
Sustained versus repetitive standing trunk extension results in greater spinal growth and pain improvement in back pain:A randomized clinical trial
Abstract
BACKGROUND:
McKenzie standing trunk extension exercises have been used for the management of low back pain (LBP). However, no study to date has investigated the effect of standing trunk extension postures on spinal height and clinical outcomes.
OBJECTIVE:
To evaluate in subjects with LBP following a period of trunk loading how spinal height, pain, symptoms’ centralization and function outcome measures respond to two standing postures interventions: (1) repetitive trunk extension (RTE) and (2) sustained trunk extension (STE).
METHODS:
A consecutive sample of convenience of people with LBP were recruited to participate in 2-session physical therapy using either RTE or STE in standing.
RESULTS:
Thirty participants (18 women) with a mean age of 53
CONCLUSION:
People with LBP experienced greater spine growth and improvements of pain during standing STE as compared to RTE. People with LBP could use such postures and movements to alleviate their LBP and improve spine height while in a weight bearing position.
1.Background
According to the United States Department of Labor, there were more than one million injuries and illnesses requiring days away from work amongst private industry, state and local government employees. Among these injuries and illnesses, 16.6% were low back related equating to 191,479 low back injuries requiring days away from work [1].
The American College of Physicians and the American Pain Society classified low back pain (LBP) into three categories: (1) nonspecific LBP; (2) LBP potentially associated with radiculopathy or spinal stenosis; and (3) LBP potentially associated with another specific spinal cause. Of these three, lumbar intervertebral disc (IVD) herniation is one of the most common spinal degenerative disorders leading to LBP associated with radiculopathy [2, 3, 4]. In order to better understand the IVD’s role in the development or persistence of LBP and spinal stenosis, there have been many stadiometric studies primarily focused on lumbar spinal height changes associated with various positions and movements [6, 7, 8]. These studies were designed to investigate if spinal height could be restored following spinal shrinkage using various postures. Natural IVD height preservation is so important that the biomedical field has examined the use of growth factors for IVD biologic regeneration [9]. This was done to more naturally preserve IVD biomechanical and physiological function as opposed to surgical disruption.
People spend about 61% of time standing in the work and home environment [1]. Although prolonged weight bearing postures, such as standing and walking, have been associated with decreased spine height [10, 11] some studies reported that seated weight bearing postures could result in spine height gain [12]. Sustained and repetitive lumbar extension postures frequently occur after periods of prolonged unloading such as sleep. These extension postures are periodically repeated throughout the day during activities such as standing and walking [1]. People presenting with directional preferences that include lumbar extension tend to respond well to exercises geared toward trunk extension [13, 14, 15]. Significant and rapid changes in central and distal pain intensity and location have resulted from standing end range trunk extension in patients with low back and referred pain [16]. Additional studies reported that standing back extension exercises resulted in back pain episodes’ prevention and decreased back pain in care workers [17, 18]. Standing exercises have the advantage to be functional and easily performed in work and home settings [19].
Lumbar extension range of motion (ROM) is positively correlated with symptoms’ centralization in LBP patients [20]. Clinicians assess symptoms’ centralization, which refers to symptoms retreating towards the spine midline in response to repeated movements or guided positioning [21, 22]. The operational definition and measurement techniques for centralization have been laid out in several studies [23, 24]. Several methods have been used to increase spinal ROM including static, repeated, passive postures, and proprioceptive neuromuscular facilitation. Both standing and prone lumbar extension postures are effective for treating low back dysfunction syndrome [25]. However, which method is best suited for increasing spinal ROM remains debated [26, 27]. One author found static prone postures to increase ROM more effectively with 30–60 second sustained postures as compared to 15-second postures, but no difference between the effectiveness of 30-second and 60-second postures [28, 29]. Additionally, patients with LBP chose to perform their extension posture for home exercise in standing 80.8% of the time and only 19.2% of the time in the prone position, resulting in similar clinical outcomes where both groups showed equal improvements in lumbar extension ROM [30].
Previous studies investigated the effects of postures and movements in lying (unloaded) or seated positions on spinal height (Owens 2009, Gerke, et al. 2010; Pape 2018). These studies primarily focused on spinal height following static patient positioning and showed that both the lying and supported seated positions resulted in mean spinal height gains of 2 to 5 mm. However, most rehabilitation programs focused on LBP prevention and management use both repetitive and/or sustained spinal extension exercises to improve patients’ outcomes [32, 33]. Such exercises can be performed in lying or standing position. Although patients with acute and recurrent low back and referred pain tend to respond well to directional preference postures [34], subjects with chronic symptoms tend to display greater signs of sensitization, biopsychosocial issues [35], and tend to respond less favorably to directional preferences postures and exercises [36].
No study to date has investigated the effects of standing extension postures on spinal height, pain, centralization and function. Therefore, the purposes of this study will be to evaluate in a sample of LBP patients the effect of standing trunk extension, both sustained and repetitive, following a period of spinal loading, on (1) spinal height; (2) pain; (3) symptoms centralization and (4) functional measures. The results of this study could impact rehabilitation programs that could use standing trunk extension postures at home or in the work environment to grow and/or prevent spinal shrinkage.
2.Methods
2.1Research design(s)
A pre-test, post-test comparison group design (randomized clinical trial) was used to determine how spinal height changes in response to standing sustained trunk extension (STE) and repetitive trunk extension (RTE) after a period of spinal loading. The study used a 2 (between subjects – type of trunk extension: sustained vs. repetitive)
2.2Power analysis – sample size
Power calculations were performed to determine the sample size required for the study using the spinal height change as the primary outcome measure. The study was designed with the
2.3Pre-study approvals
The Texas Tech University Health Sciences Center Institutional Review Board (IRB) approved this study (L19-024). The trial was registered at https://clinicaltrials.gov (NCT03785457) prior to the start of data collection in January 2019. This was followed by stadiometric instrument reliability testing, with the first subject entering the study in January 2020 and data collection ending January 2022.
2.4Subjects/specimens
Systematic consecutive sampling of 35 subjects with musculoskeletal LBP were recruited from physician offices, Sports medicine and Physical therapy clinic and the general Fredericksburg community and surrounding areas Our recruitment was inclusive of LBP subjects that demonstrated a directional preference toward trunk extension, regardless of the chronicity of symptoms to increase the external validity of the findings.
• Inclusion Criteria were: (1) Ability and willingness to come twice to the physical therapy clinic for approximately 60 minutes each; (2) Subjects with LBP and directional preference in back extension; (3) Age 18–80 [38]; (4) Ability to stand for 5 minutes; (5) Ability to sit for 10 minutes; and (6) Low back pain on Numerical Pain Rating scale (NPRS) of at least 2/10 and less or equal to 9/10 [39].
• Exclusion Criteria were: (1) Pregnancy by subject report; (2) history of back surgery or spinal fractures within the last six months; (3) history of spinal fusion or physician’s diagnosis of spinal instability; (4) current history of acute systemic infection, active inflammatory disease, or malignancy; and (5) subjects engaged in legal/compensation claims for their back symptoms.
Figure 1.
Consort chart.
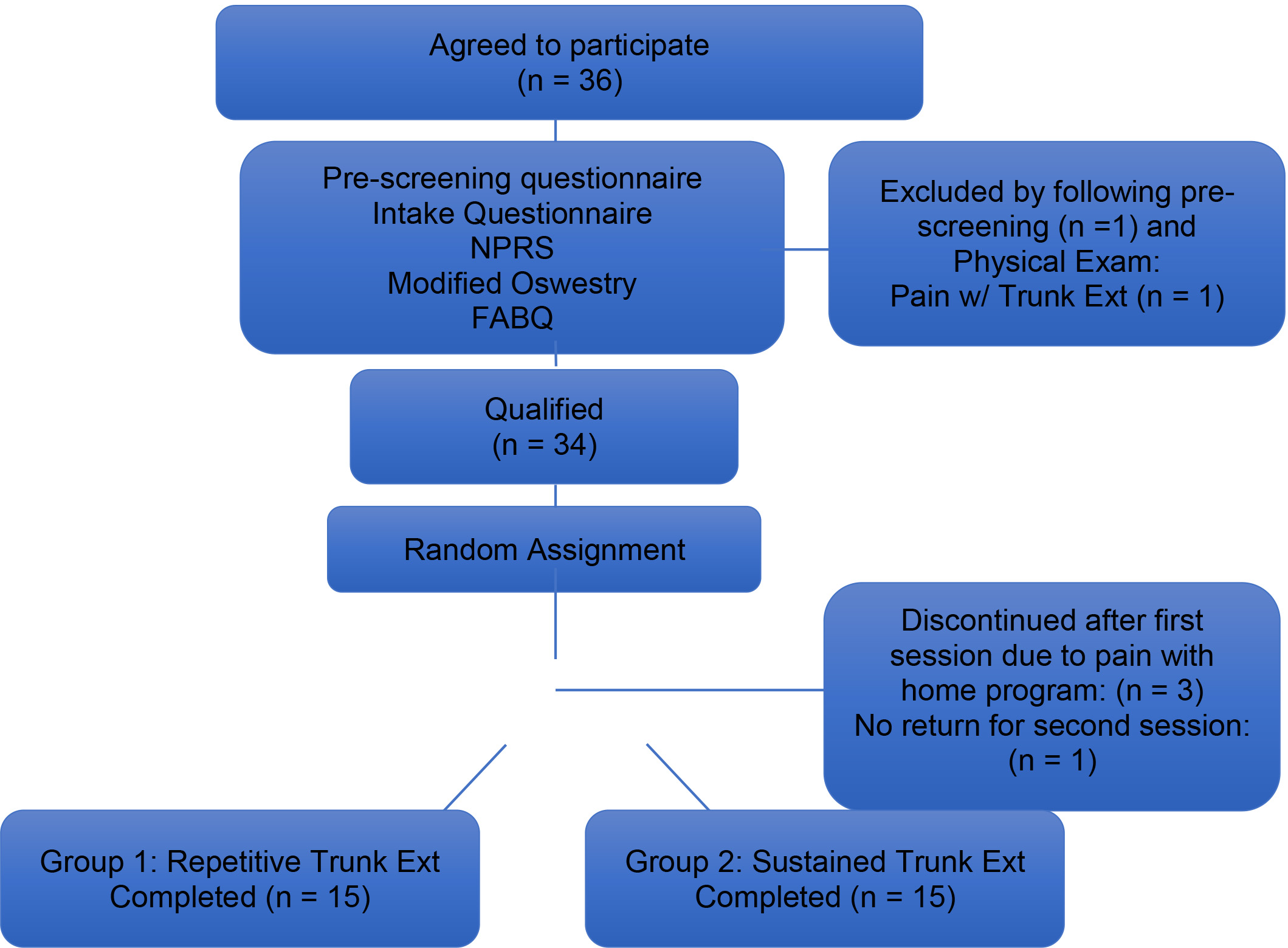
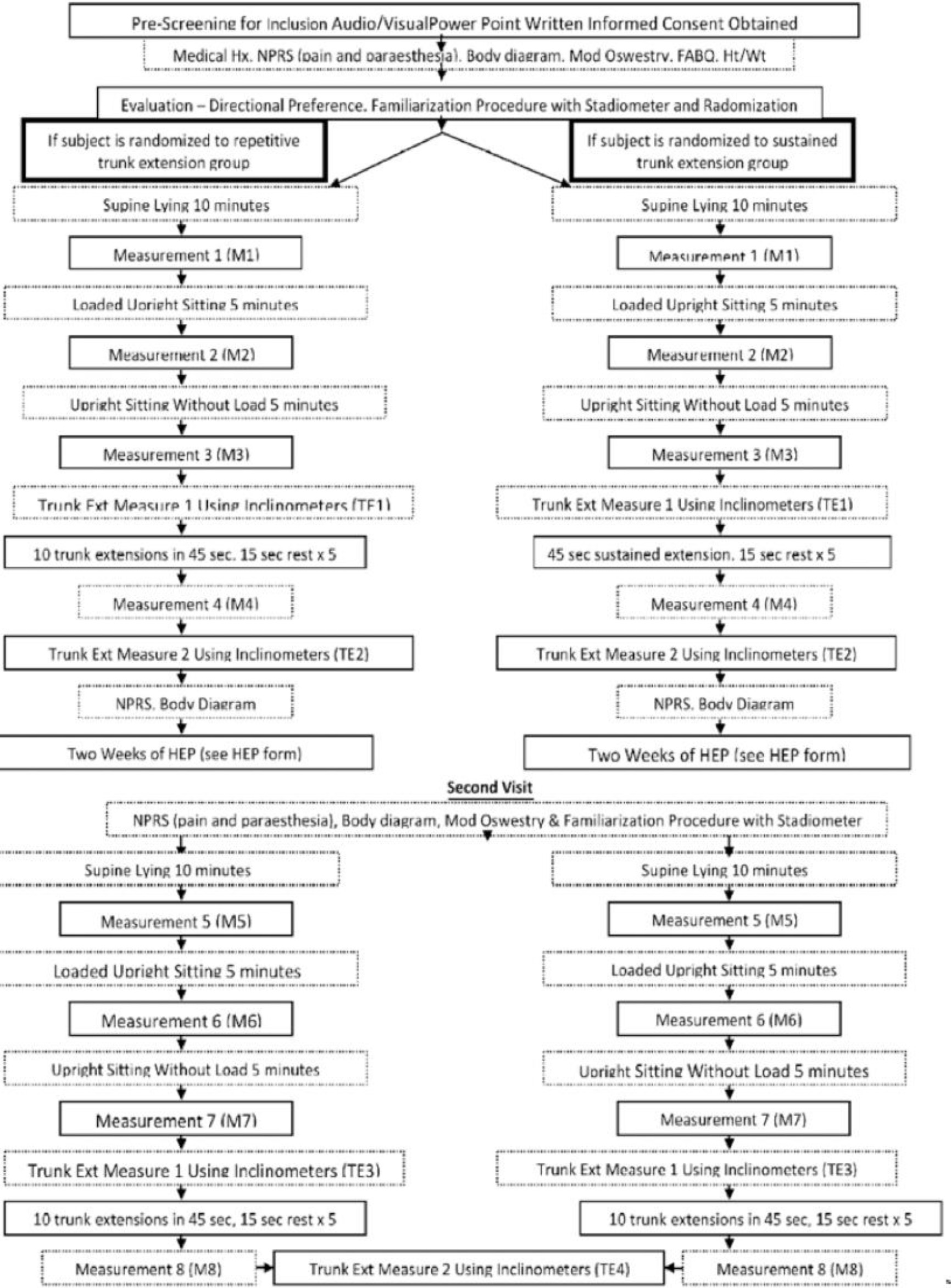
Figure 2.
Flow chart of test positions and testing sequence.
2.5Testing sequence
Subjects attended two physical therapy sessions to complete the study.
2.5.1Session 1
Each participant watched an audio-visual power point presentation explaining the study, test procedures and including a video describing the interventions (standing RTE and standing STE). Written informed consent was obtained. To determine directional preference, the principal investigator (JH) used the guidelines set forth in the directional preference definition [40] and based off of standards set forth in randomized clinical trials [41]. A questionnaire including pertinent medical history was completed. Participants completed (1) a Numerical Pain Rating Scale (NPRS) to rate their current, minimum, maximum and average LBP over the last two days [39] as well as paresthesia signs/symptoms intensity; (2) Body Diagram for indicating location of symptoms; (3) Modified Oswestry LBP questionnaire [42]; (4) Fear Avoidance Belief Questionnaire [43] (Fig. 1). A researcher recorded participant’s height and weight. A Flow chart illustrates study sequence in details (Fig. 2).
Participants meeting the criteria for study inclusion completed a familiarization procedure to determine the consistency to reposition themselves in the stadiometer. Participants able to reposition themselves in the stadiometer with a SD of 1.3 mm or less for five consecutive measurements [31, 32, 44] were included in the study. The stadiometer digital display was covered to blind the researcher performing the measurements.
Figure 3.
Starting position for trunk extensions; B: End position for sustained trunk extension that was held for 45 seconds and repeated 5 times (sustained trunk extension group), and for repetitive trunk extensions that were repeated 10 times for a period of 45 seconds followed by 15 seconds break (repetitive trunk extension group).

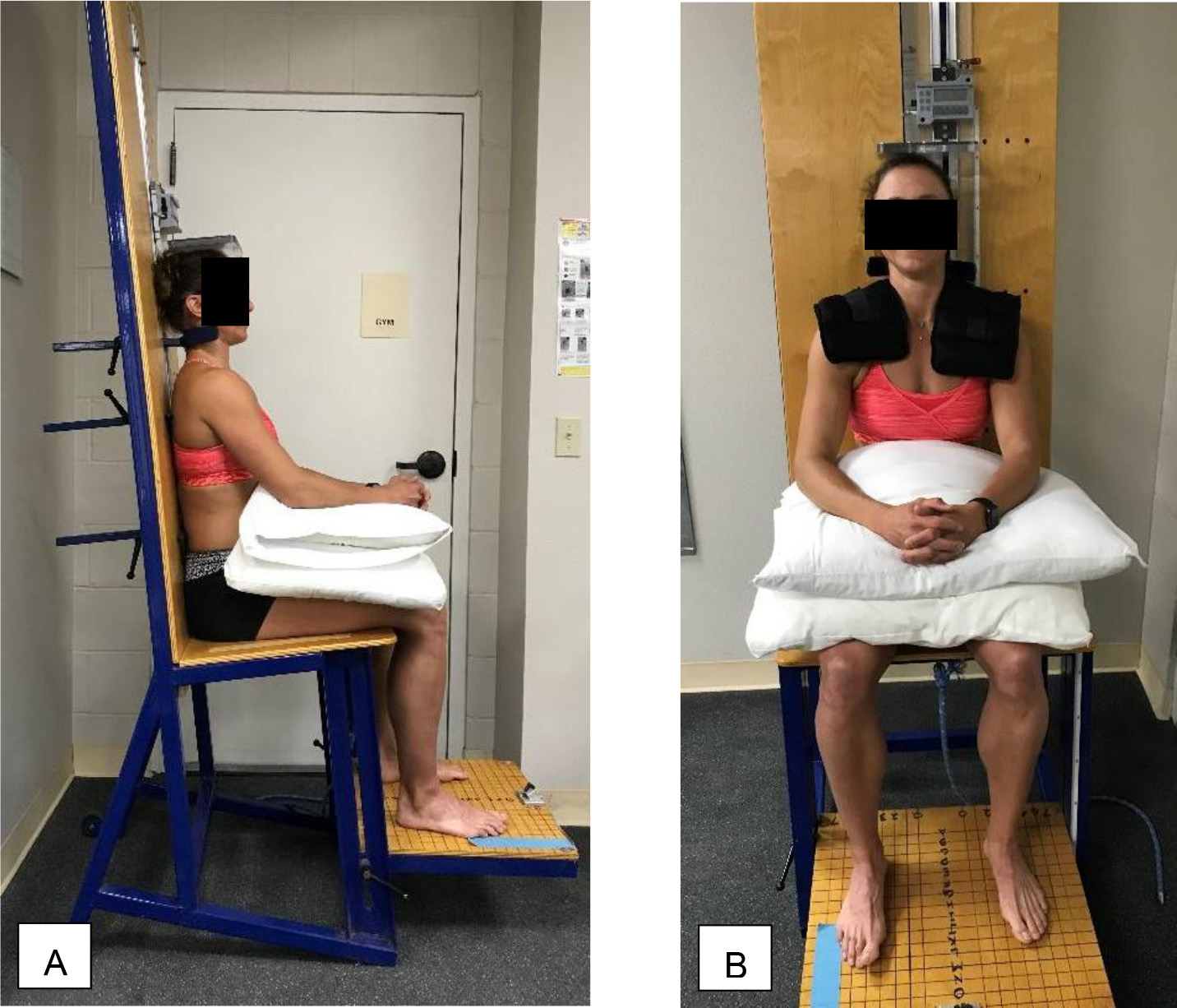
Figure 4.
Position of participant – A: for spinal height measurement in stadiometer unit; and B: during spinal loading time in sitting with 5lb on each shoulder.
At the beginning of data collection, a randomization plan generator (http://www.randomization.com) assigned each participant to one of two interventions: (1) standing RTE at a rate of 10 per 45 seconds, repeated five times with 15-second rest breaks; or (2) standing STE for 5
The participant repositioned on the stadiometer and spinal height was measured (Measurement 4). Participants scored their low back and lower extremity symptoms using NPRS [40], and mapped their pain on a body pain diagram prior to intervention, immediately after and 2-week following the intervention to determine pain rating and centralization of symptoms [8]. The principal investigator applied a numeric overlay template to the participants’ body diagrams to document the most distal pain location scores between 0 (no LBP) and 6. Higher score indicated a more distal symptoms’ location.
2.5.2Home instructions
Participants were instructed to continue to use their medications, as prescribed by their primary healthcare provider and not to change them during the follow-up two-week period. A sheet including home exercise instructions was provided to each participant. Instructions included RTE or STE based on random group assignment, performed approximately 5 times per day. Each participant completed a sheet recording home exercise compliance.
2.5.3Session 2
Participants completed same questionnaires, trunk unloading procedure and four stadiometric measurements as in Session 1. The participants then scored their low back and lower extremity symptoms using NPRS [39], and mapped their pain on a body pain diagram.
2.5.4Investigator blinding
The principal investigator was involved with data collection, supervised positioning in the stadiometer and stadiometric measurements. The investigator was blinded to the intervention and the stadiometric measurements during the experiment.
2.6Data analysis
Descriptive and inferential statistics were carried out using Excel and SPSS 23.0 for Windows (SPSS, Chicago, IL, USA). Descriptive statistics including mean, median, mode, standard deviation, minimum and maximum values, frequency counts were collected for age, height, weight, body mass index, pain, centralization, function (Modified Oswestry LBP Disability Questionnaire), FABQ, spinal height, and spinal height changes after repetitive and sustained standing trunk extension after a period of spinal loading. To assess differences between the groups for these variables at the beginning of data collection, independent t-tests and Mann Whitney-U were used. Levene’s test and Shapiro-Wilk test of normality were used to test for variance and measurements distribution of spinal height, changes in spinal height, degrees of spinal extension, pain, and function outcomes.
Table 1
Baseline characteristics of the 30 study participants by group
| Variables | Repetitive trunk extension (RTE) group | Sustained trunk extension (STE) group | |
| Age (years) | 59.13 | 48.53 | 0.10 |
| Height (m) | 1.49 | 1.50 | 0.73 |
| Weight (kg) | 67.93 | 70.07 | 0.70 |
| BMI | 26.67 | 26.8 | 0.95 |
| NPRS (most) | 5.80 | 5.37 | 0.55 |
| NPRS (average) | 2.67 | 3.33 | 0.19 |
| NPRS (minimum) | 1.53 | 2.27 | 0.10 |
| NPRS (present) | 2.40 | 3.43 | 0.15 |
| Chronicity of symptoms (weeks) | 399.00 | 73.63 | 0.09 |
| Modified Oswestry (visit 1) (%) | 19.60 | 13 | 0.03* |
| Modified Oswestry (visit 2) (%) | 14.67 | 6.40 | 0.02* |
| Centralization median (IQR) | 2 (IQR | 2 (IQR | 0.36 |
| Gender | 6♂& 9♀ | 6♂& 9♀ | 1 |
| FABQ | 23.60 | 22.20 | 0.79 |
Notes: BMI
A Wilcoxon sign-rank test was used to assess differences in spinal height, centralization and pain outcomes improvements following STE and RTE postures. A 2 (between participants – type of trunk extension: STE vs. RTE) x 2 (within participants – time: change at visit 1 and change at visit 2) mixed ANOVA’s examined differences in (1) spinal height change and (2) function outcomes as a result of sustained and repetitive standing trunk extension after a period of spinal loading. Post hoc paired t-tests explored further for significant differences in spinal height, pain and function outcomes between the four conditions. A 2 (between participants – type of trunk extension: STE vs. RTE)
3.Results
Of the 35 subjects recruited for the study, 34 met all inclusion criteria. One subject was excluded secondary to pain with standing trunk extension upon evaluation after subjectively reporting no pain with this posture on pre-screening questionnaire. Three participants developed pain several days after the first session while participating in the home exercise program and were asked to discontinue the program and no follow up session was scheduled. One participant did not report pain with the home program until the follow up session and at that time, only NPRS, Modified Oswestry and pain body diagram questionnaires were completed. This participant was excluded.
Table 2
Descriptive statistics including mean
| Variables | RTE Group Before Session 1 | RTE Group immediately after Session 1 | Changes b/w before and after RTE | STE Group Before Session 1 | STE Group immediately after Session 1 | Changes b/w before and after STE |
|---|---|---|---|---|---|---|
| Treatment Session 1 | ||||||
| NPRS (most) | 5.80 | NA | NA | 5.40 | NA | NA |
| NPRS (average) | 2.67 | NA | NA | 3.33 | NA | NA |
| NPRS (minimum) | 1.53 | NA | NA | 2.27 | NA | NA |
| NPRS (present) | 2.40 | 2.33 | 0.07 | 3.47 | 2.33 | 1.14 |
| Modified Oswestry (%) | 19.60 | NA | NA | 13 | NA | NA |
| Spinal Height (mm) | 246.30 | 248.37 | 2.07 | 257.46 | 262.00 | 4.54 |
| Centralization (median and IQR) | 2 (IQR | 2 (IQR | 0 | 2 (IQR | 1 (IQR | 1 |
| FABQ | 23.6 | NA | NA | 22.20 | NA | NA |
| RTE Group Before Session 2 | RTE Group immediately after Session 2 | Changes b/w before and after RTE | STE Group Before Session 2 | STE Group immediately after Session 2 | Changes b/w before and after STE | |
| Treatment Session 2 | ||||||
| NPRS (most) | 4.20 | NA | NA | 2.60 | NA | NA |
| NPRS (average) | 2.47 | NA | NA | 1.47 | NA | NA |
| NPRS (minimum) | 1.27 | NA | NA | 0.83 | NA | NA |
| NPRS (present) | 2.20 | 1.93 | 0.27 | 1.00 | 0.87 | 0.13 |
| Modified Oswestry (%) | 14.67 | NA | NA | 6.40 | NA | NA |
| Spinal Height (mm) | 245.50 | 247.90 | 2.39 | 258.17 | 261.62 | 3.91 |
| Centralization (median & IQR) | 2 (IQR | 1 (IQR | 1 | 1 (IQR | 1 (IQR | 0 |
Notes: RTE
Thirty participants (18 women and 12 men) randomized into two groups of 15 with a mean age of 59.1
4.Discussion
This is the first study to evaluate spine growth during standing extension postures commonly used in Mechanical Diagnosis and Therapy (the McKenzie Method) [46] in a population of people with LBP. Clinicians use such methods across a broad spectrum of ages, pathologies and disabilities. Therefore, this study was designed to avoid exclusion based on age and lumbar pathology as not to limit the generalizability of the results and to better understand the effect of standing trunk extension postures on these populations. Standing trunk extension may be a safer option for cardiovascular patients because of less hemodynamic demand as compared to prone or supine lying trunk extension [46]. Additionally, STE posture can be more practical and easier to achieve for subjects depending on convenience and physical ability. The results indicated that STE posture for 45 seconds repeated five times caused greater spine growth as compared to RTE posture for 10 repetitions repeated five times within five minutes, displaying large effect sizes. Moreover, LBP decreased to a greater extent when the participants did sustained versus repetitive trunk extension in standing. It is possible that the RTE group showed less spinal height increase and pain reduction due to their higher average age and chronicity of symptoms (Table 2) This could be attributable to the biomechanical changes that occur during the spinal degenerative process of a depressurized nucleus and irregular spikes of excessive IVD loading and an increased neutral zone with advancing IVD degeneration [47, 48, 49]. These findings suggest that people that respond favorably to standing trunk extension exercise could use such postures and movements to alleviate their LBP and improve spine height while in a weight bearing position. Four of the 35 participants with LBP (11%) initially recruited for the study did not tolerate the standing trunk extension exercise program and were excluded from the study, indicating that such program may not be appropriate for all patients with LBP. The spinal growth recorded of about 4 mm during five time 45 seconds hold STE posture was similar to that reported previously in the seated slouched position using a lumbar support [51], which suggests that people experiencing pain relief and symptoms’ centralization in such standing posture could adopt it to increase spine height and rehydrate the lumbar IVDs Although the spinal height changes were temporary, as shown in previous studies, new research shows that dynamic loading significantly increases small and large solute transport through the cartilage end-plates. The clinician’s goal is therefore not to sustain spinal height growth but to enhance transport of nutrients into the IVD [51].
Our results support those previously reported in prone position where increased spinal height recovery was greater following prone hyperextension (7 mm) as compared to prone lying (6 mm) [52]. Moreover, both prone [31] and supine hyperextended postures resulted in spinal height increase (6.37
Although lying postures resulted in greater spine height growth of 5 mm [32] and larger decreased in pain and centralization in elderly people with nerve root compression syndromes [8] as compared to our study results, the standing techniques used in our study could be recommended as 57% (17 out of 30) of participants in our investigation reported greater or equal to 2/10 pain improvement (MCID). Such improvements in pain are noteworthy as the participants’ FABQ (Table 2) averaged 23, which indicated a greater risk of reporting no improvement in Oswestry Disability Questionnaire at 6-month and persistent problems [53]. The two groups reported very similar home program compliance at the end of two weeks with the RTE group reporting 91% compliance and the STE group reporting 87% compliance.
The Modified Oswestry resulted in seven participants (23%) reaching the MCID of decreased 12/100 points for the Oswestry LBP questionnaire. No MCID for centralization has been established; however, centralization resulted in a median change of one in both RTE and STE groups from before Session 1 to after Session 2. The RTE group had five subjects and the STE group had seven who had equal to or greater than a twopoint change in their centralization score after two weeks. Future research is needed to investigate the characteristics of those patients that centralized the most with standing extension, which could help guide patient care as patients with lumbar stenosis may not be able to tolerate such standing extension postures.
Limitations of this study include some difference in age and initial Modified Oswestry scores between the groups, a relatively low initial current pain level amongst participants, and no long term follow up. Future studies with longer follow up and recordings of medication usage duration prior to entry in the study are warranted. Additionally, the groups were heterogenous for symptoms’ chronicity, as there were three participants in the RTE group with years of symptoms reported as compared one participant reporting eight years of symptoms in the STE group. The chronic nature of symptoms for these participants may have influenced the outcomes of the study as the RTE group did show less pain reduction although similar improvements in function as the STE group. Future studies including subjects with greater initial LBP would be useful in determining effectiveness in reducing pain.
5.Conclusion
People with LBP experienced greater spine growth and improvements of pain that were clinically meaningful during standing STE as compared to RTE. These findings suggest that people with LBP could use such postures and movements to alleviate their LBP and improve spine height while in a weight bearing position. Sustained trunk extension may prove more effective in restoring spinal height loss as compared to the RTE intervention and provides alternative ergonomic postural option for people with LBP seeking to rehydrate their lumbar IVDs.
Author contributions
Jeremy J. Harrison: literature review, study design, data collection, analysis and writing.
Jean-Michel Brismée: study design, data analysis and review writing.
Phillip S. Sizer Jr: study design, review writing.
Brent K. Denny: piloting of study, data analysis.
Stéphane Sobczak: study design, and critical review.
Data availability statement
Data are available upon request to the Principal Investigator of the study.
Ethical approval
The Texas Tech University Health Sciences Center Institutional Review Board (IRB) approved this study (L19-024). The trial was registered at https://clinicaltrials.gov (NCT03785457) prior to the start of data collection in January 2019.
Funding
Not applicable.
Informed consent
All participants voluntarily consented to participate in the study and signed an informed consent form.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-230118.
Acknowledgments
We would like to thank the study participants for their willingness to contribute to research and for Sports Medicine & Physical Therapy of Fredericksburg for allowing us to conduct our study.
Conflict of interest
We affirm that none of the authors have financial affiliation (including research funding) or involvement with any commercial organization that has a direct financial interest in any matter included in this manuscript.
References
[1] | US Department of Labor Bureau of Labor Statistics: Standing or walking versus sitting on the job in 2016 ((2017) March 01); https//www.bls.gov/opub/ted/2017/standing-or-walking-versus-sitting-on-the-job-in-2016.htm; Accessed 12/08/2017. |
[2] | Chou R, Qaseem A, Snow V, Casey D, Cross JT, Jr., Shekelle P, Owens DK. Clinical efficacy assessment subcommittee of the american college of physicians; American College of Physicians; American pain society low back pain guidelines panel. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. (2007) ; 147: : 478-491. |
[3] | Cunha C, Silva AJ, Pereira P, Vaz R, Gonçalves RM, Barbosa MA. The inflammatory response in the regression of lumbar disc herniation. Arthritis Research & Therapy. (2018) ; 20: : 1-9. |
[4] | McCall IW. Lumbar herniated disks. Radiol Clin North Am. (2000) ; 38: : 1293-1309. |
[5] | Kourtis D, Magnusson ML, Smith F, Hadjipavlou A, Pope MH. Spine height and disc height changes as the effect of hyperextension using stadiometry and MRI. Iowa Orthop J. (2004) ; 24: : 65-71. |
[6] | Magnusson ML, Aleksiev AR, Spratt KF, Lakes RS, Pope MH. Hyperextension and spine height changes. Spine. (1996) ; 21: : 2670-5. |
[7] | Lazzarini M, Brismee JM, Owens SC, Dedrick GS, Sizer PS. Spinal height change in response to sustained and repetitive prone lumbar extension after a period of spinal unloading. J Manipulative Physiol Ther. (2014) ; 37: (8): 586-592. |
[8] | Simmerman SM, Sizer PS, Dedrick GS, Apte GG, Brismee JM. Immediate changes in spinal height and pain after aquatic vertical traction in patients with persistent low back symptoms: a crossover clinical trial. PM R. (2011) ; 3: : 447-457. |
[9] | Masuda K, Oegema TR Jr, An HS. Growth factors and treatment of intervertebral disc degeneration. Spine. (2004) ; 29: : 2757-2769. |
[10] | Koshy JM, Devi GD, Archana R, Johnson WM. Diurnal variation of height in south indian adolescent. Int J Anat Res. (2017) ; 5: (3.3): 4432-35. |
[11] | Puntumetakul R, Trott P, Williams M, Fulton I. Effect of time of day on the vertical spinal creep response. Appl Ergon. (2009) ; 40: : 33-8. |
[12] | Magnusson M, Pope M. Body height changes with hyperextension. Clin Biomech (Bristol, Avon). (1996) ; 11: (4): 236-238. |
[13] | Lam OT, Strenger DM, Chan-Fee M, Pham PT, Preuss RA, Robbins SM. Effectiveness of the mckenzie method of mechanical diagnosis and therapy for treating low back pain: literature review with meta-analysis. J Orthop Sports Phys Ther. (2018) Jun; 48: (6): 476-490. doi: 10.2519/jospt.2018.7562. Epub 2018 Mar 30. PMID: 29602304. |
[14] | Swinkels A, Cochrane K, Burt A, Johnson L, Lunn T, Rees AS. Exercise interventions for non-specific low back pain: An overview of systematic reviews. Phys Ther Rev. (2009) ; 14: : 247-259. |
[15] | Oliveira VC, Ferreira PH, Maher CG, Pinto RZ, Refshauge KM, Ferreira ML. Effectiveness of self-management of low back pain: Systematic review with meta-analysis. Arthri Care Res. (2012) ; 64: : 1739-1748. |
[16] | Albert HB, Hauge E, Manniche C. Centralization in patients with sciatica: are pain responses to repeated movement and positioning associated with outcome or types of disc lesions? Eur Spine J. (2012) Apr; 21: (4): 630-6. doi: 10.1007/s00586-011-2018-9. Epub 2011 Sep 23. PMID: 21947819; PMCID: PMC3326129. |
[17] | Matsudaira K, Hiroe M, Kikkawa M, Sawada T, Suzuki M, Isomura T, Oka H, Hiroe K, Hiroe K. Can standing back extension exercise improve or prevent low back pain in Japanese care workers? J Man Manip Ther. (2015) ; 23: (4): 205-9. |
[18] | Dunsford A, Kumar S, Clarke S. Integrating evidence into practice: Use of McKenzie-based treatment for mechanical low back pain. J Multidiscip Healthc. (2011) ; 4: : 393-402. |
[19] | Tonosu J, Matsudaira K, Oka H, Okazaki H, Oshio T, Hanaoka I, et al. A population approach to analyze the effectiveness of a back extension exercise “One Stretch” in patients with low back pain: A replication study. J Orthop Sci. (2016) ; 21: : 414-418. |
[20] | Bybee RF, Olsen DL, Cantu-Boncser G, Allen HC, Byars A. Centralization of symptoms and lumbar range of motion in patients with low back pain. Physiother Theory Pract. (2009) ; 25: : 257-267. |
[21] | Brennan G, Fritz J, Hunter S, Thackeray A, Delitto A, Erhard R. Identifying subgroups of patients with acute/subacute “nonspecific” low back pain: results of randomized clinical trial. Spine. (2006) ; 31: : 623-631. |
[22] | Laslett M, Oberg B, Aprill C, McDonald B, Centralization as a predictor of provocation discography results in chronic low back pain, and the influence of disability and distress on diagnostic power. Spine J. (2005) ; 5: : 370-380. |
[23] | Aina A, May S, Clare H. The centralization phenomenon of spinal symptoms – a systematic review. Man Ther. (2004) ; 9: : 134-143. |
[24] | Werneke MW, Hart DL, Resnik L, Stratford PW, Reyes A. Centralization: prevalence and effect on treatment outcomes using a standardized operation definition and measurement method. J Orthop Sports Phys Ther. (2008) ; 38: : 116-125. |
[25] | McKenzie RA, May S. The Lumbar Spine Mechanical Diagnosis and Therapy, 2 ed. Spinal Publications Ltd. (2003) ; 647-667. |
[26] | Fahmy E, Shaker H, Ragab W, et al. Efficacy of spinal extension exercise program versus muscle energy technique in treatment of chronic mechanical low back pain. Egypt J Neurol Psychiatry Neurosurg 55. (2019) ; 77. doi: 10.1186/s41983-019-0124-5. |
[27] | Nordez A, Gross R, Andrade R, et al. Non-muscular structures can limit the maximal joint range of motion during stretching. Sports Med. (2017) ; 47: : 1925-1929. |
[28] | Bandy W, Irion J. The effect of time on static stretch on the flexibility of the hamstring muscles. Phys Ther. (1994) ; 74: (9): 845-50. |
[29] | Page P. Current concepts in muscle stretching for exercise and rehabilitation. Int J Sports Phys Ther. (2012) ; 7: : 109-119. |
[30] | Bybee RF, Mamantov J, Meekins W, Witt J, Byars A, Greenwood M. Comparison of two stretching protocols on lumbar spine extension. J Back Musculoskeletal Rehabil. (2008) ; 21: : 153-159. |
[31] | Owens SC, Brismee JM, Pennel PN, Dedrick GS, Sizer PS, James CR. Changes in spinal height following sustained lumbar flexion and extension postures: a clinical measure of intervertebral disc hydration using stadiometry. J Manipulative Physiol Ther. (2009) ; 32: : 358-63. |
[32] | Gerke DA, Brismee JM, Sizer PS, Dedrick GS, James CR. Change in spine height measurements following sustained mid-range and end-range flexion of the lumbar spine. Appl Ergon. (2011) ; 42: : 331-336. |
[33] | Surkitt LD, Ford JJ, Hahne AJ, Pizzari T, McMeeken JM. Efficacy of directional preference management for low back pain: a systematic review. Phys Ther. (2012) ; 92: : 652-665. |
[34] | Machado LA, de Souza Mv, Ferreira PH, Ferreira ML. The McKenzie method for low back pain: a systematic review of the literature with a meta-analysis approach. Spine. (2006) ; 31: : 254-262. |
[35] | Huysmans E, Ickmans K, Van Dyck D, et al. Association between symptoms of central sensitization and cognitive behavioral factors in people with chronic nonspecific low back pain: a cross-sectional study. J Manipulative Physiol Ther. (2017) ; 17: : 30151-3. |
[36] | Garcia AN, Costa LDCM, Hancock MJ, et al. McKenzie method of mechanical diagnosis and therapy was slightly more effective than placebo for pain, but not for disability, in patients with chronic non-specific low back pain: a randomized placebo controlled trial with short and longer term follow-up. Br J Sports Med. (2017) ; 52: : 594-600. |
[37] | Portney LG, Watkins MP. Foundations of clinical research: Applications to practice, 3 ed. F.A. Davis Company: Philadelphia, PA, USA, (2015) ; ISBN 978-0131716407. |
[38] | Yarznbowicz R, Tao M, Owens A, Wlodarski M, Dolutan J. Pain pattern classification and directional preference are associated with clinical outcomes for patients with low back pain. J Man Manip Ther. (2018) ; 26: : 18-24. |
[39] | Ferreira-Valente MA, Pais-Ribeiro JL, Jensen MP. Validity of four pain intensity rating scales. Pain. (2011) ; 152: : 2399-2404. |
[40] | Werneke MW, Hart DL, Cutrone G, et al. Association Between Directional Preference and Centralization in Patients With Low Back Pain. J Orthop Sports Phys Ther. (2011) ; 41: : 22-31. |
[41] | May S, Donelson R. Evidence-informed management of chronic low back pain with the McKenzie method. Spine J. (2008) ; 8: : 134-141. |
[42] | Fritz JM, Irrgang JJ. A comparison of a modified Oswestry Low Back Pain Disability Questionnaire and the Quebec Back Pain Disability Scale. Phys Ther. (2001) ; 81: : 776-788. |
[43] | Cleland JA, Fritz JM, Brennan GP. Predictive validity of initial fear avoidance beliefs in patients with low back pain receiving physical therapy: is the FABQ a useful screening tool for identifying patients at risk for a poor recovery? Eur Spine J. (2008) ; 17: : 70-79. |
[44] | Stothart JP, McGill SM. Stadiometry: on measurement technique to reduce variability in spine shrinkage measurement. Clin Biomech. (2000) ; 15: : 546-8. |
[45] | Mann SJ, Lam JC, Singh P. McKenzie Back Exercises. [Updated 2022; Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. (2022) Jan; Available from: https//www.ncbi.nlm.nih.gov/books/NBK539720/. |
[46] | Al-Obaidi S, Anthony J, Dean E, Al-Shuwai N. Cardiovascular responses to repetitive McKenzie lumbar spine exercises. Phys Ther. (2001) ; 81: (9): 1524-33. doi: 10.1093/ptj/81.9.1524, PMID: 11688589. |
[47] | Sengupta DK, Fan H. The basis of mechanical instability in degenerative disc disease a cadaveric study of abnormal motion versus load distribution. Spine. (2014) ; 39: (13): 1032-43. |
[48] | Alexander LA, Hancock E, Agouris I, Smith FW, MacSween A. The response of the nucleus pulposus of the lumbar intervertebral discs to functionally loaded positions. Spine. (2007) ; 32: : 1508-1512. |
[49] | Rousseau MA, Bradford DS, Hadi TM, Pedersen KL, Lotz JC. The instant axis of rotation influences facet forces at L5/S1 during flexion/extension and lateral bending. Eur Spine J. (2006) ; 15: : 299-307. |
[50] | Pape JL, Brismee JM, Sizer PS. Increased spinal height using propped slouched sitting postures: Innovative ways to rehydrate intervertebral discs. Appl Ergon. (2018) ; 66: : 9-17. |
[51] | Sampson SL, Sylvia M, Fields AJ. Effects of dynamic loading on solute transport through the human cartilage endplate. J Biomech. (2019) ; 83: : 273-279. |
[52] | Magnusson ML, Pope MH, Hansson T. Does hyperextension have an unloading effect on the intervertebral disc? Scand J Rehabil Med. (1995) ; 27: (1): 5-9. |
[53] | George SZ, Fritz JM, Childs JD. Investigation of elevated fear-avoidance beliefs for patients with low back pain: a secondary analysis involving patients enrolled in physical therapy clinical trials. J Orthop Sports Phys Ther. (2008) ; 38: (2): 50-58. |


