
Clinical Decision Trees to Guide Physical Therapy Management of Persons with Huntington’s Disease
Abstract
Background:
In 2020, our group published physical therapy clinical practice guidelines (CPG) for people with Huntington’s disease (HD). The guideline recommendations were categorized according to six primary movement impairment classifications.
Objective:
To facilitate implementation of this CPG, we have developed guideline-based algorithms for physical therapy assessments and interventions and recommendations for therapists to overcome barriers to CPG implementation for people with HD.
Methods:
We conducted a literature review of papers that evaluated physical therapy interventions in individuals with HD (n = 26) to identify assessments for each of the primary movement impairment classifications, and then searched for papers (n = 28) that reported their clinometric/psychometric properties in HD. Assessments were evaluated using modified Movement Disorder Society Committee on Rating Scales criteria and other relevant criteria.
Results:
We identified a “core set” of physical therapy assessments for persons with HD, including the Six Minute Walk Test, Timed Up and Go Test, Berg Balance Scale, and the Medical Outcomes Study Short Form 36 (SF-36). We then developed guideline-based decision trees to assist in decision making and implementation of the CPG into practice for persons with HD across the continuum of care. Finally, we developed strategies for overcoming barriers to implementation, such as seeking specialized training in HD, engaging caretakers or family members to help the person with HD to exercise, and establishing clinical pathways that support early physical therapy referrals.
Conclusion:
Knowledge translation documents such as this are essential to promoting implementation of the physical therapy CPGs into clinical practice.
INTRODUCTION
Huntington’s disease (HD) is a progressive hereditary neurodegenerative disease that causes death of neurons in the basal ganglia, impacting motor, cognitive, and psychological function [1]. HD affects approximately 40,000 Americans [2], with another 200,000 at risk of developing the condition [3]. The physical therapist is a key member of the interdisciplinary team for persons with HD. Without disease modifying therapies, physical therapy and other rehabilitation interventions offer the next best option for secondary prevention and optimizing functional abilities over the course of neurodegenerative diseases [4]. The role of the physical therapist in the care of persons with HD will vary through the course of the disease, ranging from prevention of mobility restriction in the prodromal and early manifest stages, to maintaining function and slowing down progression in the middle stages, and to limiting the impact of complications and providing supportive care in late stages of the disease [5].
Physical therapy improves motor function in persons with HD [6]. We recently published clinical practice guidelines to guide physical therapy interventions for persons with HD [7]. Specifically, there is Grade A evidence to support 1) aerobic exercise paired with strengthening exercises to improve fitness and to stabilize or improve motor function; and 2) one-on-one supervised gait training to improve spatiotemporal measures of gait. Grade B evidence supports 1) individualized exercise, including balance exercise, to improve balance and balance confidence; and 2) inspiratory and expiratory training to improve respiratory muscle strength and cough effectiveness. The clinical guidelines were further categorized according to six previously identified treatment-based classifications, referred to as primary movement impairment classifications in this paper, to better match clinical guidelines with the individual’s primary movement problems (e.g., mobility and function, balance and falls risk) [7].
As a next step to implementation of these clinical guidelines into practice, we have now developed guideline-based decision tree models and provide recommendations for physical therapy assessments. Visually-based decision tree models can assist physical therapists to plan and make decisions regarding the management of individuals with complex and heterogeneous disorders such as HD [8]. Clinical decision trees help guide clinicians through physical therapy evaluation and plan of care with specific attention to identifying the primary movement dysfunction, choosing appropriate assessments with published psychometrics for persons with HD, and selecting evidence-supported interventions. To improve the translation of clinical guidelines into practice, we identified the need for assessments to screen for dysfunction and to assess changes resulting from physical therapy interventions in body structure and function, activity, and participation [9].
This paper aims to: 1) recommend clinical assessments based on available literature for each of the primary movement impairment classifications; 2) provide guideline-based decision trees to aid in decision-making and implementation of a physical therapy plan of care for individuals with HD; 3) apply the proposed decision trees using patient examples, and 4) recommend strategies to overcome barriers and to facilitate implementation of the guidelines.
PHYSICAL THERAPY ASSESSMENTS FOR PERSONS WITH HD
Literature search
We conducted a literature review to determine assessments that have been used to evaluate physical therapy interventions in individuals with HD. A systematic approach was employed; we used the same search terms from our 2017 systematic review [6] to capture all studies included in the clinical guidelines and any studies published since from 2017 to January of 2022 (n = 26). We reviewed the assessments used in each study and then searched for articles that reported on their clinometric/psychometric properties in HD (n = 28). Our search focused on assessments that measure activity and participation levels of the International Classification of Functioning, Disability and Health (ICF) [10] and align with the primary movement classifications detailed in the CPG [4]. Impairment-based assessments that are used as part of the standard neurologic examination of a patient (e.g., manual muscle testing, range of motion) were not included.
Critical appraisal process
We evaluated each of the listed measures by adapting the criteria for rating scales proposed by the Movement Disorders Society Committee on Rating Scales Development [11]. Clinical assessments were recommended if the measures had (1) been used in the HD population; (2) used in HD by groups other than the original developers and data on their use were available; and if (3) the available clinometric/psychometric data in HD supported properties of reliability and/or predictive accuracy (i.e., test-retest reliability, minimal detectable change, sensitivity/specificity and score cut-offs), and validity (i.e., discriminative and/or concurrent), and responsiveness to interventions in clinical trials. For assessments not developed for use in HD, criterion 2 could also be fulfilled if used in at least one group in HD that reported any kind of clinometric/psychometric properties in HD. Clinical assessments were suggested if the measures had (1) been used in the HD population; and (2) only one other criterion (2) or (3) from the recommended category were fulfilled. Clinical assessments were listed if the measures had been applied to the HD population, but no further criteria were met. Through an iterative consensus process, we evaluated assessments with the modified MDS ratings scale recommendations (Table 1). Recommended measures for persons with HD were then examined to determine their 1) clinical research utility in terms of psychometrics (Table 1); 2) clinical utility in terms of time to complete, ease of use, and accessibility; and 3) alignment with the Academy of Neurologic Physical Therapy (ANPT) recommended core outcomes measures [12], to develop a recommended core set of assessments for physical therapists to use with all persons with HD (see Fig. 1).
Table 1
Physical Therapy Assessments in Huntington’s Disease
| Measure | Recommendation | Test-Retest Reliability | MDC | Fall risk cutoff | Discriminative and Concurrent Validity/Responsiveness (DCR) |
| Activity-Specific Balance Scale** | Suggested for assessing level of self-reported balance confidence in HD. | ICC = 0.74 [31] | 27.33 [31] | Unknown in HD | D –discriminates fallers vs. non-fallers [32] C –unknown R –conflicting results: positive 1 study [33], but negative 2 studies [34, 35] |
| Backward walking velocity (m/s) | Listed for assessing backward walking speed. | ICC = 0.98 [31] | 0.17 [31] | Unknown in HD | D –unknown C –unknown R –unknown |
| Berg Balance Scale (BBS) original** | Recommended for assessing severity of balance impairment in ambulatory clients with HD across all stages and fall risk screening. | ICC = 0.86 pre-manifest; 0.96 manifest [36] | 1 in pre-manifest; 5 in manifest HD [36] | <40 predicts being a “faller” with probability of 60% [23] | D –discriminates Stage I vs. II/III [36, 37] C –concurrent validity with UHDRS-TFC & -TMS, HD-ADL [38] and falls [37] R –positive evidence 1 study [39] |
| Berg Balance Scale (BBS) Shortened version (Busse, 2014 [38]) | Suggested; Shortened version is items 7, 11, 12, 13, 14. | ICC = 0.90 [38] | 4 in manifest [38] | Unknown in HD | D –AUC for ROC analysis for discrimination pre-manifest or manifest with original BBS = 0.91 [38] C –unknown R –unknown |
| Dynamic Gait Index | Listed for assessing gait performance in manifest HD. | Unknown | Unknown | Unknown in HD | D –unknown C –unknown R –responsive to anti-choreic medication intervention [39] |
| Fitness (predicted (Storer et al. [40]) or actual VO2 max) | Recommended for assessing cardiovascular fitness. | Unknown but often considered the “gold standard” for assessing the effect of exercise training on cardiorespiratory fitness [41] | Unknown | N/A | D –discriminates manifest HD from pre-manifest and healthy control at 50 W submaximal exercise intensity [42] C –unknown R –positive evidence 2 studies [43, 44] |
| Five Times Sit-to-Stand Test (5TSST)** | Listed for assessing ability to perform transitional movements. | Unknown | Unknown | N/A | D –unknown C –unknown R –responsive to anti-choreic medication intervention [45] |
| Four Square Step Test (FSST) | Suggested for assessing dynamic balance in premanifest and early-stage HD. | ICC = 0.91 pre-manifest; 0.78 in manifest [36] | 1.9 in pre-manifest; 15.2 in manifest [36] | Unknown in HD | D –Poor discrimination across stages [36] C –Moderate to high correlations with the ABC, TMT, and gait velocity [31] R –unresponsive in 1 study [31] |
| Goal Attainment Scale | Listed for assessing individualized goal setting (Quinn et al. [46]) | N/A | Unknown | N/A | D –unknown C –unknown R –responsive to task-specific training intervention (91% goal attainment) [46] |
| HDQLIFE End of Life Measures | Listed to measure domains including meaning and purpose, concern with death/dying, and end of life planning. | ICC > 0.7 [47] | Unknown | Unknown | D –unknown C –unknown R –unknown |
| Huntington’s disease health-related quality of life questionnaire (HDQoL) | Suggested for assessing Health-Related Quality of life. Domains include physical-functional, cognitive, mood, and worries. | ICC = >0.7 for all domains [48] | Unknown | N/A | D –unknown C –summary score moderately correlated with SF-12 version2 and EuroQol domains [48] R –limited evidence 1 study (effect size 0.19) [46] |
| Huntington’s Disease Quality of Life - Caregiver Scale (HD-QoL-C) | Suggested for use with HD caregivers to assess caregiver burden. | Pearson’s correlation coefficients 0.78–0.90 [49] | Unknown | N/A | D –unknown C –low correlation with WHOQOL-BREF [49] R –unknown |
| International Physical Activity Questionnaire (IPAQ) physical activity (MET min/week) | Suggested for assessing self-reported physical activity. | ICC = 0.44 pre-manifest; 0.74 manifest [36] | 3,632 in pre-manifest; 2,792 in manifest [36] | N/A | D –discriminates Stage I vs. II/III [36]; control vs. HD [50] C –unknown R –some positive evidence [14, 43] |
| Medical Outcomes Study Short-Form 36 (SF-36 version 1 and 2) and Medical Outcomes Study Short-Form 12 (SF-12 version 1 and 2) | Recommended (SF-36) 36 item patient-reported outcome measure to quantify health status and measure health-related quality of life. Suggested (SF-12) 12 item patient-reported outcome measure to quantify health status and measure health-related quality of life. | ICC > 0.7 for all dimensions of SF-36 [51] Reliability unknown for SF-12 | Unknown in HD | N/A | D –unknown C –concurrent validity of physical functioning and mental health SF-36 subscales with UHDRS [51] R –total score, vitality score, and mental component SF-36 score responsive to change in manifest HD clinical trials [52]; SF-12 physical component sensitive to change following multi-disciplinary rehabilitation [35] |
| Mini-Balance Evaluation Systems Test (Mini BESTest) | Suggested for assessing severity of balance impairment in HD. | Unknown in HD | Unknown in HD | Unknown in HD | D –discriminates people with HD vs. healthy controls [44] C –concurrent validity with UHDRS-TFC & -TMS [44] R –unknown |
| Physical activity (measured by physical activity monitors (amount of time in sedentary, MVPA or step counts) | Listed for assessing physical activity. | Unknown in HD | Unknown in HD | N/A | D –Fitbit activity scores did not discriminate between prodromal/ Stage I participants with HD and healthy controls [41]; GeneActiv wearable accelerometer discriminates between manifest HD and healthy controls [53] C –unknown R –unresponsive 1 study [54] |
| Physical Performance Test (PPT) | Suggested for assessing severity of impairment of physical function in tasks simulating ADLs across all disease stages. | ICC = 0.76 pre-manifest; 0.95 in manifest [36] | 3 points pre-manifest; 5 points for manifest [36] | N/A | D –discriminates premanifest/ I vs. II/III; ceiling effect in pre-manifest HD [36] C –concurrent validity with UHDRS-TMS, -FAS, and -TFC [38] R –unknown |
| Posturography | Listed for assessing balance impairment if equipment is available | Unknown in HD | Unknown in HD | Unknown in HD | D –static sway in eyes open and eyes closed discriminates controls from persons with manifest HD and pre-manifest HD from manifest HD [55]. Static sway during single and dual-tasks discriminates controls from persons with manifest HD [20]. (Muratori) Sway in sitting and standing discriminates controls from pre-manifest and manifest HD [56]. C –unknown R –unresponsive in pre-manifest HD (Bartlett, 2020 [57]; responsive in early-mid stage HD in 1 study [33]. |
| Six-Condition Romberg Test | Suggested for assessing severity of balance impairment in HD. | ICC = 0.73 pre-manifest; 0.89 manifest [36] | 29.70 in pre-manifest; 37.43 in manifest [36] | Unknown in HD | D –discriminates pre-manifest vs. manifest HD [36] C –unknown R –unresponsive in 1 study [45] |
| Six-Minute Walk Test** | Recommended for assessing respiratory and walking endurance and exercise capacity across HD severity. | ICC = 0.98 premanifest; 0.94 manifest [27] | 39.2 m pre-manifest; 86.6 m manifest HD [27] | N/A | D –discriminates Stage I vs. II/III [36] C –unknown R –positive evidence 1 study [52] (moderate effect size), but unresponsive in 1 study [14] |
| The Step Test Evaluation of Performance on Steps (STEPS) | Listed for assessing stair climbing in manifest HD. | ICC = 0.89–0.91 for manifest [58] | Unknown | Unknown in HD | D –unknown C –Correlated with UHDRS-TMS (r = –0.66), Tinetti (r = 0.82), 10MWT (r = 0.60), TUG (r = –0.62), single leg stance (r = 0.59–0.61) and Stair Self Efficacy (r = 0.60) [58]. R –unknown |
| Ten-Meter Walk Test (10MWT)** | Suggested for assessing walking speed in manifest HD (most data on self-paced). | ICC = 0.96 pre-manifest; 0.95 manifest [36] | 0.23 s in pre-manifest; 0.34 manifest [36] | Unknown in HD | D –discriminates Stage I vs. II/III [36] C –No correlation with UHDRS-TMS or -TFC, and weak (r = 0.35) correlation with UHDRS-FAS [38] R –some positive evidence [33, 59, 60] (large effect size [59]); unresponsive in 1 study [61] |
| Thirty Seconds Chair Sit to Stand Test (30CST) | Suggested for assessing ability to perform transitional movement. | ICC = 0.99 [62] | 2.2 in manifest HD [49] | N/A | D –unknown C –concurrent validity with gait velocity and cadence, TUG, BBS, and PPT [62] R –positive evidence 1 study [59] |
| Timed Up and Go Test (TUG) | Recommended for assessing severity of balance and mobility and fall risk screening early to mid-stage HD. | ICC = 0.93 pre-manifest; 0.96 manifest [36] | 1.34 s in pre-manifest; 2.98 manifest [36] | <14 s predicts being a “faller” with probability of 60% [32] | D –discriminates Stage I vs. II/III [37] C –correlated with falls [37]; no correlation with UHDRS-TMS or -TFC and weakly (r = –0.33) correlated with UHDRS-FAS [38] R –positive evidence 1 study (small effect size 0.17) [46] |
| Tinetti Mobility Test (TMT) original | Recommended for assessing gait and balance in manifest HD (up to stage III) and falls screening. | TMT total ICC = 0.92 pre-manifest; 0.91 manifest HD [36] | 1 in pre-manifest; 4 in manifest [36] | <21 (74% sensitivity, 60% specificity) [63] | D –unknown C –concurrent validity with gait speed, UHDRS-FAS, -TFC, and -TMS [31, 38, 63] R –Positive results 2 studies [45, 64], but negative 1 study [34] |
| Tinetti Mobility Test (TMT) shortened version [38] | Suggested for assessing gait and balance Shortened version for HD includes items 2, 4, 5, 6, 7, 8, 9, 10, 16, 17, 18, 19, 20. | ICC = 0.89 [38] | 4 in manifest [38] | Unknown in HD | D –AUC for ROC analysis for discrimination pre-manifest or manifest with original BBS = 0.96 [38] C –unknown R –unknown |
| UHDRS-Functional Assessment Scale (FAS) | Suggested for assessing severity of limitation in functional capacity. | Unknown | Unknown | N/A | D –unknown C –concurrent validity with other parts of UHDRS [65] R –responsive in several HD pharmacological studies (see Mestre et al. [66]) |
| World Health Organization Disability Assessment Schedule (WHODAS) | Suggested to measure health and disability including domains of cognition, mobility, self-care, getting along, life activities and participation. | Test-retest reliability not available; Internal consistency reliability = 0.94 [67] | Unknown | N/A | D –Statistically significant differences between prodromal, early and late manifest HD [67] C –Moderate convergent validity with TFC and SF-36 (r = 0.41–0.76) [68] R –Detects longitudinal change better than TFC and SF-36 [69] |
AUC, area under curve; HD, Huntington’s disease; HD-ADL, Huntington’s Disease-Activities of Daily Living Questionnaire; MVPA, moderate-to-vigorous physical activity; ROC, receiver operating curve; Stage I, early stage with TFC 11–13; Stage II, middle stage with TFC 7–10; Stage III, late stage with TFC < 7; UHDRS-FAS, Unified Huntington’s Disease Rating Scale-Functional Activity Assessment; UHDRS-TFC, UHDRS-Total Functional Capacity; UHDRS-TMS, UHDRS-Total Motor Score; WHOQOL-BREF, World Health Organization-Brief Version. Bolded measures are the core assessments for persons with HD. **indicates that measure is an American Physical Therapy Association Academy of Neurologic Physical Therapy core outcome measure for assessing adults with neurologic conditions undergoing rehabilitation [12].
Fig. 1
Physical Therapy Evaluation Decision Tree. This figure presents a recommended algorithm for physical therapists to follow in their evaluation of a person with Huntington’s disease. 6MWT, Six-minute walk test; BBS, Berg Balance Scale; SF-36, Medical Outcomes Study Short-Form 36; TMT, Tinetti Mobility Test.
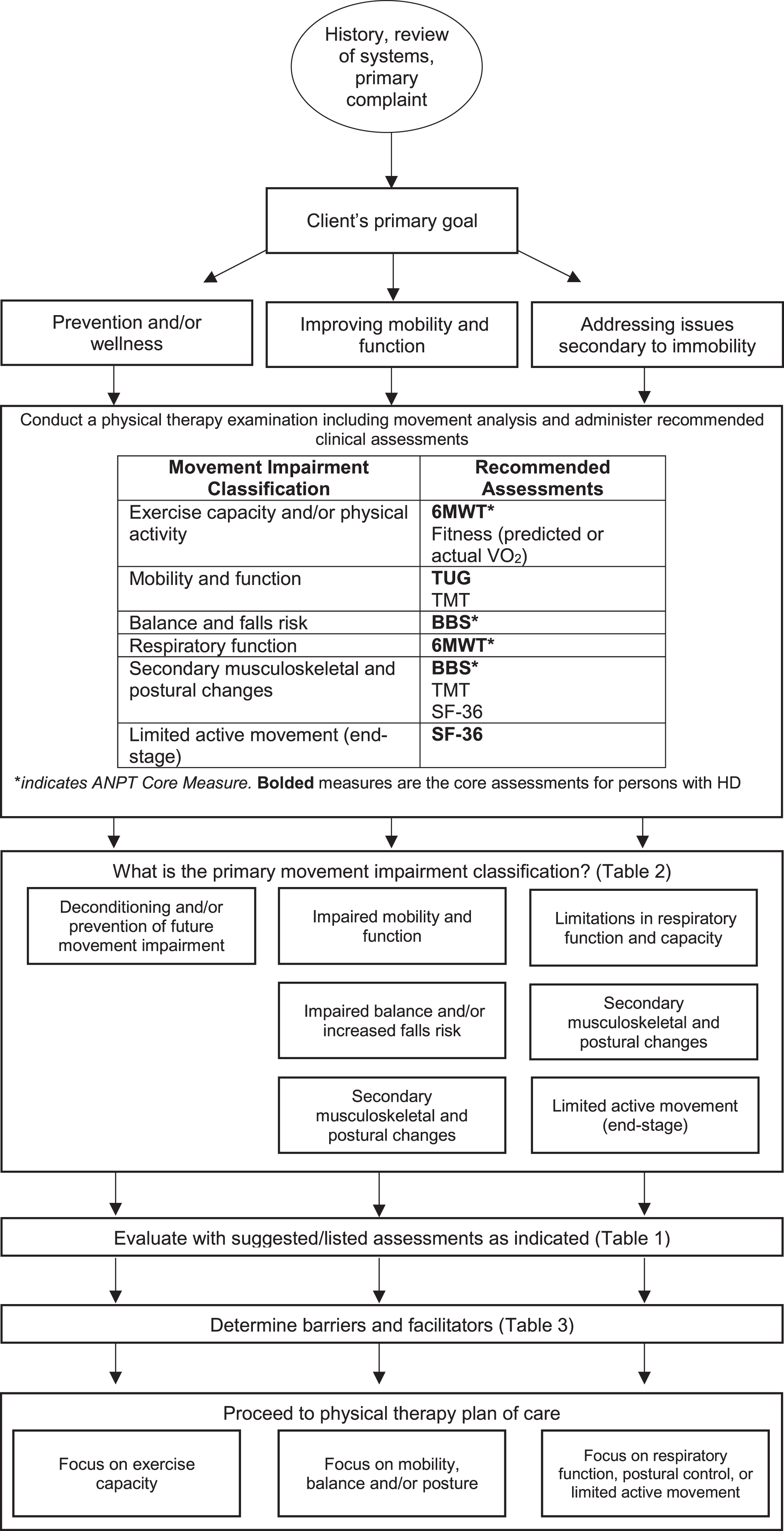
Core assessments for HD
For measurement of aerobic fitness and endurance, we selected the Six Minute Walk Test (6MWT) as a core assessment because its psychometric properties have been evaluated in HD, it is commonly administered in physical therapy practice, and it is a core measure recommended by the ANPT. However, the 6MWT measures sub-maximal aerobic capacity rather than maximal capacity and may be challenging to administer in manifest HD because of the demands of sustained attention. While cardiopulmonary exercise testing using VO2 measures is considered the gold standard for measuring aerobic capacity, we did not select it as a core assessment because it has limited psychometric data in HD, and it is difficult for persons with HD to maintain consistent lip closure on the standard mouthpiece to provide accurate measurement. Further, VO2 measurement is limited by ecological utility as the required equipment and experienced administrators are not commonly available in the clinic setting. Future work needs to examine if predicted aerobic capacity using either standard algorithms (i.e., 220-age) or algorithms adapted for HD have clinical utility. The Timed Up and Go (TUG) test was selected over the Tinetti Mobility Test (TMT) as a core assessment for measuring mobility and function because it is more commonly used and takes less time to administer than the TMT. However, the TMT may be used by physical therapists needing a more detailed assessment of balance and gait deficits than the TUG. The Berg Balance Scale (BBS) met all of the criteria to be included as a core assessment of balance and falls risk. The Medical Outcomes Study Short Form 36 (SF-36) was selected as a core assessment because it was the only patient-reported health-related quality of life measure that met the modified MDS recommended criteria. However, it is more commonly used in research than in clinical practice and the length of time to administer it makes it impractical to use in a variety of clinical settings. Physical therapists may want to consider using the WHODAS for assessing quality of life because it has excellent clinical utility in HD, is able to distinguish between manifest and prodromal HD, is more responsive to change than the SF-36, and has moderate convergent validity with the SF-36. Additional research is needed on the WHODAS to determine reliability and minimum detectable change before including it as a recommended measure. The core assessments should be part of the clinical examination of all patients with HD and those with good responsiveness can be used as outcome measures while some may be used as screening tools to differentiate between fallers and non-fallers.
GUIDELINE-BASED DECISION TREES
Physical therapy evaluation decision tree (Fig. 1)
Physical therapists should conduct a thorough examination of each person with HD, beginning with a detailed history, review of systems and primary problem(s) [13]. The next step in the flow chart is selection, administration, and interpretation of the recommended clinical assessments for HD (Fig. 1). From the subjective and objective examination findings, the therapist prioritizes the individual’s goals throughout the continuum of care, beginning with prevention and wellness at the early stages of disease, improving mobility and balance during the early-to-mid stages, and addressing issues secondary to immobility during the mid-to-advanced stages of disease. Therapists may decide to administer additional suggested/listed assessments (Table 1) to obtain more information on the person with HD’s movement deficits for treatment planning. Table 2 presents primary movement impairment classifications, and related impairments in body structure and function, activity limitations and participation restrictions for ambulatory and non-ambulatory persons, respectively. The final step in the evaluation process is to determine potential barriers and facilitators to participation in physical therapy (Table 3).
Table 2
Primary movement impairment classifications and recommended interventions for persons with HD
| Primary Movement Impairment | Participation Restrictions & Activity Limitations | Impairments in Body Structure & Function | Recommendation [7] | Specific Intervention Ideas |
| Exercise capacity and/or physical activity | No problems in premanifest and early disease stages; as disease progresses there may be difficulty sustaining activities for long durations or at high intensities due to deconditioning and fatigue. | -Absence of or limited motor impairment in functional activities; potential for cognitive and/or behavioral issues in premanifest and early stages. -Lack of motivation and/or apathy, anxiety and/or depression, and sleep disturbances may be present. | Physical therapists should prescribe aerobic exercise (moderate intensity, 55–90% heart rate maximum) paired with upper and lower body strengthening 3 times per week for a minimum of 12 weeks to improve fitness and to stabilize or improve motor function. | -Gym and home-based exercise; progressive home walking program. -Duration of aerobic exercise varied from 10–30 min (median = 25 min). -Resistance training focused on upper body, lower body and core. Specific dosing and progression information can be found in the Appendix of Quinn, 2016 [43]. -Tailor interventions according to disease stage: Early stages: focus on prevention of future movement system impairments. Later stages: focus shifts to restorative. |
| Mobility and function | -Difficulty participating in recreational sports that require balance and mobility. -Difficulty walking backwards, sideways, turning/changing direction, in open environments, or while performing a secondary cognitive task due to attentional deficits. | -Impairments in strength, balance or fatigue resulting in mobility limitations; gait impairments (e.g., decreased speed; stride length; stride width, increased variability in gait parameters). -Bradykinesia, dystonia, chorea, rigidity, and impaired motor control/force modulation may be present. | Physical therapists should prescribe one-on-one supervised gait training to improve spatiotemporal measures of gait. | -Supervised task-specific training of walking and transfers; multidisciplinary rehabilitation. -Assess need for assistive devices; rollator walkers have been shown to improve gait parameters in persons with HD. -Addition of secondary cognitive tasks to challenge dual-task performance |
| Balance and falls risk | -Fear of falling may cause unwillingness to participate in home, work, and community activities. -Difficulty participating in recreational sports that require balance and mobility. -Difficulty getting in/out of chairs and beds. | -Impairments in balance; increased falls risk. -Fatigue may lead to falls. -Balance deficits (increased sway in stance and during functional tasks of daily living, delayed responses to perturbations, difficulty with tandem standing and walking). -Bradykinesia, dystonia, chorea, rigidity and impaired motor control/force modulation may be present. | Physical therapists may prescribe individualized exercises, including balance exercises, delivered at a moderate frequency and intensity to improve balance and balance confidence. | -Task-specific training of balance; multidisciplinary rehabilitation -Transfer training; walking and balancing on compliant surfaces; reaching, stair climbing, turning. -Progressive static and dynamic standing (or sitting) balance exercises including narrowed/ altered base of support, forward/side/backward lunges, balancing with eyes open and closed, standing with/without arm support, addition of a secondary cognitive task, and perturbation training. |
| Respiratory function | -Restrictions in social activities. -Restrictions in exercise activities. -Decreased exercise tolerance; limited ability to perform activities of daily living and ambulation. | -Impaired respiratory function and capacity, limited endurance, and/or airway clearance, resulting in restrictions in functional activities and risk for infection. -Ineffective cough and dystonia of trunk muscles may also be present. | Physical therapists may provide regular breathing exercises, including inspiratory and expiratory training, to improve respiratory muscle strength and cough effectiveness. | -Inspiratory and expiratory training, with and without resistance. -Anecdotal evidence that postural and position training combined with caregiver education on breathing techniques and chest clearance techniques may be helpful. |
| Secondary musculoskeletal and postural changes | -Decreased participation in ADLs, social or work environments. -Increased caregiver burden. -Withdrawal from society. -Deconditioning and reduced endurance leading to low daily walking and physical activity levels. -Difficulty with ADLs, including washing, dressing. -Difficulty with feeding and swallowing. Inability to stand or sit independently. | -Musculoskeletal (e.g., loss of range of motion and strength due to deconditioning) and/or respiratory (e.g., endurance) changes resulting in physical deconditioning and increased fall risk. -Altered alignment in sitting or standing due to secondary adaptive changes, involuntary movements, muscle weakness, and incoordination resulting in limitations in functional activities in sitting or standing. -Weight loss may contribute to weakness and fatigue. -Pain from dystonia, muscle imbalances or immobility may also be present. | Physical therapists may prescribe an individually tailored program to improve postural control and may use positioning devices to optimize posture. | -Transfer and postural stability training tailored to disease stage: Early stages: focus on active exercises to improve core stability, muscle strengthening, fall prevention, functional exercises such as sit to stand, getting up from the floor, and posture correction. Later stages: focus on practice of bed mobility, transfer training, and getting in and out of bed. -Use of positioning devices and supports (wedge cushions, bolsters, pillows, bed railings, wheelchair safety belt) may be helpful. -Other interventions used frequently but not formally investigated include stretching for contracture management and prevention, range of motion exercise, and specific positioning to encourage feeding and swallowing. |
| Limited Active Movement (End-Stage) | -Complete dependence in functional skills; social isolation. -Unable to ambulate; dependent for most ADLs; difficulty maintaining upright sitting position. | -Active or passive range of motion limitations and poor active movement control. -Increased risk for aspiration/respiratory infection; risk for pressure sores and pain due to positioning or contractures. -Difficulty or inability to communicate may be present. | -Physical therapists should ensure that care plans for individuals with limited active movement and end-stage disease include appropriate positioning and seating, active movement, position, respiratory exercise, and education. Family and caregiver training to provide strategies for maintaining appropriate ongoing activity and participation for as long as possible is an important focus for the physical therapy team as part of end-stage care. | -Multisensory stimulation, hydrotherapy, and video-based exercise. -Late stage care in HD focuses on supporting ADLs, optimizing attention, posture, positioning, and seating, particularly during meal and post-meal times. The focus is on prevention of falls, analysis of previous falls, and development of mid-fall strategies to minimize injury risk. -Experts specifically mentioned environmental modifications and seating adaptations to maximize posture and positioning. -Additional treatments used frequently but not formally investigated include prevention of decubiti and airway clearance. |
ADL, Activity of Daily Living; HD, Huntington’s Disease.
Table 3
Barriers and Facilitators of Exercise in Persons with HD
| Facilitators | Personal Factors External Environmental Factors Training Factors | •Self-efficacy of the participant and his/her outcome expectations. •Identification and commitment of the caregiver/contact person. •Good accessibility to resources and/or equipment. •Individualized plans and schedules •Intensive training •Being part of a group •External cues provided by a therapist/caregiver or an exercise DVD. |
| Barriers | Personal Factors External Environmental Factors | •Cognitive impairment •Physical factors (poor balance) •Lack of motivation •Lack of social support •Lack of accessibility to resources and/or equipment. |
Physical therapy plan of care decision tree (Fig. 2)
The plan of care should be derived directly from the therapist’s evaluation and the individual’s goals. Using the decision tree, the therapist determines the primary focus of the plan of care, which we have divided into three areas according to the therapist’s prioritization of the person with HD’s goals as described in Fig. 1 : 1) exercise capacity; 2) mobility, balance and/or posture; and/or 3) respiratory function, postural control and/or limited active movement (Fig. 2). This individualized plan of care should address specific movement system deficits that have been identified while optimizing factors that facilitate and/or remove barriers to compliance (Table 3). The plan of care is adjusted based on regular assessment of outcome measures and it considers the individual’s values and preferences. Caregivers are a crucial element of any plan of care for individuals with HD and should be involved when appropriate. Both the person with HD and caregiver should be educated regarding the importance of ongoing physical activity [14]. Therapists should consider all factors and for those not addressed by physical therapy include appropriate referral to other health care providers such as occupational, speech and respiratory therapists, social workers, nutritionists, nurses, and neuropsychologists (Fig. 2).
Fig. 2
Physical Therapy Plan of Care Decision Tree. This figure presents a recommended algorithm for physical therapists to follow in their development of a plan of care for a person with Huntington’s disease.
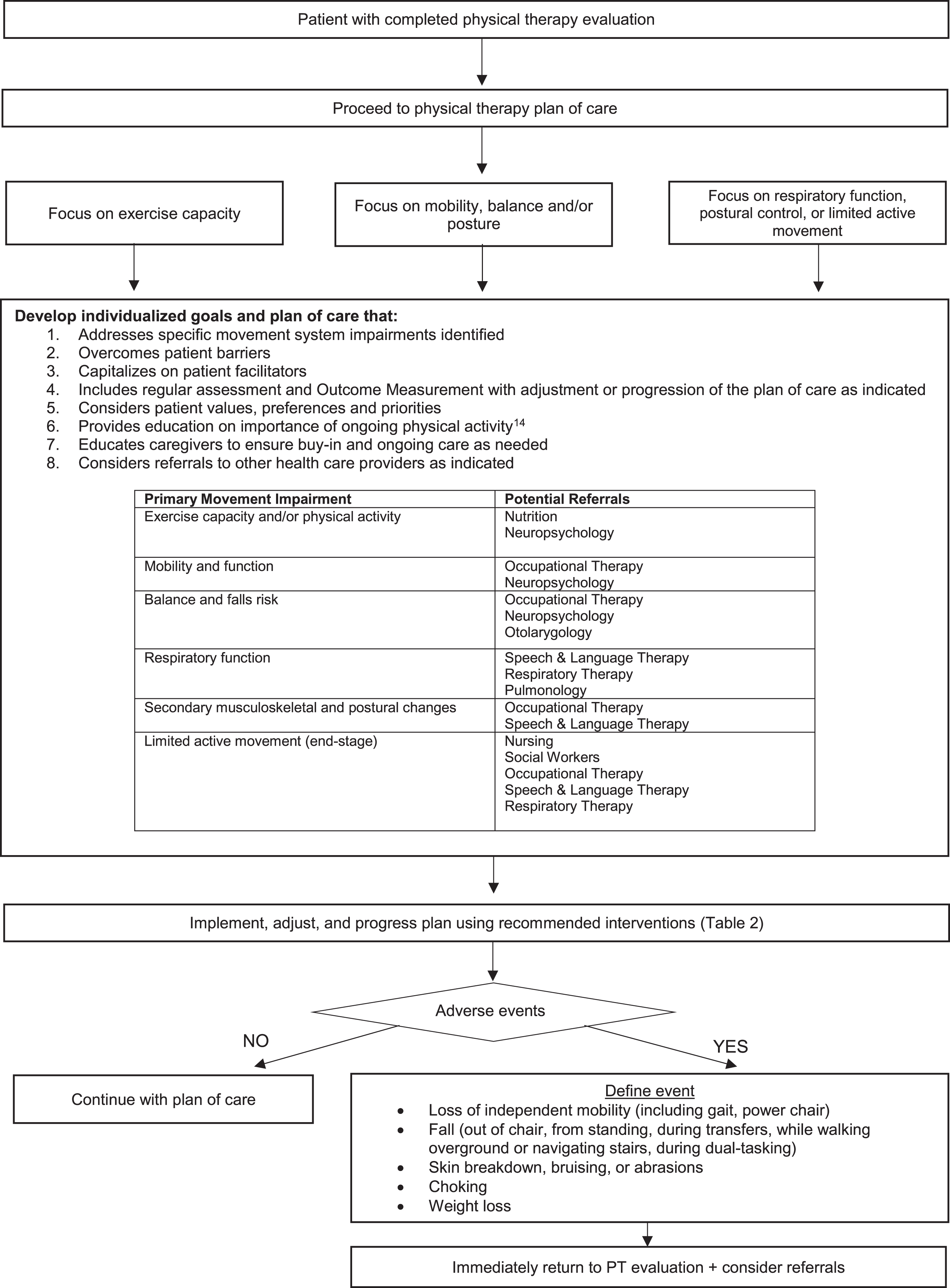
Recommended interventions based on the primary movement impairment classification that were published in a clinical practice guideline are found in Table 2 [7]. Individuals with HD who engage in regular aerobic exercise in gym and home settings can improve their fitness. One-on-one supervised mobility training is recommended to improve walking. Therapist prescription of interventions such as task specific training or exercises that challenge balance by including narrowed base of support, reliance on vision and changes in direction are proposed as beneficial interventions for individuals with balance deficits. Respiratory training and an individualized program to improve postural control may be prescribed for individuals with respiratory and postural changes [7]. End-stage care for individuals with HD may include provision of positioning devices and encouragement of individuals with HD to remain active based on their abilities. Caregiver education and involvement are crucial during later stages of the disease. Throughout the plan of care therapists should monitor for adverse events and declines in condition that could result in a loss of independence and/or medical emergencies (Fig. 2). Appropriate referrals to health care professionals should be made.
APPLICATION OF THE DECISION TREES TO PATIENT EXAMPLES
To better illustrate the use of these algorithms (Figs. 1 and 2), we provide example patients (Table 4). As seen in this table, the decision trees allow therapists to adapt and individualize assessment and plan of intervention for persons at early, middle, and late stages of the disease.
Table 4
Application of decision trees to patient examples
| Patient 1 –Early Stage HD | Patient 2 –Middle Stage HD | Patient 3 –Late Stage HD | |
| History/ Review of Systems/ Primary complaint and goals for therapy | •A 32-year-old female diagnosed with HD six months ago being seen by physical therapist at a HD Center of Excellence 100 miles from her home. She is a homemaker and lives with her husband in a double wide trailer in a small rural town with their two children ages 3 and 1. •Her recent UHDRS total motor score is 15 (some chorea, slowness of eye movements, finger taps and pronation/supination) and her TFC score is 12 (Stage I). Symbol digit modalities testing is mildly impaired. •She reports that she is presently able to do all household tasks and take care of her children. However, she reports some difficulty with cutting with scissors and buttoning clothes and feeling more tired at the end of the day. She states that she needs to be able to continue to take care of her children as there are no family members nearby to help her and they cannot afford childcare. She worries that she won’t be able to lift and carry her children and get on and off the floor in the future, and wants to know what exercises she can do to maintain her current functional abilities. | •A divorced 45-year-old male diagnosed with HD 5 years ago who comes to an outpatient PT clinic with his 16-year-old daughter. He lives alone in a two-story townhouse with the bedroom upstairs. •His recent UHDRS total motor score is 45 (issues across the board) and his TFC score is 5 (Stage III). Symbol digit modalities testing is moderately impaired. •He complains that his balance and walking are getting worse, and that he lost his job as a salesperson at Walmart because he was having difficulty keeping his balance while standing or walking and talking to customers. When asked what he does during the day he states that he mostly watches the television or sleeps until his daughter comes over after school to visit him and help with domestic chores and ADLs. He is falling 1-2 times per week when walking and recently fell due to a misstep on the stairs going down, hurting his back. He states that he is only coming to therapy so that his family doesn’t put him in a nursing home. | •A 70-year-old female diagnosed with HD 10 years ago who is referred by primary physician for home physical therapy. She lives in a ranch home with her husband. •Her recent UHDRS total motor score is 70 and her TFC score is 2 (Stage IV). Symbol digit modalities testing is severely impaired. •She sits with a forward flexed and posterior pelvic tilt posture on the couch and tends to fall backwards when she attempts to stand. Her husband states that he stands in front of her and pulls her to standing using her arms. Due to her severe chorea she is no longer able to use her rollator walker and walks short distances hand in hand or holding on to furniture or to the wall. Her gait is wide-based and slow with short and variable step lengths and frequent pauses or hesitations. She exhibits shortness of breath and fatigues quickly with exertion. Her husband states that she has fallen when getting out of bed to go to the bathroom at night. He states that he is having a difficult time caring for her 24/7 a day. The only time that she goes outside the home is to go to her doctor appointments. |
| Physical Therapy Examination Findings | Recommended Core Assessments: •Six minute walk test: 450 feet •Timed Up and Go test: 7.20 s •Berg Balance Scale: 55/56 (single leg stance = 8 s) •SF-36: Physical Score 55.84, Mental Score 53.14 | Recommended Core Assessments: •Six minute walk test: 550 feet •Timed Up and Go test: 15.40 s (high fall risk) •Berg Balance Scale: 40/56 (high fall risk) •SF-36: Physical score 36.00, Mental score 33.80 | Recommended Core Assessments: •Two minute walk test (cannot do 6 minute walk test): 70 feet •Timed Up and Go test: 28.51 s (high fall risk) •Berg Balance Scale: 16/56 •SF-36: Physical Score 21.13, Mental Score 19.54 |
| Primary Movement Impairment Classification | •Deconditioning and/or prevention of future movement impairment; physical capacity and/or physical activity movement impairment classification. | •Impairments in balance and increased falls risk; balance and falls risk movement impairment classification. | •Impaired respiratory function and capacity and limited endurance; respiratory function movement impairment classification. •Limited active movement; end stage movement impairment classification. |
| Additional Suggested/ Listed Assessments | •Dynamic Gait Index: 23/24 (2/3 on stepping over obstacle) •5 Times Sit-To-Stand: 7 s | •Dynamic Gait Index: 17/24 •Activities-Specific Balance Confidence Scale: 55% •5 Times Sit-To-Stand: 16 s | •5 Times Sit-To-Stand: 60 s with arm use |
| Additional Movement-Based Impairments | •Difficulty with high-level balance; mobility and function movement impairment classification. | •Difficulty with walking while doing a secondary cognitive or motor task; mobility and function movement impairment classification. | •Loss of strength and deconditioning leading to postural alterations, decreased walking and increased fall risk; secondary musculoskeletal and postural changes movement impairment classification. |
| Barriers and Facilitators of exercise | Barriers: •Lack of time to exercise due to family responsibilities. •Lack of exercise equipment in home and unable to pay for gym membership. Facilitators: •High motivation to exercise. •Husband is supportive. | Barriers: •Cognitive impairment, likely contributing to dual task deficits. •Lack of motivation to exercise. Facilitators: •Daughter committed to helping father get to PT and to follow exercise program. | Barriers: •Severe cognitive impairment •Poor balance, mobility and endurance •Husband may be experiencing caregiver burnout Facilitators: •Social support and accessibility to resources and equipment through local HD support group. |
| Summary of Physical Therapy Evaluation | She has decreased endurance and mild balance and gait impairments; low fall risk. She is having mild chorea, fine motor incoordination, and higher-level balance problems. | His balance and gait are impaired and he is has had multiple falls; high fall risk. He is not able to work, and needs assistance for ADLs, domestic chores, and finances. | She requires assistance to stand and walk. She is mostly dependent for her ADLs. |
| Plan of Care | •Progressive walking program at a brisk pace for cardiovascular health and increased endurance at nearby high school track or park with friend 2-3 times per week up to 30 min in evenings and weekends when husband is home. Alternatively, she could use an exercise DVD in home while her children are taking naps. •To increase daily walking, she is advised to park further from the door of the stores where she shops, and to walk rather than drive to visit a friend who lives in her neighborhood. Strengthening exercises using theraband to prevent muscle weakness on days that she doesn’t walk. •Single leg stance 10 reps 3 times per day to improve balance. She is advised to incorporate the exercises into her daily life such as when she is standing beside a sink washing dishes or brushing her teeth or beside a table after finishing a meal. •Referral to occupational therapy for hand dexterity training. | •Progressive balance training including dual task exercises to improve balance and prevent falls. •Task-specific practice of functional activities (i.e., dual task walking and stair climbing) that are problematic for him to train balance control during ADLs. •Environmental modifications: removal of clutter, glass tops, and sharp edges on furniture. •Fall prevention interventions such as teaching to: “STOP-THINK-HOLD HANDRAIL” on stairs, and holding on to shopping cart at stores. •If needed, train in use of rollator walker to ambulate safely, especially in unfamiliar or crowded places. •Referral to neuropsychologist for cognitive and behavioral testing. | •Daily walking program (3-4 times per day for 5-10 min) when assistance can be given. •Optimize sitting position via tilt-in-space customized wheelchair or Broda chair. •Perform daily breathing exercises using incentive spirometer. •Teach husband to cue her to slide her hands down her thighs to her knees and bend at the hips to get her center of mass forward before standing up. •Train husband in use of a gait belt to assist with transfers and gait. •Bedside commode for toileting at night. •Participation in as many household chores (folding laundry, arts and crafts) and activities (e.g., socializing with HD support group and church members) as possible. •Referral to social worker for care assistance for husband. |
ADL, Activity of Daily Living, TFC, Total Functional Capacity; HD, Huntington’s Disease; UHDRS, United Huntington’s Disease Rating Scale.
SPECIAL CONSIDERATIONS IN THE PHYSICAL THERAPY MANAGEMENT OF PERSONS WITH HD
HD is a complex disease with most individuals presenting with a triad of cognitive, motor, and behavioral impairments that impact functional abilities. Cognitive dysfunction, in particular, can be a barrier to evaluation of the person with HD and implementation of the plan of care. Cognitive dysfunction may also manifest as mobility impairment [15, 16] or difficulty performing tasks requiring simultaneous motor and cognitive function [17, 18], thus impacting the ability to perform daily life tasks. In early HD, individuals may exhibit subtle problems with memory, thinking, and planning activities [19]. Thus, therapists may wish to include an assessment of dual-task [17, 20–26] in addition to the core set of recommended outcomes (Fig. 1) to monitor dual-task performance over time; our recent work suggests that the TUG Cognitive may be a sensitive measure of dual-task walking in HD [20]. Providing clear instructions and written materials and including the caregiver and/or family in education can help to overcome this barrier throughout the disease course. Considering the learning style of the person with HD may also be helpful; providing videos may allow for greater adherence in some persons with HD compared to photos of the exercises alone. Another strategy may be to introduce only a few exercises at once, allowing the person to become independent with these before adding additional home exercises. To ensure understanding, the therapist should ask the person with HD to demonstrate the exercise and repeat instructions to ensure safety.
Apathy or lack of motivation can also significantly impact engagement in exercise and affect outcomes [27]. A frank discussion with individuals with HD about activities they enjoy will allow the therapist to tailor the rehabilitation program to the individual’s interests, capitalize on salience and maintain sufficient intensity in the program. Apathy is common among persons with HD and related to quality of life and physical function [28]. The therapist should educate care partners on the importance of routine exercise (i.e., at the same time each day), keeping a log of their daily activity to see progress, and having a supportive exercise partner. Studies in persons with HD have demonstrated that a supportive caregiver can be the difference between success and failure with an exercise program [29]. The therapist should also stress the importance of frequent in-person check-ins to update the wellness plan and monitor function.
IMPLEMENTATION OF THE GUIDELINES
Clinical practice guidelines encourage the use of evidence-based practice and reduce variation in treatment. In a rare disease like HD, such guidelines can be particularly useful, as clinicians are unlikely to encounter persons with HD on a regular basis. To assist physical therapists to implement the guidelines, we propose strategies to address potential barriers, as well as facilitators, to implementation.
Strategies to overcome barriers to implementation
Physical therapists who plan to work with individuals with HD should seek specialized knowledge and training to be able to manage the unique symptoms and impairments of HD. Accessing freely available resources available from the Academy of Neurologic Physical Therapy (https://www.neuropt.org) Synapse Education Center (https://www.anptsynpasecenter.com) can facilitate the knowledge translation of the clinical recommendations [7].
Due to the complexity of the disease, time and resources needed to examine, evaluate, and treat people with HD may be more than with other neurodegenerative diseases. For example, it may be helpful to have a quiet space where therapy can be performed if the individual is easily distractible or becomes agitated. Care provided by physical therapists in the home is an environment that frequently works well for individuals with HD due to issues with transportation. Recommendations for home health therapists are to have a heart rate monitor and/or pulse oximeter available along with a gait belt and balance equipment such as a thick foam pad.
Finally, as mentioned earlier, caregiver support is critically important for the success of the person with HD undergoing rehabilitation. Physical therapists are encouraged to engage the caregiver in education early and often, including strategies on how to help people with HD stay active and adhere to physical therapy exercise recommendations. Specific education on the importance of exercise throughout the disease course is warranted. Caregivers may also benefit from resources available from the European Huntington’s Association (https://eurohuntington.org/active-huntingtons/).
Facilitators to implementation
Ideally, individuals with HD should receive care at a multidisciplinary clinic or within a health care provider network consisting of providers specially trained in HD who can work together to help manage patients with HD. However, clinical pathways that support patient early referral and treatment flows congruent with the decision trees in this paper can facilitate direct integration of patients with HD into local practice settings. This, in turn, will facilitate the use of evidence-based treatments in the management of persons with HD.
A critical step in the knowledge translation process is the wide-spread implementation of guidelines into clinical practice. In the context of models of implementation science,30 future research should develop knowledge translation tools that facilitate the adoption of these guidelines across settings and across the disability spectrum, to meet the needs of persons with HD. Within the translation phase of the implementation science model, a clear plan for dissemination is needed for individuals and organizations to use the information to improve the health of persons with HD. Importantly, adoption of knowledge translation by institutions requires training, financial resources and improving organizational capacity. To aid in implementation the European Huntington’s Disease Network Physiotherapy Working Group has made the CPG available in both lay language formats and in multiple languages (https://www.ehdn.org/de/clinical-guidelines/).
Additional research is needed to advance evidence-based practice for persons with HD. Our review of clinical assessments in HD revealed very few measures specifically developed for persons with HD; future work should not only determine psychometric properties of existing measures within the HD population, but also work to develop HD-specific assessments. Research to determine optimal clinical assessments for use with persons with HD through a Delphi process may be particularly useful. Large-scale collaborative trials are needed to systematically quantify outcomes through comparative effectiveness research to determine the best physical therapy interventions for persons with HD at each disease stage and within each movement impairment classification.
CONCLUSION
In summary, this work adds to the current literature by establishing a core set of clinical assessments for persons with HD and providing evidence-based decision trees to aid in the implementation of a physical therapy plan of care for individuals with HD. Our algorithms overcome limitations of prior approaches by spanning disease stages and guiding decision making based on the individual’s primary movement impairment classification. The tools developed by this study (decision trees and core set of measures) are immediately scalable and can be easily implemented by physical therapists into clinical practice to improve rehabilitation for persons with HD.
CONFLICT OF INTEREST
The authors declare that there is no conflict of interest.
REFERENCES
[1] | Ghosh R , Tabrizi SJ . Huntington disease. Handb Clin Neurol. (2018) ;147: :255–78. doi: 10.1016/B978-0-444-63233-3.00017-8. |
[2] | Yohrling G , Raimundo K , Crowell V , Lovecky D , Vetter L , Seeberger L . Prevalence of Huntington’s disease in the US (954). Neurology. (2020) ;94: (15 Supplement). https://n.neurology.org/content/94/15_Supplement/954. |
[3] | National Organization for Rare Disorders. Rare Disease Information. Huntington’s Disease. Accessed August 30, 2021. https://rarediseases.org/rare-diseases/huntingtons-disease/. |
[4] | Quinn L , Morgan D . From disease to health: Physical therapy health promotion practices for secondary prevention in adult and pediatric neurologic populations. J Neurol Phys Ther. (2017) ;41: (Suppl 3 IV STEP Spec Iss):S46–S54. doi: 10.1097/NPT.0000000000000166. |
[5] | Busse ME , Khalil H , Quinn L , Rosser AE . Physical therapy intervention for people with Huntington disease. Phys Ther. (2008) ;88: (7). doi: 10.2522/ptj.20070346. |
[6] | Fritz NE , Rao AK , Kegelmeyer D , Kloos A , Busse M , Hartel L , et al. Physical therapy and exercise interventions in Huntington’s disease: A mixed methods systematic review. J Huntingtons Dis. (2017) ;6: (3). doi: 10.3233/JHD-170260. |
[7] | Quinn L , Kegelmeyer D , Kloos A , Rao AK , Busse M , Fritz NE . Clinicalrecommendations to guide physical therapy practice for Huntingtondisease. Neurology. (2020) ;94: (5):217–28. doi: 10.1212/WNL.0000000000008887. |
[8] | Quatman-Yates CC , Hunter-Giordano A , Shimamura KK , Landel R , Alsalaheen BA , Hanke TA , et al. Physical therapy evaluation and treatment after concussion/mild traumatic brain injury. J Orthop Sports Phys Ther. (2020) ;50: (4):CPG1–CPG73. doi: 10.2519/jospt.2020.0301. |
[9] | Jette AM . Toward a common language for function, disability, and health. Phys Ther. (2006) ;86: (5):726–34. doi: 10.1093/ptj/86.5.726. |
[10] | World Health Organization. International Classification of Functioning, Disability and Health Classifications. Accessed August 30, 2022. https://apps.who.int/classifications/icfbrowser/. |
[11] | Schrag A , Barone P , Brown RG , Leentjens AF , McDonald WM , Starkstein S , et al. Depression rating scales in Parkinson’s disease: Critique and recommendations. Mov Disord. (2007) ;22: (8):1077–92. doi: 10.1002/mds.21333. |
[12] | Moore JL , Potter K , Blankshain K , Kaplan SL , O’Dwyer LC , Sullivan JE . A core set of outcome measures for adults with neurologicconditions undergoing rehabilitation: A clinical practice guideline. J Neurol Phys Ther. (2018) ;42: (3):174–220. doi: 10.1097/NPT.0000000000000229. |
[13] | American Physical Therapy Association. Guide to Physical Therapist Practice.; 2016.. |
[14] | Busse M , Quinn L , Drew C , Kelson M , Trubey R , McEwan K , et al. Physical activity self-management and coaching compared to social interaction in Huntington disease: Results from the ENGAGE-HD randomized, controlled pilot feasibility trial. Phys Ther. (2017) ;97: (6):625–39. doi: 10.1093/ptj/pzx031. |
[15] | Kloos AD , Kegelmeyer DA , Fritz NE , Daley AM , Young GS , Kostyk SK . Cognitive dysfunction contributes to mobility impairments in Huntington’s disease. J Huntingtons Dis. (2017) ;6: (4):363–70. doi: 10.3233/JHD-170279. |
[16] | Cruickshank T , Reyes A , Peñailillo L , Thompson J , Ziman M . Factors that contribute to balance and mobility impairments in individuals with Huntington’s disease. Basal Ganglia. (2014) ;4: (2), 67–70. |
[17] | Fritz NE , Hamana K , Kelson M , Rosser A , Busse M , Quinn L . Motor-cognitive dual-task deficits in individuals with early-mid stage Huntington disease. Gait Posture. (2016) ;49: . doi: 10.1016/j.gaitpost.2016.07.014. |
[18] | McIsaac TL , Fritz NE , Quinn L , Muratori LM . Cognitive-motor interference in neurodegenerative disease: A narrative review and implications for clinical management. Front Psychol. (2018) ;9: :2061. doi: 10.3389/fpsyg.2018.02061. |
[19] | Ho AK , Sahakian BJ , Brown RG , Barker RA , Hodges JR , Ané MN , et al. Profile of cognitive progression in early Huntington’s disease. Neurology. (2003) ;61: (12), 1702–6. |
[20] | Muratori LM , Quinn L , Li X , Youdan G , Busse M , Fritz NE . Measures of postural control and mobility during dual-tasking as candidate markers of instability in Huntington’s disease. Hum Mov Sci. (2021) ;80: :1028–81. doi: 10.1016/j.humov.2021.102881. Epub 2021 Sep 25. PMID: 34583142. |
[21] | Purcell NL , Goldman JG , Ouyang B , Liu Y , Bernard B , O’Keefe JA . The effects of dual-task cognitive interference on gait and turning in Huntington’s disease. PLoS One. (2020) ;15: (1), e0226827. |
[22] | Lo J , Reyes A , Pulverenti TS , Rankin TJ , Bartlett DM , Zaenker P , et al. Dual tasking impairments are associated with striatal pathology in Huntington’s disease. Ann Clin Transl Neurol. (2020) ;7: (9):1608–19. doi: 10.1002/acn3.51142. |
[23] | Reyes A , Bartlett DM , Rankin TJ , Zaenker P , Turner K , Teo WP , et al. Clinical determinants of dual tasking in people with premanifest Huntington disease. Phys Ther. (2021) ;101: (4):pzab016. doi: 10.1093/ptj/pzab016. |
[24] | Purcell NL , Goldman JG , Ouyang B , Bernard B , O’Keefe JA . The effects of dual-task cognitive interference and environmental challenges on balance in Huntington’s disease. Mov Disord Clin Pract. (2019) ;6: (3):202–12. doi: 10.1002/mdc3.12720. |
[25] | Reyes A , Rankin T , Pulverenti TS , Bartlett D , Georgiou-Karistianis N , Lampit A , et al. The effect of multidisciplinary therapy on dualtask performance in preclinical Huntington’s disease: An exploratorystudy. Ann Phys Rehabil Med. (2021) ;64: (4):1014–21. doi: 10.1016/j.rehab.2020.06.006. |
[26] | de Tommaso M , Ricci K , Montemurno A , Vecchio E , Invitto S . Walking-related dual-task interference in early-to-middle-stage Huntington’s disease: An auditory event related potential study. Front Psychol. (2017) ;8: :1292. doi: 10.3389/fpsyg.2017.01292. |
[27] | Teixeira ALJ , Caramelli P . Apathy in Alzheimer’s disease. Rev Bras Psiquiatr. (2006) ;28: (3), 238–41. |
[28] | Fritz NE , Boileau NR , Stout JC , Ready R , Perlmutter JS , Paulsen JS , et al. Relationships among apathy, health-related quality of life, and function in Huntington’s disease. J Neuropsychiatry Clin Neurosci. (2018) ;30: (3):194–201. doi: 10.1176/appi.neuropsych.17080173. |
[29] | Khalil H . An exploratory study of mobility-related outcome measures and an exercise intervention in people with Huntington’s disease (HD). PhD thesis, Cardiff University. Published online 2012. https://orca.cardiff.ac.uk/33705/. |
[30] | Centers for Disease Control and Prevention. Applying the knowledge to action (K2A) framework: Questions to guide planning. Atlanta, GA. Centers for Disease Control and Prevention, US Dept of Health and Human Services. |
[31] | Kloos AD , Fritz NE , Kostyk SK , Young GS , Kegelmeyer DA . Clinimetric properties of the Tinetti Mobility Test, Four Square Step Test, Activities-specific Balance Confidence Scale, and spatiotemporal gait measures in individuals with Huntington’s disease. Gait Posture. (2014) ;40: (4):647–51. doi: 10.1016/j.gaitpost.2014.07.018. |
[32] | Busse ME , Wiles CM , Rosser AE . Mobility and falls in people with Huntington’s disease. J Neurol Neurosurg Psychiatry. (2009) ;80: (1):88–90. doi: 10.1136/jnn2008.147793. |
[33] | Thompson JA , Cruickshank TM , Penailillo LE , Lee JW , Newton RU , Barker RA , et al. The effects of multidisciplinary rehabilitation in patients with early-to-middle-stage Huntington’s disease: A pilot study. Eur J Neurol. (2013) ;20: (9):1325–9. doi: 10.1111/ene.12053. |
[34] | Kloos AD , Fritz NE , Kostyk SK , Young GS , Kegelmeyer DA . Video game play (Dance Dance Revolution) as a potential exercise therapy in Huntington’s disease: A controlled clinical trial. Clin Rehabil. (2013) ;27: (11):972–82. doi: 10.1177/0269215513487235. |
[35] | Piira A , van Walsem MR , Mikalsen G , Nilsen KH , Knutsen S , Frich JC . Effects of a one year intensive multidisciplinary rehabilitationprogram for patients with Huntington’s disease: A prospectiveintervention study. PLoS Curr. (2013) ;5: . doi: 10.1371/currents.hd.9504af71e0d1f87830c25c394be47027. |
[36] | Quinn L , Khalil H , Dawes H , Fritz NE , Kegelmeyer D , Kloos AD , et al. Reliability and minimal detectable change of physical performance measures in individuals with pre-manifest and manifest Huntington disease. Phys Ther. (2013) ;93: (7):942–56. doi: 10.2522/ptj.20130032. |
[37] | Rao AK , Muratori L , Louis ED , Moskowitz CB , Marder KS . Clinical measurement of mobility and balance impairments in Huntington’s disease: Validity and responsiveness. Gait Posture. (2009) ;29: (3):433–6. doi: 10.1016/j.gaitpost.2008.11.002. |
[38] | Busse M , Quinn L , Khalil H , McEwan K . Optimising mobility outcome measures in Huntington’s disease. J Huntingtons Dis. (2014) ;3: (2):175–88. doi: 10.3233/jhd-140091. |
[39] | Fekete R , Davidson A , Jankovic J . Clinical assessment of the effectof tetrabenazine on functional scales in huntington disease: A pilotopen label study. Tremor Other Hyperkinet Mov (N Y). (2012) ;2: :tre-02-86-476-4. doi: 10.7916/D8DN43SC. |
[40] | Storer TW , Davis JA , Caiozzo VJ . Accurate prediction of VO2max in cycle ergometry. Med Sci Sports Exerc. (1990) ;22: (5), 704–12. |
[41] | Katzel LI , Sorkin JD , Macko RF , Smith B , Ivey FM , Shulman LM . Repeatability of aerobic capacity measurements in Parkinson disease. Med Sci Sports Exerc. (2011) ;43: (12):2381–7. doi: 10.1249/MSS.0b013e31822432d4. |
[42] | Steventon JJ , Collett J , Furby H , Hamana K , Foster C , O’Callaghan P , et al. Alterations in the metabolic and cardiorespiratory response to exercise in Huntington’s disease. Parkinsonism Relat Disord. 2018;(January):0-1. |
[43] | Quinn L , Hamana K , Kelson M , Dawes H , Collett J , Townson J , et al. A randomized, controlled trial of a multi-modal exercise intervention in Huntington’s disease. Parkinsomism Relat Disord. (2016) ;31: :46–52. doi: http://dx.doi.org/10.1016/j.parkreldis.2016.06.023. |
[44] | Frese S , Petersen JA , Ligon-Auer M , Mueller SM , Mihaylova V , Gehrig SM , et al. Exercise effects in Huntington disease. J Neurol. (2017) ;264: (1):32–9. doi: 10.1007/s00415-016-8310-1. |
[45] | Kegelmeyer DA , Kloos AD , Fritz NE , Fiumedora MM , White SE , Kostyk SK . Impact of tetrabenazine on gait and functional mobility in individuals with Huntington’s disease. J Neurol Sci. (2014) ;347: (1-2):219–23. doi: 10.1016/j.jns.2014.09.053. |
[46] | Quinn L , Debono K , Dawes H , Rosser AE , Nemeth AH , Rickards H , et al. Task-specific training in Huntington disease: A randomized controlled feasibility trial. Phys Ther. (2014) ;94: (11):1555–68. doi: 10.2522/ptj.20140123. |
[47] | Carlozzi NE , Boileau NR , Paulsen JS , Perlmutter JS , Lai JS , Hahn EA , et al. End-of-life measures in Huntington disease: HDQLIFE meaning and purpose, concern with death and dying, and end of life planning. J Neurol. (2019) ;266: (10):2406–22. doi: 10.1007/s00415-019-09417-7. |
[48] | Hocaoglu MB , Gaffan EA , Ho AK . The Huntington’s Disease health-related Quality of Life questionnaire (HDQoL): A disease-specific measure of health-related quality of life. Clin Genet. (2012) ;81: (2):117–22. doi: 10.1111/j.1399-0004.2011.01823.x. |
[49] | Aubeeluck A , Buchanan H . The Huntington’s disease quality of life battery for carers: Reliability and validity. Clin Genet. (2007) ;71: (5):434–45. doi: 10.1111/j.1399-0004.2007.00784.x. |
[50] | Wallace M , Downing N , Lourens S , Mills J , Kim JI , Long J , et al. Isthere an association of physical activity with brain volume,behavior, and day-to-day functioning? A cross sectional design inprodromal and early Huntington disease. PLoS Curr. (2016) ;8: . doi: 10.1371/currents.hd.cba6ea74972cf8412a73ce52eb018c1e. |
[51] | Ho AK , Robbins AOG , Walters SJ , Kaptoge S , Sahakian BJ , Barker RA . Health-related quality of life in Huntington’s disease: A comparison of two generic instruments, SF-36 and SIP. Mov Disord. (2004) ;19: (11):1341–8. doi: 10.1002/mds.20208. |
[52] | Mestre TA , Carlozzi NE , Ho AK , Burgunder JM , Walker F , Davis AM , et al. Quality of life in Huntington’s disease: Critique and recommendations for measures assessing patient health-related quality of life and caregiver quality of life. Mov Disord. (2018) ;33: (5):742–9. doi: 10.1002/mds.27317. |
[53] | Jacobs JV , Boyd JT , Hogarth P , Horak FB . Domains and correlates ofclinical balance impairment associated withHuntington’s disease. Gait Posture. (2015) ;43: (3):867–70. doi: 10.1016/j.gaitpost.2015.02.018. |
[54] | Keren K , Busse M , Fritz NE , Muratori LM , Gazit E , Hillel I , et al. Quantification of daily-living gait quantity and quality using a wrist-worn accelerometer in Huntington’s disease. 42. (2021) ;12: :7194. doi: 10.3389/fneur.2021.719442. |
[55] | Beckmann H , Bohlen S , Saft C , Hoffmann R , Gerss J , Muratori L , et al. Objective assessment of gait and posture in premanifest and manifest Huntington disease - A multi-center study. Gait Posture. (2018) ;62: :451–7. doi: 10.1016/j.gaitpost.2018.03.039. |
[56] | Porciuncula F , Wasserman P , Marder KS , Rao AK . Quantifying postural control in premanifest and manifest Huntington disease using wearable sensors. Neurorehabil Neural Repair. (2020) ;34: (9):771–83. doi: 10.1177/1545968320939560. |
[57] | Bartlett DM , Govus A , Rankin T , Lampit A , Feindel K , Poudel G , et al. The effects of multidisciplinary rehabilitation on neuroimaging, biological, cognitive and motor outcomes in individuals with premanifest Huntington’s disease. J Neurol Sci. (2020) ;416: :117022. doi: 10.1016/j.jns.2020.117022. |
[58] | Kloos AD , Kegelmeyer DA , Ambrogi K , Kline D , McCormack-Mager M , Schroeder B , et al. The Step Test Evaluation of Performance on Stairs (STEPS): Validation and reliability in a neurological disorder. PLoS One. (2019) ;14: (3):e6980213. doi: 10.1371/journal.pone.0213698. |
[59] | Khalil H , Quinn L , van Deursen R , Dawes H , Playle R , Rosser A , et al. What effect does a structured home-based exercise programme have on people with Huntington’s disease? A randomized, controlled pilot study. Clin Rehabil. (2013) ;27: (7):646–58. doi: 10.1177/0269215512473762. |
[60] | Mirek E , Filip M , Banaszkiewicz K , Rudzińska M , Szymura J , Pasiut S , et al. The effects of physiotherapy with PNF concept ongait and balance of patients with Huntington’s disease - pilotstudy. Neurol Neurochir Pol. (2015) ;49: (6):354–7. doi: 10.1016/j.pjnns.2015.09.002. |
[61] | Busse M , Quinn L , Debono K , Jones K , Collett J , Playle R , et al. A randomized feasibility study of a 12-week community-based exercise program in people with Huntington’s disease. J Neurol Phys Ther. (2013) ;37: (4):149–58. doi: 10.1097/NPT.0000000000000016. |
[62] | Khalil H , van Deursen R , Quinn L , Rosser A , Busse M . Clinical measurement of sit to stand performance in people with Huntington’s disease: Reliability and validity for the 30 second chair sit to stand test. J Neurol Neurosur Psychiatry. (2010) ;81: , A28. |
[63] | Kloos AD , Kegelmeyer DA , Young GS , Kostyk SK . Falls risk assessment using the Tinetti mobility in individuals with Huntington’s disease. Mov Disord. (2010) ;25: (16):2838–44. doi: 10.1002/mds.23421. |
[64] | Zinzi P , Salmaso D , De Grandis R , Graziani G , Maceroni S , Bentivoglio A , et al. Effects of an intensive rehabilitation programme on patients with Huntington’s disease: A pilot study. Clin Rehabil. (2007) ;21: (7), 603–13. |
[65] | Group HS . Unified Huntington’s Disease Rating Scale: Reliability andconsistency. Mov Disord.. (1996) ;11: (2), 136–42. |
[66] | Mestre TA , Busse M , Davis AM , Quinn L , Rodrigues FB , Burgunder JM , et al. Rating scales and performance-based measures for assessmentof functional ability in Huntington’s disease: Critique andrecommendations. Mov Disord Clin Pract. (2018) ;0: (December 2017), 1–12. doi: 10.1002/mdc3.12617. |
[67] | Carlozzi NE , Kratz AL , Downing NR , Goodnight S , Miner JA , Migliore N , et al. Validity of the 12-item World Health Organization Disability Assessment Schedule 2. 0 (WHODAS 2.0) in individuals with Huntington disease (HD). Qual Life Res. (2015) ;24: (8):1963–71. doi: 10.1007/s11136-015-0930-x. |
[68] | Downing NR , Kim JI , Williams JK , Long JD , Mills JA , Paulsen JS , et al. WHODAS 2. 0 in prodromal Huntington disease:Measures of functioning in neuropsychiatric disease. Eur J HumGenet. (2014) ;22: (8):958–63. doi: 10.1038/ejhg.2013.275. |
[69] | Kim JI , Long JD , Mills JA , Downing N , Williams JK , Paulsen JS , et al. Performance of the 12-item WHODAS 2. 0 in prodromal Huntington disease. Eur J Hum Genet. (2015) ;23: (11):1584–7. doi: 10.1038/ejhg.2015.11. |

