
Development and Pilot Validation of the DuMAND Checklist to Screen for Duchenne Muscular Dystrophy-Associated Neurobehavioral Difficulties (DuMAND)
Abstract
Background:
Patients with Duchenne muscular dystrophy (DMD) face a higher risk of neurobehavioral problems, yet an international consensus on screening, assessing, and managing these difficulties is lacking.
Objective:
This report introduces the term Duchenne Muscular Dystrophy-Associated Neurobehavioral Difficulties (DuMAND) to comprehensively cover the spectrum of neurobehavioral issues in DMD patients, including behavior, psychiatric disorders, and various cognitive, academic, and psychosocial deficits. To facilitate screening, the DuMAND Checklist, a 43-item tool with five subscales, was developed.
Methods and results:
DuMAND categories were derived through literature review, parent (48 mothers and 37 fathers), and expert (n = 28) input and feedback. The DuMAND Checklist subscales were developed iteratively, incorporating item selection, expert panel (n = 10) assessment for face validity, comprehensiveness, and a pilot validation study in a DMD sample (n = 20). DuMAND encompasses five categories: cognition and learning, social responsiveness, emotion regulation, externalizing behavior, and eating and sleeping. Preliminary validation of the DuMAND Checklist indicates acceptable-to-excellent internal consistency and construct validity.
Conclusion:
By introducing the DuMAND concept, this study seeks to inspire a consensus approach for screening, assessing, and managing neurobehavioral issues in DMD. Incorporating screening, using the DuMAND Checklist, in addition to medical follow-up will facilitate early intervention, addressing a critical gap in identification of neurobehavioral disorders in DMD. Future research is needed to further evaluate psychometric properties of the DuMAND Checklist and investigate the natural course of DuMAND.
Highlights:
– This report introduces the term Duchenne Muscular Dystrophy-Associated Neurobehavioral Difficulties (DuMAND) to comprehensively cover the spectrum of neurobehavioral issues in DMD patients, including behavior, psychiatric disorders, and various cognitive, academic, and psychosocial deficits.
– DuMAND encompasses five categories: cognition and learning, social responsiveness, emotion regulation, externalizing behavior, and eating and sleeping.
– Preliminary validation of the DuMAND Checklist indicates acceptable-to-excellent internal consistency and construct validity.
INTRODUCTION
Duchenne muscular dystrophy (DMD) is a progressive neuromuscular disorder, caused by a mutation in the dystrophin gene on the X-chromosome, hindering dystrophin protein production and expression in various body tissues [1]. In muscles, dystrophin deficiency results in progressive muscle degeneration and motor function difficulties [2]. However, dystrophin also plays a role in brain development and function as distinct dystrophin isoforms contribute across different stages of neuronal growth, and disruption in their production correlates with elevated incidence of cognitive, neuropsychological, and behavioral issues [3, 4]. There is a higher prevalence of intellectual disorders in patients with DMD compared to the general population [5]. DMD patients tend to have a discrepant neuropsychological profile, with often an impaired working memory [6]. Furthermore, the risk of neurodevelopmental disorders such as attention deficit hyperactivity disorder (ADHD), autism spectrum disorder (ASD) and learning disorders is elevated [4]. DMD patients also encounter psychiatric problems like obsessive-compulsive disorder (OCD) and anxiety disorders (AD) more frequently than the general population [7]. Recent research underscores that a substantial proportion of individuals with DMD experience not only one, but multiple neurodevelopmental or psychiatric issues, presenting a broad spectrum of behavioral challenges [8, 9]. Furthermore, the neurobehavioral profile in DMD patients is notably heterogeneous. The conventional categorical diagnostic approach, such as that outlined in DSM-5, may prove impractical for a considerable number of DMD patients, despite the profound impact of these behavioral challenges on their daily functioning [7, 8]. Additionally, as motor function diminishes, behavioral expression can change and differ from behavioral criteria used within the general population. Overall, the current knowledge about the underlying pathophysiological mechanisms and empirical support for management of DMD-related neurobehavioral challenges remains limited. Clinical care guidelines provide comprehensive insights into monitoring and handling of the physical consequences of DMD, yet recommendations on screening for and managing of the neurobehavioral phenotype are only briefly covered [10]. Moreover, no consensus exists on the optimal assessment approach for this population, and the questionnaires commonly used in pediatric psychology and child and youth psychiatry often lack adaptation to the specifics of this disease.
This issue extends beyond DMD patients and mirrors situations in other medical conditions involving the central nervous system associated with neurobehavioral comorbidities. Communities dealing with Human Immunodeficiency Virus (HIV) and Tuberous Sclerosis Complex (TSC) have pioneered concepts like HIV-associated neurocognitive disorders (HAND) and TSC-associated neuropsychiatric disorders (TAND) [11, 12]. The TSC community developed the TAND-L and TAND-SQ Checklists to facilitate screening for TAND in clinical routine follow up of these patients [13–15]. This initiative eventually yielded consensus recommendations for screening and management of TAND by the TAND Consortium [16].
Inspired by these successful examples, we propose the term Duchenne Muscular Dystrophy-Associated Neurobehavioral Difficulties, DuMAND, as a comprehensive concept that encompasses the full range of manifestations associated with DMD that relate to behavior, psychiatric disorders, and intellectual, academic, neuropsychological, and psychosocial disabilities. The primary objective of this study is to establish a clear conceptualization of the term DuMAND by determining the specific manifestations covered by this umbrella term. Additionally, this research manuscript outlines the initial stages in the development of a DuMAND screening tool intended for clinical practice. The resulting tool, named the DuMAND Checklist, aims to serve as a resource for healthcare professionals and families, aiding in the screening for DuMAND and facilitating an action plan for next steps.
METHODOLOGY
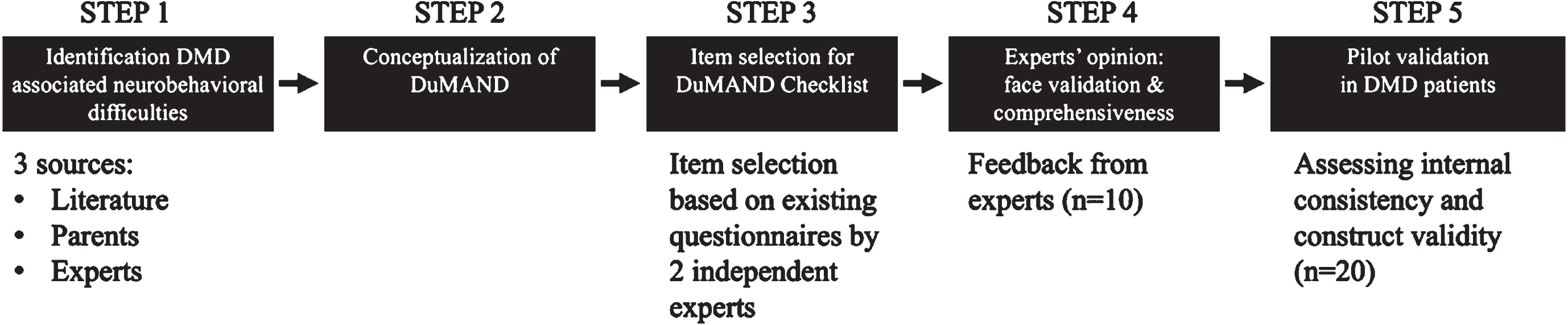
The conceptualization of the term DuMAND and the development of the DuMAND Checklist consisted of a series of distinct steps in a multi-method design, as depicted in Fig. 1. The conceptualization of the term DuMAND started with the identification of prevalent behavioral, cognitive, psychological, and psychiatric issues associated with DMD. This process involved a comprehensive analysis of data from three primary sources: scientific literature, input from parents of DMD patients, and expert healthcare professionals working in the field of DMD. Subsequently, to develop the DuMAND Checklist, a set of specific items was curated to compose a comprehensive questionnaire in alignment with these DuMAND symptoms. Finally, a group of psychologists critically evaluated this first version of the questionnaire, which was consequently modified and subjected to pilot testing within a cohort of DMD patients. Each of these steps is described in the subsequent sections.
Fig. 1
Overview of different steps for the conceptualization of DuMAND and the development of the DuMAND Checklist.
The study was approved by the Ethical Committee of the University Hospitals Leuven (S67617) and conducted in accordance with the principles outlined in the Declaration of Helsinki.
Identification of DuMAND symptoms
Literature review
The PICO model was used to find relevant articles for a scoping literature review [17]. We devised a refined search query by defining the following components:
• Population: patients of all age groups diagnosed with DMD.
• Intervention: studies employing specific instruments such as observations, questionnaires, neuropsychological tests, and interviews, among others, to measure the outcomes elucidated below.
• Comparison: against the general population.
• Outcomes: all outcomes related to behavior, cognition, psychology, or psychiatry.
Utilizing this model, our search string in PubMed was formulated as: (“Muscular Dystrophy, Duchenne’’[Mesh]) AND (“Behavior’’[Mesh] OR “Cognition’’[Mesh] OR “Mental disorders’’[Mesh] OR “psychological phenomena’’[Mesh]). Our search was initially conducted in March 2019 at the project’s inception and re-run in August 2023 during the drafting of this article to check for new studies. Newly published studies were included in this manuscript and checked for new evidence but didn’t alter the conclusions.
Subsequently, the studies identified through this search underwent an initial screening process led by SG, which involved evaluating the titles and abstracts by using the software Rayyan [18]. Studies were considered for inclusion if they aligned with the objectives outlined by the PICO model and if they were available in the English language. Studies concentrating on animal models, those only focusing on quality of life, and those exploring psychological impact on parents or siblings of DMD patients were deliberately excluded from this review.
Neurobehavioral difficulties reported by parents of DMD patients
To identify prevalent behaviors within the context of DMD, we engaged both fathers and mothers of DMD patients in completing the Child Behavior Checklist (CBCL) [19]. This questionnaire encompasses 113 items reflecting a spectrum of behaviors and emotions. Parents scored the occurrence frequency of each item over the preceding 6 months on a scale of 0 (never), 1 (sometimes), or 2 (a lot). Rather than computing scale scores, we harnessed scores from individual items to pinpoint the most severe and most frequently reported neurobehavioral issues associated with DMD. The parental participants encompassed both mothers and fathers of DMD patients aged 6-18 years. Eligible patients were those under the care of the Neuromuscular Reference Center (NMRC) for children at the UZ Leuven, a university hospital in Belgium. Inclusion criteria stipulated genetically confirmed diagnosis of DMD, aged between 6-18 years old and Dutch as the native language. Prior to participation, parents provided written informed consent, while children aged 12 and above provided assent.
Given the dynamic evolution of behaviors across age, we dissected the outcomes into two age groups (6-11 years and 12-18 years) for each respondent (fathers and mothers). As an indicator of the severity of each item, we calculated the average item scores, referred to as the severity score, alongside the percentage of parents reporting the specific item, the frequency score. Items with a reported severity score above 0.80 (corresponding with the 90th percentile) or reported by more than 50% of at least one of the parents in at least one age group, were categorized as highly prevalent DMD neurobehavioral difficulties.
Neurobehavioral difficulties reported by clinical experts in DMD
In 2019, we launched an online survey directed at clinical experts ((child) neurologists, pediatricians, rehabilitation specialists and a psychologist and social worker) specializing in the field of DMD, to investigate their experience with occurrence and management of neurobehavioral symptoms in clinical practice. One section of the survey, detailed and elaborated upon elsewhere (manuscript submitted), focused on assessing the prevalence of specific behavioral, cognitive, psychological, and psychiatric symptoms encountered in their clinical interactions with DMD patients and families. Experts were asked to indicate the frequency with which each symptom manifests in their experience with DMD patients. Responses were categorized into levels representing “very often” (5), “often” (4), “sometimes” (3), “rarely” (2), or “never” (1). The average scores on this five-point scale were then computed. Symptoms receiving an average score of three out of five or higher were categorized as highly frequent DMD neurobehavioral difficulties.
Conceptualization of DuMAND
The previous stages of our study led to the identification of neurobehavioral difficulties frequently seen in patients with DMD. To structure this list, two experienced child psychologists (SG and JL) examined the list, organizing behaviors into cohesive groupings based on their shared characteristics. This process led to the emergence of five distinct categories: cognition and learning, social responsiveness, emotion regulation, externalizing behavior, and eating & sleeping. The proposed categorization was then deliberated upon by the entire author group to ensure consensus and agreement with this division. These categories constitute the fundamental concept of the term DuMAND, and form the structure and subscales of the DuMAND Checklist.
Item selection for the DuMAND Checklist
In the subsequent step, items representing DuMAND symptoms within each category were carefully selected. We achieved this by looking at different items of well-established instruments known for their validity in the pediatric domain, including the Child Behavior Checklist (CBCL), Strengths and Difficulties Questionnaire (SDQ) [20], Personal Adjustment and Role Skills Scale-III (PARS-III) [21], and the TAND-L Checklist [12]. These instruments were independently reviewed by two experienced child psychologists (JL and SG). They assessed these items by assigning a rating (0 or 1) based on their representativeness for the DuMAND categories (cognition and learning, social responsiveness, emotion regulation, externalizing behavior, and eating & sleeping). Only items that achieved unanimous agreement between the raters (100%) were incorporated and utilized in the formulation of items for the DuMAND Checklist. Subsequently, duplicate or highly similar items were eliminated, and the phrasing and wording were refined to better suit a population with physical limitations.
Expert opinion: face validity and comprehensiveness
Finally, a panel of 10 child and youth psychologists working in the DMD domain was assembled to evaluate the individual items within the checklist. To test face validity, participants were asked to allocate the items to the respective DuMAND category they perceived to be representative for the item’s nature. Furthermore, input was gathered from the psychologists regarding item phrasing, clarity, comprehensiveness, and relevance for the DMD population. Items that were inaccurately allocated or formulated were modified based on the feedback provided, to ensure face validity and comprehensiveness.
Pilot validation
Procedure
The first version of the DuMAND Checklist was administered to parents of patients with DMD from the NMRC for children at the University Hospitals Leuven, Belgium. Participants were included if their child had a confirmed genetic diagnosis of DMD and was 6-18 years old. Parents from DMD patients who participated in the earlier phase of this study were not included in the pilot validation. Different from the previous phase (described in section 2.1.2), only one parent (mother or father) was asked to participate. Parents needed to have Dutch as their native language. Due to the behavior regulating effects, parents of DMD patients treated with psychopharmaceutical drugs, were also not included.
The DuMAND Checklist was completed by indicating how frequent the behavior was seen in their child over the past 3 months. Parents could rate this as “never” (1); “rarely” (2); “sometimes” (3); “often” (4) or “very often” (5). For every DuMAND category, a subscale score was calculated by adding up the item scores representing the category.
After completion of the DuMAND Checklist, qualitative feedback was asked from the parents regarding clarity, comprehensiveness, and ease of use. This was done during a small conversation after completing the questionnaires. The opportunity was provided to give feedback on individual items or on the questionnaire in general.
To assess construct validity, parents were requested to complete well-validated and widely recognized rating scale measures tailored for the evaluation of specific cognitive, behavioral, or psychiatric problems in children. In particular, we employed the school scale from the CBCL to examine the construct validity of the subscale cognition and learning. To assess the construct validity of the subscale social responsiveness, the total scale score of the Social Responsiveness Scale –second edition (SRS-2) was used [22]. For the subscale emotion regulation, construct validity was explored using the emotional symptoms scale and the internalizing scale from the SDQ, as well as the anxiety/depression scale and withdrawal scale from the PARS-III. For the subscale externalizing behavior, we examined construct validity by considering the scales related to conduct disorders, hyperactivity, and externalizing behavior from the SDQ, along with the hostility scale from the PARS-III. The subscale eating and sleeping was not assessed on construct validity in this phase.
Statistical analyses
SPSS Version 29 was used for statistical analysis [23]. Descriptive statistics were used to calculate frequencies, percentages, means and standard deviations (SD).
Internal consistency assessment of the DuMAND Checklist involved the calculation of Cronbach’s alpha coefficient (α) for each category. The interpretation of Cronbach alpha values was guided by Streiner et al. (2003) [24], categorizing them as excellent (α > 0.9), good (0.7 < α < 0.9), acceptable (0.6 < α < 0.7), poor (0.5 < α < 0.6), or unacceptable (α < 0.5).
The analysis of construct validity relied on the Pearson correlation coefficient (r) to determine the strength of the relationship between the outcomes on the DuMAND Checklist subscales and the respective subscales of the chosen validation tools. Correlation strength was interpreted as strong (>0.7), moderate (0.4 to 0.7), or low (<0.4) [25].
RESULTS
Identification of DuMAND symptoms
Literature search
The flowchart depicting the outcome of the scoping literature review is presented in Fig. 2. Following the step-by-step selection process, a comprehensive total of 118 studies emerged as candidates for analysis. An exhaustive overview of these studies and the results derived from the comprehensive analysis is documented in detail in Supplementary Table 1. The majority of these studies (109) exclusively encompassed DMD patients, whereas 20 studies also included Becker muscular dystrophy (BMD) patients. We decided to also include studies with BMD patients as they may represent additional information on intermediate phenotypes with DMD-like features. Among all studies, six case studies, two guideline documents, one editorial letter, two meeting reports, three narrative reviews and 13 systematic reviews were included. Original research was presented in 89 studies.
Fig. 2
Flowchart with distinct steps of the article selection process.

Table 1
DMD behaviors frequently reported by parents
| Mothers | Fathers | ||||||||
| 6–11 years | 12–18 years | 6–11 years | 12–18 years | ||||||
| (n = 24) | (n = 24) | (n = 20) | (n = 17) | ||||||
| CBCL item | Neurobehavioral item | Sev | Freq | Sev | Freq | Sev | Freq | Sev | Freq |
| 1 | Acts too young for his/her age | 0.71 | 63% | 1.04 | 71% | 0.95 | 74% | 1.12 | 76% |
| 4 | Fails to finish things he/she starts | 0.63 | 58% | 0.46 | 46% | 0.63 | 53% | 0.47 | 41% |
| 5 | There is very little he/she enjoys | 0.58 | 46% | 0.50 | 38% | 0.53 | 37% | 0.59 | 53% |
| 8 | Can’t concentrate, can’t pay attention for long | 1.17 | 83% | 0.75 | 58% | 1.32 | 95% | 0.88 | 59% |
| 9 | Can’t get his/her mind off certain thoughts | 0.63 | 54% | 0.63 | 54% | 0.84 | 58% | 0.47 | 35% |
| 11 | Clings to adults or too dependent | 0.83 | 67% | 1.29 | 79% | 0.95 | 79% | 1.00 | 71% |
| 17 | Daydreams or gets lost in his/her thoughts | 0.92 | 63% | 0.71 | 58% | 0.58 | 42% | 0.41 | 35% |
| 19 | Demands a lot of attention | 1.08 | 71% | 0.92 | 67% | 1.00 | 63% | 0.82 | 65% |
| 22 | Disobedient at home | 0.58 | 58% | 0.25 | 21% | 0.47 | 42% | 0.18 | 12% |
| 36 | Gets hurt a lot, accident prone | 0.42 | 38% | 0.17 | 17% | 0.84 | 68% | 0.35 | 29% |
| 42 | Would rather be alone than with others | 0.42 | 38% | 0.63 | 54% | 0.47 | 37% | 0.35 | 29% |
| 45 | Nervous, highstrung, or tense | 0.58 | 54% | 0.42 | 33% | 0.58 | 47% | 0.29 | 24% |
| 62 | Poorly coordinated or clumsy | 0.63 | 54% | 0.33 | 29% | 0.47 | 47% | 0.59 | 41% |
| 74 | Showing off or clowning | 0.38 | 33% | 0.21 | 17% | 0.63 | 53% | 0.18 | 12% |
| 75 | Too shy or timid | 0.58 | 50% | 0.67 | 50% | 0.37 | 32% | 0.71 | 53% |
| 78 | Inattentive or easily distracted | 1.17 | 79% | 0.54 | 50% | 0.95 | 74% | 0.41 | 35% |
| 86 | Stobburn, sullen, or irritable | 0.79 | 63% | 0.58 | 54% | 1.00 | 74% | 0.53 | 41% |
| 95 | Temper tantrums or hot temper | 0.58 | 54% | 0.42 | 38% | 0.58 | 47% | 0.35 | 24% |
| 102 | Underactive, slow moving, or lacks energy | 0.46 | 38% | 0.83 | 58% | 0.53 | 37% | 0.53 | 35% |
| 109 | Whining | 0.88 | 63% | 0.46 | 38% | 0.63 | 58% | 0.29 | 24% |
| 112 | Worries | 0.50 | 46% | 0.67 | 54% | 0.26 | 21% | 0.41 | 35% |
Items meeting the criteria (severity score above 0.80 or a frequency exceeding 50% by at least one parent in any age group) are highlighted in bold. Severity scores are reported as means with a range from 0–2; frequency scores are reported as percentages. CBCL = Child Behavior Checklist; Sev = severity score: Freq = frequency score.
Eighty studies reported about cognitive development and intellectual functioning, while 39 more deeply assessed neuropsychological aspects encompassing working memory, executive functioning, and attention domains. Additionally, 23 studies included a nuanced assessment of language-related capacities, including expressive and receptive language abilities, and reading and speech competence. Twenty-five studies focused on psychiatric diagnoses, whereas 39 studies demonstrated the spectrum of behaviors within the DMD population.
Cognitive functioning and intellectual challenges manifested as prevalent comorbidities among DMD boys. Concomitant with these are learning disorders, accompanied by distinct neuropsychological issues such as impaired working memory, implicit learning difficulties, and more complex higher-order executive function deficits such as sustained attention complications, attention control issues, and inhibition challenges. Neurodevelopmental disorders like ASD and ADHD, and psychiatric disorders like affective disorders, emerged as prominently mentioned in literature. Some studies additionally delineated the occurrence of OCD. The behavioral dimension encompassed a spectrum of manifestations, including anxiety-related issues, affective dysregulation, challenges in emotion coping, and tendencies towards aggressive behaviors.
Parents
A total of 48 families of DMD patients participated in this study, with an average patient age of 11.83 years (SD = 4.20, age range: 6 to 18 years). All 48 mothers and 37 fathers in the sample returned the completed CBCL questionnaires. A comprehensive overview of the most frequently reported neurobehavioral difficulties, and the difficulties identified as the most severe, stratified by age group and respondent, is provided in Table 1. Supplementary Tables 2–5 present these issues, ranked by frequency, for each age group, categorized by the respondents.
DMD professionals
Twenty-eight clinical DMD experts from 16 different countries completed the survey: 15 child neurologists, 3 adult neurologists, 4 pediatricians, 3 rehabilitation specialists, 1 child psychologist, 1 general practitioner, and 1 social worker (manuscript submitted). All of them had substantial experience in the field of DMD, with 24 of them having more than a decade of experience, and 15 of them seeing over 100 DMD patients each year. All experts indicated the frequency with which each symptom manifests in their experience with DMD patients. Table 2 displays the items with an average score of 3 out of 5 or higher, which we consider as frequently reported neurobehavioral difficulties in DMD.
Table 2
Neurobehavioral difficulties in DMD frequently reported by clinical experts
| Neurobehavioral item | N | Score |
| Learning problems | 26 | 4.0 |
| Dependent from adults | 24 | 4.0 |
| Anxiety | 26 | 3.9 |
| Concentration problems | 27 | 3.9 |
| Social problems | 26 | 3.8 |
| Problems with reading | 24 | 3.6 |
| Worrying | 26 | 3.6 |
| Shyness | 26 | 3.5 |
| Problems with math | 24 | 3.5 |
| Rigide thoughts | 25 | 3.4 |
| Doesn’t take initiative | 25 | 3.3 |
| Claiming to adults | 23 | 3.3 |
| Is clumsy | 24 | 3.3 |
| Temper Tantrums | 25 | 3.2 |
| Unappropriate eye contact | 25 | 3.2 |
| Demands a lot of attention | 26 | 3.2 |
| Compulsive behavior | 26 | 3.2 |
| Acts too young for his age | 25 | 3.2 |
| Doesn’t pay attention | 25 | 3.2 |
| Doesn’t have friends | 25 | 3.2 |
| Stubborn | 26 | 3.1 |
| Obsessive toughts | 25 | 3.1 |
| Sleeping problems | 25 | 3.1 |
| Depressive feelings | 26 | 3.1 |
| Can’t let go of specific thoughts | 26 | 3.0 |
| Can’t be alone | 26 | 3.0 |
| Can’t see things from the point of views of others | 24 | 3.0 |
Scores are average scores on the survey with a range from 1 (never) –5 (very often). Only items with an average score above 3.0 are displayed.
Conceptualization of DuMAND
The selected items were systematically organized into different categories under the umbrella term DuMAND. We have identified five distinct behavior categories frequently associated with difficulties in DMD patients: cognition and learning, social responsiveness, emotion regulation, externalizing behavior, and eating & sleeping. Table 3 displays the allocation of specific evidence to the respective categories.
Table 3
Overview DuMAND categories
| Source | |||
| Literature | Parents | Expert | |
| Category 1: Cognition and learning | |||
| Cognitive and intellectual deficits | x | ||
| Learning disorders | x | x | |
| Neuropsychological deficits | x | ||
| Problems with executive functioning | x | x | x |
| Concentration problems | x | x | x |
| Poorly coordinated or clumsy | x | x | x |
| Inattentive or easily distracted | x | x | x |
| Category 2: Social responsiveness | |||
| Autism-like features | x | x | x |
| Can’t get his/her mind off certain thoughts | x | ||
| Would rather be alone than with others | x | ||
| Too shy or timid | x | x | x |
| Rigid though, stubborn | x | x | x |
| Unappropriated eye contact | x | x | |
| Doesn’t have friends | x | ||
| Can’t let go of specific thoughts | x | ||
| Can’t see things from the point of view of others | x | x | |
| Social problems | x | x | |
| Category 3: Emotion regulation | |||
| Dependent from adults, clings to adults | x | x | |
| Anxiety, nervousness, tensed | x | x | x |
| Worrying | x | x | |
| Shyness | x | x | |
| Compulsive behavior | x | x | |
| Obsessive thoughts | x | ||
| Depressive feelings | x | ||
| Can’t let go of specific thoughts | x | x | |
| Can’t be alone | x | ||
| There is very little he/she enjoys | x | ||
| Category 4: Externalizing behavior | |||
| Temper Tantrums | x | x | |
| Hyperactivity | x | x | x |
| Demands a lot of attention | x | x | |
| Doesn’t pay attention | x | x | |
| Disobedient | x | x | |
| Verbal or physical aggression | x | x | |
| Showing of or clowning | x | ||
| Whining | x | ||
| Category 5: Eating &sleeping | |||
| Sleeping problems | x | ||
| Selective eating | x | ||
| Eating too much/ too little | x | ||
Item selection for the DuMAND Checklist
In a comprehensive item selection process, a total of 205 items drawn from the SDQ, TAND Checklist, PARS-III, and CBCL 6-18 years were assessed for their representativeness to the predefined DuMAND categories. This process was conducted independently by two experienced psychologists, SG and JL. Among these items, it was mutually agreed upon by both researchers that 89 were not suitable for categorization within any of the predefined categories. Additionally, there was insufficient consensus on 22 items, resulting in their exclusion from the DuMAND Checklist. Ultimately, both psychologists reached a consensus on 94 items that were deemed representative of one of the five designated DuMAND categories. After filtering to remove highly similar items and to ensure suitability for a population with physical limitations, 43 items were retained. These were distributed as following: seven items for category 1, ten items for category 2, twelve items in category 3, ten items in category 4, and four items in category 5.
The following example illustrates this process. Anxiety emerged as a behavioral symptom mentioned across all three sources, leading to its categorization within the emotion regulation category. Within the DuMAND Checklist, Anxiety is assessed by the item “He is afraid of many things or easily becomes anxious”. This formulation was distilled by amalgamating items such as “many fears, easily scared” from the SDQ, “difficulties with anxiety” from the TAND Checklist, and two items from the CBCL: “fears certain animals, situations, or places” and “is too anxious or easily scared”. By synthesizing items from well-validated questionnaires, we aimed to ensure the comprehensiveness and accuracy of the DuMAND Checklist items.
Expert opinion: face validity and comprehensiveness
The above 43 items were presented to an expert panel of 10 clinical psychologist working with boys with DMD in Belgium (Flanders) or the Netherlands. A total of twenty-eight items received major consensus, as seven or more participants from the expert group allocated them to their original category. In two instances, experts unanimously agreed on the allocation, however their allocation differed from the original category. In response, these items were re-categorized to align with the experts’ consensus.
Conversely, for the remaining thirteen items, consensus was not achieved based on initial allocation. These items underwent further discussion, with rephrasing to enhance clarity and alignment with one category, guided by feedback from the experts. Additionally, all (n = 43) items were refined as necessary, incorporating feedback provided by the expert group. This resulted in the refined items displayed in Table 4.
Table 4
Items per category selected for the DuMAND Checklist
| Category 1: Cognition and learning |
| There are difficulties with reading |
| He often forgets what he needs to do when asked |
| There are difficulties with spelling |
| He struggles to concentrate or focus on his work |
| He has difficulty speaking or speaking fluently in certain situations |
| There are difficulties with math |
| It’s challenging for him to complete a task he has started |
| He acts younger than his age |
| Category 2: Social responsiveness |
| He struggles to engage in conversation with people other than his family members |
| He is noticably shy |
| He finds it difficult to consider the feelings of others |
| He has difficulty connecting with new people |
| He exhibits rigid behavior and struggles with changing routines |
| He has difficulty seeing things from other people’s perspectives |
| He becomes angry when things don’t go the way he wants |
| He is closed-off and shows little of what’s going on inside him |
| He prefers to do things the same way |
| He doesn’t make eye contact when speaking to people. |
| Category 3: Emotion regulation |
| He is afraid of many things or easily becomes anxious |
| He displays repetitive behavior, such as repeating the same action over and over |
| He frequently worries or has excessive thoughts |
| He is hesitant to do things without adults or clings to them |
| He has trouble letting go of certain thoughts or ideas |
| He exhibits strange or bizarre behaviors |
| He appears unhappy or sad |
| He seems to worry a lot |
| It’s difficult for him to be alone |
| His mood or feelings change suddenly |
| He lacks initiative or doesn’t know what he wants to do |
| Category 4: Externalizing behavior |
| He is restless, overly active, and cannot sit still for long |
| He frequently has tantrums or outbursts of anger |
| He is demanding and often bossy |
| He displays impulsive behavior |
| He is difficult to control and seems unaffected by rewards or punishments |
| He frequently argues or seeks out conflicts |
| He is disobedient |
| He whines a lot or asks many questions |
| Small details can trigger restlessness or anger |
| He demands a lot of attention |
| Category 5: Eating and sleeping |
| He has difficulty falling asleep |
| He has poor appetite |
| He experiences sleep problems |
| He is inexplicably tired |
Pilot validation study
Descriptive results
Parents of 20 DMD patients (mean age = 13.37 years, SD = 3.68 years) participated in this phase. These were individuals who did not take part in the previous phase described in Section 3.1.2. Supplementary Table 6 provides an overview of the average outcomes on the subscales of the DuMAND Checklist and of the relevant subscales of the instruments used to investigate construct validity.
Qualitative feedback
Completion time of the DuMAND Checklist was 4-11 minutes. All twenty parents found the DuMAND Checklist to be comprehensive, easy to use, and efficient in its administration. We received seven qualitative comments from parents, primarily providing additional details to make items and situations more specific to their child. Overall, the feedback regarding the administration of the DuMAND Checklist was positive.
Internal consistency
The items in the cognition and learning subscale showed good internal consistency (α = 0.799). The items in the social responsiveness subscale (α = 0.798) and in the emotion regulation subscale (α = 0.788) also generated a high α value. The items of the subscale externalizing behavior generated an excellent α value (α = 0.930), while the internal consistency of the category eating and sleeping was very poor (α = 0.281).
Construct validity
The school subscale in the CBCL is a measure of positive results and a strong negative correlation was demonstrated between the results on this CBCL subscale and the DuMAND Checklist subscale cognition and learning (r = –0.76, p < 0.001). A moderate correlation was revealed between the results on the subscale social responsiveness and the total score on the SRS-2 (r = 0.69, p < 0.001). The results on the DuMAND Checklist subscale emotion regulation showed a strong correlation with the results on the emotional symptoms scale and the internalizing scale from the SDQ (respectively r = 0.78, p < 0.001 and r = 0.76, p < 0.001) and the anxiety/depression scale of the PARS-III (r = 0.73, p < 0.001), and a moderate correlation with the results on the withdrawal scale from the PARS-III (r = 0.50, p < 0.05). Results on the subscale externalizing behavior of the DuMAND Checklist showed a strong correlation with the results on the conduct disorder and externalizing behavior of the SDQ (respectively r = 0.80, p < 0.001 and r = 0.76, p = 0.001) and the hostility scale from the PARS-III (r = 0.75, p < 0.001), and a moderate correlation with the hyperactivity scale of the SDQ (r = 0.52, p < 0.05).
DISCUSSION
In this study, we aimed to introduce and conceptualize the term DuMAND, which stands for Duchenne Muscular Dystrophy-Associated Neurobehavioral Difficulties. DuMAND serves as an umbrella term encompassing the diverse array of manifestations related to behavior, psychiatric disorders, as well as intellectual, academic, neuropsychological, and psychosocial deficits frequently seen in DMD patients. The term DuMAND was developed through a multistep process starting from identification of the most prevalent neurobehavioral difficulties in DMD. Based on a scoping literature review and input gathered from both parents of individuals with DMD and clinical experts in the field, we identified five categories in which patients with DMD may exhibit neurobehavioral difficulties.
In addition, this study developed, and pilot validated a tool for efficient screening of DuMAND manifestations in a clinical setting. The resultant DuMAND Checklist is formed by 43 items distributed across five subscales that correspond to the five DuMAND categories. Caregivers can complete the checklist, aiding clinicians in systematic screening for DuMAND symptoms by rating the prevalence of each item over the past three months on a 5-point Likert scale. The DuMAND Checklist was developed by an iterative process with feedback from clinical DMD experts to improve face and content validity. Moreover, evaluation of internal consistency and construct validity suggested that the DuMAND Checklist has acceptable-to-excellent psychometric properties. These findings suggest that the DuMAND Checklist may be a valuable instrument for identification of issues related to the following five categories identified as highly prevalent among DMD patients.
The first category pertains to cognition and learnings. Difficulties in these domains are most frequently cited in literature and encompass cognitive problems, intellectual disorders, as well as specific neuropsychological deficits such as executive functioning, attention problems, working memory deficits, and learning disorders. It is important to note that these challenges can significantly impact daily functioning, particularly in the context of school performance, academic achievement, and psychosocial development [26].
The second category is centered on problems related to social responsiveness, which can be defined as an individual’s capacity to effectively engage with and adapt to the demands and expectations of their social environment [27]. This consists of the ability to respond to evolving societal values and norms and extends to being proactive in recognizing and responding to social needs, rather than merely reacting to them. Difficulties with social responsiveness can result in behavior that is incongruent with the social context, leading to challenges in social integration and even social isolation. Furthermore, it may cause a burden on the immediate environment, potentially manifesting in challenging social interactions and misaligned expectations [28].
Category three encompasses issues related to emotion regulation, which involves a child’s capacity to efficiently manage and adjust their emotional responses across diverse situations [29]. This facet of emotional development includes the strategies children acquire during psychosocial development to recognize, express, and effectively cope with their emotions in a manner that is not only adaptive but also socially appropriate [29]. When a child struggles with emotion regulation, it can have several adverse consequences, including heightened anxiety, decreased overall well-being, and challenges in forming healthy relationships, excelling academically, and navigating life’s obstacles with increasing independence from parents [30].
In the fourth category externalizing behavior is addressed, encompassing a spectrum of behaviors and actions directed outwardly or externally. These behaviors are typically characterized by the potential to disrupt the external environment, influence interactions with others, and transgress societal norms and rules [31]. Externalizing behaviors may manifest as acts of aggression, defiance, impulsivity, hyperactivity, and conduct problems that directly impact the individual’s interactions and surroundings. Importantly, these behaviors can impose a significant burden on both the individuals themselves and their immediate environment [31, 32].
Category five serves as a miscellaneous category encompassing difficulties related to eating and sleeping. The items in this subscale did not appear to have good internal consistency, which is not unexpected as items questioning eating behavior not necessarily are related with items measuring sleeping behavior. Due to the unique composition no construct validation was performed for this specific subscale. While issues with eating and sleeping may not be as prevalent as those in other categories, they are of particular significance due to their association with fundamental human needs [33]. Disruption in eating and sleeping patterns can potentially have a cascading effect, impacting various aspects of an individual’s life. Consequently, addressing these challenges is important to ensure holistic care for and well-being in DMD patients.
It is important to note that these categories are not mutually exclusive in individual DMD patients. On the contrary, they often significantly overlap. Hence, a DMD patient may simultaneously manifest neurobehavioral symptoms that fall into multiple categories, creating a DuMAND profile. Furthermore, the DuMAND profile of a DMD patient will likely evolve over time as they progress through various stages of psychosocial development and disease progression.
Further validation studies will facilitate the implementation of the concept DuMAND and integration of the DuMAND Checklist into the standards of care for DMD patients. The implementation of annual screening for DuMAND manifestations could potentially bridge the gap in identification of neurobehavioral disorders in DMD, paving the road towards earlier and more proactive treatment of these difficulties. Addressing these problems may involve a spectrum of actions, ranging from psycho-education, parental guidance or providing information regarding self-care strategies, to referral to a specialist setting for further evaluation and eventual psychotherapeutic and/or psychopharmaceutic treatment if needed. Initiatives such as TAND in TSC [12], have played an important role in raising awareness and establishing a shared language for description, assessment, diagnosis and management of neurobehavioral issues in TSC [16].
Despite the encouraging preliminary findings from this pilot study, it is essential to acknowledge the limitations. We only measured internal consistency; other reliability measures, such as test-retest reliability, were not assessed. The investigation of the various psychometric properties of the DuMAND Checklist, as well as validation in a larger and more diverse international cohort of DMD individuals, will be a next step in the research process. Importantly, we aim to involve focus groups with patients and parents in this next step to ensure their perspectives are incorporated as well. While the conceptualization of the term DuMAND was based on a literature search and insights from international clinical experts in DMD, it is important to note that data obtained from parents and the pilot validation phase were collected from a DMD population aged between 6-18 years old followed in a single center in Belgium. Many of these patients receive standard of care treatment with daily deflazacort. It is crucial to recognize that the behavioral side effects of corticosteroid treatment may differ based on the regimen or the age. Therefore, replication of this study in an international cohort with different steroid regimens and age groups is necessary before these findings can be considered representative for the entire DMD community.
CONCLUSION
By introducing and defining the term DuMAND, we hope to have taken the initial step to catalyze a similar process aimed at reaching a consensus approach for the screening, assessment, and management of neurobehavioral difficulties in DMD, which is urgently needed [34]. Moreover, our findings strongly suggest that the DuMAND Checklist is a valuable screening tool for identification of individuals with DMD who are at risk of neurobehavioral difficulties and is suitable for implementation.
ACKNOWLEDGMENTS
We genuinely thank all participants for contributing to this study.
This work is generated within the European Reference Network for Rare Neuromuscular Diseases ERN EURO-NMD; Project ID No. 739543.
AUTHOR CONTRIBUTIONS
SG, JL, NG and LDW were involved in the conception and design of the study. SG was involved in the acquisition and analysis of the data. SG, JL, NG, ND and LDW played an important role in the interpretation of the results. SG drafted a significant proportion of the manuscript. All authors reviewed the final manuscript.
FUNDING
This study received financial support from Pfizer SA/NV (grant number 77677327). It is important to note that Pfizer had no involvement in the design of the study, data acquisition and analyses, or the preparation of this publication.
CONFLICT OF INTEREST
N o conflict of interest was reported.
DATA AVAILABILITY STATEMENT
The data supporting the findings of this study are available within the article and/or its supplementary material.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JND-240012.
REFERENCES
[1] | Deenen JC , Horlings CG , Verschuuren JJ , Verbeek AL , van Engelen BG . The Epidemiology of Neuromuscular Disorders: A Comprehensive Overview of the Literature. J Neuromuscul Dis. (2015) ;2: :73–85, |
[2] | Duan D , Goemans N , Takeda S , Mercuri E , Aartsma-Rus A . Duchenne muscular dystrophy. Nat Rev Dis Primers. (2021) ;7: :13. doi: 10.1038/s41572-021-00248-3. |
[3] | Doorenweerd N , Mahfouz A , van Putten M , Kaliyaperumal R , PAC TH , Hendriksen JGM , et al. Timing and localization of human dystrophin isoform expression provide insights into the cognitive phenotype of Duchenne muscular dystrophy. Sci Rep. (2017) ;7: :12575. doi: 10.1038/s41598-017-12981-5. |
[4] | Banihani R , Smile S , Yoon G , Dupuis A , Mosleh M , Snider A , et al. Cognitive and Neurobehavioral Profile in Boys With Duchenne Muscular Dystrophy. J Child Neurol. (2015) ;30: :1472–82. doi: 10.1177/0883073815570154. |
[5] | Weerkamp PM , Mol EM , Sweere DJ , Schrans DG , Vermeulen RJ , Klinkenberg S , et al. Wechsler Scale Intelligence Testing in Males with Dystrophinopathies: A Review and Meta-Analysis. Brain Sciences. (2022) ;12: :1544, |
[6] | D’Angelo MG , Lorusso ML , Civati F , Comi GP , Magri F , Del Bo R , et al. Neurocognitive profiles in Duchenne muscular dystrophy and gene mutation site. Pediatr Neurol. (2011) ;45: :292–9. doi: 10.1016/j.pediatrneurol.2011.08.003. |
[7] | Ricotti V , Mandy WP , Scoto M , Pane M , Deconinck N , Messina S , et al. Neurodevelopmental, emotional, and behavioural problems in Duchenne muscular dystrophy in relation to underlying dystrophin gene mutations. Dev Med Child Neurol. (2016) ;58: :77–84. doi: 10.1111/dmcn.12922. |
[8] | Darmahkasih AJ , Rybalsky I , Tian C , Shellenbarger KC , Horn PS , Lambert JT , et al. Neurodevelopmental, behavioral, and emotional symptoms common in Duchenne muscular dystrophy. Muscle Nerve. (2020) ;61: :466–474. doi: 10.1002/mus.26803. |
[9] | Weerkamp PMM , Geuens S , Collin P , Goemans N , Vermeulen RJ , De Waele L , et al. Psychopharmaceutical treatment for neurobehavioral problems in Duchenne muscular dystrophy: a descriptive study using real-world data. Neuromuscul Disord. (2023) ;33: :619–626. doi: 10.1016/j.nmd.2023.05.011. |
[10] | Birnkrant DJ , Bushby K , Bann CM , Apkon SD , Blackwell A , Colvin MK , et al. Diagnosis and management of Duchenne muscular dystrophy, part 3: primary care, emergency management, psychosocial care, and transitions of care across the lifespan. The Lancet Neurology. (2018) ;17: :445–455. doi: 10.1016/s1474-4422(18)30026-7. |
[11] | Smail RC , Brew BJ . HIV-associated neurocognitive disorder. Handb Clin Neurol. (2018) ;152: :75–97. doi: 10.1016/b978-0-444-63849-6.00007-4. |
[12] | de Vries PJ , Whittemore VH , Leclezio L , Byars AW , Dunn D , Ess KC , et al. Tuberous sclerosis associated neuropsychiatric disorders (TAND) and the TAND Checklist. Pediatr Neurol. (2015) ;52: :25–35. doi: 10.1016/j.pediatrneurol.2014.10.004. |
[13] | Cervi F , Saletti V , Turner K , Peron A , Bulgheroni S , Taddei M , et al. The TAND checklist: a useful screening tool in children with tuberous sclerosis and neurofibromatosis type 1. Orphanet J Rare Dis. (2020) ;15: :237. doi: 10.1186/s13023-020-01488-4. |
[14] | de Vries PJ , Wilde L , de Vries MC , Moavero R , Pearson DA , Curatolo P . A clinical update on tuberous sclerosis complex-associated neuropsychiatric disorders (TAND). Am J Med Genet C Semin Med Genet. (2018) ;178: :309–320. doi: 10.1002/ajmg.c.31637. |
[15] | Heunis TM , Chambers N , Vanclooster S , Bissell S , Byars AW , Capal JK , et al. Development and Feasibility of the Self-Report Quantified Tuberous Sclerosis Complex-Associated Neuropsychiatric Disorders Checklist (TAND-SQ). Pediatr Neurol. (2023) ;147: :101–123. doi: 10.1016/j.pediatrneurol.2023.07.001.. |
[16] | Vanclooster S , Bissell S , van Eeghen AM , Chambers N , De Waele L , Byars AW , et al. The research landscape of tuberous sclerosis complex-associated neuropsychiatric disorders (TAND)-a comprehensive scoping review. J Neurodev Disord. (2022) ;14: :13. doi: 10.1186/s11689-022-09423-3. |
[17] | Eriksen MB , Frandsen TF . The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: a systematic review. J Med Libr Assoc. (2018) ;106: :420–431. doi: 10.5195/jmla.2018.345. |
[18] | Ouzzani M , Hammady H , Fedorowicz Z , Elmagarmid A . Rayyan-a web and mobile app for systematic reviews. Syst Rev. (2016) ;5: :210. doi: 10.1186/s13643-016-0384-4. |
[19] | Achenbach TM . The Child Behavior Checklist and related instruments. 1999. |
[20] | Goodman R . The Strengths and Difficulties Questionnaire. 1997. |
[21] | Walker DK , Stein RE , Perrin EC , Jessop DJ . Assessing psychosocial adjustment of children with chronic illnesses: a review of the technical properties of PARS III. J Dev Behav Pediatr. (1990) ;11: :116–21. |
[22] | Constantino JN , Gruber D , Social Responsiveness scale- Second Edition (SRS-2). 2012, Western Psychological Services: Torrance, CA. |
[23] | CorI, IBM SPSS Statistics. 2021: Armonk, NY. |
[24] | Streiner DL . Starting at the beginning: an introduction to coefficient alpha and internal consistency. J Pers Assess. (2003) ;80: :99–103. doi: 10.1207/s15327752jpa8001_18. |
[25] | Dancey CP , Reidy J , Statistics Without Maths for Psychology: Using SPSS for Windows. 2004. |
[26] | Snow WM , Anderson JE , Jakobson LS . Neuropsychological andneurobehavioral functioning in Duchenne muscular dystrophy: Areview. Neuroscience & Biobehavioral Reviews. (2013) ;37: :743–752. doi: 10.1016/j.neubiorev.2013.03.016. |
[27] | Constantino JN , Davis SA , Todd RD , Schindler MK , Gross MM , Brophy SL , et al. Validation of a brief quantitative measure of autistic traits: comparison of the social responsiveness scale with the autism diagnostic interview-revised. J Autism Dev Disord. (2003) ;33: :427–33. doi: 10.1023/a:1025014929212. |
[28] | Silveira-Zaldivara T , Özerk Gl , Özerk K . Developing Social Skills and Social Competence in Children with Autism. |
[29] | Crowell JA . Development of Emotion Regulation in Typically Developing Children. Child Adolesc Psychiatr Clin N Am. (2021) ;30: :467–474. doi: 10.1016/j.chc.2021.04.001. |
[30] | Wong TKY , Colasante T , Malti T . A longitudinal examination of school-related and mental health mediators linking emotion regulation to academic achievement. J Sch Psychol. (2023) ;101: :101253. doi: 10.1016/j.js2023.101253. |
[31] | Liu J . Childhood externalizing behavior: theory and implications. J Child Adolesc Psychiatr Nurs. (2004) ;17: :93–103. doi: 10.1111/j.1744-6171.2004.tb00003.x. |
[32] | Olivier E , Morin AJS , Langlois J , Tardif-Grenier K , Archambault I . Internalizing and Externalizing Behavior Problems and Student Engagement in Elementary and Secondary School Students. J Youth Adolesc.-. (2020) ;49: :2327–2346. doi: 10.1007/s10964-020-01295-x. |
[33] | Fukuda K , Hasegawa T , Kawahashi I , Imada S . Preschool children’s eating and sleeping habits: late rising and brunch on weekends is related to several physical and mental symptoms. Sleep Med. (2019) ;61: :73–81. doi: 10.1016/j.slee2019.03.023. |
[34] | Hendriksen JGM , Thangarajh M , Kan HE , Muntoni F , group Etws. 249th ENMC International Workshop: The role of brain dystrophin in muscular dystrophy: Implications for clinical care and translational research, Hoofddorp, The Netherlands, November 29th-December 1st. 2019. Neuromuscul Disord. (2020) ;30: :782–794. doi: 10.1016/j.nmd.2020.08.357. |


