4] | Ramdas S , Servais L . New treatments in spinal muscular atrophy: An overview of currently available data. Expert Opin Pharmacother. (2020) ;21: (3):307–15. |
[5] | Kakazu J , Walker NL , Babin KC , Trettin KA , Lee C , Sutker PB , et al. Risdiplam for the Use of Spinal Muscular Atrophy. Orthop Rev [Internet]. 2021 Jul 12 [cited 2023 Aug 30];13(2). Available from: https://orthopedicreviews.openmedicalpublishing.org/article/25579-risdiplam-for-the-use-of-spinal-muscular-atrophy |
[6] | Naveed A , Calderon H . Onasemnogene Abeparvovec (AVXS-101) for the Treatment of Spinal Muscular Atrophy. J Pediatr Pharmacol Ther. (2021) ;26: (5):437–44. |
[7] | Deconinck N , Devos E . Risdiplam as an orphan drug treatment of spinal muscular atrophy in adults and children (2 months or older). Expert Opin Orphan Drugs. (2022) ;10: (1):65–72. |
[8] | Costa MMB . Neural Control Of Swallowing. Arq Gastroenterol. (2018) ;55: (suppl 1):61–75. |
[9] | Chen YS , Shih HH , Chen TH , Kuo CH , Jong YJ . Prevalence and Risk Factors for Feeding and Swallowing Difficulties in Spinal Muscular Atrophy Types II and III. J Pediatr. (2012) ;160: (3):447–451.e1. |
[10] | Van Der Heul AMB , Wijngaarde CA , Wadman RI , Asselman F , Van Den Aardweg MTA , Bartels B , et al. Bulbar Problems Self-Reported by Children and Adults with Spinal Muscular Atrophy. J Neuromuscul Dis. (2019) ;6: (3):361–8. |
[11] | Van Den Engel-Hoek L , Erasmus CE , Van Bruggen HW , De Swart BJM , Sie LTL , Steenks MH , et al. Dysphagia in spinal muscular atrophy type II: More than a bulbar problem? Neurology. (2009) ;73: (21):1787–91. |
[12] | Willig TN , Paulus J , Lacau Saint∧Guily J , Béon C , Navarro J . Swallowing problems in neuromuscular disorders. Arch Phys Med Rehabil. (1994) ;75: (11):1175–81. |
[13] | Choi YA , Suh DI , Chae JH , Shin HI . Trajectory of change in the swallowing status in spinal muscular atrophy type I. Int J Pediatr Otorhinolaryngol. (2020) ;130: :109818. |
[14] | Belaala M . Troubles de la déglutition chez l’enfant en situation de handicap: évaluation des pratiques professionnelles de dépistage et d’évaluation diagnostique en France. [Internet]. Rouen; 2019. Available from: https://dumas.ccsd.cnrs.fr/dumas-02869883/document |
[15] | Kroon RHMJM , Kalf JG , De Swart BJM , Van Der Sluijs BM , Glennon JC , Raz V , et al. Longitudinal Assessment of Strength, Functional Capacity, Oropharyngeal Function, and Quality of Life in Oculopharyngeal Muscular Dystrophy. Neurology [Internet]. 2021 Oct 12 [cited 2024 Jan 22];97(15). Available from: https://www.neurology.org/doi/10.1212/WNL.0000000000012640 |
[16] | Trucco F , Salmin F , Lizio A , Coratti G , Albamonte E , Frisoni MC , et al. Assessing Prevalence and Characteristics of Oro-bulbar Involvement in Children and Adults with SMA Type 2 and 3 Using a Multimodal Approach. Dysphagia [Internet]. 2023 Jun 8 [cited 2023 Sep 11]; Available from: https://link.springer.com/10.1007/s00455-023-10584-z |
[17] | Wadman RI , De Amicis R , Brusa C , Battezzati A , Bertoli S , Davis T , et al. Feeding difficulties in children and adolescents with spinal muscular atrophy type 2. Neuromuscul Disord. (2021) ;31: (2):101–12. |
[18] | Cohen JT , Manor Y . Swallowing disturbance questionnaire for detecting dysphagia: Swallowing Disturbance Questionnaire. The Laryngoscope. (2011) ;121: (7):1383–7. |
[19] | Medical professionals – IOPI Medical [Internet]. Available from: https://iopimedical.com/medical-professionals/ |
[20] | Potter NL , Short R . Maximal Tongue Strength in Typically Developing Children and Adolescents. Dysphagia. (2009) ;24: (4):391–7. |
[21] | McKay R , Smart S , Cocks N . Investigating Tongue Strength and Endurance in Children Aged 6 to 11 Years. Dysphagia. (2020) ;35: (5):762–72. |
[22] | Adams V , Mathisen B , Baines S , Lazarus C , Callister R . A Systematic Review and Meta-analysis of Measurements of Tongue and Hand Strength and Endurance Using the Iowa Oral Performance Instrument (IOPI). Dysphagia. (2013) ;28: (3):350–69. |
[23] | O’Hagen JM , Glanzman AM , McDermott MP , Ryan PA , Flickinger J , Quigley J , et al. An expanded version of the Hammersmith Functional Motor Scale for SMA II and III patients. Neuromuscul Disord. (2007) ;17: (9–10):693–7. |
[24] | Leys C , Ley C , Klein O , Bernard P , Licata L . Detecting outliers: Do not use standard deviation around the mean, use absolute deviation around the median. J Exp Soc Psychol. (2013) ;49: (4):764–6. |
[25] | Jamovi [Internet]. 2022. (The Jamovi Project). Available from: https://www.jamovi.org |
[26] | Bearzotti F , Tavano A , Fabbro F . Development of Orofacial Praxis of Children from 4 to 8 Years of Age. Percept Mot Skills. (2007) ;104: (3_suppl):1355–66. |
[27] | Rothbart MK , Posner MI . Mechanism and variation in the development of attentional networks. In: Handbook of Developmental Cognitive Neuroscience. (2001) . pp. 353–363. |
[28] | Mano T , Katsuno M , Banno H , Suzuki K , Suga N , Hashizume A , et al. Tongue pressure as a novel biomarker of spinal and bulbar muscular atrophy. Neurology. (2014) ;82: (3):255–62. |
[29] | Finkel RS , Mercuri E , Darras BT , Connolly AM , Kuntz NL , Kirschner J , et al. Nusinersen versus Sham Control in Infantile-Onset Spinal Muscular Atrophy. N Engl J Med. (2017) ;377: (18):1723–32. |
[30] | Mercuri E , Deconinck N , Mazzone ES , Nascimento A , Oskoui M , Saito K , et al. Safety and efficacy of once-daily risdiplam in type 2 and non-ambulant type 3 spinal muscular atrophy (SUNFISH part 2): A phase 3, double-blind, randomised, placebo-controlled trial. Lancet Neurol. (2022) ;21: (1):42–52. |
[31] | Mercuri E , Darras BT , Chiriboga CA , Day JW , Campbell C , Connolly AM , et al. Nusinersen versus Sham Control in Later-Onset Spinal Muscular Atrophy. N Engl J Med. (2018) ;378: (7):625–35. |
[32] | Darras BT , Masson R , Mazurkiewicz-Bełdzińska M , Rose K , Xiong H , Zanoteli E , et al. Risdiplam-Treated Infants with Type 1 Spinal Muscular Atrophy versus Historical Controls. N Engl J Med. (2021) ;385: (5):427–35. |
[33] | Van Der Heul AMB , Cuppen I , Wadman RI , Asselman F , Schoenmakers MAGC , Van De Woude DR , et al. Feeding and Swallowing Problems in Infants with Spinal Muscular Atrophy Type 1: An Observational Study. J Neuromuscul Dis. (2020) ;7: (3):323–30. |
[34] | Printza A , Boziki M , Triaridis S , Kiousi V , Arnaoutoglou M , Constantinidis J , et al. Tongue strength, dysphagia questionnaire, pharyngeal secretions and FEES findings in dysphagia management in amyotrophic lateral sclerosis. Auris Nasus Larynx. (2021) ;48: (4):672–82. |


