
Upper Limbs Muscle Co-Contraction Changes Correlate With The Physical Motor Impairments in CMT
Abstract
Background:
Subjects with Charcot-Marie-Tooth (CMT) disease show hands impairment which is a relevant problem affecting the quality of life. This symptom is related to muscle weakness and reduced motor coordination of the upper limb. However, most studies focus on lower limb impairment, therefore the investigation of upper limb disability is necessary to identify biomarkers able to monitor disease-specific features and to tailor rehabilitation.
Objective:
This study aimed at characterizing upper limb muscle co-contraction using the co-contraction index (CCI) in CMT population.
Methods:
Upper limb kinematic and electromyography (EMG) data were collected from fourteen CMT subjects (6-CMT1A and 8-CMT1X) during motor tasks typical of daily living activities. Rudolph’s CCI was used to quantify muscle co-contraction of four muscle pairs acting on shoulder, elbow and wrist. All CMT subjects underwent clinical examination. Thirteen healthy subjects served as the normative reference (HC).
Results:
CMT1X and CMT1A showed a significant reduction in CCI for distal and proximal muscle pairs compared to HC. Furthermore, CMT1A showed greater values of CCI compared to CMT1X mainly for the axial and axial-to-proximal muscle pairs. Movement speed and smoothness were not altered compared to HC. In addition, EMG metrics showed moderate-to-strong significant correlations with clinical outcomes.
Conclusions:
CCI was able to quantify disease-specific deficits with respect to the normative reference, highlighting motor control alterations even before motor output impairment. CCI was also sensitive in detecting CMT subtypes-based differences and adopted compensatory strategies. Our findings suggest that CCI can be an outcome measure for CMT disease monitoring and interventional studies.
INTRODUCTION
Charcot-Marie-Tooth (CMT) disease is the most common hereditary neuropathy. Although the number of new CMT diagnoses has recently increased, probably due to the improvement of diagnostic strategies, CMT is still considered a rare disease.
There is an important variability in the clinical expression of the disease. The first symptoms reported by the patient, for example difficulty in running and frequent falls, concern the lower limbs. Upper limbs involvement usually appears later and is less severe, with deficit of the intrinsic muscles of the hand, loss of opposition, grip strength and dexterity and consequently difficulties in manipulating objects [1]. Ninety-eight percent of CMT1A patients report limitations in upper limb functioning, particularly affecting the dominant hand [2]. They perceive impairment in work, family roles, and outdoor activities. Unfortunately, the diagnostic improvement has not been accompanied by a therapeutic one in terms of both drugs and physical therapy. With regard to the latter, probably this could be due to the fact that patients with the same genetic disorder show different clinical features thus making it necessary to identify deficit-specific biomarkers to create a highly personalized rehabilitation program based on the patients’ needs. Moreover, until now the research effort has been mostly focused on lower limbs impairment but, according to the needs reported by patients, the upper limbs function is crucial as well [3]. For these reasons, quantification of upper extremity disabilities or motor adaptive strategies is essential for developing tailored upper limb rehabilitation for CMT patients.
Most of the studies concern the distal lower limb function, although some studies investigated also the function of spared proximal segment in order to assess possible motor strategies to recover the distal loss of function [4]. This approach could give important information also for the upper limb function that, according to recent studies focused on rehabilitation and patients’ needs [3, 5], has a great impact on daily and working life of CMT patients.
Electromyographic and kinematic analysis are commonly used in the current clinical practice to evaluate lower limbs in many neurological and orthopaedical conditions [6, 7]. Gait Analysis is a very useful instrument to assess gait disorders and to guide the possible therapies or rehabilitative interventions [8–10]. Instrumental indices calculated by surface electromyography (sEMG) have already proven to be a useful tool for identifying biological biomarkers to follow the disease progression of CMT [11, 12]. In fact, sEMG can be a suitable measure to study diseases affecting muscle and nerve, such as CMT, as it provides crucial information on the neuromuscular changes/progress induced by the disease [13].
One of the most critical clinical features of CMT is muscle weakness leading to an alteration of co-contraction mechanism between agonist and antagonist muscles [14], which is a neural strategy adopted by the central nervous system to stabilize joints and ensure movement accuracy [15]. sEMG-based co-contraction indices (CCI) are used in literature to quantify the muscle co-contraction, defined as the simultaneous activation of agonist and antagonist muscles during human movement [15], and have proven to be promising tools for quantifying motor deficit levels [16]. This muscle activation mechanism is a strategy for regulating joint stiffening. In fact, CCI can be considered as an alternative correlate for estimating joint stiffness, since the latter is difficult to measure experimentally or calculate computationally [17]. Two of the most common CCIs are suggested by Falconer and Winter et al. [18] and Rudolph et al. [19]. The former is based on the ratio between the less activated muscle and the total muscle activation and provides a numerical value related to the magnitude of co-contraction level, while the latter, calculated as the ratio between the less and the more active muscles multiplied by the total muscle activation, provides an estimation of the magnitude of co-activation as well as the relative activity observed in the two muscles. In the light of this feature, i.e. the possibility of accounting both for the similarity and the magnitude of the EMG signals, and in consideration of its greater correlation with the joint stiffness, the Rudolph index is the one most used in the literature [15, 20].
The demyelinating and axonal features of CMT could cause an imbalance in the muscle co-contraction during movements. This abnormal tightening of muscles results in stiffened joints, which cause deformities of the limbs [5]. Therefore, the quantification of this phenomenon using sEMG-based CCI in CMT subjects could allow a better understanding of how the disease progression alters the myoelectric activity of upper limb muscles. Few studies have investigated the muscle activations in the lower limb during dynamic conditions [21, 22], while for what concerns the upper limb, to our knowledge, no EMG-based movement data have been published yet.
To achieve this goal, the aim of this exploratory observational study was two-fold: (1) to characterize the muscle co-contractions of subjects with CMT1A and CMT1X compared to healthy subjects during upper limb motor tasks and (2) to analyze the concurrent validity of the sEMG-based index with clinical scales.
MATERIALS AND METHODS
Participants
We recruited CMT patients with a confirmed genetic diagnosis of CMT who were attending the multidisciplinary outpatient clinic for the diagnosis and treatment of inherited peripheral neuropathies at the IRCCS Ospedale Policlinico San Martino of Genoa, Italy. Exclusion criteria were: underage subjects, inflammatory arthritis, diabetes, hearing loss, uncontrolled pain, the presence of other neurological diseases or unrelated clinical conditions affecting motor functions and previous surgical interventions at the upper limb limiting joint ROM.
The protocol was approved by the local ethical committee (N. Registro CER Liguria: 113REG2017). All participants provided written informed consent to the study, which was conducted in accordance with the Helsinki Declaration.
Clinical evaluation
All subjects underwent a clinical evaluation by means of the Sollerman Hand Function Test (SHFT), executed following the published protocol, Short Form 36 (SF36), Disability of Arm, Shoulder and Hand (DASH) and CMT Examination Score (CMTES). We also assessed upper limb strength by mean of Medical Research Council (MRC) on the following muscles: deltoids (DEL), biceps (BIC), triceps (TRI), wrist (WE) and finger (FE) extensors, short abductor of the thumb (SAT), first interosseous (FI).
The SHFT is a standardized hand function test consisting of 20 activities of daily living [23]. Each tested hand is given a score (Sollerman score) ranging from 0 to 80 points, with a higher score indicating better hand function.
Thumb opposition was evaluated according to the Kapandji opposition score, which defines 10 stages of opposition, with full opposition scored as stage 10 [24, 25].
The CMTES is a subscore of the total CMTNS that includes 7 items based on patients’ symptoms and examination findings and excludes the electrophysiology, with a maximum total score of 28 points (indicating the worst condition) [26].
We completed the clinical assessment with the DASH and SF36 questionnaires for a subjective evaluation of upper limb disability and quality of life.
The DASH questionnaire consists of 30 questions that inquire about symptoms and functions of the upper limbs [27]. These provide a single main score, the DASH function/symptoms (DASH-FS) score, which is basically a summation of the responses. The questions test the degree of difficulty in performing a variety of physical activities because of arm, shoulder or hand problems. They also investigate the severity of pain, activity-related pain, tingling, weakness and stiffness and the effect of the upper limb problem on social activities, work, sleep and self-image. Higher scores of the DASH questionnaire indicate a more severe disability.
The SF36 total score (SF36-TOT) consists of 36 questions on the general health status of patients, with higher scores indicating a better health status. This questionnaire provides separate subscores, of which four are related to physical activity (Physical Functioning (PF), Role-Physical (RP), General Health (GH).
Instrumented clinical assessment
Dynamometer
The maximal isometric voluntary contraction of both hands was assessed by a hand-held dynamometer (Citec CT 3001, CIT Technics BV, Groningen, The Netherlands) measuring hand grip (DYN-HG) and tripod pinch (DYN-TP). Both measures were performed according to a standardized testing procedure [24, 28, 29].
SEGT
The sensor-engineered glove test (SEGT) was used according to a previously published protocol. It was used to evaluate finger opposition movements using motor sequences in a quantitative spatial-temporal way in both dominant (DH) and non-dominant hands (NDH). An “eyes-closed paradigm” was chosen to avoid possible confounding effects because of the integration of acoustic and visual information. The patients were instructed to execute finger opposition movements of different complexities: finger tapping (FT) sequence (opposition of thumb to index) and index-medium-ring-little (IMRL) sequence (opposition of thumb to index, medium, ring, and little finger) at maximum velocity. The tasks comprised the execution of a repetition of each sequence, lasting 30 seconds, with alternate hands. Data were processed with customized software from Glove Analyzer System which permits selection to acquisition and experimental protocol. The following parameters were measured: touch duration (TD) or contact time between thumb and another finger (in ms); inter-tapping interval (ITI) or time between the end of the contact of the thumb and another finger and the beginning of successive contact (in ms); movement rate (MR) [1/ (TD + ITI)] or frequency of complete motor task (in Hz). The MR has been recognized to be the most sensitive glove parameter to detect differences between subjects affected by CMT and controls [30]. Patients with some limitation of the range of motion of their hands or weakness were encouraged to try to complete the task or to make the efforts to perform at their best. The SEGT software calculated the total amount of touches and recorded any “errors” in the sequence.
Experimental setup
Participants were asked to perform different motor tasks, while they were seated on a chair, with his/her feet fully resting on the floor. During each task, the hand’s marker (end-effector) trajectory was recorded by an optoelectronic system (Vicon Motion Systems Ltd., Oxford, UK) with frequency of 100 Hz and then low-pass filtered at 6 Hz. The motor tasks were:
• Shoulder Abduction Task (SAT): starting from the rest position with the arm lying on the body side with the wrist in neutral position and fingers extended, subjects were asked to carry out the shoulder abduction movement (90 degrees).
• Elbow Flexion Task (EFT): starting from the rest position with the arm lying on the body side with the forearm supinated, subjects were asked to flex the arm until the hand was placed in front of the shoulder.
• Wrist Flexion Task (WFT): starting with the pronated forearm placed on a table with adjustable height and the hand open outside the edge of the table, subjects were asked to actively flex the wrist to the maximum.
• Wrist Extension Task (WET): starting with the pronated forearm placed on a table with adjustable height and the hand open outside the edge of the table, subjects were asked to actively extend the wrist to the maximum.
• Drinking Task: starting from the rest position where subjects were seated in front of the table with both hands placed on the table which had a glass placed at 400 mm from its edge aligned with the subject sagittal plane, subjects were required to reach and grasp for the glass with his/her arm (DGT, grasping phase) and to lift it from the table to the mouth (DLT, lifting phase).
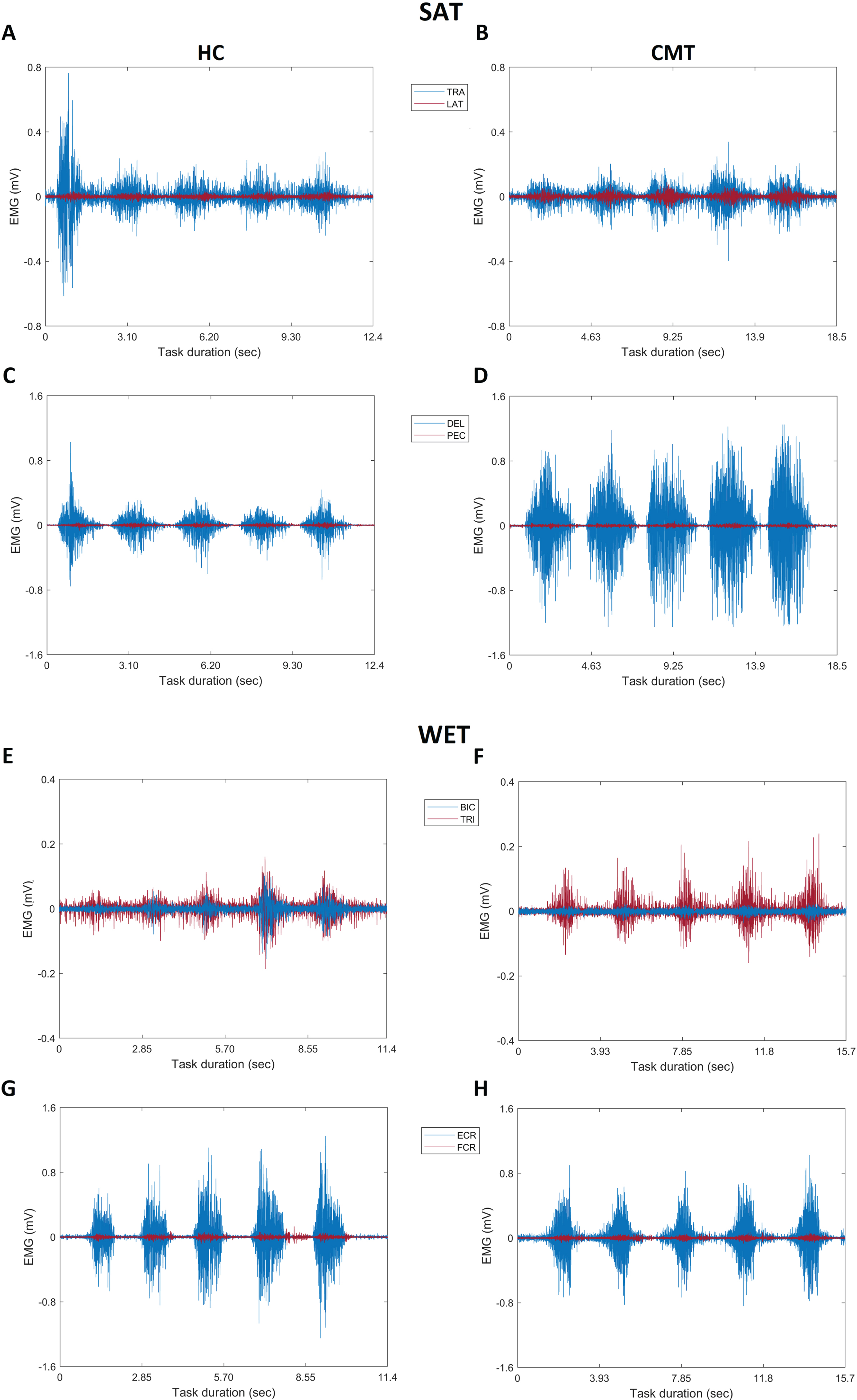
Surface electromyography was recorded using self-adhesive Ag-AgCl electrodes (Medtronic Kendall, diameter: 24 mm, diameter of the active part: 10 mm, bipolar configuration, interelectrode distance: 20 mm) and the system EMG wave/zerowire 8 channels (Cometa Srl, Italy) with a sampling frequency of 1000 Hz. The surface electrodes were placed over the muscles of interest, according to the anatomical guidelines [31] and SENIAM specifications [32]. The myoelectric activity of the 8 muscles was recorded from the following four muscle pairs: (1) trapezius and latissimus dorsi (TRA/LAT; axial muscle pair), (2) deltoid and pectoralis (DEL/PEC, axial-to-proximal muscle pair), (3) biceps and triceps brachialis (BIC/TRI, proximal muscle pair), and (4) flexor and extensor carpi radialis (FCR/ECR, distal muscle). Figure 1 shows an example of the collected raw EMG data for all the four antagonist muscle pairs in a healthy and CMT subject during the shoulder abduction and wrist extension tasks.
Fig. 1
Raw EMG signals of a healthy control and a subject with CMT. The panel on the left shows the raw EMG of the agonist (blue) and antagonist (red) muscle pairs of a healthy subject, while the one on the right shows the data of a subject with CMT. (A, B) report the data for the trapezius and latissimus dorsi and (C, D) for deltoid and pectoralis during the shoulder abduction task. (E, F) report the data for biceps and triceps brachialis and (G, H) for extensor and flexor carpi radialis during the wrist extension task. SAT: shoulder abduction task; WET: wrist extension task; TRA: trapezius; LAT: latissimus dorsi; DEL: deltoid; PEC: pectoralis, BIC: biceps brachialis; TRI: triceps brachialis; ECR: extensor carpi radialis; FCR: flexor carpi radialis.
The EMG probes were placed, unilaterally, on the dominant side of both HC subjects and CMT subjects selected according to MRC values of fingers extensors or, in case the latter were identical, of wrist extensors. The instants of initiation and termination of each repetition were computed from the velocity of the hand’s marker positioned. A movement was considered to begin when the marker velocity first became greater than 5% of the peak velocity and was considered to end after the speed dropped and remained below the 5% threshold again. Raw EMG signals were band-pass filtered (10–400 Hz, 2nd order), full wave rectified and then low-pass filtered (4 Hz, 4th order) in order to obtain the EMG linear envelopes [33]. Finally, all data were time-normalized to 100% of the movement duration and then, in order to not alter the variability in EMG, the EMG linear envelopes of each muscle was amplitude-normalized to their maximum value obtained across recorded different tasks [34, 35], thus also taking into account force-velocity and length-tension relationships in the muscles [19].
Co-contraction index (CCI)
Rudolph’s CCI in the version proposed by Don in 2007 (Equation 1) [36, 37], has been calculated to quantify the muscle co-contraction of the four antagonist muscle groups. This index estimates the level of simultaneous activations of muscles regardless of their action (i.e., a muscle pair can reverse their muscle activation in a specific time interval) [36].
(1)
In this expression (Equation 1) i represents the sample number, n indicates the number of data sample in the interval, while lowerEMGi and higherEMGi represent respectively the minimum and the maximum value at sample i of the EMG linear envelopes from the antagonist muscle pair [36]. The index is expressed in percentage (%) ranging from 0 to 100, where higher co-contraction values represent higher level of activation of both muscles [19]. The CCI was computed in each trial and subsequently averaged across the repetitions for each participant.
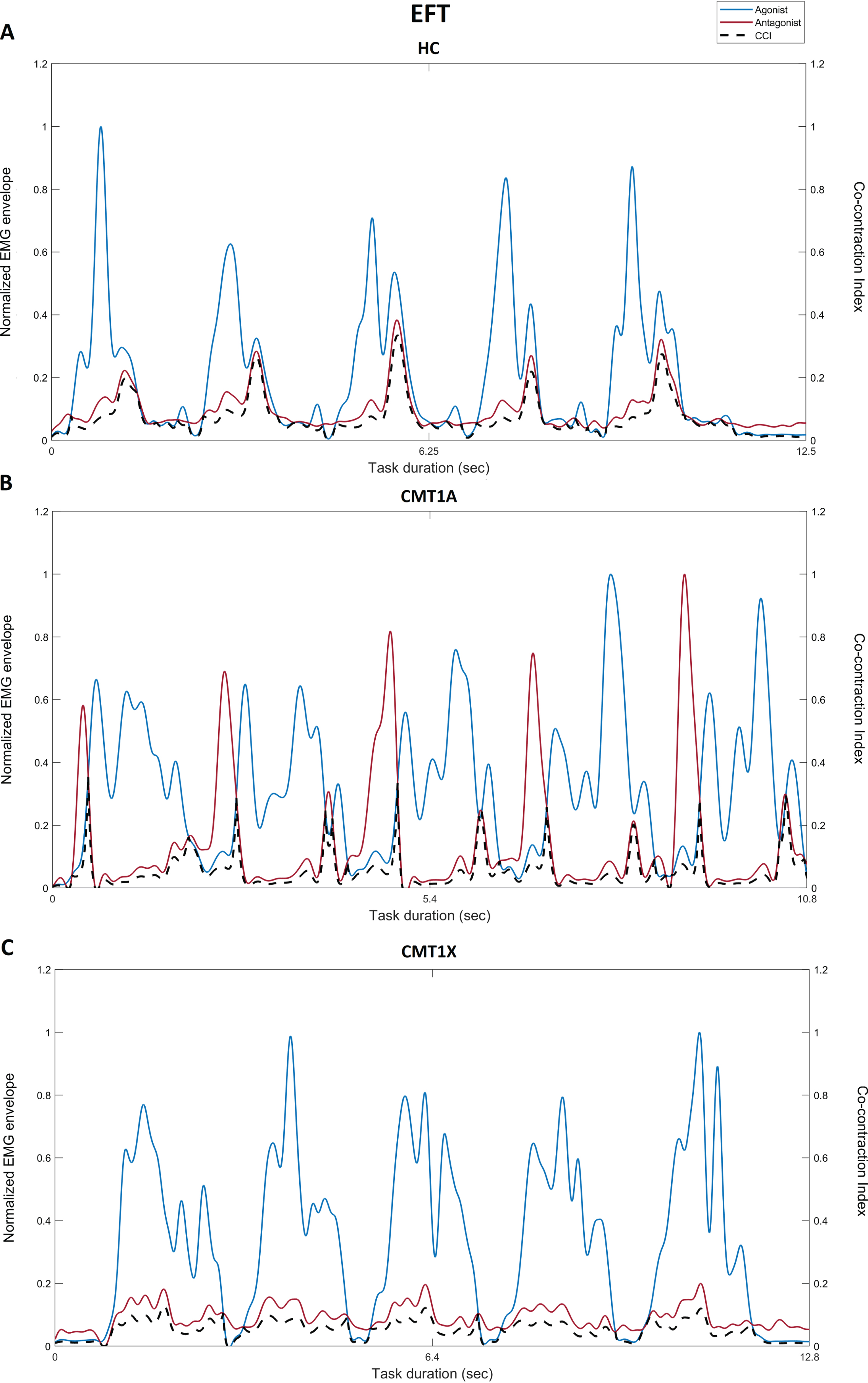
Magnitude of CCI is defined as the relative magnitude of simultaneous contraction between opposing muscles (Fig. 2) and is classified using terms such normal, increased or reduced magnitude with respect to the normative reference [38].
Fig. 2
Normalized EMG envelope and CCI of a healthy control, subject with CMT1A and CMT1X. Normalized EMG envelope for the biceps (agonist, blue line) and triceps brachialis (antagonist, red line) as well as the CCI (black dotted line) of the two muscles during the elbow flexion task for a healthy subject (A, HC), a subject with CMT1A (B, CMT1A) and a subject with CMT1X (C, CMT1X). EFT: elbow flexion task.
Kinematic analysis
The kinematics of the movement was assessed by calculating speed and smoothness variables during each repetition of the tasks and then averaged across the repetitions for each participant. Movement speed was computed using the spatial 3D coordinates of the hand marker as the ratio between the trajectory length at each time instant and the time spent. Higher values indicate faster movements. Smoothness was calculated by identifying the number of Peaks (i.e., movement units) of the tangential velocity of the hand’s marker, as velocity peaks indicate the alternation of deceleration and acceleration phases of the hand. Lower number of peaks indicates better smoothness [39].
Statistical analysis
Statistical analysis was performed using SPSS. Since the normality of the instrumental parameters data (co-contraction and kinematic indices) was satisfied (Shapiro-Wilk test), descriptive statistics are reported as means and standard deviations
For each task the differences between CMT1A, CMT1X and the Healthy Control (HC) groups were statistically tested using the parametric ANOVA test with Bonferroni correction for differences between unpaired groups.
Between-group (CMT1AvsHC, CMT1XvsHC, CMT1AvsCMT1X) effect sizes of the co-contraction index were examined by calculating the Cohen’s d value and was classified according to its absolute value as small (0.20–0.49), moderate (0.50–0.79) or large (≥0.80) [41].
Spearman’s correlation analysis was used to determine the relationship between CCIs and clinical scales in the whole CMT group. To interpret the magnitude of the correlation coefficients, the following absolute values-based guidelines from Campbell et al. [40] were followed, as very slight (0–0.19), slight (0.20–0.39), moderate (0.40–0.59), strong (0.60–0.79) and very strong (0.80–1).
P < 0.05 was selected to indicate significance in the statistical analysis carried out.
RESULTS
A total of 18 patients were enrolled. One subject was excluded because the diagnosis of CMT was not genetically confirmed. Three subjects were excluded because they did not undergo the kinematic evaluation. The mean age of the remaining 14 patients was 51.1±15.7, range 28–83 yo and the male/female ratio was 1.3. The CMT subtype distribution of participants in this study was 43% of CMT1A, 57% of CMT1X (Table 1). Only one person was left-handed. At the CMTES score, 7 subjects fell into the category of moderate disability, while the other 7 of mild disability [42]. No subjects had severe disability scores.
Table 1
Demographic and clinical characteristics of CMT patients
| CMT patients | |
| N | 14 |
| Age, Mean (SD) | 51.13 (15.7) |
| Sex, N(%) | |
| Male | 8 (57%) |
| Female | 6 (43%) |
| CMT type, N(%) | |
| CMT 1A | 6 (43%) |
| CMT 1X | 8 (57%) |
| DH, N(%) | |
| DH | 13 (93%) |
| NDH | 1 (7%) |
| CMTES | |
| Mean (SD) | 9.8 (3.04) |
| Range | 5–15 |
N: number; SD: standard deviation.
We also tested a group of 13 age matched healthy subjects with a mean age of 48.5±11.7, range 29–72 yo and male/female ratio of 0.8.
Comparison of motor performances among groups
All CMT performed the tasks independently, without any assistance. During all tasks no significant differences were found among groups for movement speed (Table 2). For what concern the movement smoothness, only CMT1X showed abnormal values with respect to HC during the drinking grasping task, indicating a reduction in the movement quality (P = 0.02).
Table 2
Mean and standard deviation of speed and smoothness parameters for healthy subjects and CMT subgroups during all the motor tasks
| Motor task | HC (N = 13) | CMT1A (N = 6) | CMT1X (N = 8) | |
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| Speed (m/s) | SAT | 0.616 (0.098) | 0.735 (0.020) | 0.737 (0.021) |
| EFT | 0.379 (0.097) | 0.315 (0.012) | 0.428 (0.019) | |
| WET | 0.135 (0.028) | 0.138 (0.023) | 0.159 (0.047) | |
| WFT | 0.143 (0.030) | 0.145 (0.045) | 0.171 (0.048) | |
| DGT | 0.183 (0.049) | 0.192 (0.041) | 0.184 (0.068) | |
| DLT | 0.205 (0.055) | 0.195 (0.048) | 0.220 (0.068) | |
| Smoothness (#peaks) | SAT | 1 (0) | 1 (0) | 1 (0) |
| EFT | 1 (0) | 1.02 (0.04) | 1 (0) | |
| WET | 1 (0) | 1 (0) | 1 (0) | |
| WFT | 1 (0) | 1.02 (0.04) | 1 (0) | |
| DGT | 1.03 (0.09) | 1.33 (0.38) | 1.5 (0.65)* | |
| DLT | 1.21 (0.32) | 1.17 (0.15) | 1.13 (0.25) |
SD: standard deviation; HC: healthy control; SAT: shoulder abduction task; EFT: elbow flexion task; WET: wrist extension task; WFT: wrist flexion task; DGT: drinking grasping task; DLT: drinking lifting task. The speed is reported in m/s, while the smoothness in peaks. *P < 0.05 indicates significant difference between HC and CMT1X.
Comparison of CCIs among groups
The CCIs values of all motor tasks are reported in Fig. 3 for CMT groups and HC.
Fig. 3
Co-contraction indices during upper extremity motor tasks in CMT groups and Healthy Controls. CCI values for all the muscle pairs during the following motor tasks: (A) shoulder abduction, (B) elbow flexion, (C) wrist extension, (D) wrist flexion, (E) drinking grasping and (F) drinking lifting. Bars charts and error bars represent, respectively, mean and standard error of CCIs for Healthy Controls (HC, white), CMT1A (gray) and CMT1X (black). *P < 0.05 indicates significant differences between CMT1A or CMT1X and HC, or between CMT1A and CMT1X. SAT: shoulder abduction task; EFT: elbow flexion task; WET: wrist extension task, WFT: wrist flexion task; DGT: drinking grasping task; DLT: drinking lifting task; TRA/LAT: trapezius and latissimus dorsi muscle pair; DEL/PEC: deltoid and pectoralis muscle pair, BIC/TRI: biceps and triceps brachialis muscle pair; FCR/ECR: flexor and extensor carpi radialis muscle pair.
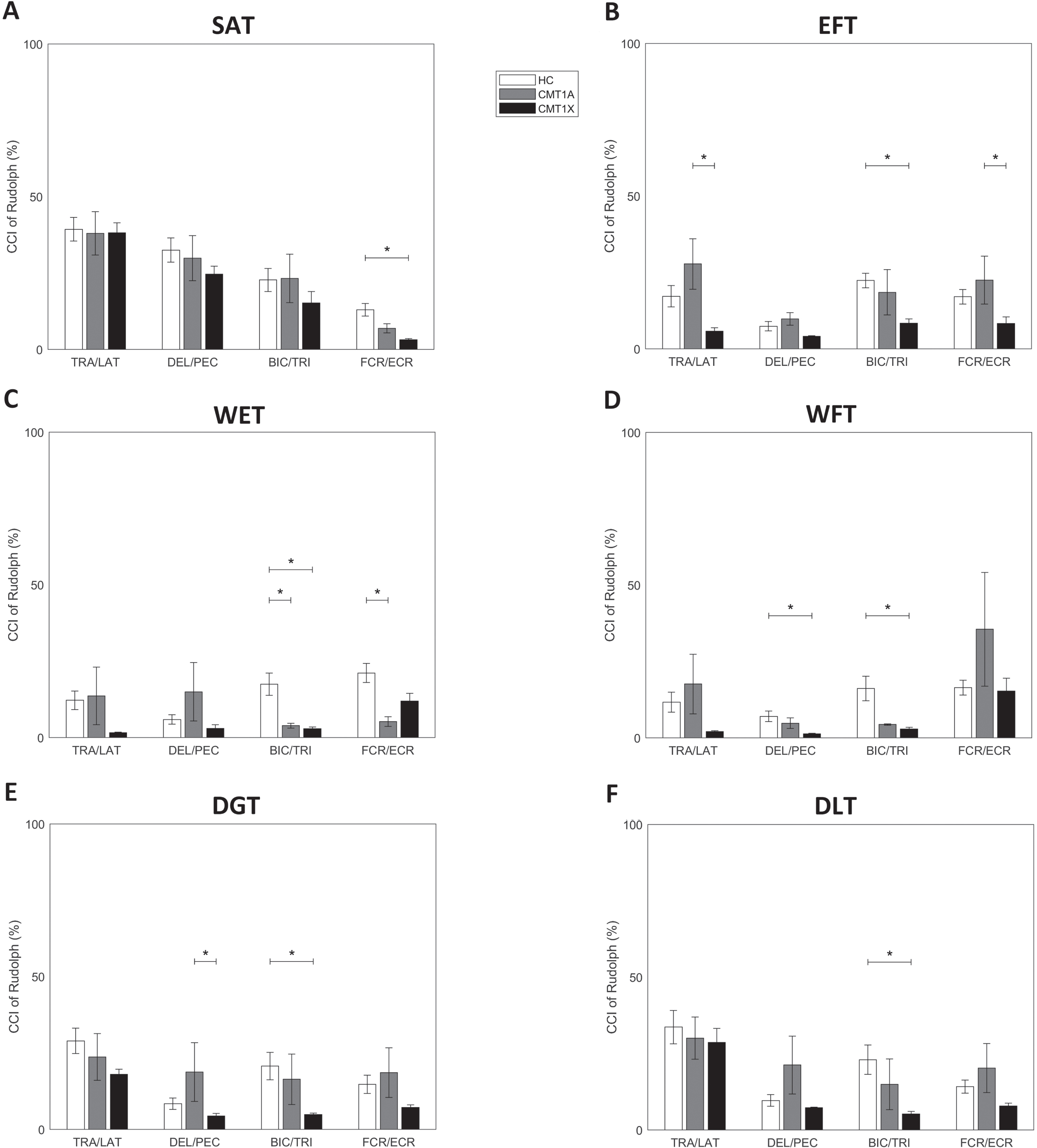
The CMT1X showed a reduction in the CCIs in all tasks for at least one muscle pair (Fig. 3A FCR/ECR Cohen’s d = 1.63, P < 0.01; 3B BIC/TRI Cohen’s d = 1.95, P < 0.01; 3 C BIC/TRI Cohen’s d = 1.38, P < 0.01; 3D DEL/PEC Cohen’s d = 1.14, P = 0.02 and BIC/TRI Cohen’s d = 1.15, P = 0.01; 3E BIC/TRI Cohen’s d = 1.23, P = 0.01; 3F BIC/TRI Cohen’s d = 1.29, P = 0.02), while the CMT1A only during the wrist extension task (Fig. 3 C BIC/TRI Cohen’s d = 1.22, P = 0.01 and FCR/ECR Cohen’s d = 1.63, P < 0.01).
CMT1A group showed a significant increase of the CCIs with respect to CMT1X for the axial muscle pair TRA/LAT during the elbow flexion task (Fig. 3B Cohen’s d = 1.66, P < 0.01), for the axial-to-proximal muscle pair DEL/PEC during the drinking grasping phase (Fig. 3E Cohen’s d = 0.94, P = 0.02), and for the distal muscle pair FCR/ECR during the elbow flexion task (Fig. 3B Cohen’s d = 1.07, P = 0.02).
Correlation between CCIs and clinical-based outcome measures
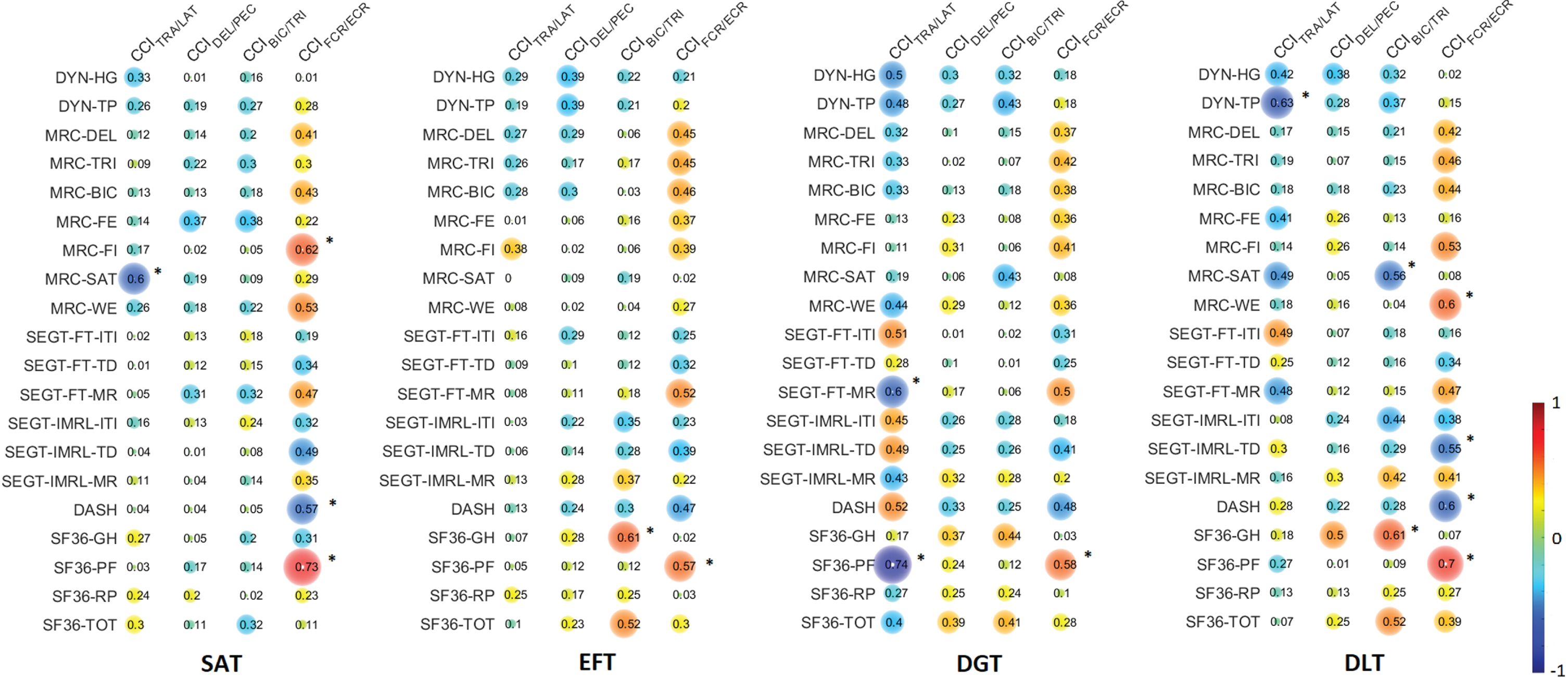
Figure 4 reports the correlation analysis between clinical outcomes and CCIs parameters. EMG metrics showed statistically significant correlations with the clinical outcomes. In particular, CCIFCR/ECR showed moderate-to-strong correlations with the following clinical scales: 1) DASH (disability, in SAT P = 0.03 and DLT P = 0.02), 2) MRC (distal muscle strength, FI item in SAT P = 0.02, WE item in DLT P = 0.02), 3) SF36-PF (physical functioning related to the Health-Related Quality of Life, in SAT P < 0.01, EFT P = 0.03, DGT P = 0.03, DLT P = 0.01) and 4) SEGT-IMRL-TD (finger opposition movements quality, in DLT P = 0.04). CCIBIC/TRI showed strong correlation with the general health status of the Health-Related Quality of Life (SF36-GH in EFT P = 0.02 and DLT P = 0.02) and moderate correlation with distal muscle strength (MRC-SAT in DLT P = 0.04). CCITRA/LAT showed strong correlation with distal muscle strength (MRC-SAT in SAT P = 0.02), finger opposition movements quality (SEGT-FT-MR in DGT P = 0.03), physical functioning related to the Health-Related Quality of Life (SF36-PF in DGT P < 0.01), and the pinch strength (DYN-TP in DLT P = 0.02).
Fig. 4
Correlation analysis between clinical scores and EMG-based co-contraction assessment. Spearman’s correlation coefficients between CCI and clinical scales and their sub-items in the whole CMT group during the motor tasks of shoulder abduction, elbow flexion, drinking grasping and drinking lifting. The dimension and the pixel intensity of circles represent the correlation coefficients, within the range from –1 to 1 as indicated by the legend at the bottom right. Significant correlations are indicated with *P < 0.05 (Spearman’s correlation test). DYN-HG: hand grip dynamometer; DYN-TP: tripod pinch dynamometer; MRC: Medical Research Council; MRC-DEL: deltoid; MRC-TRI: triceps; MRC-BIC: biceps; MRC-FE: finger extensor; MRC-FI: first interosseous; MRC-SAT: short abductor of the thumb; MRC-WE: wrist extensor; SEGT: Sensor-Engineered Glove Test; FT: finger tapping; IMRL: index-medium-ring-little; ITI: inter-tapping interval; TD: touch duration; MR: movement rate; SF36: Short Form 36; GH: General Health; PF: Physical Functioning; RP: Role-Physical; TOT: total score; SAT: shoulder abduction task; EFT: elbow flexion task; DGT: drinking grasping task; DLT: drinking lifting task; TRA/LAT: trapezius and latissimus dorsi; DEL/PEC: deltoid and pectoralis, BIC/TRI: biceps and triceps brachialis; FCR/ECR: flexor and extensor carpi radialis.
DISCUSSION
In this study, we investigated the sensitivity of an EMG-based metric to detect differences of the motor performance among CMT subtypes and healthy subjects. Different methods have been introduced in the literature to quantify muscle co-contraction, however a gold standard has not yet been established [43]. Among the different CCI formulations, Rudolph’s CCI is the one most commonly used by clinical researchers to quickly and easily assess the simultaneous activation of the agonist-antagonist muscle from sEMG data [15]. Specifically, this index provides values which include both the temporal and magnitude components of EMG signals of antagonistic muscles [19], thus overcoming the limitations of the other CCI formulations, relating only to the intensity of simultaneous muscle activation. In addition, this index avoids divide-by-zero errors [19] and does not require a-priori classification of muscles in agonist and antagonist [36].
Our findings highlighted that the EMG-based analysis here presented allow to characterize the motor behavior of the CMT persons with respect to the normative reference during motor tasks typically involved in activities of daily living.
Persons with CMT recruited in this study were in a mild-to-moderate status of severity disease, with no difference in CMTES and SHFT between the two groups according to the CMT subtypes: CMT1A and CMT1X. Kinematic results showed that CMT1A and CMT1X persons, overall, performed the motor tasks at similar movement speed and smoothness compared to the control group, except for the reaching movement of the drinking grasping task where the CMT1X movement quality was lower than the reference one (Table 2).
The most marked difference between the two CMT groups and the control group, was found in the wrist extension task, where both CMT1A and CMT1X showed a significant reduction of muscle co-contraction in the proximal muscle pairs. In addition, CMT showed also a marked deficit in the distal synergy, especially CMT1A (Fig. 3 C), while no alterations on the proximal-to-axial and axial muscle pairs were found. This is in line with the characteristics of CMT that most commonly causes progressive muscle weakness starting from the body extremities up to the mid-axial part, reaching a level of impairment mild to moderate for the former and slight for the latter. The reduction in the CMT co-contraction indices was probably the result of degeneration of axons and myelin of nerves. This damage causes dispersion in the muscle activation signal by reducing the subjects’ ability to modulate the coactivation of agonist and antagonist muscles around the articular joints. During dynamic movements the agonist muscle requires more effort to move the limb with respect to the antagonist one. Therefore, a minor recruitment of agonist muscle, can appear as an increased activity of the antagonist muscle, resulting in reduced CCI. This co-contraction deficit was particularly evident in CMT1X subjects, who showed a reduction in CCI indices in all functional movements for at least one muscle pair. These subjects may have had a greater damage of the motor nerve conduction compared to the CMT1A subjects, whose disease progression is slower when compared to other forms of CMT [44]. Interestingly, CMT1A showed an increased co-contraction with respect to the CMT1X, especially for the more proximal muscle pairs with a lower level of conduction damage. These features could be the result of a structural reorganization in the brain of CMT1A patients, mostly probably involving the anterior cerebellum and possibly reflecting compensatory mechanisms in response to peripheral nerve pathology [45]. It is well known that co-contracting muscles is an effective strategy for providing articular joints stability by modulating mechanical impedance and thereby allowing the central nervous system to develop adaptive strategy of functioning movement [46]. A recent study found that distributed cerebellar-parietal-frontal network functions are able to regulate muscle co-contraction with the cerebellum as its key component [46]. Therefore, the CMT1A-induced changes in the cerebellar cortex could be the origin of the increased co-contraction in these subjects as compensatory strategy used to reduce movement instability caused by muscle weakness [47, 48]. However, literature evidences report that CMT1A subjects are usually less compromised in the upper limb compared to CMT1X. Therefore, CMT1A subjects may still be able to perform an effective movement although with altered motor control and, probably, a multidisciplinary examination may be able to capture these subtle differences in the impairment, not detectable by clinical scales.
This study found correlations between indices of co-contraction and clinical signs of CMT, especially for the tasks related to the ADLs (SAT and DLT). The negative correlation between upper limb disability (DASH) and distal co-contraction (CCIFCR/ECR) indicates that the lower the upper limb disability is, the lower the muscle co-contraction deficit results. This is compatible with the characteristics of the disease related to the first symptoms onset which mostly involves the distal muscle part with abnormalities of the nerve conduction. In fact, reduced nerve conduction velocities (more deficit) can result in reduced values of CCI, while greater-to-normal conduction velocities in greater values of CCI (less deficit).
The association between the maximum voluntary contraction (DYN-TP) and axial muscle co-contraction (CCITRA/LAT) instead probably reflects the disease-induced compensatory strategy, as CMT did not show a reduction of the CCI but rather an increase, especially CMT1A (Fig. 3). In fact, the lower the distal muscle strength is, the higher the axial muscle co-contraction results. The correlation between SF36-PF and SEGT-FT-MR and CCITRA/LAT can be interpreted from the same point of view: the better the subject health status and movement ability are, the lower the need for compensation strategy is. While the other correlation of the CCIFCR/ECR with the clinical scale relative to muscle strength (MRC), global health status (SF36-PF and DASH) and movement ability (SEGT-IMRL-TD) indicate that the better the conservation of the distal physiological co-contraction (higher CCIFCR/ECR) is, the better the clinical evaluation results.
In conclusion, the CCI may be more sensitive in early recognition of an altered motor pattern even in subjects with mild impairment or small changes over time. These aspects are very relevant in a slow-course disease, where patients often complain of distal weakness or difficulties in common activities of daily living without the most used clinical scales being able to capture these variations. The implications are important to plan a tailored rehabilitation treatment to preserve strength and dexterity and to perform a better and more complete assessment even in clinical trials, since until now there is no therapy available to cure CMT patients.
Limitations
Despite the novelty of this study, the small sample size could limit the generalization of the results. However, the Cohen’s d values of the CCIs showed large effect sizes in the contrast analysis, both between CMT groups and between a sub-group of CMT (CMT1A or CMT1X) and HC. An a-posteriori power analysis was conducted on the basis of the CCI effect sizes of the proximal muscle pair BIC/TRI between CMT sub-groups and the control group during the WET. Fixed a ratio β/α equal to 4, the study mean power was calculated and resulted 0.82, indicating that the sample size of the present study was adequate to support future investigations of the use of CCIs as potential index in CMT to quantify disease-specific co-contraction features in CMT.
CONCLUSIONS
The results of this study indicate that the EMG-based indices are promising measures to detect the initial deterioration of agonist-antagonist muscle control associated to CMT disease, even when the movement kinematics is not yet altered with respect to the healthy subjects. In addition, the analysis here presented was able to quantify deficits and compensation strategies characteristic of the disease, which were adopted to regulate the joint movement in order to obtain a better performance to such an extent that it was comparable to that of the healthy subjects. The results obtained by this study contribute to the identification of outcome measurements to monitor CMT disease, to plan the training of CMT subjects and to detect the rehabilitation-induced changes.
ACKNOWLEDGMENTS
Finally, we thank all the persons who participated in the trial and the colleagues of the CMT-RF Study Group.
FUNDING
The work of MF was supported by #NEXTGENERATIONEU (NGEU) and funded by the Ministry of University and Research (MUR), National Recovery and Resilience Plan (NRRP), project MNESYS (PE0000006)—A Multiscale integrated approach to the study of the nervous system in health and disease (DN. 1553 11.10.2022).
This work was also supported by the Italian Ministry of Health, RICERCA CORRENTE.
CONFLICTS OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY STATEMENT
The data that support the findings of this study are available from the corresponding author upon reasonable request.
APPENDIX 1: CMT-RF STUDY GROUP
Marco Germanotta (IRCCS Fondazione Don Carlo Gnocchi Onlus, Florence, Italy); Costanza Pazzaglia (UOC Neuroriabilitazione ad Alta Intensità, Fondazione Policlinico Universitario A. Gemelli IRCCS); Sara Massucco (Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genoa, Italy; Department of Neuroscience, IRCCS Ospedale Policlinico San Martino, Genoa, Italy); Lucio Marinelli (Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genoa, Italy; Department of Neuroscience, IRCCS Ospedale Policlinico San Martino, Genoa, Italy); Marina Grandis (Department of Neuroscience, Rehabilitation, Ophthalmology, Genetics, Maternal and Child Health, University of Genoa, Italy; Department of Neuroscience, IRCCS Ospedale Policlinico San Martino, Genoa, Italy).
REFERENCES
[1] | Reynaud V , Conforto I , Givron P , Clavelou P , Cornut-Chauvinc C , Taithe F , et al. Multidimensional evaluation is necessary to assesshand function in patients with Charcot-Marie-Tooth disease type 1A. Ann Phys Rehabil Med. (2021) ;64: :101362.https://doi.org/10.1016/j.rehab.2020.02.002. |
[2] | Videler AJ , Beelen A , van Schaik IN , de Visser M , Nollet F Limited upper limb functioning has impact on restrictions in participation and autonomy of patients with hereditary motor and sensory neuropathy 1a. J Rehabil Med. (2009) ;41: :746–50.https://doi.org/10.2340/16501977-0419. |
[3] | Padua L , Pazzaglia C , Schenone A , Ferraro F , Biroli A , Esposito C , et al. Rehabilitation for Charcot Marie tooth: A survey study of patients and familiar/caregiver perspective and perception of efficacy and needs. Eur J Phys Rehabil Med. (2014) ;50: , 25–30. |
[4] | Ferrarin M , Bovi G , Rabuffetti M , Mazzoleni P , Montesano A , Moroni I , et al. Reliability of instrumented movement analysis as outcomemeasure in Charcot–Marie–Tooth disease: Results from amultitask locomotor protocol. Gait Posture. (2011) ;34: :36–43.https://doi.org/10.1016/j.gaitpost.2011.03.007. |
[5] | Mori L , Schenone C , Cotellessa F , Ponzano M , Aiello A , Lagostina M , et al. Quality of life and upper limb disability inCharcot-Marie-Tooth disease: A pilot study. Front Neurol. (2022) ;13: :964254.https://doi.org/10.3389/fneur.2022.964254. |
[6] | Papagiannis GI , Triantafyllou AI , Roumpelakis IM , Zampeli F , Garyfallia Eleni P , Koulouvaris P , et al. Methodology of surface electromyography in gait analysis: Review of the literature. J Med Eng Technol. (2019) ;43: :59–65.https://doi.org/10.1080/03091902.2019.1609610. |
[7] | Celik Y , Stuart S , Woo WL , Godfrey A Gait analysis in neurologicalpopulations: Progression in the use of wearables. Med Eng Phys. (2021) ;87: :9–29.https://doi.org/10.1016/j.medengphy.2020.11.005. |
[8] | Baker R Gait analysis methods in rehabilitation. J Neuroeng Rehabil. (2006) ;3: :4.https://doi.org/10.1186/1743-0003-3-4. |
[9] | Baker R , Esquenazi A , Benedetti MG , Desloovere K Gait analysis: Clinical facts. Eur J Phys Rehabil Med. (2016) ;52: , 560–74. |
[10] | Klöpfer-Krämer I , Brand A , Wackerle H , Müßig J , Kröger I , Augat P Gait analysis – Available platforms for outcome assessment. Injury. (2020) ;51: :S90–6.https://doi.org/10.1016/j.injury.2019.11.011. |
[11] | Lencioni T , Piscosquito G , Rabuffetti M , Bovi G , Di Sipio E , Diverio M , et al. Responsiveness of gait analysis parameters in a cohort of 71 CMT subjects. Neuromuscul Disord. (2017) ;27: :1029–37.https://doi.org/10.1016/j.nmd.2017.07.003. |
[12] | Noto Yichi , Watanabe K , Holobar A , Kitaoji T , Tsuji Y , Kojima Y , et al. High-density surface electromyography to assess motor unit firing rate in Charcot-Marie-Tooth disease type 1A patients. Clinical Neurophysiology. (2021) ;132: :812–8.https://doi.org/10.1016/j.clinph.2020.11.040. |
[13] | Campanini I , Disselhorst-Klug C , Rymer WZ , Merletti R Surface EMG in clinical assessment and neurorehabilitation: Barriers limiting its use. Front Neurol. (2020) ;11.https://doi.org/10.3389/fneur.2020.00934. |
[14] | Stino AM , Atway S , Anthony M , Kline D , Kissel JT Foot measures in patients with pes cavus with and without charcot-marie-tooth disease: A pilot study. Muscle Nerve. (2019) ;59: :122–5.https://doi.org/10.1002/mus.26309. |
[15] | Li G , Shourijeh MS , Ao D , Patten C , Fregly BJ How well do commonly used co-contraction indices approximate lower limb joint stiffness trends during gait for individuals post-stroke? Front Bioeng Biotechnol. (2021) ;8. https://doi.org/10.3389/fbioe.2020.588908. |
[16] | Bandini V , Carpinella I , Marzegan A , Jonsdottir J , Frigo CA , Avanzino L , et al. Surface-electromyography-based co-contraction index for monitoring upper limb improvements in post-stroke rehabilitation: A pilot randomized controlled trial secondary analysis. Sensors. (2023) ;23: :7320.https://doi.org/10.3390/s23177320. |
[17] | Pfeifer S , Vallery H , Hardegger M , Riener R , Perreault EJ Model-based estimation of knee stiffness. IEEE Trans Biomed Eng. (2012) ;59: :2604–12.https://doi.org/10.1109/TBME.2012.2207895. |
[18] | Falconer K , Winter DA Quantitative assessment of co-contraction at the ankle joint in walking. Electromyogr Clin Neurophysiol. (1985) ;25: , 135–49. |
[19] | Rudolph KS , Axe MJ , Snyder-Mackler L Dynamic stability after ACLinjury: Who can hop? Knee Surgery, Sports Traumatology, Arthroscopy. (2000) ;8: :262–9.https://doi.org/10.1007/s001670000130. |
[20] | Falk J , Strandkvist V , Pauelsen M , Vikman I , Nyberg L , Röijezon U Increased co-contraction reaction during asurface perturbation is associated with unsuccessful postural control among older adults. BMC Geriatr. (2022) ;22: :438.https://doi.org/10.1186/s12877-022-03123-2. |
[21] | Lencioni T , Piscosquito G , Rabuffetti M , Sipio E Di , Diverio M , Moroni I , et al. Electromyographic and biomechanical analysis ofstep negotiation in Charcot Marie Tooth subjects whose level walk isnot impaired. Gait Posture. (2018) ;62: :497–504.https://doi.org/https://doi.org/10.1016/j.gaitpost.2018.04.014. |
[22] | Kuciel NM , Konieczny GK , Oleksy Ł , Wrzosek Z Lower extremity muscles activity in standing and sittingposition with use of sEMG in patients suffering from Charcot-Marie-Tooth syndrome. Neurol Neurochir Pol. (2016) ;50: :195–9.https://doi.org/10.1016/j.pjnns.2016.01.011. |
[23] | Sollerman C , Ejeskär A Sollerman hand function test: A standardised method and its use in tetraplegicpatients. Scand J Plast Reconstr Surg Hand Surg. (1995) ;29: :167–76.https://doi.org/10.3109/02844319509034334. |
[24] | Videler AJ , Beelen A , van Schaik IN , Verhamme C , van den Berg LH , de Visser M , et al. Tripod pinch strength and thumb opposition are the major determinants of manual dexterity in Charcot–Marie–Tooth disease type 1A. Journal of Neurology, Neurosurgery & Amp; Psychiatry. (2010) ;81: :828–33.https://doi.org/10.1136/jnn2009.187302. |
[25] | Kapandji A Cotation clinique de l’opposition et de lacontre-opposition du pouce. Annales de Chirurgie de La Main. (1986) ;5: :67–73.https://doi.org/https://doi.org/10.1016/S0753-9053(86)80053-9. |
[26] | Fridman V , Sillau S , Acsadi G , Bacon C , Dooley K , Burns J , et al. A longitudinal study of CMT1A using Rasch analysis based CMT neuropathy and examination scores. Neurology. (2020) ;94: :e884 LP-e896.https://doi.org/10.1212/WNL.0000000000009035. |
[27] | Eklund E , Svensson E , Häger-Ross C Hand function and disability of the arm, shoulder and hand inCharcot-Marie-Tooth disease. Disabil Rehabil. (2009) ;31: :1955–62.https://doi.org/10.1080/09638280902874170. |
[28] | Solari A , Laurà M , Salsano E , Radice D , Pareyson D Reliability of clinical outcome measures in Charcot-Marie-Tooth disease. Neuromuscular Disorders. (2008) ;18: :19–26.https://doi.org/https://doi.org/10.1016/j.nmd.2007.09.006. |
[29] | Svensson E , Häger-Ross C Hand function in Charcot Marie Tooth:Test retest reliability of some measurements. Clin Rehabil. (2006) ;20: :896–908.https://doi.org/10.1177/0269215506072184. |
[30] | Alberti MA , Mori L , Francini L , Poggi I , Monti Bragadin M , Bellone E , et al. Innovative quantitative testing of hand function in Charcot-Marie-Tooth neuropathy. J Peripher Nerv Syst. (2015) ;20: :410–4.https://doi.org/10.1111/jns.12150. |
[31] | Criswell Eleanor. CRAM’s Introduction to Surface Electromyography. 2nd edition. Sudbury: Jones & Bartlett Learning; 2011. |
[32] | Hermens HJ , Freriks B , Disselhorst-Klug C , Rau G Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. (2000) ;10: :361–74.https://doi.org/10.1016/s1050-6411(00)00027-4. |
[33] | Charafeddine J , Pradon D , Chevallier S , Alfayad S , Khalil M Neuromotor strategy of gait rehabilitation for lower-limb spasticity. International Conference on Advances in Biomedical Engineering, ICABME, Tripoli, Lebanon: IEEE; 2019, p. 1-4.https://doi.org/10.1109/ICABME47164.2019.8940263. |
[34] | Yang JF , Winter DA Electromyographic amplitude normalization methods: Improving their sensitivity as diagnostic tools in gait analysis. Arch Phys Med Rehabil. 1984; 65. |
[35] | Gribble PL , Mullin LI , Cothros N , Mattar A Role of cocontraction in arm movement accuracy. J Neurophysiol. (2003) ;89: :2396–405.https://doi.org/10.1152/jn.01020.2002. |
[36] | Di Giminiani R , Giovannelli A , Capuano L , Izzicupo P , Di Blasio A , Masedu F Neuromuscular strategies in stretch–shortening exercises with increasing drop heights: The role of muscle coactivation in leg stiffness and power propulsion. Int J Environ Res Public Health. (2020) ;17: :1–15.https://doi.org/10.3390/ijerph17228647. |
[37] | Don R , Ranavolo A , Cacchio A , Serrao M , Costabile F , Iachelli M , et al. Relationship between recovery of calf-muscle biomechanicalproperties and gait pattern following surgery for achilles tendonrupture. Clin Biomech (Bristol, Avon). (2007) ;22: :211–20.https://doi.org/10.1016/j.clinbiomech.2006.10.001. |
[38] | Rosa MCN , Marques A , Demain S , Metcalf CD Lower limb co-contractionduring walking in subjects with stroke: A systematic review. Journalof Electromyography and Kinesiology. (2014) ;24: :1–10.https://doi.org/10.1016/J.JELEKIN.2013.10.016. |
[39] | Rohrer B , Fasoli S , Krebs HI , Hughes R , Volpe B , Frontera WR , et al. Movement smoothness changes during stroke recovery. Journal of Neuroscience. (2002) ;22: :8297–304.https://doi.org/10.1523/jneurosci.22-18-08297.2002. |
[40] | Campbell MJ , Swinscow TDV Statistics at Square One. Thomas, D.V., Ed.; Wiley-Blackwell/BMJ Books: Hoboken, NJ, USA, 2009; ISBN 9781405191005; n.d. |
[41] | Cohen J Statistical power analysis. Curr Dir Psychol Sci. (1992) ;1: :98–101.https://doi.org/10.1111/1467-8721.ep10768783. |
[42] | Shy ME , Blake J , Krajewski K , Fuerst DR , Laura M , Hahn AF , et al. Reliability and validity of the CMT neuropathy score as a measure ofdisability. Neurology. (2005) ;64: :1209–14https://doi.org/10.1212/01.WNL.0000156517.00615.A3. |
[43] | Di Nardo F , Morano M , Strazza A , Fioretti S Muscle co-contraction detection in the time–frequency domain. Sensors. (2022) ;22: :4886.https://doi.org/10.3390/s22134886. |
[44] | Fridman V , Bundy B , Reilly MM , Pareyson D , Bacon C , Burns J , et al. CMT subtypes and disease burden in patients enrolled in the Inherited Neuropathies Consortium natural history study: A cross-sectional analysis. J Neurol Neurosurg Psychiatry. (2015) ;86: :873–8.https://doi.org/10.1136/jnnp-2014-308826. |
[45] | Pontillo G , Dubbioso R , Cocozza S , Tozza S , Severi D , Iodice R , et al. Brain plasticity in Charcot-Marie-Tooth Type 1A patients? A combined structural and diffusion MRI study. Front Neurol. (2020) ;11: :795.https://doi.org/10.3389/fneur.2020.00795. |
[46] | Babadi S , Vahdat S , Milner TE Neural substrates of muscle co-contraction during dynamic motor adaptation. J Neurosci. (2021) ;41: :5667–76.https://doi.org/10.1523/JNEUROSCI.2924-19.2021. |
[47] | Mari S , Serrao M , Casali C , Conte C , Martino G , Ranavolo A , et al. Lower limb antagonist muscle co-activation and its relationship with gait parameters in cerebellar ataxia. The Cerebellum. (2014) ;13: :226–36.https://doi.org/10.1007/s12311-013-0533-4. |
[48] | Griffin TM , Guilak F The role of mechanical loading in the onset and progression of osteoarthritis. Exerc Sport Sci Rev. (2005) ;33: :195–200.https://doi.org/10.1097/00003677-200510000-00008. |


