
Personality construct as a biomarker in fibromyalgia: A narrative review from an autonomic rehabilitation perspective
Abstract
BACKGROUND:
The heterogeneity of symptoms and ineffective treatment raise questions about the current diagnostic criteria of fibromyalgia (FM). Misdiagnosis of FM often leads to less than efficacious treatment and poor quality of life.
OBJECTIVE:
This article reviews relevant evidence-based literature on personality traits in FM patients with an autonomic dysfunction perspective based on a hierarchical model to explain the utility of considering the personality trait in FM diagnosis.
METHODS:
A narrative review of articles concerning chronic pain, FM, and personality traits with respect to autonomic dysfunction in FM was conducted after extensive relevant literature searches.
RESULTS:
Reports discussing the predisposing factors, including coping styles, anger, suicide risk, a lack of physical activity and social support, in maintaining persistent pain in FM exist. Relationships between pain duration and severity and personality traits like neuroticism and extraversion have been reported. Coexisting clinical manifestations of FM like sleep disorders, anxiety, and intestinal irritability indicate autonomic dysfunction.
CONCLUSIONS:
This article lays out a constructive framework for individualized and personalized medicine for the effective rehabilitation of FM patients. The quest to find a definitive diagnosis of FM should include personality biomarkers that might translate into personalized medicine. An individualistic approach may bank upon artificial intelligence algorithms for both diagnostic as well as prognostic purposes in FM.
1.Introduction
Fibromyalgia (FM) is a chronic pain disorder that is characterized by diffuse musculoskeletal pain, fatigue, sleep disturbance, stiffness, and mood changes [1]. This disorder is present in 2–4% of the population, with a high preponderance in women [2]. An interplay of biology (estrogen), psychology, and sociocultural factors lead to a female preponderance in FM [3]. FM affects the quality of life and productivity because of absenteeism and disability [4].
The diagnosis of FM is based on the clinical evaluation and the New American College of Rheumatology (ACR) criteria centered on diffuse pain index and symptom severity score. A lack of definitive treatment for FM disorder raises questions about the current diagnostic criteria [5]. A systematic review carried out to discuss personality and FM, focuses on the types and models of personality as available in the literature. However, it fails to reach a consensus about a specific personality type in FM patients and instead, highlights heterogeneity in measures of personality as summarised in the results and discussion of this systematic review [5]. Our review, in contrast, discusses personality types in a functional manner i.e. how different personality types affect coping strategies and stress responses lead to autonomic dysfunction in FM. We also state that personality also affects exercise behavior and physical fitness and thereby further modulates the autonomic status in FM. Therefore we focus primarily on autonomic dysfunction as affected by personality in our narrative review.
The role of central sensitization [the higher gain setting of pain processing] and peripheral tissue abnormalities in FM have been discussed [6]. The phenomenon of central sensitization occupies a central stage in the pathogenesis of FM in causing allodynia and hyperalgesia. This phenomenon may be responsible for amplified pain perception and manifest as reduced mechanical and thermal thresholds in FM patients. A peripheral stimulus in a susceptible individual is amplified by the sensory system at the dorsal roots and further increases in intensity as it reaches the somatosensory cortex and causes high-level nociceptive perception. Thus a higher gain setting causes central amplification. Such amplification of pain perception, which is generated in an abnormal and progressively increased response over time, similar to the epilepsy wind-up or kindling phenomenon, forms the basis of widespread pain in FM patients [7, 8]. FM seems to be in a continuum ranging from peripheral nociceptive to neuropathic and finally to centralized pain conditions [9]. Abnormal stress response and poor social relationships contribute to maintaining and reinforcing pain in FM. In the framework of a diathesis-stress model of disease, the personality plays a vital role in making people more vulnerable to stressors leading to FM [10]. Personality modulates the neurophysiological milieu, which may underlie the pathogenesis of chronic pain syndromes such as FM [11]. The impact of predisposing personality on multiple symptoms, including widespread pain, in the context of autonomic dysfunction in FM remains to be deciphered and thus forms the primary objective of this study.
Chronic widespread pain is associated with a high sympathetic and low parasympathetic tone among FM patients. The resultant physical inactivity and behavioral changes are often modulated by personality constructs [12, 13]. The role of personality attributes in shaping coping processes and interpersonal relationships across different trajectories of chronic pain disorders in old age has been described [14]. Personality constructs leading to symptom heterogeneity affect the compliance of FM patients with medical and psychological interventions and treatment utilization [15]. Pain-prone personality is known to exist, but the status of FM-specific personality is yet unknown. In light of autonomic dysfunction, it would also be worthwhile to investigate how personality traits affect the pain threshold, how an ‘FM-prone’ personality evolves as the disease progresses, and how FM-specific personality affects perception and amplification of pain further. The other pertinent questions posed are how FM-specific personality affects pain-induced stress response, how people with different personality types assess stressful events which may trigger, exaggerate or maintain widespread pain response only in a few individuals, and how personality-dependent stress response manifests in terms of multi-system affliction involving autonomic nervous system in FM. Most importantly, an individually targeted approach may be framed to help manage personality traits, such as catastrophizing, that might interfere with treatment and recovery. Such an approach would also assist in framing management protocols for FM patients for their efficient autonomic- and pain rehabilitation. In this paper, we present a logical flow of evidence based on the literature search to highlight the need and various aspects of personality factors interacting with autonomic function and stress response in FM. Such an approach appears to be rational because it also includes a mechanistic modelling approach to elaborate on how personality affects and integrates various stress responses. This paper also has an elaborate section on the limitations of existing diagnostic modalities of FM and underscores the importance of a personalized medicine for such patients. Personality determines and influences behavior and a bidirectional effect ensues which is implicated in wide spread chronic pain, fatigue and sleep changes. Such biopsychological factors involved in the pathogenesis of FM can be described using a hierarchical model which is described in detail in the following text. This article intends to present a viewpoint based on evidence-based literature on personality traits in FM patients with an autonomic nervous system dysfunction perspective, based on the hierarchical model to explain the importance of including the personality biomarker in diagnosis of FM. This study was not registered in any international protocols registry, such as Prospero, because it is a narrative review.
2.Challenges with existing diagnostic modalities for FM
All attempts to identify a single, objective, measurable biomarker for FM diagnosis have been futile [16]. Heart rate variability (HRV) analysis in FM patients shows significantly lower HRV indicating a lower parasympathetic and increased sympathetic activity. A decreased HRV response to physical and mental stress and a characteristic nocturnal increase in sympathetic activity is seen in FM patients [17]. However, the HRV features are non-specific and have to be correlated with clinical features for FM diagnosis. Some disorders like irritable bowel syndrome are characterized by impaired pain processing and sympathetic hyperactivity. Although recurrent abdominal pain associated with altered bowel habits, and non-painful abdominal discomfort is pathognomic of irritable syndrome, majority of patients present with anxiety and depression as well as other visceral and somatic pain-related symptom [18, 19]. Overlapping symptoms of FM and irritable bowel syndrome suggest dysregulation of the gut-brain axis pointing to autonomic dysfunction [20]. Metabolic markers (hippuric acid, 2-hydroxyisobutyric, and lactic acids) in the gut microbiome indicate an impaired gut-brain axis due to stress in FM [21]. Some metabolites and associated metabolic pathways related to pain characteristics, including severity, have been discussed [22]. Detection of metabolite markers (taurine, Creatine, and succinic acid) is related to pain and fatigue in FM. Several neurotransmitters/factors are elevated (e.g. substance P, glutamate, Nerve growth factor, Calcitonin gene-related peptide, brain-derived neurotrophic factors, Corticotrophin-Releasing hormone) or lowered (Mu-opioid receptors on B lymphocytes) significantly in FM patients [21, 23].
Muscle symptoms are due to pain and inactivity and this vicious cycle further fuels the pain mechanisms. Muscle structure in FM reveals no difference amongst FM patients and healthy controls on histological examination and imaging. However, muscle cross-sectional area and muscle thickness correlates inversely with social isolation and fatigue respectively. Muscle strengthening, exercise stretching, aerobic training, balance training , and postural stabilization have been discussed in FM but still, there is no widely accepted notion on type, duration, and intensity of physical activity in FM [24, 25].
Functional brain imaging techniques can detect FM patients’ functional and structural abnormalities, neural substrates, and alterations in pain and autonomic pathways. Functional magnetic resonance imaging (fMRI) studies reveal abnormal functional connectivity between various brain areas in FM patients and may demarcate new FM subtypes [26, 27]. Specific personality characteristics can be studied vis-à-vis frontal lobe hemodynamics (oxyhemoglobin levels) [28]. However, the objective functional brain imaging marker alone may not detect the complexity of the subjective nature of pain syndromes. Non-restorative sleep in FM patients is associated with other symptoms (e.g. psychological distress and fatigue). Low sleep efficiency, long wake time after sleep onset, and a high proportion of light sleep are common in FM sleep patterns. The presence of alpha waves during Non-rapid eye movement sleep (NREM) sleep is due to a vigilant arousal state and a shift toward wakefulness in patients with FM patients [29]. A higher incidence of alpha-delta sleep may aggravate pain [30]. However, a lack of consensus amongst various study groups and data heterogeneity suggests that an EEG signature of FM disorder is still challenging.
Likewise, gene polymorphisms affect monoamine metabolism or transport and may change the sensory pain processing and stress response. Some characteristic epigenetic modifications and single-nucleotide polymorphisms (SNPs) may be associated with anxiety-related personality traits and stress-related depression, and disparities in temporal summation to pain and resting nociceptive sensitivity [31]. Gene polymorphisms, having a role in NO metabolism, may lead to susceptibility to and pain sensitivity in FM [32]. Hypomethylated DNA patterns in genes implicated in stress response, DNA repair, and subcortical neuronal abnormalities are implicated in FM patients [33].
3.Shortcomings in the diagnosis of FM
No specific diagnostic laboratory test or biomarker is available for FM diagnosis. Inadequate attention has been paid to identifying personality profiles per se to utilize its benefit in managing multiple FM symptoms. Certain personality characteristics, such as neuroticism and extroversion, have been studied in FM patients, but the clinical validity is limited.
Existing reports, including cross-sectional studies, have not proven whether the predisposing personality traits to chronic pain persist throughout life or whether the personality characteristics develop and get altered after the initiation and progression of chronic pain disorders like FM [34].
4.Need to include personality biomarkers for FM diagnosis
Despite a considerable stride in employing various putative biomarkers for the diagnosis of FM, most modalities of objective biomarkers in FM are in their nascent state or are inconclusive. Just one biomarker for FM’s multifaceted symptoms may not be sufficient. Artificial intelligence (AI) based analytical tools can be used to combine multiple biomarkers into a “composite pain biomarker signature” [35]. Knowledge of the personality profile of patients with FM may assist clinicians in faster diagnosis and administration of psychotherapy to alleviate their symptoms [36, 37]. Identification and inclusion of specific personality traits as a biomarker with other diagnostic modalities would positively impact the rehabilitation of FM patients. Applying machine learning algorithms to generate classifiers to identify personality traits for diagnosing and subgrouping patients with FM can be very beneficial. Machine learning algorithms have been used to predict the risk of mental health conditions such as postpartum depression, and suicide in children and adolescents. Such algorithms have been developed based on Electronic Health records. A study was carried out for the development of a screening algorithm for borderline personality disorder which incorporates machine learning (ML) in a 2-step framework. In the first step, potential patients are selected based on the presence of comorbidities and characteristics. In the second step, predictive modelling is done to see if the patients most likely have borderline personality disorder [38]. Similarly, a multimodal AI-based framework has been used to monitor stress based on facial expressions, posture, heart rate, and computer interaction. Such models have been used to detect stress and identify stress over some time [39].
A lack of understanding of the complex association between personality and FM pathogenesis may lead to inefficient interventions. Individual phenotypic subtypes and comorbidities may affect FM presentations [21]. Highly heterogeneous subgroups are identified based on the attributes such as resilience and vulnerability to stress [40]. Clinical heterogeneity forms an essential picture of FM patients who can be regrouped based on the accompanying clinical variables such as pain, anxiety, depression, sleep disorders and psychological aspects, including personality and perceived social support [15, 41]. Subgroups based on different coping styles, self-esteem, and depression have been discussed in the literature, raising the need for actively considering different personality characteristics during management. This subgrouping would help formulate tailored rehabilitation programs for FM patients [42]. A dispositional personality may mold the pain experience and affect the rehabilitation of FM patients. The personality itself may alter with the change in the disease expression over time and pain-induced stress. The phenomenon of concept drift has been discussed in the context of machine learning (ML) application in personality research which describes how the prediction of a model is not constant over time because of everchanging traits/features and how the prediction error of a trained model increases over the application period of the model in such cases. Therefore a paradigm shift from fixed models to continuously learning models is required which is frequently evaluated and retrained [43].
A broader picture of life span trajectories that shape the personality might be considered during mechanistic causal model ling to ensure individualized treatment for FM patients. The management protocols should identify and analyze the coping strategies and various dimensions and psychophysiological endophenotypes of the personality of the FM patients concerning environment and genetic milieu [44].
5.How to study predisposing personality in FM?
Scores of emotional and behavioral characteristics constitute the personality per se which can be viewed as a spectrum from healthy variants to pathological attributes. Several models put forward many traits and dimensions that define various personality constructs. Many studies addressing personality in patients with chronic pain have used MMPI (Minnesota Multiphasic Personality Inventory) to demarcate organic and functional pain and predict treatment outcomes [45]. Other instruments to understand personality function in chronic pain include e.g. Neuroticism-Extroversion-Openness Personality Inventory (NEO-PI), the Myers–Briggs Type Indicator (MBTI), Millon Clinical Multiaxial Inventory (MCMI), the Temperament character inventory (TCI) [46]. Common consensus appears to advocate the human personality assessment across five (Big 5) dimensions: Openness to Experience, Conscientiousness, Agreeableness, Extraversion, and Neuroticism. An artificial intelligence algorithm can be used to extract a multidimensional personality profile in sync with clinical symptoms and other existing diagnostic markers in FM. The future holds promise in the successful extraction of biomarkers by using multi-approaches (e.g. decision trees and deep learning) and multimodal (behavioral, genetic, and metabolic) data [47].
Machine learning has been used in the diagnosis of breast cancer from x-rays, predicting the onset of gestational diabetes from electronic health records and identifying clusters of patients that share common features (both risk factors and treatment response) [48]. Artificial neural network, another popular form of AI has been widely used in clinical diagnosis and monitoring, image analysis and interpretation, and biomedical signal analysis [49]. Machine learning models are well-suited to study personality psychology from the data about human behavior, gathered from mobile sensing studies, digital footprints, and standard questionnaires [43].
Although MMPI and NEO-personality inventory can determine the relationship between personality traits and the development and maintenance of chronic pain. The TCI based on the psychobiological model of personality may be a better plausible model. The temperament element, which relies on the neurotransmitter levels affecting a stimulus-response pattern, maybe a reliable tool to determine personality in FM patients [2].
6.The FM personality in literature: An enigma?
Many studies explore how pain patients differ regarding personality dimensions and adaptation styles [50]. Personality affects the perception and acceptance of pain and produces variability in patients’ pain ratings with the same disease or trauma [51]. The FM patients have been found to possess personality traits such as being perfectionist, conscientious, committed, honest, and well-organized, but cause-and-effect relationships are yet to be established. Different coping strategies with a chronic stressful situation, i.e., chronic pain per se, have been studied. The association between personality and anger, self-efficacy, and social support, in patients with FM has been evaluated [52]. Traumatic childhood experiences may be the harbinger of FM disorder manifesting with psychological impairment [53].
Maladaptive personality traits (e.g., neuroticism) are emotionally unstable, associated with increased susceptibility to stressful life events, and utilize avoidance-coping mechanisms and catastrophizing to deal with stress. Higher neuroticism is also associated with symptom severity [54]. Neuroticism and openness experience has been considered positive predictive factors for the perception of labor pain [55]. The adaptive personality traits (e.g., high extraversion and conscientiousness) are less affected by daily stresses [56]. People with high extroversion levels are impulsive, uninhibited, and sociable and have active coping strategies for handling chronic pain [57].
The inadequate coping mechanism associated with maladaptive personality traits may underlie a chain of physiological responses that ultimately exacerbate the symptoms in FM patients [54, 58]. Poor coping, harm avoidance, fear avoidance, and pain catastrophizing behavior worsen pain by causing a conditioned avoidant response to aversive stimuli. This vicious cycle fuels the pain further and may maintain widespread pain [59]. FM patients are likely to have neurotic personalities, which form the basis of pain-anxiety [23]. FM patients may manifest as either an increased anxiety sensitivity resulting in exacerbation of fear-avoidance beliefs and avoidance behavior or as psychologically rewarding and maintaining a chronic pain behavior [60].
Many studies have shown the presence of alexithymic traits in FM patients, which may negatively affect coping mechanisms [61]. The alexithymic person’s failure to regulate negative emotions results in an altered autonomic status characterized by altered/higher levels of resting (tonic) sympathetic or cardiovascular activity [62]. FM patients with alexithymia as a personality construct find difficulty identifying and communicating feelings and might interpret emotional arousal as physical illness. Such patients tend to amplify their symptoms which manifest as widespread pain and distress. A high score on measures of anger is another characteristic personality construct in FM disorder [63]. Self-oriented perfectionism, neglect of basic bodily needs, and hyperactivity characterize a FM personality. Psychological variables, daily hassles, health behaviors, financial satisfaction, and social activity lower the threshold for perceived pain. High pain scores are also associated with abnormal concerns over bodily functions and vague somatic complaints [64].
7.Autonomic dysfunction: A tangible factor in relation to the personality construct in FM?
As a discrete instrument, the personality construct adds an exciting dimension and is associated with stress-related cardiovascular activity [65]. Such association may qualify as a good research question, the answer to which may help to broaden our knowledge about autonomic nervous system dysfunction in FM. The neurovisceral integrative model of dynamic autonomic regulation discusses stress-induced hypoactivation of the prefrontal cortex, which results in the disinhibition of the amygdala. This model brings the role of personality in the context of regulation of autonomic regulation to the forefront [66]. Stress-induced disinhibition of the amygdala results in increased sympathetic drive and a higher sympathetic tone. Cognitive and emotional awareness of painful symptoms stimulates the sympathetic nervous system and worsens the pain [67].
Personality characteristics and HRV may be promising biomarkers for subject-specific differences in pain perception and response and prognostication. Studies addressing the effect of personality on pain-induced autonomic responses are sporadic [50]. Similarly, the studies addressing the general relation between autonomic and personality variables are inconclusive because of differences and discrepancies in study design and subject selection. Furthermore, many factors determine autonomic parameters and personality variables, making it challenging to study a linear correlation between them [68].
The HRV is positively related to some personality traits (Extroversion, Openness, Agreeableness, Conscientiousness), but negatively associated with neuroticism [69]. The relationship between extroversion and a higher pain threshold has been noted. Neuroticism is associated with a sympathetic dominant resting state, lower resting parasympathetic reactivity and its slow recovery, and heightened parasympathetic reactivity to pain. The neuroticism score is highly predictive of the development of post-infectious infectious bowel syndrome, which shows autonomic symptoms similar to FM [70].
In those who score high on neuroticism, heightened and sustained sympathetic and cardiovascular reactivity and high morning cortisol levels are seen. However, normal cortisol reactivity in such individuals may represent a ceiling effect due to persistent baseline high cortisol levels. Neuroticism is also associated with disrupted circadian rhythms, which might manifest as sleep disorders in FM [71]. Differential autonomic responses to pain stimuli provide a common link that connects personality constructs and pain in FM disorder [68]. A plausible association between autonomic symptoms and personality explains the high sympathetic tone and maladaptive autonomic responses underlying diverse symptoms of e.g. anxiety and depression in FM [69].
Vagally mediated pain inhibition has been described in the literature, which supports the antinociceptive role of the parasympathetic system [72]. A low parasympathetic tone is observed in patients with FM, although the cause-and-effect relationship is not yet established [73].
8.Personality biomarker related to physical activity status in FM
Personality has been linked to physical activity and health behaviors; therefore, the exercise prescription in FM might be affected by personality traits [74]. The seeking for and avoidance of physical activity behavior is seen in individuals scoring high in Extraversion and Neuroticism, respectively. Regular physical activity may trim down sub-traits of neuroticism which can be ascribed to its anxiolytic and antidepressive effects. A physically active lifestyle is coupled with a lesser decrease in extraversion, agreeableness, conscientiousness, and openness to experience [74].
FM patients present with a vicious cycle of chronic pain and physical inactivity, which further leads to deconditioning of muscles and persistent pain and fatigue [75]. A cohesive narrative review discusses the association of psychosocial (e.g., personality traits) and behavioral (e.g. physical activity) factors with some biomarkers of pain and inflammation in chronic pain patients. Higher physical activity is associated with lower interleukin-6 and C-reactive protein levels. Needless to say, lower neuroticism is found to be related to elevated interleukin-6 levels [76].
9.FM and stress response: Do HPA axis abnormality and sympathetic dysfunction lead to pain proneness?
Insufficient adaptation to stressors, increased catastrophizing, and poor coping skills prevail in pain patients [77]. Maladaptive coping strategies lead to deficient stress response to changes in the reactivity of the HPA axis and autonomic nervous system [78] Patients with FM show an abnormal underactive stress reactivity involving the hypothalamic-pituitary axis (HPA) [79]. Inconsistent results regarding the HPA axis abnormalities in FM exist in the literature (decreased or normal urinary free cortisol, loss of diurnal cortisol fluctuation, and elevated evening cortisol levels). As seen in response to physiological stimuli, a loss of resiliency of the HPA axis may be the putative cause of basal hypercortisolemia with a lack of circadian variation in FM patients [80]. The HPA hypofunction in FM is revealed by low secretion of corticotropin-releasing hormone (CRH) and adrenocorticotropic hormone (ACTH) levels. This hypofunction results in either secondary atrophy of the adrenal glands or reduced response of adrenal cortisol to ACTH [81].
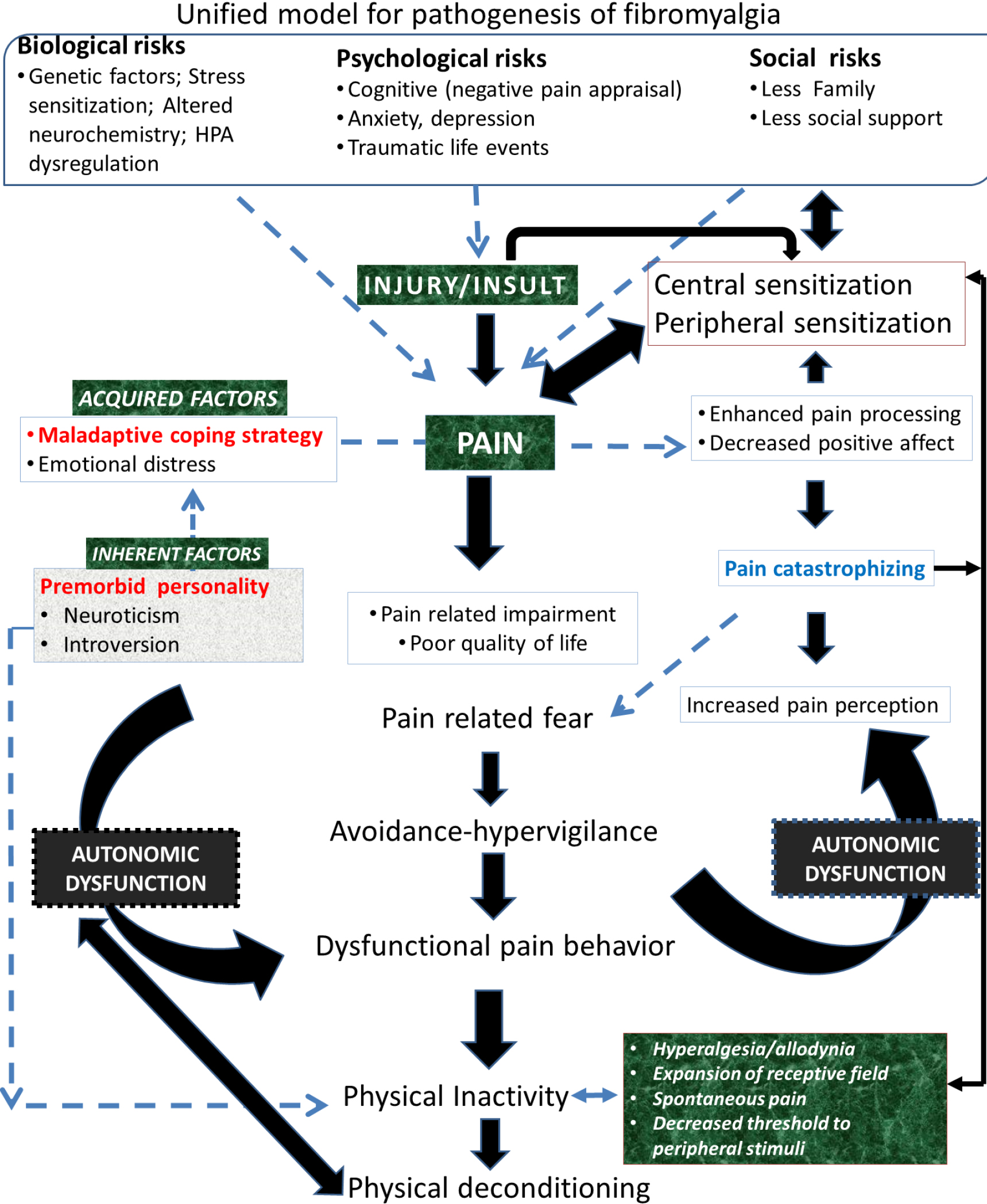
Figure 1.
A hierarchical model inclusive of personality and associated psychophysiological correlates that may affect the etiopathogenesis of fibromyalgia has been proposed on the framework of the top-down biopsychosocial model. This model also encompasses the physiological mechanism of widespread pain caused due to both central and peripheral sensitization. Autonomic dysfunction is proposed to be the key element connecting characteristic personality traits and behavior adaptations bringing out widespread pain in fibromyalgia.
10.Proposed model for FM inclusive of personality with an inherent autonomic dysfunction
The biopsychosocial model of illness includes various internal and external factors affecting the pathophysiology of FM. This model highlights multiple aspects of pain perception and amplification [77]. A hierarchical model is derived from the existing reductionist biopsychosocial model, which connects personality, coping mechanisms, and neurobiological responses (Fig. 1). In this hierarchical model, the personality assumes a more significant role as an effector for physiological responses leading to diverse clinical features in patients with FM [2]. Integrating the central sensitization process of pain-related neural pathways with biopsychosocial inputs may underlie the bidirectional brain-body pathway responses [82]. The bi-directionality of the response mechanism is implicated in triggering a vicious cycle of pain, sleep changes, and fatigue which is intensified by maladaptive coping techniques and lack of physical activity. All bio-psycho-social factors causing emotional distress may activate abnormal physiological stress responses if there is an inadequate filtering mechanism (including personality and culturally determined belief systems). Certain personality disturbances developing over time might be primarily a consequence of the pain problem and not a predisposing factor. Nevertheless, this model corroborates the relationship between personality and coping strategies chosen by a stressed individual.
We also propose that as the mechanistic evidence for the etiopathogenesis of FM remains sparse, autonomic dysfunction as a function of personality can be considered central to the development and persistence of widespread pain and other coexisting symptoms in our unified model of FM. This autonomic abnormality assumes greater importance because of a lack of physical inactivity in FM patients, which, in turn, promotes further worsening of autonomic status in an endless loop.
11.Conclusion
The ‘personality’ may directly predispose to FM or may rope in other psychosocial traits like anxiety and depression to aggravate and maintain pain by intensifying the sensitization process both at the peripheral and central levels. Even if this hypothesis is only partly supported, it makes a case for personality assessment to be a universal part of the practice of FM diagnosis. Pain research has, of late, acknowledged that personality is an important variable associated with vulnerability to chronic pain and the pain experience. The evidence warrants the assessment of personality to augment the effectiveness of FM diagnosis and treatment in view of best clinical practices. Adherence to active coping strategies in FM patients with maladaptive traits may help enhance their quality of life and improve their pain.
Moreover, ‘at risk’ individuals associated with multifaceted symptoms and behaviors can be identified using the Big 5 and Temperament and Character Inventory, respectively. We believe that including personality biomarkers in the FM diagnosis can help complement and foster personalized medicine. As personality seems to be an unavoidable factor in the etiopathogenesis of FM, future research should be tailored and designed to generate characteristic personality classifiers using ML algorithms that might also predict therapeutic outcomes. Further longitudinal studies can be planned to identify features associated with FM to develop an appropriate ML algorithm for an early diagnosis and risk stratification in FM.
Ethical approval
This study, as a literature review, is exempt from Institutional Review Board approval.
Informed consent
Not applicable.
Funding
None to report.
Author contributions
Both authors have equally contributed to the preparation of the manuscript.
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
None to report.
References
[1] | Kulshreshtha P, Gupta R, Yadav RK, et al. A comprehensive study of autonomic dysfunction in the fibromyalgia patients. Clin Auton Res. (2012) ; 22: : 117-122. |
[2] | Malin K. Personality and Fibromyalgia Syndrome. Open Rheumatol J. (2012) ; 6: : 273-285. |
[3] | Yunus MB. The role of gender in fibromyalgia syndrome. Curr Rheumatol Rep. (2001) ; 3: : 128-134. |
[4] | Maugars Y, Berthelot JM, Le Goff B, et al. Fibromyalgia and Associated Disorders: From Pain to Chronic Suffering, From Subjective Hypersensitivity to Hypersensitivity Syndrome. Front Med; 8; Epub ahead of print 2021. doi: 10.3389/fmed.2021.666914. |
[5] | Conversano C, Marchi L, Ciacchini R, et al. Personality Traits in Fibromyalgia (FM): Does FM Personality Exists? A Systematic Review. Clin Pract Epidemiol Ment Heal. (2018) ; 14: : 223-232. |
[6] | Staud R. Biology and therapy of fibromyalgia: Pain in fibromyalgia syndrome. Arthritis Res Ther. (2006) ; 8: : 1-7. |
[7] | Treede RD. Gain control mechanisms in the nociceptive system. Pain. (2016) ; 157: : 1199-1204. |
[8] | Eller-Smith OC, Nicol AL, Christianson JA. Potential mechanisms underlying centralized pain and emerging therapeutic interventions. Front Cell Neurosci. (2018) ; 12: : 1-18. |
[9] | Arnold LM, Choy E, Clauw DJ, et al. Fibromyalgia and chronic pain syndromes: A white paper detailing current challenges in the field. Clin J Pain. (2016) ; 32: : 737-746. |
[10] | Thiagarajah AS, Guymer EK, Leech M, et al. The relationship between fibromyalgia, stress and depression. Int J Clin Rheumtol. (2014) ; 9: : 371-384. |
[11] | Malin K, Littlejohn GO. Neuroticism in young women with fibromyalgia links to key clinical features. Pain Res Treat. (2012) ; Epub ahead of print 2012. doi: 10.1155/2012/730741. |
[12] | Kulshreshtha P, Gupta R, Yadav RK, et al. Effect of Low-Dose Amitriptyline on Autonomic Functions and Peripheral Blood Flow in Fibromyalgia: A Pilot Study. Pain Med. (2012) ; 13: : 131-136. |
[13] | Livermore JJA, Klaassen FH, Bramson B, et al. Approach-Avoidance Decisions Under Threat: The Role of Autonomic Psychophysiological States. Front Neurosci. (2021) ; 15: : 1-12. |
[14] | Wettstein M, Schilling OK, Wahl H-W. Trajectories of Pain in Very Old Age: The Role of Eudaimonic Wellbeing and Personality. Front Pain Res. (2022) ; 3: : 1-15. |
[15] | Gonzalez B, Novo R, Ferreira AS. Fibromyalgia: heterogeneity in personality and psychopathology and its implications. Psychol Heal Med. (2020) ; 25: : 703-709. |
[16] | Caboni P, Liori B, Kumar A, et al. Metabolomics analysis and modeling suggest a lysophosphocholines-PAF receptor interaction in fibromyalgia. PLoS One. (2014) ; 9: : 1-8. |
[17] | Meeus M, Goubert D, De Backer F, et al. Heart rate variability in patients with fibromyalgia and patients with chronic fatigue syndrome: A systematic review. Semin Arthritis Rheum. (2013) ; 43: : 279-287. |
[18] | Chalaye P, Goffaux P, Bourgault P, et al. Comparing pain modulation and autonomic responses in fibromyalgia and irritable bowel syndrome patients. Clin J Pain. (2012) ; 28: : 519-526. |
[19] | Mayer EA, Ryu HJ, Bhatt RR. The neurobiology of irritable bowel syndrome. Mol Psychiatry. (2023) ; 1-15. |
[20] | Malatji BG, Mason S, Mienie LJ, et al. The GC-MS metabolomics signature in patients with fibromyalgia syndrome directs to dysbiosis as an aspect contributing factor of FMS pathophysiology. Metabolomics. 15: ; Epub ahead of print 2019. doi: 10.1007/s11306-019-1513-6. |
[21] | Siracusa R, Di Paola R, Cuzzocrea S, et al. Fibromyalgia: Pathogenesis, mechanisms, diagnosis and treatment options update. (2021) ; Epub ahead of print 2021. doi: 10.3390/ijms22083891. |
[22] | Menzies V, Starkweather A, Yao Y, et al. Exploring Associations Between Metabolites and Symptoms of Fatigue, Depression and Pain in Women With Fibromyalgia. Biol Res Nurs. (2021) ; 23: : 119-126. |
[23] | Littlejohn G, Guymer E. Key milestones contributing to the understanding of the mechanisms underlying fibromyalgia. Biomedicines. (2020) ; 8: : 1-12. |
[24] | Umay E, Gundogdu I, Ozturk EA. What happens to muscles in fibromyalgia syndrome. Ir J Med Sci. (2020) ; 189: : 749-756. |
[25] | Sosa-Reina MD, Nunez-Nagy S, Gallego-Izquierdo T, et al. Effectiveness of Therapeutic Exercise in Fibromyalgia Syndrome: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Biomed Res Int. (2017) ; Epub ahead of print 2017. doi: 10.1155/2017/2356346. |
[26] | Tu Y, Cao J, Bi Y, et al. Magnetic resonance imaging for chronic pain: diagnosis, manipulation, and biomarkers. Sci China Life Sci. (2021) ; 64: : 879-896. |
[27] | López-Solà M, Woo CW, Pujol J, et al. Towards a neurophysiological signature for fibromyalgia. Pain. (2017) ; 158: : 34-47. |
[28] | Ehlis AC, Schneider S, Dresler T, et al. Application of functional near-infrared spectroscopy in psychiatry. Neuroimage. (2014) ; 85: : 478-488. |
[29] | Diaz-Piedra C, Di Stasi LL, Baldwin CM, et al. Sleep disturbances of adult women suffering from fibromyalgia: Asystematic review of observational studies. Sleep Med Rev. (2015) ; 21: : 86-99. |
[30] | Hackshaw KV. The Search for Biomarkers in Fibromyalgia. |
[31] | Gescher DM, Kahl KG, Hillemacher T, et al. Epigenetics in Personality Disorders: Today’s Insights. Front Psychiatry 9; Epub ahead of print 2018. doi: 10.3389/fpsyt.2018.00579. |
[32] | Janssen LP, Medeiros LF, DE Souza A, et al. Fibromyalgia: A review of related polymorphisms and clinical relevance. An Acad Bras Cienc. (2021) ; 93: : 1-13. |
[33] | D’Agnelli S, Arendt-Nielsen L, Gerra MC, et al. Fibromyalgia: Genetics and epigenetics insights may provide the basis for the development of diagnostic biomarkers. Mol Pain 15; Epub ahead of print 2019. doi: 10.1177/1744806918819944. |
[34] | Naylor B, Boag S, Gustin SM. New evidence for a pain personality? A critical review of the last 120 years of pain and personality. Scand J Pain. (2017) ; 17: : 58-67. |
[35] | Tracey I, Woolf CJ, Andrews NA. Perspective Composite Pain Biomarker Signatures for Objective Assessment and Effective Treatment. Neuron. (2019) ; 101: : 783-800. |
[36] | Bartkowska W, Samborski W, Mojs E. Cognitive functions, emotions and personality in woman with fibromyalgia. Anthropol Anzeiger. (2018) ; 75: : 271-277. |
[37] | Romeo A, Benfante A, Geminiani GC, et al. Personality, Defense Mechanisms and Psychological Distress in Women with Fibromyalgia. Behav Sci (Basel) 12 Epub ahead of print 2022. doi: 10.3390/bs12010010. |
[38] | Zang C, Goodman M, Zhu Z, et al. Development of a screening algorithm for borderline personality disorder using electronic health records. Sci Rep 12. Epub ahead of print 1 December 2022. doi: 10.1038/S41598-022-16160-Z. |
[39] | Walambe R, Nayak P, Bhardwaj A, et al. Employing Multimodal Machine Learning for Stress Detection. J Healthc Eng. (2021) ; Epub ahead of print 2021. doi: 10.1155/2021/9356452. |
[40] | Estévez-López F, Segura-Jiménez V, Álvarez-Gallardo IC, et al. Adaptation profiles comprising objective and subjective measures in fibromyalgia: The al-Ándalus project. Rheumatol (United Kingdom). (2017) ; 56: : 2015-2024. |
[41] | Yim YR, Lee KE, Park DJ, et al. Identifying fibromyalgia subgroups using cluster analysis: Relationships with clinical variables. Eur J Pain (United Kingdom). (2017) ; 21: : 374-384. |
[42] | Lundberg G, Anderberg UM, Gerdle B. Personality features in female fibromyalgia syndrome. J Musculoskelet Pain. (2009) ; 17: : 117-130. |
[43] | Stachl C, Pargent F, Hilbert S, et al. Personality Research and Assessment in the Era of Machine Learning. |
[44] | López-López A, González JL, Guerrero ÁL, et al. Stress, coping, and personality in patients with Epicrania fugax, and their relation to the clinical characteristics of pain. Pain Med (United States). (2017) ; 18: : 152-160. |
[45] | Weisberg JN, Boatwright BA. Mood, anxiety and personality traits and states in chronic pain. Pain. (2007) ; 133: : 1-2. |
[46] | Butcher JN, Williams CL. Personality Assessment with the MMPI-2: Historical Roots, International Adaptations, and Current Challenges. Appl Psychol Heal Well-Being. (2009) ; 1: : 105-135. |
[47] | Cerasa A, Lofaro D, Cavedini P, et al. Personality biomarkers of pathological gambling: A machine learning study. J Neurosci Methods. (2018) ; 294: : 7-14. |
[48] | Goecks J, Jalili V, Heiser LM, et al. How Machine Learning Will Transform Biomedicine. Cell. (2020) ; 181: : 92-101. |
[49] | Ramesh AN, Kambhampati C, Monson JRT, et al. Artificial intelligence in medicine. Ann R Coll Surg Engl. (2004) ; 86: : 334-338. |
[50] | Nitch SR, Boone KB. Normal personality correlates of chronic pain subgroups. J Clin Psychol Med Settings. (2004) ; 11: : 203-209. |
[51] | Vendrig AA. The Minnesota Multiphasic Personality inventory and chronic pain: A conceptual analysis of a long-standing but complicated relationship. Clin Psychol Rev. (2000) ; 20: : 533-559. |
[52] | Amir M, Neumann L, Bor O, et al. Coping styles, anger, social support, and suicide risk of women with fibromyalgia syndrome. J Musculoskelet Pain. (2000) ; 8: : 7-20. |
[53] | Vera Cruz G, Bucourt E, Réveillère C, et al. Machine learning reveals the most important psychological and social variables predicting the differential diagnosis of rheumatic and musculoskeletal diseases. Rheumatol Int. (2021) ; 1-10. |
[54] | Seto A, Han X, Price LL, et al. The role of personality in patients with fibromyalgia. Clin Rheumatol. (2019) ; 38: : 149-157. |
[55] | Yadollahi P, Khalaginia Z, Vedadhir A, et al. The study of predicting role of personality traits in the perception of labor pain. Iran J Nurs Midwifery Res. (2014) ; 19: : S97-S102. |
[56] | Afshar H, Roohafza HR, Keshteli AH, et al. The association of personality traits and coping styles according to stress level. J Res Med Sci. (2015) ; 20: : 353-358. |
[57] | Ramírez-Maestre C, López Martínez AE, Zarazaga RE. Personality characteristics as differential variables of the pain experience. J Behav Med. (2004) ; 27: : 147-165. |
[58] | Shepherd D, Mulgrew J, Hautus MJ. Exploring the autonomic correlates of personality. Auton Neurosci Basic Clin. (2015) ; 193: : 127-131. |
[59] | Conrad R, Schilling G, Bausch C, et al. Temperament and character personality profiles and personality disorders in chronic pain patients. Pain. (2007) ; 133: : 197-209. |
[60] | Pérez-Pareja J, Sesé A, González-Ordi H, et al. Fibromyalgia and chronic pain: Are there discriminating patterns by using the Minnesota Multiphasic Personality Inventory-2 (MMPI-2)? Int J Clin Heal Psychol. (2010) ; 10: : 41-56. |
[61] | Di Tella M, Tesio V, Ghiggia A, et al. Coping strategies and perceived social support in fibromyalgia syndrome: Relationship with alexithymia. Scand J Psychol. (2018) ; 59: : 167-176. |
[62] | Lumley MA, Neely LC, Burger AJ. The assessment of alexithymia in medical settings: Implications for understanding and treating health problems. J Pers Assess. (2007) ; 89: : 230-246. |
[63] | Sayar K, Gulec H, Topbas M. Alexithymia and anger in patients with fibromyalgia. Clin Rheumatol. (2004) ; 23: : 441-448. |
[64] | Lichtenberg PA, Swensen CH, Skehan MW. Further investigation of the role of personality, lifestyle and arthritic severity in predicting pain. J Psychosom Res. (1986) ; 30: : 327-337. |
[65] | Sperry SH, Kwapil TR, Eddington KM, et al. Psychopathology, everyday behaviors, and autonomic activity in daily life: An ambulatory impedance cardiography study of depression, anxiety, and hypomanic traits. Int J Psychophysiol. (2018) ; 129: : 67-75. |
[66] | Thayer JF, Lane RD. Claude Bernard and the heart-brain connection: Further elaboration of a model of neurovisceral integration. Neurosci Biobehav Rev. (2009) ; 33: : 81-88. |
[67] | De Ridder D, Adhia D, Vanneste S. The anatomy of pain and suffering in the brain and its clinical implications. Neurosci Biobehav Rev. (2021) ; 130: : 125-146. |
[68] | Paine P, Kishor J, Worthen SF, et al. Exploring relationships for visceral and somatic pain with autonomic control and personality. Pain. (2009) ; 144: : 236-244. |
[69] | Shepherd D, Mulgrew J, Hautus MJ. Exploring the autonomic correlates of personality. Auton Neurosci Basic Clin. (2015) ; 193: : 127-131. |
[70] | Paine P, Worthen SF, Gregory LJ, et al. Personality differences affect brainstem autonomic responses to visceral pain. Neurogastroenterol Motil. (2009) ; 21: : 1155-1163. |
[71] | Lahey BB. Public Health Significance of Neuroticism. Am Psychol. (2009) ; 64: : 241-256. |
[72] | Multon S, Schoenen J. Pain control by vagus nerve stimulation: From animal to man…and back. Acta Neurol Belg. (2005) ; 105: : 62-67. |
[73] | Reyes del Paso GA, de la Coba P. Reduced activity, reactivity and functionality of the sympathetic nervous system in fibromyalgia: An electrodermal study. PLoS One. (2020) ; 15: : 1-14. |
[74] | Rhodes RE, Boudreau P, Rhodes RE, et al. Physical Activity and Personality Traits. Oxford Res Encycl Psychol. (2017) ; 1-16. |
[75] | Kulshreshtha P, Deepak KK. Autonomic nervous system profile in fibromyalgia patients and its modulation by exercise: A mini review. Clinical Physiology and Functional Imaging. (2013) ; 33: : 83-91. |
[76] | Graham EK, Bastarache ED, Milad E, et al. Physical activity mediates the association between personality and biomarkers of inflammation. SAGE Open Med. (2018) ; 6: : 205031211877499. |
[77] | Ferrari R. The biopsychosocial model – A tool for rheumatologists. Best Pract Res Clin Rheumatol. (2000) ; 14: : 787-795. |
[78] | Grisart J, Scaillet N, Michaux M, et al. Determinants of representational and behavioral hyperactivity in patients with fibromyalgia syndrome. J Health Psychol. (2020) ; 25: : 1128-1137. |
[79] | Kadetoff D, Kosek E. Evidence of reduced sympatho-adrenal and hypothalamic-pituitary activity during static muscular work in patients with fibromyalgia. J Rehabil Med. (2010) ; 42: : 765-772. |
[80] | Crofford LJ, Young EA, Engleberg NC, et al. Basal circadian and pulsatile ACTH and cortisol secretion in patients with fibromyalgia and/or chronic fatigue syndrome. (2004) ; 18: : 314-325. |
[81] | Úbeda-D’Ocasar E, Jiménez Díaz-Benito V, Gallego-Sendarrubias GM, et al. Pain and Cortisol in Patients with Fibromyalgia: Systematic Review and Meta-Analysis. Diagnostics. (2020) ; 10: : 922. |
[82] | Disorders P, Trauma A. Innovations in Symptom Management Medical Symptoms without Identified Pathology? Relationship to. Ann Intern Med. (2001) ; 917-925. |


