
Prevention of non-specific back pain through exercise and education: A systematic review and meta-analysis
Abstract
BACKGROUND:
Clinical practice guidelines stress the importance of prevention and treatment of non-specific back pain through exercise therapy. However, it has not yet been confirmed whether the combination of exercise plus education is more effective than such interventions taken separately.
OBJECTIVE:
To determine if the combination of exercise plus education is more effective for the prevention of non-specific back pain than exercise or education alone.
METHOD:
A systematic search of studies whose sample consisted of participants without non-specific back pain (primary prevention) and participants with non-specific back pain (secondary and tertiary prevention) was conducted in the following databases in March 2023: PubMed, Scopus, Web of Science and Medline.
RESULTS:
A total of 16 articles were selected. Statistically significant results were found in the pain variable with SMD
CONCLUSION:
Interventions that combine exercise and education seem to have a greater preventive effect on non-specific back pain, disability and kinesiophobia than those that include exercise or education in an isolated manner.
1.Introduction
Back pain is a common and disabling issue, and the leading cause of years lived with disability worldwide [1]. Back pain has become one of the main causes of demand for medical care in developed countries and a major cause of incapacity for work, all of which led to significant economic costs. In the United States, the total cost exceeds $97.4 billion. As for the United Kingdom, the total cost is approximately £11 billion [2, 3, 4]. The most common spinal disorder is non-specific back pain (NBP), in that it cannot be reliably attributed to a specific underlying condition such as cancer, infection, ankylosing spondylitis, or other inflammatory or infectious diseases [3].
In order to avoid these serious socioeconomic problems caused by NBP, it is essential to prevent its progression and avoid limiting consequences such as the loss of functionality or work capacity [2, 3, 4, 5]. The general term prevention can have three different distinctions: primary, secondary, or tertiary. Primary prevention means preventing the occurrence of a disease. Secondary prevention involves interrupting the disease process before a clinically recognizable disease emerges. Tertiary prevention focuses on reducing the complications of a disease, disability or injury through treatment and rehabilitation [5, 6]. Clinical practice guidelines stress the importance of NBP prevention and treatment through exercise therapy (i.e., yoga, stretching, Pilates and strength training) and health education (i.e., self-management techniques, pacing strategies, back protection techniques and pain neuroscience education) [3, 7, 8, 9].
A meta-analysis published in 2019 concluded that exercise is more cost-effective compared to usual medical care for subacute and chronic low back pain [10]. In fact, there are several systematic reviews that have examined the benefits of exercise for the prevention of low back pain with regard to pain reduction, improvement of disability, quality of life and kinesiophobia [11, 12, 13, 14]. There are also some reviews that show these improvements in the cervical region [15, 16, 17, 18, 19, 20]. Furthermore, in terms of education, it provides short-term improvements in pain and disability related to NBP, but, as a sole treatment for patients with spinal pain, the effects are small and may be insufficient [21].
However, there are no recent systematic reviews comparing whether the combination of exercise plus education is more effective for the prevention of NBP than such interventions taken separately. Therefore, our primary aim was to determine if the combination of exercise plus education is more effective for the prevention of NBP than exercise alone or education alone. In addition, as secondary objectives, we investigated the effects on other pain-related variables such as disability and kinesiophobia.
2.Materials and methods
2.1Data sources and searches
This study was prospectively registered on PROSPERO (code: CRD42021290875) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) [22] reporting guidelines for Exercise, Rehabilitation, Sport Medicine and Sports (PERSIST) [23], and the recommendations from the Cochrane Collaboration [24]. The PICO question was then chosen as follows: P – population: patients with NBP and participants without NBP; I – intervention: exercise therapy plus health education; C – control: only exercise or only education; O – outcome: characteristics of pain, kinesiophobia and disability; S – study designs: randomized controlled trial.
A systematic search for publications was conducted in March 2023 in the following databases: PubMed, Scopus, Web of Science and Medline. The search strategy included different combinations with the following Medical Subject Headings (MeSH) terms: Back Pain, Neck Pain, Musculoskeletal Pain, Exercise, Exercise Therapy, Health Education, Cognitive Behavioral Therapy, Primary Prevention, Secondary Prevention, Tertiary Prevention and Clinical Trial. The word ‘Prevention’ was used as a free term. The search strategy according to the focused PICOS question is presented in supplementary material I.
2.2Study selection
After removing duplicates, two reviewers independently screened articles for eligibility. In case of disagreement, a third reviewer made the final decision as to whether the study should be included or not. The following inclusion criteria were applied for the study selection: (i) published since 2016; (ii) studies where the intervention group performed exercise (i.e., yoga, stretching, Pilates and strength training) and received health education (i.e., self-management techniques, pacing strategies, back protection techniques and pain neuroscience education) were administered compared to a group performing exercise only or receiving education only; and (iii) the sample consisted of participants without NBP (primary prevention) and participants with NBP (secondary and tertiary prevention). NBP referred to lumbar, dorsal or neck pain (including various combinations of these areas). On the other hand, studies were excluded from this review: (i) non-randomized controlled trials; (ii) participants with specific causes of back pain; (iii) pregnant participants.
After screening the data, and extracting, obtaining, and screening the titles and abstracts for inclusion criteria, the full texts of the selected abstracts were obtained. Titles and abstracts lacking sufficient information regarding the inclusion criteria were also obtained in full. Full text articles were selected in case of compliance with the inclusion criteria by the two reviewers by using a data extraction form. The two reviewers mentioned independently extracted data from the included studies using a customized data extraction table on Microsoft Excel. In case of disagreement, both reviewers debated the issue until an agreement was reached.
2.3Data extraction and quality assessment
The following data were extracted for further analysis: demographic information (title, authors, journal, and year), the characteristics of the sample (age, gender, inclusion and exclusion criteria, and number of participants), study-specific parameters (duration of the intervention, adverse events, methods of exercise, and health education) and the results obtained (variables analyzed, instruments used, and time of follow-up). Tables were used to describe both the studies’ characteristics and the extracted data. The Jadad and PEDro scales were used to assess the quality of these studies. The risk of bias was assessed using the Cochrane Collaboration Toolkit RoB2. Finally, the GRADE system was used to evaluate the overall assessment of certainty. Two reviewers (P.H-L; J.L-B) applied the Jadad, Pedro, RoB2 and GRADE scales. In case of disagreement, a third author (R-L-R) also participated in the process to reach an agreement.
2.4Data synthesis and analysis
Standardized mean differences (SMD) and their 95% confidence interval (CI) were calculated as the between-group difference in means divided by the pooled standard deviation (SD) [25]. When these data were not available in the study, they were requested to the authors via email. Effect sizes were interpreted using the following cut-off values: 0 to 0.2: very small; from 0.2 to 0.5: small; from 0.5 to 0.8: moderate; and from 0.8: strong [26]. The same increments were used for negative values. The significance level was set to
The following units of measurement were used for the variables analyzed: pain (Visual Analogue Scale, Numeric Rating Scale and Pain Bothersomeness), disability (Roland Morris Disability Questionnaire, Neck Disability Index, Oswestry Disability Index and Working Ability Index), and kinesiophobia (Tampa Scale of Kinesiophobia and Fear Avoidance Beliefs Questionnaire). For the meta-analysis, the evaluated value of each result (pain, disability and kinesiophobia) was that obtained at the end of each intervention.
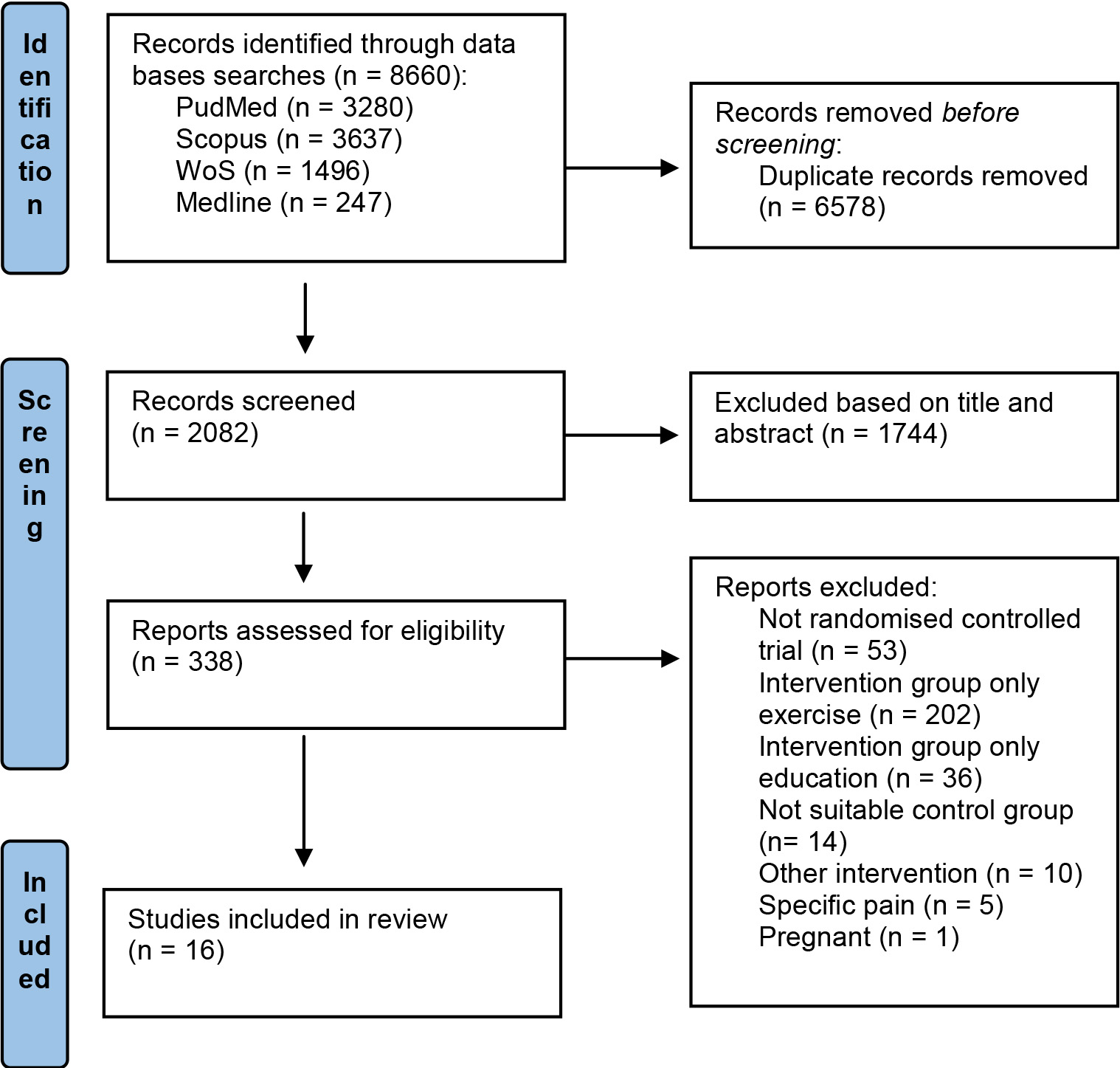
Figure 1.
PRISMA flowchart.
3.Results
3.1Included studies
Out of 8,660 search results, 2,082 studies were considered eligible for inclusion after removing duplicates. Among the 2,082 papers screened, 1,744 were excluded after abstract and title screening. After the first reading of all the prospective full texts, the Kappa score for reviewers 1 and 2 was 0.85, which was almost perfect [27]. Out of the 16 full-text articles assessed for eligibility, all of them were finally included in the synthesis (Fig. 1).
3.2Methodological quality of the studies and assessment of certainty
In the analysis of methodological quality using the Jadad scale, 11 articles obtained four or more points [28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38], four articles obtained three points [39, 40, 41, 42], and only one obtained two points [43]. The most common methodological shortcoming was the absence of blinding. (Supplementary material II).
At the same time, all studies were five or more points on the PEDro scale and the mean and nine items have seven or more points in the scala PEDro [29, 30, 32, 33, 34, 35, 36, 37, 38]. The most inconsistent PEDro scale item was the blindness of subjects and therapists. The average score of all articles on the PEDro scale was 6.9 points, which is considered a good methodological quality [44] (Table 1). The overall risk of bias was low in eight articles [29, 31, 33, 35, 36, 37, 40, 41], in four articles was some concerns [30, 34, 38, 39] and in four articles was high [28, 32, 42, 43] (Fig. 2). The degree of certainty assessed by the GRADE system shows a moderate degree of certainty which means that additional research is likely to have an important impact on our confidence in the estimate of the effect and may change the estimate [45] (Table 2).
Table 1
Risk of bias assessment using the physiotherapy evidence database (PEDro) scale
| Author | 1* | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Aliyu et al. (2018) | Yes | Yes | No | Yes | No | Yes | No | Yes | No | Yes | Yes | 6 |
| Andersen et al. (2016) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 10 |
| Bagheri et al. (2020) | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | No | Yes | Yes | 8 |
| Bodes et al. (2018) | Yes | Yes | Yes | Yes | No | No | No | Yes | No | Yes | Yes | 6 |
| Cherkin et al. (2016) | No | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7 |
| Garcia et al. (2018) | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Gorji et al. (2022) | Yes | Yes | Yes | Yes | No | No | No | Yes | No | Yes | Yes | 6 |
| Járomi et al. (2018) | Yes | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | 7 |
| Javdaneh et al. (2020) | Yes | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | 7 |
| Javdaneh et al. (2021) | Yes | Yes | Yes | Yes | No | Yes | No | Yes | No | Yes | Yes | 7 |
| Kuvačić et al. (2018) | Yes | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6 |
| Llamas-Ramos et al. (2022) | Yes | Yes | Yes | Yes | No | No | Yes | Yes | No | Yes | Yes | 7 |
| Montero-Cuadrado et al. (2022) | Yes | Yes | Yes | Yes | No | No | No | Yes | No | Yes | Yes | 6 |
| Rabiei et al. (2021) | Yes | Yes | Yes | Yes | No | No | No | Yes | No | Yes | Yes | 6 |
| Tunwattanapong et al. (2016) | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8 |
| Turner et al. (2016) | Yes | Yes | No | No | No | No | No | Yes | Yes | Yes | Yes | 5 |
Criteria: (1) Eligibility criteria specified; (2) Subjects randomly allocated to groups; (3) Concealed allocation; (4) Groups were similar at baseline; (5) Blinding of all subjects; (6) Blinding of all therapists; (7) Blinding of all assessors; (8) Measures obtained from more than 85% of subjects allocated to groups; (9) Subjects received treatment or control condition as allocated, or intention-to-treat analysis; (10) Between-group statistical comparisons reported for at least one outcome; (11) Both point measures and measures of variability were reported. High, high risk of bias; low, low risk of bias. *This item relates to external validity and therefore does not contribute to the total score.
Figure 2.
Risk of bias. D1: randomization process; D2: deviations from the intended interventions; D3: missing outcome data; D4: measurement of the outcome; D5: selection of the reported result.
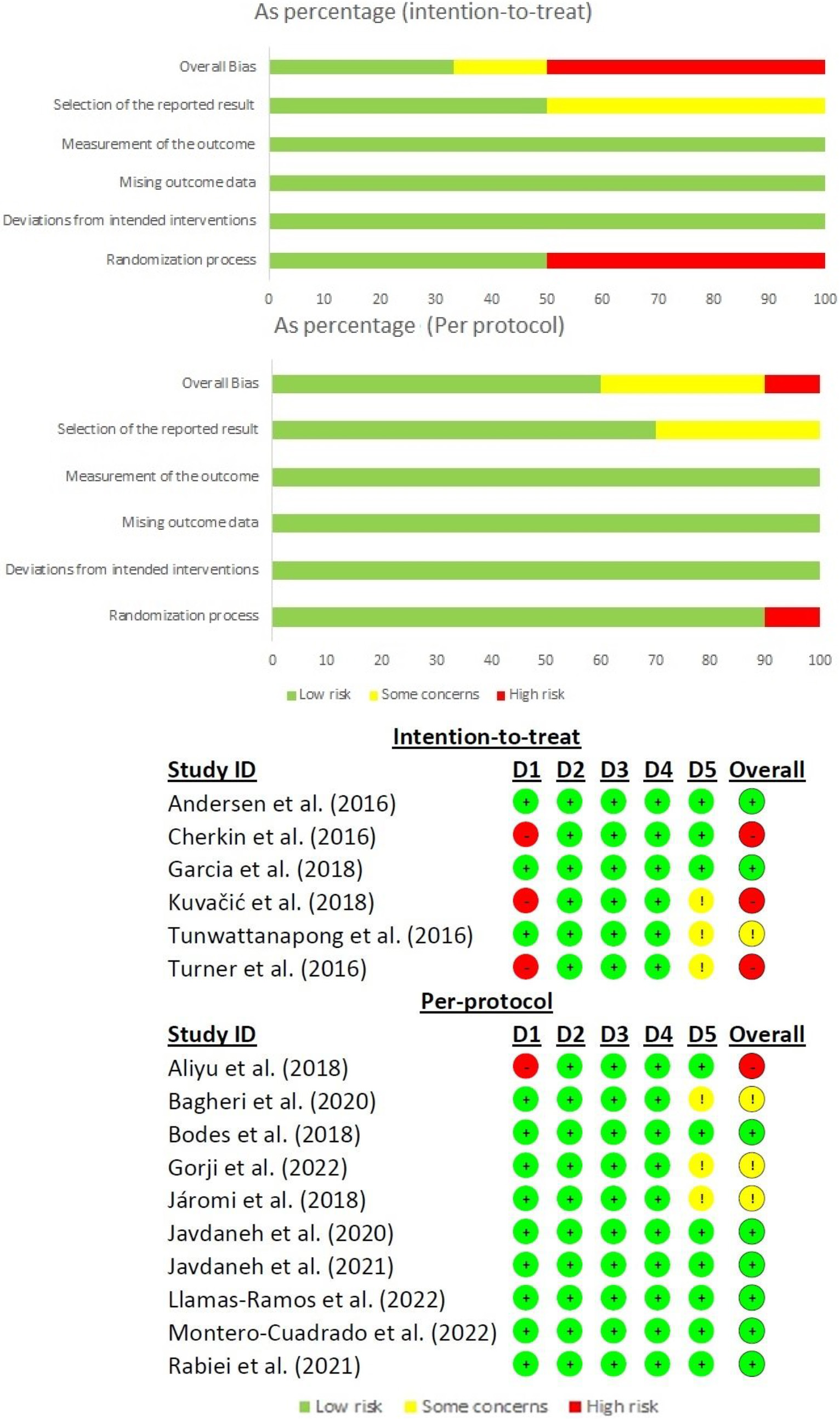
Table 2
Certainty of the evidence (GRADE)
| Outcomes | No of participants (studies) | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | Absolute effect | Certainty of the evidence (GRADE) |
|---|---|---|---|---|---|---|---|---|
| Pain | 1197 (14 RCTs) | Not seriousa | Seriousb | Not serious | Seriousd | Publication bias strongly suspected very strong associationc,e,f,g | SMD | Moderate |
| Disability | 1017 (12 RCTs) | Not seriousa | Seriousb | Not serious | Seriousd | Publication bias strongly suspected very strong associationc,e,f,g | SMD | Moderate |
| Kinesiophobia | 686 (8 RCTs) | Not seriousa | Seriousb | Not serious | Seriousd | Publication bias strongly suspected very strong associationc,e,f,g | SMD | Moderate |
SMD: standardized mean difference. aThe average methodological quality of the studies according to the PEdro scale is good. bLow methodological heterogeneity but high statistical heterogeneity among trials (I2> 25%). cThe Funnel Plot diagram shows possible publication bias and the Egger’s test
Table 3
Characteristics of the studies
| Authors | Pain area | Initial sample (women) | Intervention (final sample) | Supervisor | Weeks | Sessions per week (duration) | Outcome measures | Results |
|---|---|---|---|---|---|---|---|---|
| Aliyu et al. (2018) | NLBP | 37 (56.8%) | G1 ( | PT | 6 | G1: 3 sessions (30’) G2: 2 sessions (30’) | VAS; ODI; FABQ | Both groups showed significant improvements in pain and disability from baseline but not between groups. There were no significant differences in fear between groups. |
| Andersen et al. (2016) | NBP | 141 (not described) | G1 ( | PT | G1: 10 G2: 6 | G1: 3 sessions (50’) G2: 1 session (150’) G3: 1 session (90’) | VAS; WAI; TSK; AC; RTW | All groups showed significant improvements in pain, disability and kinesiophobia from baseline but not between groups. G2 and G3 showed significant improvements in aerobic capacity from baseline but not between groups. All groups show similar patterns of facilitating return-to-work. |
| Bagheri et al. (2020) | NLBP | 40 (100%) | G1 ( | PT | 8 | 3 sessions (60’) | RMDQ; FABQ; ADIM; ASLR | Both groups showed significant improvements in disability from baseline. G1 showed significant improvements in fear and the thickness of the Transversus abdominis muscle during ADIM task from baseline and versus G2. Not significant improvements in ASLR. |
| Bodes et al. (2018) | NLBP | 56 (78.6%) | G1 ( | PT | 12 | 7 sessions (30’–50’) | NRS; PCS; PPT; RMDQ; TSK; PGIC; FFD | Both groups showed significant improvements in pain, disability, kinesiophobia, impression of change and flexibility from baseline. G1 significantly improved all variables versus G2. |
| Cherkin et al. (2016) | NLBP | 342 (65.7%) | G1 ( | PSC | 8 | 1 session (120’) | PB; CPI; RMDQ; PHQ; GAD-2; SF-12 | G1 and G2 showed significant improvements in pain and disability versus G3 at 8, 26 and 52 weeks. G2 showed significant improvements in depression and anxiety versus G1 and G3 at 8 and 26 weeks. G1 and G2 showed significant improvements in the mental component of SF-12 versus G3 at 8 weeks. G2 showed significant improvements in the mental component of SF-12 versus G3 at 26 weeks. |
| Garcia et al. (2018) | NLBP | 148 (76.2%) | G1 ( | PT | 5 | 2 sessions (30’ – 40’) | NRS; RMDQ; PSFS; TSK; GPE | G1 showed significant improvements in pain from baseline and versus G2. There were no significant differences in disability, function and global perceived effect between groups. |
| Gorji et al. (2022) | NLBP | 42 (100%) | G1 ( | PT | 8 | G1: 19 sessions (45’– 60’). G2: 24 sessions (45’– 60’) | VAS; RMDQ; USB; TUG | Both groups significantly improved all outcomes from baseline to post-intervention. G1 showed significant improvements in pain and disability versus G2. |
| Javdaneh et al. (2021) | NNP | 72 (48.6%) | G1 (A | PT | 6 | G1: 1st week, 1 session (60’); 2nd-5th, 1 session (30’–45’) | NPAD; PCS; PSEQ; FABQ | G1 and G2 significantly improved all variables versus G3. G1 showed significant improvements in neck pain and disability, catastrophism and fear versus G2. |
|
Table 3, continued | ||||||||
|---|---|---|---|---|---|---|---|---|
| Authors | Pain area | Initial sample (women) | Intervention (final sample) | Supervisor | Weeks | Sessions per week (duration) | Outcome measures | Results |
| Javdaneh et al. (2020) | NNP | 72 (47.2%) | G1 ( | PT; PSC; Trainer | 6 | G1 and G2: 3 sessions (45’) G3: 1 session | VAS; TSK-17; EMG | G1 and G2 showed significant improvements in pain, kinesiophobia and muscle activity from baseline and versus G3. G2 showed significant improvements in pain, kinesiophobia and muscle activity versus G1. |
| Járomi et al. (2018) | NLBP | 137 (93.4%) | G1 ( | PT | 12 | 2 sessions (60’) | VAS; VET; HET | G1 significantly reduced NLBP and increased the number of properly executed horizontal and vertical patient lifting techniques from baseline and versus G2. |
| Rabiei et al. (2021) | NLBP | 73 (53.4%) | G1 ( | PT | 8 | 2 sessions (30’–60’) | VAS; RMDQ; PSEQ; FABQ | Both groups showed significant improvements in pain, disability, self-efficacy and fear from baseline. G1 showed significant improvements in pain self-efficacy and fear avoidance beliefs versus G2. |
| Kuvačić et al. (2018) | NLBP | 30 (46.7%) | G1 ( | Yoga teacher | 8 | 2 sessions (75’) | NRS; ODI; SDS; SAS | G1 showed significant improvements in pain, depression and anxiety versus G2. Both groups showed improvements in disability from baseline but not between groups. |
| Llamas-Ramos et al. (2022) | NNP | 62 (100%) | G1 ( | Nurse; Social worker; PT | 12 | G1: 4 sessions (90’) | VAS; NDI; ROM; HAND GRIP STRENGTH | G1 demonstrated significant improvements in all the outcomes compared to G2 except total lateral cervical flexion. |
| Montero-Cuadrado et al. (2022) | NBP | 62 (100%) | G1 ( | Nurse; Social worker; PT | 12 | G1: 4 sessions (90’) | VAS; RMDQ; NDI; SF-36; GOLBERG; YESAVAGE; ZARIT; VO2MAX; HAND GRIP STRENGTH | G1 demonstrated significant improvements in all the outcomes compared to G2. |
| Tunwattanapong et al. (2016) [38] | NNP | 96 (90.7%) | G1 ( | Physician | 4 | G1: 5 sessions (10’–15’ twice a day) | VAS; NPNPQ; SF-36 | G1 showed significant improvements in pain and physical dimension of quality of life versus G2. There were no significant differences in the mental dimension of the quality of life between groups |
| Turner et al. (2016) | NLBP | 342 (65.7%) | G1 ( | PSC | 8 | 1 session (120’) | PCS; PSEQ; CPAQ-8. | G1 and G2 showed significant improvements in pain catastrophizing, pain self-efficacy and pain acceptance versus G3. G2 obtained higher results than G1. |
NNP: Non specific neck pain; NLBP: Non specific low back pain; G1: Group 1; G2; Group 2; G3: Group 3; ET: Exercise therapy; HE: Health education; UC: Usual care; PT: Physiotherapist; PSC: Psychologist; NPAD: Neck pain and disability scale; PCS: Pain catastrophizing scale; PSEQ: Patient self-efficacy questionnaire; FABQ: Fear avoidance beliefs questionnaire; VAS: Visual analogue scale; RMDQ: Roland morris disability questionnaire; WAI: Working ability index; TSK: Tampa scale of kinesiophobia; EMG: Electromyography; VET: Vertical lifting technique; HET: Horizontal lifting technique; PB: Pain bothersomeness; NRS: Numeric rating scale; ODI: Oswestry disability index; SDS: Sick-listed status; SAS: Zung self-rating anxiety scale; NPNPQ: Northwick park neck pain questionnaire; SF-36: Short form 36 health survey; CPAQ: The chronic pain acceptance questionnaire; USB: Unipodal static balance; TUG: Timed up and go test.
3.3Participants
A total of 1,814 participants with NBP took part in the 16 studies. Two articles [29, 40] analyzed back pain in all regions, ten studies analyzed [28, 30, 31, 32, 33, 34, 39, 41, 42, 43] it specifically in the lumbar region, four papers [35, 36, 37, 38] analyzed it specifically in the cervical region and none of them analyzed it specifically in the thoracic region. The average age was 49 years and 74.9% of the participants were women (Table 3). It is worth mentioning that the article by Andersen et al. [29] did not report the number of women. Participants only experienced adverse effects in one case and these were minor adverse events [32].
No studies were found that examined effects in participants without NBP; therefore, results relating to primary prevention were not included.
3.4Interventions
The average number of sessions was 20.7, with the most usual number of sessions per intervention being 16 sessions [30, 39, 41, 43]. The mean frequency of sessions per week was four sessions per week, the most common being two sessions per week [28, 33, 34, 41, 43]. Although it is important to mention that there was great diversity in the frequency of sessions per week. The mean duration of the sessions was 57 minutes, with 30–60 minutes being the most common range of session time [28, 30, 31, 33, 34, 35, 36, 39, 41] (Table 3).
The most common exercises were yoga [32, 42, 43], stabilization exercises [28, 29, 30], motor control exercises [31, 34, 35, 36, 39, 41], and strength and stretch trunk exercises [29, 31, 34, 37, 38, 40]. On the other hand, the most common education topics were ergonomics [35, 36, 38, 43], health guidance [29, 33, 34], pain neuroscience education [36, 39, 41] and cognitive behavioral therapy [28, 30, 32, 42]. It is usual for exercise interventions to be structured in warm-up, main part and cool-down. All the interventions are in groups except for two [33, 41], in which they do individualized exercise. No intervention was mainly aimed at primary prevention, as all participants had NBP. These interventions were supervised by physiotherapists in 75% of the studies, and in the other cases, by physicians, psychologists, trainers, or yoga teachers. For more details on each intervention, see Supplementary material III.
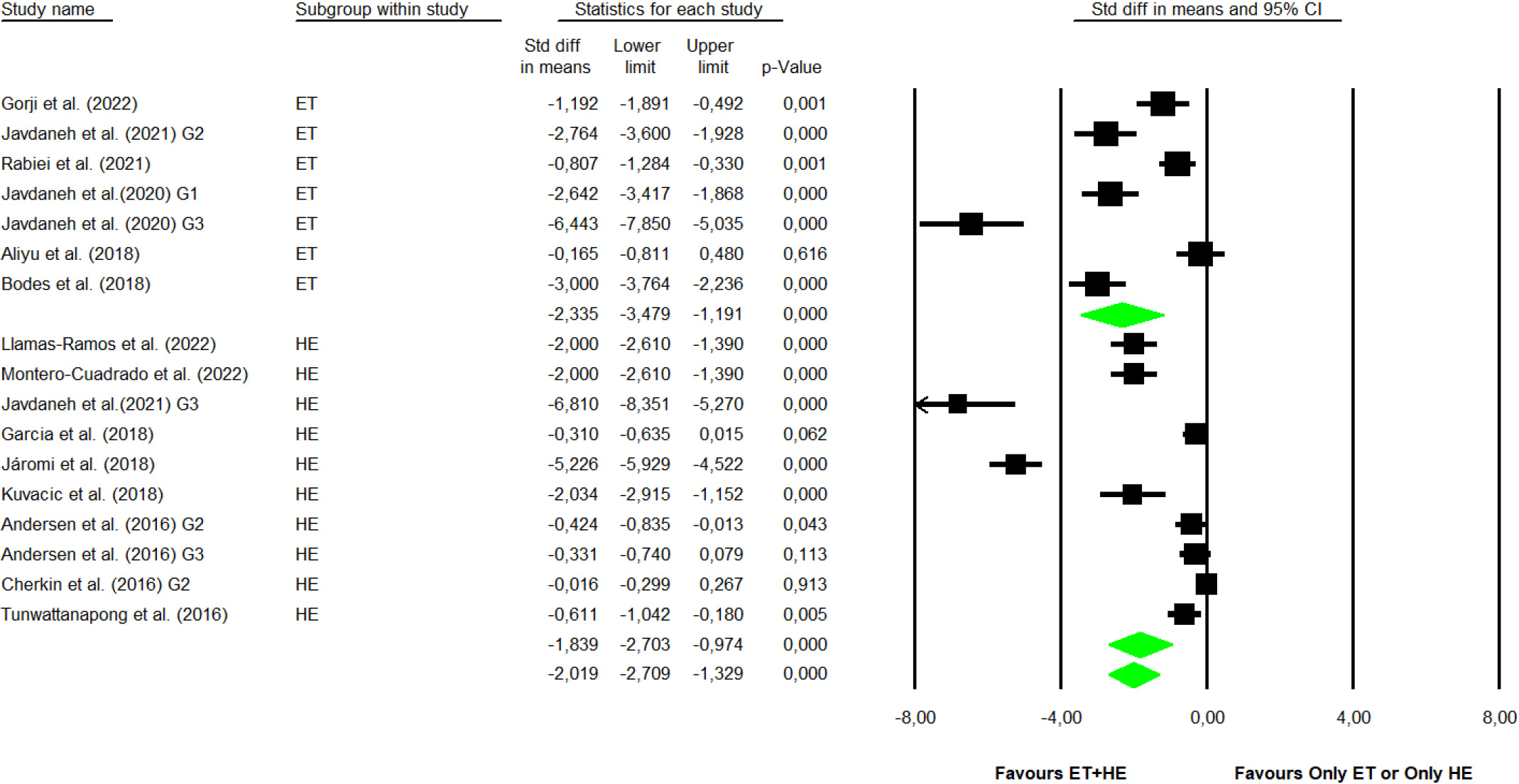
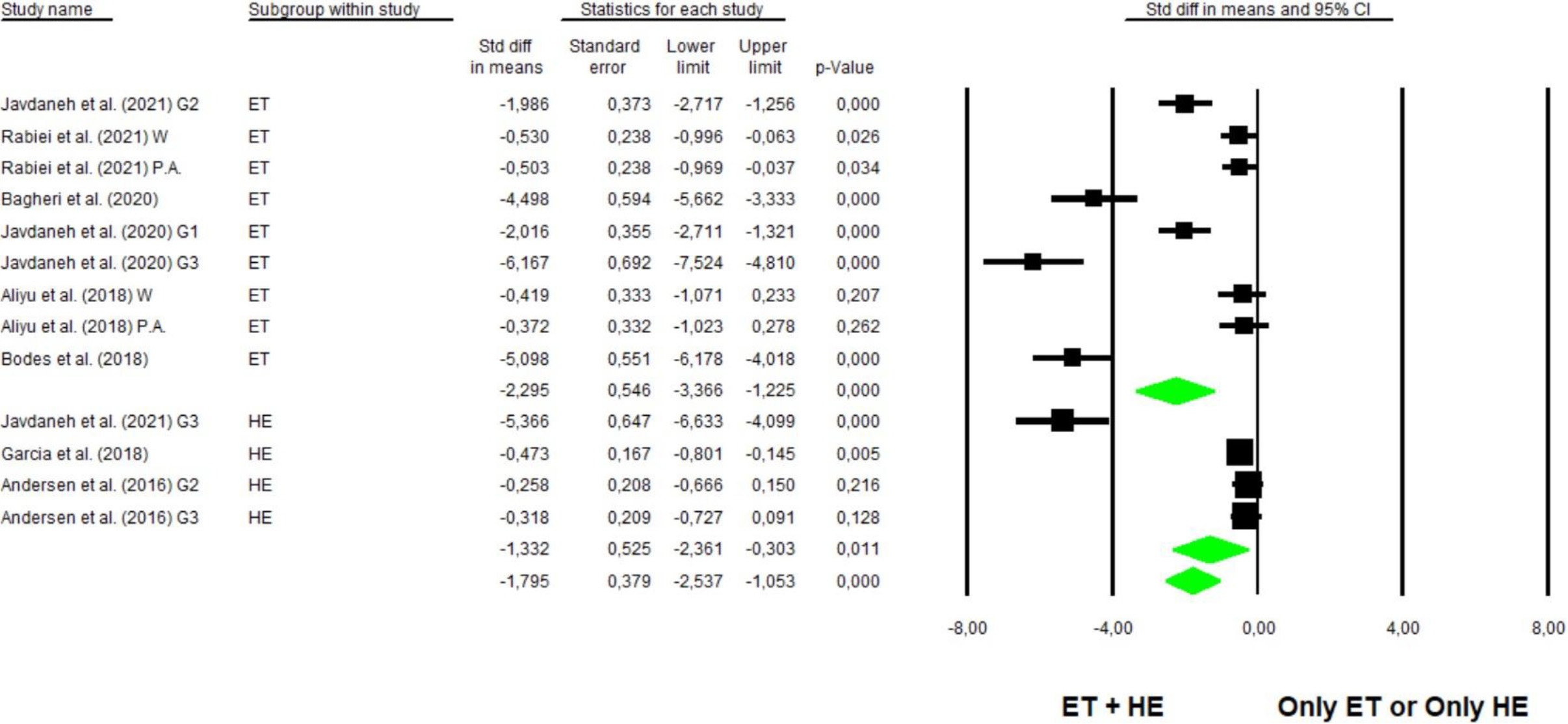
Figure 3.
Forest plot for pain. (ET: Exercise therapy; HE: Health education).
3.5Effects on pain, disability and kinesiophobia
Out of the analyzed studies, 14 of them [28, 29, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 43] analyzed the pain variable. The analysis was divided into two subgroups: exercise therapy plus health education versus isolated exercise therapy or isolated health education. The analysis in the first subgroup indicated a statistically significant decrease in the pain score in the combined group compared to the exercise therapy group with SMD
Figure 4.
Forest plot for disability. (ET: Exercise therapy; HE: Health education).
Out of the analyzed studies, 12 articles [28, 29, 30, 31, 32, 33, 36, 37, 39, 40, 41, 43] analyzed the disability variable. The analysis was divided into two subgroups: exercise therapy plus health education versus isolated exercise therapy or isolated health education. The analysis in the first subgroup indicated a statistically significant decrease in the disability score in the combined group compared to the exercise therapy group with SMD
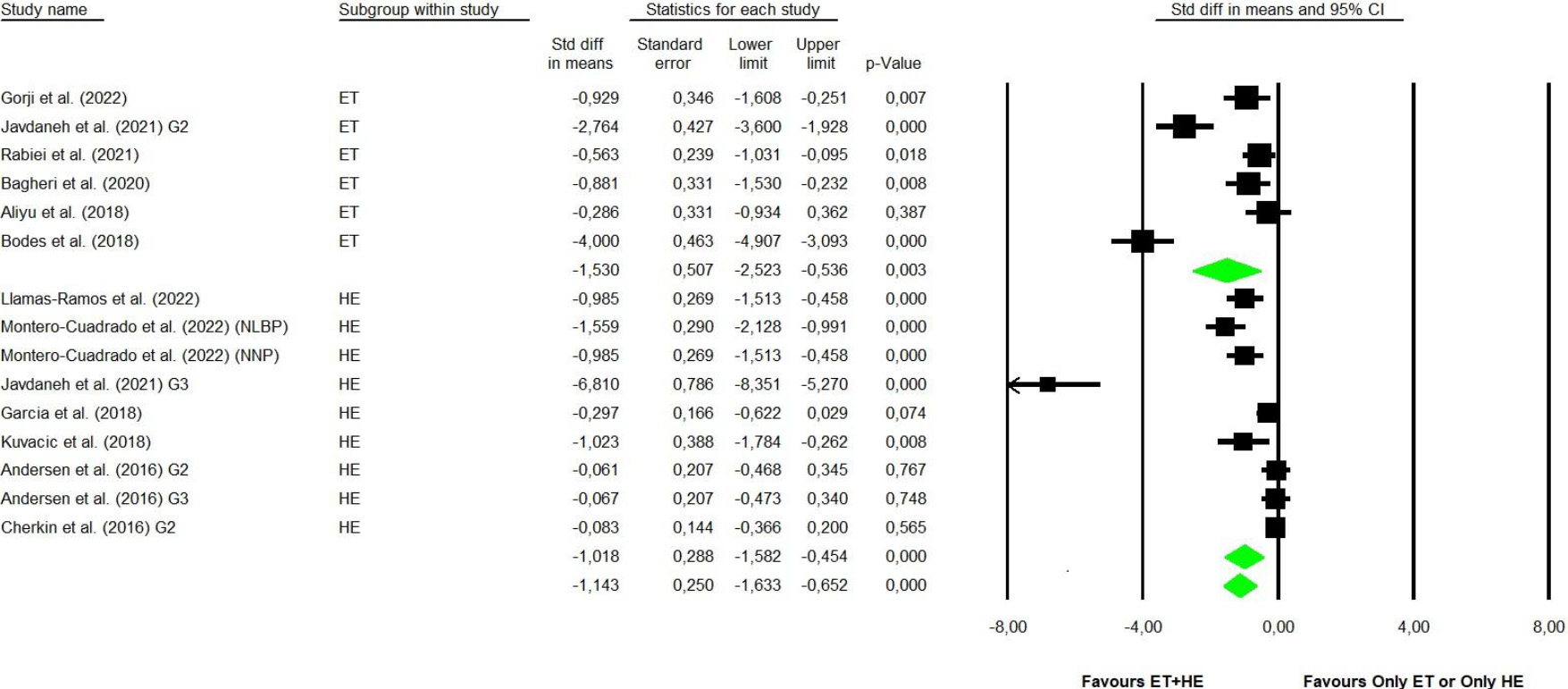
Figure 5.
Forest plot for kinesiophobia. (ET: Exercise therapy; HE: Health education; W: Work related scores; PA: Physical activity related scores).
Out of the analyzed studies, eight articles [28, 29, 30, 31, 33, 35, 36, 41] analyzed the kinesiophobia variable. The analysis was divided into two subgroups: exercise therapy plus health education versus isolated exercise therapy or isolated health education. The analysis in the first subgroup indicated a statistically significant decrease in the kinesiophobia score in the combined group compared to the exercise therapy group with SMD
In addition, subgroup analyses were performed, analyzing the effect on the lumbar and cervical regions separately. Statistically significant improvements were found in both regions in the variables pain (SMD
4.Discussion
The objective of this research was to determine whether the combination of exercise therapy plus health education is more effective for the prevention of NBP than these interventions taken separately. The results suggest that the combination of exercise therapy and health education has a positive effect on the prevention of NBP. Furthermore, the effects on other variables, such as disability or kinesiophobia, were studied. On these other variables, it was also observed that the combination of both is more effective than the isolated implementation of exercise therapy and health education.
The combination of exercise therapy and health education has a strong effect on the pain variable compared to exercise therapy alone or health education alone [31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 43]. Moreover, the pain improved in more than two points. This is a novel and clinically relevant finding [46]. Different reviews have confirmed the benefits of exercise on the prevention of NBP in the lumbar [11, 12, 13, 14] and cervical regions [15, 17, 19, 20]. However, the positive effect of education on NBP prevention remains unclear. The results seem to indicate that theoretical-practical interventions have better results in the prevention of NBP than only practical or theoretical interventions. Perhaps this effect is due to the multifactorial origin of NBP: some risk factors for NBP have a biophysical origin, such as the lack of strength or flexibility of the spinal musculature [47, 48]; other factors have a psychological origin, such as fear or stress, or we can even mention social factors, such as false beliefs about NBP or work-related factors [49, 50].
The disability variable also showed a strong effect in the meta-analysis [28, 29, 30, 31, 32, 33, 36, 37, 39, 40, 41, 43]. This finding is congruent because disability is strongly related to pain [51]. Fundamentally, this is due to the relationship between physical (such as neural activation) and psychosocial (such as motivation) components [51]. Accordingly, Frizziero et al. also identified perceived improvements through exercise in the lumbar region and [19] observed them in the cervical region. Parallel to this, disability is related to kinesiophobia [52]. In fact, patients with NBP and high levels of kinesiophobia have a 41% higher risk of developing disability [52]. A strong effect was also observed in kinesiophobia, with an improvement of SMD more than one point [28, 29, 30, 31, 33, 35, 36, 41]. This phenomenon may be due to the fact that graded exercise and patient education are key elements to reducing kinesiophobia [8]. The International Association for the Study of Pain also establishes a relationship between fear-pain-knowledge, as they state that pain not only represents the sensation of physical harm, but also an emotional experience that can be influenced by other emotions, such as anxiety or fear of the unknown [53]. In fact, it has already been identified that benefits in the pain level, disability and kinesiophobia are maintained up to three months after the end of the intervention [31]. However, these effects do not seem to be maintained in the long term [32, 42].
Currently, the biopsychosocial model is the most recommended paradigm for the treatment and prevention of NBP [54]. Therefore, the latest NBP clinical intervention guideline published in 2021 recommends exercise and education as key elements in NBP clinical interventions [7]. Different types of exercise and health education programmes have been included in this review which could affect the specificity of the results. Although, different authors conclude that the important aspect is to exercise regardless of the type of exercise [55, 56], and in terms of educational interventions, all of them followed the recommendations of the main clinical guidelines [7, 8].
It should be noted that this is the first meta-analysis analyzing the effects of the combination of exercise therapy and health education compared to exercise therapy alone or health education alone for the prevention of NBP.
Among the limitations of the present research, the authors must acknowledge that they have not taken into account analyses differentiated by gender and age subgroups, nor have they included studies comparing the combination of exercise and education with the usual medical care or with passive physiotherapy interventions.
However, it is worth mentioning that, due to the high heterogeneity in the analyzed studies, it has not been possible to establish which exercise and education interventions are the most effective, as well as the most appropriate frequency and duration of sessions. The mix of different exercise programmes and health education strategies may affected the specificity of the conclusions. In addition, studies were not found that assessed the intervention on primary prevention. There are also no articles that analyze dorsal back pain and only six articles analyze neck pain. In view of the above, further research is needed to compare the effects of different interventions with the aim of developing specific NBP prevention protocols.
5.Conclusions
Interventions that combine exercise and education seem to have a greater preventive effect on NBP than those that include exercise or education in an isolated manner. Furthermore, combining exercise with educational interventions improves disability and kinesiophobia more than if implemented separately. The results obtained can help healthcare professionals to increase the efficiency of their clinical interventions and thus reduce the serious socioeconomic impact caused by NBP worldwide.
Author contributions
P. H.-L., R. L.-R., J. L.-B., and J. L.G.-S. conceptualized and designed the study, drafted the initial manuscript, designed the data collection instruments, collected data, carried out the initial analyses, and critically reviewed the manuscript for important intellectual content. All authors read and agreed to the published version of the manuscript.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author (P. H-L.) upon reasonable request.
Ethical approval
Not applicable.
Funding
The study was supported by the Professional College of Physiotherapists of Castilla y León, Salamanca, Spain (grant number: INV2023-38).
Informed consent
Not applicable.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-230252.
Acknowledgments
None to report.
Conflict of interest
The authors declare that there is no conflict of interest.
References
[1] | James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. (2018) Nov; 392: (10159): 1789-858. |
[2] | Bartys S, Frederiksen P, Bendix T, Burton K. System influences on work disability due to low back pain: An international evidence synthesis. Health Policy. (2017) Aug; 121: (8): 903-12. |
[3] | Dagenais S, Caro J, Haldeman S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. (2008) Jan; 8: (1): 8-20. |
[4] | Maniadakis N, Gray A. The economic burden of back pain in the UK. Pain. (2000) Jan 1; 84: (1): 95-103. |
[5] | Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: evidence, challenges, and promising directions. The Lancet. (2018) Jun; 391: (10137): 2368-83. |
[6] | Baumann LC, Ylinen A. Prevention: Primary, secondary, tertiary. In: Encyclopedia of behavioral medicine. Springer. (2020) ; 1738-40. |
[7] | Corp N, Mansell G, Stynes S, Wynne-Jones G, Morsø L, Hill JC, et al. Evidence-based treatment recommendations for neck and low back pain across Europe: A systematic review of guidelines. Eur J Pain. (2021) Feb; 25: (2): 275-95. |
[8] | George SZ, Fritz JM, Silfies SP, Schneider MJ, Beneciuk JM, Lentz TA, et al. Interventions for the Management of Acute and Chronic Low Back Pain: Revision 2021: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability and Health From the Academy of Orthopaedic Physical Therapy of the American Physical Therapy Association. J Orthop Sports Phys Ther. (2021) Nov; 51: (11): CPG1-60. |
[9] | Hurwitz EL, Randhawa K, Yu H, Côté P, Haldeman S. The Global Spine Care Initiative: a summary of the global burden of low back and neck pain studies. Eur Spine J. (2018) Sep; 27: (S6): 796-801. |
[10] | Miyamoto GC, Lin CWC, Cabral CMN, van Dongen JM, van Tulder MW. Cost-effectiveness of exercise therapy in the treatment of non-specific neck pain and low back pain: a systematic review with meta-analysis. Br J Sports Med. (2019) Feb; 53: (3): 172-81. |
[11] | Domingues de Freitas C, Costa DA, Junior NC, Civile VT. Effects of the pilates method on kinesiophobia associated with chronic non-specific low back pain: Systematic review and meta-analysis. J Bodyw Mov Ther. (2020) Jul; 24: (3): 300-6. |
[12] | Frizziero A, Pellizzon G, Vittadini F, Bigliardi D, Costantino C. Efficacy of Core Stability in Non-Specific Chronic Low Back Pain. J Funct Morphol Kinesiol. (2021) Apr 22; 6: (2): 37. |
[13] | Hayden JA, Wilson MN, Stewart S, Cartwright JL, Smith AO, Riley RD, et al. Exercise treatment effect modifiers in persistent low back pain: an individual participant data meta-analysis of 3514 participants from 27 randomised controlled trials. Br J Sports Med. (2020) Nov; 54: (21): 1277-8. |
[14] | Hayden JA, Ellis J, Ogilvie R, Malmivaara A, van Tulder MW. Exercise therapy for chronic low back pain. Cochrane Back and Neck Group, editor. Cochrane Database Syst Rev [Internet]. (2021) Sep 28 [cited 2022 Jan 3]; 2021: (10). Available from: doi: 10.1002/14651858.CD009790.pub2. |
[15] | Arimi SA, Bandpei MAM, Javanshir K, Rezasoltani A, Biglarian A. The effect of different exercise programs on size and function of deep cervical flexor muscles in patients with chronic nonspecific neck pain: a systematic review of randomized controlled trials. Am J Phys Med Rehabil. (2017) ; 96: (8): 582-8. |
[16] | Cheng CH, Su HT, Yen LW, Liu WY, Cheng HYK. Long-term effects of therapeutic exercise on nonspecific chronic neck pain: a literature review. J Phys Ther Sci. (2015) ; 27: (4): 1271-6. |
[17] | Gross A, Kay TM, Paquin JP, Blanchette S, Lalonde P, Christie T, et al. Exercises for mechanical neck disorders. Cochrane Back and Neck Group, editor. Cochrane Database Syst Rev [Internet]. (2015) Jan 28 [cited 2022 Jan 3]; Available from: doi: 10.1002/14651858.CD004250.pub5.: |
[18] | Kay TM, Gross A, Goldsmith CH, Rutherford S, Voth S, Hoving JL, et al. Exercises for mechanical neck disorders. Cochrane Database Syst Rev. (2012) Aug 15; CD004250.pub4. |
[19] | O’Riordan C, Clifford A, Van De Ven P, Nelson J. Chronic Neck Pain and Exercise Interventions: Frequency, Intensity, Time, and Type Principle. Arch Phys Med Rehabil. (2014) Apr; 95: (4): 770-83. |
[20] | Sihawong R, Janwantanakul P, Sitthipornvorakul E, Pensri P. Exercise Therapy for Office Workers With Nonspecific Neck Pain: A Systematic Review. J Manipulative Physiol Ther. (2011) Jan; 34: (1): 62-71. |
[21] | Jones CM, Shaheed CA, Ferreira GE, Kharel P, Christine Lin CW, Maher CG. Advice and education provide small short-term improvements in pain and disability in people with non-specific spinal pain: a systematic review. J Physiother. (2021) Oct; 67: (4): 263-70. |
[22] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) Mar 29; n71. |
[23] | Ardern CL, Büttner F, Andrade R, Weir A, Ashe MC, Holden S, et al. Implementing the 27 PRISMA 2020 Statement items for systematic reviews in the sport and exercise medicine, musculoskeletal rehabilitation and sports science fields: the PERSiST (implementing Prisma in Exercise, Rehabilitation, Sport medicine and SporTs science) guidance. Br J Sports Med. (2022) Feb; 56: (4): 175-95. |
[24] | Cumpston M, Li T, Page MJ, Chandler J, Welch VA, Higgins JP, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. (2019) ; 10: (ED000142). |
[25] | Higgins JP, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, et al. Cochrane handbook for systematic reviews of interventions. John Wiley & Sons. (2019) . |
[26] | Ferguson CJ. An effect size primer: A guide for clinicians and researchers. Prof Psychol Res Pract. (2009) Oct; 40: (5): 532-8. |
[27] | Cicchetti DV. Assessing Inter-Rater Reliability for Rating Scales: Resolving some Basic Issues. Br J Psychiatry. (1976) Nov; 129: (5): 452-6. |
[28] | Aliyu FY, Wasiu AA, Bello B. Effects of a combined lumbar stabilization exercise and cognitive behavioral therapy on selected variables of individuals with non-specific low back pain: A randomized clinical trial. Fisioterapia. (2018) Sep; 40: (5): 257-64. |
[29] | Andersen L, Juul-Kristensen B, Sørensen T, Herborg L, Roessler K, Søgaard K. Longer term follow-up on effects of Tailored Physical Activity or Chronic Pain Self-Management Programme on return-to-work: A randomized controlled trial. J Rehabil Med. (2016) ; 48: (10): 887-92. |
[30] | Bagheri R, Hedayati R, Ehsani F, Hemati-Boruojeni N, Abri A, Taghizadeh Delkhosh C. Cognitive behavioral therapy with stabilization exercises affects transverse abdominis muscle thickness in patients with chronic low back pain: A double-blinded randomized trial study. J Manipulative Physiol Ther. (2020) Jun; 43: (5): 418-28. |
[31] | Bodes Pardo G, Lluch Girbés E, Roussel NA, Gallego Izquierdo T, Jiménez Penick V, Pecos Martín D. pain neurophysiology education and therapeutic exercise for patients with chronic low back pain: A single-blind randomized controlled trial. Arch Phys Med Rehabil. (2018) Feb; 99: (2): 338-47. |
[32] | Cherkin DC, Sherman KJ, Balderson BH, Cook AJ, Anderson ML, Hawkes RJ, et al. Effect of mindfulness-based stress reduction vs cognitive behavioral therapy or usual care on back pain and functional limitations in adults with chronic low back pain: A randomized clinical trial. JAMA. (2016) Mar 22; 315: (12): 1240. |
[33] | Garcia AN, Costa L da CM, Hancock MJ, Souza FS de, Gomes GVF de O, Almeida MO de, et al. McKenzie Method of Mechanical Diagnosis and Therapy was slightly more effective than placebo for pain, but not for disability, in patients with chronic non-specific low back pain: a randomised placebo controlled trial with short and longer term follow-up. Br J Sports Med. (2018) May; 52: (9): 594-600. |
[34] | Jaromi M, Kukla A, Szilagyi B, Simon-Ugron A, Bobaly VK, Makai A, et al. Back School programme for nurses has reduced low back pain levels: A randomised controlled trial. J Clin Nurs. (2018) Mar; 27: (5-6): E895-902. |
[35] | Javdaneh N, Letafatkar A, Shojaedin S, Hadadnezhad M. Scapular exercise combined with cognitive functional therapy is more effective at reducing chronic neck pain and kinesiophobia than scapular exercise alone: a randomized controlled trial. Clin Rehabil. (2020) Dec; 34: (12): 1485-96. |
[36] | Javdaneh N, Saeterbakken AH, Shams A, Barati AH. Pain neuroscience education combined with therapeutic exercises provides added benefit in the treatment of chronic neck pain. Int J Environ Res Public Health. (2021) Aug 22; 18: (16): 8848. |
[37] | Llamas-Ramos R, Barrero-Santiago L, Llamas-Ramos I, Montero-Cuadrado F. Effects of a family caregiver care programme in musculoskeletal pain and disability in the shoulder-neck region – A randomised clinical trial. Int J Environ Res Public Health. (2023) ; 20: (1): 376. |
[38] | Tunwattanapong P, Kongkasuwan R, Kuptniratsaikul V. The effectiveness of a neck and shoulder stretching exercise program among office workers with neck pain: a randomized controlled trial. Clin Rehabil. (2016) Jan; 30: (1): 64-72. |
[39] | Gorji SM, Mohammadi Nia Samakosh H, Watt P, Henrique Marchetti P, Oliveira R. Pain neuroscience education and motor control exercises versus core stability exercises on pain, disability, and balance in women with chronic low back pain. Int J Environ Res Public Health. (2022) ; 19: (5): 2694. |
[40] | Montero-Cuadrado F, Barrero-Santiago L, Llamas-Ramos R, Llamas-Ramos I. Musculoskeletal pain in family caregivers: Does a therapeutic physical program in primary care work? A randomized controlled trial. Int J Environ Res Public Health. (2022) ; 20: (1): 185. |
[41] | Rabiei P, Sheikhi B, Letafatkar A. Comparing pain neuroscience education followed by motor control exercises with group-based exercises for chronic low back pain: A randomized controlled trial. Pain Pract. (2021) Mar; 21: (3): 333-42. |
[42] | Turner JA, Anderson ML, Balderson BH, Cook AJ, Sherman KJ, Cherkin DC. Mindfulness-based stress reduction and cognitive behavioral therapy for chronic low back pain: similar effects on mindfulness, catastrophizing, self-efficacy, and acceptance in a randomized controlled trial. Pain. (2016) Nov; 157: (11): 2434-44. |
[43] | Kuvačić G, Fratini P, Padulo J, Antonio DI, De Giorgio A. Effectiveness of yoga and educational intervention on disability, anxiety, depression, and pain in people with CLBP: A randomized controlled trial. Complement Ther Clin Pract. (2018) May; 31262-7. |
[44] | Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Phys Ther. (2003) Aug 1; 83: (8): 713-21. |
[45] | Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. Bmj. (2008) ; 336: (7650): 924-6. |
[46] | van der Roer N, Ostelo RWJG, Bekkering GE, van Tulder MW, de Vet HCW. Minimal clinically important change for pain intensity, functional status, and general health status in patients with nonspecific low back pain: Spine. (2006) Mar; 31: (5): 578-82. |
[47] | Behennah J, Conway R, Fisher J, Osborne N, Steele J. The relationship between balance performance, lumbar extension strength, trunk extension endurance, and pain in participants with chronic low back pain, and those without. Clin Biomech. (2018) ; 5322-30. |
[48] | França FR, Burke TN, Caffaro RR, Ramos LA, Marques AP. Effects of muscular stretching and segmental stabilization on functional disability and pain in patients with chronic low back pain: a randomized, controlled trial. J Manipulative Physiol Ther. (2012) ; 35: (4): 279-85. |
[49] | Pincus T, Burton AK, Vogel S, Field AP. A systematic review of psychological factors as predictors of chronicity/disability in prospective cohorts of low back pain. Prim Care. 12. |
[50] | Shiri R, Falah-Hassani K, Heliövaara M, Solovieva S, Amiri S, Lallukka T, et al. Risk factors for low back pain: A population-based longitudinal study. Arthritis Care Res. (2019) Feb; 71: (2): 290-9. |
[51] | Arnstein P, Caudill M, Mandle CL, Norris A, Beasley R. Self efficacy as a mediator of the relationship between pain intensity, disability and depression in chronic pain patients. Pain. (1999) Apr 1; 80: (3): 483-91. |
[52] | Trocoli TO, Botelho RV. Prevalence of anxiety, depression and kinesiophobia in patients with low back pain and their association with the symptoms of low back spinal pain. Rev Bras Reumatol Engl Ed. (2016) Jul; 56: (4): 330-6. |
[53] | Raja SN, Carr DB, Cohen M, Finnerup NB, Flor H, Gibson S, et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. (2020) Sep; 161: (9): 1976-82. |
[54] | Knezevic NN, Candido KD, Vlaeyen JWS, Van Zundert J, Cohen SP. Low back pain. The Lancet. (2021) Jul; 398: (10294): 78-92. |
[55] | Van Middelkoop M, Rubinstein SM, Verhagen AP, Ostelo RW, Koes BW, van Tulder MW. Exercise therapy for chronic nonspecific low-back pain. Best Pract Res Clin Rheumatol. (2010) ; 24: (2): 193-204. |
[56] | Hayden JA, Van Tulder MW, Malmivaara AV, Koes BW. Meta-analysis: exercise therapy for nonspecific low back pain. Ann Intern Med. (2005) ; 142: (9): 765-75. |


