
The Ripple Effect: A Qualitative Overview of Challenges When Growing Up in Families Affected by Huntington’s Disease
Abstract
Background:
The average age for the onset of Huntington’s disease (HD) is an age when many people have children and caretaking responsibilities; HD is therefore likely to impact the whole family, including children and adolescents. Despite an increased understanding of the challenges for young people of growing up in a family affected by HD, a continuing lack of available knowledge has led to inadequate youth-focused support in many countries.
Objective:
This study explored the risks of growing up in a family affected by HD, and provided a participant-generated overview of the main challenges the participants experienced, in order to enhance awareness and promote more youth-focused support.
Methods:
As part of a larger national study, this qualitative paper included 36 semi-structured interviews with young people and adults who had previous or current experiences of growing up in families affected by HD. The interviews were analysed using thematic analysis.
Results:
The participants described challenges relating to four main domains of everyday life: family functioning, emotions and reactions, social functioning, and public and care services.
Conclusion:
This study contributes to an increased understanding of risk factors posed on young people by growing up with a parent with HD. The study highlighted challenges in several areas of life presenting a risk to the overall health and functioning of young people. We propose that this knowledge should be applied within a bioecological framework, to increase understanding and promote awareness of the possible risks posed, for young people, by HD.
INTRODUCTION
HD is a progressive neurodegenerative disease with a 50% risk of genetic transmission, with no current cure, and limited interventions available for the improvement of quality of life or symptom relief [1]. The intertwined and complex symptomatology of the disease includes a deterioration in physical, psychological, and cognitive functioning, and inevitably results in complete dependence on caregivers for affected individuals [2]. A diagnosis is made when a person presents with overt physical symptoms, but prodromal symptoms that negatively affect cognition, mental health, and motor skills may be present for years prior to a diagnosis [3, 4]. The typical age of onset for HD is 35 to 45 years [2], and many of those affected will therefore have caretaking responsibilities for children and families when the symptoms first appear; hence, HD is likely to impact the whole family, including children and adolescents, at a vulnerable stage of their lives [5–7].
A relatively small, but valuable, body of research has considered the impact of having a parent with HD can have on young people. These studies have suggested that the disease poses a severe risk to the lives of young people in the family, through a variety of practical, developmental, and social stressors [8–12]. A prominent challenge for children and adolescents dealing with HD in their family is the inevitably disruptive effect the disease has on the family environment; for instance, neurobiological and behavioural symptoms may lead to dysfunctional parenting, high levels of conflict in the family, instability, and an increased risk of exposure to adverse and potentially traumatic events [10, 11, 13]. Practical stressors may also arise from having a parent with HD, and many young people describe having overwhelming caretaking responsibilities at home [7, 12, 14]. Additional distress is placed on these young people by having to observe the detrimental effects HD has on their parent, knowing they have a 50% chance of developing the disease themselves, and having to decide whether they want to have a pre-symptomatic genetic test for the disease, while not knowing when symptoms will develop and being aware that there is no available cure [15–17].
Families have an increased need for personal and systemic support to cope with the inevitably demanding life tasks brought on by the disease. In many countries, formal and informal services are available for young people to help coping when a parent has HD, such as the web-based Huntington’s Disease Youth Organization (HDYO). However, recent research, including a worldwide survey, with over half the respondents coming from Europe, indicated that young people impacted by HD want, but may not be receiving, the support they need [8, 18, 19]. The lack of adequate support, despite the availability of services, could indicate that local healthcare and support providers do not have sufficient knowledge about HD to enable families to promote access to, and utilise, services [8]; hence, increasing knowledge and awareness about the possible risks posed by growing up in families affected by HD should be a priority.
To date, no research has exclusively considered how young people in Norway experience HD. The Norwegian and Scandinavian public services are unique in that they are free-of charge, available to all residents, and include services ranging from education to health care. A few recent Norwegian studies have examined caregivers and individuals with HD’s views on the provision of support and services that are available to them. Similar to findings from other countries, these studies have indicated that services appropriate for the management of HD and family care may still be quite limited, and neither the patients nor their families feel that they receive the support they need [20, 21]. Given the possible risks posed by HD on the wellbeing of children and adolescents, there is a need for research to more exclusively investigate the challenges these young people may experience, in order to guide our understanding of the areas of life in which they might need additional support.
This study aimed to provide a participant-generated overview of the main challenges experienced in everyday life by those growing up with a parent with HD, in order to shed light on areas of risk for young people and promote the provision of youth-focused support.
MATERIALS AND METHODS
Sample and setting
Qualitative data was gathered in 2018 as part of a larger study with the aim of describing the experience of growing up in a family affected by HD. In this paper, we focused on areas the participants described as challenging, in order to provide a preliminary framework for areas of focus in the provision of support for this group.
Anyone in Norway over the age of 12 years who had, or used to have, a parent with HD was invited to participate in the study. Information about the study was distributed in several settings where individuals who had grown up with a parent with HD could be reached. Information was distributed verbally and through information sheets. The main locations for distributing information included educational courses for families affected by HD and venues for family interactions with counsellors at the Oslo and Haukeland University Hospitals, and St. Olavs Hospital. Information about the study was also distributed through Facebook and the Norwegian Association for Huntington’s Disease. The information sheets outlined the research purpose, provided information about the interview topics, and provided the main researcher’s name and contact information.
In response to formal and informal information and invitations, 42 participants gave their initial written consent to participate. Of these, six people could not be reached when contacted for an interview. A total of 36 participants were interviewed and included in the analysis. The participants’ demographics are presented in Table 1. Participants ranged in age from 13 to 65 years (Mage = 36.6 years). The study included current and retrospective experiences of growing up with HD. The first interviews revealed that older participants were able to look back and contribute specific, emotionally laden, and vivid memories from their own childhoods. Inclusion of this subgroup was seen as ethically important, and their contribution was believed to potentially shed a different light on the findings.
Table 1
Demographic characteristics of the participants (N = 36)
| Variable | Label | N | |
| Age | 13–18 years | Teenager | 7 |
| 19–35 years | Young adult | 10 | |
| 36–65 years | Adult | 19 | |
| Gender | Female | 26 | |
| Male | 10 | ||
| Ethnicity | Norwegian | 33 | |
| Other | 3 | ||
| Parent with HD | Mother | 19 | |
| Father | 17 | ||
| Family status | Parent | 16 | |
| No children | 15 | ||
| Unknown | 5 |
Data collection and processing procedures
An interview guide was created, based on the relevant literature and feedback on the guide’s relevance from clinical experts. A group of user representatives (individuals with personal experience of being a carer for a parent with HD, or a partner with HD in families with children) also provided feedback on how the questions were understood, as well as on their completeness and relevance to the selected topics and research questions. Individual semi-structured interviews were conducted, focusing on both the challenges and protective factors, in order to cover the scope of the larger study. Semi-structured interviews permitted an open exploration of the interviewees’ experiences, while the structure helped the interviewer to focus on specific issues. Table 2 displays the interview topics and sample items. Interview topics included the participants’ childhood narratives and family situations, their relationships with parents, their understanding or lack of understanding of HD as a child, openness about the disease, and experiences of support. On average, the interviews lasted 60 minutes (range: 27 minutes to 90 minutes). Face-to-face interviews were preferred (n = 33), but telephone interviews were an option for some participants (n = 3). Interviews were mainly conducted at the Centre for Rare Disorders at the Oslo University Hospital or in the homes of a few participants. Interviews were conducted by postgraduate psychology students from the University of Oslo and University of Bergen, or by trained health professionals at Oslo University Hospital in Norway. The students had no previous experience with HD, but the health professionals from the Centre for Rare Disorders had previous experience of researching the disease. Counsellors from the Centre for Rare Disorders, with long clinical experience of HD, were involved in planning the study and developing the interview guide, but due to their potential knowledge of, and connection to, potential participants, they were not involved in the data analyses or the interpretation of the results. An inductive (data-driven) approach to analysis was chosen, where data were collected and coded without trying to fit them into pre-existing clinical preconceptions [22]. Our analysis did not set out to prove or disprove hypotheses or clinical evidence; rather, it sought to collect participant-driven data from which an understanding of challenges associated with growing up in families affected by HD could be developed. All the interviewers had, or received, formal training in qualitative methods before conducting the interviews. The interviewers had no previous contact with the study participants. To ensure the fidelity and consistency of all interviewers’ practices, the project manager, who was an experienced and licenced clinical psychologist, participated in at least two interviews conducted by novice researchers; hence, supervision regarding interview techniques and clinical safeguards could be provided if needed. The project manager also discussed and supervised the need for a follow-up with participants after the interviews.
Table 2
Main topics and sample items applied in the semi-structured interview guide
| Interview Topic | Sample Question |
| Background information | What is your motivation to participate in this study? |
| Can you describe the family you grew up in? | |
| Childhood experience | Tell us about your experience of your childhood? |
| Can you describe how your parents’ disease affected your family? | |
| What was your relationship with your mother and father like? | |
| In what ways has growing up with a parent with HD affected you? | |
| Disease- and self-disclosure | What is your experience of disclosing information about HD growing up? |
| What are your thoughts on how parents should inform their children about HD? | |
| Resources and support | What were your sources of support growing up? |
| How did you/ do you feel about having friends over to visit? | |
| If you had the chance, what would you say to someone in a similar situation as you are/ were? |
Data analysis
The interviews were recorded, transcribed verbatim, and subjected to a qualitative thematic analysis that investigated common themes relating to the challenges described by the participants. The project manager performed sample tests on the correspondence between the interviews and transcripts to ensure accuracy. The analysis followed the structured guidance of Braun and Clarke [22]. The first and second authors, who were not involved in the interviews, initially became familiar with the data by reading and re-reading the interview transcripts. Prevalent topics were noted during this stage. The first and second authors then generated initial codes by isolating phrases, sentences, and paragraphs, and generated a list of codes representing every transcript. Code reliability was subsequently assessed by comparing the codes generated by the first two authors with those of the project manager (third author). The lists of codes were collated to search for themes according to the similarities between them. Themes were chosen for their prevalence in relation to the research question. These themes were reviewed against the data and discussed between the three authors until full agreement was reached; the final themes were then determined and named. Finally, the report was produced. The analysis was seen as a recursive process, and detailed notes were written throughout.
In line with the study’s aim to present a qualitative overview of common themes, all the challenges described by the participants were included in the analysis. No challenges failed to fit within the categories that emerged from the data and constituted the main themes. The most commonly described challenges within each main theme were included as sub-themes and/or will be described in the results section. Quotes that represented the themes were selected and translated from the original language into English. The participants were given pseudonyms to preserve their anonymity.
To account for the large age range of the study participants, the experiences of the two age groups were compared during the analysis. The first group included teenagers and young adults who had had experiences reflecting contemporary support systems (13 to 35 years), and the second group included adults older than 35 years, whose experiences might reflect different societal attitudes and/or experiences of support (36 to 5 years). For some participants their parents had been diagnosed or developed symptoms of HD in their early childhood, whereas others had experiences of the disease during later childhood and adolescence. The interviewers asked participants to provide their approximate age when sharing childhood memories. Given this study’s focus on childhood experiences, only accounts described as childhood memories (approximately 0 to 18 years) were included in the analysis.
Ethical considerations
The regional ethics committee in Norway granted approval for the study (2017/864347). Written consent was obtained from all the participants and they were informed of their right to withdraw at any time. Confidentiality of participant information was ensured throughout the research process. In addition to adult participants’ own consent, parental consent was obtained for participants under the legal age for health consent (16 years in Norway). The larger study did not exclude participants with a pre-symptomatic or symptomatic diagnosis of HD. Given the genetic specificity of HD, some participants could have inherited the disease and might have symptoms of HD. Since HD does not affect long-term memory [23], affected individuals may recall their childhood without major interference from the disease. To evaluate validity and assess whether data from affected participants should be included, a clinical screening of insight, awareness of symptoms, and life situation was included during the interviews. Patients with communication or cognitive functioning difficulties that might have affected their participation in the in-depth interviews would have been excluded from the data, but no participants were excluded from the study on this basis.
Due to the sensitivity of the topics discussed during the interviews, relevant referrals or subsequent follow-ups were arranged by the trained clinical psychologist performing the interviews, if necessary. All the participants received a follow-up call within two weeks after the interview to assess the need for referral to a clinical psychologist. Three participants wished to receive follow-up after the interviews and were referred to a clinical psychologist.
RESULTS
Analysis of the data identified four main themes reflecting participants challenging experiences: (1) family functioning, (2) emotions and reactions, (3) social functioning, and (4) public and care services. Themes and sub-themes are presented in Table 3.
Table 3
Main themes and sub-themes
| Themes | Sub-Themes |
| Family Functioning | Parent characteristics |
| Family dynamics | |
| Home life | |
| Aversive and traumatic experiences | |
| Emotions and Reactions | Disease and childhood experiences |
| Inheritability | |
| Information | |
| Social Functioning | Peer relationships |
| Activities and community participation | |
| Public and Care Services | School |
| Health- and care services |
Theme 1: Family functioning
Participants in this study gave narratives of a variety of examples of household dysfunction in their upbringing, that included challenges with the characteristics of HD, family dynamics, diseases other than HD affecting the family, their living conditions, and experiences of adverse or potentially traumatic events. Although the severity and impact the disease had on family functioning varied between individuals, these experiences did not appear to differ substantially between the group of teenagers and young adults, compared to the older participants.
Parent characteristics
Participants generally described challenges that directly resulted from the symptom progression and characteristics of HD. Many explained that the disease symptoms had overshadowed other qualities of the parent. Such as Jacob, a young adult male who grew up with a mother with HD: ‘She became less like a mother and more like a patient ( ... ) more like a disease, instead of a parent.’ Participants consistently emphasised the disease’s psychological and cognitive symptoms as the most difficult to cope with. Psychological and cognitive symptoms had often been present and negatively impacting their family functioning, long before physical symptoms were apparent or a diagnosis was made. Elisabeth, an adult female explained how HD had affected her mother: ‘She would get mad about things you couldn’t understand. What you were allowed to do yesterday wasn’t allowed the next day. What you did last week you couldn’t do the next. It’s an absurdity you cannot understand as a child.’ Several participants also described challenges with illness and diseases other than HD in their family. Often, their other parent had also suffered from illness, including physical illness, psychiatric disorders, and substance abuse. For some of the participants, the other diseases that challenged family functioning had occurred as a result of the strain HD had on the other family members. Josephine, a young adult female who grew up with a mother with HD, stated that she felt she had lost both parents because of HD: ‘My dad has been without a job ever since my mum got sick. So in a way he got sick too. He doesn’t seem to live anymore either.’
Family dynamics
Participants gave consistent descriptions of issues in the dynamics of their family. Their relationships with their parents and relationships between their parents were often characterised by conflict, instability, and impressions of not receiving sufficient or appropriate care. Many had experienced verbal and/or physical fights and separation or divorce. Sally, a young adult female who grew up with a father with HD described: ‘All the fighting my parents did and all those conflicts ... and the discomfort of being at home ... It’s been a lot [to take].’ They had also typically experienced conflict with their extended family, and intrigues and a lack of support had been common here too. For example, Ava, an adult female who grew up with a mother with HD, recalled: ‘On that side of the family, there has not been one point in time where they have all been friends.’
Home life
Participants typically described difficulties with their living situation throughout their upbringing. Many experienced being overwhelmed by chores and household duties, as well as having to physically and mentally care for their sick parent(s). Sue, an adult female who grew up with a mother with HD, recalled: ‘You are put to work cleaning floors, doing laundry, vacuuming, changing the beds, and you ask yourself: “Am I doing this so that you can hide that you are no longer able to do these things?” We always had chores.’ A few participants also mentioned unstable living conditions, such as their parent having to relocate. There were several descriptions of the parent’s disease contributing to financial and occupational strains for the family, such as described by Amy, a young adult female who grew up with a father with HD: ‘I saw how much my mum struggled in the beginning, doing everything she could. She took time off work and stayed at home, so it affected our financial situation.’
Adverse experiences
Participants typically described being exposed to several events during childhood that were distressing, adverse, and/or potentially traumatic. Most frequently were descriptions of the conflict-ridden divorces and separations of parents, emotional neglect, and exposure to aggression and/or violence in the home. Participants also described family members’ suicides or suicide attempts. Incidences of aggression and violence were either directed at the children themselves, witnessed by children when they occurred between parents, or between other family members. Mary, an adult female who grew up with a father with HD, described: ‘My dad was violent with my mom, psychologically abusing her, things of that nature.’
Theme 2: Emotions and reactions
Participants gave consistent descriptions of a multitude of emotional challenges during their upbringing. These were often related to how participants experienced the disease and impressions of their childhoods, the emotional impact of potentially inheriting the disease, and their feelings and reactions to information about HD.
Disease and childhood experiences
Participants frequently described difficult psychological experiences relating to their parents’ disease and their childhood. Common thoughts and feelings about HD included feelings of embarrassment over illness symptoms, anger, powerlessness over the progress and impact of the disease, and feelings of losing their caregiver. The descriptions did not appear to differ substantially between younger and older participants. Lucy, an adult female who grew up with a mother with HD, described: ‘The embarrassment I felt, and the feeling that something was missing. I wasn’t supposed to be the one supporting her; she was supposed to be the one supporting me.’ Participants typically reported their childhood as being overshadowed by negative feelings, such as fear and a lack of security as the result of conflicts at home, and feelings of living with constant chaos and unpredictability. Several of the younger participants described such childhood experiences; however, they appeared to be more prominent in descriptions provided by the group of older participants. Alf, an adult male who grew up with a father with HD, described:
My childhood felt unsafe. We never knew what to expect at home. He [his father] was suspicious, always ‘right’, and very irritable. We kids always had to be considerate of him: never saying what we really felt, not getting into fights. If he didn’t take it out on us, he took it out on our mum.
Many emphasised that they had felt invisible due to their parent’s illness, experiencing loneliness, or using isolation as a means to mentally escape from their home life.
Inheritability
Being at risk of inheriting HD had been a common concern to many participants growing up, with feelings characterised by a loss of hope and/or not being motivated to make plans for their own future, such as investment in education and romantic relationships. Although several of the adult participants described experiencing the inheritability of the disease as problematic during their upbringing, the topic appeared to be more prevalent among the younger participants. Emma, a teenage female with a father with HD, said:
My future is pitch black. Others are talking about having boyfriends, having a future, a house, a car, and an education. I can’t have any of that. There is no point in me starting a long university degree. If I meet someone I like, I have to tell them about this before we start to date, and if I haven’t inherited this, my siblings may have. I can’t plan ahead.
Some participants also described how they had been searching for symptoms, thinking they had inherited the gene, a challenge that was also often linked to another prominent emotional difficulty; whether or not to be genetically tested for the disease. Nick, a young adult male who grew up with a father with HD, described: ‘It’s like having a noose around your neck constantly. You don’t know if it’s there or not, and that’s what makes it so much harder. I have a 50/50 [chance of a] death sentence. Believe it or not, it’s shit; fucking unfair.’
Information
Participants generally described negative feelings relating to the information they did, or did not, receive about HD during childhood. Experiences of how and whether participants were informed about their parents’ disease did not appear to differ substantially between the younger participants and the older ones. They provided descriptions of a lack of disclosure and communication within the family, and a desire for more information. Some felt they had been presented with incorrect or misleading information about their parent’s disease. Miriam, a teenage female with a mother with HD, told: ‘I wish I had been raised with the knowledge that mom would get sick, instead of them lying about it and the disease coming as a shock.’ Due to a lack of alternative explanations, the change in their parents’ behaviour was often believed by participants to be a consequence of their own wrongdoing, leading to feelings of self-blame and guilt. Sue, an adult female who grew up with a mother with HD, described: ‘You have that fear, right, when you don’t get any information, and then you ruminate: “What is happening? Did I do anything?” ... that guilt.’ Regardless of the content of or amount of information the participants received, most participants described emotionally challenging reactions to first learning about the disease, with descriptions of anger, shock, and fear being common.
Theme 3: Social functioning
Several of the challenges experienced by the participants extended beyond the impact HD had on their family. These descriptions included how the disease had impacted their ability to maintain normal social lives, such as through peer relations or participation in social activities in the communities where they lived.
Peer relations
Participants had frequently experienced difficulties in establishing and maintaining peer relationships in childhood. Their ability to form and maintain friendships had often been limited, due to the inability to have visitors at home, or to visit others, as a result of their parent’s illness and their living situation. Katie, a young adult female who grew up with a father with HD, said: ‘I was very hesitant to bring people home, because we never knew ... It was embarrassing that other people should also see them fight.’ Many had felt envious of their peers who seemingly had well-functioning families. Having difficulties with peer relationships as a result of their parents’ disease did not appear to differ substantially between the younger participants and the adults; however, the need to be open about the disease with their friends appeared to be a more pervasive issue for the younger participants, compared to the adults. How to be open about the disease was a challenge in peer relationships for many participants. Thomas, an adult male who grew up with a father with HD, reflected on his lack of openness with childhood friends, recalling: ‘I used to not want to talk about it, but now I see that I lost contact with a lot of my friends. I think it was largely because I distanced myself like that.’ Some feared negative reactions from friends if they talked about their parent’s disease and their home lives, while others experienced that their friends did not understand what they were going through, and consequently chose to not disclose this part of their lives.
Activity and community participation
Participants typically described challenging interactions within the communities they grew up in, often related to social interactions and a lack of support from community residents. Although there were individual differences in these descriptions, how the disease affected participants’ abilities to participate in social or organised activities, or to be a part of the communities they lived in, did not appear to differ substantially between the younger and older participants. Ashley, an adult female who grew up with a father with HD, told: ‘We had neighbours we tried to talk to, but they did nothing, so it didn’t help; and there were friends of my dad’s, but nobody reacted or did anything ( ... ). People are very scared of meddling in other people’s lives.’ Misunderstandings and stigmatisation as a result of HD had been common, such as their parent’s symptoms being mistaken for alcohol abuse. Some participants reported feeling isolated and withdrawing from social participation in the community, often from fear of standing out or being embarrassed by their parent’s behaviour outside the home. Some described challenges with participating in social and organised activities during their upbringing. Activities were described as restricted because parents could not facilitate them, or by limitations on participants’ free time due to responsibilities at home. Amy, a young adult female who grew up with a father with HD, said:
I could never do anything with my classmates. They would ask me to do homework with them and I would have to tell them ‘No, I have to go home’, but I never told them why. I never told them what I had to do.
Theme 4: Public and care services
Participants indicated a multitude of challenges influencing their encounters and experiences with the public, health, and social care system.
School
Participants typically described challenges with normal participation in school during childhood. Many had felt a lack of support and understanding regarding their parents’ disease and their demanding living conditions at school. Olanna, a young adult female who grew up with a father with HD, described feeling rejected when she tried to confide in her teachers at about the chaos she was experiencing at home and the bullying she was subjected to: ‘Teachers in primary school whom I talked to didn’t believe me. If they had actually believed me, it would have helped.’ Several participants also found it difficult to attend school as required. When they had attended, they often described a lack of concentration and motivation, making it hard to perform at the same level as other students. For younger participants, issues of bullying, school absence, and a lack of concentration appeared to be more pervasive than for older participants. Katie, a young adult female who grew up with a father with HD, stated: ‘I was the type of person that really wanted to do well in school, but there was just too much chaos around.’
Health and social care services
Participants generally described having several challenging encounters and interactions with public health and social care services during their upbringing. These experiences involved a wide variety of services that the families had been in contact with, and included (but were not limited to) home visits made by police, child protection services checking up on the family, home carers for the parent with HD, nursing homes in which the parents with HD lived, and ambulance services responding to emergencies. Regardless of the type of public health or care service described by participants, feelings of lack of support and understanding were common. Many of the participants felt that the formal care system lacked knowledge about the disease and its ramifications. Older participants gave more descriptions of an absence of available support and knowledge, whereas younger participants, to a larger extent, explained that support services were available to them, but that the available provision of support was not what they needed. Josephine, a young adult female who grew up with a mother with HD, stated:
We would call the ambulance occasionally, because she [her mom] would be acting crazy, screaming and throwing things, but the ambulance never showed up until half an hour later, and by that time she had already calmed down. They didn’t understand that there was anything wrong with her; she was just sitting there smoking. What the ambulance workers saw was nothing. At times they would even suggest I was the one in need of psychiatric help.
When in contact with formal health and care services, some participants had held back information and did not share the true impact their parent’s disease had on the family. This was described as an attempt to be loyal to, and to protect, their family, or from fear of the perceived consequences of telling the truth. Karen, an adult female who grew up with a mother with HD, recalled how she lied in a meeting with the child protection services, because she was scared of the perceived consequences of telling them about her mother’s psychiatric symptoms and medication abuse: ‘I was very scared they [child protection services] would take my brother away from us, so in the meeting, I was defending my mum with every means possible. I regretted it later on.’
DISCUSSION
This qualitative study has provided a participant-generated overview of challenging experiences brought on young people’s lives by growing up with a parent with HD. The study has shown that having a parent with HD may present risks within several areas of life, including family functioning, emotions and reactions, interaction with peers and communities, participation and performance at school, and interactions with public health and care services.
The impact of HD on family functioning
Growing up in a family affected by HD had presented multiple challenges to how the participants’ families functioned. Similar to findings from previous studies [7, 9, 12, 24], many felt that they had to be the caregiver, and that responsibilities such as chores, caring for siblings, and personal and social care for their sick parent, often fell on the young people in the family. The psychological and cognitive symptoms of HD described, including inhibition, irritability, and aggression, had interfered with the appropriateness of responses and actions of parents and had severely impacted the relationships between all the family members. These symptoms had been apparent before physical symptoms were present or a diagnosis was made, and were emphasised as particularly disrupting and confusing during childhood, and experienced as more challenging than physical symptoms. The negative impact HD can have on dynamics in a family has been well documented [5, 9, 10, 13]; however, there is limited knowledge, so far, on how prodromal symptoms impact young people who have a parent with HD. The findings therefore provide new knowledge suggesting that children who grow up in families affected by HD may be particularly vulnerable to prodromal psychiatric and cognitive symptoms in the affected parent, even in the very early stages of the disease. Based on our results, it should be a priority to identify young people living in families impacted by HD, and to provide early intervention and support. Young people in this situation may require help to develop useful coping strategies. They will need information about the early symptoms of HD, in order to increase their understanding and appropriate interpretation of changes occurring in their parent as a result of the disease. Both practical and emotional support should be offered to young people to help them effectively deal with the complex caregiving tasks, and the challenges associated with changes observed in their parent at home.
Participants in this study were also commonly exposed to adverse and potentially traumatic events in their upbringing. To date, only a few studies have described how young people in families affected by HD may be exposed to adverse and possibly traumatic events during their upbringing [13]. Although little is known about how adversity in families affected by HD may have an impact on young people in the long term, these possible risks should not be underestimated. Being exposed to continuous stressors, instability, and adversity during childhood and adolescence can change a child’s biological, psychological, and social trajectories and lead to immediate and long term consequences for their mental and physical health [6, 25–27]. We believe it is vital to provide support to families impacted by HD to minimise possible risks to family functioning, and to help young people cope with the possibly adverse or traumatic events they may experience. We also strongly suggest that the adverse and/or potentially traumatic events this population may have to endure needs to be further researched.
The impact of HD on emotional and social functioning
The emotional strain and negative impact HD had on the participants psychological wellbeing is a major area of concern. Growing up with a parent with HD included persistent feelings of instability, insecurity, and/or fear, as well as the presence of additional emotional strain during their upbringing. Clinical experience and previous studies have supported our findings regarding the multitude of emotional challenges experienced by young people who have parents with HD [9, 13, 17, 18, 28] and have indicated that many struggle with anxiety and depression [8]. For participants in our study, psychological wellbeing and adjustment to the disease appeared to be negatively influenced when they were given little or no information about HD; information that would have explained the changes they observed in their parents’ behaviour. Previous work indicated that the level of information and explanation given to children about HD may be essential for young people’s emotional adjustment, influencing self-esteem, anxiety, distress, and feelings of isolation [9, 10]; thus, a combination of chronic stressors and emotional challenges, brought on when a parent has HD, may present a high risk to the psychological wellbeing of young people. Appropriate help and support for coping with the emotional impact HD can have on wellbeing should therefore be a priority.
To help with these emotional strains, facilitating peer support may, in some cases, be more beneficial than support from health or care services [8, 9, 19, 29]. Lacking peer relationships and support through social activities may increase the risk of poor psychological adjustment, causing social isolation and stress [18]. For the participants in this study, complex interactions between the demanding family environments and the psychological strain caused by the disease also affected a variety of social factors, such as the ability to maintain peer relationships and socialise within the communities where they lived. Previous work also suggested that the demanding and unpredictable everyday lives at home, for young people in families impacted by HD, limits the ability to partake in social and organised activities [8, 9]. Formal and informal support services should refer young people to available arenas for peer support, such as the Huntington’s Disease Youth Organization (HDYO), Young People Affected by HD (YPAHD), and the Huntington’s Disease Society of America’s National Youth Alliance (NYA). These services can easily be used to connect with others in similar situations, possibly decreasing feelings of isolation, loneliness, and lack of social support.
Experiences with public health and care services
Another major area of concern was the multitude of problematic experiences the participants had with public, health and care services. Available research has suggested that almost half the young people in families affected by HD have limited time for school [8], and they describe poor performance in school as a result of the difficulties of multitasking with the responsibilities at home [24]. Participants in our study had also been struggling with participation and performance in school, and felt a lack of appropriate support from school to cope effectively. Their difficulties at school appeared to be intertwined with other challenges brought on by HD, such as difficulties with peer interactions and, importantly, a lack of motivation linked to the fear of inheriting the disease; hence, growing up with a parent with HD may limit educational and occupational opportunities. School employees should be aware of how having a parent with HD can potentially adversely affect educational and occupational trajectories, and aid in the facilitation of young people’s motivation, participation, and performance in school.
The participants’ interactions with available health and social care providers were also, often, described as challenging; many felt they had not received adequate or appropriate support, and they were often left frustrated by a lack of information and appropriate action from health and care services. Few studies have specifically investigated the provision of support for young people in families affected by neurodegenerative diseases [8, 18, 29], and results from past research have often drawn on small or very mixed samples [5, 20, 21]. Available research has, however, suggested that, despite a need for support, young people may still feel that the impact the disease has on their childhood is overlooked by the available services [8, 18, 19]; hence, although both formal and informal services are available, those services may not be provided to families affected by HD, as there is a lack of understanding and information available about the impact of HD can have on young people, which may lead to inappropriate or inadequate support. A lack of understanding, and a lack of appropriate measures taken to help young people in families affected by HD, may leave support providers in danger of further exacerbating feelings of loneliness and isolation that are already a challenge in their lives. The impact of being a young carer, combined with the general lack of sufficient support described in this study is a highly serious matter. Health is an important theme in all the human rights conventions, and all governments are obliged by law to protect the health and wellbeing of children. Children have a right to grow up in environments that does not negatively impact their well-being, a right to be conferred in matters that affects them and their families [30], and governments should make sure that young people’s tasks as carers does not negatively affect their own health [31]. Seemingly, the multitude of complex tasks of growing up with a parent with HD described by many of our participants could be in violation of these rights. Health and care professionals in contact with families affected by HD need to have sufficient knowledge and awareness of the complex ramifications of HD for young people, in order to adapt their provision of services according to individual rights and needs.
Ripple effect
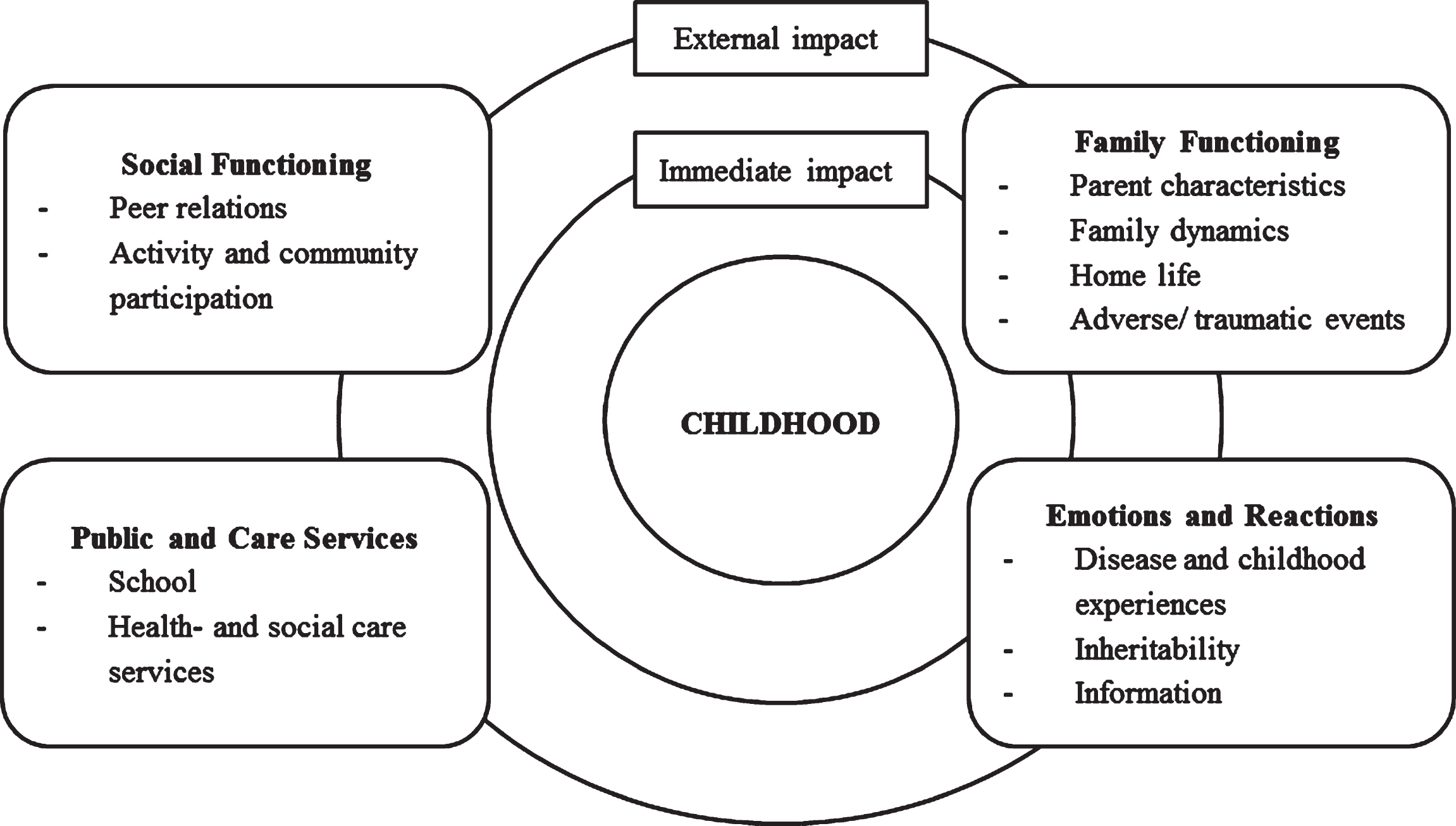
The multiple burdens of having a parent with HD, as found in this study, cannot be overstated. Our findings demonstrated a substantial need for more awareness and knowledge about the complex impact HD can have on young people in affected families, and a need to promote the provision of more youth-focused support, at all levels of services and within multiple areas of life, for this group. To decrease the gap in the provision of support, promoting awareness and knowledge that can easily be applied would be valuable. The overview of challenges highlighted by this study, can provide a useful template to guide the areas of young people’s lives that need to be explored and possibly supported by service providers that are contact with families impacted by HD. To understand the support needs of young people affected by HD, our results could be applied within a bioecological framework [32], as illustrated in Fig. 1. The bioecological model of human development has been used to explain how children’s development is affected by their environment in many ways. By applying the challenges provided by the participants in this study within a well-established framework of human development, awareness and knowledge about the multiple risks presented by HD for young people would be more easily accessible to a broad range of support services, including families, social networks, and public health and care services. According to this framework, and in line with this study’s findings, human development is influenced by a continuous interaction between internal and external environments, and a disruption at any significant point in a child’s life will create a ‘ripple effect’, possibly impacting all other areas of the child’s life [25, 27, 32, 33]. The immediate environment during childhood, such as the family environment, will have the greatest impact on developmental outcomes [32, 33, 34]. Correspondingly, previous research, clinical experience, and the current study have strongly suggested that the impact HD has on family functioning is a key challenge during upbringing. The rupture in the normal fabric of family life, created by their parent’s disease, influences a variety of factors outside the family. Our study demonstrated complex and constant challenging emotions and reactions, and a variety of difficulties with peer relationships and social support. The challenges posed by having a parent with HD interacted and appeared to ripple through many areas of life. Even when resources were available, the participants in this study clearly stated that they were in need of support, care, and understanding, now and during their upbringing. Young people currently affected by HD in their families will be at school, will be in contact with teachers and guidance counsellors, and will probably be in contact with multiple public health and care providers. For appropriate, early, and effective help with the multitude of challenges this group may be facing, it is vital to provide support services with sufficient knowledge and an appropriate understanding of the possible risks HD may pose for the lives of young people. Any source of support can use this framework to ask young people appropriate questions on how they experience and are coping in areas at risk highlighted in this study.
Fig. 1
Areas of life impacted when growing up in families affected by HD, illustrated within a Bioecological framework.
Strengths and limitations
This study offers a framework to understand the ‘ripple effect’ on challenges posed on the lives of young people by having a parent with HD. The presented template can be used to guide knowledge and awareness about how growing up with a parent with HD impact children, in order to support, at any level, the provision of more youth-focused intervention and family care; however, further research is still needed to establish the specific support needs of this group. From a qualitative perspective, the study’s relatively large sample is a major strength. Participants were broadly recruited and believed to be representative of the population under study; nevertheless, the qualitative nature of the study may limit the generalisability of the results. The participants in this study were teenagers and adults reflecting on their upbringing, and adult participants’ memories may have been affected by the time that had passed since the events. The results, particularly considering experiences of support from health and care services for older study participants, did not reflect current support services, such as web-based education, information, and support; youth summer camps; or counselling services. Nevertheless, older participants presented vivid and specific childhood memories, and their accounts of the impact of HD had on their lives were of equal importance. The study focused on experienced challenges, so evaluations of strengths, positive childhood impressions and emotions, and coping mechanisms were not included in the present paper. We acknowledge that there may be several aspects of growing up with a parent with HD that was not accounted for by this study, including factors that could moderate or protect against the challenges of HD, and experiences of challenges that went beyond childhood and adolescence for the adult participants. However, the present study is a part of a larger study, and further in-depth exploration of coping strategies and beneficial experiences will continue to be explored. Finally, the present study described the perceived challenges as a representation of a bioecological understanding of human development at a very basic level. This was done to provide a working template for the provision of support and understanding for young people in families affected by HD. Future studies could test the model or provide support for the effective application of this theoretical framework.
Conclusion
This qualitative study provided a participant-generated overview of areas of risk for young people growing up with a parent with HD, demonstrating how HD creates a ‘ripple effect’ on challenges, affecting multiple areas of life. The participants emphasised challenges within four domains during their childhood and adolescence: family functioning, emotions and reactions, social functioning, and public health and care services. Importantly, our findings indicated that young people with a parent with HD may be at high risk of harmful short- and long-term effects on their mental and physical health. The study also identified a gap in the provision of appropriate support from formal and informal health and care services for effectively dealing with the strain caused by having a parent with HD. Our findings highlighted the need for early intervention and collaboration between all support services for people growing up with a parent affected by HD. When applied within a bioecological framework the findings can be used to promote awareness and understanding among support providers about the complex impact the disease can have on young people. We have identified the risks that were emphasised by most of the participants, despite individual differences, differences in age, and differences in the availability of services. By recognising these similarities, we can enhance our knowledge about the challenges HD poses for the lives of young people and develop a better understanding of the need for formal and informal sources of support for this vulnerable group.
CONFLICTS OF INTEREST
The authors have no conflicts of interest to report.
ACKNOWLEDGMENTS
We thank those who participated in the study, and their families. We also thank the Norwegian Association for Huntington’s Disease, user representatives, and health professionals at the Centre for Rare Disorders at Oslo University Hospital (in particular Gunvor A. Ruud) for their invaluable collaboration and assistance in the development of the study, the recruitment of participants, and their encouragement throughout the research process. The study was funded by Extra Stiftelsen.
REFERENCES
[1] | Roos RA . Huntington’s disease: A clinical review. Orphanet J Rare Dis. (2010) ;5: (1):40. doi:10.1186/1750-1172-5-40 |
[2] | Sturrock A , Leavitt BR . The clinical and genetic features of Huntington disease. J Geriatr Psychiatry Neurol. (2010) ;23: (4):243–59. doi: 10.1177/0891988710383573 |
[3] | Duff K , Paulsen JS , Beglinger LJ , Langbehn DR , Stout JC . Psychiatric symptoms in Huntington’s disease before diagnosis: The predict-HD study. Biol Psychiatry. (2007) ;62: (12):1341–6. doi: 10.1016/j.biopsych.2006.11.034 |
[4] | Paulsen J , Langbehn D , Stout J , Aylward E , Ross C , Nance M , et al. Detection of Huntington’s disease decades before diagnosis: The predict-HD study. J Neurol Neurosurg Psychiatry. (2008) ;79: (8):874–80. doi: 10.1136/jnnp.2007.128728 |
[5] | Parekh R , Nordberg A , Praetorius R . T. Carers’ experiences in families impacted by Huntington’s disease: A qualitative interpretive meta-synthesis. Br J Soc Work. (2017) ;48: (3):675–92. doi: 10.1093/bjsw/bcw173 |
[6] | Shonkoff JP , Garner AS , Siegel BS , Dobbins MI , Earls MF , McGuinn L , et al. The lifelong effects of early childhood adversity and toxic stress. Pediatrics. (2012) ;129: (1):232–46. doi: 10.1542/peds.2011-2663 |
[7] | Mand CM , Gillam L , Duncan RE , Delatycki MB . ‘I’m scared of being like mum’: The experience of adolescents living in families with Huntington disease. J Huntingtons Dis. (2015) ;4: (3):209–17. 10.3233/jhd-150148 |
[8] | Lewit-Mendes MF , Lowe GC , Lewis S , Corben LA , Delatycki MB . Young people living at risk of Huntington’s Disease: The lived experience. J Huntingtons Dis. (2018) ;7: (4):391–402. doi: 10.3233/jhd-180308 |
[9] | Forrest Keenan K , Miedzybrodzka Z , Van Teijlingen E , McKee L , Simpson SA . Young people’s experiences of growing up in a family affected by Huntington’s disease. Clin Genet. (2007) ;71: (2):120–9. doi: 10.1111/j.1399-0004.2006.00702.x |
[10] | Vamos M , Hambridge J , Edwards M , Conaghan J . The impact of Huntington’s disease on family life. Psychosomatics. (2007) ;48: (5):400–4. doi: 10.1176/appi.psy.48.5.400 |
[11] | van der Meer L , Timman R , Trijsburg W , Duisterhof M , Erdman R , Van Elderen T , et al. Attachment in families with Huntington’s disease: A paradigm in clinical genetics. Patient Educ Couns. (2006) ;63: (1-2):246–54. doi: 10.1016/j.pec.2005.11.019 |
[12] | Sparbel KJ , Driessnack M , Williams JK , Schutte DL , Tripp-Reimer T , McGonigal-Kenney M , et al. Experiences of teens living in the shadow of Huntington disease. J Genet Couns. (2008) ;17: (4):327–35. doi: 10.1007/s10897-008-9151-6 |
[13] | van der Meer L , van Duijn E , Wolterbeek R , Tibben A . Adverse childhood experiences of persons at risk for Huntington’s disease or BRCA1/2 hereditary breast/ovarian cancer. Clin Genet. (2012) ;81: (1):18–23. doi: 10.1111/j.1399-0004.2011.01778.x |
[14] | Williams JK , Ayres L , Specht J , Sparbel K , Klimek ML . Caregiving by teens for family members with Huntington disease. J Fam Nurs. (2009) ;15: (3):273–94. doi: 10.1177/1074840709337126 |
[15] | Crozier S , Robertson N , Dale M . The psychological impact of predictive genetic testing for Huntington’s disease: A systematic review of the literature. J Genet Counsel. (2015) ;24: (1):29–39. doi: 10.1007/s10897-014-9755-y |
[16] | Quaid KA , Eberly SW , Kayson-Rubin E , Oakes D , Shoulson I , Huntington Study Group PHAROS Investigators and Coordinators. Factors related to genetic testing in adults at risk for Huntington disease: The prospective Huntington at-risk observational study (PHAROS). Clin Genet. (2017) ;91: (6):824–31. doi: 10.1111/cge.12893 |
[17] | Dondanville DS , Hanson-Kahn AK , Kavanaugh MS , Siskind CE , Fanos JH . ‘This could be me’: Exploring the impact of genetic risk for Huntington’s disease young caregivers. J Community Genet. (2019) ;10: (2):291–302. doi: 10.1007/s12687-018-0395-z |
[18] | Kavanaugh MS , Noh H , Studer L . “It’d be nice if someone asked me how I was doing. Like, ‘cause I will have an answer’: Exploring support needs of young carers of a parent with Huntington’s disease. Vulnerable Child Youth Stud, (2014) ;10: (1):12–25. doi: 10.1080/17450128.2014.980370 |
[19] | Forrest Keenan K , van Teijlingen E , McKee L , Miedzybrodzka Z , Simpson SA . How young people find out about their family history of Huntington’s disease. Soc Sci Med. (2009) ;68: (10):1892–900. doi: 10.1016/j.socscimed.2009.02.049 |
[20] | Røthing M , Malterud K , Frich JC . Family caregivers’ views on coordination of care in Huntington’s disease: A qualitative study. Scand J Caring Sci. (2015) ;29: (4):803–9. doi: 10.1111/scs.12212 |
[21] | van Walsem MR , Howe EI , Iversen K , Frich JC , Andelic N . Unmet needs for healthcare and social support services in patients with Huntington’s disease: A cross-sectional population-based study. Orphanet J Rare Dis. (2015) ;10: (1):124–34. doi: 10.1186/s13023-015-0324-8 |
[22] | Braun V , Clarke V . Using thematic analysis in psychology. Qual Res Psychol. (2006) ;3: (2):77–101. doi: 10.1191/1478088706qp063oa |
[23] | Ghosh R , Tabrizi SJ . Huntington disease. Handb Clinical Neurol. (2081) ;147: :255–78. doi: 10.1016/B978-0-444-63233-3.00017-8 |
[24] | Kavanaugh MS . Children and adolescents providing care to a parent with Huntington’s disease: Disease symptoms, caregiving tasks and young carer well-being. Child Youth Care Forum. (2014) ;43: (6):675–90. doi: 10.1007/s10566-014-9258-x |
[25] | Rosa EM , Tudge J . Urie Bronfenbrenner’s theory of human development: Its evolution from ecology to bioecology. J Fam Theory Rev. (2013) ;5: (4):243–58. doi: 10.1111/jftr.12022 |
[26] | Cottrell B , Monk P . Adolescent-to-parent abuse: A qualitative overview of common themes. J Fam Issues. (2004) ;25: (8):1072–95. doi: 10.1111/jftr.12165 |
[27] | Gorman-Smith D , Tolan PH , Henry DB . A developmental-ecological model of the relation of family functioning to patterns of delinquency. J Quant Criminol. (2000) ;16: (2):169–98. doi: 10.1037/0893-3200.10.2.115 |
[28] | Ellison M . The impact of Huntington disease on young people. Handb Clin Neurol. (2017) ;144: :179–82. doi: 10.1016/b978-0-12-801893-4.00015-8 |
[29] | Ferm U , Nilsson S , Nolbris MJ , Linnsand P , Jonsson A . Impact of a parent’s neurodegenerative disease and care on the daily life of children. In Mollaoglu M, editor. Care-giving and Home Care. Riejeka: IntechOpen; 2017. doi: 10.5772/intechopen.68839. Available from: https://www.intechopen.com/books/caregiving-and-home-care/impact-of-a-parent-s-neurodegenerative-disease-and-care-on-the-daily-life-of-children |
[30] | United Nations, Convention on the Rights of the Child; 1989. (https://www.unicef.org/child-rights-convention/convention-text) |
[31] | Council of Europe, European Social Charter; 1961. (https://www.coe.int/en/web/conventions/full-list/-/conventions/treaty/035) |
[32] | Bronfenbrenner U , Morris PA . The bioecological model of human development. In Damon W, Lerner RM, editors. Handbook of Child Psychology. New Jersey (US): John Wiley & Sons; 2007. doi:10.1002/9780470147658.chpsy0114 |
[33] | Bronfenbrenner U , Ceci SJ . Nature-nuture reconceptualized in developmental perspective: A bioecological model. Psychol Rev. (1994) ;101: (4):568–86. doi: 10.1037/0033-295X.101.4.568 |
[34] | Shonkoff JP . Building a new biodevelopmental framework to guide the future of early childhood policy. Child Dev. (2010) ;81: (1):357–67. doi: 10.1111/j.1467-8624.2009.01399.x |

