
Clarification of the “pain neuroscience education” concept in the management of patients with persistent low back pain: A scoping review
Abstract
BACKGROUND:
Patient education is a recommended treatment strategy for persistent low back pain (PLBP). Pain neuroscience education (PNE) is an emerging concept with boundaries still unclear.
OBJECTIVE:
To clarify the PNE concept and identify its key characteristics in PLBP management.
METHODS:
A systematic search was conducted using the following databases: Pubmed, ScienceDirect, Google Scholar, Cochrane, and Pedro. Inclusion criteria: publications in English or French on pain neuroscience education and chronic low back pain, educational books cited in white literature. Three reviewers independently selected eligible studies for final inclusion. Numerical analysis and narrative synthesis were carried out from the extracted data.
RESULTS:
From 919 identified publications, 54 were selected. Ten educational resources were added. PNE refers to a theoretical framework, a specific educational intervention, and an overall care approach. It is characterized by the intention to help the patient reconceptualize their PLBP from a tissue injury marker to a protective, neurobiological perspective, and then to increase adherence to biopsychosocial rehabilitation and normalize cognitive-behavioral responses. Pain sciences concepts are presented with an optimization of learning strategies.
CONCLUSION:
PNE stands out from other educational and cognitive behavioral approaches through its objective of changing the pain concept.
1.Background
It is now well established that low back pain is a complex condition whose persistence can be influenced by various modifiable and non-modifiable factors [1]. The patient’s beliefs about pain is a modifiable factor; hence, patient education may be a therapeutic strategy capable of positively influencing the health trajectory of patients suffering from persistent low back pain (PLBP) [1]. Several educational models have been described in the literature, including pain neuroscience education (PNE) [2]. PNE is designed for the management of many chronic pain conditions, including PLBP [2, 3, 4]. Thanks to a large number of scientific [5, 6, 7] and educational [8, 9, 10] publications on this theme, PNE has grown in popularity over the past 20 years and was recently mentioned for the first time in national practice guidelines [11]. PNE is often described as a specific educational intervention that seeks to explain pain from a neuroscience perspective, with the objective of producing a therapeutic effect [12]. While some researchers define PNE as a specific strategy, others describe it as an overall approach to care [13]. Furthermore, PNE is sometimes confused with other concepts in pain education, such as cognitive behavioral therapy (CBT) [2] and cognitive functional therapy [3, 14], which blurs the definition of this concept. Hence, in order to better identify and understand PNE, it seems necessary to clarify the concept and identify its key characteristics. Although systematic reviews of PNE have been published [5, 6, 7], they mainly focused on the concept’s efficacy and thus included randomized, controlled trials only. By broadening the inclusion criteria to literature reviews, expert opinions and/or some or all of the gray literature, scoping reviews are better suited to addressing broader issues (such as concept clarification) while maintaining a systematic, rigorous search method [15]. Although a scoping review on PNE was published recently, its aim was not to clarify the concept of PNE as applied to the management of patients with PLBP [16].
Given this context, the objectives of the present scoping review were to map the literature on PNE for PLBP, clarify the PNE concept, and identify its key characteristics.
2.Methods
2.1Ethical considerations
This study, as a literature review, is exempt from Institutional Review Board approval.
2.2Registration and protocol
The review is reported in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) and, in particular, the extension for scoping reviews (PRISMA-ScR). Our methodology was in line with the recommendations on scoping reviews published by Arskey and O’Malley. The initial protocol (detailing the context and the search method) has been published elsewhere [17] and has been available at DOI: 10.1016/j.kine.2021.01.007 since February 24
2.3Substantial modifications
The initial protocol has been substantially modified [17]. This methodological flexibility is allowed in scoping reviews [15]. Given the extent of the collected data, and in order to comply with the editorial guidelines of specialist journals, we decided to exclude two of the initial objectives: (i) understanding how the PNE concept is implemented, and (ii) identifying knowledge gaps to determine research needs. These modifications prompts the removal of the corresponding data extraction columns (e.g. skills, limitations, interview, physical examination, clinical reasoning, and education in practice). The inclusion criteria were clarified. Firstly, the term “educational book” was replaced by “educational resource”, so as to encompass educational resources like digital formats. Secondly, the term “providing clarification” has been replaced by “whose main objective is to provide clarification”, in order to specify the criterion during the selection process. The modification of this last criterion required some adjustments to the publication selection process: some articles initially included were subsequently excluded because clarification of the PNE concept was not the main objective.
2.4Research questions
The research questions for this review were (i) which data are available in the white and educational literature on PNE for the management of patients with PLBP?; (ii) what are the “contours” of PNE (i.e. defining what it is and, conversely, what it is not)?; and (iii) what are the key characteristics of PNE?
2.5Study selection criteria
The inclusion criteria were as follows: publications in English or French; white literature on PNE and PLBP (in a clinical trial dealing with non-specific persistent spinal pain, at least 50% of the participants must have low back pain); white literature on PNE and chronic pain and whose primary objective was to clarify the PNE concept; and educational resources for patients and clinicians cited in the white literature. We excluded grey literature not mentioned in the selected white literature, conference abstracts, comments, editorials, and citations. The eligible studies were as follows: systematic reviews with or without a meta-analysis, non-systematic reviews, narrative reviews, randomized controlled trials, non-controlled clinical trials, qualitative studies, case studies, protocol studies, and expert opinions.
2.6Search strategy
We searched the literature up until September 2020. We have constructed our search query by combining keywords designating PNE with keywords designating PLBP. To designate PNE, the keywords were pain neuroscience education, therapeutic neuroscience education, pain biology education, pain physiology education, and pain neurophysiology education. The MeSH terms associated with the individual keywords were also included. To designate PLBP, the keywords were chronic back pain and low back pain; again, the corresponding MeSH terms were included. We searched the following databases: PubMed, ScienceDirect, Google Scholar, Pedro, and Cochrane Library. For example, the PubMed search equation was: ((((((pain[MeSH Terms]) OR (Pain[Title/Abstract]))) OR ((therapeutic[MeSH Terms]) OR (therapeutic[Title/Abstract]))) AND (((((((Neuroscience[Title/Abstract]) OR (Neuroscience[MeSH Terms])) OR ((Physiolog*[Title/Abstract]) OR (physiology[MeSH Terms]))) OR ((Neurophysiolog*) OR (neurophysiology[MeSH Terms]))) OR ((Biolog*[Title/Abstract]) OR (biology[MeSH Terms])))))) AND (((Education[Title/Abstract]) OR (Education[MeSH Terms])))) AND ((((chronic[Title/Abstract]) OR (Persistent[Title/Abstract])) OR (Chronic pain[MeSH Terms])) AND (((Low back pain[Title/Abstract]) OR (Low back pain[MeSH Terms])))).
2.7Study selection
We used the covidence.org web application to manage the publication screening and selection steps. The investigators divided the screened databases between them: NA and KG screened PubMed, Science Direct, PEDRO, and the Cochrane Library, and NA and NS screened Google Scholar. Publications were selected on the basis of the title and the abstract; in the event of doubt, the publication was provisionally selected. Next, the full-text versions of all selected publication were read. Disagreements between two investigators with regard to the selection (or not) of a publication were resolved by consensus or referral to a third investigator.
2.8Data extraction
General and specific data were extracted from each publication, using a specific table (Table 1). Additional categories could emerge during the data collection process. The raw data were extracted and then summarized, to facilitate the narrative synthesis. The first ten publications to be selected were independently extracted by two investigators (NA and KG), to determine whether the extraction method was consistent from one investigator to another. Once the method’s reliability had been confirmed the data extraction task was shared between the two investigators.
Table 1
Data extraction
| General data on the publication | Specific data on PNE |
|---|---|
|
|
|
2.9The numerical, narrative synthesis
In order to make sense of the data extracted from the various sources, a numerical, narrative synthesis was produced by one of the investigators (NA). The narrative synthesis was constructed after a vertical and horizontal reading of the extracted data (Table 1). KG and NS reviewed and checked the level of consistency between the extracted data and the narrative synthesis. Considering the influence that a researcher can exert on the results (including the narrative synthesis), it is important to disclose his/her point of view; the reader can then consider how this might have influenced the study’s results. NA considers first that PNE can be a cognitive mindset (based on a pain neuroscience model) that influences how healthcare professionals communicate with patients about pain and treatment. He believes that PNE can secondarily be a person-centered educational strategy that blends cognitive and experiential learning in a constructivist manner.
Figure 1.
Flowchart.
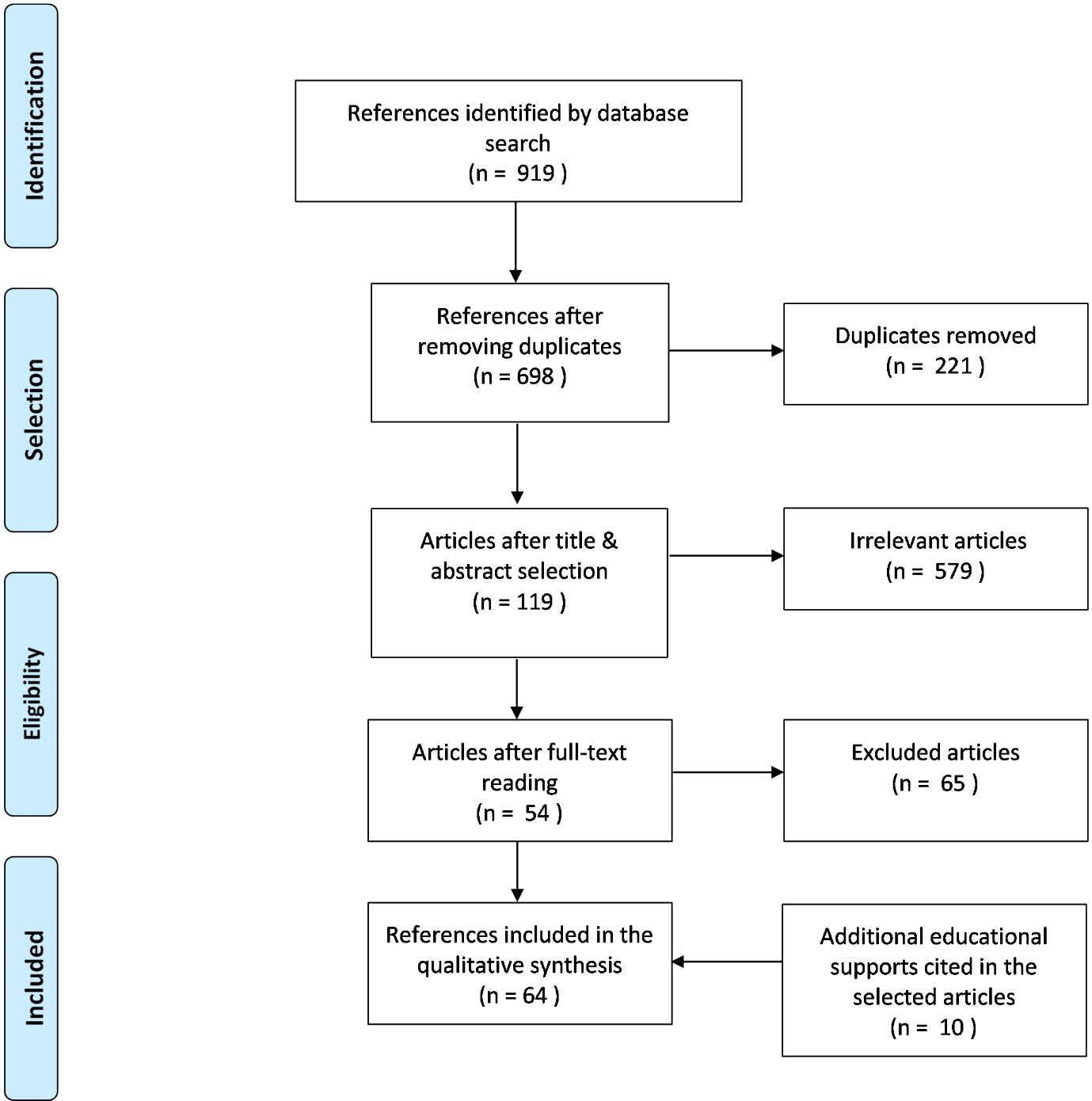
Figure 2.
PNE as a theoretical model.
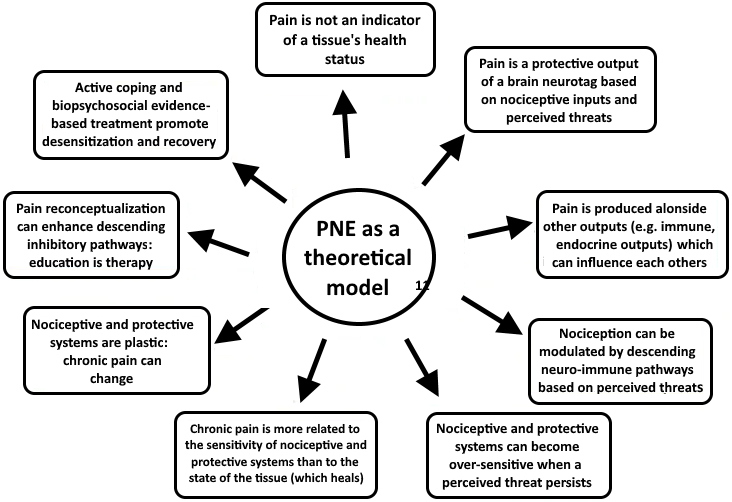
Figure 3.
PNE as an overall approach.
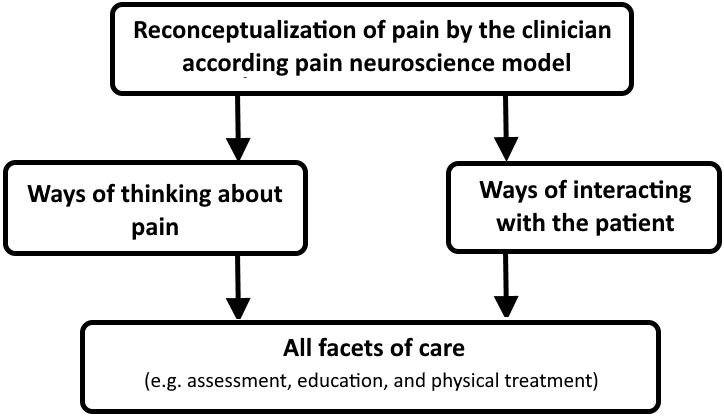
Figure 4.
PNE as a specific educational approach.
3.Results
3.1Descriptive analysis
The initial search identified 919 publications. After duplicates were removed, 698 publications remained. After application of the various selection criteria, 54 publications from the literature search were included. After reading the fulltext publications, 10 educational supports (including two for clinicians) cited in the selected publications were added manually. Hence, a total of 64 publications or documents were included in this review (Fig. 1). Specific data on PNE concept are shown in Supplementary Table 1 and general data from the included publications can be found in Supplementary Table 2.
3.2Numerical synthesis
Of the 54 publications from the literature search, 41 had been published since 2015 (76%) [2, 6, 7, 12, 14, 17, 18, 19, 20, 21, 22, 23, 24, 25, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 48, 49, 51, 54, 55, 56, 57, 60, 61, 62, 69, 70, 71, 73] with 7 published since 2010 (13%) [5, 27, 31, 53, 57, 58, 59, 62], and 6 published since 2002 (11%) [41, 42, 44, 45, 46, 47]. There were 10 study protocols (19%) [17, 18, 19, 20, 21, 57, 61, 62, 69, 70], 14 randomized, controlled trials (26%) [25, 28, 32, 33, 35, 41, 45, 47, 49, 51, 53, 54, 56, 71], 4 non-controlled trials (7%) [31, 37, 46, 73], 4 systematic reviews (7%) [5, 6, 7, 14], 1 non-systematic review (2%) [22], 1 qualitative study (2%) [48], 6 case studies or case series (11%) [23, 24, 29, 34, 44, 58] and 14 expert opinions or similar (26%) [2, 12, 26, 27, 30, 31, 36, 38, 39, 40, 42, 55, 59, 60]. Of the 10 educational resources included , 2 are intended for clinicians only [13, 18], 8 are intended for patients and/or clinicians [8, 9, 10, 63, 64, 65, 66, 68] (Table 2).
3.3Narrative synthesis
Names used
In the literature reviewed here, several names were used to designate the PNE concept: “pain neurophysiology education”, “explain pain”, etc. The most frequently used name was “pain neuroscience education” [7, 17, 18, 19, 20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39], which will henceforth be used in this narrative synthesis.
The context
According to some researchers, the emergence of PNE was prompted by observations of a lack of effectiveness of educational strategies and the modest effects of treatment in people suffering from chronic pain [2, 13, 40, 41]. Moseley and Butler explained these findings in terms of the counter-intuitive nature of the existing educational models: the structural tissue-based model (also covered by [42]), and the structural centralnervous system-based model [2]. The researchers suspected an amalgam between nociception and pain, implying that pain cannot be changed because a peripheral or central generator cannot be removed [2] (also covered by [13, 40]). Moseley and Butler rejected these models because of their lack of coherence, biological plausibility and clinical plausibility. The lack of coherence was due to the suggestion that pain is influenced by thoughts, emotions, behaviors, and therefore the program aims to change them. On the other hand, it is argued that the purpose is not to reduce pain. The lack of biological plausibility is due to the fact that pain can decrease, depending on the meaning given to it, through descending modulatory pathways. Finally, the lack of clinical plausibility was due to evidences showing that these programs, whose aim is not to reduce pain, have an effect on pain.
Furthermore, Moseley and Butler wondered why a patient would be motivated to commit to lasting behavioral changes if he/she believed that their pain could not be changed [2]. Other researchers hypothesize that tissue-based educational strategies (i) do not sufficiently target cognitive-behavioral aspects which are nevertheless strong predictors of pain chronicity [41], and (ii) are likely to increase levels of fear and (indirectly) pain [13, 36]. Several researchers argue that PNE is therefore designed to target these limitations, and increase the effectiveness of treatment [2, 13, 36, 41].
The initial concept
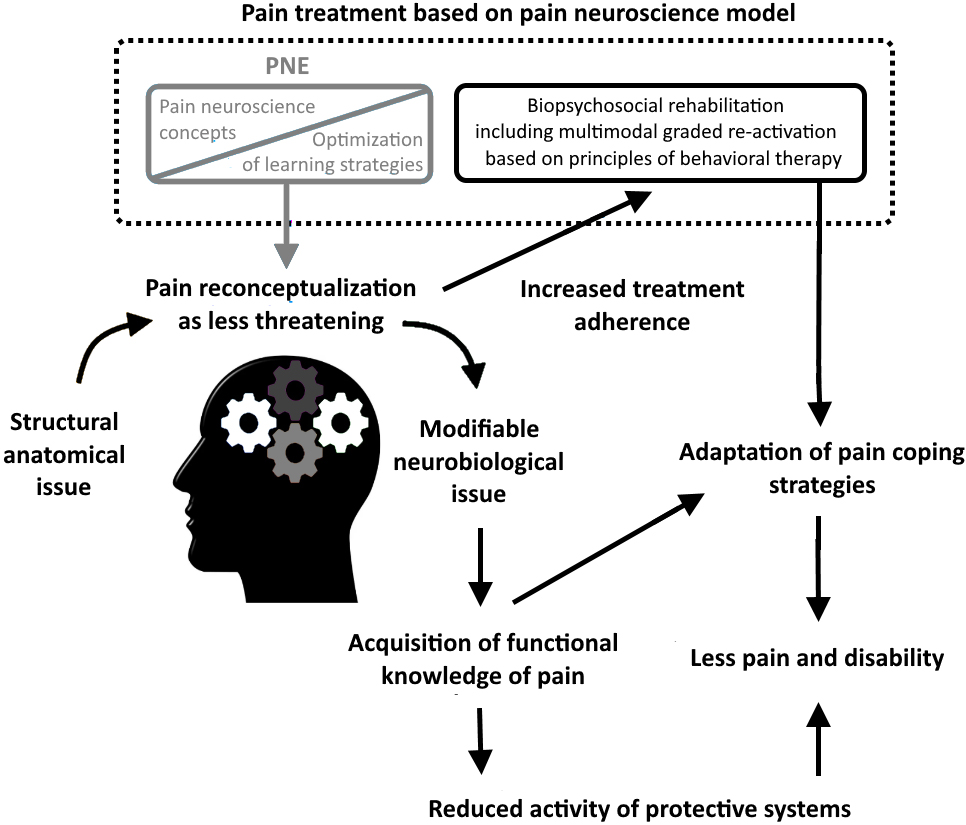
In his conceptual paper, Moseley defines PNE as an educative strategy that aims to reconceptualize someone’s meaning of pain from a neurophysiological point of view [42] (also covered by [2, 8, 13, 19, 26, 27, 38, 39, 41, 43, 44, 45, 46, 47]). Educational material is described in the Explain Pain book [8] and includes detailed information on the neurophysiology of pain (also covered by [2, 12, 13, 17, 19, 23, 28, 30, 36, 27, 38, 46, 48, 49, 50, 51]). Information is presented accurately (rather than being diluted for the sake of simplicity) and in a respectful manner that acknowledges the patient’s suffering. The objective is to reduce the threat value associated with pain (also covered by [2, 8, 13, 19, 22, 26, 27, 38, 39, 43, 44, 48, 52, 53]) by promoting deep learning of pain neurophysiology (also covered by [2, 8, 20, 36, 39, 43]) and assuming that more appropriate cognitive, behavioral responses will follow (also covered by [2, 13, 18, 19, 41, 43, 44, 45, 48, 52, 54, 55, 56, 57]). Moseley distinguishes superfical learning and deep learning; in the latter case, information is remembered and also understood, integrated in someone’s belief and attitude, and applied to solve problems (also covered by [2, 8, 28, 43]). To support deep learning, metaphors (also covered by [5, 13, 17, 23, 24, 25, 27, 28, 32, 33, 34, 36, 43, 44, 52, 53, 56, 58, 59, 60, 61]) and pictures (also covered by [5, 13, 17, 23, 32, 43, 44, 53, 58, 61, 62]) are used to present educational material. In Moseley’s publication, PNE is integrated into a multimodal approach (several treatment modalities that target different mechanisms or factors) based on its own theoretical model: the pain neuromatrix also described in Explain Pain (also covered by [2, 8, 13, 27, 27, 39]). In this model, pain is conceptualized as a protective output produced when the brain perceives that body tissues are in danger, and that action is required to protect them (also covered by [2, 8, 9, 13, 17, 43]). Pain occurs following the activation of an individual specific neuronal network called the “pain neurotag” and is experienced in the virtual body (also covered by [8, 9, 13, 43]). Chronic pain is thought to be promoted by impaired nociceptive and nonnociceptive systems (beliefs and attitudes) that increase the brain’s conviction that body tissues are in danger, thereby increasing pain neurotag activity (also covered by [8, 13, 43]). The longer the pain persists, the more the pain neurotag undergoes profound changes – including an increase in its synaptic efficacy (also covered by [8, 13, 43]). The aim of the multimodal approach is to reduce the sensitivity of the pain neurotag by (i) reducing threatening inputs (both nociceptive and nonnociceptive); (ii) activating specific components of the pain neurotag without activating the whole pain neurotag; and (iii) increasing physical and functional tolerance of the pain neurotag through graded exposure to threatening inputs by preventing flares-up (also covered by [8]). PNE is integrated in this approach by targeting a reduction in nonnociceptive inputs.
Variants of the PNE concept
Other researchers have subtly modified the initial concept. For example, Nijs’ research group adapted educational concepts from Explain Pain in a more synthetic way [63] in order to implement it in two 30-minute sessions before biopsychosocial CBT-based rehabilitation [52] (also covered by [20, 22, 26, 27, 62]. Emphasis was placed on the central sensitization concept, in order to explain chronic pain and the potential biopsychosocial factors that maintain it [52, 62]. Louw’s research group offered metaphorical and simplified adaptations of Explain Pain, together with original content [10, 13, 64]. Pain concepts were approached in a more “peripheral” way with an emphasis on the nervous system rather than the brain (e.g. pain is more related to peripheral nerve sensitization than pain neurotag sensitization), in order to avoid strong reactions like “do you think that pain is in my head?” [36]. Unlike the first publications on PNE [41, 46], Louw’s group included tissue stories (asymptomatic imaging and tissue healing) [10, 36, 37] to deconstruct Cartesian beliefs about pain before introducing an alternative view based on biology [13]. Unlike other researchers who deliver PNE in purely educational blocks [13, 36], Louw et al. offers to cut PNE into small educational pieces integrated and spread over physical therapy session (paced education) [13, 36]. According to these researchers, the objective is to better take account of the patient’s expectations so that they does not think that they are receiving “cognitive” treatment only [13]. Other educational resources from the white literature contain subtle variations on the educational content, pictures and metaphors used [65, 66]. According to Moseley and Butler, the unifying aspect of all these approaches is explanation of the key biological concepts that underlie pain, with the aim of giving the patient a functional knowledge of it [2] (also covered by [43]). Thus, patients can integrate functional knowledge of pain into their pain-related beliefs, attitudes, behaviors, treatment and lifestyle choices, in a way that reduces pain and improves function and quality of life [2] (also covered by [43]).
PNE as an educational approach
Researchers have variously defined PNE as a cognitive [13, 23, 32, 38, 71], cognitive-behavioral [48, 53, 58, 68] and/or educational [2, 12, 14, 17, 18, 19, 28, 31, 33, 37, 38, 40, 46, 48, 57, 60] approach for explaining pain to patients from a neurophysiological viewpoint [2, 12, 13, 17, 19, 23, 27, 28, 30, 31, 36, 38, 46, 48, 49, 50, 51]. Moseley and Butler stated that PNE can refer to a set of educational strategies that aim to change someone’s understanding of what pain is and what its purpose is [2] (also covered by [40]). More precisely, the researchers consider that PNE involves changing someone’s conception of pain from a marker of tissue injury to the perceived need to protect bodily tissues [2] (also covered by [7, 28, 40]) with a neurobiological perspective (e.g. brain output, sensitive nervous system) [17, 27, 37, 60]. Pain is presented as an emerging (rather than linear) phenomenon that is counter-intuitive when viewed against dominant structural models [2] (also covered by [42]). That is why Moseley and Butler argue that PNE challenges existing concepts based on optimizing learning and multimedia strategies, rather than simply delivering information [2]. To deliver it, several researchers believe that clinicians must first have a reconceptualization of pain according to the neuroscience model of pain [2, 36, 40, 43, 67]. By emphasizing a change in the concept of the patient’s pain, PNE differs from educational approaches to pain neuroscience that consider nociception and pain to be analogs (e.g. osteoarthritis equals pain; also covered by [40]). The researchers also differentiate between PNE and strategies that seek to teach coping strategies (e.g. pacing, goal setting, problem solving, and relaxation training) – with which PNE can nevertheless be combined (also covered by [40]). Lastly, PNE differs from approaches that focus on psychosocial aspects of pain [2] and can only be delivered through a biopsychosocial paradigm, with the integrated treatment of peripheral and central nociceptive drivers [2] (also covered by [8, 13, 26, 27]). Lotze and Moseley differentiate between PNE and pain education provided in CBT based programs because the latter are limited to applying science (e.g. teaching that pain does not equal injury) rather than covering pain science itself (e.g. teaching why pain does not equal injury) [40]. Louw et al. conceptualized PNE as a cognitive restructuring strategy integrated into a physical therapy, like a behavioral component of CBT [13]. However, some researchers point out that PNE can use experiential elements from other approaches (e.g. exercise, graded motor imagery, and manual therapy) to reinforce previously integrated educational concepts [38, 40, 43, 60]. While PNE was evaluated as the sole therapy in some clinical trials [19, 23, 28, 35, 44, 45, 46, 47, 48], Moseley and Butler argue that this is not its intention; rather, the goal is to increase adherence to biopsychosocial rehabilitation, in order to reduce pain and disability [2] (also covered by [7, 8, 13, 17, 18, 36, 43, 47, 52]). In the literature reviewed here, PNE has been combined with several other approaches, such as exercise/activity therapy [2, 8, 9, 10, 13, 19, 20, 22, 25, 26, 27, 29, 30, 31, 32, 34, 36, 38, 39, 41, 43, 45, 53, 54, 56, 58, 61, 63, 64, 65, 66, 68, 69], manual therapy [10, 13, 19, 22, 30, 32, 33, 36, 41, 51, 60, 64, 70], relaxation/meditation techniques [10, 13, 24, 27, 34, 36, 58, 64, 65, 69, 56], hypnosis [67], sensory retraining [71], and dry needling [49]. However, several researchers recommend that this management should include multimodal therapy based on cognitive-behavioral reactivation [2, 13, 20, 26, 27, 39, 40, 42, 58, 62].
PNE as a theoretical model
In their narrative review, Moseley and Butler stated that PNE refers to both an approach and a theoretical model from which to consider the treatment of pain [2]. This theoretical model was described initially in Explain Pain [8] and then adapted in several publications [26, 27, 39, 40, 42] and educational resources [9, 10, 13, 43, 63, 64, 65, 66, 68]. The model’s main tenet is that pain is a marker of the brain’s perceived need to protect the body’s tissues, rather than a marker of tissue injury [2] (also covered by [8, 9, 13, 43, 65, 66]). More specifically, pain is produced following the activation of a set of neural networks in the brain called the pain neurotag [42] (also covered by [8, 9, 13, 43, 68]). Pain occurs when the brain concludes (after a probabilistic evaluation of all nociceptive inputs (including immune and endocrine molecules that stimulate nociceptors and tissues) and nonnociceptive inputs (cognitive, emotional, sensory and social factors) that body tissues are in danger and action is required to protect them [42] (also covered by [2, 8, 9, 13, 43, 65, 66, 68]). Hence, pain is conceptualized as a perception combined with other perceptive responses (e.g. thoughts, emotions, and feelings) and neurobiological responses (e.g. sympathetic, endocrine and motor responses) that seek to protect and maintain homeostasis [43] (also covered by [8, 9, 13]). Through descending nociceptive pathways and the hypothalamic-pituitary-adrenal axis, this physiological reaction can influence peripheral processes such as blood flow, tissue healing and the inflammatory response; in turn, these peripheral processes influence the information analyzed by the brain within a circular system [43] (also covered by [8, 9, 13]). As a result, nociceptive information is neither necessary nor sufficient to produce pain: nociceptors are danger detectors and not pain detectors [8] (also covered by [2, 10, 13, 42, 43, 63, 64, 65, 66]). This concept implies that pain can occur in the absence of tissue damage if the brain’s analysis concludes that tissues are in danger (i.e. powerful danger perception). Conversely, tissue damage can occur without causing any pain if the brain concludes that its tissues are safe (i.e. strong safety perception). Excluding certain particular contexts, pain is conceptualized as a protector that is triggered before tissues get injured; in other words, there is a buffer zone between the pain threshold and the tissue tolerance threshold [8] (also covered by [9, 43]). In this model, chronic pain is contrasted against acute pain as being more related to central nervous system sensitivity (including the pain neurotag and the second-order neuron in the dorsal horn) rather than the state of the tissues, which heal linearly – at least after three to six months [8] (also covered by [9, 10, 13, 26, 42, 43, 63, 64, 65, 66]). The brain relies on erroneous information about the state of the tissues, and the pain neurotag is likely to be activated by events that are usually insufficient to activate it (e.g. light movement, thoughts, and emotions) [8] (also covered by [9, 13, 43]). Pain becomes overprotective, increasing the buffer effect between it and the tissue tolerance threshold [8] (also covered by [9, 43]). Central nervous system sensitization can help to make sense of persistent, disproportionate, widespread pain states or those triggered by non-physical factors [8] (also covered by [9, 13, 43]. According to the researchers, this central sensitization is favored by the persistence of factors that accentuate danger perception (e.g. beliefs of vulnerability, catastrophic thoughts, and fear of movement [2, 8, 9, 13, 26, 40, 42, 43, 65]), maladaptive behaviors (e.g. avoidance of fear, and perseverance despite pain) [8, 9, 10, 13, 63, 64, 66], factors disrupting homeostasis (e.g. sleep disturbance, sedentary behavior, and comorbidities) [10, 26, 64, 65, 66] or other overactive protective systems [10, 26, 64, 65, 66]. Protective systems (including the nervous system) are considered to be plastic and adaptable, meaning that chronic pain reversibility is biologically plausible whatever the state of the body tissues [43] (also covered by [8, 9, 10, 13, 64, 65, 66]). Active coping and evidencebased treatment strategies that include PNE are designed to promote this reversibility and recovery [43] (also covered by [8, 9, 10, 13, 26, 27, 39, 40]). This model offers a metaphorical rationale for conceptualizing pain management by integrating treatment of peripheral and central nociceptive contributors (see the initial concept). This theoretical framework has been built from a wide range of anecdotes (e.g. various facts of people who suffered from serious injuries without experiencing pain, or people who felt pain without evidence of injuries), other theories (e.g. Melzack’s neuromatrix theory, Bayesian predictive coding theory, and conceptual change theory) and scientific research (e.g. work on central sensitization, neuroimaging studies, asymptomatic imaging studies, and so on) [2] (also covered by [8, 13]).
PNE as an overall approach to care
While PNE is mostly described as a specific educational intervention, some researchers give it a broader definition [13, 43]. Moseley and Butler describe PNE as a way of thinking about pain based on an understanding of a theoretical model [43]. According to Louw et al., PNE can be described as an overall approach that permeates all facets of care [13]. Other researchers describe this type of an approach implicitly in the selected literature (e.g. pain neuroscience approach, pain neuromatrix approach or PNE plus) [12, 26, 27, 36, 39, 42, 55, 60]. According to some researchers, pain reconceptualization leads clinicians to observe patients and manage them through the prism of pain mechanism [12, 26, 27, 39, 40, 42, 55], the biopsychosocial model [2, 36, 42] or danger and safety evidence (including tissues) [40, 43]. Patients can be observed through this lens from the initial assessment and throughout their treatment [40] (also covered by [12, 13, 26, 27, 39, 42, 43, 55]). According to Lotze and Moseley, the unifying principle is always being aware of providing evidence of safety [40]. For example, Lotze and Moseley state that a friendly attitude, being perceived as an expert, spending time focusing on the person and their needs, and explaining pain and rehabilitation in an understandable manner are all elements that can provide evidence of safety [40]. On the same lines, Louw et al. recommend conducting an in-depth interview, conscientiously examining the patient, and taking care to explain the test results in a reassuring manner when appropriate [36]. According to Louw et al. PNE in the broad sense can represent a general language for communicating with the patient [13]. Several researchers recommend adjusting communication during treatment in a way that remains consistent with the educational model [13, 22, 38, 40, 60]. Communication has to use safe language while limiting the use of words, metaphors and explanatory models reflecting the structural model of pain, which are likely to increase danger perception [12, 13, 22, 36, 43]. Several researchers argue that exercise therapy must be adapted and include a time- or load-contingent approach, rather than symptomcontingent approach [40] (also covered by [26, 27, 38, 39, 42, 60]), and can include discussion of pain cognition before and after exercise to facilitate pain reconceptualization [20, 26, 27, 38, 39, 62].
Key characteristics of PNE
The theoretical model
PNE is based on its own theoretical model which includes biological concepts that underlie pain and its management. The model predicates that education, reassurance, and graded exposure have important roles in the therapeutic approach. The objective is to help patients reconceptualize their pain, reduce the associated perceived threat (thus reducing the activation of protective systems), and increase adherence to biopsychosocial rehabilitation (thus desensitizing the central nervous system). This model distinguishes PNE from other educational and CBT-based approaches, and is one of its key characteristics. More details are given in the “context” and “initial concept” sections.
Educational content
PNE’s educational content is intended to promote the reconceptualization of pain [41]. The content covers broad pain concepts explained through neuroscientific knowledge [40, 43]. In their narrative review, Moseley and Butler describe the key biological concepts that PNE can include: the variable relationship between nociception and pain (also covered by [8, 9, 10, 13, 63, 64, 65, 66, 68]), the powerful influence of context on pain (also covered by [8, 43, 65]), sensitization of the nociceptive system when pain persists (also covered by [8, 13, 26, 36, 43, 52, 58, 60, 65, 66]), the coexistence of several protective systems (including pain) (also covered by [8, 9, 13, 43]), the potential influence of other protective systems (sympathetic, endocrine, immune and motor systems) on pain (also covered by [8, 9, 13, 43]), the adaptability/trainability of our biology (also covered by [8, 9, 10, 13, 43, 63, 64, 65, 66, 68]), the knowledge that a return to normal is likely to be slow (also covered by [43]) [2]. In Explain Pain Supercharged, Moseley and Butler add some further concepts: pain is normal, personal and always real (also covered by [8, 10, 13, 63, 64, 65, 66, 68]), there is danger receptor and no pain receptor (also covered by [8, 9, 13, 63, 64, 65, 66, 68]), pain depends on the balance between danger and safety (also covered by [8, 9, 10, 13, 42, 63, 64, 65, 66, 68, 73]), pain involves distributed brain activity (also covered by [8, 9, 13, 26, 43, 52, 64]), learning about pain can help the individual and society (including that knowing pain can ease pain) and active treatment strategies promote recovery (also covered by [2, 8, 9, 10, 13, 63, 64, 65, 66]) [43]. In Recovery strategies, Lehman addresses some subtle variations of the original concepts (e.g. pain is more about sensitivity than damage, several factors can influence sensitivity, and the body is strong and adaptable) and adds other key messages: different mobility does not mean pain (also covered by [10, 69]), the body does not need to put back in place (also covered by [10]), and no movement should be banned forever [66]. Historically, the knowledge used to explain this broader pain concept was limited to pain neuroscience information [41, 42, 47]. According to Louw et al., it can include information about nociception and nociceptive pathways (e.g. neurons, action potentials, synapses, and primary and secondary nociceptors) [8, 13, 26, 32, 42, 43, 46, 47, 52, 63, 65, 66], spinal inhibition (also covered by [2, 8, 9, 10, 13, 26, 42, 43, 46, 52, 63, 64, 64, 66, 68, 72]), spinal facilitation (also covered by [2, 8, 13, 26, 42, 43, 45, 50, 52, 63, 65, 70]), peripheral sensitization (also covered by [8, 13, 26, 32, 33, 36, 43, 46, 47, 52, 58, 65]), central sensitization (also covered by [8, 13, 26, 28, 32, 33, 36, 43, 47, 52, 53, 58, 59, 60, 62, 63, 65, 68]) and nervous system plasticity [2, 8, 9, 10, 13, 18, 26, 32, 33, 35, 43, 52, 63, 64, 65, 66]. The role of the brain (e.g. the pain neuromatrix theory, and pain as a brain output based on danger perception) is also covered by many researchers [2, 13, 18, 20, 26, 31, 32, 33, 42, 43, 52, 73]. The virtual body (Penfield’s homunculus) is mentioned by some researchers [8, 13, 43, 51, 68]. However, PNE can include content on tissues and anatomy if it promotes the de-education of pain misconceptions or reinforces educational concepts (see the section on variants of the PNE concept). On the same lines, content on biomechanics (e.g. spinal curves, leg length discrepancies, etc.) [10, 66], physical factors (e.g. posture, load bearing, strength, and flexibility) [10, 66, 69, 70] can be found in some educational materials. Louw et al. added that PNE can also include content on beliefs (e.g. fear avoidance) and psychosocial factors (e.g. catastrophism, fear of movement, hypervigilance, and avoidance and perseverance behaviors) that influence pain [13] (also covered by [5, 8, 10, 18, 31, 32, 33, 34, 36, 52, 53, 56, 58, 61, 63, 64, 65, 66, 70]). Other biopsychosocial factors such as lifestyle factors (e.g. a sedentary lifestyle and sleep hygiene) [13, 65, 66, 70] and comorbidities [66] are considered by some researchers to contribute to nervous system sensitivity in a biopsychosocial model. Specific content related to low back pain is found in some studies [17, 36, 56, 61, 69], patient education books [8, 10, 66], and clinicians education books [13, 43]. These variations of content allow for taking into account anatomical (e.g. the solidity of the lumbar spine with “it’s not out, never out”), neurophysiological (e.g. the solid but sensitive nature of the lumbar spine with “the jewels of the crown”), pathoanatomical (e.g. disc degeneration with “stable platform”), diagnostic (e.g. the meaning of the nonspecific low back pain label with “back pain is like pimples”), or therapeutic particularities by integrating it and representations around the management of persistent low back pain (e.g. posture, ergonomics, etc.) [43]. However, Moseley and Butler have pointed out that PNE does not include simplistic explanations such as gate control theory or the conflation of nociception and pain (e.g. pain is caused by structural damage to the central nervous system, and nerves send pain messages to the brain) [2]. Lastly, several publications did not consider the presentation of treatment options to be part of PNE [12, 23, 24, 25, 39, 44, 45, 46, 47, 48, 68, 71]; in contrast, other publications [28, 32, 33, 34, 53, 56, 60, 61, 69, 73] and educational resources [8, 9, 10, 13, 43, 64, 65, 66] encompassed treatment with a pain neuroscience perspective (i.e. with the objective of desensitizing the nervous system).
Optimization of learning strategies
According to Moseley and Butler, PNE refers to the quality of the content taught and how the content is taught [2]. They argue that deep learning requires the optimization of learning strategies [2] (also covered by [13, 36, 43]) and is thus a key feature of PNE. While a few studies have assessed the value of delivering educational materials alone [73], several researchers (i) acknowledge that this strategy alone does not produce significant behavioral changes and clinical effects and (ii) recommend that education be guided by a healthcare professional [13, 43]. Although a lecture format is described in some clinical trials [17, 45, 48, 54, 56, 61, 69], several researchers do not recommend this learning approach [13, 22, 43, 53, 62]. Moseley and Butler argue that it places the learner in a passive role that does not promote conceptual change [43]. They recommend a constructivist approach, placing the clinician as a guide and the patient in an active position seeking to make sense of the information presented to him/her [43]. To this end, some researchers present educational concepts in a conversational, interactive style [13, 22, 23, 26, 38, 40, 43, 56, 57, 61, 63]. Nijs et al. used a Socratic dialogue [39]. According to Moseley and Butler, learning a concept produces a neurotag associated with that concept, whose influence can be strengthened by the use of metaphors (strengthening of the synaptic efficiency of the neurotag), visual aids (increasing the precision of the neurotag), repetition and variation of modalities to present the same concept (increasing the mass of the neurotag) [43]. That’s why many researchers state that the message can be presented with metaphors [5, 13, 17, 18, 20, 23, 24, 27, 28, 32, 33, 35, 36, 42, 43, 44, 52, 53, 56, 60, 61], examples [13, 20, 23, 26, 28, 36, 44, 46, 47, 52, 60] and/or stories [13, 43]. Pictures can also be used, to illustrate the therapist’s discourse [5, 13, 17, 23, 32, 43, 44, 53, 58, 62]. They can be prepared in advance [34, 47, 61] or drawn freehand [13, 35, 42, 46, 50]. According to these researchers, this content can take the form of a graph [18, 28, 32, 42], a diagram [47, 50, 52, 56, 61, 62], a video [13, 18, 23, 34, 43] and/or a photo [13]. PowerPoint presentations [24, 28, 32, 33, 49, 52, 54, 69], books, booklets, and brochures [2, 8, 9, 10, 13, 20, 27, 31, 52, 56, 63, 64, 66, 68, 69, 73] are frequently used to present these pictures. Other researchers use websites [27, 65, 69], video servers [23, 24, 34], infographics [18], posters [13] and/or educational cards [13]. Moseley and Butler recommend that the messages must be understandable (also covered by [20, 26, 38, 40, 43, 56, 61]), coherent (also covered by [38, 40, 43, 48]), attractive, and plausible [43]. Many researchers also recommend that educational content should be individualized [18, 20, 24, 31, 32, 36, 43, 49, 55, 59]. For example, several researchers argue that this content should take the patient’s concerns into account [13, 24, 36, 43, 58]. According to the researchers, the content must take account of their signs and symptoms [13, 36, 43, 55, 71], beliefs [43], experiences [20], motivation to change [55], and/or intellectual abilities [26]. Other educational strategies are used by various researchers, such as prompting the patient to read educational material [20, 28, 31, 47, 52, 62, 69, 71, 72] or ask questions [13, 36, 26, 28, 49, 50, 69], self-explanation [18, 36, 26, 43, 52, 58], cognitive homework [13, 23, 36, 49, 57], paced education [13, 36, 43], quiz [26, 52, 58], and explanatory feedback [43]. Finally, according to Blickenstaff et al., experiential learning can reinforce (conceptual) change [38], that is why several researchers describe the use of experiential elements from other therapeutic approaches to reinforce the accommodation of education concepts [13, 38, 39, 43, 60].
4.Discussion
Our review showed that PNE can variously refer to a theoretical model that conceptualizes pain and its treatment a cognitive approach to healthcare and a specific educational approach. The review also clarified the context from which the concept emerged and highlighted the concept’s evolution. The theoretical framework (built from other existing theories, anecdotes and scientific research) conceptualizes pain as a perceptual, protective response modulated by nociceptive and nonnociceptive information (including the meaning of pain). In contrast to acute pain, persistent pain is more related to sensitization of the central nervous system and prolongation of the (over)protective effect of pain beyond the body tissues’ healing time. This neuronal sensitization is presumed to be maintained biologically by the persistence of factors promoting danger perception and/or factors disturbing homeostasis. These systems are assumed to be plastic, meaning that reversibility of chronic pain becomes plausible. According to this model, understanding the pain mechanisms associated with biopsychosocial rehabilitation (including graded and multimodal reactivation) promotes plasticity of the body and recovery. However, PNE is mostly described as a cognitive educational approach that uses conceptual change strategies about pain science to change the understanding of pain. More specifically, PNE is intended to help the person reconceptualize their pain, with a shift from a threatening, structural and immutable point of view to a safe, biopsychosocial and modifiable point of view. This conceptual change seeks to reduce the threat perception related to pain by acquiring functional knowledge about pain, making it possible to produce more appropriate cognitive, emotional and behavioral reactions to pain. It concomitantly increases adherence to active strategies based on a biopsychosocial framework and seeks to significantly reduce pain and disability. PNE differs from therapies based on structural models that conflate nociception and pain, and emphasizes pain management rather than pain treatment. PNE also differs from cognitive-behavioral strategies in terms of its emphasis on changing the understanding of pain and thus painrelated cognition and behavior rather than changing cognition and behavior directly. To this end, PNE is characterized by teaching the patient key biological concepts from its own theoretical model (e.g. pain is a protective response based on a perceived threat; chronic pain is more related to nervous system sensitivity than the state of the tissue; protective systems are plastic and can therefore be changed by active coping strategies) through knowledge of pain science (including neurophysiological, anatomical and psychosocial knowledge) and thus making sense of pain and its treatment. More than delivering information, PNE is characterized by the optimization of learning strategies (including a constructivist, interactive approach rather than a lecturing approach) through stories, metaphors and multimedia strategies in an individualized, understandable manner. PNE can also borrow elements of other therapeutic strategies (like exercise therapy) to add experiential learning to cognitive learning. Lastly, PNE has occasionally been defined more broadly as an overall approach to care in which the clinician thinks carefully, interacts with the patient and adapts the treatment in accordance with the pain neuroscience model. In this approach, clinician must be aware of the need to provide evidence of safety in all phases of care, from the initial assessment and throughout the treatment.
4.1Theoretical reflections
The aim of this review was to clarify the PNE concept and identify its key characteristics, not to perform a critical analysis of the concept. However, the completion of this synthesis work has raised several reflections: i) What is the quality of scientific basis on which the theoretical model is based? For example, a group of researchers argue that the concept that “nociception is not necessary to produce pain” is based only on weak evidence (clinical trials where characteristics of requests are not controlled [74]), biased extrapolations of case series and anecdotes [75]. They criticize the PNE model for its use of speculative extrapolations presented as facts (e.g., it is the brain that decides to produce pain), and its excessive use of teleological arguments (e.g., pain is a marker of the need for protection) [76]. It would be relevant to explore the strength and relevance of the scientific foundations that support the model’s core concepts, such as the “bioplasticity of the body” concept or the idea that “reconceptualizing pain can reduce it”. ii) Is Pain Neuroscience Education the most appropriate name for this educational approach? On the one hand, it allows us to differentiate it from structural model-based educational approaches and approaches that teach coping strategies. On the other hand, the primary goal of this approach is to help the patient to reconceptualize his/her pain from a neurobiological and protective point of view. To do this, this narrative synthesis highlighted that PNE did not only consist of cognitive strategies of neuroscience content learning, and that experiential and reflective learning strategies could be used to favor the reconceptualization of pain. Some authors prefer the term “Pain Education” as it does not systematically include neuroscience content or “Guided Discovery [of Pain]” to incorporate a more constructivist and experiential vision of learning [77]. iii) Given the narrative synthesis, one could wonder if the content of PNE changes for persistent low back pain. While it is true that many contents and concepts can be used interchangeably with different painful conditions, adaptations may be necessary depending on anatomical, neurophysiological, diagnostic, prognostic and therapeutic particularities to increase consistency with the clinical context (see “educational content” section). Furthermore, since low back pain is a heterogeneous clinical condition, content can be adapted according to clinical presentation. For example, for chronic low back pain with a predominance of nociceptive pain, the explanation of peripheral sensitization or the use of a more vague metaphor such as the alarm system may be preferred to content explicitly illustrating central sensitization. iv) Finally, PNE is mostly described as a specific educational strategy, particularly in controlled and randomized trials whose aim is to evaluate its effectiveness [25, 32, 33, 35, 41, 45, 47, 49, 51, 53, 54, 56, 71]. While the interest of these clinical trials is obvious, the described format may not be suitable for everyday care contexts in physiotherapy [36, 78]. To implement the approach, Barbari et al. suggest that clinicians keep in mind that the main goal is to help patients to reconceptualize their pain according to the neuroscience model [78]. Therefore, PNE can be conceptualized as a new mode of communication where all the characteristics of rehabilitation (e.g. therapeutic alliance, reassurance, positive expectations, explaining persistant low back pain and treatment, gradual exposure) are thought of and built through the perspective of pain neuroscience, in order to take into account the clinical context and the individual characteristics of the patient. This implementation proposal is reminiscent of the characteristics of PNE in a broad definition [13, 40, 43]. From our point of view, Cognitive Functional Therapy can be likened to a broad sense of PNE, integrating experiential learning strategies and little neuroscience content, but whose aim is to help the patient reconceptualize his/her low back pain with a safe, biopsychosocial and modifiable perspective [79, 80].
4.2Limitations
This scoping review had several limitations. Firstly, we did not assess the methodological quality of the included publications; this decision was taken because (i) this type of assessment did not particularly match the review’s objectives, (ii) this flexibility is allowed in Arskey and O’Malley’s methodology, and (iii) the assessment is not required by the PRISMA-ScR guidelines. Secondly, we cannot rule out bias in the selection process; relevant publications might have been missed by our search equation, our language criteria (publications in English or in French only), and the exclusion of part of the gray literature (i.e. educational resources not cited in the selected white literature) or certain types of publication (editorials, comments, and conference abstracts). Thirdly, doubts were expressed during the selection of certain publications because the PNE term was not clearly cited (e.g. “patient education”, “pain education”, “modern pain education”, etc.), even though the spirit and content of the publication was consistent with the concept of PNE. We tried to limit this bias by having three investigators select the publications in four steps. Fourthly, the clarification of certain objectives led us to modify the selection process while the narrative synthesis was being written, which may have introduced bias during the updated selection stage. Fifthly, we cannot rule bias during the extraction stage, which was mainly carried out by one investigator (NA). We attempted to reduce this bias by improving the reliability of the extraction approach: extraction instructions were written down, and data from the first ten publications were extracted independently. The results were pooled and discussed in order to determine whether our extraction approach was coherent and to increase the level of inter-rater reliability. Furthermore, NS reviewed the extracted data to ensure consistency with the extraction categories. Lastly, we cannot rule out bias during the narrative synthesis created solely by NA. We are aware that the investigator may have paid particular attention to certain extracted data when drafting the synthesis, as acknowledged by Arksey and O’Malley. To limit this bias, the other investigators reread and checked the consistency between the extracted data and the narrative synthesis.
5.Conclusion
PNE refers to both an approach and the theoretical model that conceptualizes this approach. In a broad sense, PNE can be described as an overall approach to care. Strictly speaking, it can be described as a set of educational strategies intended to make people understand the key biological concepts underlying pain. PNE does more than providing new information; it seeks to accommodate potentially challenging concepts based on pain science. The idea is that patients will integrate functional knowledge on pain that can then change their beliefs, attitudes and behaviors in a way that reduces pain and disability. To this end, PNE is characterized by its own theoretical model, educational concepts based on that model, and the optimization of strategies that facilitate the learning of educational concepts. PNE does not solely use cognitive strategies; it can also adopt experiential learning techniques from other approaches and reinforce biological concepts. Understanding that PNE can be an overall approach to care and that it cannot be applied without considering the corresponding theoretical model and educational skills will help clinicians to define their learning priorities and thus to implement PNE. Lastly, our review should prompts researchers publishing in this field to clarify what they mean by PNE, so that the reader can be confident that a misconception of PNE is not being evaluated.
Funding
The study was funded by the APPRL (Lille, France).
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-220370.
Acknowledgments
The authors thank Anthony Halimi for helpful discussions about this topic.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | O’Sullivan P, Caneiro JP, O’Keeffe M, O’Sullivan K. Unraveling the complexity of low back pain. J Orthop Sports Phys Ther. (2016) Nov; 46: (11): 932-937. doi: 10.2519/jospt.2016.0609. PMID: 27802794. |
[2] | Moseley GL, Butler DS. Fifteen years of explaining pain: The past, present, and future. J Pain. (2015) Sep; 16: (9): 807-13. doi: 10.1016/j.jpain.2015.05.005. Epub 2015 Jun 5. PMID: 26051220. |
[3] | Louw A, Zimney K, Puentedura EJ, Diener I. The efficacy of pain neuroscience education on musculoskeletal pain: A systematic review of the literature. Physiother Theory Pract. (2016) Jul; 32: (5): 332-55. doi: 10.1080/09593985.2016.1194646. Epub 2016 Jun 28. PMID: 27351541. |
[4] | Watson JA, Ryan CG, Cooper L, Ellington D, Whittle R, Lavender M, Dixon J, Atkinson G, Cooper K, Martin DJ. Pain neuroscience education for adults with chronic musculoskeletal pain: A mixed-methods systematic review and meta-analysis. J Pain. (2019) Oct; 20: (10): 1140.e1-1140.e22. doi: 10.1016/j.jpain.2019.02.011. Epub 2019 Mar 1. PMID: 30831273. |
[5] | Clarke CL, Ryan CG, Martin DJ. Pain neurophysiology education for the management of individuals + with chronic low back pain: Systematic review and meta-analysis. Man Ther. (2011) Dec; 16: (6): 544-9. doi: 10.1016/j.math.2011.05.003. Epub 2011 Jun 25. PMID: 21705261. |
[6] | Tegner H, Frederiksen P, Esbensen BA, Juhl C. Neurophysiological pain education for patients with chronic low back pain: A systematic review and meta-analysis. Clin J Pain. (2018) Aug; 34: (8): 778-786. doi: 10.1097/AJP.0000000000000594. PMID: 29443723. |
[7] | Wood L, Hendrick PA. A systematic review and meta-analysis of pain neuroscience education for chronic low back pain: Short-and long-term outcomes of pain and disability. Eur J Pain. (2019) Feb; 23: (2): 234-249. doi: 10.1002/ejp.1314. Epub 2018 Oct 14. PMID: 30178503. |
[8] | Butler D, Moseley L. Explain Pain. 2 |
[9] | Moseley L, Butler D. The Explain Pain Handbook: Protectometer. Noi Group Publications; (2015) . |
[10] | Louw A, Flynn T, Puentedura E. Everyone Has Back Pain. 1st edition. Orthopedic Physical Therapy Products; (2015) . |
[11] | Haute Autorité de Santé. Lombalgie chronique de l’adulte et chirurgie. Recommandations de bonnes pratiques. Méthode recommandation pour la pratique clinique. Argumentaire scientifique. (2015) . (cited 2023 Apr 18). Available from: https://www.has-sante.fr/upload/docs/application/pdf/2016-03/arg_pertinence_chir-lombalgie.pdf. |
[12] | Diener I, Kargela M, Louw A. Listening is therapy: Patient interviewing from a pain science perspective. Physiother Theory Pract. (2016) Jul; 32: (5): 356-67. doi: 10.1080/09593985.2016.1194648. Epub 2016 Jun 28. PMID: 27351690. |
[13] | Louw A, Puentedura E, Schmidt S, Zimney K. Pain Neuroscience Education. 2nd ed. Orthopedic Physical Therapy Products; (2018) . |
[14] | Barbari V, Storari L, Ciuro A, Testa M. Effectiveness of communicative and educative strategies in chronic low back pain patients: A systematic review. Patient Educ Couns. (2020) May; 103: (5): 908-929. doi: 10.1016/j.pec.2019.11.031. Epub 2019 Dec 4. PMID: 31839351. |
[15] | Arksey H, O’Malley L. Scoping studies: Towards a methodological framework. Int J Soc Res Methodol. (2005) ; 8: : 19-32. doi: 10.1080/1364557032000119616. |
[16] | Ziegler AM, Minkalis AL, Langdon ER, Vining R. Learning the neurobiology of pain: A scoping review of pain education from an instructional design perspective. Patient Educ Couns. (2022) Jun; 105: (6): 1379-1401. doi: 10.1016/j.pec.2021.09.021. Epub 2021 Sep 14. PMID: 34579995. |
[17] | Adenis N, Gosselin K. Pain neuroscience education: A protocol for a scoping review in the management of patient with chronic low back pain. Kinesither Rev. (2021) Feb; 21: (240): 19-24. doi: 10.1016/j.kine.2021.01.007. |
[18] | Galán-Martín MA, Montero-Cuadrado F, Lluch-Girbes E, Coca-López MC, Mayo-Iscar A, Cuesta-Vargas A. Pain neuroscience education and physical exercise for patients with chronic spinal pain in primary healthcare: A randomised trial protocol. BMC Musculoskelet Disord. (2019) Nov 3; 20: (1): 505. doi: 10.1186/s12891-019-2889-1. PMID: 31679512; PMCID: PMC6825712. |
[19] | Lane E, Fritz JM, Greene T, Maddox D. The effectiveness of training physical therapists in pain neuroscience education on patient reported outcomes for patients with chronic spinal pain: A study protocol for a cluster randomized controlled trial. BMC Musculoskelet Disord. (2018) Oct 25; 19: (1): 386. doi: 10.1186/s12891-018-2269-2. PMID: 30360762; PMCID: PMC6203285. |
[20] | Malfliet A, Kregel J, Meeus M, Cagnie B, Roussel N, Dolphens M, Danneels L, Nijs J. Applying contemporary neuroscience in exercise interventions for chronic spinal pain: Treatment protocol. Braz J Phys Ther. (2017) Sep-Oct; 21: (5): 378-387. doi: 10.1016/j.bjpt.2017.06.019. Epub 2017 Jul 8. PMID: 28736211; PMCID: PMC5628368. |
[21] | Malfliet A, Bilterys T, Van Looveren E, Meeus M, Danneels L, Ickmans K, Cagnie B, Mairesse O, Neu D, Moens M, Goubert D, Kamper SJ, Nijs J. The added value of cognitive behavioral therapy for insomnia to current best evidence physical therapy for chronic spinal pain: Protocol of a randomized controlled clinical trial. Braz J Phys Ther. (2019) Jan-Feb; 23: (1): 62-70. doi: 10.1016/j.bjpt.2018.10.007. Epub 2018 Oct 29. PMID: 30389347; PMCID: PMC6546904. |
[22] | Malfliet A, Ickmans K, Huysmans E, Coppieters I, Willaert W, Bogaert WV, Rheel E, Bilterys T, Wilgen PV, Nijs J. Best evidence rehabilitation for chronic pain part 3: Low back pain. J Clin Med. (2019) Jul 19; 8: (7): 1063. doi: 10.3390/jcm8071063. PMID: 31331087; PMCID: PMC6679058. |
[23] | Agarwal V, Louw A, Puentedura EJ. Physician-delivered pain neuroscience education for opioid tapering: A case report. Int J Environ Res Public Health. (2020) May 11; 17: (9): 3324. doi: 10.3390/ijerph17093324. PMID: 32403225; PMCID: PMC7246593. |
[24] | Anandkumar S, Manivasagam M, Kee VTS, Meyding-Lamade U. Effect of physical therapy management of nonspecific low back pain with exercise addiction behaviors: A case series. Physiother Theory Pract. (2018) Apr; 34: (4): 316-328. doi: 10.1080/09593985.2017.1394410. Epub 2017 Nov 7. PMID: 29111859. |
[25] | Galan-Martin MA, Montero-Cuadrado F, Lluch-Girbes E, Coca-López MC, Mayo-Iscar A, Cuesta-Vargas A. Pain neuroscience education and physical therapeutic exercise for patients with chronic spinal pain in spanish physiotherapy primary care: A pragmatic randomized controlled trial. J Clin Med. (2020) Apr 22; 9: (4): 1201. doi: 10.3390/jcm9041201. PMID: 32331323; PMCID: PMC7230486. |
[26] | Nijs J, Meeus M, Cagnie B, Roussel NA, Dolphens M, Van Oosterwijck J, Danneels L. A modern neuroscience approach to chronic spinal pain: Combining pain neuroscience education with cognition-targeted motor control training. Phys Ther. (2014) May; 94: (5): 730-8. doi: 10.2522/ptj.20130258. Epub 2014 Jan 30. PMID: 24481595. |
[27] | Nijs J, Clark J, Malfliet A, Ickmans K, Voogt L, Don S, den Bandt H, Goubert D, Kregel J, Coppieters I, Dankaerts W. In the spine or in the brain? Recent advances in pain neuroscience applied in the intervention for low back pain. Clin Exp Rheumatol. (2017) Sep-Oct; 35 Suppl 107(5): 108-115. Epub 2017 Sep 29. PMID: 28967357. |
[28] | Orhan C, Lenoir D, Favoreel A, Van Looveren E, Yildiz Kabak V, Mukhtar NB, Cagnie B, Meeus M. Culture-sensitive and standard pain neuroscience education improves pain, disability, and pain cognitions in first-generation Turkish migrants with chronic low back pain: A pilot randomized controlled trial. Physiother Theory Pract. (2021) May; 37: (5): 633-645. doi: 10.1080/09593985.2019.1639231. Epub 2019 Jul 8. PMID: 31280694. |
[29] | Peterson S, Denninger T. Physical therapy management of patients with chronic low back pain and hip abductor weakness. J Geriatr Phys Ther. (2019) Jul/Sep; 42: (3): 196-206. doi: 10.1519/JPT.0000000000000148. PMID: 28914719. |
[30] | Puentedura EJ, Flynn T. Combining manual therapy with pain neuroscience education in the treatment of chronic low back pain: A narrative review of the literature. Physiother Theory Pract. (2016) Jul; 32: (5): 408-14. doi: 10.1080/09593985.2016.1194663. Epub 2016 Jun 30. PMID: 27362980. |
[31] | Rufa A PT, DPT, OCS, Beissner K PT, PhD, Dolphin M PT, DPT, MS, OCS. The use of pain neuroscience education in older adults with chronic back and/or lower extremity pain. Physiother Theory Pract. (2019) Jul; 35: (7): 603-613. doi: 10.1080/09593985.2018.1456586. Epub 2018 Mar 30. PMID: 29601227. |
[32] | Saracoglu I, Arik MI, Afsar E, Gokpinar HH. The effectiveness of pain neuroscience education combined with manual therapy and home exercise for chronic low back pain: A single-blind randomized controlled trial. Physiother Theory Pract. (2022) Jul; 38: (7): 868-878. doi: 10.1080/09593985.2020.1809046. Epub 2020 Aug 19. PMID: 32812478. |
[33] | Saracoglu I, Arik MI, Afsar E, Gokpinar HH. The short-term effects of neuroscience pain education on quality of life in patients with chronic low back pain: A single-blinded randomized controlled trial. European Journal of Integrative Medicine. (2020) Jan; 33: : 101046. doi: 10.1016/j.eujim.2019.101046. |
[34] | Toomey D, Reid D, White S. How manual therapy provided a gateway to a biopsychosocial management approach in an adult with chronic post-surgical low back pain: A case report. J Man Manip Ther. (2021) Apr; 29: (2): 107-132. doi: 10.1080/10669817.2020.1813472. Epub 2020 Sep 15. PMID: 32930642; PMCID: PMC8023601. |
[35] | Ünal M, Evci KE, Kocatürk M, Algun ZC. Investigating the effects of myofascial induction therapy techniques on pain, function and quality of life in patients with chronic low back pain. J Bodyw Mov Ther. (2020) Oct; 24: (4): 188-195. doi: 10.1016/j.jbmt.2020.07.014. Epub 2020 Aug 1. PMID: 33218510. |
[36] | Louw A, Zimney K, O’Hotto C, Hilton S. The clinical application of teaching people about pain. Physiother Theory Pract. (2016) Jul; 32: (5): 385-95. doi: 10.1080/09593985.2016.1194652. Epub 2016 Jun 28. PMID: 27351903. |
[37] | Louw A, Zimney K, Johnson EA, Kraemer C, Fesler J, Burcham T. De-educate to re-educate: Aging and low back pain. Aging Clin Exp Res. (2017) Dec; 29: (6): 1261-1269. doi: 10.1007/s40520-017-0731-x. Epub 2017 Mar 9. PMID: 28275956. |
[38] | Blickenstaff C, Pearson N. Reconciling movement and exercise with pain neuroscience education: A case for consistent education. Physiother Theory Pract. (2016) Jul; 32: (5): 396-407. doi: 10.1080/09593985.2016.1194653. Epub 2016 Jun 29. PMID: 27356079. |
[39] | Nijs J, Lluch Girbés E, Lundberg M, Malfliet A, Sterling M. Exercise therapy for chronic musculoskeletal pain: Innovation by altering pain memories. Man Ther. (2015) Feb; 20: (1): 216-20. doi: 10.1016/j.math.2014.07.004. Epub 2014 Jul 18. PMID: 25090974. |
[40] | Lotze M, Moseley GL. Theoretical considerations for chronic pain rehabilitation. Phys Ther. (2015) Sep; 95: (9): 1316-20. doi: 10.2522/ptj.20140581. Epub 2015 Apr 16. PMID: 25882484. |
[41] | Moseley L. Combined physiotherapy and education is efficacious for chronic low back pain. Aust J Physiother. (2002) ; 48: (4): 297-302. doi: 10.1016/s0004-9514(14)60169-0. PMID: 12443524. |
[42] | Moseley GL. A pain neuromatrix approach to patients with chronic pain. Man Ther. (2003) Aug; 8: (3): 130-40. doi: 10.1016/s1356-689x(03)00051-1. PMID: 12909433. |
[43] | Moseley GL, Butler D. Explain Pain Supercharged. Adelaide: Noi Group Publication; (2017) . |
[44] | Moseley GL. Widespread brain activity during an abdominal task markedly reduced after pain physiology education: fMRI evaluation of a single patient with chronic low back pain. Aust J Physiother. (2005) ; 51: (1): 49-52. doi: 10.1016/s0004-9514(05)70053-2. PMID: 15748125. |
[45] | Moseley L. Joining forces – combining cognition-targeted motor control training with group or individual pain physiology education: A successful treatment for chronic low back pain. Journal of Manual & Manipulative Therapy. (2003) apr; 11: (2): 88-94. doi: 10.1179/106698103790826383. |
[46] | Moseley GL. Evidence for a direct relationship between cognitive and physical change during an education intervention in people with chronic low back pain. Eur J Pain. (2004) Feb; 8: (1): 39-45. doi: 10.1016/S1090-3801(03)00063-6. PMID: 14690673. |
[47] | Moseley GL, Nicholas MK, Hodges PW. A randomized controlled trial of intensive neurophysiology education in chronic low back pain. Clin J Pain. (2004) Sep-Oct; 20: (5): 324-30. doi: 10.1097/00002508-200409000-00007. PMID: 15322439. |
[48] | King R, Robinson V, Elliott-Button HL, Watson JA, Ryan CG, Martin DJ. Pain reconceptualisation after pain neurophysiology education in adults with chronic low back pain: A qualitative study. Pain Res Manag. (2018) Sep 12; 2018: : 3745651. doi: 10.1155/2018/3745651. PMID: 30275918; PMCID: PMC6157134. |
[49] | Téllez-García M, de-la-Llave-Rincón AI, Salom-Moreno J, Palacios-Ceña M, Ortega-Santiago R, Fernández-de-Las-Peñas C. Neuroscience education in addition to trigger point dry needling for the management of patients with mechanical chronic low back pain: A preliminary clinical trial. J Bodyw Mov Ther. (2015) Jul; 19: (3): 464-72. doi: 10.1016/j.jbmt.2014.. Epub 2014 Nov 22. PMID: 26118519. |
[50] | Ryan CG, Gray HG, Newton M, Granat MH. Pain biology education and exercise classes compared to pain biology education alone for individuals with chronic low back pain: A pilot randomised controlled trial. Man Ther. (2010) Aug; 15: (4): 382-7. doi: 10.1016/j.math.2010.03.003. Epub 2010 Mar 31. PMID: 20359937. |
[51] | Louw A, Farrell K, Landers M, Barclay M, Goodman E, Gillund J, McCaffrey S, Timmerman L. The effect of manual therapy and neuroplasticity education on chronic low back pain: A randomized clinical trial. J Man Manip Ther. (2017) Dec; 25: (5): 227-234. doi: 10.1080/10669817.2016.1231860. Epub 2016 Sep 22. PMID: 29449764; PMCID: PMC5810776. |
[52] | Nijs J, Paul van Wilgen C, Van Oosterwijck J, van Ittersum M, Meeus M. How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines. Man Ther. (2011) Oct; 16: (5): 413-8. doi: 10.1016/j.math.2011.04.005. Epub 2011 May 31. PMID: 21632273. |
[53] | Pires D, Cruz EB, Caeiro C. Aquatic exercise and pain neurophysiology education versus aquatic exercise alone for patients with chronic low back pain: A randomized controlled trial. Clin Rehabil. (2015) Jun; 29: (6): 538-47. doi: 10.1177/0269215514549033. Epub 2014 Sep 8. PMID: 25200879. |
[54] | Bodes Pardo G, Lluch Girbés E, Roussel NA, Gallego Izquierdo T, Jiménez Penick V, Pecos Martín D. Pain neurophysiology education and therapeutic exercise for patients with chronic low back pain: A single-blind randomized controlled trial. Arch Phys Med Rehabil. (2018) Feb; 99: (2): 338-347. doi: 10.1016/j.apmr.2017.10.016. Epub 2017 Nov 11. PMID: 29138049. |
[55] | Wijma AJ, van Wilgen CP, Meeus M, Nijs J. Clinical biopsychosocial physiotherapy assessment of patients with chronic pain: The first step in pain neuroscience education. Physiother Theory Pract. (2016) Jul; 32: (5): 368-84. doi: 10.1080/09593985.2016.1194651. Epub 2016 Jun 28. PMID: 27351769. |
[56] | Ibrahim AA, Akindele MO, Ganiyu SO. Motor control exercise and patient education program for low resource rural community dwelling adults with chronic low back pain: A pilot randomized clinical trial. J Exerc Rehabil. (2018) Oct 31; 14: (5): 851-863. doi: 10.12965/jer.1836348.174. PMID: 30443533; PMCID: PMC6222156. |
[57] | Werner EL, Storheim K, Løchting I, Grotle M. The COPE LBP trial: Cognitive patient education for low back pain – a cluster randomized controlled trial in primary care. BMC Musculoskelet Disord. (2010) Feb 16; 11: : 33. doi: 10.1186/1471-2474-11-33. PMID: 20158897; PMCID: PMC2839981. |
[58] | Louw A, Puentedura EL, Mintken P. Use of an abbreviated neuroscience education approach in the treatment of chronic low back pain: A case report. Physiother Theory Pract. (2012) Jan; 28: (1): 50-62. doi: 10.3109/09593985.2011.562602. Epub 2011 Jul 3. PMID: 21721995. |
[59] | van Wilgen CP, Keizer D. The sensitization model to explain how chronic pain exists without tissue damage. Pain Manag Nurs. (2012) Mar; 13: (1): 60-5. doi: 10.1016/j.pmn.2010.03.001. Epub 2010 Jul 22. PMID: 22341140. |
[60] | Louw A, Nijs J, Puentedura EJ. A clinical perspective on a pain neuroscience education approach to manual therapy. J Man Manip Ther. (2017) Jul; 25: (3): 160-168. doi: 10.1080/10669817.2017.1323699. Epub 2017 May 22. PMID: 28694679; PMCID: PMC5498797. |
[61] | Ibrahim AA, Akindele MO, Ganiyu SO, Bello B. Effects of motor control exercise and patient education program in the management of chronic low back pain among community-dwelling adults in rural Nigeria: A study protocol for a randomized clinical trial. Integr Med Res. (2019) Jun; 8: (2): 71-81. doi: 10.1016/j.imr.2019.02.001. Epub 2019 Feb 21. PMID: 31080731; PMCID: PMC6506610. |
[62] | Dolphens M, Nijs J, Cagnie B, Meeus M, Roussel N, Kregel J, Malfliet A, Vanderstraeten G, Danneels L. Efficacy of a modern neuroscience approach versus usual care evidence-based physiotherapy on pain, disability and brain characteristics in chronic spinal pain patients: Protocol of a randomized clinical trial. BMC Musculoskelet Disord. (2014) May 8; 15: : 149. doi: 10.1186/1471-2474-15-149. PMID: 24885889; PMCID: PMC4028010. |
[63] | Paininmotion.be. [cited 2022 Sep 29]. Available from: http://www.paininmotion.be/EN/Education-booklet-FRENCH. |
[64] | Louw A. Why Do I Hurt? A Neuroscience Approach to Pain. OPTP; Minneapolis, MN, USA: (2013) . |
[65] | Francais – [Internet]. Retrain Pain Foundation. [cited 2022 Sep 29]. Available from: https://www.retrainpain.org/francais. |
[66] | Recovery strategies – pain guidebook – [Internet]. Greg Lehman. [cited 2022 Sep 29]. Available from: http://www.greglehman.ca/recovery-strategies-pain-guidebook. |
[67] | Tegner H, Frederiksen P, Esbensen BA, Juhl C. Neurophysiological pain education for patients with chronic low back pain: A systematic review and meta-analysis. Clin J Pain. (2018) Aug; 34: (8): 778-786. doi: 10.1097/AJP.0000000000000594. PMID: 29443723. |
[68] | Moseley GL: Painful Yarns. Metaphors and Stories to Help Understand the Biology of Pain. Canberra, Australia, Dancing Giraffe Press, (2007) . |
[69] | O’Keeffe M, Purtill H, Kennedy N, O’Sullivan P, Dankaerts W, Tighe A, Allworthy L, Dolan L, Bargary N, O’Sullivan K. Individualised cognitive functional therapy compared with a combined exercise and pain education class for patients with non-specific chronic low back pain: Study protocol for a multicentre randomised controlled trial. BMJ Open. (2015) Jun 1; 5: (6): e007156. doi: 10.1136/bmjopen-2014-007156. PMID: 26033941; PMCID: PMC4458611. |
[70] | Vier C, Bracht MA, Neves ML, Junkes-Cunha M, Santos ARS. Effects of spinal manipulation and pain education on pain in patients with chronic low back pain: A protocol of randomized sham-controlled trial. Integr Med Res. (2018) Sep; 7: (3): 271-278. doi: 10.1016/j.imr.2018.04.003. Epub 2018 May 10. PMID: 30271716; PMCID: PMC6160616. |
[71] | Wälti P, Kool J, Luomajoki H. Short-term effect on pain and function of neurophysiological education and sensorimotor retraining compared to usual physiotherapy in patients with chronic or recurrent non-specific low back pain, a pilot randomized controlled trial. BMC Musculoskelet Disord. (2015) Apr 10; 16: : 83. doi: 10.1186/s12891-015-0533-2. PMID: 25887550; PMCID: PMC4413527. |
[72] | Rizzo RRN, Medeiros FC, Pires LG, Pimenta RM, McAuley JH, Jensen MP, Costa LOP. Hypnosis enhances the effects of pain education in patients with chronic nonspecific low back pain: A randomized controlled trial. J Pain. (2018) Oct; 19: (10): 1103.e1-1103.e9. doi: 10.1016/j.jpain.2018.03.013. Epub 2018 Apr 11. PMID: 29654980. |
[73] | Mansouri E, Kostur L. Preliminary descriptive study on pain neurophysiologie education for patients with chronic low back pain: Use of an illustrative brochure. Kinésithérapie, la Revue. (2018) Jan; 18: (193): 10-8. doi: 10.1016/j.kine.2017.11.003. |
[74] | Quinter J et Cohen M. Painlosophy. What is at hub of “pain revolution”? [cited 2023 Apr 18]. Available from: https://painlosophy.wordpress.com/2023/02/07/what-is-at-the-hub-of-pain-revolution/. |
[75] | Roy M. Can pain be re-experienced as a conditioned response? PAIN. (2022) ; 163: : e1102-e1103. doi: 10.1097/j.pain.0000000000002622. |
[76] | Cohen M, Weisman A, Quintner J. Pain is not a “thing”: How that error affects language and logic in pain medicine. J Pain. (2022) Aug; 23: (8): 1283-1293. doi: 10.1016/j.jpain.2022.03.235. Epub 2022 Apr 12. PMID: 35427806. |
[77] | Dontenwille M, Halimi A, Jarroir C et Moulin M. Guide d’éducation à la douleur [cited 2023 Apr 18]. Available from: http://www.kinefact.com/wp-content/uploads/2021/12/Guide-Final-Rev-6.pdf. |
[78] | Barbari V, Storari L, Maselli F, Testa M. Applicability of pain neuroscience education: Where are we now? J Back Musculoskelet Rehabil. (2021) ; 34: (4): 511-520. doi: 10.3233/BMR-200091. PMID: 33749636. |
[79] | O’Sullivan PB, Caneiro JP, O’Keeffe M, Smith A, Dankaerts W, Fersum K, O’Sullivan K. Cognitive functional therapy: An integrated behavioral approach for the targeted management of disabling low back pain. Phys Ther. (2018) May 1; 98: (5): 408-423. doi: 10.1093/ptj/pzy022. Erratum in: Phys Ther. 2018 Oct 1; 98(10): 903. PMID: 29669082; PMCID: PMC6037069. |
[80] | Caneiro JP, Smith A, Bunzli S, Linton S, Moseley GL, O’Sullivan P. From fear to safety: A roadmap to recovery from musculoskeletal pain. Phys Ther. (2022) Feb 1; 102: (2): pzab271. doi: 10.1093/ptj/pzab271. PMID: 34971393. |


