
Open Bite Malocclusion and Orofacial Dysfunction in Patients with Myotonic Dystrophy Type 1 and Duchenne Muscular Dystrophy
Abstract
Open bite (OB) is a common malocclusion in individuals with orofacial dysfunction and syndromes, especially in neuromuscular diseases.
Objectives:
The objectives were to explore the prevalence of OB in myotonic dystrophy type 1 (DM1) and Duchenne muscular dystrophy (DMD) and to create and compare orofacial dysfunction profiles.
Methods:
In this database study, 143 individuals with DM1 and 99 with DMD were included. The Mun-H-Center questionnaire and observation chart were used together with the Nordic Orofacial Test –Screening (NOT-S) to create orofacial dysfunction profiles. OB was categorised as: lateral (LOB); anterior (AOB); severe anterior (AOBS); or both types of anterior OB (AOBTot). Descriptive and multivariate statistics were used to compare the OB prevalence and to study associations with orofacial variables, respectively.
Results:
There was a statistically significant difference in OB prevalence between the DM1 (37%) and DMD (49%) groups (p = 0.048). LOB was seen in < 1% of DM1 and 18% of DMD. LOB was associated with macroglossia and closed mouth posture, AOB with hypotonic lips, and open mouth posture and AOBS with hypotonic jaw muscles. The orofacial dysfunction profiles showed similar patterns, although the mean NOT-S total scores for DM1 and DMD were 4.2±2.8 (median 4.0, min-max 1–8) and 2.3±2.0 (median 2.0, min-max 0–8), respectively.
Limitations:
The two groups were not age- or gender-matched.
Conclusion:
OB malocclusion is common in patients with DM1 and DMD and is associated with different types of orofacial dysfunction. This study highlights the need for multi-disciplinary assessments to support tailored treatment strategies that improve or sustain orofacial functions.
INTRODUCTION
Open bite (OB) is one of the most common malocclusions in patients with orofacial dysfunction (OD) and syndromes [1], and in patients with intellectual and developmental disabilities [2, 3]. Weak orofacial muscles, anterior positioning of the tongue, mouth breathing, and open mouth posture (OMP) are common findings in patients with open bites [4, 5]. Myotonic dystrophy type 1 (DM1) and Duchenne muscular dystrophy (DMD) are progressive myopathies in which malocclusion, particularly lateral and anterior open bites, are common [6] Although both diseases result in muscle weakness, they differ with respect to pathogenetic mechanisms, course of the disease and clinical expression.
DM1 is a rare, inherited, autosomal-dominant disease caused by a trinucleotide repeat (CTG) in the DMPK-gene on chromosome 19q (19q13.3), which codes for the myosin kinase expressed in skeletal muscle. DM1 affects 13–19/100 000 inhabitants in Sweden [7]. The classification of the disease is based on the age at onset and severity of symptoms, dividing them into four main subgroups: congenital, childhood, adult, and late onset. The pattern with which the orofacial muscles are affected often gives individuals with DM1 a characteristic facial appearance. Ptosis of the eyelids, open mouth at rest, hypotonic lips (HL), and weak jaw-elevating muscles are common facial traits [8]. The tongue has been found to be less affected than the other orofacial muscles in patients with DM1 [9]. The craniofacial morphology of patients with DM1 is characterised by a retrognathic profile, large gonial angle, and a steep mandibular plane with a long lower-facial height [10]. Young patients with congenital or childhood onset DM1 display an altered craniofacial morphology already at an early stage, which does not seem to improve during growth [11]. Malocclusions are common in both children and adults and previous studies have reported cases of class II occlusion, class III occlusion, anterior open bite and lateral cross-bite [10, 11]. One theory that has been proposed to explain this appearance is that an open mouth posture with the mandible and tongue in a lowered position allows over-eruption of the posterior teeth, as well as stretching of the facial muscles, creating an imbalance between the intra-oral and extra-oral pressures [10]. Although orthodontic treatment in combination with orthognathic surgery often can correct severe malocclusions, the muscular imbalance and weakness may interfere negatively with the long-term stability of the treatment result [12–14].
Duchenne Muscular dystrophy is a rare X-linked, inherited, recessive disease involving a mutation in the dystrophin gene (Xp21.2) that affects 7/100,000 male inhabitants [15]. Dystrophin is an intracellular muscle fibre protein, the function of which is to stabilise the muscle membrane during contraction. The mutation in the dystrophin gene causes the encoded protein to be dysfunctional, resulting in breakdown of the cellular membrane, muscle atrophy, and replacement of the muscle with fat and fibrous tissue [16]. Different treatment strategies, such as corticosteroids, have been shown to prolong the ambulatory stage, quality of life, and life expectancy of individuals with DMD [16, 17]. The continuous replacement of muscle fibres with adipose tissue leads to hypertrophy of the tongue, sometimes resulting in macroglossia [18]. The cheeks appear full due to the side-effects of corticosteroid treatment, and possibly also due to tissue replacement with fat. The orofacial dysfunction coincides with deterioration of the general health of the patients with DMD [19]. A previous study has found that the jaw muscles start to diminish 2 years prior to the perioral muscles [20]. Another report has described how the muscles of the submental group and the tongue are affected only in the late non-ambulatory stage of DMD [18]. Several studies have noted a tendency towards a skeletal class III pattern in patients with DMD over time [19, 21]. One study has shown that the maxillary plane angle (NL/NSL) is larger than normal, while the anterior upper face height (NSp) is smaller, as compared with unaffected controls [21]. Most individuals with DMD develop a dentoalveolar malocclusion. DMD patients often present with an increase in width of both dental arches, and especially in the lower posterior part, resulting in cross-bite, lateral open bite or anterior open bite [6, 19, 21–23]. The increased tongue hypertrophy can lead to not only malocclusion, but also a reduced number of occlusal contacts, which affects masticatory function [24].
Groups that are affected by a known genetic disease are considered as a well-defined population that can contribute to the design of medical models that aim to develop personalised medicine or targeted therapeutic strategies. By studying the relationship between phenotype and genotype, we can learn more about what influences and regulates typical development. More importantly, this allows us to define the pre-disposition to disease or symptoms, so that we can offer timely and targeted prevention or treatment [25].
The aims of this study were to explore the open bite prevalence rates in DM1 and DMD and the relationship to orofacial function, and to create and compare orofacial dysfunction profiles for the two cohorts.
SUBJECTS AND METHODS
This database study of two cohorts was based on data collected from the MHC (Mun-H-Center, National Orofacial Resource Centre for Rare Disease) database in Gothenburg, Sweden. This database was created in 1996 to collect data on orofacial function and oral health in Swedish patients with rare diseases. The participants were assessed using a standardised chart and questionnaire used in several publications [26–30]. Data from the period 1996–2019 were used in this study. In total, 143 individuals with genetically verified DM1 (71 women, 72 men; mean age, 20.1±13.1 years; median age, 16 years; range 3–64 years,) were identified and included. The DM1 group consisted of 116 subjects with the congenital or childhood-onset form and 27 with the adult form of the disease. Ninety-nine individuals with DMD (99 men; mean age, 13.8±7.6 years; median, 13 years, range, 3–48 years) were also included. Four individuals in the DM1 group had received orthodontic treatment, and one had also had orthognathic surgery prior to the dental examination. The orthodontic treatment result in these individuals had to some extent or completely relapsed, which is the reason for inclusion. In the DMD group, only one patient had been treated orthodontically. The subjects were referred to the MHC National Orofacial Resource Centre for Rare Diseases, participated in the Ågrenska National Centre of Competence for Rare Diseases family programme or were recruited to participate in research projects for neuromuscular disorders. Informed consent was provided by all the participants or their caregivers prior to participation.
Clinical examination
All patients were examined in a clinical setting in a dental chair or wheelchair. A dental mirror, examination probe and a ruler were used for the examination. Each participant was assessed by a dentist and speech-language pathologist together. In total, there were 17 examiners, 14 dentists and 3 speech-language pathologists performing the assessments in this sample. A manual with consensus-based definitions of the clinical variables included in the examination protocol was used. The examiners were continuously calibrated through regular meetings.
Main outcome measures
The MHC observation chart and questionnaire [1] were used to assess malocclusion, as well as clinical orofacial variables. The presence of open bite was categorised as lateral open bite (LOB), anterior open bite (AOB), or severe anterior open bite with molar contacts only (AOBS) (Fig 1, a-c). AOBTot (or AOB(T)) was used to summarise the anterior open bites in total (AOB+AOBS). The sagittal relation (Cl I, Cl II, Cl III), high or narrow palate, along with space anomalies were also registered.
Fig. 1
A-C Open bite categories: A) lateral open bite (LOB); B) anterior open bite (AOB); and C) severe anterior open bite (AOBS).

The clinical orofacial variables selected in this study were those occurring in≥10% of the patients in either group. The occurrence of tonsillar hypertrophy and the use of ventilators were variables that were added from the MHC questionnaire due to their reported influences on craniofacial and dentoalveolar development [31, 32].
Occurrence of clinical orofacial variables (yes/no):
• Open mouth posture (OMP)
• Hypotonia of the lips (HL)
• Hypotonia of the tongue (HT)
• Impaired tongue mobility (ITM)
• Hypotonia of the jaw muscles (HJM)
• Mentalis muscle hyperactivity (MMH)
• Reduced mouth opening capacity (RMO)
• Macroglossia (MG)
• The occurrence of tonsillar hypertrophy (TH)
• The use of ventilators (Vent)
The Nordic Orofacial test –Screening (NOT-S) [33] was used to assess orofacial function and to create orofacial dysfunction profiles for each group. NOT-S is a reliable and validated test that contains a structured Interview part and Examination part [33]. Caregivers assisted the participants when needed during the interview part. The test comprises 12 domains (six in the Interview part and six in the Examination part), with one to five items in each domain. There is a maximum of one score per domain and a high total score (maximum, 12) reflects a high degree of orofacial dysfunction. Children (>5 years of age) with typical development have a mean dysfunction score of < 2 [34]. NOT-S was developed in 2007 and was not part of the data collection for the MHC database until 2013. NOT-S was performed on 40 individuals with DM1 and 53 with DMD. The DM1 group consisted of 34 individuals with the congenital or childhood form and 6 with the adult form of DM1. The mean age for the DM1 group was 21.2 years (±14.6) and that for the DMD group was 12.9 years (±7.7).
The domains in the Interview part of NOT-S were: I, Sensory; II, Breathing; III, Habits; IV, Chewing and swallowing; V, Drooling; and VI, Dry mouth. The domains in the Examination part were: 1, Face at rest; 2, Nose breathing; 3, Facial expression; 4, Masticatory muscles and jaw function; 5, Oral motor function; and 6, Speech.
Statistics
The data were analysed using the Statistical Package for the Social Sciences (SPSS Statistics 22). The level of significance was set at p < 0.05. Descriptive statistics were used for the prevalence of open bite categories and clinical orofacial variables in the two groups. A statistical non-parametric test (Spearman’s rank correlation coefficient) was used for correlations and comparisons between the groups and to correlate the clinical variables to the open bite categories of AOB and AOBS respectively. The two groups, DM1 and DMD, were combined in the multivariate data analysis.
Multivariate data analysis (MVA) was performed using the SIMCA-P software ver.13 (Umetrics AB, Umeå, Sweden). PCA (Principal Component Analysis) was carried out to get an overview of the data. Hotelling’s T2, corresponding to a multivariate generalisation of the 95% confidence interval, was utilised to identify outliers (Fig. 2). OPLS-DA (Orthogonal Projections to Latent Structures –Discriminant Analysis) was used for pattern recognition across two matrices. In the present study, the X-variables (predictor variables) comprised all the selected clinical variables, and Y represented the outcome variables AOBTot/no AOBTot (named AOB(T) in the figure), LOB/no LOB (Fig. 3a-b). The cumulative projections result in the formation of the model where the variables are plotted along the orthogonal axis. Variable importance in the projection (VIP) involves a ranking of the original variables according to their individual contributions to the model. VIP was used to summarise the importance of the predictors in the Y matrix, where VIP > 1 indicates that the predictor variables are influential in explaining the response variables. The quality of the MVA was assessed based on the following parameters: R2X, i.e., how well the variation of the Y-variable is explained by the model, the goodness of fit; and Q2, i.e., how well the variable can be predicted by the model, the goodness of prediction [35]. The result from an MVA model can provide a statistical analysis and an overview of data that incorporates the inter-dependency between variables that occur in a biological system, rather than evaluating each variable in isolation.
Fig. 2
PCA (Principal Component Analysis) Score Scatter Plot. The scatter plot provides a graphical overview of all the obtained data with each point corresponding to one individual. The PCA score shows trends and diversity within the sample as well as detect outliers. In this dataset where both groups are combined, the outliers reveal those individuals with a very high or very low NOT-S score. There were also more outliers in the DM1 group. The green colour represents the group with Myotonic dystrophy type 1, and the blue colour Duchenne muscular dystrophy.
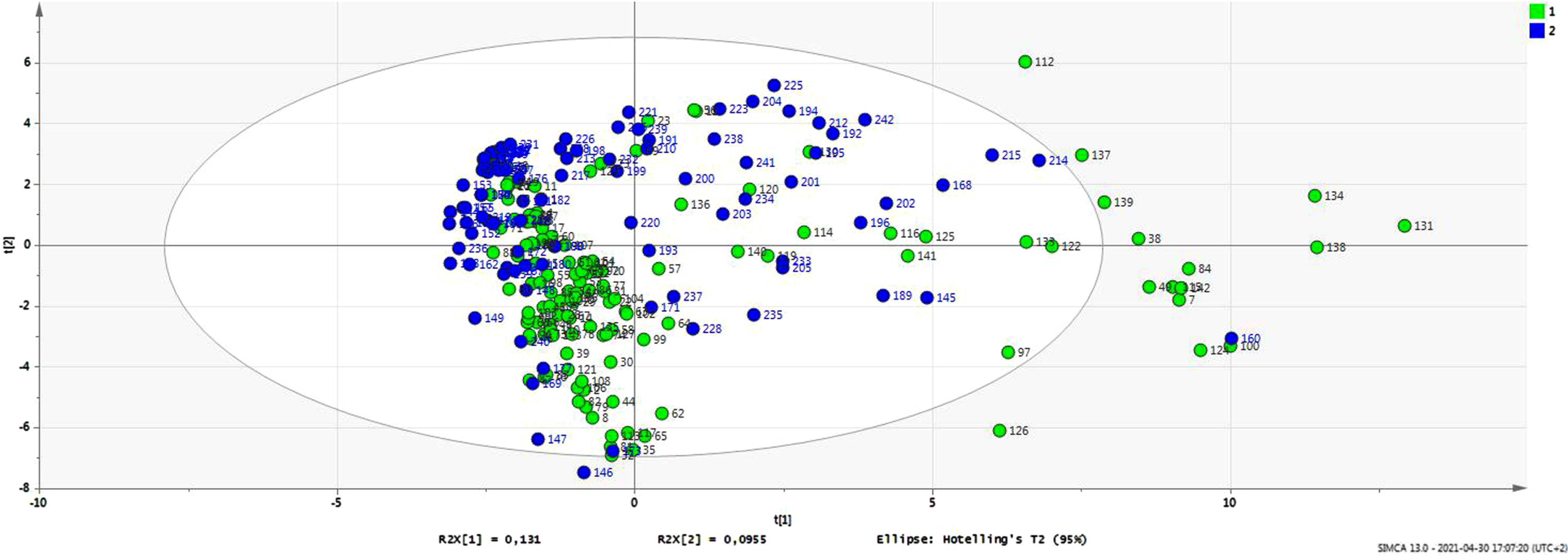
Fig. 3
a-b Orthogonal projections to latent structures (OPLS-DA) Loading Scatter Plot. The loading graph is plotted against the outcome variable. The two groups, myotonic dystrophy type 1 and Duchenne muscular dystrophy, are combined (N = 242) in this multivariate analysis. The scatter plot gives a visual overview of how each independent predictor variable is associated to the outcome variable as well as to the other predictors. The horizontal separation of the data-points (between group-variation) is determined by the colours of their VIP values. The variable importance in the projection (VIP) summarises the importance of the predictors in the Y matrix (within-group variation), where VIP > 1 indicates that the predictor variables are influential in explaining the outcome variables. The R2 and Q2 values present the goodness of fit and predictability of the original model, respectively. In panel a) on the left-hand x-axis the outcome variable corresponds to not having a lateral open bite [LOB(0)], and on the right-hand x-axis a lateral open bite is present [LOB(1)]. In panel b) on the right-hand x-axis the outcome variable corresponds to not having any of the anterior open bite types [AOBTot(0)] and on the left-hand x-axis, all of the anterior open bite types are present [AOBTot(1)].
![a-b Orthogonal projections to latent structures (OPLS-DA) Loading Scatter Plot. The loading graph is plotted against the outcome variable. The two groups, myotonic dystrophy type 1 and Duchenne muscular dystrophy, are combined (N = 242) in this multivariate analysis. The scatter plot gives a visual overview of how each independent predictor variable is associated to the outcome variable as well as to the other predictors. The horizontal separation of the data-points (between group-variation) is determined by the colours of their VIP values. The variable importance in the projection (VIP) summarises the importance of the predictors in the Y matrix (within-group variation), where VIP > 1 indicates that the predictor variables are influential in explaining the outcome variables. The R2 and Q2 values present the goodness of fit and predictability of the original model, respectively. In panel a) on the left-hand x-axis the outcome variable corresponds to not having a lateral open bite [LOB(0)], and on the right-hand x-axis a lateral open bite is present [LOB(1)]. In panel b) on the right-hand x-axis the outcome variable corresponds to not having any of the anterior open bite types [AOBTot(0)] and on the left-hand x-axis, all of the anterior open bite types are present [AOBTot(1)].](https://ip.ios.semcs.net:443/media/jnd/2023/10-5/jnd-10-5-jnd230025/jnd-10-jnd230025-g003.jpg)
Reliability test
Krippendorff’s alpha (α) coefficient was used [36] to estimate the inter-rater reliability. All available data were used from the assessments of 16 patients (not part of this sample) carried out by 8 of the 14 dentists. The results showed a variation in reliability. The occlusal variables presented a strong inter-rater reliability (open bite α=1,000, Angle class I α=0.894, Angle class II α=1.000, Angle class III α=0.845). The orofacial variables displayed poorer inter-rater reliability, varying from moderate (OMP α=0.788, HL α=0.743) to low (HPal α=0.691) to very low (NPal α=0.453, HJM α=0.120).
Ethical considerations
The study was approved by the Ethics Committee at The Sahlgrenska Academy, University of Gothenburg, and by the Swedish Data Inspection Board (Dnr: 3041-95, 544-11).
RESULTS
Prevalence of open bite
There was a small but significant difference in open bite prevalence between the DM1 (37%) and DMD (49%) groups (p = 0.048). In the DM1 group, AOBTot was seen in 36% of cases, with one-third of these being severe. AOB was as common in the congenital/childhood onset form as in the adult form, whereas AOBS was twice as common in the congenital/childhood form (14% vs 7%). LOB was rare (1%) in the DM1 group. In the DMD group, AOBTot was 26%, with one-third of these being severe. LOB was seen in 18% of cases.
Orofacial dysfunction profiles and associations with malocclusion
Open mouth posture (OMP) was the most common clinical orofacial variable but did not correlate with age in any of the groups. In the DM1 group, 79% displayed OMP (congenital or childhood onset form, 83%; adult form, 63%), whereas in the DMD group 23% displayed OMP. Individuals < 6 years (n = xx) and over > 20 years (n = 4) of age in the DMD group had a higher prevalence of OMP, 50% and 36%, respectively. The second most prevalent clinical variable in DM1 was hypotonic lips (HL) (77%), whereas in DMD it was macroglossia (23%). The respiratory prerequisites were also similar between the groups. Nine individuals (6%) in the DM1 group and eight in the DMD group (8%) received respiratory support. Tonsillar hypertrophy was found in four individuals with DM1 (3%) and in one person with DMD (1%).
The dominant trends of the groups’ separation are revealed in the data overview (Fig. 2). When observing the two diagnoses, there seems to be a similarity in pattern but a difference in the spread of observations. There are more outliers in the DM1 group (green colour) than in the DMD group (blue colour). Closer examination of these outliers reveals individuals with very high or very low NOT-S scores.
LOB
For the subjects who displayed LOB, there was a strong positive association with macroglossia (Fig. 3a). This variable occurred mainly in the DMD group. Individuals that presented with LOB were all > 10 years old, however no association with age was found in this sample. LOB was also negatively associated with open mouth posture (OMP) and hypotonic lips (HL). The predictive power of the applied model for LOB was 62% (Q2 = 0.618252).
AOBTot
Five clinical variables were identified as associated with AOBTot (Fig. 3b). Hypotonic lips (HL), open mouth posture (OMP), hypotonic tongue (HT), class III malocclusion (clIII) and spacing (Spac) were positively associated with AOBTot along with a negative association to class I sagittal relation (clI). The predictive power of the applied model for AOBTot was 51% (Q2 = 0.514512).
AOB and AOBS
AOB was significantly correlated to hypotonic lips (HL) (r = 0.316) and open mouth posture (OMP) (r = 0.243) and displayed a weak but significant negative correlation to age (r=-0.153). AOBS correlated to hypotonic jaw muscles (HJM) (r = 0.316).
NOT-S
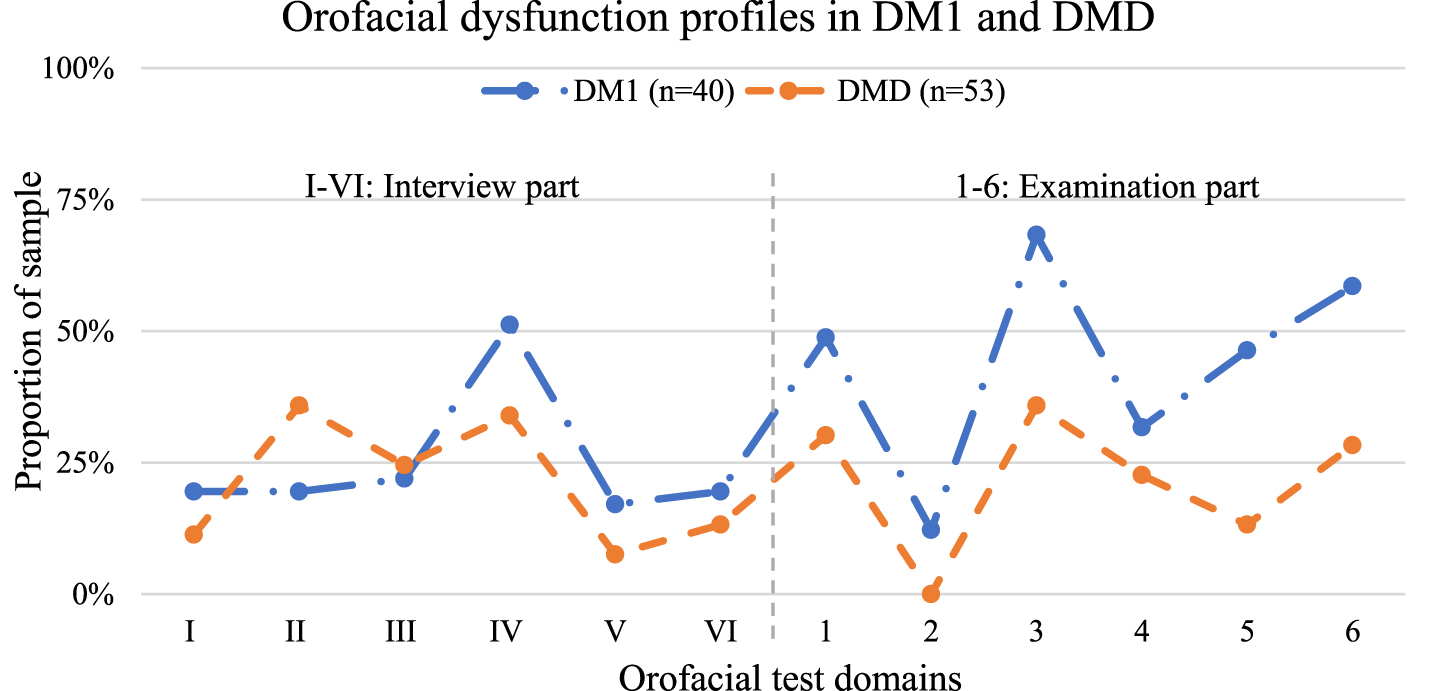
The mean total NOT-S dysfunction score for DM1 was 4.2±2.8 (median, 4.0; min-max,0–9) and for DMD it was 2.3±2.0 (median, 2.0; min-max, 0–8) (Fig. 4). The DM1 group’s mean score for the interview part was 1.53 (median 1.5; min-max, 0-6) and for DMD the mean score was 1.26 (median, 1.0; min-max; 0-4). The DM1 group’s mean score for the examination part was 2.73 (median, 2.5; min-max, 0-6) while the DMD group scored 1.3 (median1.0; min-max; 0-5). There was no statistical difference between the groups in the two parts, respectively. The DM1 group had the largest proportion of orofacial dysfunction in almost all the domains, with the exception of the domain “Breathing”, where reported difficulties were more common in the DMD group. The most prevalent orofacial dysfunctions in the DM1 group were in the domains of “Facial expression” (68%), “Speech” (56%), “Chewing and swallowing” (51%), “Face at rest” (49%), and “Oral motor function” (46%). The most-prevalent orofacial dysfunctions in the DMD group were in the domains of “Breathing” (36%), “Facial expression” (36%), “Chewing and swallowing” (34%) and “Face at rest” (30%). Both groups had no or very few subjects who showed any sign of obstructed nose breathing.
Fig. 4
Orofacial dysfunction profiles. Prevalence of orofacial dysfunctions in the DM1 (N = 40) and DMD (N = 53) groups in each domain according to the Nordic Orofacial Test –Screening (NOT-S). The two dysfunction profiles display a similar pattern. The DM1 group presents the largest proportion of orofacial dysfunction in almost all the domains, with the exception of the domain “Breathing”. There was no significant difference between the two groups in each part, respectively. The domains in the Interview part are: I, Sensory; II, Breathing; III, Habits; IV, Chewing and swallowing; V, Drooling; and VI, Dry mouth. The domains in the Examination part are: 1, Face at rest; 2, Nose breathing; 3, Facial expression; 4, Masticatory muscles and jaw function; 5, Oral motor function; and 6, Speech.
DISCUSSION
Open bite was a frequent finding in individuals with DM1 or DMD. LOB was especially common in DMD and was associated with the presence of macroglossia, closed mouth posture and not having hypotonic lips. AOB was associated with open mouth posture and hypotonic lips. AOBS was as common in DMD as in the congenital or childhood form of DM1 and correlated to hypotonic jaw muscles The orofacial dysfunction profiles derived from the NOT-S were similar, although the DM1 group displayed a larger proportion of dysfunctions, except for the domains of “Breathing”, “Speech” and “Oral motor function”.
The prevalence of AOBTot in this sample (33%) was broadly in accordance with the prevalence found in individuals with developmental disabilities (39.85%) [3]. However, it was twice as high as the reported global prevalence of AOB (16.52% in children and adolescents aged 2–16 years) [37] and eight times higher than that of Swedish school-children (4%) [38]. In the adult global population, AOB is 4%, with the highest prevalence found in the African population (8%) [39].
LOB was highly associated with macroglossia, in combination with not having an open mouth posture and not having hypotonic lips. The predictive variables correspond well with how the disease affects the orofacial area in DMD. As the disease progresses during adolescence, the usually presented orofacial symptoms are diminishing strength of the jaw muscles, together with an enlarged tongue. The muscle function of the submental group, m. orbicularis oris, and tongue mobility are often affected years later, such that there is adequate lip strength to counteract the tongue pressure anteriorly and, as a consequence, sustain the incisor position This suggests that in order to make space for the enlarged tongue and to secure the airways, the dental arches need to make room and expand transversally. Decreased extra-oral pressure from the masseter muscles and increased intra-oral pressure from the tongue may expand the arches, tip the teeth buccally and open the bite laterally.
The orofacial dysfunction pattern of LOB differs significantly from that of AOB. The factors associated with AOBTot were hypotonic lips, open mouth posture, hypotonic tongue, class III malocclusion and spacing. Hypotonia of the orofacial muscles together with open mouth posture are characteristic traits for DM1, and especially for the childhood and congenital forms. Tonsillar hypertrophy, mouth breathing, and oral habits are well-known aetiological factors in the development of anterior open bite [31, 40–42]. As mentioned previously, in this sample with DM1 and DMD, the prevalence of open bite is almost eight times that of the general population. However, the frequencies of occurrence of tonsillar hypertrophy, obstructed nose breathing and oral habits such as non-nutritive sucking are very low. This means that obstructed nose breathing, and oral habits do not explain the high prevalence of open bite in this sample. Orofacial hypotonia or muscle weakness can result in lowering of the mandible and inactive lips, manifested as open mouth posture. The predictive power (Q2) of the model was lower for AOBTot than for LOB. The group with AOBTot comprised individuals with both DM1(N = 51) and DMD (N = 26), so it was more heterogenic, whereas the group with LOB almost solely consisted of individuals with DMD. The difference in predictive power may be explained by these two cohorts having different anterior open bite aetiologies.
The results obtained for AOBTot support the findings presented in a schematic model in 1989 [10], where they compared the occlusal and craniofacial features of DM1 to the concept of “adenoid facies” [31, 40]. The aetiologies differ but the results of the open mouth posture with a low tongue position can be very similar, i.e., long face, posterior rotation of the mandible, over-eruption of the posterior teeth creating high and narrow palatal vaults and anterior open bites. Even though a posteriorly rotated mandible and a convex profile are often present in DM1, the class III molar relation was also correlated to AOBTot. When the mandible rotates posteriorly, the hypotonic tongue may exert pressure in an anterior-inferior direction due to gravity. The steeper the mandibular plane becomes, the more anterior pressure is applied by the tongue onto the lower incisors. This causes the anterior part of the dental arch to protrude, and gradually the posterior teeth follow, eventually developing into a class III molar relation. When the lower lip decreases in tonicity and loses the ability to prevent the incisors from proclining, spacing of the lower incisors occurs, which was also associated with AOBTot. The increase in lower incisor proclination over time has previously been observed in a craniofacial follow-up study of children with DM1, who are also a part of this sample [11].
The less-severe category of anterior open bite (AOB) was correlated to HL and OMP. Unlike individuals with LOB, the muscular imbalance between the intra- and extra-oral pressures in AOB seems to be mainly derived from hypotonia of the perioral muscles rather than from an increase in intra-oral pressure. The prevalence of AOB in DM1 was almost the same in the congenital/childhood form as in the adult form, although OMP and HL were more prevalent in the former. In a recent follow-up study of malocclusion in DM1 [43], the authors found that malocclusion was present already at an early age. DM1 patients had a higher prevalence of anterior open bite, posterior cross-bite, and class III malocclusions. Compared to controls, individuals with DM1 (congenital or childhood form) presented with a high palatal vault, smaller upper and lower inter-molar, and inter-canine widths, which continued to decrease over time [43]. The participants in that study (N = 26) are also part of this sample. A craniofacial follow-up study on the same sample revealed a hyper-divergent facial morphology with an increased mandibular plane angle and a larger inter-maxillary angle that was already present in early adolescence and that remained unchanged over a 5-year period [11]. In comparison to another Swedish growth study of typically developing individuals in the same age group [44], the mean ANB angle was 3.4-times larger and the inter-maxillary angle was 1.2-times larger at baseline for the DM1 sample. It seems likely that individuals with DM1 establish an altered craniofacial and dentoalveolar morphology already early in life. Case reports have described signs of facial hypotonia in DM1 already in foetal life, with the characteristic tent-shaped mouth appearing in ultrasound images [45]. This suggests that craniofacial development is influenced by low muscular activity from the very beginning. In the current study, the group with adult form DM1 exhibited more AOB than expected. This may explain why AOB was the only category of open bite that showed some correlation with age.
AOBS correlated strongly to hypotonia of the jaw muscles. Weakness of the jaw elevator muscles has long been one of the explanatory factors for dolichofacial type development [46, 47]. This ties in with a low position of the mandible, allowing more-extensive over-eruption of the teeth, together with posterior rotation of the mandible. The prevalence of AOBS in this study was the same for DM1 as for DMD, although it was twice as common in the childhood/congenital form as in the adult form of DM1. In individuals with DMD and AOBS, only one-third had hypotonic jaw muscles and one-third had open mouth posture. In addition, only half of the group with DMD and AOBS presented with macroglossia. This could mean that more variables need to be considered in the prediction of severe open bite in cases of DMD. Neck instability, for example, is a common finding in DMD [48], and it can be expected to affect head posture (head tilted posteriorly) and, consequently, mouth posture. Scoliosis is another possible factor that can influence posture and function. The NOT-S domain of “Breathing” revealed a high proportion of dysfunction in DMD and was not part of the MVA. Breathing difficulties may influence head posture, mouth posture, and tongue placement, which may interfere with chewing and swallowing.
The NOT-S was performed on participants examined after 2013 and adds functional difficulties from an objective as well as subjective aspect. Not only does it clarify which orofacial functions that needs further assessment, but it also elucidates on group level in which functional domain these individuals might need early intervention or adjustments in daily life. Comparing the two groups and their dysfunction profiles is challenging due to the differences in age and the progressive natures of DM1 and DMD. However, these orofacial dysfunction profiles are in agreement with those seen in previous research and clinical experience [9, 49–51]. Difficulties with facial expressions, chewing and swallowing and open mouth posture, with or without tongue protrusion, are common features in both DM1 and DMD. In DM1, speech problems and oral motor problems were seen in more than half of the participants, whereas in DMD less than one-quarter of the participants had such difficulties. The DMD group reported breathing difficulties (36%) as their most common dysfunction domain, although only 13% received assisted ventilatory support and none of the participants had difficulties with obstructed nose breathing. It is likely that their breathing difficulties mainly derive from weak respiratory muscles and scoliosis rather than from any obstruction of the airways.
A multi-disciplinary team is necessary to provide different perspectives and create a more-comprehensive picture. Identifying cause-and-effect relationships in this type of complex situation is difficult and requires probing the field and looking for patterns. Multivariate analysis (MVA) allows one to study the relationships between variables in their context and to quantify the relationship between variables. The advantage of MVA includes the ability to acquire a more-realistic picture than looking at a single variable. Open bite development is in many cases not caused by one single factor. Several intrinsic as well as extrinsic causes have been described in the orthodontic literature over the years. These factors may be strongly or partly under genetic control which makes it complex to study a causal genotype - phenotype relationship. It may be possible in the future to use this approach to look for patterns or clusters of genetic variables within this association and determine the risk for severe malocclusion in certain groups. Besides targeted medical treatment to slow down the progression rate of the disease, early interventions of low-intensity oral motor training [52] as well as orthodontic treatment may be important tools. This might prevent severe malocclusion and orofacial dysfunction and improve quality of life for this patient group. This study contributes by describing and comparing the orofacial phenotypes in two large cohorts of DM1 and DMD in relation to open bite malocclusion. It uses a multi-disciplinary approach to enhance our understanding of the intricate linkages between orofacial function and open bite development.
Limitations
The studied groups were not matched for gender or age, so as to be able to use all the available data. The time of onset of symptoms and course of the disease differ both between the groups and within each group. The mean age and median age are lower in the subjects in the DMD group than in the DM1 group. However, DMD progresses more rapidly than DM1. Currently, treatment of DMD with corticosteroids (and in some cases, also with gene therapy) decreases the severity of symptoms and prolongs the ambulatory stage [53]. Some of the participants were examined almost 20 years ago at a time when this treatment was not as widely available. This means that they might show more severe orofacial dysfunction in relation to age. Both age distribution and difference in progression of the disease are important factors that may affect the difference in the NOT–S dysfunction score. The skewness of the age distribution and the nominal outcome measurements may be the explanation why age was not associated to open bite development in our multivariate model when the two cohorts were combined. As the DM1 group consisted of adults with the adult form of the disease, they were less-affected in terms of orofacial function than the rest of the group, however the variability was high. They still presented with a high prevalence of anterior open bite (AOB). Only 7 % (n = 2) of the adults in DM1 presented with the severe form of open bite (AOBs). The reason for this variation in phenotype can be several. It is reported though, that in general, many symptoms occur earlier when CTG-repeats are longer, although there is an extreme variation is seen across individuals and even within specific tissues. There are several biomarkers that have been investigated but still no definitive relationships between the phenotype and levels of DNA methylation, expansion size, age-at-onset have yet been found [54].
The low alpha-value obtained for some variables may be negatively influenced by several factors. First, a relatively small sample was used. Second, the manual that describes how to assess HJM and palatal dimensions was unclear at that point in time; it has been revised and improved subsequently. Third, there is a lack of adequate quantitative measures of muscle tone, and the existing tools are not suited to orofacial muscles. Dentists are often not as experienced as speech-language pathologists in assessing muscle tone. In the current study, all assessments were made through consensus agreement between a dentist and a speech-language pathologist, which strengthens the reliability of the study.
Cross-bite is also a common malocclusion in DM1 and DMD. This variable was not used in the MHC Observation chart until recently. Instead, we included the variable “narrow palate (NP)”, which is more difficult to assess without quantitative measurements. This is unfortunate since it is reasonable to assume that we would have found a strong association between cross-bite and open bite in this study.
CONCLUSION
Open bite malocclusion is a common finding in patients with DM1 or DMD but is associated with different characteristics. The factors that are most frequently associated with open bite in DM1 and DMD are orofacial hypotonia and macroglossia, respectively. The frequency of orofacial dysfunction was higher in patients with DM1 than in patients with DMD, although the dysfunction profiles were similar. This study highlights the need for multi-disciplinary assessments and interventions to improve or sustain orofacial functionality and to create a favourable environment for occlusal development in individuals with DM1 and DMD.
ACKNOWLEDGMENTS
The authors would like to thank the participants and their families for their participation in this study.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest.
FUNDING
This research was funded by Public Dental Service of Västra Götaland and Sällsyntafonden, Ågrenska Foundation.
DATA AVAILABILITY
The authors confirm that the data supporting the findings of this study are available within the article. The data will be shared on reasonable request to the corresponding author.
REFERENCES
[1] | Sjogreen L , Andersson-Norinder J , Bratel J . Oral health and oromotor function in rare diseases–a database study. Swedish Dental Journal. (2015) ;39: (1):23–37. |
[2] | Cabrita JP , Bizarra MF , Graca SR . Prevalence of malocclusion in individuals with and without intellectual disability: A comparative study. Special care in dentistry: official publication of the American Association of Hospital Dentists, the Academy of Dentistry for the Handicapped, and the American Society for Geriatric Dentistry. (2017) ;37: (4):181–6. |
[3] | de Castilho LS , Abreu M , Pires ESLGA , Romualdo LTA , Souza ESME , Resende VLS . Factors associated with anterior open bite in children with developmental disabilities. Special care in dentistry: official publication of the American Association of Hospital Dentists, the Academy of Dentistry for the Handicapped, and the American Society for Geriatric Dentistry. (2018) ;38: (1):46–50. |
[4] | Rijpstra C , Lisson JA . Etiology of anterior open bite: a review. Journal of orofacial orthopedics=Fortschritte der Kieferorthopadie: Organ/official journal Deutsche Gesellschaft fur Kieferorthopadie. (2016) ;77: (4):281–6. |
[5] | Mendes SL , Ribeiro ILA , de Castro RD , Filgueiras VM , Ramos TB , Lacerda RHW . Risk factors for anterior open bite: A case-control study. Dental Research Journal. (2020) ;17: (5):388–94. |
[6] | Kiliaridis S , Katsaros C . The effects of myotonic dystrophy and Duchenne muscular dystrophy on the orofacial muscles and dentofacial morphology. Acta Odontologica Scandinavica. (1998) ;56: (6):369–74. |
[7] | Lindberg C , Bjerkne F . Prevalence of myotonic dystrophy type 1 in adults in western Sweden. Neuromuscular Disorders: NMD. (2017) ;27: (2):159–62. |
[8] | Turner C , Hilton-Jones D . Myotonic dystrophy: diagnosis, management and new therapies. Current Opinion in Neurology. (2014) ;27: (5):599–606. |
[9] | Sjogreen L , Engvall M , Ekstrom AB , Lohmander A , Kiliaridis S , Tulinius M . Orofacial dysfunction in children and adolescents with myotonic dystrophy. Developmental Medicine and Child Neurology. (2007) ;49: (1):18–22. |
[10] | Kiliaridis S , Mejersjo C , Thilander B . Muscle function and craniofacial morphology: a clinical study in patients with myotonic dystrophy. European Journal of Orthodontics. (1989) ;11: (2):131–8. |
[11] | Fontinha C , Engvall M , Sjögreen L , Kiliaridis S . Craniofacial morphology and growth in young patients with congenital or childhood onset myotonic dystrophy. European Journal of Orthodontics. (2018) ;40: (5):544–8. |
[12] | Cacucci L , Ricci B , Moretti M , Gasparini G , Pelo S , Grippaudo C . Surgical Orthodontic Treatment of a Patient Affected by Type 1 Myotonic Dystrophy (Steinert Syndrome). Case Reports in Dentistry. (2017) ;2017: :7957961. |
[13] | Usseglio J , Pagès E , Touzet-Roumazeille S , Brie J , Salle L , Ferri J . Dental and maxillofacial manifestations of Steinert’s myotonic dystrophy: A retrospective case series and therapeutic investigation. Journal of Stomatology, Oral and Maxillofacial Surgery. (2022) ;123: (6):e995–e1001. |
[14] | Antonarakis GS , Herzog G , Kiliaridis S . Vertical relapse after orthodontic and orthognathic surgical treatment in a patient with myotonic dystrophy. European Journal of Paediatric Dentistry. (2019) ;20: (1):53–8. |
[15] | Crisafulli S , Sultana J , Fontana A , Salvo F , Messina S , Trifirò G . Global epidemiology of Duchenne muscular dystrophy: an updated systematic review and meta-analysis. Orphanet Journal of Rare Diseases. (2020) ;15: (1):141. |
[16] | Gieron-Korthals M , Fernandez R . New Developments in Diagnosis, Treatment, and Management of Duchenne Muscular Dystrophy. Advances in Pediatrics. (2020) ;67: :183–96. |
[17] | Werneck LC , Lorenzoni PJ , Ducci RD , Fustes OH , Kay CSK , Scola RH . Duchenne muscular dystrophy: an historical treatment review. Arquivos de neuro-psiquiatria. (2019) ;77: (8):579–89. |
[18] | van den Engel-Hoek L , Erasmus CE , Hendriks JC , Geurts AC , Klein WM , Pillen S , et al. Oral muscles are progressively affected in Duchenne muscular dystrophy: implications for dysphagia treatment. Journal of Neurology. (2013) ;260: (5):1295–303. |
[19] | Egli F , Botteron S , Morel C , Kiliaridis S . Growing patients with Duchenne muscular dystrophy: longitudinal changes in their dentofacial morphology and orofacial functional capacities. European Journal of Orthodontics. (2018) ;40: (2):140–8. |
[20] | Eckardt L , Harzer W . Facial structure and functional findings in patients with progressive muscular dystrophy (Duchenne). American Journal of Orthodontics and Dentofacial Orthopedics: Official Publication of the American Association of Orthodontists, its Constituent Societies, and the American Board of Orthodontics. (1996) ;110: (2):185–90. |
[21] | Morel-Verdebout C , Botteron S , Kiliaridis S . Dentofacial characteristics of growing patients with Duchenne muscular dystrophy: a morphological study. European Journal of Orthodontics. (2007) ;29: (5):500–7. |
[22] | Ghafari J , Clark RE , Shofer FS , Berman PH . Dental and occlusal characteristics of children with neuromuscular disease. American Journal of Orthodontics and Dentofacial Orthopedics: Official Publication of the American Association of Orthodontists, its Constituent Societies, and the American Board of Orthodontics. (1988) ;93: (2):126–32. |
[23] | Symons AL , Townsend GC , Hughes TE . Dental characteristics of patients with Duchenne muscular dystrophy. ASDC Journal of Dentistry for Children. (2002) ;69: (3):277–83, 34. |
[24] | van den Engel-Hoek L , de Groot IJ , Sie LT , van Bruggen HW , de Groot SA , Erasmus CE , et al. Dystrophic changes in masticatory muscles related chewing problems and malocclusions in Duchenne muscular dystrophy. Neuromuscular Disorders: NMD. (2016) ;26: (6):354–60. |
[25] | The Council of the European Union. Council conclusions on personalised medicine for patients Official Journal of the European Union: The Council of the European Union; 2015 [Volume 58:[Available from: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=OJ%3AC%3A2015%3A421%3AFULL. |
[26] | Sjögreen L , Andersson-Norinder J , Jacobsson C . Development of speech, feeding, eating, and facial expression in Möbius sequence. International Journal of Pediatric Otorhinolaryngology. (2001) ;60: (3):197–204. |
[27] | Sjögreen L , Engvall M , Ekström AB , Lohmander A , Kiliaridis S , Tulinius M . Orofacial dysfunction in children and adolescents with myotonic dystrophy. Developmental Medicine and Child Neurology. (2007) ;49: (1):18–22. |
[28] | Strömland K , Miller M , Sjögreen L , Johansson M , Joelsson BM , Billstedt E , et al. Oculo-auriculo-vertebral spectrum: associated anomalies, functional deficits and possible developmental risk factors. American Journal of Medical Genetics Part A. (2007) ;143a: (12):1317–25. |
[29] | Strömland K , Sjögreen L , Johansson M , Ekman Joelsson BM , Miller M , Danielsson S , et al. CHARGE association in Sweden: malformations and functional deficits. American Journal of Medical Genetics Part A. (2005) ;133a: (3):331–9. |
[30] | Engvall M , Sjögreen L , Kjellberg H , Robertson A , Sundell S , Kiliaridis S . Oral health in children and adolescents with myotonic dystrophy. European Journal of Oral Sciences. (2007) ;115: (3):192–7. |
[31] | Linder-Aronson S . Adenoids. Their effect on mode of breathing and nasal airflow and their relationship to characteristics of the facial skeleton and the denition. A biometric, rhino-manometric and cephalometro-radiographic study on children with and without adenoids. Acta oto-laryngologica Supplementum. (1970) ;265: :1–132. |
[32] | Bariani RCB , Guimarães TM , Cappellette MJ , Moreira G , Fujita RR . The impact of positive airway pressure on midface growth: aliterature review. Brazilian Journal of Otorhinolaryngology. (2020) ;86: (5):647–53. |
[33] | Bakke M , Bergendal B , McAllister A , Sjögreen L , Asten P . Development and evaluation of a comprehensive screening for orofacial dysfunction. Swedish Dental Journal. (2007) ;31: (2):75–84. |
[34] | McAllister A , Lundeborg Hammarström I . Oral Sensorimotor Functions in Typically Developing Children 3 to 8 Years Old, Assessed by the Nordic Orofacial Test, NOT-S. (2013) ;21: :51–9. |
[35] | Eriksson L , Byrne T , Johansson E , Trygg J , Vikström C . Multi-and megavariate data analysis basic principles and applications: Umetrics Academy; 2013. |
[36] | Hayes AF , Krippendorff K . Answering the Call for a Standard Reliability Measure for Coding Data. Communication Methods and Measures. (2007) ;1: (1):77–89. |
[37] | Avrella MT , Zimmermann DR , Andriani JSP , Santos PS , Barasuol JC . Prevalence of anterior open bite in children and adolescents: a systematic review and meta-analysis. European Archives of Paediatric Dentistry : Official Journal of the European Academy of Paediatric Dentistry. 2021. |
[38] | Thilander B , Myrberg N . The prevalence of malocclusion in Swedish schoolchildren. Scandinavian Journal of Dental Research. (1973) ;81: (1):12–21. |
[39] | Alhammadi MS , Halboub E , Fayed MS , Labib A , El-Saaidi C . Global distribution of malocclusion traits: A systematic review. Dental Press Journal of Orthodontics. (2018) ;23: (6):40.e1–.e10. |
[40] | Subtelny JD . The Significance of Adenoid Tissue in Orthodontia *. The Angle Orthodontist. (1954) ;24: (2):59–69. |
[41] | Zhao Z , Zheng L , Huang X , Li C , Liu J , Hu Y . Effects of mouth breathing on facial skeletal development in children: a systematic review and meta-analysis. BMC Oral Health. (2021) ;21: (1):108. |
[42] | Warren JJ , Slayton RL , Bishara SE , Levy SM , Yonezu T , Kanellis MJ . Effects of nonnutritive sucking habits on occlusal characteristics in the mixed dentition. Pediatric Dentistry. (2005) ;27: (6):445–50. |
[43] | Fontinha C , Engvall M , Sjögreen L , Mårtensson Å , Ekström AB , Kiliaridis S . Occlusal traits and longitudinal dental changes in children and adolescents with congenital or childhood onset myotonic dystrophy. European Journal of Orthodontics. 2020. |
[44] | Al-Taai N , Persson M , Ransjö M , Levring Jäghagen E , Fors R , Westerlund A . Craniofacial changes from 13 to 62 years of age. European Journal of Orthodontics. 2022. |
[45] | Mashiach R , Rimon E , Achiron R . Tent-shaped mouth as a presenting symptom of congenital myotonic dystrophy. Ultrasound in Obstetrics & Gynecology: the Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology. (2002) ;20: (3):312–3. |
[46] | Ingervall B , Helkimo E . Masticatory muscle force and facial morphology in man. Archives of Oral Biology. (1978) ;23: (3):203–6. |
[47] | Proffit WR , Fields HW . Occlusal forces in normal- and long-face children. Journal of Dental Research. (1983) ;62: (5):571–4. |
[48] | Bozgeyik S , Alemdaroglu I , Bulut N , Yılmaz Ö , Karaduman A . Neck flexor muscle strength and its relation withfunctional performance in Duchenne muscular dystrophy. EuropeanJournal of Paediatric Neurology: EJPN: Official Journal of theEuropean Paediatric Neurology Society. (2017) ;21: (3):494–9. |
[49] | Botteron S , Verdebout CM , Jeannet PY , Kiliaridis S . Orofacial dysfunction in Duchenne muscular dystrophy. Archives of Oral Biology. (2009) ;54: (1):26–31. |
[50] | Berggren KN , Hung M , Dixon MM , Bounsanga J , Crockett B , Foye MD , et al. Orofacial strength, dysarthria, and dysphagia in congenitalmyotonic dystrophy. Muscle & Nerve. (2018) ;58: (3):413–7. |
[51] | Papaefthymiou P , Kekou K , Özdemir F . Orofacial Manifestations Associated with Muscular Dystrophies: A Review. Turkish Journal of Orthodontics. (2022) ;35: (1):67–73. |
[52] | Sjögreen L , Tulinius M , Kiliaridis S , Lohmander A . The effect of lip strengthening exercises in children and adolescents with myotonic dystrophy type 1. International Journal of Pediatric Otorhinolaryngology. (2010) ;74: (10):1126–34. |
[53] | Matthews E , Brassington R , Kuntzer T , Jichi F , Manzur AY . Corticosteroids for the treatment of Duchenne muscular dystrophy. The Cochrane Database of Systematic Reviews. (2016) ;2016: (5):Cd003725. |
[54] | Yum K , Wang ET , Kalsotra A . Myotonic dystrophy: disease repeat range, penetrance, age of onset, and relationship between repeat size and phenotypes. Current Opinion in Genetics & Development. (2017) ;44: :30–7. |


