
A Comparison of Depressive Symptoms in Medical and Psychology Students in Germany – Associations with Potential Risk and Resilience Factors
Abstract
Background:
Previous studies have shown that medical students are more prone to suffer from symptoms related to depression than other students. Even though there is some evidence that psychology students also experience such symptoms, research concerning the mental health of future psychologists is scarce.
Objective:
The aims of this study were threefold: (a) to determine the prevalence of symptoms related to depression among medical and psychology students (b) to investigate risk factors, which may have a potential influence on the development of depressive symptoms and (c) to examine resilience factors in order to indicate possible approaches to improve the mental health of the students.
Methods:
A total of 673 medical and psychology students completed the Beck Depression Inventory-II (BDI-II) to assess depressive symptoms, a neuroticism scale, and a standardized questionnaire for 13 risk and eight resilience factors derived from the literature.
Results:
While the results of previous research concerning the prevalence of depressive symptoms could be replicated for medical students (22% exceeding the cut-off in the BDI-II), psychology students demonstrated an even higher prevalence (28%). Ten potential risk factors and five potential resilience factors could be identified, which also showed a cumulative effect: The more risk factors students reported, the more depressive symptoms they experienced; the inverse effect was observed for resilience factors.
Conclusions:
Not only medical but also psychology students show elevated depressive symptomatology. In the university context, notably, the pressure to perform represents a potential risk factor, whereas the presence of just two resilience factors such as emotional support and study satisfaction contribute to a decrease of symptoms.
INTRODUCTION
Depression is one of the most worrisome health concerns of our time. According to disability-adjus-ted life years (DALY), a measurement for overall disease burden, depression is referred to as “the most burdensome disorder of all diseases in the EU” [1]. In Germany, depression has a 12-month prevalence of more than four million adults – more than the population of Berlin [2, 3]. The age of onset of depression is primarily during young and middle adulthood [4], and it is especially important to note that the prevalence of depressive symptoms is highest among the 18- to 29-year-olds. In this age group, 12% of the women and 8% of the men reportedly suffer from symptoms related to depression [5], and even though they might not yet fulfill the criteria for a mental disorder, depressive symptoms not only go along with impairment but also with a higher risk for depression. University students mainly represent the age group of young adults. Hence, according to the reported epidemiological studies [4], they belong to the group with the highest prevalence of depressive symptoms. This conclusion is consistent with the reports by one of the leading German health insurance companies, which also discloses that a diagnosis of depression more often occurs among students than among young employees [6].
Several American and Canadian studies reveal that medical students are more prone to suffer from depressive symptoms than other students and that, in comparison to the general population, their mental stress is elevated [7]. A meta-analysis, published in 2016 [8], which included 183 studies from 43 countries (N = 122,356) arrived at the same conclusion and therefore drew international attention to the mental health of medical students. According to the authors, depression among medical students had a point prevalence of over 27% , and more than 11% of the students reported suicidal ideation. However, less than 16% of individuals received psychological support. Even though there are not many studies published on the mental health of medical students in Germany, similar results have been found; at the University of Leipzig (Saxony) 13% of the medical students suffered from a depressive syndrome, and 9% endured a Major Depression [9]. In comparison, 8% of the people in the control group of similar age reported to suffer from a depressive syndrome, and the prevalence for major depression was less than 2% . Jurkat et al. [10] from the University in Gießen (Hessen) obtained similar results; 13% out of 651 medical students surveyed, suffered from mild to moderate depression, 6% of the students reported clinically relevant depressive symptoms.
Although the subjective assessment of mental stress does not differentiate between medical and psychology students [11], there are even fewer studies on the mental health of psychology students. According to a survey by Grützmacher et al. [12], the pre-valence of a depressive syndrome among the subject group “social science, psychology, and educational science” is 18% . A comparison of students of sports science, psychology, and medicine showed that psychology students reported the most strain and difficulties [13]. Schmidt-Gürtler investigated the prevalence of depression among psychology students in Gießen; more than 39% of the participating students (N = 143) suffered from depressive symptoms [14]. Thus, this result shows that psychology students may be even more burdened than medical students, but it is important to note that the reported studies are not directly comparable as different psychological tests were used. The heavy pressure to perform may be responsible for the elevated depressive symptomatology among psychology students. Opportunities for psychology students appear to be highly competitive as less students are admitted to the master program in German public University psychology departments than have actually completed a Bachelors’ degree in psychology. Therefore, grade pressure is high [15] – grades are typically an important selection criterion. At the investigated university, for instance, only students with a GPA of no worse than 1.201 were even considered for the master program in psychology in 2019, and only about 4% of the applicants were allowed into the program. Of course, students know about the selection criteria and the selection numbers and may, therefore, experience elevated levels of pressure. Previous research into the link between a competitive social environment and depression showed that vulnerability to depression may increase due to the pressure to assert oneself in a competitive environment [16].
Given the well-established notion of a multifactorial genesis of depressive disorders [17], numerous risk factors have been linked to depression: female gender [5], positive family history [18], personality traits like neuroticism [19, 20], abuse of prescription drugs or illicit drugs [21], alcohol consumption [21], a low socioeconomic status [5], life events like loss of a parent [22], and financial worries [23]. These risk factors represent general risk factors for depression and do not refer to adolescents in specific. However, some of these factors more often apply to students than adults of the general population: The prevalence of risky alcohol consumption is higher among students (40%) than in the general population (14%) [12], and similarly, an above-average proportion of people with financial worries can be assumed for the student population. Additionally, the following stress factors can be related to the university context, and have been associated with the development of depressive symptoms in the past: uncertain prospects [23], the pressure to perform [23], excessive demands [24], shortage of time [10], and competition among students [16].
Resilience factors are protective factors that moderate the effect of risk factors and alleviate or neutralize their consequences [25]. Many resilience factors about depression have been discussed, as the risk factors affect a multitude of people and notably students; however, not all of them develop depressive symptoms. The following resilience factors, inter alia, have been associated with an amelioration of depressive symptoms: using relaxation techniques such as yoga or progressive muscle relaxation [26], sport [27, 28], religiousness [29], a healthy diet (e.g. the Mediterranean diet) [30], emotional support [31], actively making music [32], satisfaction with one’s studies [31], and having enough time for social contacts [33].
Having considered potential risk and resilience factors, the question arises to what extent the groups of medical and psychology students differ regarding these characteristics. For example, previous surveys of student health have shown that medical students are more likely to have a higher socioeconomic background than psychology students. In terms of study, there was no difference in stress experience, but medical students reported significantly higher perceived social support from fellow students than psychology students. Furthermore, medical students (47%) were more likely to be physically active than psychology students (37%) and reported a higher level of general life satisfaction [12]. To the best of our knowledge, however, information on how these groups differ before they begin their academic studies is scarce.
The psychological stress that students affected by depressive symptoms experience is one important issue of concern. However, consequences that may occur during the future exercise of their profession in the medical or psychotherapeutic/other psychological field need to be taken into consideration, too; for example, doctors, who suffer from depression make six times more medication errors than their healthy colleagues [34]. Moreover, stress and depressive symptoms harm not only the efficiency of treatment but also the quality of the relationship between therapist and patient [35, 36]. Thus, regarding their potential role in the health system, the mental health of medical and psychology students should also be a matter of general concern, and, therefore, it can be advantageous to know about risk and resilience factors in order to support this occupation group already during their training. Accordingly, the goal of this study is not only to address the prevalence of depressive symptoms among medical and psychology students but also the risk and resilience factors associated with symptoms related to depression. As the current data on the prevalence of depression among psychology students is meager, and the available data is inconsistent [12, 14], we expect that these two groups of students differ by the prevalence of symptoms related to depression. Furthermore, we expect a positive correlation between the risk factors and depression and, therefore, a negative between resilience factors and depression. Finally, we expect that the more risk factors students report, the more depressive symptoms should be reported. Conversely, the more resilience factors students experience, the less depressive symptoms should be reported.
MATERIALS AND METHODS
Participants
A total of N = 673 students of the medical faculty and the department of Psychology of a medium-sized university in Germany participated. All students have received oral and written information about the study. The subsequent participation in the survey was voluntary, anonymous and there were no disadvantages if students did not participate or discontinued participation. Therefore, participation served as informed content. The psychology students (n = 109) taking part were undergraduates and for better comparability, only medical students (n = 564) from the preclinical years (year one and year two) were included in this study. Participating medical students, (representing 88% of the medical students enrolled), had a mean age of 21.52 (SD = 3.68) years, and were primarily in the first semester (62% , n = 350); n = 214 (38%) were third-semester students. Among the participating psychology students (representing 53% of the bachelor psychology students matriculated), n = 48 (44%) were in the first, n = 22 (20%) in the third and n = 38 (35%) in the fifth semester; on average, psychology students were 22.03 (SD = 3.93) years old. There were more women in the group of psychology students (84% ; n = 92) than among the medical students (67% ; n = 376); χ² (df = 1) = 13.567, p < 0.001.
Design and measures
In this empirical, cross-sectional study medical and psychology students provide self-reports on depressive symptoms as well as related risk and resilience factors. Hence, depressiveness (total score of the Beck Depression Inventory [BDI-II]) is the dependent variable; the subject of study (psychology/medicine), as well as risk and resilience factors, are independent variables. Three questionnaires operationalized these variables.
First, subjects completed a standardized questionnaire, which included items on sociodemographic data and potential risk and resilience factors. The questionnaire assessed seven general risk factors, five study-related risk factors and eight resilience factors. The risk factor “positive family history” was given if at least one first or second-degree relative (siblings or [grand-]parent) was under treatment for at least one mental disorder other than dementia. To determine the risk factor “female gender” the biological gender was assessed. The risk factor “low socioeconomic status” was defined present if at least one of the following response alternatives applied to both the father and the mother of the student: “without graduation”, “lower secondary education” or “unskilled”. “Loss of parent” was rated present if the student reported divorce or death of a parent. To investigate the risk factor “financial worries”, we asked the students whether they had sufficient financial resources and considered this risk factor to be present if they answered with “sometimes too little”, “often too little”, or “I am mostly under great financial pressure”. Furthermore, we considered students, who reported drinking more than eight (men) or six (women) drinks per occasion at least once a month, to apply to the risk factor “alcohol consumption”. The risk factor “drug abuse” was defined as present if students reported consumption of medication or drugs to improve concentration or performance, for sedation or sleep.
The item “Are there any things that currently make it difficult for you to be happy with your study decision?” recorded risk factors, which can be summarized under study-related risk factors. In comparison to the risk factors mentioned so far, these factors included particular currently present burdens due to the study. The item could be answered with possible multiple answers, whereby the following stress factors were taken into account as risk factors concerning the development of depressive symptoms: “uncertain prospects”, “competition among students”, “shortage of time” as well as “pressure to perform” and “excessive demands”.
Finally, the questionnaire assessed resilience factors. When students reported that they used relaxation techniques (e.g., PMR) it was assumed that the resilience factor “use of relaxation techniques” was present. The resilience factor “study satisfaction” consists of three items and was present if the following items were answered positively: “Do you enjoy your studies?”, “From today’s perspective, would you decide to study psychology/medicine again?” and “how satisfied are you overall with your studies?”. If students indicated that religion was of extreme or moderate importance to them, the resilience factor “religiousness” was considered present. By answering the questions “Do you have regular meals?” and “Do you maintain a healthy diet?” with “yes” or “mostly” we considered the resilience factor “healthy diet” existent. When students reported playing music for one hour or more or doing sports for at least two hours per week, the resilience factors “actively making music” or “sport” were considered present. Finally, the resilience factors “social contact”, i.e. spending time with family, friends and partner, and “emotional support” were given if the corresponding items were answered with “more than enough” or “enough”.
Additionally, because of the often reported link between the personality trait neuroticism and depression [19, 20], participating students also completed the neuroticism subscale of the NEO-FFI [37]. This subscale includes twelve items that can be combined into a total score which, divided by the number of answered items, leads to a scale average ranging from zero to four; the higher the average, the stronger the characteristic of neuroticism. The NEO-FFI is one of the most commonly used personality questionnaires, and there is strong support for its reliability and validity [37]. In the present study, the neuroticism subscale yielded a Cronbach’s Alpha of 0.87.
The BDI-II [38], which is a widely used questionnaire in both clinical and non-clinical samples of adults and adolescents over 13 years [39], was used to assess depressive symptoms. Psychometric properties and validity are well-established [39, 40]. It must be noted that the BDI-II assesses self-reports of experienced symptoms (at different levels of severity), but does not provide diagnosis. The BDI-II covers 21 multiple-choice items that can be rated on a 4-point Likert-type scale ranging from zero to three (maximum total score = 63). Scores above a cut-off of 14 or higher indicate mild depression, 20 and higher moderate depression, and 29 or higher severe depression (<13 = no depression).
Hypotheses
H1: Psychology students differ from medical students by their BDI-II total score.
H2: Risk factors surveyed correlate positively with the BDI-II total score and
H3: resilience factors correlate negatively with the BDI-II total score.
H4: The more risk factors students report, the higher their BDI-II total score, and
H5: the more resilience factors students experience, the lower their BDI-II total score.
Data analysis
The Statistical Package for Social Sciences (SPSS 25.0) was used to carry out the statistical analysis. Descriptive statistics (M, SD, range) were used for the sociodemographic description of the sample, and group differences between medical and psychology students were considered using χ2 and F-test statistics. The investigation of the prevalence of depressive symptoms and the description of the whole sample, as well as of the BDI-II total scores of the two groups, resulted from descriptive statistics (M, SD, median, range) and determination of the absolute and relative frequencies. In addition, significance of the results of the BDI-II was determined by evaluating the degrees of severity [38].
Testing of the first hypothesis was carried out by analysis of covariance controlling for the cofactor gender after homogeneity of variance was verified via the Levene test. Kolmogorov-Smirnov-test compared the empirical distribution function to the normal distribution function, and in case of deviation from the normal distribution, results from the ANCOVA were verified by Kruskal-Wallis-test. Mann-Whitney-U-Test investigated whether differences in the BDI-II classifications (BDI-II severities) were significant. Descriptive statistics and relative frequencies addressed the occurrence of the risk and resilience factors, and χ2-test statistics recorded potential differences between the two groups of students. Pearson’s correlation coefficient was used to show potential connections between risk factors, resilience factors, and the BDI-II total score. Therefore, the remaining hypotheses were tested by Pearson’s r and multiple regression analysis. In order to identify the strongest risk and resilience factors, a post hoc linear regression analysis was calculated including all significant correlating risk and resilience factors. To address the problem of multicollinearity we used a stepwise forward model (pin < 0.05; pout > 0.10) and report VIF statistics. Exploratory, we calculated separate correlations between the BDI-II and the risk or resilience factors for the two groups of students to bring out differences between medical and psychology students.
RESULTS
BDI-II total scores
Table 1 shows the descriptive statistics of the BDI-II total scores. Within all subjects (N = 673) the average total score was M = 9.02 points (SD = 7.16). The mean BDI-II total score among psychology students (n = 109, M = 9.95, SD = 7.34) was more than one point higher than the average score among medical students (n = 564, M = 8.84, SD = 7.12). Inventory scores convert into 12% of the medical and 20% of the psychology students going through mild depression, 6% of the medical students and almost 4% of the psychology students suffering from moderate depression. Almost 3% of the medical students and 4% of the psychology students had a total score of 29 or above which indicates severe depression.
Table 1
Descriptive statistics of the results of the BDI-II total scores and classification of severities for the total sample as well as for the two groups of university students
| Course of study | |||
| Total sample | Medicine | Psychology | |
| (N = 673) | (n = 564) | (n = 109) | |
| BDI-II score | |||
| M (SD) | 9.02 (7.16) | 8.84 (7.12) | 9.95 (7.34) |
| Median | 7 | 7 | 9 |
| Range | 0 –43 | 0 –43 | 0 –36 |
| BDI-II severity | |||
| 0 –13 (%) | 527 (78) | 448 (79) | 79 (72) |
| 14 –19 (%) | 89 (13) | 67 (12) | 22 (20) |
| 20 –28 (%) | 39 (6) | 35 (6) | 4 (4) |
| ≥29 (%) | 18 (3) | 14 (3) | 4 (4) |
Note. BDI-II = Beck Depression Inventory-II, BDI-II severity: 0 –13 points = no or minimal symptoms, 14 –19 points = mild depression, 20 – 28 points = moderate depression, ≥29 points = severe depression.
The Levene-Test (F1,671 = 0.054, p = 0.817) indicated homogeneity of variances across the two groups. Controlling for the difference of gender distribution between the two groups, the group difference in the BDI-II total score was significant (F [df = 1] = 261.9, p = 0.039). The cofactor gender (male/female) also showed a significant influence on the BDI-II total score (F [df = 1] = 5527.7, p = 0.009), the interaction of both factors, however, was not significant (F [df = 1] = 0.001, p = 0.970). Additionally, medical and psychology students differed significantly in the severity of the BDI-II (U = 55371, p = 0.050), however, this does not include correction for gender. Thus, findings support the hypothesis (H1) that medical and psychology students differ by their BDI-II total score (d = 0.16). Descriptive statistics indicate higher BDI-II total scores among psychology students (M = 9.95 vs. M = 8.84). The main effects of the grouping variable and the gender variable were verified non-parametrically (Kruskal-Wallis H = 25.22, p < 0.001), because of a significant deviation of the BDI-II total scores from the normal distribution (Kolmogorov-Smirnov-Z = 0.136, p < 0.001).
Risk and resilience factors
On average, students which participated in this study (N = 673) reportedly were affected by M = 4.15 risk factors (SD = 1.86) and agreed to M = 3.93 (SD = 1.40) resilience factors.
Psychology students showed an average of M = 4.53 (SD = 1.67) risk and M = 4.03 (SD = 1.36) resilience factors; medical students indicate an average of M = 4.08 (SD = 1.89) risk and M = 3.91 (SD = 1.41) resilience factors.
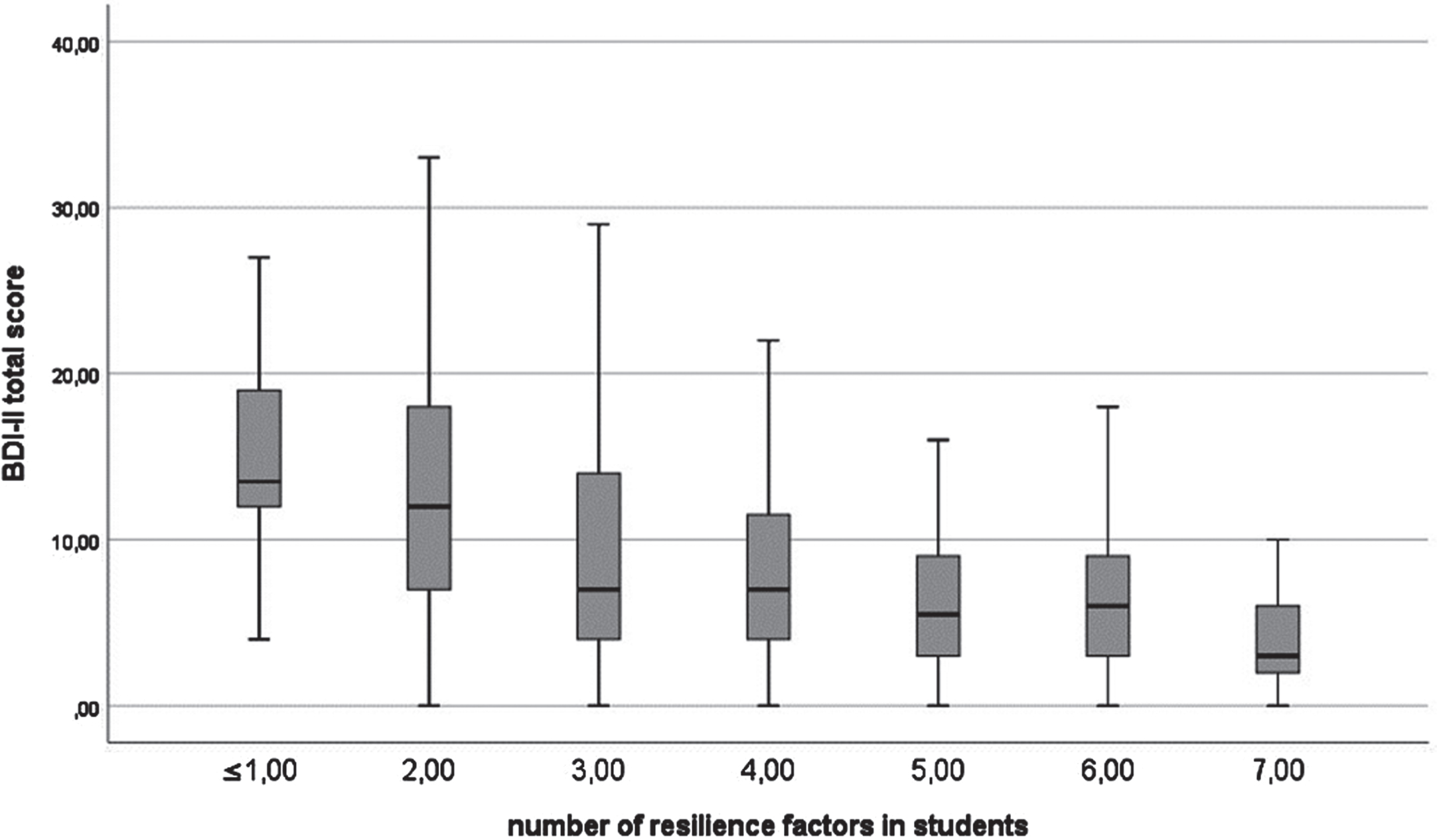
Table 2 shows the bivariate relationship between risk factors including risk factors that are related to the university context and resilience factors, and the BDI-II total score as well as frequencies of these factors among the two groups of students and distribution differences of the variables (Chi-Square Test). The sum of all risk factors showed a significant positive correlation with the BDI-II total score r = .49, p < 0.001 (H2). The more risk factors students experienced the higher was their BDI-II total score (H4; see Fig. 1). An inverse relationship (see Fig. 2) was found between resilience factors and the BDI-II total score; the more resilience factors students experienced, the lower their BDI-II total score r = –0.34, p < 0.001 (H3, H5).
Table 2
Comparison of Prevalence (% , χ2) of Subjectively Reported Risk and Resilience Factors and Pearson Correlation (r) with BDI-II Total Score in Students of Medicine and Psychology
| BDI-II total score r and % | ||||||
| Total r | Medicine | Psychology | ||||
| r | (%) | r | (%) | χ2 (df = 1) | ||
| Risk factor | ||||||
| Positive family history | 0.16 ** | 0.14 ** | 48 | 0.25 * | 55 | 1.58 |
| Female gender | 0.18 ** | 0.18 ** | 67 | 0.14 | 84 | 13.57 ** |
| Low socioeconomic status | 0.06 | 0.06 | 1 | 0.07 | 2 | 0.12 |
| Loss of parent | 0.06 | 0.06 | 17 | 0.02 | 18 | 0.06 |
| Financial worries | 0.18 ** | 0.20 ** | 20 | 0.10 | 22 | 0.26 |
| Alcohol consumption | –0.01 | –0.00 | 29 | –0.03 | 25 | 0.72 |
| Drug abuse | 0.28 ** | 0.33 ** | 9 | 0.02 | 10 | 0.11 |
| Neuroticism (> M+1 SD)a | 0.61 ** | 0.60 ** | 11 | 0.51 ** | 12 | 0.28 |
| Risk factor related to university context | ||||||
| Uncertain prospects | 0.13 ** | 0.12 ** | 2 | 0.14 | 28 | 109.55 *** |
| Competition among students | 0.24 ** | 0.27 ** | 8 | 0.13 | 28 | 37.40 *** |
| Shortage of time | 0.15 ** | 0.16 ** | 51 | 0.14 | 28 | 19.04 *** |
| Excessive demands | 0.30 ** | 0.31 ** | 26 | 0.32 ** | 11 | 11.75 ** |
| Pressure to perform | 0.27 ** | 0.30 ** | 48 | 0.11 | 66 | 12.08 ** |
| Resilience factor | ||||||
| Use of relaxation techniques | 0.04 | 0.06 | 19 | –0.10 | 39 | 21.01 *** |
| Study satisfaction | –0.27 *** | –0.29 ** | 81 | –0.18 | 73 | 3.35 |
| Religiousness | –0.02 | –0.00 | 24 | –0.07 | 16 | 3.81 |
| Healthy diet | –0.14 *** | –0.13 ** | 61 | –0.18 | 65 | 0.61 |
| Actively making music | –0.01 | –0.01 | 32 | –0.03 | 41 | 3.07 |
| Sport | –0.20 *** | –0.20 ** | 69 | –0.18 | 64 | 1.42 |
| Emotional support | –0.40 *** | –0.41 ** | 81 | –0.34 ** | 81 | 0.01 |
| Time for social contacts | –0.16 *** | –0.22 ** | 21 | 0.07 | 32 | 5.95 ** |
Note. r = Pearson’s correlation coefficient, N = 673, medical students n = 564, psychology students n = 109, BDI-II = Beck Depression Inventory-II. aNeuroticism scale –BDI-II correlation r = 0.72 ***, in medical students: r = 0.73 **, in psychology students: r = 0.64 **. *p < 0.05. **p < 0.01. ***p < 0.001.
Fig. 1
Distribution of risk factors as a function of the BDI-II total score. Since sum of risk factors >8 only occurred in n = 8 students, these subjects were added to sum ≥8.
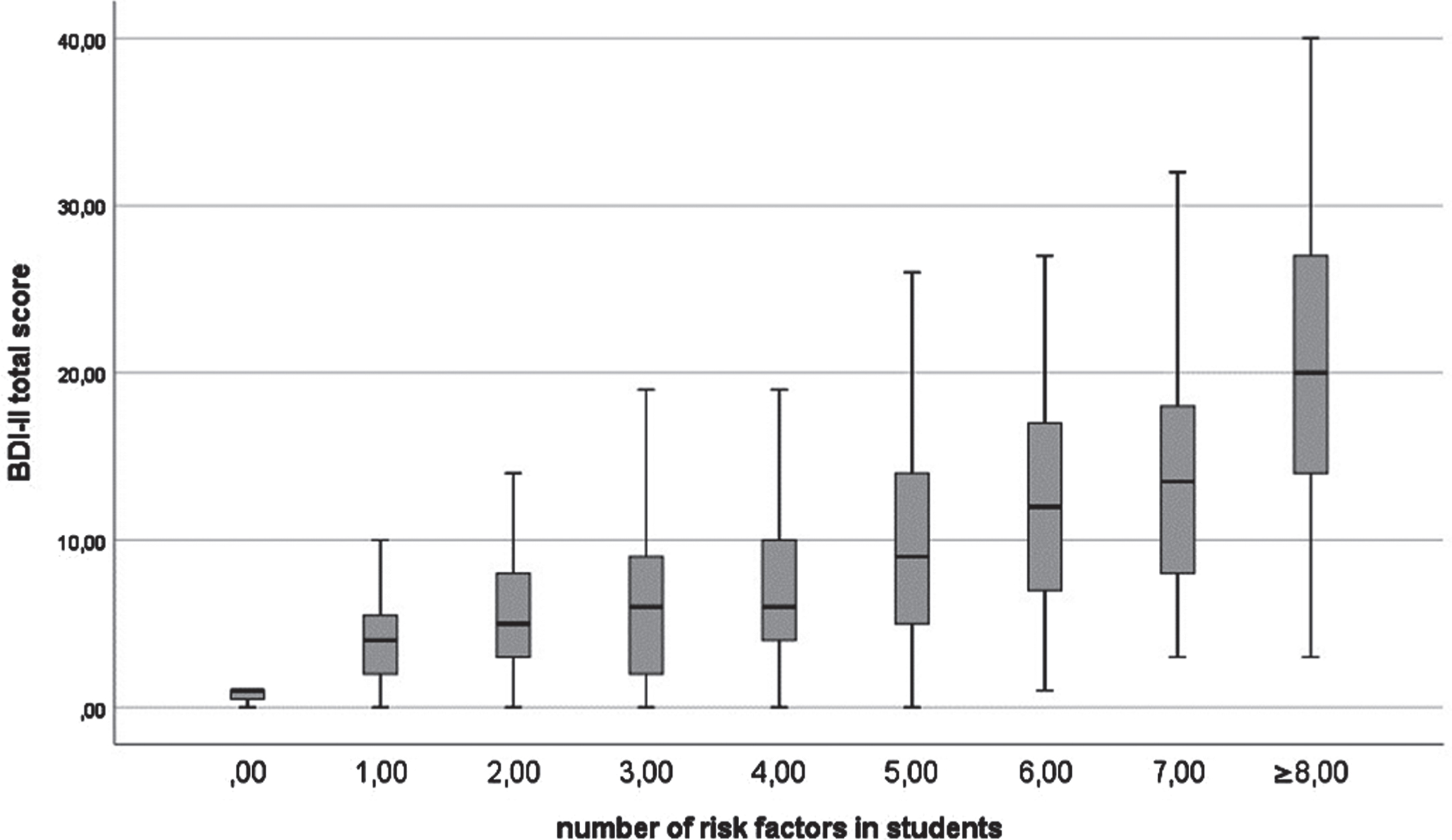
Fig. 2
Distribution of resilience factors as a function of the BDI-II total score. Since sum of resilience factors of 0 only occurred in n = 2 students, these subjects were added to sum ≤1.
A multiple regression analysis (stepwise, pin =0.05, pout = 0.10) for the total sample indicated that the risk factors surveyed were predictive for depressiveness (BDI-II total score). The model for the total sample explains 44% of the variance (corrected R2) of the BDI-II total score and included the following predictors: neuroticism (β= 0.48, p < 0.001), pressure to perform (β= 0.13, p < 0.001), drug abuse (β=0.12, p < 0.001), excessive demands (β= 0.14, p < 0.001), competition amongst students (β= 0.09, p =0.002), financial worries (β= 0.09, p = 0.004), positive family history (β= 0.07, p = 0.020), and shortage of time (β= 0.06, p = 0.037). VIF statistics of the model showed values between 1.03 and 1.12. Overall, the most important predictor neuroticism explained 34% of the variance of the BDI-II total score in the total sample, in the group of medical students neuroticism explained 36% and in the group of psychology students, neuroticism accounted for 25% of the variance.
Moreover, a multiple regression analysis (stepwise, pin = 0.05, pout = 0.10) showed that the resi-lience factors were useful to predict depressiveness (BDI-II total score). The model explains 25% of the variance (corrected R2) of the BDI-II total score and included the following predictors: emotional support (β= –0.33, p < 0.001), study satisfaction (β=–0.22, p < 0.001), sport (β= –0.15, p < 0.001), time for social contacts (β= –0.11, p < 0.001), and a healthy diet (β= –0.08, p = 0.023).
DISCUSSION
Thus far, studies about the mental health of students mainly focus on depressive symptoms among medical students [9, 10]. Interestingly, however, psychology students, do not seem to be less burdened by mental disorders [11], but less frequently studied. Furthermore, the majority of previous research did not take the potential influence of risk and resilience factors on the depressiveness of university students into account. Hence, the present study aimed to assess the prevalence of symptoms related to depression among medical and psychology students and to investigate the influence of certain risk and resilience factors on their mental health. The primary aim was to identify risk factors associated with depressiveness, regardless of the field of study. Additionally, we investigated these correlations separately for both student groups.
Discussion of the results of the BDI-II
We found that the prevalence of self-reported depression (at least mild expressions) was higher in the psychology students (28%) than in the medical students (22%). Thus, the prevalence of depressive symptoms in the present sample of medical students exceeds the prevalence among 18- to 29-year old’s of the general population [5] and is concordant to previous research [10]. Moreover, both groups differ with regard to the BDI-II classification, which additionally indicates that medical and psychology students also differ in terms of the reported severity of depressive symptoms.
Hence, a substantial number of students in both groups reported depressive symptoms. These are figures that call for further attention in future research and may also have practical consequences when thinking of supporting students to successfully and healthy completing their studies. Even higher prevalence rates among the psychology students may relate to a larger number of women that study psychology [15]. Taking the higher prevalence of depressive symptoms in women than in men [5] into account may partially explain the findings. Even though these propositions also apply to the present study, the difference in the prevalence of depressive symptoms cannot be completely explained by the gender difference as the group difference remains even after adjusting for gender.
Although the correlations between competition among students, the pressure to perform, uncertain future prospects and the BDI-II total score fail to reach significance due to the small sample size among psychology students, we would like to emphasize their absolute frequencies and the need for further studies that this implies.
Psychology students more often than medical students report competition among themselves. Given the fact that there are more bachelor graduates in psychology than consecutive postgraduate programs in Germany [15], elevated competition among psychology students is not surprising. Previous studies, in addition, showed a link between a competition-oriented social environment and depression [16].
Supplemental to the increased competition, more than two-thirds of psychology students included in this study find the pressure to perform trying. The pressure to perform can accordingly be interpreted as a logical consequence of the shortage of master programs and the resulting pressure to achieve grades and is also linked to symptoms related to depression [23]. Less than 50% of the medical students reportedly experience pressure to perform and even fewer (<8%) experience competition, which implies a less competitive environment among medical students. Finally, these findings indicate that especially the combination of a competitive environment and pressure to perform facilitates the development of depressive symptoms among psychology students.
Additionally, uncertain prospects are not an issue for medical students but are for almost one third of the psychology students surveyed. Uncertain prospects that include worries about the future are not only regarded as a symptom of depression [41] but also associated with the development of depressive symptoms [23]. Therefore, we assume that uncertain prospects represent a risk factor for the development of depressive symptoms especially for psychology students, even though we cannot determine whether uncertain prospects predominate as a symptom or as a cause of depression.
Summing up and putting back differences in gender distribution, medical and psychology students primarily differ in the prevalence of risk factors related to the university context. The question, if these and other potential differences can causally explain the difference in the BDI-II total scores needs to be tested in future research.
Discussion of potential risk factors
Except for the risk factor neuroticism, which was assessed with the relevant subscale of the NEO-FFI, the potential risk factors were surveyed with a standardized questionnaire. The results support the hypothesis of a positive correlation between risk factors and the BDI-II total score for all risk factors related to the university context and for five of the eight general risk factors. Three risk factors (low socioeconomic status, loss of parent, alcohol consumption) show no association with the BDI-II total score.
The risk factor neuroticism shows the numerically highest correlation with the BDI-II total score and explains 25% of the variance in BDI-II total scores among psychology students and 36% of the variance among medical students. Thus, while neuroticism is an important predictor of depression in both groups, it can be concluded that different mechanisms of action contribute to the development of depressive symptoms. Possibly, among medical students, those who score high in neuroticism are the most vulnerable to depression. People with a high score on neuroticism are regarded as being emotionally unstable and more prone to mental disorders than people with a lower expression of this personality trait [19, 20]. However, it is necessary to indicate again that this explanatory approach may be overestimated by cognitive bias because it is yet unclear how depressive states affect the self-assessment of neuroticism as a trait [42, 43].
The risk factor drug abuse holds the second strongest association to the BDI-II total score, meaning that students who consume drugs more often suffer from symptoms related to depression. This result is in accord with previous research as the link between drug abuse and the development of depressive symptoms is presented in prior studies [21] and, for example, has been reported for cannabis consumption [44]. However, when looking at the groups separately, it is noticeable that, despite almost equal percentages, this applies only to the group of medical students. It would therefore be helpful for future investigations to examine the types of drugs consumed in order to better understand the difference between the groups.
Unsurprisingly, students with financial worries had a higher BDI-II total score than students for whom this risk factor did not apply. Thus, our outcome is in line with results from Aselton [23], who surveyed students in North America, and supports the finding that financial worries can potentially increase students’ depressiveness. When differentiating between the groups, it is apparent that financial worries are primarily associated with depressive symptoms among medical students. The percentage of financial worries, however, is similar in both groups, suggesting that psychology students are less affected by their financial worries. With regard to the risk factors female gender and positive family history, this study yields findings in the expected direction; the prevalence of depressive symptoms is higher among women than among men, and students whose parents, siblings or grandparents suffer from any mental disorder reportedly suffer from more symptoms related to depression than students whose family is not affected by mental disorders. However, this correlation can only be interpreted as small [45] and is robustly lower than correlations reported by McGuffin et al. [46] and Lieb et al. [18], which may relate to the fact that the present study records mental disorders in general and not depression specifically. No significant correlation could be found between the socioeconomic status of the students’ parents and depressiveness or between the loss of parent and depressiveness. Therefore, we could not identify these factors as potential risk factors in the present study. Only a very few students of the present sample reportedly come from a family with low socioeconomic status, so that by the majority this potential risk factor does not affect the students surveyed.
Looking at potential risk factors related to the university context, each of the examined factors indicates a positive correlation with the BDI-II total score. Aside from those mentioned, excessive demands and shortage of time need to be highlighted. Both factors are predominant in the group of medical students; more than 50% of the medical students reportedly suffer from a shortage of time and one-third report excessive demands. Different from the psychology course, medical students must take a test either before or after most of the seminars, sometimes several times per week. Furthermore, medical students need to study more than 40 hours per week [47], which is above average and may represent an extra burden. Hence, shortage of time and excessive demands especially among medical students are not surprising and our findings replicate the results from Jurkat et al. [10]; the higher the perceived shortage of time and workload of the students, the worse their depressive symptoms.
Finally, ten of the risk factors investigated in this study not only have an individual but also a cumulative effect on the prevalence of depressive symptoms among medical and psychology students; the more risk factors students report, the higher their BDI-II total score. Altogether 33% of the variance of the BDI-II total score (i.e., of the variation in depressiveness among the students), can be explained with the identified risk factors.
Discussion of potential resilience factors
Five of the eight resilience factors surveyed show the expected correlation and therefore a potential buffering effect against the development of symptoms related to depression. Moreover, students’ depressiveness decreases with an increasing number of resilience factors. More than 24% of the variance in the BDI-II total scores can be explained with the following resilience factors: emotional support, study satisfaction, healthy diet, sport and time for social contacts. Emotional support indicates the strongest association with the BDI-II total score in the present study; the more emotional support students experience the lower their depressive symptoms. Therefore, findings from Dyrbye et al. [7], indicating a positive relationship between support from family, friends or lecturer and resilience are also replicated within the present sample. Looking at the two groups separately, notable, only the latter potential resilience factor is significantly associated with the depressiveness of psychology students. Other factors (healthy diet, exercise, and study satisfaction) show similar correlation coefficients that, however, fail to reach statistical significance due to a smaller sample size.
Possible practical implications
These findings lead to various possible starting points for supporting students in their studies and counteracting the development of depressive symptoms. First of all, the results of the BDI-II emphasize the importance of psychosocial counseling services at universities. Here, we feel it is particularly important to make the existing services more visible and accessible to students. Moreover, we see our results as a good starting point for the development of concrete interventions for students to help them cope with study-related stressors and organizational issues (e.g., planning their courses; help with making deadlines for administrative issues; etc.). Drug consumption showed the second-highest correlation with the BDI-II total score. Consequently, a further implication could be to educate students to a greater extent about the consequences which drugs can cause on mental health and therefore promote the use of evidence-based prevention programs.
Limitations and future research
All in all, the present investigation highlights the mental stress among medical students, indicates an even higher prevalence of depressive symptoms among psychology students, and points out a potential link between several risk and resilience factors and depressive symptoms. The correlations between risk or resilience factors and results of the BDI-II total score, however, do not allow us to draw any conclusions about causality. Furthermore, the ability to generalize the results is limited, since the present sample is drawn from one single German university. Nevertheless, it is plausible to assume that studies in medicine and psychology are comparable between different cities in Germany and that students, by the majority, are exposed to the same risk factors. Therefore, we suppose that similar results can also be expected at other universities. Regardless, further research at more universities is needed to enhance the meaningfulness of the results. Further research is also essential with regard to risk and resilience factors. The present study only takes up a selection of potential factors, which may cause depressive symptoms or have a protective effect against depression. Future research, investigating additional risk and resilience factors, can potentially support a deeper understanding of the development of depressive symptoms among medical and psychology students. At this point, we would like to mention the use of positive cognitive strategies (e.g., positive reappraisal) as another potential resilience factor. Due to limited resources, we could not address this factor in the present study, but we see its relevance also for potential interventions. The effectiveness of cognitive strategies as a resilience factor has already been demonstrated in previous studies [48, 49]. In the future, it will, therefore, be of vital importance to address to what extent students are equipped with effective cognitive coping strategies or whether interventions in the university setting can be helpful in this respect.
Moreover, the present cross-sectional research design does not imply information about the intraindividual development of depressive symptoms in the course of studies. Further research questions arise at this point: How does the prevalence of symptoms related to depression vary between the first and the last semester, and how do bachelor students differ from postgraduate students? Regarding a comparison between bachelor and master psychology students, it seems reasonable to suppose that graduate students experience less pressure to perform and competition among students, as they do not have to worry about getting into the master program at this point. In this context, we would like to make a reference to the new law reform regarding education in psychological psychotherapy in Germany which becomes effective in September of 2020. This reform provides for the establishment of a course of study exclusively for psychotherapy next to the existing studies of psychology2.
Consequently, the reform may alleviate the current shortage of master degree programs and therefore ease the tense situation regarding the competition among students. However, currently open questions and debates about the financing of the new programs may be perceived as additional strain to psychology students though.
In addition, the extent to which the problems described can be transferred to other countries needs to be discussed. As a result of the Bologna reform, there has been an international standardization of study programs, which is why we assume that the above-mentioned difficulties, particularly with regard to university risk factors, are also of cross-border relevance. One difference, however, is the postgraduate training to become a psychological psychotherapist, which is not necessary in non-German speaking countries. The extent to which this additional training has an impact on the mental health of students will have to be investigated in future studies and the effects of the new reform will have to be shown.
Above all, it is crucial to point out that questionnaires used in the present survey are based on self-assessment and therefore may be biased (e.g., socially desirable responding). Diagnostic methods conducted by clinicians are imperative for diagnosis of depression, whereas self-report instruments such as the BDI-II can only give an indication about the prevalence or severity of the symptoms. There is scientific discourse about the accuracy of self-report instruments: while some argue that these instruments tend to overestimate the prevalence of depression [50], others discuss the opposite [51]. Hunt‘s, Auriemma and Cashaw’s investigations reveal a possible underestimation of depression by using the BDI-II, even indicating an underestimated prevalence of depressive symptoms [51]. While remaining critical towards self-report instruments, we would like to point out not only the high concordance between clinical diagnosis of depression and results of the BDI-II, but also its ability to distinguish between different levels of severity as well as its sensitivity to change [52]. To sum up, the BDI-II has not been developed to diagnose depression, but it is reliable to assess the prevalence of symptoms related to depression.
Whisman and Richardson investigated a norming sample consisting of students of various disciplines and found an average BDI-II total score which is only slightly different from that of the present study [53]. Finally, we want to pose the question, how students of other courses are affected by an increased prevalence of symptoms related to depression.
Acknowledgements including sources of support
We like to thank all students that participated in this study.
ACKNOWLEDGMENTS
The authors have no acknowledgments to report.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
REFERENCES
[1] | Wittchen HU , Jacobi F , Rehm J , Gustavsson A , Svensson M , Jönsson B , et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. European Neuropsychopharmacology. (2011) ;21: :655–79. doi:10.1016/j.euroneuro.2011.07.018 |
[2] | Jacobi F , Höfler M , Strehle J , Mack S , Gerschler A , Scholl L , et al. Psychische Störungen in der Allgemeinbevölkerung. Studie zur Gesundheit Erwachsener in Deutschland und ihr Zusatzmodul Psychische Gesundheit (DEGSI-MH). Nervenarzt. (2014) ;85: :77–87. doi:10.1007/s00115-013-3961-y |
[3] | Depression and Other Common Mental Disorders: Global Health Estimates. Geneva: World Health Organization; 2017. Licence: CC BY-NC-SA 3.0 IGO. |
[4] | Wittchen HU , Jacobi F , Klose M , Ryl L . Depressive Erkrankungen. In: Robert Koch-Institut, editors. Gesundheitsberichterstattung des Bundes (Heft 51). Berlin: RKI; 2010. PP. 1-46. |
[5] | Busch MA , Maske UE , Ryl L , Schlack R , Hapke U . Prävalenz depressiver Symptomatik und diagnostizierter Depression bei Erwachsenen in Deutschland. Bundesgesundheitsblatt. (2013) ;56: :733–9. doi:10.1007/s00103-013-1688-3 |
[6] | Grobe T , Steinmann S . Gesundheit von Studierenden. In Techniker Krankenkasse, editors. Gesundheitsreport 2015. Hamburg: Techniker Krankenkasse; 2015. |
[7] | Dyrbye LN , Thomas MR , Shanafelt TD . Systematic Review of Depression, Anxiety and Other Indicators of Psychological Distress among U. S. and Canadian Medical Students. Academic Medicine. (2006) ;81: (4):354–65. Available from: https://journals.lww.com/academicmedicine/Fulltext/2006/04000/Systema-tic_Review_of_Depression,_Anxiety,_and.9.aspx |
[8] | Rotenstein LS , Ramos MA , Torre M , Segal JB , Peluso MJ , Guille C , et al. Prevalence of Depression, Depressive Symptoms, and Suicidal Ideation Among Medical Students A Systematic Review and Meta-Analysis. JAMA The Journal of the American Medical Association. (2016) ;316: (21):2214–36. doi:10.1001/Jama.2016.17324 |
[9] | Seliger K , Brähler E . Psychische Gesundheit von Studierenden der Medizin. Psychotherapeut. (2007) ;52: (4):280–6. doi:10.1007/s00278-006-0529-3 |
[10] | Jurkat HB , Richter L , Cramer M , Vetter A , Bedau S , Leweke F , Milch W . Depressivität und Stressbewältigung bei Medizinstudierenden. Nervenarzt. (2011) ;82: (5):646–52. doi:10.1007/s00115-010-3039-z |
[11] | Von Sydow K . Psychotherapeuten und ihre psychischen Probleme. Psychotherapeut. (2014) ;59: (4):283–92. doi:10.1007/s00278-014-1056-2 |
[12] | Grützmacher J , Gusy B , Lesener T , Sudheimer S , Willige J . Gesundheit Studierender in Deutschland 2017. In: Techniker Krankenkasse, Freie Universität Berlin, Deutsches Zentrum für Hochschul- und Wissenschaftsforschung, editors. 2018. |
[13] | Masten R , Tušak M , Zalar B , Ziherl S . (2009). Stress, Coping and Social Support in Three Groups of University Students. Psychiatria Danubina. (2009) ;21: (1):41–8. Available from: https://pdfs.semanticscholar.org/3c58/2adfa52d25708e160c476b99acc253f1ae01.pdf |
[14] | Schmidt-Gürtler LSU . Stressbewältigung und Lebensqualität im Bachelorstudiengang Psychologie (Inauguraldissertation). 2013. [cited 2019 May 5] Available from: http://geb.uni-giessen.de/geb/voltexte/2015/11400/ |
[15] | Abele-Brehm A . Zur Lage in der Psychologie. Psychologische Rundschau. (2017) ;68: (1):1–19. doi:10.1026/0033-3042/a000346 |
[16] | Gilbert P , McEwan K , Bellew R , Mills A , Gale C . The dark side of com-petition: How competitive behavior and striving to avoid inferiority are linked to depression, anxiety, stress and self-harm. Psychology and Psychotherapie Theory, Research and Practice. (2009) ;82: :123–36. doi:10.1348/147608308X379806 |
[17] | Brakemeier EL , Normann C , Berger M . Ätiopathogenese der unipolaren Depression. Gesundheitsblatt.. (2008) ;51: (4):379–91. doi:10.1007/s00103-008-0505-x |
[18] | Lieb R , Isensee B , Höfler M , Pfister H , Wittchen HU . Parental Major Depression and the Risk of Depression and Other Mental Disorders in Offspring. Arch Gen Psychiatry. (2002) ;59: :365–74. doi:10.1001/archpsyc.59.4.365 |
[19] | Costa PT , McCrae RR . Normal Personality Assessment in Clinical Practice: The NEO Personality Inventory. Psychological Assessment. (1992) ;4: (1):5–13. |
[20] | Malouff JM , Thorsteinsson EB , Schutte NS . The Relationship Between the Five-Factor Model of Personality and Symptoms of Clinical Disorders: A Meta-Analysis. Journal of Psychopathology and Behavioral Assessment. (2005) ;27: (2):101–14. doi:10.1007/s10862-005-5384 |
[21] | Kupferschmidt H , Fattinger K . Medizinische Probleme beim Konsum illegaler Drogen. [updated n. d.; cited 2019 May 20] Available from: https://docplayer.org/10108660-Medizinische-prob-leme-beim-konsum-illegaler-drogen.html |
[22] | Kendler KS , Karkowski LM , Prescott CA . Causal Relationship between Stressful Life Events and the Onset of Major Depression. American Journal of Psychiatry. (1999) ;156: (6):837–41. doi:10.1176/ajp.156.6.837 |
[23] | Aselton P . Sources of Stress and Coping in American College Students Who Have Been Diagnosed With Depression. Journal of Child and Adolescent Nursing. (2012) ;25: :119–23. doi:10.1111/j.1744-6171.2012.00341.x |
[24] | Misra R , Castillo LG . Academic Stress among College Students: Comparison of American and International Students. International Journal of Stress Management. (2004) ;11: (2):132–48. doi:10.1037/1072-5245.11.2.132 |
[25] | Noeker M , Petermann F . Resilienz: Funktionale Adaptation an widrige Umgebungsbedingungen. Zeitschrift für Psychiatrie, Psychologie und Psychotherapie. (2008) ;56: :255–63. doi:20.1024/1661-4747.56.4.255 |
[26] | Lolak S , Connors GL , Sheridan MJ , Wise TN . Effects of Progressive Muscle Relaxation Training on Anxiety and Depression in Patients Enrolled in an Outpatient Pulmonary Rehabilitation Program. Psychotherapy and Psychosomatics. (2008) ;77: :119–25. doi:10.1159/000112889v |
[27] | Babiss LA , Gangwish JE , James E . Sports Participation as a Protective Factor against Depression and Suicidal Ideation in Adolescents as Mediated by Self-Esteem and Social Support. Journal of Developmental & Behavioral Pediatrics. (2009) ;30: (5):376–84. doi:10.1097/DBP.0b013e3181b33659 |
[28] | Greist JH , Klein MH , Eischens RR , Faris J , Gurman AS , Morgan WP . Running as a Treatment for Depression. Comprehensive Psychiatry. (1979) ;20: (1):41–54. doi:10.1016/0010-440X(79)90058-0 |
[29] | Bonelli R , Dew RE , Koenig HG , Rosmarin DH , Vasegh S . Religious and Spiritual Factors in Depression: Review and Integration of the Research. Depression Research and Treatment. 2012;ID:962860. doi:10.1155/2012/962860 |
[30] | Schek A . Einfluss der Ernährung auf Depressivität und Stresstoleranz. Psychotherapeutische Praxis. (2003) ;3: (4):163–72. doi:10.1026//1616-1041.3.4.163 |
[31] | Dyrbye LN , Power DV , Massie FS , Eacker A , Harper W , Thomas MR , et al. Factors associated with resilience to and recovery from burnout: a prospective, multi-institutional study of US medical students. Medical Education. (2010) ;44: :1016–26. doi:10.1111/j.1365-2923.2010.03754.x |
[32] | Seinfeld S , Figueroa H , Ortiz-Gil J , Sanchez-Vives MV . Effects of music learning and piano practice on cognitive function, mood and quality of life in older adults. Frontiers Psychology. (2013) ;4: (810):1–13. doi:10.3389/fpsyg.2013.00810 |
[33] | Dupuis SL , Smale BJA . An Examination of Relationship Between Psychological Well-Being and Depression and Leisure Activity Participation Among Older Adults. Loisir et Sciété/Society and Leisure. (1995) ;18: (1):67–92. doi:10.1080/07053436.1995.10715491 |
[34] | Fahrenkopf AM , Sectish TC , Barger LK , Sharek PJ , Lewin D , Chiang VW , et al. Rates of medication among depressed and burnt out residents: Prospective cohort study. BMJ. (2008) ;336: (7642):488–91. doi:10.1136/bmj.39469.763218.BE |
[35] | Enochs WK , Etzbach CA . Impaired Student Counselors: Ethical and Legal Considerations for the Family. The Family Journal. (2004) ;12: (4):396–400. doi:20.1177/1066480704267240 |
[36] | Guy JD , Poelstra PL , Stark MJ . Personal distress and therapeutic effectiveness: National survey of psychologists practicing psychotherapy. Professional Psychology: Research and Practice. (1989) ;20: (1)48–50. doi:10.1037/0735-7028.20.1.48 |
[37] | Borkenau P , Ostendorf F , editors. NEO-Fünf-Faktoren-Inventar nach Costa und McCrae. 2nd ed. Göttingen: Hogrefe; 2008. |
[38] | Hautzinger M , Keller F , Kühner C , editors. Beck-Depression-Inventar-II German edition. 2nd ed. Frankfurt: Pearson Assessment; 2009. |
[39] | Kühner C , Bürger C , Keller F , Hautzinger M . Reliabilität und Validität des revidierten Beck-Depressions-inventar (BDI-II). Der Nervenarzt. (2007) ;78: (6):651–6. doi:10.1007/s00115-006-2098-7 |
[40] | Herzberg PY , Goldschmidt S , Heinrichs N . Beck Depression-Inventar (BDI-II) Revision. Reportpsychologie. (2008) ;33: (6):301–2. |
[41] | Dilling H , Mombour W , Schmidt MH editors. Internationale Klassifikation psychischer Störungen ICD-10. Bern: Verlag Hans Huber; 2005. Chapter V (F). |
[42] | Griens AMGF , Jonker K , Blom . The influence of depressive state features on trait measurement. Journal of affective Disorders. (2002) ;70: (1):95–9. doi:10.1016/S0165-327(00)00371-2 |
[43] | Liebowitz MR , Stallone F , Dunner DL , Fieve RF . Personality features of patients with primary affective disorder. Acta Psychiatrica Scandinavia. (1979) ;60: (2):214–24. doi:10.1111/j.1600-0447.1979.tb03590.x |
[44] | Horwood LJ , Fergusson DM , Coffey C , Patton GC , Tait R , Smart D , et al. Cannabis and depression: An integrative data analysis of four Australian cohorts. Drug and Alcohol Dependence. (2012) ;126: (3):369–78. doi:10.1016/j.drugalcdep.2012.06.002 |
[45] | Cohen J . Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale, N.J.: Erlbaum Associates; 1988. |
[46] | McGuffin P , Rijsdijk F , Andrew M , Sham P , Katz R , Cardno A . The Heritability of Bipolar Affective Disorder and the Genetic Relationship to Unipolar Depression. Arch Gen Psychiatry. (2003) ;60: :497–502. doi:10.1001/archpsyc.60.5.497 |
[47] | Multus F , Majer S , Bargel T , Schmidt M . Studiensituation und studentische Orientierung –13. Studierendensurvey an Universitäten und Fachhochschulen. In: Bundesministerium für Bildung und Forschung, editors. Berlin: BMBF; 2017. pp. 8-16. |
[48] | Garnefski N , Teerds J , Kraaji V , Legerstee J , van den Kommer T . Cognitive emotion regulation strategies and depressive symptoms: differences between males and females. Personality and Individual Differences. (2004) ;36: (2):267–76. doi:10.1016/S0191-8869(03)00083-7 |
[49] | Garnefski N , Legerstee J , Kraaji V , van den Kommer T , Teerds J . Cognitive coping strategies and symptoms of depression and anxiety: a comparison between adolescents and adults. Journal of Adolescence. (2002) ;25: (6):603–11. doi:10.1006/jado.2002.0507 |
[50] | Thombs BD , Kwakkenbos L , Levis AW , Benedetti A . Addressing overestimation of the prevalence of depression based on self-report screening questionnaires. CMAJ. (2018) ;190: (2):E44–E49. doi: 10.1503/cmaj.170691 |
[51] | Hunt M , Auriemma J , Cashaw ACA (2003). Self-Report Bias and Underreporting of Depression on the BDI-II. Journal of Personality Assessment. (2003) ;80: (1):26–30. doi: 10.1207/S15327752JPA8001_10 |
[52] | Kühne C , Bürger C , Keller F , Hautzinger M (2007). Reliabilität und Validität des revidierten Beck-Depressions-inventars (BDI-II). Nervenarzt. (2007) ;78: :651–6. doi: 10.1007/s00115-006-2098-7 |
[53] | Whisman MA , Richardson ED . Normative Data on the Beck-Depression- Inventory –Second Edition (BDI-II) in College Students. Journal of Clinical Psychology. (2015) ;71: (9):898–907. doi:10.1002/jclp.22188 |
Notes
1 The German grading system ranges from 1 (= best) to 5 (= worst). There is a chance of getting in with worse grades if being on a waitlist. Students usually apply at many Universities for a place in the master program and select from their offers.
2 Pending open questions of financing issues for the Psychology Departments.


