
COVID-19 pandemic lockdown effect on neonatal hospital admissions from the community
Abstract
BACKGROUND:
The lockdowns imposed by countries due to COVID-19 pandemic had enormous impact on healthcare. Our goal is to determine consequences of the COVID-19 pandemic lockdown on neonatal hospitalizations and disease incidence in our hospital.
METHODS:
Observational retrospective study comparing newborns admitted to the neonatal care unit (NCU) from emergency department (ED). Newborns were distributed in two groups according to the date of the lockdown (22/3/2020): pre-lockdown group (12 month before) and post-lockdown group (12 month after). Categorical variables were compared according to chi square test and continuous variables with Mann-Whitney test. A Bonferroni corrected p-value < 0.006 was considered statistically significant. The monthly hospitalization rate between the two groups was analyzed with Generalized Method of Moments – System.
RESULTS:
We included 99 patients, 65/99 (65.7%) in the pre-lockdown group and 34/99 (34.3%) in the post-lockdown group. Pre-lockdown group: median age at hospitalization 19 (10–26) days, duration of symptoms 12 (5.5–36) hours. Post-lockdown group: median age at hospitalization 16 (6–24) days, duration of symptoms 14 (6–72) hours. The incidence of contagious disease was higher in the pre-lockdown group: 27/65 (41.5%) versus 3/34 (8.8%) in post-lockdown group (p = 0.001). No statistically significant difference in gestational age, gender, age at hospitalization, duration of symptoms and length of stay.
CONCLUSION:
Lockdown decreased admissions in NCU due to the decrease in contagious infections. The similar duration of symptoms before age at hospitalization in the two groups might indicate that health care accessibility has been maintained.
1Introduction
The coronavirus disease 2019 (COVID-19) pandemic caused by SARS-CoV-2, recognized in January 2020, is the largest pandemic since the Spanish flu, with a vast number of deaths among the adult population [1–3]. However, in terms of severity and mortality, it does not have the same impact on individuals of pediatric age [1–5]. Unfortunately, not only the direct impact of disease matters. The pandemic had enormous impact on society and healthcare, and due to the high rates of transmission around the world many governments imposed measures to try to decrease transmission within the community and the burden of health care due to the large number of admissions and mortality rate [3–7]. These impositions, together with the imposition of eviction of social contact and telework, constitute a set of measures that define the “lockdown”. Many countries imposed lockdowns, which were followed by a decrease on the demand for health care.
There was no memory of having applied this measure recently in Portugal and it was expected that the impact on the reduction would not be exclusive to cases of coronavirus infection, but also on other infections [8]. A state of emergency was decreed in our country, starting on 22/03/2020 with mandatory home collection, teleworking, closure of several services, with only essential goods and health services remaining open. Schools closed on March 16. With this closure, the economic costs, the social isolation and the interruption of learning increased [3].
In several reports around the world, there was a decrease in admissions to hospital services, both for infectious and non-infectious conditions, which may be related not only to the lockdown, but also to the change in healthcare-seeking behavior, with emphasis in care avoidance. Looking at it from another perspective, this delay can lead to admissions of patients with more advanced disease. In addition, diseases that require observation and emergent action continue to appear [3, 4, 6–11].
It was reported, in pediatric age, a decrease in cases of respiratory pathology, requiring intensive care, as well as an increase in the time spent seeking health care and in the number of cases of non-accidental injuries [4].
Regarding newborn admissions, there is not much information in the literature. Although newborns are included in pediatrics, and the same associations can be made, they constitute a population with particular characteristics. In addition to the increased risk of severe invasive disease, comorbidities associated with pregnancy, childbirth and postpartum, they are a group in which, out of fear and anxiety, parents more easily seek emergency services. Difficulty in accessing peripheral health services can even contribute to the increase in admissions of newborns to hospital emergencies [12].
The aim of this study was to determine the consequences of the COVID-19 pandemic on disease incidence and on the hospitalizations of neonatal patients from the community after the first lockdown.
2Methods
2.1Study design
This study was a single-centre, retrospective, observational, population-based analysis of admissions in the neonatal care unit (NCU) of Hospital Senhora da Oliveira, from emergency pediatric department between March 22 2019 and March 21 2021.
Within this period, a division into two groups was carried out, considering the date of imposition of the lockdown, and a comparison was made between them.
2.2Data source and collection
All admissions of newborns (≤28 days of life or <4 weeks of corrected age in case premature) to the NCU from the emergency department (ED) were considered. No hospitalizations were excluded. The sample size corresponds to the total number of hospitalizations.
Data were obtained from informatics system software (B-ICU.Care®, version 2021.02.1, Porto, Portugal), and converted in an anonymized form and was conducted according to the general data protection regulation. Data were recorded in IBM® Statistical Package for the Social Sciences (SPSS®) and StataCorp LLC® Statistical Software for Data Science (STATA®).
Ethical permission granted by the hospital ethics committee.
2.3Variables
The monthly admission number of newborns to the ED, as well as the monthly number of hospitalizations, were collected.
The following variables, from each newborn, were collected: gender, gestational age, age at hospitalization, duration of symptoms until hospitalization, length of stay, diagnosis and etiology.
Hospitalizations by pathology were grouped and classified as infectious and non-infectious. Subsequently, the infectious group was sub-classified into contagious and non-contagious, according to the known agent.
2.4Statistical analysis
Newborns were distributed in two groups according to the date of hospitalization in regard to the lockdown (22/3/2020): Pre-lockdown group (12 month before) and post-lockdown group (12 month after).
Statistical analysis of data collected from each newborn hospitalized was conducted using SPSS®, version 26 (Armonk, NY, USA). For continuous variables (age, duration of symptoms and length of stay), as they are non-parametric variables, the median and interquartile range (IQR) were calculated and they were compared using the Mann-Whitney test. We calculated absolute and relative frequency in categorical variables. These were compared according to chi square test. Bonferroni manual correction was applied for multiple comparisons. We performed 8 comparisons. A p-value < 0.006 was considered statistically significant.
The monthly hospitalization rate between the two groups was statistically analyzed using STATA®, version 17 (College Station, Texas, USA), with regression analysis – Generalized Method of Moments – System, considering a statistically significant p < 0.05.
3Results
During the study period, 529 ED admissions were recorded, 337/529 (63.7%) in pre-lockdown group and 192/529 (36.3%) in post-lockdown group. In our study, we included 99 newborns, 55/99 (55.6%) male, 44/99 (44.4%) female, corresponding to 99 hospital inpatients.
The median age was 18 days (IQR: 8–24), duration of symptoms was 12 hours (IQR: 6–48) and length of stay was 3 days (IQR: 2–7).
After grouping, according to the lockdown date, 65/99 (65.7%) newborns were included in the pre-lockdown group and 34/99 (34.3%) in the post-lockdown group.
36/65 (55.4%) newborns in the pre-lockdown group were male. In terms of gestational age, in the pre-lockdown group, 14/65 (21.5%) were preterm; 6/65 (9.2%) newborns were younger than 31 weeks, 5/65 (7.7%) were 32–32 weeks, and 3/65 (4.6%) were 34–36 weeks. The median age at hospitalization was 19 days (IQR: 10–26)
In the post-lockdown group 19/34 (55.9%) newborns were male, 2/34 (5.9%) were preterm (both with less than 32 weeks of gestational age). The median age at hospitalization was 16 (IQR: 6–24) days (Table 1).
Table 1
Newborns admitted to the NCU (gestational age, gender, age and length of stay)
| Pre-lockdown n = 65 | Post-lockdown n = 34 | p | ||
| Gestational age | < = 31 weeks | 6/65 (9.2%) | 2/34 (5.9%) | 0.044 |
| 32–33 weeks | 5/65 (7.7%) | 0/34 (0%) | ||
| 34–36 weeks | 3/65 (4.6%) | 0/34 (0%) | ||
| Term | 51/65 (78.5%) | 32/34 (94.1%) | ||
| Gender | Male | 36/65 (55.4%) | 19/34 (55.9%) | 0.962 |
| Female | 29/65 (44.6%) | 15/34 (44.1%) | ||
| Age at hospitalization (days) | 19 (IQR: 10–26) | 16 (IQR:6–24) | 0.210 | |
| Length of stay (days) | 3 (IQR: 2–7) | 3 (IQR: 2–7) | 0.855 | |
There was no statistically significant difference in age at hospitalization, between gestational age and between genders in both groups (Table 1).
Regarding the duration of symptoms, when pre-lockdown group was analyzed median was 12 (IQR: 5.5–36) hours and in post-lockdown group median was 14 (IQR: 6–72) hours. The median hospital length of stay in both groups was 3 (IQR: 2–7) days (pre-lockdown 3, post-lockdown 3). There was no statistically significant difference in duration of symptoms (p = 0.691) and length of stay (p = 0.855) between both groups.
The diagnosis at admission to the neonatology unit, in both groups, are identified in Table 2. In other infections are included: Cellulitis of the finger and conjunctivitis. In “other diagnosis” were included: Seizures, inguinal hernia, aortic coarctation, cow’s milk protein allergy, feeding difficulties, hypotony, vomiting, grunting, umbilical cord alteration, West Syndrome, rash, maternal anxiety, and refusal to feed.
Table 2
Diagnosis at hospitalization, per group
| Pre-lockdown group n = 65 | Post-lockdown group n = 34 | |
| Bronchiolitis | 20/65 (30.8%) | 1/34 (2.9%) |
| Jaundice | 6/65 (9.2%) | 7/34 (20.6%) |
| Urinary tract infection | 3/65 (4.6%) | 7/34 (20.6%) |
| BRUE | 8/65 (12.3%) | 3/34 (8.8%) |
| Nasopharyngitis | 5/65 (7.7%) | 1/34 (2.9%) |
| Sépsis | 4/65 (6.2%) | 1/34 (2.9%) |
| Dehydration | 2/65 (3.1%) | 1/34 (2.9%) |
| Pneumonia | 1/65 (1.5%) | 1/34 (2.9%) |
| Excessive weight loss | 2/65 (3.1%) | 0/34 (0%) |
| Meningitis | 1/65 (1.5%) | 0/34 (0%) |
| Mastitis | 1/65 (1.5%) | 0/34 (0%) |
| Perianal abcess | 0/65 (0%) | 1/34 (2.9%) |
| Other infectious | 4/65 (6.2%) | 1/34 (2.9%) |
| Other non-infectious | 8/65 (12.3%) | 10/34 (29.4%) |
We verified that 52/99 (52.5%) of all hospitalizations was due to infectious causes, 39/65 (60%) of admissions in the pre-lockdown group and 13/34 (38.2%) in the post-lockdown group.
Bronchiolitis was the most frequent pre-lockdown diagnosis and both jaundice and urinary tract infection were most frequent diagnosis in the post-lockdown group.
We reclassified infectious group disease according to contagiousness. We included bronchiolitis, pneumonia, nasopharyngitis and meningitis in the contagious group. There was an overall incidence of 30/99 (30%) of contagious diseases. The incidence of contagious infectious disease was higher in the pre-lockdown group: 27/65 (41.5%), versus 3/34 (8.8%) in post-lockdown group (Table 3). This decrease is statistically significant (p = 0.001).
Table 3
Hospitalizations to the NCU, according to contagiosity, per group
| Pre-lockdown group n = 65 | Post-lockdown group n = 34 | p | ||
| Non-infectious | 26/65 (40.0%) | 21/34 (61.8%) | 0.039 | |
| Infectious | Contagious | 27/65 (41.5%) | 3/34 (8.8%) | 0.001 |
| Non-contagious | 12/65 (18.5%) | 10/34 (29.4%) | 0.213 | |
When we compare both groups according to monthly rate hospitalization we observe in pre-lockdown group, mean of 26 newborn ED admissions per month (11–40). Hospitalizations in the NCU per month variates between 0 and 15, with mean 5, standard deviation (SD) 3.98. The monthly rate of hospitalizations varies between the null value, given that in some periods there were no hospitalizations and 15/31 (48.4%), with mean 19.7%.
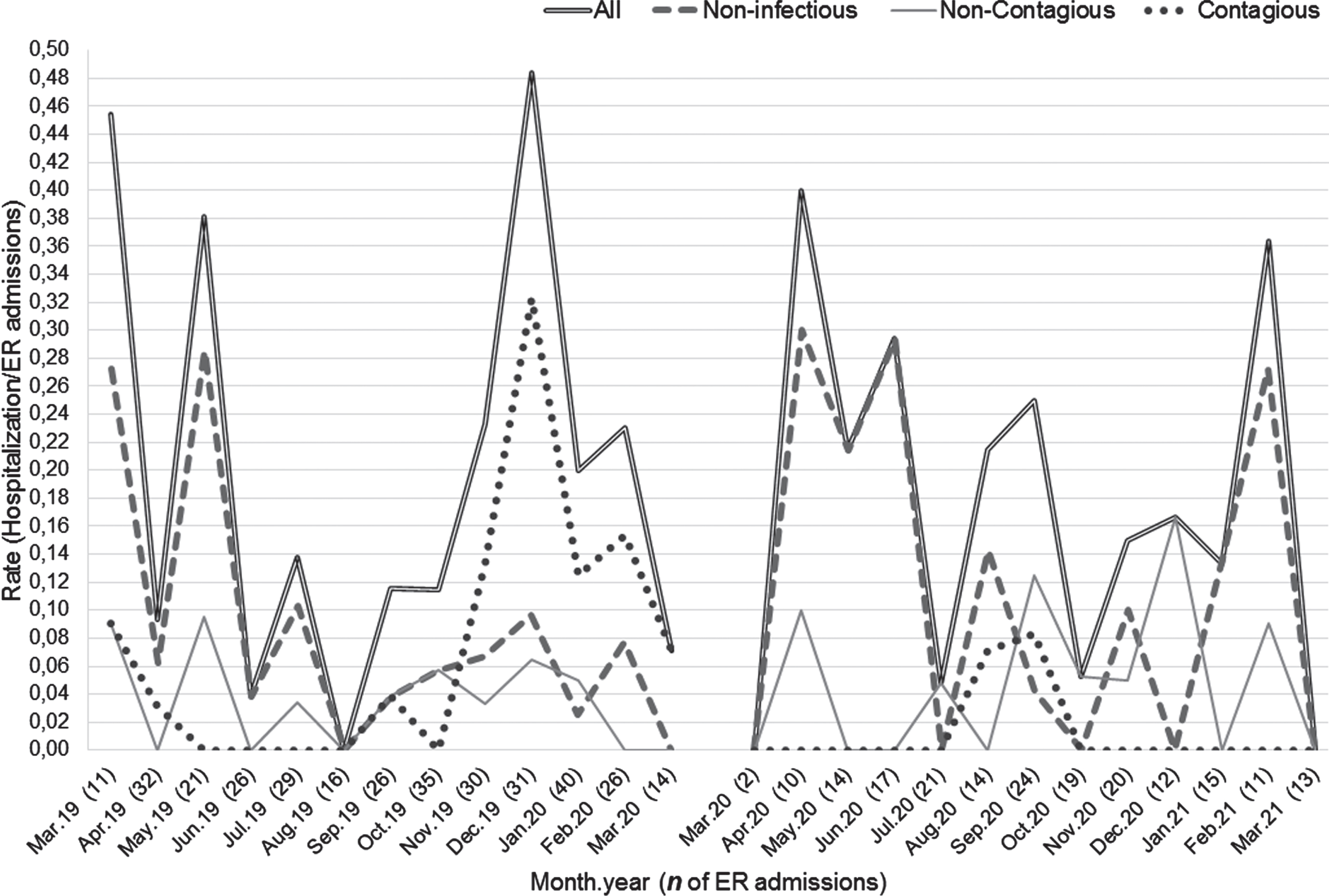
In post-lockdown group, mean of 15 admissions per month (2–24). Hospitalizations per month variates between 0 and 6, with mean 3, SD 1.85. The monthly rate of hospitalizations varies between the null value and 4/10 (40.0%), with mean 17.6%. The rates of all hospitalizations and categories of hospitalizations are show in Fig. 1.
In the pre-lockdown group, non-infections have a very weak relationship with the number of admissions (ρ= 0.0187). The same is not true for the total number of non-contagious and contagious, given that they have a moderate relationship with the number of admissions, so they can have a significant impact on them, verified by the obtained correlation coefficient (ρ= 0.4451 and ρ= 0.3904). The same is verified in the post-lockdown group, however, in relation to the contagious group, the correlation coefficient obtained (ρ= 0.4536) is higher than pre-lockdown.
Estimation with Generalized Method of Moments – System allowed to conclude that, with regard to the total rate of hospitalizations, there are no differences considered statistically significant between the two analyzed periods, due to the high proof value. The same result for non-infections and infectious non-contagious.
Nonetheless, for contagious infectious causes, differences considered statistically significant were found between the two groups. We found a decrease in rate of hospitalizations post-lockdown, and this finding is statistically significant (p = 0.04). In pre-lockdown group, there is an important increase in the contagious infections in December of the year considered. On the other hand, the months from May to August have zero hospitalizations. In post-lockdown group there are no peaks as high as in the previous case, the oscillations are smaller and the differences between the periods become evident (Fig. 1).
Fig. 1
Lines plot showing rates for total hospitalizations and for each category. Monthly raw numbers of total admissions are shown, by month, on the x-axis (inside parentheses). Abbreviations: ER, Emergency Room; Jan, January; Feb, February; Mar, March; Apr, April; Jun, June; Jul, July; Aug, August; Sep, September; Oct, October; Nov, November; Dec, December.
4Conclusion
Lockdowns associated with COVID-19 pandemic decreased hospital admissions in this NCU, as reported, at the pediatric level, in some international studies. Williams et al. [4] in a retrospective study, showed that the decrease in hospitalizations to pediatric intensive care units was largely due to the reduction in admissions for respiratory diseases, which seems to be similar to what we found in our reality where the main causal factor seems to be the decrease in contagious infectious conditions.
This situation happened likely due to hygiene and confinement measures that decreased transmission and incidence of contagious infections. In fact, when looking in the literature, it appears that the decrease in the number of admissions to emergency services after the application of lockdown is multifactorial. These factors include fear of contracting the disease in the hospital, travel restrictions and avoidance to reduce overloading the health systems [3–9].
There are reports showing an increase in the number of newborns (including low-birth-weight and premature) cared for in the ED and admitted in neonatal units, in a likely context of reduced accessibility and delay to access to health services (including local health care) [9, 12]. When analyzing the data obtained, we verified there was no increase in the duration of symptoms at the time of hospitalization. This might reflect the maintenance of health care access at our hospital, although we cannot conclude it in a solid manner, since the referred studies encompass different populations. As SARS-CoV-2 disease is usually mild in pediatric patients, it may also contribute to this fact [1, 4, 5, 13].
Looking at our data, the clear reduction in contagious conditions caused by the lockdown will be the likely cause of the drop observed in NCU hospitalizations.
Some studies reports possibility of pressure on the part of caregivers and professionals for earlier discharge, due to avoiding long stays in the hospital environment. Our study showed similar length of stay in both groups but it is not possible to conclude about the real cause of these data, because it can be multifactorial. A directed study would be necessary to reveal the causes of this finding.
Another interesting fact is about prematurity. SARS-CoV-2 infection in pregnant woman is associated with increase in preterm delivery, premature rupture of membranes and small gestational age babies [9, 14, 15]. Despite this fact, we know that preterm infants are more likely to contract infectious diseases and, given the above, the lower number of contagious cases translates into a lower number of hospitalized preterm infants. However, we did not find statistically significant data (Table 1) that would allow us to formalize a conclusion about this factor.
The main limitation of this study is the number of patients included. In addition to this, the study does not allow to calculate the weight of each isolated lockdown measure in the reduction of the burden of hospital admissions. This reduction was compared taking into account several measures taken together, associated with the lockdown. Even so, the observed reduction is most likely associated with the global drop in infectious and contagious etiologies.
In our sample, lockdown was not associated with an apparent decrease in access to healthcare, but a strong association is not possible, as this depends on many factors. However, we can conclude that there was a decrease in hospitalizations for contagious pathology after the lockdown, in the age group studied.
Disclosure statements
The authors have no conflicts of interest relevant to this article to disclose.
Funding and support
No funding was secured for this study.
This research submitted to the journal was approved and conducted in accordance with the ethical standards of all applicable national and institutional committees and the World Medical Association’s Helsinki Declaration.
References
[1] | Manti S , Licari A , Montagna L , Votto M , Leonardi S , Brambilla I , et al. SARS-CoV-2 infection in pediatric population. Acta Biomed. ((2020) );91: (11-S). |
[2] | Dong Y , Mo X , Hu Y , Qi X , Jiang F , Jiang Z , et al. Epidemiology of COVID-19 among children in China. Pediatrics. ((2020) )145: (6). |
[3] | Rajmil L , Hjern A , Boran P , Gunnlaugsson G , Camargo OK , Raman S , et al. Impact of lockdown and school closure on children’s health and well-being during the first wave of COVID-19 A narrative review. BMJ Paediatr Open. ((2021) ) 5: (1). |
[4] | Williams TC , MacRae C , Swann OV , Haseeb H , Cunningham S , Davies P , et al. Indirect effects of the COVID-19 pandemic on paediatric healthcare use and severe disease: A retrospective national cohort study. Arch Dis Child ((2021) ) 106: (9), 911–7. |
[5] | Siebach MK , Piedimonte G , Ley SH COVID-19 in childhood: Transmission, clinical presentation, complications and risk factors. Pediatr Pulmonol ((2021) ) 56: (6), 1342–56. |
[6] | Isba R , Edge R , Jenner R , Broughton E , Francis N , Butler J Where have all the children gone? Decreases in paediatric emergency department attendances at the start of the COVID-19 pandemic of 2020. Arch Dis Child. ((2020) ) 105: (7), 704. |
[7] | Angoulvant F , Ouldali N , Yang DD , Filser M , Gajdos V , Rybak A , et al. Coronavirus disease pandemic: Impact caused by school closure and national lockdown on pediatric visits and admissions for viral and nonviral infections-a time series analysis. Clin Infect Dis ((2021) ) 72: (2), 319–22. |
[8] | Kruizinga MD , Peeters D , Veen MV , Houten MV , Wieringa J , Noordzij JG , et al. The impact of lockdown on pediatric ED visits and hospital admissions during the COVID19 pandemic: A multicenter analysis and review of the literature. Eur J Pediatr ((2021) ) 180: (7), 2271–9. |
[9] | Burt JF , Ouma J , Lubyayi L , Amone A , Aol L , Sekikubo M , et al.Indirect effects of COVID-19 on maternal, neonatal, child, sexual and reproductive health services in Kampala, Uganda. BMJ Glob Health .((2021) )6: (8). |
[10] | Rennert-May E , Leal J , Thanh NX , Lang E , Dowling S , Manns B , et al.The impact of COVID-19 on hospital admissions and emergency department visits: A population-based study. PLoS One .((2021) )16: (6). |
[11] | Santana R , Sousa J , Soares P , Lopes S , Boto P , Rocha JV The demand for hospital emergency services: Trends during the first month of COVID-19 response. Port J Public Health ((2020) ) 38: , 30–36. |
[12] | Cheek JA , Craig SS , West A , Lewena S , Hiscock H Emergency department utilisation by vulnerable paediatric populations during the COVID-19 pandemic. Emerg Med Australas ((2020) ) 32: (5), 870–1. |
[13] | Kim TY , Kim EC , Agudelo AZ , Friedman L COVID-19 hospitalization rate in children across a private hospital network in the United States: COVID-19 hospitalization rate in children. Arch Pediatr ((2021) ) 28: (7), 530–2. |
[14] | Martinez-Perez O , Rodriguez PP , Hernandez MM , Pardilla MBE , Perez NP , Hernandez MRV , et al. The association between SARS-CoV-2 infection and preterm delivery: A prospective study with a multivariable analysis. BMC Pregnancy Childbirth ((2021) ) 21: (1), 273. |
[15] | Mullins E , Hudak ML , Banerjee J , Getzlaff T , Townson J , Barnette K , et al. Pregnancy and neonatal outcomes of COVID- Coreporting of common outcomes from PAN-COVID and AAP-SONPM registries. Ultrasound Obstet Gynecol ((2021) ) 57: (4), 573–81. |


