
The association between marathon running and high-sensitivity cardiac troponin: A systematic review and meta-analysis
Abstract
BACKGROUND:
Marathon running is an extreme sport with a distance of about 42 kilometers. Its relationship to high-sensitivity cardiac troponin (hs-cTn) remains controversial.
OBJECTIVE:
As the gold standard for detecting myocardial injury, the trends of hs-cTn before and after a marathon were investigated and analyzed.
METHODS:
A literature search was conducted in PubMed, EMBASE, and Cochrane Library databases by combing the keywords marathon and troponin, and studies regarding high-sensitivity cardiac troponin I (hs-cTnI) and high-sensitivity cardiac troponin T (hs-cTnT) concentrations before and after marathon running (not for half-marathon and ultra-marathon) were included. “Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group” were used to assess the risk of bias. Statistical analysis was performed using Review Manager, presenting data as mean values and 95% confidence intervals (CIs). Sensitivity analysis and subgroup analysis were performed if there was high heterogeneity among studies based on I
RESULTS:
A total of 13 studies involving 824 marathoners were included in this systematic review and meta-analysis. Both hs-cTnI (MD 68.79 ng/L, [95% CI 53.22, 84.37],
CONCLUSION:
The concentrations of hs-cTnI and hs-cTnT were increased after marathon running, but the change of hs-cTnT is usually not seen as irreversible myocardial injury.
1.Introduction
Running has long been recognized as a physical activity that offers many benefits, such as improving aerobic fitness [1], enhancing cardiovascular function [2], and even reducing all-cause and cardiovascular mortality risk [3]. Therefore, an increasing number of people are attracted by this sport and take part in it regardless of age and gender, especially marathon running. According to global marathon statistics, more than 1.29 million people participated in the 2018 marathon [4]. However, many studies have reported changes in certain cardiac markers after a marathon, including ventricular structure and function [5], the rhythm of the heart [6], and myocardial biomarkers [7]. In fact, whether these changes are beneficial or harmful to humans is still unclear and needs further study.
As far as myocardial injury is concerned, it can be observed through the release of serum biomarkers after marathon running. There are many kinds of biomarkers commonly used in the clinical evaluation of the myocardial injury, including cardiac troponin (cTn), N-terminal pronatriuretic peptide (NT-proBNP), and creatine kinaseic peptide (CK-MB) [8, 9]. Among them, cTn has high specificity and sensitivity. It only exists in cardiomyocytes and is a complex composed of cardiac troponin I (cTnI), cardiac troponin T (cTnT), and cardiac troponin C (cTnC) subunits [10]. cTnI and cTnT are specific antigens to cardiomyocytes, which are degraded from myocardial fibers during cardiomyocyte injury [11]. Therefore, cTn I and cTn T are the most convenient and reliable detection indexes and are even considered the gold standard for detecting the state of myocardial injury [12].
With time, the detection sensitivity was further improved with the introduction of high-sensitivity cardiac troponin (hs-cTn) in 2007 [13], which has been widely used as the diagnostic threshold for myocardial infarction (MI) with its 99th percentile upper reference limit (URL) that refers to the normal upper limit value from 99% of the normal population measured [14]. Compared with traditional cTn, hs-cTn can measure disease-free people with accuracy down to single digits per liter of nanogram (ng/L). Furthermore, hs-cTn appears to be able to detect the release of cTn at an earlier stage, thus increasing the sensitivity of early diagnosis of myocardial injury [15]. For those patients with MI, high-sensitivity cardiac troponin I (hs-cTnI) and high-sensitivity cardiac troponin T (hs-cTnT) will rise within 1 hour and remain elevated for several days [16].
The debate on the association between marathon running and myocardial injury has lasted for a long time, but it can be mainly divided into two aspects: 1) whether marathon exercise will cause the increase of myocardial injury markers such as cTn; and 2) if the increase is indeed caused, then whether or not it represents pathological changes [17]. There was only one previous meta-analysis regarding the incidence of cTn elevations in marathon runners published in 2010, which is more than a decade ago [18]. In this systematic review and meta-analysis, we aimed to investigate the trends of hs-cTnI and hs-cTnT in marathon runners over time and to discuss the significance of these changes.
2.Methods
This systematic review and meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement [19]. This study, as a literature review, was exempt from Institutional Review Board approval. The protocol for this systematic review was registered on PROSPERO (registration ID CRD42022347908).
2.1Literature search
Considering the difference in the level of serum detection technology in different years [13], a literature search of English articles published from January 2007 to September 2022 in PubMed, EMBASE, and Cochrane Library databases was conducted. The keywords “marathon” and “troponin” were used. After eliminating duplicates, the abstracts were reviewed by two independent authors to further screen suitable studies based on inclusion and exclusion criteria. Subsequently, the full texts of the chosen studies were read to finalize which articles were included in this systematic review and meta-analysis. If there was a disagreement between the two authors in the literature screening process, the third author would participate in this process and make the final decision.
2.2Inclusion and exclusion criteria
The inclusion and exclusion criteria were established on the basis of the PICO principle: 1) ll study participants were healthy individuals who were free from heart disease; 2) the type of exercise was only a full-distance marathon, excluding half-marathon and ultra-marathon; 3) the self-control studies mainly compared the changes of biomarkers before and after marathon running were included; 4) there were two outcome indicators for assessing myocardial injury: hs-cTnI and hs-cTnT.
Table 1
Characteristics of the included studies
| Author (year) | Sample size (male) | Age (years) | BMI (kg/m | Marathon finish time (min) | Indicator | 99th percentile URL (ng/L) | Time points of sampling post-marathon (h) | Quality scores | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Backer et al. (2013) | 45 | (NM) | NM | NM | NM | hs-cTnT | 14 | 0 | Fair | |||
| Bernat-adell et al. (2019) | 86 | (74) | 38.62 | NM | 214.53 | hs-cTnT | 30 | 0, 24, 48, 96 | Fair | |||
| Eijsvogels et al. (2015) | 82 | (65) | 45 | 22.9 | 227 | hs-cTnI | 40 | 0 | Poor | |||
| Grabs et al. (2015) | 20 | (20) | 45 | 24.1 | 239 | hs-cTnT | 22 | 0 | Fair | |||
| Kaleta-Duss et al. (2020) | 35 | (35) | 39 | 25 | 234 | hs-cTnI | 34.2 | 0 | Fair | |||
| Kosowski et al. (2019) | 33 | (33) | 57 | 23.85 | 248 | hs-cTnT | 6.1 | 0 | Fair | |||
| Martínez-Navarro et al. (2020) | 77 | (64) | 38.72 | 22.87 | 215 | hs-cTnT | 14 | 0, 24, 48, 96 | Fair | |||
| Möhlenkamp et al. (2014) | 74 | (NM) | NM | 250 | hs-cTnI | 40 | 0 | Fair | ||||
| Paana et al. (2019) | 40 | (NM) | 48.19 | 23.63 | 248.1 | hs-cTnT | 14 | 0 | Fair | |||
| Richardson et al. (2018) | 52 | (39) | 39 | NM | 262 | hs-cTnT | 14 | 0 | Fair | |||
| Roca et al. (2017) | 79 | (57) | 39 | NM | 211.11 | hs-cTnT | 14 | 0, 48 | Poor | |||
| Scherr et al. (2011) | 102 | (NM) | 42.0 | 23.6 | 227 | hs-cTnT | 18 | 0, 24, 72 | Good | |||
| Schwarz et al. (2017) | 99 | (77) | 48.7 | 23.3 | 246.7 | hs-cTnT | NM | 0, 48 | Fair | |||
The data were presented as mena
2.3Data extraction
By reading the whole texts of included studies, the relevant data concerning the characteristics of participants (number, gender, age, BMI, and marathon finish time) and indicators (name, the 99th percentile URL, and measure time point) were extracted by two reviewers. The third reviewer checked the data and resolved the discrepancy.
2.4Quality assessment
Two researchers respectively assessed the included articles through the “Quality Assessment Tool for Before-After (Pre-Post) Studies With No Control Group” proposed by National Heart Lung and Blood Institute [20]. The tool contains 12 questions that can be answered in one of the following three ways: “Yes”, “No”, or “Other” (CD, cannot determine; NA, not applicable; NR, not reported). The overall quality of the included studies was rated good, fair, or poor. If the rating differed, the article was discussed by two researchers to reach a consensus. The third researcher would intervene to determine grades when there was still a disagreement.
2.5Statistical analysis
All data regarding characteristics of the included studies were presented as mean
3.Results
3.1Search results
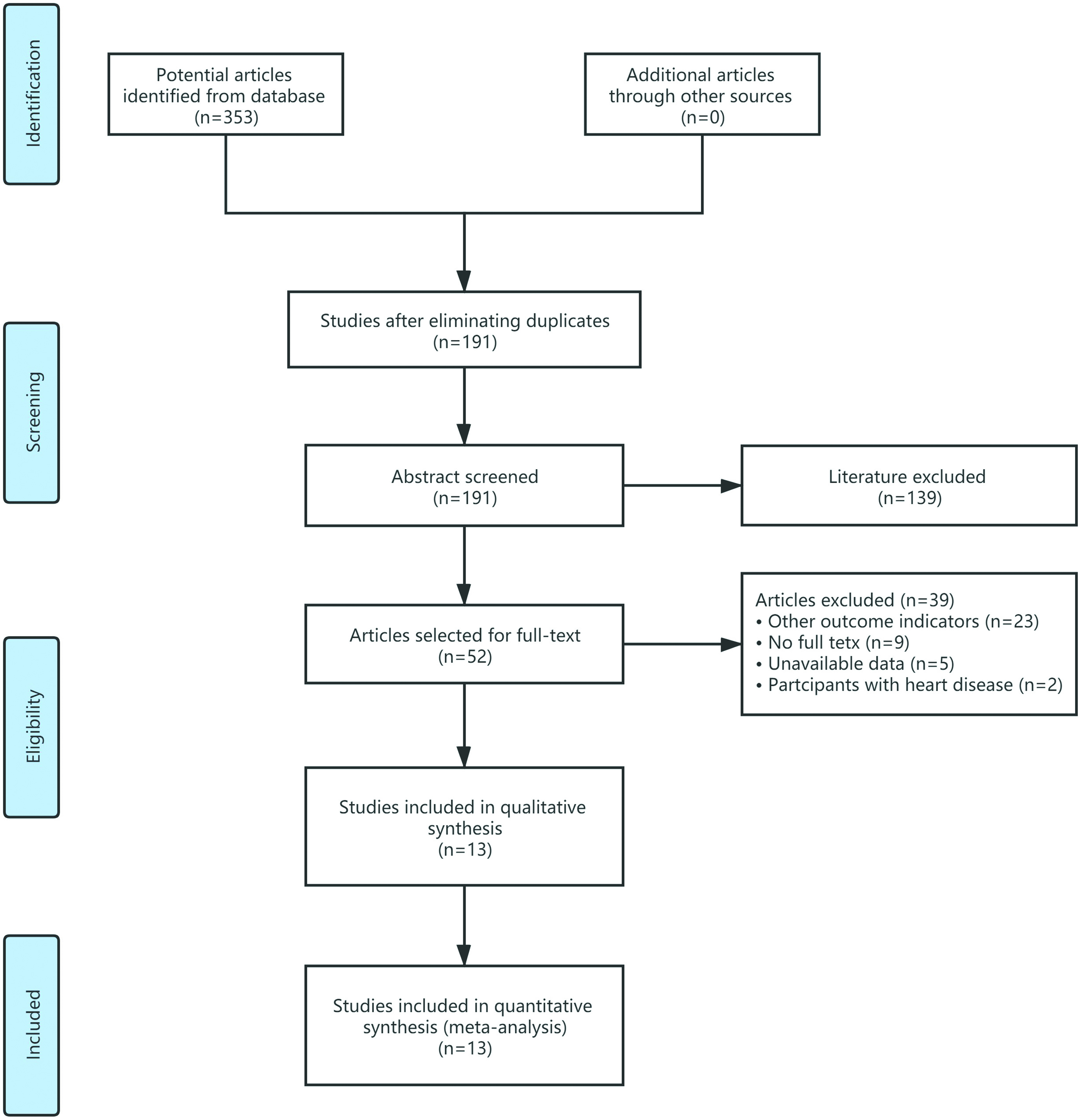
A primary search of three databases obtained 353 articles, and 191 abstracts were screened after eliminating the duplicates. Full texts of 52 studies were read to determine which literature was ultimately included, and 39 were excluded due to participants with heart disease, other outcome indicators, no full texts, and unavailable data. Therefore, a total of 13 articles were included in this systematic review and meta-analysis [26, 27, 38]. The detailed literature screening process is shown in Fig. 1.
Figure 1.
Literature screening process of systematic review and meta-analysis.
3.2Characteristics of the included studies
A total of 824 marathoners were included in this systematic review and meta-analysis, with a mean age of over 38 and an average BMI of over 22.87. The outcome indicator involved cTnI in 3 articles and cTnT in 10, which were measured from before and immediately after marathon running to 96 hours. The quality ratings are also exhibited in Table 1, except for one good and two poor, all of which were fair.
3.3The trends of hs-cTnI over time
Figure 2 shows that hs-cTnI was significantly increased after marathon running (MD 68.79 ng/L, [95% CI 53.22, 84.37],
Figure 2.
Forest plot for the trends of hs-cTnI over time.

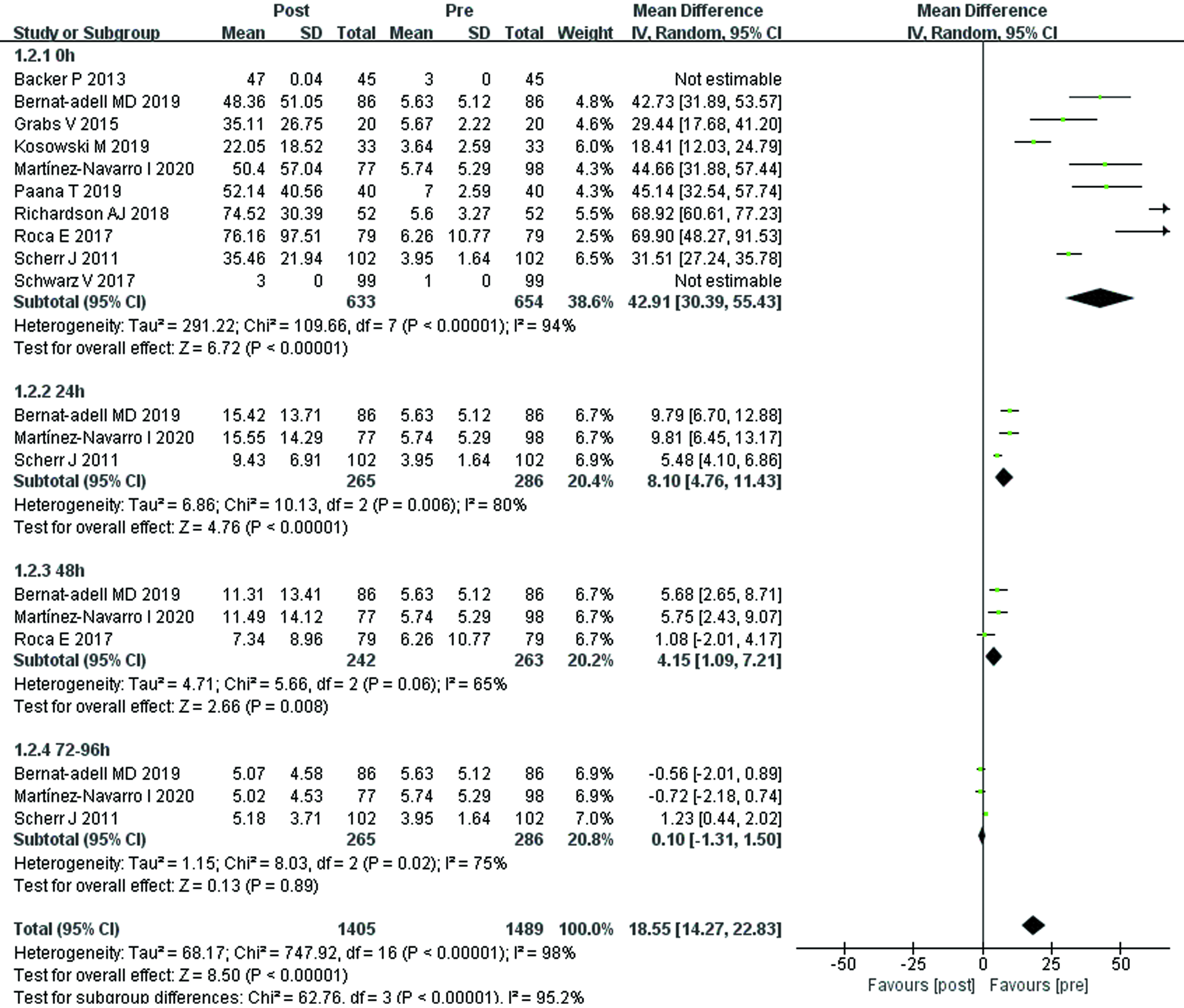
3.4The trends of hs-cTnT over time
Ten studies demonstrated the trends of hs-cTnT over time, all showing the results immediately after marathon running (MD 42.91 ng/L, [95% CI 30.39, 55.43],
Figure 3.
Forest plot for the trends of hs-cTnT over time.
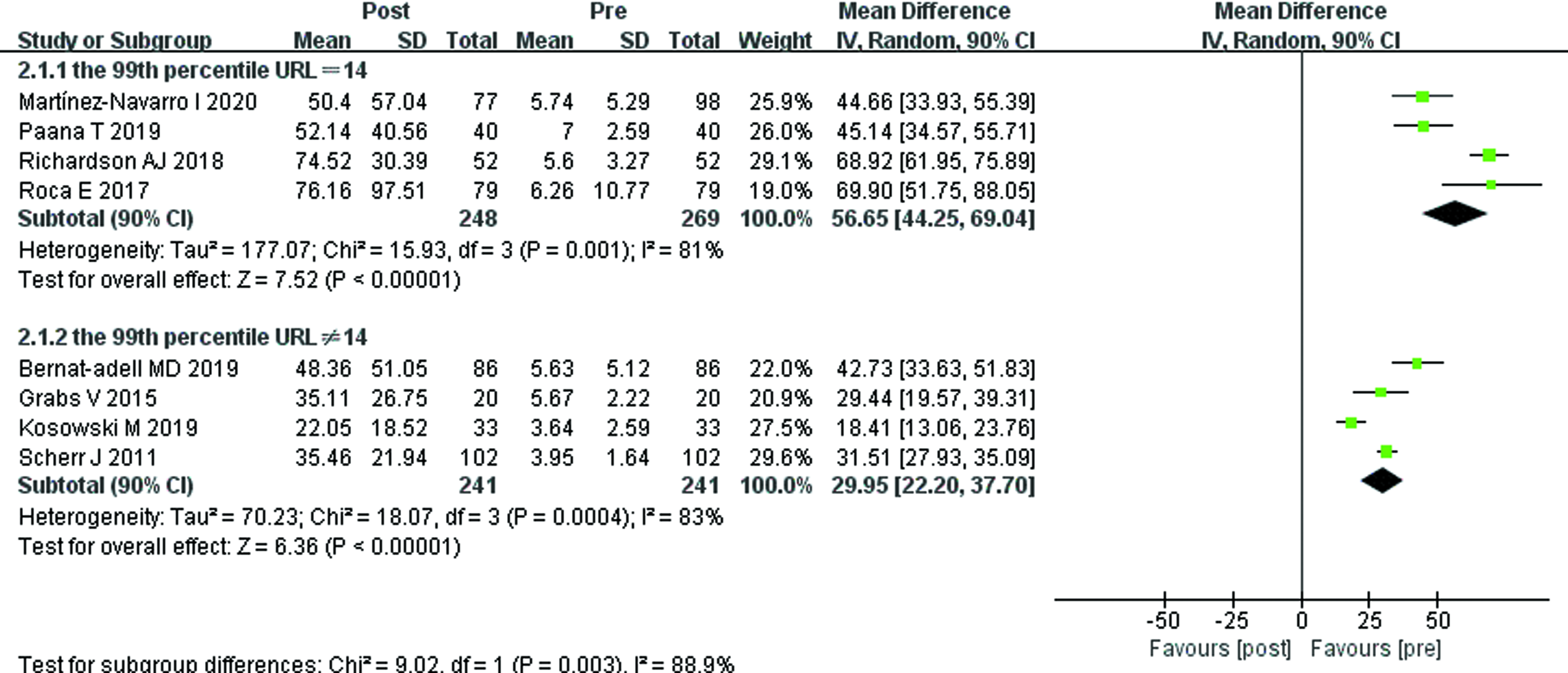
3.5Sensitivity analysis and subgroup analysis
Sensitivity analysis using the leave-one-out method indicated that no single study was a heterogeneous source of changes in hs-cTnT.
As shown in Fig. 4, subgroup analysis found that hs-cTnT of different 99th percentile URL groups were significantly increased after marathon running compared with before (MD 56.65 ng/L, [95% CI 44.25, 69.04],
Table 2
Subgroup analysis of hs-cTnT
| No. of trails | No. of participants | I | Mean (95% CI) | ||
|---|---|---|---|---|---|
| Overall | 8 | 633 | 0.94 | 42.91 [30.39, 55.43] | |
| Mean age (y) | |||||
| | 5 | 396 | 0.94 | 50.70 [33.17, 68.24] | 0.09 |
| | 3 | 93 | 0.86 | 30.29 [14.62, 45.97] | |
| Average marathon finish time (min) | |||||
| | 5 | 364 | 0.77 | 40.68 [32.31, 49.04] | 0.85 |
| | 3 | 125 | 0.98 | 44.08 [15.71, 72.44] | |
| The 99th percentile URL (ng/L) | |||||
| | 4 | 248 | 0.81 | 56.65 [44.25, 69.04] | 0.003 |
| | 4 | 241 | 0.83 | 29.95 [22.20, 37.70] |
URL: upper reference limit.
Figure 4.
Subgroup analysis for the 99th percentile URL of hs-cTnT.
4.Discussion
In this meta-analysis, we found that both hs-cTnI and hs-cTnT were elevated after running a marathon, but the concentration of hs-cTnT returned to baseline after 72 to 96 h post-race. The results of subgroup analyses concerning hs-cTnT demonstrated that the 99th percentile URL of hs-cTnT might be the source of heterogeneity among studies. As there are many other influences but few data, the factors causing the differences in measurement results of hs-cTnT need to be further studied and analyzed.
The results of our meta-analysis demonstrated that both the levels of hs-cTnI and hs-cTnT after the marathon running were significantly higher than those before the marathon. Similarly, the data from a meta-analysis of 45 studies showed that the mean hs-cTnI and hs-cTnT concentrations were markedly evaluated after strenuous exercise (such as half marathon, marathon, ultramarathon, and triathlon), with changes of 40 and 26 ng/L from baseline, respectively [39]. The mechanism regarding the elevation of hs-cTn is unclear, but it might be explained by endurance exercise that will enhance the permeability of the cardiomyocyte membrane, following the release of troponin from the cytosolic pool [40]. Another hypothesis of the mechanism could be the function of integrins (bidirectional signaling molecules). Stimulated by myocardial stretch, integrins mediates the release of cTn out of cardiomyocytes [41].
The analytical precision of cTn was improved over time, resulting in a wide spectrum of detection quality [42]. However, assays used to measure hs-cTnT were not uniform in different studies, which made some variances. As with the subgroup analysis we reported, these variable assays with different 99th percentile URLs ultimately led to heterogeneity in the literature. At present, however, no unified international consensus on the number and definition of reference groups has been agreed upon. For instance, unlike other laboratories that used an overall 14 ng/L 99th percentile URL in terms of Roche hs-cTnT assay, the USA establish its unique calculations [25]. Furthermore, clinical use of the present cutoff for the hs-cTnT assay does not take into account patient race, gender, and age. However, the 99th percentile URL values for both hs-cTnT and hs-cTnI assays vary by race, gender, or age, some studies have speculated that the 99th percentile URL is relatively low for white [43], female [44], and young people [45]. Therefore, there is an urgent need to set standards for hs-cTn assay and reference limit, which have also been suggested by other studies [46, 47].
As time went on, the biomarker of myocardial injury (hs-cTnT) released after the marathon running gradually returned to the pre-race level at 72 to 96 hours with the end of high-intensity exercise, as shown in the forest plot. However, many previous studies demonstrated marathon runners return their cTn level to the normal range at 24–72 h after running [48, 49, 50]. One possible reason is the higher sensitivity of hs-cTn. Apart from that, the normal range of hs-cTnT is between the lower limit of detection and the 99th percentile of the recommended URL [51], so it may take even less time to return to the normal range of hs-cTnT. Clinically, the concentration of cTn in patients with MI would continue to rise for 4–10 days [52], indirectly proving that the myocardial injury induced by clinical disease and that caused by marathon running are two completely different injuries. To sum up, the profile of revisable hs-cTnT changes tends to be a physiological phenomenon than a pathological phenomenon, which reflects the remodeling process of the cardiomyocyte membrane and can be regarded as a temporary physiological stress response [53].
In general, the release of hs-cTnT after marathon running is a phenomenon that rose rapidly at first and then dissipated quickly. Although changes in biomarkers of myocardial injury after a marathon are a physiological process, they can also be detrimental in patients with pre-existing cardiovascular disease [54]. Therefore, it is vital to screen before exercise to prevent sudden death in runners, as suggested by both the American Heart Association [55] and the European Society of Cardiology [56]. After completing a marathon running, it is important and necessary to have enough rest time. If hs-cTn increases again due to strenuous exercise before returning to baseline, some researchers proposed that this process, which involves repetitive elevation of cardiac biomarkers, may cause some people to turn physiological phenomena into pathological changes [57, 58]. Similarly, a brief decline in left ventricular function, known as exercise-induced cardiac fatigue, was observed after marathon running [59]. These changes were also thought to be physiological phenomena, the hearts’ self-protection mechanism, which gradually dissipated after a few days of recovery [60]. Some marathoners, however, have structural changes in the atria and ventricles [61]. Therefore, the transformation of physiological phenomena into pathological changes in the heart was feasible and has occurred in some patients.
There are still some limitations in this study that need to be discussed here. First, the trend data of hs-cTnI after marathon running was lacking, future studies can focus on the change of hs-cTnI over time to see if it is consistent with the change of hs-cTnT. Second, many confounding factors, such as race, running environment, and detection reagent, can influence the results and cause heterogeneity among studies. Therefore, in order to ensure the reliability of the test results, it is very important to establish a unified standard as far as possible, especially the test assay and reference limit of cTn detection.
5.Conclusion
Both hs-cTnI and hs-cTnT were elevated after running a marathon, but the change of hs-cTnT is more of a physiological phenomenon. The mechanism underlying the time-dependent trend of hs-cTn in marathoners is not well understood, which needs further study to demonstrate it.
Ethical approval
Not applicable.
Funding
The authors report no funding.
Informed consent
Not applicable.
Author contributions
Conceptualization: XD, XZ; Data collection and analysis: YZ, ZZ, JF; Writing-original draft: XD; Writing-review and editing: XZ. All authors read and approved the final manuscript.
Acknowledgments
The authors have no acknowledgments.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | Ooms L, Veenhof C, de Bakker DH. Effectiveness of Start to Run, a 6-week training program for novice runners, on increasing health-enhancing physical activity: A controlled study. BMC Public Health. (2013) ; 13: : 697. |
[2] | Pedisic Z, Shrestha N, Kovalchik S, Stamatakis E, Liangruenrom N, Grgic J, et al. Is running associated with a lower risk of all-cause, cardiovascular and cancer mortality, and is the more the better? A systematic review and meta-analysis. British Journal of Sports Medicine. (2020) ; 54: (15): 898-905. |
[3] | Lee D-C, Pate RR, Lavie CJ, Sui X, Church TS, Blair SN. Leisure-time running reduces all-cause and cardiovascular mortality risk. J Am Coll Cardiol. (2014) ; 64: (5): 472-81. |
[4] | Jens Jakob Andersen. (2021) . Marathon Statistics 2019 Worldwide (Research). Available online at: https://runrepeat.com/research-marathon-performance-across-nations. |
[5] | Merghani A, Maestrini V, Rosmini S, Cox AT, Dhutia H, Bastiaenan R, et al. Prevalence of subclinical coronary artery disease in masters endurance athletes with a low atherosclerotic risk profile. Circulation. (2017) ; 136: (2): 126-37. |
[6] | Herm J, Tüpper A, Wutzler A, Kunze C, Krüll M, Brechtel L, et al. Frequency of exercise-induced ST-T-segment deviations and cardiac arrhythmias in recreational endurance athletes during a marathon race: Results of the prospective observational Berlin Beat of Running study. BMJ Open. (2017) ; 7: (8): e015798. |
[7] | Wegberger C, Tscharre M, Haller PM, Piackova E, Vujasin I, Gomiscek A, et al. Impact of ultra-marathon and marathon on biomarkers of myocyte necrosis and cardiac congestion: A prospective observational study. Clin Res Cardiol. (2020) ; 109: (11): 1366-73. |
[8] | Lim WY, Thevarajah TM, Goh BT, Khor SM. Paper microfluidic device for early diagnosis and prognosis of acute myocardial infarction via quantitative multiplex cardiac biomarker detection. Biosens Bioelectron. (2019) ; 128: : 176-85. |
[9] | Zhang S, Breitner S, Cascio WE, Devlin RB, Neas LM, Ward-Caviness C, et al. Association between short-term exposure to ambient fine particulate matter and myocardial injury in the CATHGEN cohort. Environ Pollut. (2021) ; 275: : 116663. |
[10] | Katrukha IA. Human cardiac troponin complex. Structure and functions. Biochemistry (Mosc). (2013) ; 78: (13): 1447-65. |
[11] | Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al. Fourth Universal Definition of Myocardial Infarction (2018). Circulation. (2018) ; 138: (20): e618-e51. |
[12] | Hartikainen TS, Sörensen NA, Haller PM, GoSSling A, Lehmacher J, Zeller T, et al. Clinical application of the 4th Universal Definition of Myocardial Infarction. Eur Heart J. (2020) ; 41: (23): 2209-16. |
[13] | Clerico A, Giannoni A, Prontera C, Giovannini S. High-sensitivity troponin: a new tool for pathophysiological investigation and clinical practice. Adv Clin Chem. (2009) ; 49. |
[14] | Chapman AR, Adamson PD, Shah ASV, Anand A, Strachan FE, Ferry AV, et al. High-sensitivity cardiac troponin and the universal definition of myocardial infarction. Circulation. (2020) ; 141: (3): 161-71. |
[15] | Thygesen K, Mair J, Giannitsis E, Mueller C, Lindahl B, Blankenberg S, et al. How to use high-sensitivity cardiac troponins in acute cardiac care. Eur Heart J. (2012) ; 33: (18): 2252-7. |
[16] | Roffi M, Patrono C, Collet J-P, Mueller C, Valgimigli M, Andreotti F, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. (2016) ; 37: (3): 267-315. |
[17] | Gresslien T, Agewall S. Troponin and exercise. Int J Cardiol. (2016) ; 221: : 609-21. |
[18] | Regwan S, Hulten EA, Martinho S, Slim J, Villines TC, Mitchell J, et al. Marathon running as a cause of troponin elevation: A systematic review and meta-analysis. J Interv Cardiol. (2010) ; 23: (5): 443-50. |
[19] | Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Journal of Clinical Epidemiology. (2021) ; 134: : 178-89. |
[20] | National Heart, Lung, and Blood Institute. (2014) . Study quality assessment tools: quality assessment tool for before-after (pre-post) studies with no control group. Available online at: https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools. |
[21] | McGrath S, Zhao X, Steele R, Thombs BD, Benedetti A. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat Methods Med Res. (2020) : 962280219889080. |
[22] | Borenstein M, Hedges LV, Higgins JPT, Rothstein HR. A basic introduction to fixed-effect and random-effects models for meta-analysis. Res Synth Methods. (2010) ; 1: (2). |
[23] | Higgins JPT, Green S. (2011) . Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0. Available online at: https://handbook5-1.cochrane.org. |
[24] | Zhang W, Liu C-Y, Ji L-N, Wang J-G. Age-stratified association of blood pressure with albuminuria and left ventricular hypertrophy in patients with hypertension and diabetes mellitus. Blood Press. (2021) ; 30: (3): 180-7. |
[25] | Apple FS, Wu AHB, Sandoval Y, Sexter A, Love SA, Myers G, et al. Sex-Specific 99th Percentile Upper Reference Limits for High Sensitivity Cardiac Troponin Assays Derived Using a Universal Sample Bank. Clin Chem. (2020) ; 66: (3): 434-44. |
[26] | Baker P, Davies SL, Larkin J, Moult D, Benton S, Roberts A, et al. Changes to the cardiac biomarkers of non-elite athletes completing the 2009 London Marathon. Emerg Med J. (2014) ; 31: (5): 374-9. |
[27] | Bernat-Adell MD, Collado-Boira EJ, Moles-Julio P, Panizo-González N, Martínez-Navarro I, Hernando-Fuster B, et al. Recovery of inflammation, cardiac, and muscle damage biomarkers after running a marathon. Journal of strength and Conditioning Research. (2021) ; 35: (3): 626-32. |
[28] | Eijsvogels TMH, Hoogerwerf MD, Maessen MFH, Seeger JPH, George KP, Hopman MTE, et al. Predictors of cardiac troponin release after a marathon. J Sci Med Sport. (2015) ; 18: (1): 88-92. |
[29] | Grabs V, Peres T, Zelger O, Haller B, Pressler A, Braun S, et al. Decreased prevalence of cardiac arrhythmias during and after vigorous and prolonged exercise in healthy male marathon runners. Am Heart J. (2015) ; 170: (1): 149-55. |
[30] | Kaleta-Duss AM, Lewicka-Potocka Z, Da̧browska-Kugacka A, Raczak G, Lewicka E. Myocardial injury and overload among amateur marathoners as indicated by changes in concentrations of cardiovascular biomarkers. Int J Environ Res Public Health. (2020) ; 17: (17). |
[31] | Kosowski M, Mç¡‘narska K, Chmura J, Kustrzycka-Kratochwil D, Sukiennik-Kujawa M, Todd JA, et al. Cardiovascular stress biomarker assessment of middle-aged non-athlete marathon runners. Eur J Prev Cardiol. (2019) ; 26: (3): 318-27. |
[32] | Martínez-Navarro I, Sánchez-Gómez J, Sanmiguel D, Collado E, Hernando B, Panizo N, et al. Immediate and 24-h post-marathon cardiac troponin T is associated with relative exercise intensity. European Journal of Applied Physiology. (2020) ; 120: (8): 1723-31. |
[33] | Möhlenkamp S, Leineweber K, Lehmann N, Braun S, Roggenbuck U, Perrey M, et al. Coronary atherosclerosis burden, but not transient troponin elevation, predicts long-term outcome in recreational marathon runners. Basic Res Cardiol. (2014) ; 109: (1): 391. |
[34] | Paana T, Jaakkola S, Bamberg K, Saraste A, Tuunainen E, Wittfooth S, et al. Cardiac troponin elevations in marathon runners. Role of coronary atherosclerosis and skeletal muscle injury. The MaraCat Study. Int J Cardiol. (2019) ; 295: : 25-8. |
[35] | Richardson AJ, Leckie T, Watkins ER, Fitzpatrick D, Galloway R, Grimaldi R, et al. Post marathon cardiac troponin T is associated with relative exercise intensity. J Sci Med Sport. (2018) ; 21: (9): 880-4. |
[36] | Roca E, Nescolarde L, Lupón J, Barallat J, Januzzi JL, Liu P, et al. The dynamics of cardiovascular biomarkers in non-elite marathon runners. J Cardiovasc Transl Res. (2017) ; 10: (2): 206-8. |
[37] | Scherr J, Braun S, Schuster T, Hartmann C, Moehlenkamp S, Wolfarth B, et al. 72-h kinetics of high-sensitive troponin T and inflammatory markers after marathon. Medicine and Science in Sports and Exercise. (2011) ; 43: (10): 1819-27. |
[38] | Schwarz V, Düsing P, Liman T, Werner C, Herm J, Bachelier K, et al. Marathon running increases circulating endothelial- and thrombocyte-derived microparticles. Eur J Prev Cardiol. (2018) ; 25: (3): 317-24. |
[39] | Sedaghat-Hamedani F, Kayvanpour E, Frankenstein L, Mereles D, Amr A, Buss S, et al. Biomarker changes after strenuous exercise can mimic pulmonary embolism and cardiac injury – a metaanalysis of 45 studies. Clin Chem. (2015) ; 61: (10): 1246-55. |
[40] | Scharhag J, George K, Shave R, Urhausen A, Kindermann W. Exercise-associated increases in cardiac biomarkers. Medicine and Science in Sports and Exercise. (2008) ; 40: (8): 1408-15. |
[41] | Shave R, Baggish A, George K, Wood M, Scharhag J, Whyte G, et al. Exercise-induced cardiac troponin elevation: Evidence, mechanisms, and implications. J Am Coll Cardiol. (2010) ; 56: (3): 169-76. |
[42] | Newby LK, Jesse RL, Babb JD, Christenson RH, De Fer TM, Diamond GA, et al. ACCF 2012 expert consensus document on practical clinical considerations in the interpretation of troponin elevations: A report of the American College of Cardiology Foundation task force on Clinical Expert Consensus Documents. J Am Coll Cardiol. (2012) ; 60: (23): 2427-63. |
[43] | Gore MO, Seliger SL, Defilippi CR, Nambi V, Christenson RH, Hashim IA, et al. Age- and sex-dependent upper reference limits for the high-sensitivity cardiac troponin T assay. J Am Coll Cardiol. (2014) ; 63: (14): 1441-8. |
[44] | Chapman AR, Lee KK, McAllister DA, Cullen L, Greenslade JH, Parsonage W, et al. Association of High-Sensitivity Cardiac Troponin I Concentration With Cardiac Outcomes in Patients With Suspected Acute Coronary Syndrome. JAMA. (2017) ; 318: (19): 1913-24. |
[45] | Shah ASV, Anand A, Strachan FE, Ferry AV, Lee KK, Chapman AR, et al. High-sensitivity troponin in the evaluation ofpatients with suspected acute coronary syndrome: A stepped-wedge, cluster-randomised controlled trial. Lancet. (2018) ; 392: (10151): 919-28. |
[46] | Apple FS, Fantz CR, Collinson PO. Implementation of high-sensitivity and point-of-care cardiac troponin assays into practice: Some different thoughts. Clin Chem. (2021) ; 67: (1): 70-8. |
[47] | Gore MO, de Lemos JA. Clinical relevance of the 99th percentile upper reference limit for high-sensitivity cardiac troponin assays. Clin Chem. (2020) ; 66: (3): 403-5. |
[48] | Frassl W, Kowoll R, Katz N, Speth M, Stangl A, Brechtel L, et al. Cardiac markers (BNP, NT-pro-BNP, Troponin I, Troponin T, in female amateur runners before and up until three days after a marathon. Clin Lab. (2008) ; 54: (3-4): 81-7. |
[49] | Traiperm N, Gatterer H, Wille M, Burtscher M. Cardiac troponins in young marathon runners. Am J Cardiol. (2012) ; 110: (4): 594-8. |
[50] | Mooren FC, Viereck J, Krüger K, Thum T. Circulating microRNAs as potential biomarkers of aerobic exercise capacity. Am J Physiol Heart Circ Physiol. (2014) ; 306: (4): H557-H63. |
[51] | Farmakis D, Mueller C, Apple FS. High-sensitivity cardiac troponin assays for cardiovascular risk stratification in the general population. Eur Heart J. (2020) ; 41: (41): 4050-6. |
[52] | Eijsvogels TMH, Fernandez AB, Thompson PD. Are there deleterious cardiac effects of acute and chronic endurance exercise? Physiol Rev. (2016) ; 96: (1). |
[53] | Koller A, Schobersberger W. Post-exercise release of cardiac troponins. J Am Coll Cardiol. (2009) ; 53: (15): 1341; author reply -; author reply 2. |
[54] | Trivax JE, McCullough PA. Phidippides cardiomyopathy: A review and case illustration. Clin Cardiol. (2012) ; 35: (2): 69-73. |
[55] | Maron BJ, Thompson PD, Ackerman MJ, Balady G, Berger S, Cohen D, et al. Recommendations and considerations related to preparticipation screening for cardiovascular abnormalities in competitive athletes: 2007 update: A scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism: endorsed by the American College of Cardiology Foundation. Circulation. (2007) ; 115: (12): 1643-455. |
[56] | Corrado D, Basso C, Schiavon M, Pelliccia A, Thiene G. Pre-participation screening of young competitive athletes for prevention of sudden cardiac death. J Am Coll Cardiol. (2008) ; 52: (24): 1981-9. |
[57] | Möhlenkamp S, Lehmann N, Breuckmann F, Bröcker-Preuss M, Nassenstein K, Halle M, et al. Running: The risk of coronary events: Prevalence and prognostic relevance of coronary atherosclerosis in marathon runners. Eur Heart J. (2008) ; 29: (15): 1903-10. |
[58] | O’Keefe JH, Patil HR, Lavie CJ, Magalski A, Vogel RA, McCullough PA. Potential adverse cardiovascular effects from excessive endurance exercise. Mayo Clin Proc. (2012) ; 87: (6): 587-95. |
[59] | Elliott AD, La Gerche A. The right ventricle following prolonged endurance exercise: Are we overlooking the more important side of the heart? A meta-analysis. British Journal of Sports Medicine. (2015) ; 49: (11): 724-9. |
[60] | Predel H-G. Marathon run: Cardiovascular adaptation and cardiovascular risk. Eur Heart J. (2014) ; 35: (44): 3091-8. |
[61] | Pedlar CR, Brown MG, Shave RE, Otto JM, Drane A, Michaud-Finch J, et al. Cardiovascular response to prescribed detraining among recreational athletes. J Appl Physiol. (2018) ; 124: (4): 813-20. |


