
Effect of taping on posture of thoracic region in patients with thoracic kyphosis using acceleration
Abstract
BACKGROUND:
In the working environment of modern society, a poor sitting posture for a prolonged time may lead to abnormal spinal alignment such as thoracic kyphosis (TK).
OBJECTIVE:
This study aimed to evaluate the efficacy of taping for posture correction of patients with TK, providing theoretical and empirical guidance for clinicians attempting to rectify TK posture.
METHODS:
The study included 15 subjects aged 30–60 years, all with a TK angle of
RESULTS:
There were no significant differences in the MIL (
CONCLUSION:
Taping serves as an effective method for immediately improving kyphotic posture. It corrects the position of the scapula and cervicothoracic line and exerts passive retraction on the relevant muscles, thus mitigating trunk imbalance.
1.Introduction
Since the advent of computers and mobile technology in the 1950s, there have been profound transformations in societal and work-related practices [1]. In work environments, it is not uncommon for employees to assume poor posture while relaxing during breaks [2], potentially leading to fatigue of the lumbar extensor muscles and difficulty maintaining the typical upright posture of the spine [3, 4]. Prolonged slouching can adversely affect spinal alignment, potentially resulting in thoracic kyphosis (TK), rounded shoulder posture (RSP), and/or forward head posture (FHP) [5, 6].
Research by Griegel et al. suggests that abnormal spinal alignment is indicative of imbalances and irregular movements within the musculoskeletal system [7]. Poor posture typically manifests when the head or shoulders are positioned further forward than the trunk, causing a forward head and chin posture [8, 9], forward and downward rotation of the scapulae, an increase in cervical lordosis, and an enhancement in upper TK. These changes can potentially lead to upper quarter pain [10, 11, 12]. Hence, imbalances in muscle strength and excessive strain on the thoracic spine, due to poor posture, are often the root causes of TK.
A TK angle of
According to Lee et al., imbalances in muscle strength due to improper spinal alignment result in compensatory overuse of postural muscles, leading to excessive energy expenditure, fatigue, and pain [19]. Similar studies suggest that TK results from improper weight-bearing and movement patterns, and that greater rigidity in the thoracic vertebrae leads to improper postural control of lumbar and cervical regions. This situation triggers compensatory behavior [20] and alterations in normal sagittal alignment, which could potentially cause pain and dysfunction in the shoulder and pelvic girdle, as well as the cervical, thoracic, and lumbar vertebrae [21]. Moreover, incorrect spinal alignment can even lead to decreased activity in surrounding tissues [22], increase the risk of falls among middle-aged and elderly individuals [23], and potentially have serious consequences such as elevated mortality rates [24].
Han et al. [25] discovered that the application of tape immediately results in passive retraction of the scapulae to correct RSP, consequently stretching the shortened pectoral muscles. Their findings revealed that the use of stretch tape significantly lengthened the pectoralis minor muscle and substantially reduced the protraction of the scapulae. Mechanistically, as an individual works at a desk, the stretched tape is placed under increased tension, prompting the shoulders to retract. Similarly, Hwang-Bo et al. [26] found that taping immediately corrected RSP and alleviated back pain in women required to sit for extended periods due to their occupations. Another study identified significant post-taping rotation of the scapulae in the sagittal plane in patients with shoulder impingement syndrome [27]. Furthermore, taping has been proven to enhance the three-dimensional movement of the scapulae [28].
From a mechanistic standpoint, taping exerts a pulling force on the target muscles, utilizing its own elasticity to restore misaligned muscles to their correct position. To date, most research on posture correction using taping technology has aimed to verify that taping can improve muscle pain and related bone positions. However, there is a lack of experimental evidence on the effect of taping technology on the daily movements of patients with TK, particularly in relation to the swinging of thoracic vertebrae in all directions.
A 3-axis accelerometer is a device designed to measure acceleration along three axes (MIL-X, AP-Y, and VT-Z axes) in space. Numerous studies have utilized 3-axis accelerometers to monitor and evaluate dynamic human activities [29, 30, 31]. Ito et al. studied the relationship between the traditional clinical rating of Parkinson’s disease and the metabolic equivalent and physical activity level measured by 3-axis accelerometer [29]. Lee et al. used a 3-axis accelerometer to measure the physical activity of the elderly with coronary artery disease, and they tested the accuracy of the accelerometer in detecting physical activity [30]. Shin et al. installed triaxial accelerometers above T2 and L3 spinous processes in the elderly with impaired vision to measure their gait time, trunk amplitude and trunk acceleration ratio, and judge the influence of vision on physical activities [31]. In a previous investigation of trunk movement in patients with flat back syndrome, the author used accelerometers to detect swinging of the lumbar spine during dynamic activities, assisting in targeted treatment [32]. In the present study, a 3-axis accelerometer was used to monitor the balance and motion of participants’ thoracic vertebrae during dynamic activities. The objective was to verify whether taping technology can enhance stability by altering the swinging of the thoracic vertebrae in all directions.
Coronal deformities, such as scoliosis, have been the primary focus of spinal surgeons for many years. However, the significance of spinal alignment in the sagittal plane has only recently been acknowledged. Underestimation of the importance of sagittal spinal alignment, in conjunction with the increasing prevalence of poor posture in modern society, has contributed to a surge in TK cases [15]. The focus of this study is on exploring the efficacy of taping to improve and prevent TK posture.
2.Methods
2.1Participants
This study recruited 15 volunteers aged 30–60 years who exhibited a TK angle
The study was approved by the Human Ethics Committee of the Faculty of Health Sciences, Inje University (number: INJE 2021-05-033-002) and informed consent was obtained from all participants prior to study commencement. The participant characteristics were as follows (data are expressed as mean
2.2Equipment
2.2.1Dual Inclinometer
Figure 1.
Dual Inclinometer.

TK angles were measured using a dual inclinometer (Acumar; Lafayette Instrument Co, Lafayette, IN, USA) (Fig. 1) [35]. Participants were instructed to stand with their feet shoulder-width apart, remain relaxed, and look straight ahead. The spinous processes of the first and twelfth thoracic vertebrae were palpated, marked, and measured thrice with the dual inclinometer; the average was then calculated.
2.2.2Accelerometer
Figure 2.
3-axis accelerometer.

A three-axis accelerometer (Fit Dot Life, Suwon, Korea; size: 35
2.2.3Steps
Figure 3.
A “low-high-low” steps.

Three steps were arranged in a “low-high-low” configuration (Fig. 3). This design, which incorporates ascending and descending steps, allows monitoring of the activity of the trunk in terms of upward acceleration and downward deceleration. Each step was 10 cm in length and 27 cm wide; the two lower steps were 16 cm high, and the elevated step was 32 cm high.
Figure 4.
The kinesiology 3NS tape.

2.2.4Taping
KT-X-050 tape (Kinesio Tex, Tokyo, Japan) was used in the experiment (Fig. 4). We analyzed tape with an elongation of 20% under natural tension and tape with an elongation of 40% under moderate tension.
2.3Experimental methods
The steps were positioned on flat ground with ample surrounding space. Participants were instructed to walk a distance of 1 m, before reaching the first step and beyond the third step, to facilitate capture of natural data. However, only recordings obtained during ascent and descent of the steps were included in the final analysis. The accelerometer was affixed at the T6 spinous process. Participants were given verbal instructions and asked to walk up and down the steps at a comfortable pace three times, with a 30-second rest and adjustment period between each trial.
Figure 5.
Application of taping to the subject.
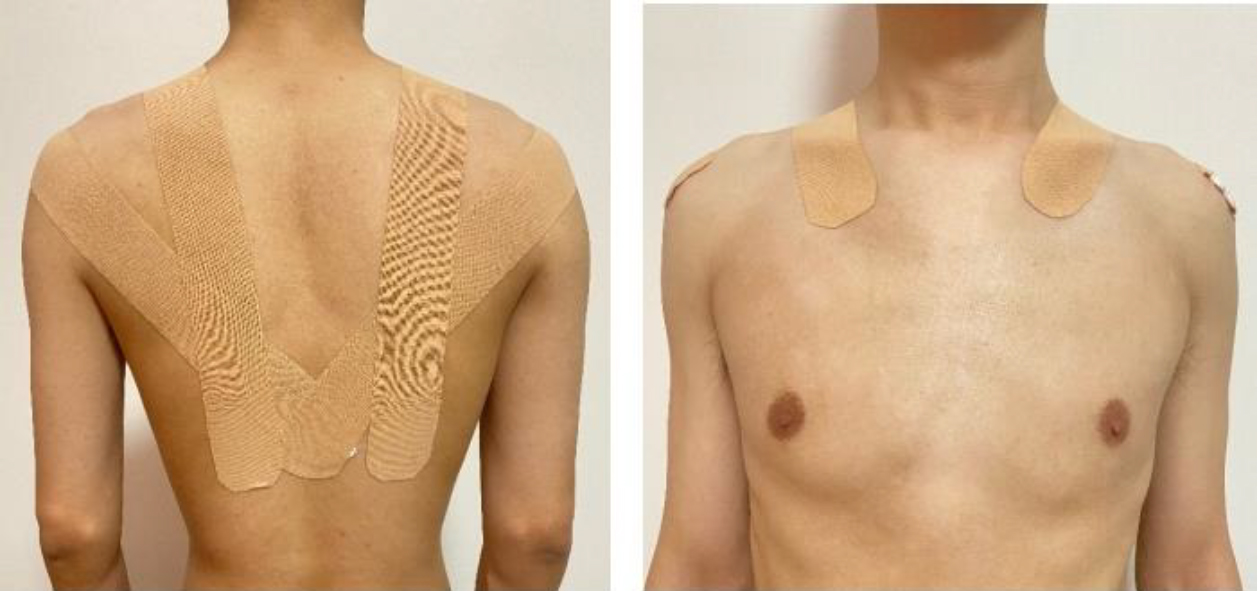
Table 1
Acceleration values (
| MIL (m/s2) | VT (m/s2) | AP (m/s2) | |
|---|---|---|---|
| Without assistance | 1.071 | 6.144 | 2.770 |
| 20% elongation | 1.058 | 5.686 | 2.256 |
| 40% elongation | 1.025 | 5.554 | 1.973 |
All values are mean
After three trials without taping assistance, there was a 5-minute rest and adjustment period. Following that, tape was applied. The length of the tape from the acromion joint to the spinous process of the tenth thoracic vertebra [25, 26], and from below the medial third of the clavicle via the upper trapezius muscle belly to the lower trapezius muscle belly, was measured [36]. Then, the tape was cut to four-fifths of the required length for a 20% stretch and three-fifths of the required length for a 40% stretch. Lastly, the tape was applied bilaterally (Fig. 5). According to Lee and Yoo, when taping is used for immediate correction, the joints should first be positioned correctly and tape should then be used to secure them in this position [37]. Therefore, volunteers were asked to remove their shirts, stand naturally, extend their upper limbs, hold their hands out slightly, retract their scapulae, look forward, retract the head, and straighten the thoracic region to a neutral position. Each taping-assisted trial was repeated three times, with 30 seconds of rest between trials, and the average of the measurements was used for analysis.
2.4Data analysis
The SPSS 20.0 statistical package (SPSS Inc., Chicago, IL, USA) was used to conduct a one-way repeated measures analysis of variance (ANOVA). A
3.Results
The acceleration values are presented in Table 1. There were no significant differences in the MIL acceleration values (1.071
4.Discussion
The change of the detected acceleration value can reflect the swing of the participants’ torso during the action, and this “swing” represents the balance and dynamic state of the trunk, that is, when the acceleration value is large, the trunk swings violently and the control ability is poor; When the acceleration value is small, the trunk swings lightly and has strong control ability. We observed a significant difference in AP movement between the 40% elongation taping and no taping groups. This result demonstrates that the sagittal plane movement of the trunk decreases after taping. Previous studies have reported that, in individuals with TK, the center of gravity is positioned farther forward than in healthy individuals, leading to an increase in bending torque on the thoracic vertebrae [38]. This mechanical change imbalance the body, reduces control of core muscles, decreases power output, and thus heightens the risk of falling [39]. Katzman et al. found that, compared to the general population, individuals with TK have poor control of the trunk, and their gait cycle is marked by longer standing phases and slower walking speed. These factors are linked to an increased fall risk [40]. In this study, the decreased AP movement in the 40% elongation taping group reflects a reduction of bending torque in the thoracic region; therefore, taping assistance can be effective immediately.
During walking, normal spinal curvature plays a pivotal role in absorbing the impact force from the ground, allowing the human body to swing and move forward within the normal range. TK is characterized by excessive posterior protrusion of the thoracic vertebra, leading to compensatory FHP and RSP. For individuals with TK, the ground reaction force is directly transmitted to the spine during walking, particularly when climbing stairs, which exacerbates trunk instability and results in larger VT movements of the center of mass (COM) compared to individuals without TK [41]. This may explain the higher acceleration values and more severe thoracic spine swing observed in the unassisted trials. In our study, taping assistance significantly decreased the acceleration of the thoracic vertebrae in the VT direction compared to the condition without taping assistance. Decreasing movement in the VT direction while ascending and descending stairs may enhance gait stability.
Balzini et al. found that FHP, scapula protraction, reduced lumbar lordosis, and decreased standing height were related to hyperkyphosis, and that individuals with these attributes exhibited poorer balance, slower gait, a wider stance and walking posture, and reduced stair-climbing speed [22]. One possible explanation is that individuals with TK require greater VT vertebral movement to maintain their COM and absorb the ground reaction force. Our results align with previous reports that analyzed the effectiveness of Kinesio taping. In the current study, we demonstrated that taping assistance can effectively control compensatory movement in the thoracic vertebrae while ascending and descending stairs. This method is a relatively efficient and cost-effective solution for correcting kyphotic posture, and it may reduce the risk of falls and fall-related mortality caused by poor balance in the elderly.
Our results hold value for office workers, as well as primary and secondary school students, who spend extended periods at desks and may unconsciously adopt poor sitting postures [2]. Moore reported that poor posture can lead to weakening of the flexor muscles in the neck and the middle and lower trapezius, along with tension and contraction in the upper trapezius, levator scapulae, pectoralis major and minor, and the rhomboids [42]. These muscle imbalances contribute to TK. When TK [43] arises in isolation, the resulting increase in spinal load can cause pain and discomfort. In an effort to mitigate this discomfort, the body responds with compensatory movements, leading to the formation of RSP and FHP [44]. Concurrently, the body attempts to compensate for changes in lumbar curvature [45], which can lead to further injury [9]. Collectively, these changes constitute what is known as “slouched posture” [46]. Deepika et al. found significant correlations between cervical lordosis and TK, and rounded shoulders and increased TK [47].
There were several limitations to our study. First, the relatively small sample size means our results may not be generalizable to all populations. Second, our study only included volunteers with TK resulting from poor posture, so the findings may not extend to cases of TK due to pathological causes or other factors. Third, we included only individuals aged 30–60 years. Lastly, our experiment did not involve long-term periodic testing, such that further experiments are needed to verify the long-term effects of taping on subjects with TK.
5.Conclusion
Taping can effectively ameliorate kyphotic posture through immediate correction of movement in the AP and VT directions, especially with 40% elongation taping. The postural impact of taping can affect the position of the scapulae and cervicothoracic line, apply traction and passive retraction to related muscles, restore spinal shock absorption, and reduce trunk imbalance. Future research should investigate whether TK caused by congenital and pathological factors can be alleviated by the taping techniques applied in this study.
Author contributions
Both authors contributed to the study design, analysis of the data, and writing of the manuscript.
Ethical approval
The study was approved by the Human Ethics Committee of the Faculty of Health Sciences, Inje University (number: INJE 2021-05-033-002).
Funding
Not applicable.
Informed consent
Each subject provided informed consent before participating in the study.
Acknowledgments
None to report.
Conflict of interest
None to report.
References
[1] | Egger M, Smith GD, Altman DG. Sestematic reviews in health care. London: BMJ Books. (2001) . |
[2] | Watanabe S, Eguchi A, Kobara K, Ishida H. Influence of trunk muscle co-contraction on spinal curvature during sitting for desk work. Electromyogr Clin Neurophysiol. (2007) ; 47: (6): 273-278. |
[3] | Carter JB, Banister EW. Musculoskeletal problems in VDT work: A review. Ergonomics. (1994) ; 37: (10): 1623-1648. |
[4] | Neumann DA. Kinesiology of the musculoskeletal system: Foundations for physical rehabilitation. St. Louis, MO: Mosby. (2002) . |
[5] | Chansirinukor W, Wilson D, Grimmer K, Dansie B. Effects of backpacks on students: Measurement of cervical and shoulder posture. Aust J Physiother. (2001) ; 47: (2): 110-116. |
[6] | Magee DJ. Orthopedic physical assessment. 2nd; ed. Philadelphia, PA: Saunders. (2002) . |
[7] | Griegel-Morris P, Larson K, Mueller-Klaus K, Oatis CA. Incidence of common postural abnormalities in the cervical, shoulder, and thoracic regions and their association with pain in two age groups of healthy subjects. Phys Ther. (1992) ; 72: (6): 425-431. |
[8] | Kim MH, Yoo WG. Effects of a visual feedback device for hip adduction on trunk muscles and sitting posture in visual display terminal workers. Asia Pac J Public Health. (2011) ; 23: (3): 378-385. |
[9] | Borstad JD. Resting position variables at the shoulder: evidence to support a posture-impairment association. Phys Ther. (2006) ; 86: (4): 549-557. |
[10] | Greenfield B. Upper quarter evaluation: Structural relationships and independence. In: Donatelli RA, Wooden MJ, eds. Orthopedic physical therapy. 3rd; ed. NY: Churchill Livingstone. (2001) . |
[11] | Greenfield B, Catlin PA, Coats PW, Green E, McDonald JJ, North C. Posture in patients with shoulder overuse injuries and healthy individuals. J Orthop Sports Phys Ther. (1995) ; 21: (5): 287-295. |
[12] | Lukasiewicz AC, McClure P, Michener L, Pratt N, Sennett B. Comparison of 3D scapular position and orientation between subjects with and without shoulder impingement. J Orthop Sports Phys Ther. (1999) ; 29: (10): 574-586. |
[13] | Neumann DA. Kinesiology of the musculoskeletal system: Foundations for rehabilitation. St. louis, ISA: Mosby. (2010) . |
[14] | Eum R, Leveille SG, Kiely DK, Kiel DP, Samelson EJ, Bean JF. Is kyphosis related to mobility, balance and disability? Am J Phys Med Rehabil. (2013) ; 92: (11): 980-989. |
[15] | Macagno AE, O’Brien MF. Thoracic and thoracolumbar kyphosis in adults. Spine. (2006) ; 31: (19): 161-170. |
[16] | Zaina A, Atanasio C, Ferraro C, Fusco A, Negrini M, Romano S, Negrini S. Review of rehabilitation and orthopedic conservative approach to sagittal plane diseases during growth: hyperkyphosis, junctional kyphosis, and scheuermann disease. Eur J Phys Rehabil Med. (2009) ; 45: (4): 595-603. |
[17] | Lee HA. A Study on the safety of spinal manipulation using finite element method. Master’s thesis, Korea University. (2010) . |
[18] | Jang HJ, Kim SY, Kim MJ. The reliability and relationships between thoracic kyphosis, postural stiffness and thoracic rotation in young subjects. Korean Acad Orthop Man Phys Ther. (2012) ; 18: (2): 49-55. |
[19] | Lee CS, Kang SS. Spino-pelvic parameters in adult spinal deformities. The Korean Orthopaedic Association. (2016) ; 51: (1): 9-29. |
[20] | Song JE, Kim SY, Jang HJ. A Comparison of the effects of self-mobilization and strengthening exercise of the thoracic region in young adults with thoracic hyperkyphosis. Korean Acad Orthop Man Phys Ther. (2013) ; 19: (2): 11-18. |
[21] | Katzman WB, Wanek L, Shepherd JA, Sellmeyer DE. Age-related hyperkyphosis: Its causes, consequences, and management. J Orthop Sports Phys Ther. (2010) ; 40: (6): 352-360. |
[22] | Balzini L, Vannucchi L, Benvenuti F, Benucci M, Monni M, Cappozzo A, et al. Clinical characteristics of flexed posture in elderly women. J Am Geriatr Soc. (2003) ; 51: (10): 1419-1426. |
[23] | Kado DM, Huang MH, Nguyen CB, Elizabeth BC, Greendale GA. Hyperkyphotic posture and risk of injurious falls in older persons: the Rancho Bernardo Study. J Gerontol A Biol Sci Med Sci. (2007) ; 62: (6): 652-657. |
[24] | Huang MH, Elizabeth BC, Greendale GA, Kado DM. Hyperkyphotic posture and risk of future osteoporotic fractures: The Rancho Bernardo study. J Bone Miner Res. (2006) ; 21: (3): 419-423. |
[25] | Han JT, Lee JH, Yoon CH. The mechanical effect of kinesiology tape on rounded shoulder posture in seated male workers: A single-blinded randomized controlled pilot study. Physiother Theory Pract. (2015) ; 31: (2): 120-125. |
[26] | Gak HB, Lee JH, Kim HD. Efficacy of kinesiology taping for recovery of dominant upper back pain in female sedentary worker having a rounded shoulder posture. Technol Health Care. (2013) ; 21: (6): 607-612. |
[27] | Shaheen AF, Bull AMJ, Alexander CM. Rigid and Elastic taping changes scapular kinematics and pain in subjects with shoulder impingement syndrome; an experimental study. J Electromyogr Kinesiol. (2015) ; 25: (1): 84-92. |
[28] | Yildiz TI, Castelein B, Harput G, Duzgun I, Cools A. Does scapular corrective taping alter periscapular muscle activity and 3-dimensional scapular kinematics? A systematic review. J Hand Ther. (2020) ; 33: (3): 361-370. |
[29] | Ito H, Yokoi D, Kobayashi R, Okada H, Kajita Y, Okuda S. The relationships between three-axis accelerometer measures of physical activity and motor symptoms in patients with Parkinson’s disease: a single-center pilot study. BMC Neurol. (2020) ; 20: (1): 340. |
[30] | Lee S, Bohplian S, Bronas UG. Accelerometer Use to Measure Physical Activity in Older Adults With Coronary Artery Disease: An Integrative Review. J Cardiovasc Nurs. (2022) Dec 22. |
[31] | Shin S, An D, Yoo W. Effects of Differences in Visual Acuity on Gait Time and Trunk Acceleration When Older Women Negotitate Stairs. European Geriatric Aledicine. (2016) ; 7: : 538-542. |
[32] | Liu YY, Yoo WG. Effects of lower trunk movement in flat-back syndrome during stair climbing: A technical note. Technol Health Care. (2022) ; 30: (2): 483-489. |
[33] | Jeong HJ, Kim BJ. The effect of thoracic joint mobilization on the changes of the thoracic kyphosis angle and static and dynamic balance. Biomed Sci Lett. (2019) ; 25: (2): 149-158. |
[34] | Greendale GA, Nili NS, Huang MH, Seeger L, Karlamangla AS. The reliability and validity of three non-radiological measures of thoracic kyphosis and their relations to the standing radiological Cobb angle. Osteoporos Int. (2011) ; 22: (6): 1897-1905. |
[35] | Lee JH, Jeon HS, Kim JH, Park JH, Yoon HB. Immediate effects of the downhill treadmill walking exercise on thoracic angle and thoracic extensor muscle activity in subjects with thoracic kyphosis. Phys Ther Korea. (2019) ; 26: (2): 1-7. |
[36] | Herzeele MV, Cingel RV, Maenhout A, Mey KD, Cools A. Does the application of kinesiotape change scapular kinematics in healthy female handball players? Int J Sports Med. (2013) ; 34: (11): 950-955. |
[37] | Lee JH, Yoo WG. Application of posterior pelvic tilt taping for the treatment of chronic low back pain with sacroiliac joint dysfunction and increased sacral horizontal angle. Phys Ther Sport. (2012) ; 13: (4): 279-285. |
[38] | Jang HJ, Hughes LC, Oh DW, Kim SY. Effects of corrective exercise for thoracic hyperkyphosis on posture, balance, and well-being in older women: A double-blind, group-matched design. J Geriatr Phys Ther. (2019) ; 42: (3): E17-27. |
[39] | Mirafzal SF, Sokhangnee Y, Sadeghi H. The effect of a combination of corrective exercise and spinal taping on balance in kyphotic adolescent. SSQ. (2011) ; 2: (2): 18-24. |
[40] | Katzman WB, Harrison SL, Fink HA, Marshall LM, Orwoll E, Elizabeth BC, et al. Physical function in older men with hyperkyphosis. J Gerontol A Biol Sci Med Sci. (2015) ; 70: (5): 635-640. |
[41] | Cho KJ, Kim YT, Seo BH, Shin JS. Radiological evaluation and classification of adult spinal deformity. J Korean Orthop Assoc. (2016) ; 51: (1): 1-8. |
[42] | Moore MK. Upper crossed syndrome and its relationship to cervicogenic headache. J Manipulative Physiol Ther. (2004) ; 27: (6): 414-420. |
[43] | Raine S, Twomey LT. Head and shoulder posture variations in 160 asymptomatic women and men. Arch Phys Med Rehabil. (1997) ; 78: (11): 1215-1223. |
[44] | Szczygieł E, Wȩglarz K, Piotrowski K, Mazur T, Mȩtel S, Golec J. Biomechanical influences on head posture and the respiratory movements of the chest. Acta Bioeng Biomech. (2015) ; 17: (2): 143-148. |
[45] | Lee JH. Effects of forward head posture on static and dynamic balance control. J Phys Ther Sci. (2016) ; 28: (1): 274-277. |
[46] | Jung SI, Lee NK, Kang KW, Kim K, Lee DY. The effect of smartphone usage time on posture and respiratory function. J Phys Ther Sci. (2016) ; 28: (1): 186-189. |
[47] | Singla D, Veqar Z. Association between forward head, rounded shoulders, and increased thoracic kyphosis: A review of the literature. J Chiropr Med. (2017) ; 16: (3): 220-229. |


