
Efficacy of percutaneous needle electrolysis versus dry needling in musculoskeletal pain: A systematic review and meta-analysis
Abstract
BACKGROUND:
Physical therapists use dry needling (DN) and percutaneous needle electrolysis (PNE) to treat musculoskeletal pain.
OBJECTIVE:
To investigate the efficacy of PNE vs. DN in the treatment of musculoskeletal pain.
METHODS:
This systematic review and meta-analysis was based on the PICOS and PRISMA protocols. The PubMed, PEDro, Cochrane Library, SCOPUS, and Google Scholar databases were searched for randomized clinical trials measuring pain intensity in various musculoskeletal syndromes using PNE and DN. Pain outcome measures were the visual analog scale or the numerical pain rating scale. Risk of bias was assessed according to Cochrane guidelines and quality of evidence was reported using the Grading of Recommendations Assessment, Development, and Evaluation approach (GRADE). Standardized mean differences were calculated using random effects models.
RESULTS:
The meta-analysis of the six included studies showed that the overall effect of PNE vs. DN for pain reduction was statistically significant at
CONCLUSIONS:
Moderate-quality evidence showed that PNE is slightly more effective than DN in reducing pain. However, because the results were not clinically significant, we cannot recommend the application of PNE over DN. More high-quality studies comparing the two interventions are needed to draw firm conclusions.
1.Introduction
Musculoskeletal pain is defined as pain affecting the bones, muscles, ligaments, tendons, and joints [1]. It can be classified as acute or chronic and can be localized in one area or generalized, i.e., involving the whole body. Typical examples of musculoskeletal pain are low back pain, neck pain, pain related to fractures, other injuries, osteoarthritis, as well as pain caused by rheumatoid arthritis [2]. Musculoskeletal pain reduces the functional ability of the patient with direct health implications. Musculoskeletal conditions with relevant pain have been shown to increase the risk of chronic disease in the general population [3]. In addition, musculoskeletal pain has also been blamed for economic, social, and psychological impacts [4, 5, 6].
According to the World Health Organization, 20–33% of the global population (1.75 billion people) has some form of chronic musculoskeletal pain [7, 8]. A recent study found the prevalence of musculoskeletal pain in Europe to be 35.7% (28.8–31.7), while it was higher in women 41.3% (40.2–42.4) than in men 29.1% (28.0–30.3) [7].
Modern guidelines for the treatment of musculoskeletal pain state that the patient-centered approach as well as the early diagnosis and treatment of the cause of the pain are the commonly accepted treatment strategies [9]. Physical therapy through the application of therapeutic exercise, manual techniques and physical means has been shown to significantly contribute to the reduction of musculoskeletal pain [1, 10].
A technique that has been found to significantly reduce musculoskeletal pain is dry needling (DN), which is used to treat myofascial trigger points (TrPs). TrPs have been described by Travell and Simons as painful palpable nodules located along a tense muscle fascicle on the belly of the muscle [11, 12]. Their presence has been found to be greatly increased in patients with musculoskeletal pain [13]. Acute overload, chronic repetitive strain, poor static posture, unsuitable sleeping positions, and poor ergonomic practices can all lead to TrPs. These TrPs can interfere with muscle function and produce severe discomfort [14]. The use of DN to treat myofascial pain has been known for decades. Travell and Simons suggested local infusion of anesthetic blocks into the TrPs as the treatment of choice [12], while Lewit investigated anesthetic injections in patients with chronic pain and argued that it was the needle and not the infiltration of the anesthetic that caused pain relief [14, 15]. Although DN is widely used in physical therapy, its potential physiological effects are not yet fully understood [16]. According to some researchers, needle insertion into muscle tissue can disrupt dysfunctional motor end plates, increase sarcomere length, and reduce the overlap between actin and myosin filaments while reducing both peripheral and central sensitization, removing the source of peripheral pain, modulating activity of the dorsal horn of the spinal cord, and activating central inhibitory pain pathways [17]. Regarding the biochemical effect, DN was found to have an effect on the pain of an MTrP by reducing the concentration of substance
Another technique that has also shown positive effects in the treatment of musculoskeletal pain is percutaneous needle electrolysis (PNE). It consists of the application of a continuous galvanic current which reaches the target organ through a needle that acts as a negative electrode and which is guided with the help of ultrasound to the target tissue [19, 20]. The aim of this technique is to cause a non-thermal electrolytic reaction in the affected tissue through the cathodic flow of the needle in order to create a controlled inflammatory response [21], which will result in the facilitation of phagocytosis and tissue regeneration [19]. The technique combines the mechanical effect resulting from the insertion of the needle and the biological effect resulting from the application of the galvanic current [22].
Several researchers have attempted to compare the effectiveness of DN and PNE in the treatment of musculoskeletal pain [20, 22, 23, 24, 25]. However, to date there is no systematic review and meta-analysis that has compared the two techniques. The use of PNE continues to increase around the world without being proven to offer anything more than DN, which is already popular in the physical therapy field. The aim of this systematic review and meta-analysis is to ascertain whether PNE is more effective than DN in the treatment of musculoskeletal pain.
2.Method
2.1Design
This systematic review and meta-analysis was performed in accordance with PRISMA guidelines [26]. The international Prospective Register of Systematic Reviews (PROSPERO) registration number was CRD42022360228.
2.2Search strategy
A Technical Expert Panel was established by 10 physical therapists to conduct the search and evaluation of the articles in the databases. A systematic, non-time-limited literature search was performed in the online databases PubMed, PEDro, Cochrane Library, SCOPUS, and Google Scholar, and completed on August 1
Table 1
Article search strategy
| Database | Search strategy |
| PubMed Scopus PEDro Cochrane library Google scholar | (ultrasound-guided percutaneous electrolysis OR percutaneous needle electrolysis OR intratissue percutaneous electrolysis OR ultrasound-guided galvanic electrolysis) AND (dry needling OR dry needle) AND (Pain OR Myofascial Pain) |
2.3Eligibility criteria and study selection
The selection criteria for this systematic review were developed according to the PICOS framework [27]. The following elements were used to develop a search strategy in the archive databases and in subsequent stages of article selection:
Population: The sample in this study was adults with musculoskeletal pain. Patients were over 18 years of age without any other age restriction. Studies involving patients with neuropathic pain or pain associated with neurological disorders were excluded. Patients with underlying systemic medical conditions causing pain such as infections, neoplasms, and metastases were also excluded from our systematic review.
Intervention: The intervention consisted of any form of PNE (i.e., application of direct galvanic current with a needle). Other interventions using pulsed current, such as percutaneous electrical nerve stimulation (PENS) or electroacupuncture were not included. For this purpose, the search strategy included the following keywords: ultrasound-guided percutaneous electrolysis OR percutaneous needle electrolysis OR intratissue percutaneous electrolysis OR ultrasound-guided galvanic electrolysis.
Control: Acceptable comparison groups were only those treated with DN. Therefore, studies that had at least one control group consisting of DN were included. Other interventions using acupuncture based on Chinese techniques were excluded from this study. Therefore, the search strategy included the following keywords: dry needling OR dry needle.
Outcomes: The main and only primary outcome measure that had to be present in the included studies was pain. Pain intensity had to be measured with the Visual Analog Scale (VAS) or the Numerical Pain Rating Scale (NPRS). Studies that assessed other outcome measures were included in this review if they investigated pain as a secondary outcome. Studies with a VAS or NPRS score lower than three were excluded.
2.4Screening, selection process, and data extraction
The studies found from the various databases were examined independently by two reviewers. First, duplicate studies were eliminated using the Mendeley program. Then, the title and abstract of the studies were reviewed for suitability. If they met the criteria, the full text of the study was retrieved and read, for further consideration of its suitability. The authors had to reach a common ground about the studies to be included in this review. In case of disagreement between the two reviewers, a third party was involved in the process to reach a consensus and decide whether the study should be included. Data from each trial were extracted by two authors into a standardized form and included study design, sample size, population diagnosis, interventions used, outcomes, and follow-up periods. Finally, the two reviewers had to reach consensus on each item on the data extraction form. If there was a disagreement, a third reviewer made the final decision.
2.5Assessment of methodological quality and risk
Using the Cochrane Risk of Bias (RoB) assessment tool [28] and the PEDro scale [29] two members of the research team assessed the methodological quality and risk of bias in the included studies.
The RoB tool includes the following types of bias: selection bias (randomization sequence generation, allocation concealment), performance bias (blinding participants, blinding therapists), detection bias (blinding outcome assessor), attrition bias (incomplete outcome data), reporting bias (source of funding bias or selective outcome reporting), and other bias (sample size) [30]. Each point was classified as low risk, high risk, or unclear according to the Cochrane Collaboration tool [30]. For an article to be assessed as low risk, all key areas had to be assessed as being at low risk of bias. If all key areas were unclear risk of bias, the article was identified as unclear risk. If one or more key areas within the study were assessed as high risk, the included study was then determined to have a high risk.
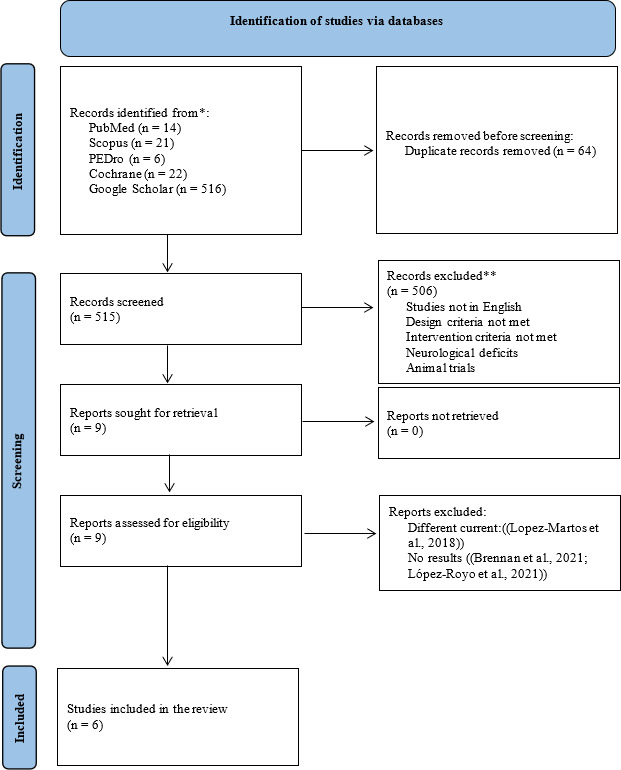
Figure 1.
Identification of studies via databases.
The PEDro scale is based on 11 criteria, 10 of which contribute to the overall score of a study. The first criterion was not included in the score as it relates to the external validity of the study. The scale assesses the following criteria: random allocation, concealed allocation, between-group similarity at baseline, participant blinding, therapist blinding, assessor blinding, dropout rate, intention-to-treat statistical analysis, between-group statistical comparison, and point measures and variability data [29]. According to Cashin and McAuley [31], if the authors of a study report an overall PEDro scale score of 0–3 this is considered “poor”, 4–5 “moderate”, 6–8 “good”, and 9–10 “excellent”. However, it is important to note that these classifications have not been validated. Furthermore, for trials evaluating complex interventions (e.g., exercise) an overall PEDro score of 8/10 is optimal [31]. In this meta-analysis a score of 6/10 and above on the PEDro scale was considered a high-quality study, based on corresponding systematic reviews and meta-analyses [19].
2.6Quality of evidence
Table 2
Characteristics of participants of the included studies
| Study | Musculoskeletal disorder | Groups | Participants | Gender, Men (Women) | Age | Pain duration |
|---|---|---|---|---|---|---|
| Rodríguez-Huguet et al. [22] | Supraspinatus tendinopathy | G | 18 | 16 (2) | 39.17 | Not reported |
| G | 18 | 11 (7) | 40.92 | |||
| Rodríguez-Huguet et al. [41] | Lateral epicondylalgia | G | 16 | 10 (6) | 40.44 | Not reported |
| G | 16 | 10 (6) | 35.88 | |||
| Lopez-Martos et al. [40] | Temporomandibular pain | G | 20 | 5 (15) | 37.83 | |
| G | 20 | 2 (18) | 36.65 | |||
| G | 20 | 1 (19) | 42.22 | |||
| Al-Boloushi et al. [23] | Plantar pain | G | 51 | 15 | 48.1 | |
| G | 51 | 15 | 49.5 | |||
| López-Royo et al. [25] | Patellar tendinopathy | G | 16 | 14 (2) | 31.3 | |
| G | 16 | 13 (3) | 33.2 | |||
| G | 16 | 15 (1) | 32.7 | |||
| Valera-Calero et al. [42] | Patellar pain syndrome | G | 5 | Not reported | 25.4 | Not reported |
| G | 5 | 26.8 | ||||
| G | 5 | 24.8 |
To evaluate the quality of evidence of PNE as well as DN, the Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) approach was used [32]. This assessment was performed independently by two authors, with a third author available if the two authors could not reach agreement. The quality of evidence was classified as high, moderate, low, or very low based on the presence of study limitations (downgraded if the bias according to RoB was large), indirectness of evidence, inconsistency of results or unexplained heterogeneity (downgraded if significant heterogeneity was presented by visual inspection of I
2.7Data synthesis and analysis
Our meta-analysis was performed using the statistical software Review Manager (RevMan version 5.4). Data synthesis was categorized by group according to the follow-up period as short-term (less than one month), intermediate (1–3 months), and long-term (3–6 months) if data were available. The data extracted from each study were the sample size, mean value, and standard deviation of each variable. It is important to note that when the study contained only standard bias, these were converted to standard deviations. Furthermore, if the study reported a non-parametric value (median and interquartile range), it was converted to mean value and standard deviation [33, 34].
Regarding the pain intensity outcome, using either the NPRS scale or the VAS, we calculated the mean difference between the PNE group and the DN group and converted it to a Standardized Mean Difference (SMD) as it has been reported that this allows the evaluation of studies that use different outcome measures to evaluate the same outcome [35]. A random-effects model was used to determine the overall SMD. An SMD effect size of 0.8 or greater was considered large, between 0.5 and 0.8 was considered moderate, and between 0.2 and 0.5 was considered small [36]. In general, P values less than 0.05 were considered statistically significant. Overall effect sizes and effect size calculations on pain intensity were obtained at short-term (0–1 months), medium-term (1–3 months), and long-term (3–6 months).
Heterogeneity of studies was assessed using the I
3.Results
3.1Search results
Table 3
Parameters of the treatments in the included clinical studies
| Study | Group | Number of insertions | Approach | Diameter (mm) | Depth (mm) | Duration | Current intensity | Device |
|---|---|---|---|---|---|---|---|---|
| Rodríguez-Huguet et al. [22] | G | 1 | The needle acting as a cathode targeted the supraspinatus tendon. The technique was according to US guidelines. | Not reported | Not reported | 1.2 minutes 1 week/ 4 weeks | 350 | EPTE |
| G | Not reported | Needling on the upper part of the trapezius towards the supraspinatus. | Not reported | Not reported | 1 week/ 4 weeks | – | – | |
| Rodríguez-Huguet et al. [41] | G | 1 | The needle acting as a cathode was aimed at the tendon ending in the lateral condyle. The technique was according to US guidelines. | 0.3mm | Not reported | 1.2 minutes 1 week/ 4 weeks | 350 | EPTE |
| G | 1 | Needling on the supinator and the extensor carpi brevis. | Not reported | Not reported | 1 week/ 4 weeks | – | – | |
| Lopez-Martoset al. [40] | G | 1 | The needle acting as a cathode was aimed at the lateral pterygoid. | 0.25 | 40 | 3 seconds 1 week/ 3 weeks | 2 mA | EPI Advanced Medicine |
| G | 1 | Needling on a trigger point on the lateral pterygoid. | 0.25 | 40 | 1 week/ 3 weeks | – | – | |
| G | 1 | Pressing of the needle into the skin with a protective plastic. | 0.25 | 40 | 1 week/ 3 weeks | – | – | |
| Al-Boloushi et al. [23] | G | Not reported | The needle acted as a cathode on all trigger points found. | 0.25–0.30 mm | 30–75 mm | 5 seconds 4 sessions/ 1 week | 1.5 mA | Physio Invasiva, PRIM Fisiotherapia, Spain |
| G | Not reported | Needling on all trigger points. The technique was as described by Hong. | 0.25–0.30 mm | 30–75 mm | 5 seconds 4 sessions/ 1 week | – | – | |
| López-Royo et al. [25] | G | Not reported | The technique was according to US guidelines. | Not reported | Not reported | 3 seconds 4 sessions every 2 weeks for 8 weeks | 3 mA | Not reported |
| G | 3 | Not reported. The technique was according to US guidelines. | 0.25mm | 25mm | 3 seconds 4 sessions every 2 weeks for 8 weeks | – | – | |
| G | 1 | The needle was placed in a specific sheath and manipulated during the intervention to simulate a real treatment. | 0.25mm | 25mm | 3 seconds 4 sessions every 2 weeks for 8 weeks | – | – | |
| Valera-Calero et al. [42] | G | 1 | The needle acting as a cathode was aimed at a trigger point of the rectus femoris. | 0.30 mm | 40 mm | 10 seconds 1 session | 660 mA | EPTE |
| G | 1 | The needle acting as a cathode was aimed at a trigger point of the rectus femoris. | 0.30 mm | 40 mm | 10 seconds 1 session | 220 mA | EPTE | |
| G | 1 | Needling on trigger point of the rectus femoris. | 0.30 mm | 40 mm | 30 seconds 1 session | – | – |
A total of 579 articles related to our topic were found from the search. After removing duplicates, 515 studies remained. After a thorough review of their titles and abstracts, nine related articles remained for further full-text screening. The full article was then accessed and three articles were removed as two of them had no final results [24, 38] and one [39] used pulsed current. Finally, a total of six articles were included in the qualitative and quantitative analysis of our review [22, 23, 25, 40, 41, 42]. The study selection flow diagram is shown in Fig. 1.
3.2Characteristics of studies
Participant characteristics of the included studies are listed in Table 2. The included studies were highly heterogeneous as they studied different musculoskeletal conditions. These were tendinopathy of the supraspinatus [43], lateral epicondylalgia [41] temporomandibular pain [40], plantar pain [23], patellar tendinopathy [25], and patellar pain syndrome [42].
Table 4
The effects of percutaneous needle electrolysis and dry needling on musculoskeletal pain
| Study | Intervention | Sample | Intervention duration, sessions or weeks | Comparison and outcome measure | Between-groups differences (95% CI) [SMD] |
|---|---|---|---|---|---|
| Rodríguez-Huguet et al. [22] | G | 1818 | 1 | Pain (NPRS) G | 4 weeks: |
| Rodríguez-Huguet et al. [41] | G | 16 16 | 1 | Pain (NPRS) G | 4 weeks: |
| Lopez-Martos et al. [40] | G | 20 20 20 | 1 | Pain at rest (VAS) G | G |
| Al-Boloushi et al. [23] | G | 51 51 | 4 | Mean pain (VAS) G | 4 weeks: 1.20 (0.13. 2.27) [0.43] 8 weeks: 0.50 ( |
| López-Royo et al. [25] | G | 16 16 16 | 4 every 2 weeks | Mean pain (VAS) G | G |
| Valera-Calero et al. [42] | G | 5 5 5 | 1 | Pain (VAS) G | G |
Table 5
Methodological rating of randomized clinical trials using the PEDro baseline scale
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Al-Boloushi et al. [23] | Y | Y | Y | N | N | Y | N | Y | Y | Y | 7 |
| López-Royo et al. [25] | Y | N | N | N | N | Y | Y | Y | N | Y | 5 |
| Lopez-Martos et al. [40] | Y | N | Y | N | N | N | Y | Y | Y | Y | 6 |
| Rodríguez-Huguet et al. [41] | Y | Y | Y | N | N | Y | Y | N | Y | Y | 7 |
| Rodríguez-Huguet et al. [22] | Y | Y | N | N | N | N | Y | Y | Y | Y | 6 |
| Valera-Calero et al. [42] | Y | Y | Y | Y | Y | Y | Y | Y | Y | Y | 10 |
Y
All included clinical studies applied PNE and DN, but there was great heterogeneity between them, in terms of number or frequency of sessions, session time, PNE current intensity, needle depth and diameter, and combined therapy. A summary of the PNE and DN parameters applied in each study can be found in Table 3. Table 4 summarizes the main results of each of the included studies.
3.3Methodological quality
Methodological quality scores ranged from five to 10 (mean
3.4Risk of systematic error
Figure 2.
Risk of systematic error charts.
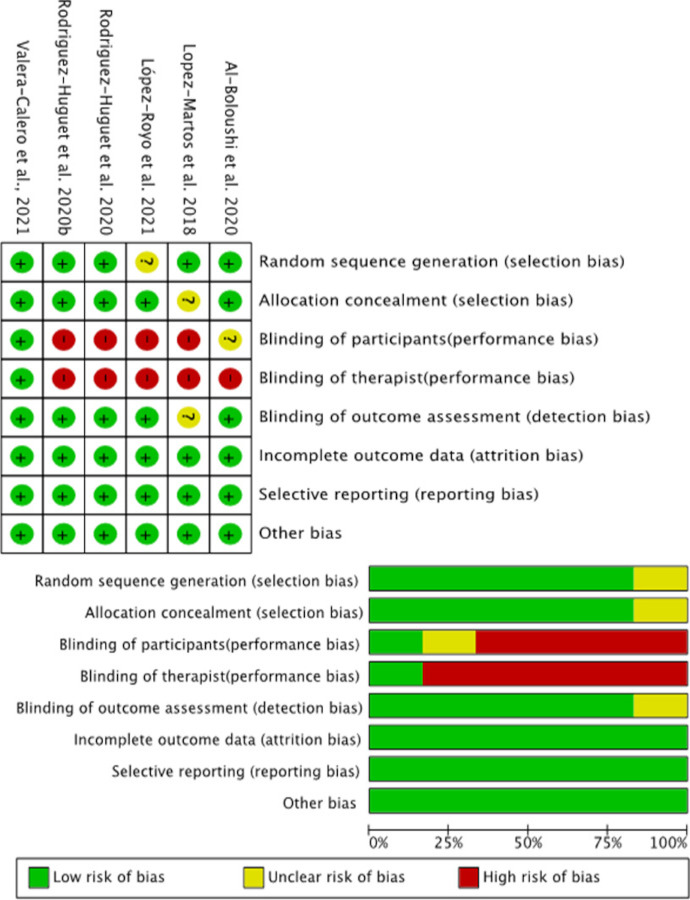
Details of the assessment of the risk of bias of the included studies are shown in Fig. 2. In general, the risk of bias of the studies included in this meta-analysis was low, apart from blinding of patients and therapists. Only one clinical trial was able to blind patients and therapists [42] while the others had a significant risk of blinding patients and therapists.
3.5Effects of PNE vs. DN on pain
Figure 3.
Comparison (mean difference) of the effects of percutaneous electrolysis versus dry needling on pain intensity.
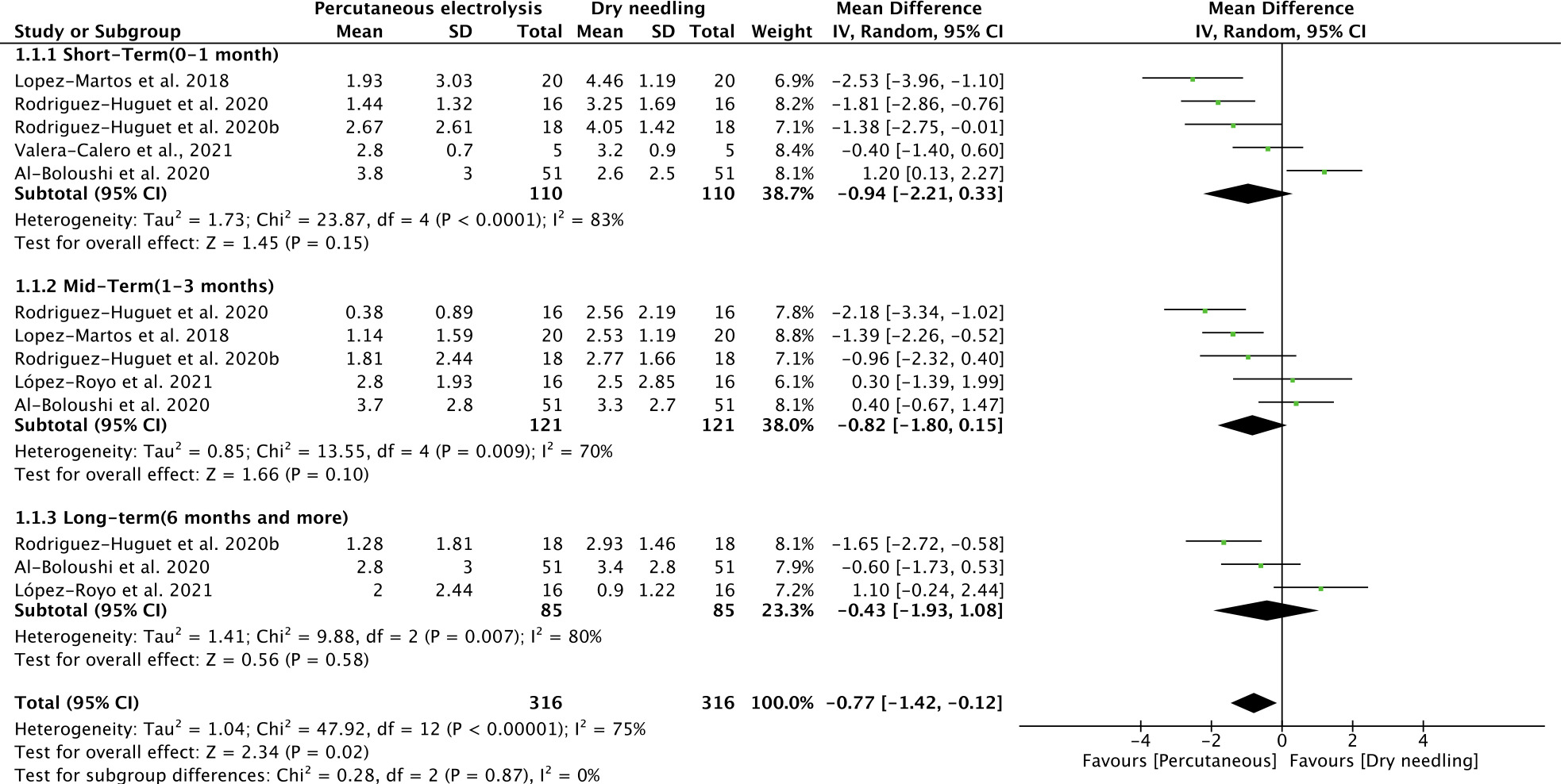
Table 6
GRADE evidence for percutaneous needle electrolysis and dry needling in pain intensity
| Number of studies | Risk of bias | Inconsistency | Indirectness of evidence | Imprecision | Publication bias | Quality of evidence | MD or SMD (95% CI) |
| Percutaneous electrolysis versus dry needling in pain intensity | |||||||
| Overall effects, ( | No | Serious (i | No | No | No | Moderate | |
| Short | No | Serious (i | No | No | No | Moderate | |
| Mid | No | Serious (i | No | No | No | Moderate | |
| Long | No | Serious (i | No | Serious | Yes | Low | |
GRADE
Figure 4.
Comparison (standardized mean difference) of the effects of percutaneous electrolysis versus dry needling on pain intensity.
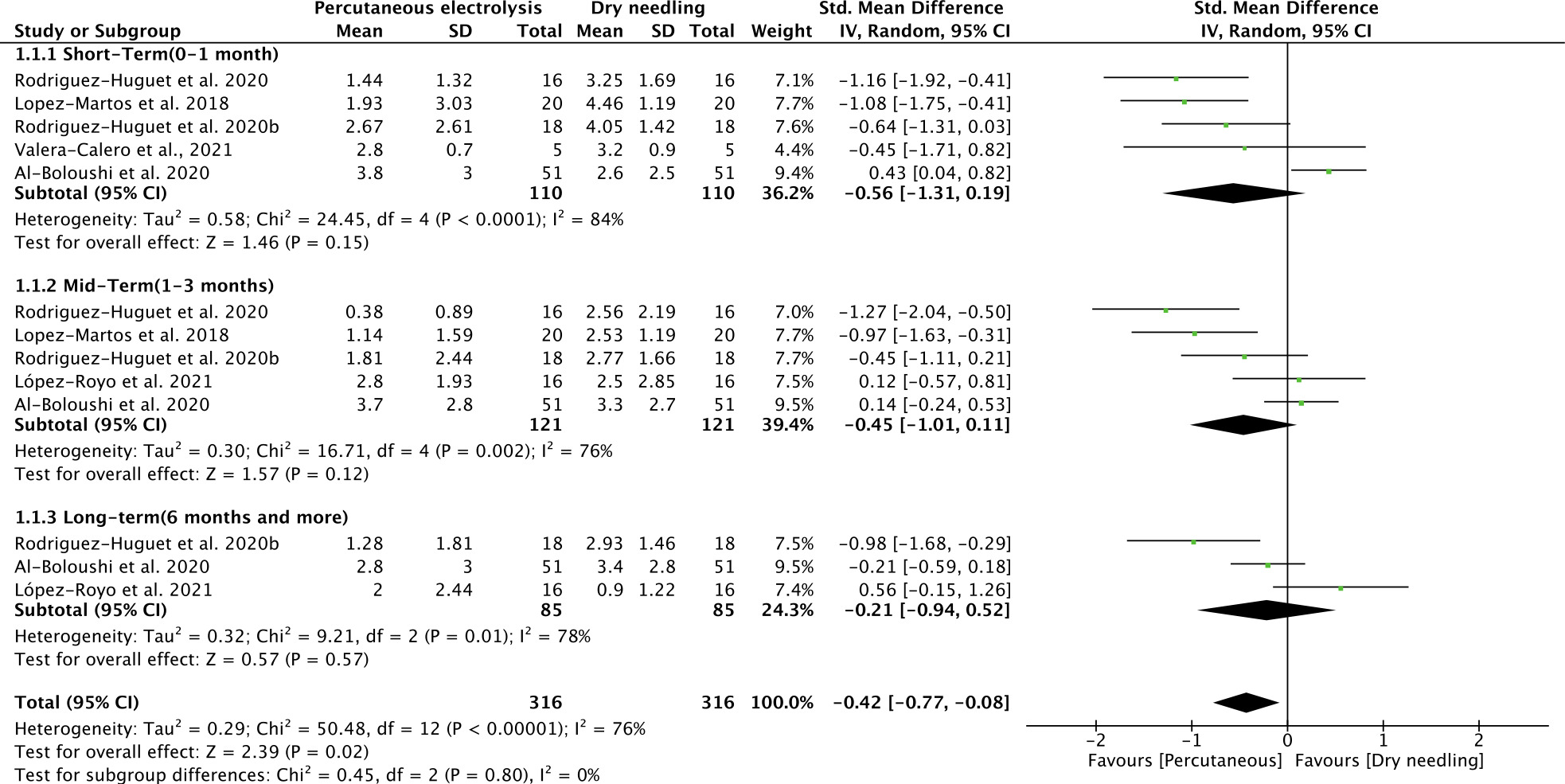
The meta-analysis (Figs 3 and 4) showed that only the overall effect of PNE vs. DN for pain reduction was statistically significant (
3.6Quality of evidence (GRADE)
Table 6 lists the details of the GRADE assessment. Severe heterogeneity, imprecision, and publication bias lowered the quality level of our studies to a moderate degree regarding the overall effect of PNE or DN on musculoskeletal pain.
4.Discussion
The aim of this meta-analysis was to compare the efficacy of PNE and DN in the treatment of musculoskeletal pain. A total of six studies involving 252 patients were included in the analysis. The results provided moderate-quality evidence that PNE has a slightly better effect on pain reduction than DN. Through the GRADE assessment, the resulting evidence was of moderate level due to heterogeneity (inconsistency) and inaccuracy (imprecision). It is important to mention that the results in the field of long-term intervention were of a low level as, in addition to the aforementioned, publication bias was serious, further reducing the level of quality.
This is the first meta-analysis to analyze and compare the effect of PNE vs. DN on musculoskeletal pain intensity. After a thorough search, the systematic reviews found to study the effect of PNE on musculoskeletal pain were only those of Gómez-Chiguano et al. [19] and Varela Rodríguez et al. [44], while as far as DN is concerned the reviews we found were those of Gattie et al. [11], Sánchez-Infante et al. [45], and Jackson et al. [46]. We were thus unable to directly compare the efficacy of the two techniques based on the findings of these reviews.
Percutaneous electrolysis is a new therapeutic intervention in the world of physical therapy, different from PENS and electroacupuncture, proposed for the treatment of pain. In contrast, DN has been used by physical therapists for more years and its effects have clearly been more studied [47]. We found that PNE was more effective in the short, medium, and long term in pain relief than DN. However, statistically significant pain relief effects were found only in the overall effect of PNE and not in the short, medium, and long term. Therefore, we cannot report the results as statistically significant.
Four clinical trials (83.33% of the included studies) in addition to PNE and DN used another intervention, such as eccentric exercises [22, 25, 41] stretching [23] and concentric exercises [42], while only one trial (16.66%) analyzed the effects of PNE and DN separately [42]. Most clinical trials (66.66%) reported differences in pain in favor of PNE compared to DN [22, 40, 41, 42], while only two studies reported positive results in favor of DN [23, 25]. Regarding the number of intervention groups, four out of six clinical studies [22, 23, 40, 41] had two groups (one intervention and one control), while in two [25, 42] there was another intervention group of placebo needle.
Regarding the clinical significance of the statistically significant changes in the overall effect, we observed a mean reduction in pain intensity of marginally less than one point at short-term, medium-term, and long-term follow-up, with a decrease in the overall mean score of
In conclusion, the results of the systematic review showed that PNE, despite having statistically significant differences, was clinically insufficient.
The mechanism due to which PNE seems to have a greater analgesic effect than DN is not entirely clear to us as it is influenced by several factors. However, its analgesic effect is based on non-thermal action of the damaged area, which produces a controlled local inflammatory response activating phagocytosis and favouring the regeneration of soft tissues [49]. It is also possible that the analgesic mechanism of PNE works at the molecular level. More specifically, a study demonstrated that PNE can activate a large number of factors generated during an active inflammation thus facilitating proper phagocytosis and regeneration of damaged tissue [21]. Finally, another possible mechanism of action of PNE is at a neurophysiological level. Ronzio et al. [50] found that the pain threshold of the PNE group was significantly increased compared to the placebo group (needle insertion without electric current), thus suggesting that PNE may have a direct effect on pain regulation. Other studies that can justify these results are those of de la Cruz Torres et al. [51] as well as García Bermejo et al. [52, 53], who found parasympathetic activation of the autonomic nervous system during application of PNE.
The other possible scenario in which the positive results in favor of PNE are superimposed are the better experimental protocols used in the included studies, the adequacy of follow-up, the treatment area on the body, and the incorrect application of DN.
Regarding the safety of the application of PNE, it is worth noting that only three of the included studies reported whether there were adverse effects [23, 40, 42], with the only adverse effect being the presence of hematoma in one patient [40]. Therefore, it can be said that PNE appears to be a safe therapeutic intervention. However, this issue needs to be further explored in future research.
Therefore, it is necessary to further study different ways of treatment for musculoskeletal pain. Evidence suggests that one similar method using electrical current (PENS) is effective in treating musculoskeletal pain [54]. The PENS method shares the same logic as dry needling with the only difference being that the electrical current is pulsed. Beyond PENS, manual therapy and exercise appeared to be effective in managing musculoskeletal pain [55].
In conclusion, another possible subject for a future meta-analysis would be a comparison between percutaneous electrolysis, dry needling, and electroacupuncture (PENS) without combining them with any other therapeutic intervention to assess whether the positive results of transdermal electrolysis are due to its mechanisms and not to the electric current or to the other therapeutic intervention it was combined with. However, appropriate clinical trials are also required as there is no relevant clinical trial in the online literature to investigate and fully understand the three means of intervention.
4.1Strengths and limitations
Even though this is the first meta-analysis to compare the effects of PNE with DN on pain, the results should always be considered under the umbrella of the potential benefits and limitations found therein. The strengths of this systematic review are the most informative question (PICO), comprehensive literature search performed in multiple scientific search engines, methodological soundness, proper data extraction, rigorous statistical analysis, and inclusion of high-quality randomized controlled trials in the quantitative analysis. Aside from the strengths, this systematic review contained several limitations that may have affected our results.
Firstly, the number of randomized controlled trials examining the effects of PNE on musculoskeletal pain was relatively small, with one clinical trial being pilot and with a small number of patients (
4.2Clinical recommendations
This meta-analysis found a fair amount of evidence to support a superior effect of PNE over DN on general musculoskeletal pain. However, this should be considered with caution as we do not know whether PNE could be beneficial in certain subgroups of patients with musculoskeletal pain as the painful areas included in this meta-analysis were heterogeneous. All that can be stated with certainty is that in cases where the musculoskeletal pain was due to tendon involvement, patients could benefit from PNE, as this intervention was originally developed for the management of chronic tendinopathy [56]. However, in this meta-analysis most of the clinical trials included musculoskeletal pain conditions where the tendon was partially (lateral epicondylalgia) or completely (plantar pain, patellar pain syndrome, patellar tendinopathy, supraspinatus tendinopathy) involved in the symptoms.
One of the most important issues to consider for the correct clinical application of PNE is the appropriate parameters (i.e., treatment duration, current intensity, number of sessions). For this reason, further studies should be conducted to draw safe conclusions. Because of the limited data we have, we cannot determine which treatment parameters are most effective for the application of PNE in all forms of pain. Only one study [42] compared two different intensities of electric current and concluded that at both intensities the results were equally beneficial. Future studies should investigate which are the most appropriate treatment parameters of transdermal electrolysis for the management of different musculoskeletal pain conditions.
5.Conclusions
Based on the GRADE approach and low- to mode-rate-quality evidence from studies involving a variety of musculoskeletal conditions, PNE was shown to have a marginally more positive effect on pain reduction than DN. However, our results were not clinically and statistically significant so we cannot recommend the application of PNE in place of DN. More high-quality studies comparing the two interventions are needed to draw firm conclusions about which of the two is the gold standard in the management of musculoskeletal pain.
Ethical approval
Not applicable.
Funding
The authors report no funding.
Informed consent
Not applicable.
Author contributions
Conceptualization, methodology, and writing (original draft preparation, review and editing): C.F., P.I., D.L., K.K., G.K., S.R.N., A.K., I.P.C., P.C., T.A. Formal analysis and approve final manuscript: T.A., I.P.C., G.K., all authors have read and agreed to the published version of the manuscript.
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | El-Tallawy SN, Nalamasu R, Salem GI, LeQuang JAK, Pergolizzi JV, Christo PJ. Management of Musculoskeletal Pain: An Update with Emphasis on Chronic Musculoskeletal Pain. Pain Ther. (2021) Jun 11; 10: (1): 181-209. doi: 10.1007/s40122-021-00235-2. |
[2] | Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. (2020) ; 396: (10267): 2006-17. doi: 10.1016/S0140-6736(20)32340-0. |
[3] | Williams A, Kamper SJ, Wiggers JH, O’Brien KM, Lee H, Wolfenden L, et al. Musculoskeletal conditions may increase the risk of chronic disease: A systematic review and meta-analysis of cohort studies. BMC Med. (2018) ; 16: (1): 1-9. |
[4] | Crofford LJ. Psychological aspects of chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. (2015) Feb; 29: (1): 147-55. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1521694215000340. |
[5] | Henschke N, Kamper SJ, Maher CG. The Epidemiology and Economic Consequences of Pain. Mayo Clin Proc. (2015) Jan; 90: (1): 139-47. Available from: https://linkinghub.elsevier.com/eve/pii/S0025619614008659. |
[6] | Bevan S. Economic impact of musculoskeletal disorders (MSDs) on work in Europe. Best Pract Res Clin Rheumatol. (2015) Jun; 29: (3): 356-73. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1521694215000947. |
[7] | Cimas M, Ayala A, Sanz B, Agulló-Tomás MS, Escobar A, Forjaz MJ. Chronic musculoskeletal pain in European older adults: Cross-national and gender differences. Eur J Pain. (2018) Feb 12; 22: (2): 333-45. doi: 10.1002/ejp.1123. |
[8] | Word Health Organization. Musculoskeletal health. (2022) . Available from: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions. |
[9] | Lin I, Wiles L, Waller R, Goucke R, Nagree Y, Gibberd M, et al. What does best practice care for musculoskeletal pain look like? Eleven consistent recommendations from high-quality clinical practice guidelines: Systematic review. Br J Sports Med. (2020) ; 54: (2): 79-86. |
[10] | Mannerkorpi K, Henriksson C. Non-pharmacological treatment of chronic widespread musculoskeletal pain. Best Pract Res Clin Rheumatol. (2007) ; 21: (3): 513-34. |
[11] | Gattie E, Cleland JA, Snodgrass S. The Effectiveness of Trigger Point Dry Needling for Musculoskeletal Conditions by Physical Therapists: A Systematic Review and Meta-analysis. J Orthop Sport Phys Ther. (2017) Mar; 47: (3): 133-49. doi: 10.2519/jospt.2017.7096. |
[12] | Travell JG, Simons DG. Myofascial Pain and Dysfunction: The Trigger Point Manual. Volume 1. Upper Half of Body. Williams & Wilkins; (1999) . |
[13] | Barbero M, Schneebeli A, Koetsier E, Maino P. Myofascial pain syndrome and trigger points: evaluation and treatment in patients with musculoskeletal pain. Curr Opin Support Palliat Care. (2019) Sep; 13: (3): 270-6. doi: 10.1097/SPC.0000000000000445. |
[14] | Fogelman Y, Kent J. Efficacy of dry needling for treatment of myofascial pain syndrome. J Back Musculoskelet Rehabil. (2015) ; 28: (1): 173-9. |
[15] | Lewit K. The needle effect in the relief of myofascial pain. Pain. (1979) Feb; 6: (1): 83-90. Available from: http://journals.lww.com/00006396-197902000-00008. |
[16] | Cagnie B, Dewitte V, Barbe T, Timmermans F, Delrue N, Meeus M. Physiologic Effects of Dry Needling. Curr Pain Headache Rep. (2013) Aug 26; 17: (8): 348. doi: 10.1007/s11916-013-0348-5. |
[17] | Fernández-de-Las-Peñas C, Nijs J. Trigger point dry needling for the treatment of myofascial pain syndrome: current perspectives within a pain neuroscience paradigm. J Pain Res. (2019) Jun; Volume 12: : 1899-911. Available from: https://www.dovepress.com/trigger-point-dry-needling-for-the-treatment-of-myofascial-pain-syndro-peer-reviewed-article-JPR. |
[18] | Garcia-De-Miguel S, Pecos-Martin D, Larroca-Sanz T, Sanz-De-Vicente B, Garcia-Montes L, Fernandez-Matias R, et al. Short-term effects of PENS versus dry needling in subjects with unilateral mechanical neck pain and active myofascial trigger points in levator scapulae muscle: A randomized controlled trial. J Clin Med. (2020) ; 9: (6): 1-16. |
[19] | Gómez-Chiguano GF, Navarro-Santana MJ, Cleland JA, Arias-Buría JL, Fernández-de-las-Peñas C, Ortega-Santiago R, et al. Effectiveness of Ultrasound-Guided Percutaneous Electrolysis for Musculoskeletal Pain: A Systematic Review and Meta-Analysis. Pain Med. (2021) May 21; 22: (5): 1055-71. Available from: https://academic.oup.com/painmedicine/article/22/5/1055/5957438. |
[20] | Margalef R, Bosque M, Minaya-Muñoz F, Valera-Garrido F, Santafe MM. Safety analysis of percutaneous needle electrolysis: a study of needle composition, morphology, and electrical resistance. Acupunct Med. (2021) ; 39: (5): 471-7. |
[21] | Abat F, Valles SL, Gelber PE, Polidori F, Stitik TP, García-Herreros S, et al. Mecanismos moleculares de reparación mediante la técnica Electrólisis Percutánea Intratisular en la tendinosis rotuliana. Rev Esp Cir Ortop Traumatol. (2014) Jul; 58: (4): 201-5. |
[22] | Rodríguez-Huguet M, Góngora-Rodríguez J, Rodríguez-Huguet P, Ibañez-Vera AJ, Rodríguez-Almagro D, Martín-Valero R, et al. Effectiveness of Percutaneous Electrolysis in Supraspinatus Tendinopathy: A Single-Blinded Randomized Controlled Trial. J Clin Med. (2020) ; 9: (1837): 1-13. |
[23] | Al-Boloushi Z, Gómez-Trullén EM, Arian M, Fernández D, Herrero P, Bellosta-López P. Comparing two dry needling interventions for plantar heel pain: a randomised controlled trial. BMJ Open. (2020) Aug 20; 10: (8): e038033. doi: 10.1136/bmjopen-2020-038033. |
[24] | Gonzalez-Perez LM, Canivell-Zabaleta M, Rodriguez-Posada F, Caro-Jimenez MJ, Lopez-Martos R, Infante-Cossio P, et al. Study comparing intratissue percutaneous electrolysis, deep dry needling and botulinum toxin for the management of temporomandibular myofascial pain. Int J Oral Maxillofac Surg. (2019) May; 48: : 280. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0901502719309622. |
[25] | López-Royo MP, Ríos-Díaz J, Galá-Díaz RM, Herrero P, Gómez-Trullén EM. A Comparative Study of Treatment Interventions for Patellar Tendinopathy: A Randomized Controlled Trial. Arch Phys Med Rehabil. (2021) ; 102: (5): 967-75. |
[26] | Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. (2009) Jul 21; 6: (7): e1000097. doi: 10.1371/journal.pmed.1000097. |
[27] | Sterne JAC, Savovič J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. (2019) ; 366: : 1-8. |
[28] | Sterne JAC, Savovič J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) Aug 28; l4898: . doi: 10.1136/bmj.l4898. |
[29] | de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: a demographic study. Aust J Physiother. (2009) ; 55: (2): 129-33. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0004951409700431. |
[30] | Higgins JPT, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. (2011) Oct 18; 343: (2): d5928. doi: 10.1136/bmj.d5928. |
[31] | Cashin AG, McAuley JH. Clinimetrics: Physiotherapy Evidence Database (PEDro) Scale. J Physiother. (2020) Jan; 66: (1): 59. Available from: https://linkinghub.elsevier.com/retrieve/pii/S183695531930092X. |
[32] | Granholm A, Alhazzani W, Müller MH. Use of the GRADE approach in systematic reviews and guidelines. Br J Anaesth. (2019) Nov; 123: (5): 554-9. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0007091219306439. |
[33] | Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. (2014) Dec 19; 14: (1): 135. doi: 10.1186/1471-2288-14-135. |
[34] | Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. (2018) Jun 27; 27: (6): 1785-805. doi: 10.1177/0962280216669183. |
[35] | Takeshima N, Sozu T, Tajika A, Ogawa Y, Hayasaka Y, Furukawa TA. Which is more generalizable, powerful and interpretable in meta-analyses, mean difference or standardized mean difference? BMC Med Res Methodol. (2014) Dec 21; 14: (1): 30. doi: 10.1186/1471-2288-14-30. |
[36] | Cohen J. Statistical Power Analysis for the Behavioral Sciences. Routledge; (2013) . Available from: https://www.taylorfrancis.com/books/9781134742707. |
[37] | Deeks JJ, Higgins JP, Altman DG. Analysing data and undertaking meta-analyses. In: Cochrane Handbook for Systematic Reviews of Interventions. Wiley; (2019) . pp. 241-84. doi: 10.1002/9781119536604.ch10. |
[38] | Gonzalez-Perez LM, Infante-Cossio P, Montes-Latorre E, Torres-Carranza E, Ruiz-Canela P, Urresti-Lopez FJ, et al. Clinical results after deep dry needling versus intratissue percutaneous electrolysis technique for the treatment of temporomandibular myofascial pain. Int J Oral Maxillofac Surg. (2017) Mar; 46: : 358. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0901502717312663. |
[39] | Brennan K, Elifritz KM, Comire MM, Jupiter DC. Rate and maintenance of improvement of myofascial pain with dry needling alone vs. dry needling with intramuscular electrical stimulation: a randomized controlled trial. J Man Manip Ther. (2021) Jul 4; 29: (4): 216-26. doi: 10.1080/10669817.2020.1824469. |
[40] | Lopez-Martos R, Gonzalez-Perez L, Ruiz-Canela-Mendez P, Urresti-Lopez F, Gutierrez-Perez J, Infante-Cossio P. Randomized, double-blind study comparing percutaneous electrolysis and dry needling for the management of temporomandibular myofascial pain. Med Oral Patol Oral y Cir Bucal. (2018) ; 23: (4): e454-62. Available from: http://www.medicinaoral.com/medoralfree01/aop/22488.pdf. |
[41] | Rodríguez-Huguet M, Góngora-Rodríguez J, Lomas-Vega R, Martín-Valero R, Díaz-Fernández Á, Obrero-Gaitán E, et al. Percutaneous Electrolysis in the Treatment of Lateral Epicondylalgia: A Single-Blind Randomized Controlled Trial. J Clin Med. (2020) Jul 1; 9: (7): 2068. Available from: https://www.mdpi.com/2077-0383/9/7/2068. |
[42] | Valera-Calero JA, Sánchez-Mayoral-Martín A, Varol U. Short-term effectiveness of high- and low-intensity percutaneous electrolysis in patients with patellofemoral pain syndrome: A pilot study. World J Orthop. (2021) Oct 18; 12: (10): 781-90. Available from: https://www.wjgnet.com/2218-5836/full/v12/i10/781.htm. |
[43] | Rodríguez-Huguet M, Góngora-Rodríguez J, Rodríguez-Huguet P, Ibañez-Vera AJ, Rodríguez-Almagro D, Martín-Valero R, et al. Effectiveness of Percutaneous Electrolysis in Supraspinatus Tendinopathy: A Single-Blinded Randomized Controlled Trial. J Clin Med. (2020) Jun 12; 9: (6): 1837. Available from: https://www.mdpi.com/2077-0383/9/6/1837. |
[44] | Varela Rodríguez S, Eduardo Cáceres Pajuelo J, Luis Sánchez Sánchez J. Percutaneous Electrolysis in Patients with Musculoskeletal Disorders: A Systematic Review. Journal of Molecular and Genetic Medicine Review Article. Artic J Mol Genet Med an Int J Biomed Res. (2021) ; J Mol Gene: (15): 476. Available from: https://www.researchgate.net/publication/349462879. |
[45] | Sánchez-Infante J, Navarro-Santana MJ, Bravo-Sánchez A, Jiménez-Diaz F, Abián-Vicén J. Is dry needling applied by physical therapists effective for pain in musculoskeletal conditions? a systematic review and meta-analysis. Phys Ther. (2021) ; 101: (3): 12-3. |
[46] | Jackson MD, Rowe K, Davenport TE. Trigger point dry needling for musculoskeletal pain and disability: A Systematic Review of Comparative Effectiveness Research. Orthopaedic Physical Therapy Practice. (2016) ; 28: . Available from: https://scholarlycommons.pacific.edu/phs-facarticles. |
[47] | Legge D. A History of Dry Needling. J Musculoskelet Pain. (2014) Sep 27; 22: (3): 301-7. doi: 10.3109/10582452.2014.883041. |
[48] | Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur J Pain. (2004) Aug; 8: (4): 283-91. doi: 10.1016/j.ejpain.2003.09.004. |
[49] | García Naranjo J, Barroso Rosa S, Loro Ferrer JF, Limiñana Cañal JM, Suarez Hernández E. A novel approach in the treatment of acute whiplash syndrome: Ultrasound-guided needle percutaneous electrolysis. A randomized controlled trial. Orthop Traumatol Surg Res. (2017) Dec; 103: (8): 1229-34. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1877056817302761. |
[50] | Ronzio OA, Villa CA, Gómez D, Valentim da Silva RM, Gill JP, D’Almeida S, et al. Effects in pressure-pain threshold of percutaneous galvanic microcurrent in the trapezius trigger points. Physiotherapy. (2015) May; 101: : e1297-8. Available from: https://linkinghub.elsevier.com/retrieve/pii/S0031940615012444. |
[51] | de la Cruz Torres B, Albornoz Cabello M, García Bermejo P, Naranjo Orellana J. Autonomic Responses to Ultrasound-Guided Percutaneous Needle Electrolysis of the Patellar Tendon in Healthy Male Footballers. Acupunct Med. (2016) Aug 1; 34: (4): 275-9. doi: 10.1136/acupmed-2015-010993. |
[52] | García Bermejo P, de la Cruz Torres B, Naranjo Orellana J, Albornoz Cabello M. Autonomic activity in women during percutaneous needle electrolysis. Eur J Integr Med. (2017) Apr; 11: : 53-8. Available from: https://linkinghub.elsevier.com/retrieve/pii/S1876382017300197. |
[53] | García Bermejo P, De La Cruz Torres B, Naranjo Orellana J, Albornoz Cabello M. Autonomic Responses to Ultrasound-Guided Percutaneous Needle Electrolysis: Effect of Needle Puncture or Electrical Current? J Altern Complement Med. (2018) Jan; 24: (1): 69-75. doi: 10.1089/acm.2016.0339. |
[54] | de Sire A, Ammendolia A, Lippi L, Farì G, Cisari C, Invernizzi M. Percutaneous electrical nerve stimulation (Pens) as a rehabilitation approach for reducing mixed chronic pain in patients with musculoskeletal disorders. Appl Sci. (2021) ; 11: (9). |
[55] | Hidalgo B, Hall T, Bossert J, Dugeny A, Cagnie B, Pitance L. The efficacy of manual therapy and exercise for treating non-specific neck pain: A systematic review. J Back Musculoskelet Rehabil. (2017) ; 30: (6): 1149-69. |
[56] | Sanchez-Ibanez JM. Clinical course in the treatment of chronic patellar tendinopathy through ultrasound guided intratissue percutaneous electrolysis (EPIÒ): study of a population series of cases in sport [PhD thesis]. Atlantic International University; (2009) . |


