
Isokinetic trunk training on pain, disability, and strength in non-specific low back pain patients: A systematic review and meta-analysis
Abstract
BACKGROUND:
Low back pain is one of the leading causes of disability globally, with a high economic and social burden. A decrease or imbalance in trunk strength has been associated with the occurrence of low back pain and its severity. Trunk strength training is helpful in the treatment of Non-specific low back pain (NSLBP) patients. However, we do not know the effects of trunk isokinetic training (IKT) on pain intensity, disability, and trunk strength.
OBJECTIVE:
This systematic review aimed to determine the effects of trunk IKT in NSLBP patients on pain intensity, disability, and trunk flexor and extensor isokinetic strength.
METHODS:
We searched PubMed, Web of Science, Scopus, CENTRAL, and PEDro, from January 2001 until March 2021 and updated to November 2022. Randomized controlled trials (RCTs) that investigated the effect of IKT in adult participants with NSLBP on pain intensity, disability, or isokinetic trunk strength were included. Mean difference (MD) and 95% confidence intervals (95% CI) were calculated for pain. Bias was assessed using the Cochrane risk of bias (RoB) tool and evidence certainty via Grading of Recommendations Assessment, Development and Evaluation (GRADE).
RESULTS:
Among 1750 retrieved articles, eight were included in this review. Meta-analysis comparing IKT (trunk isokinetic training,
CONCLUSIONS:
Trunk IKT could be a novel clinical tool for pain management in patients with NSLBP, although evidence is scarce. In addition, few RCTs exist for IKT on disability or trunk isokinetic strength in patients with NSLBP. Therefore, further research on this topic is needed.
1.Introduction
Low back pain (LBP) is one of the most common musculoskeletal condition [1, 2] and is an alarming health problem that has increased worldwide [3]. Globally, LBP is the leading global cause of years lived with disability [4]. The prevalence of LBP in 1990 was 377.5 million; however, this increased to 577 million in 2017 [4]. LBP includes pain, muscle tension, or stiffness located below the costal margin and above the lower gluteal folds, with or without sciatica [5]. It can be characterized in terms of temporality as acute LBP, less than six weeks, subacute LBP between 6 and 12 weeks, and chronic LBP, when the pain extends beyond 12 weeks [6]. Recurrence of LBP is expected; with more than two-thirds of individuals (69%) having a recurrence within 12 months after recovery. Of these, 40% will suffer functional disability or require medical care [7].
Regarding LBP, 90% of cases do not have a specific cause, so it is called non-specific LBP (NSLBP) [8]. Despite this, multiple factors have been associated with the occurrence of NSLBP [9, 10], including deconditioning the lumbar musculature [11, 12], reduced trunk muscle mass [13], imbalance, and decreased trunk strength [14, 15]. Thus, trunk strengthening has been proposed for manage LBP patients [16, 17, 18]. Furthermore, different trunk training methods have been investigated, such as motor control exercises [19], core stabilization [20, 21], and strengthening exercises using an isokinetic dynamometer [22].
The isokinetic dynamometer is the gold standard in strength assessment [23]. It has been previously used to assess trunk strength in healthy subjects and NSLBP patients [24, 25, 26]. Given its capacity to develop maximum strength, the precision with training can be programmed, and its high reproducibility, it could be considered a valuable tool for strength training [27]. In addition, it provides real-time visual and auditory feedback, which could benefit treatment adherence and allow objective monitoring of training results. The most distinctive characteristic of this device is the accommodation of the resistance provided by the dynamometer, which allows for maximal muscle loading throughout the entire range of motion [28].
Isokinetic training (IKT) helps train the shoulder musculature [29] and re-establishing rotator cuff strength ratios [30]. Furthermore, in lower limbs decrease reaction times [31] and increase strength and symmetry [32], explosive strength [33], muscle mass and strength post knee surgery [34, 35]. Isokinetic trunk training has been used in different populations. For example, IKT of the trunk rotator muscles may help improve the performance of world-class canoe sprinters [36]. In addition, isokinetic trunk muscle strength training effectively improves muscle function and proprioception in patients with chronic lumbar disc herniation [37]. However, in patients with a history of low back pain, isokinetic trunk extensor training has not been shown to decrease LBP recurrences [38]. To our knowledge, there is no consensus regarding whether isokinetic trunk training has benefits in NSLBP patients. Therefore, this review aimed to determine the effects of isokinetic trunk training on pain intensity, disability, and isokinetic trunk strength in NSLBP patients.
2.Methods
2.1Protocol and registration
The PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analyses guidelines) guidelines were used [39] (Supplementary Table S1). In addition, the protocol of this review was registered in PROSPERO (International Prospective Register of Systematic Reviews) (CRD42021247030).
2.2Search strategy
On March 30, two authors (WR-F and DJ-M) performed the search. The databases used were PubMed, Web of Science, Scopus, CENTRAL, and PEDro. The initial search was performed from January 2011 to March 30th, 2021. The following keywords were included: “CORE strengthening”, “trunk strengthening”, “isokinetic exercise”, “muscle strength”, “dynamometer”, “isokinetic training”, “CORE”, “abdominal muscles”, “abdominal wall”, “torso”, “trunk”, “low back pain”, “low back ache”, “back pain” and “lumbago”. Due to the low number of articles retrieved and to identify the largest number of potential articles for this review, a second search was performed following the same search strategy between January 2001 and December 2010. Search strategies are presented in Supplementary Table S2. Bibliographies of previous related reviews and selected studies were manually screened for new relevant studies. An update of the search was conducted until November 17, 2022.
2.3Eligibility criteria
Articles that met the following criteria were included in this review: (1) Population: adult participants (age
2.4Study selection
Articles retrieved from the initial search were entered into the Rayyan QCRI application, an App that assists in the article selection process, optimizing evaluation time, and allowing collaborative work (available for free at http://rayyan.qcri.org (accessed March 30, 2021)) [40]. Duplicate references were removed. Next, two independent investigators (WR-F and DJ-M) reviewed titles and abstracts to identify articles relevant to the systematic review. Full-text reading of these articles was then performed to assess eligibility criteria, and finally, the reference list was checked for relevant articles that could be included. Disagreements were resolved by consensus. When the agreement was not achieved, a third investigator was consulted (LC-R).
2.5Risk of bias of individual studies
The risk of bias (RoB) for each individual study was assessed with The Cochrane Collaboration Risk of Bias Tool using Review Manager 5.4 [41]. This tool evaluates the RoB according to the following six domains: random sequence generation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and “other sources of bias.” Critical assessments on the RoB are made separately for each domain, and it could be considered as “low,” “high” or “unclear” RoB (if reporting was not sufficient to assess the domain) [42]. RoB assessment were independently performed by two reviewers (WR-F and DM-G). In case of discrepancy, a third evaluator (LC-R) was consulted.
2.6Rating the quality of evidence
The quality of the evidence was rated using the Grading of Recommendation, Assessment, Development, and Evaluation (GRADE) approach [43]. GRADE offer four levels of evidence: High, moderate, low, and very low. The GRADE pro system (https://www.gradepro. org) was used for each outcome from meta-analysis to create a summary of findings (SoF) table.
2.7Data collection process
Data extraction was performed by three independent researchers (WR-F, A-RP, and DM-G); the information extracted was related to article identification (authors, country, and year of publication), participant characteristics (sample, gender, and age), and isokinetic and other training protocols (sessions/week). In addition to variables under study, and main results. All calculations were conducted using a Microsoft Excel (Microsoft, Redmond, WA, USA) spreadsheet containing data extracted from each publication.
2.8Synthesis methods
Review Manager (RevMan) version 5.4 was used for all the statistical analyses. The comparison was made between the IKT trunk group and the control group (conventional exercises). A
The effect of the IKT interventions on pain intensity was calculated using the mean difference (MD). Means and standard deviations (SD) of the post-intervention values of both IKT and control groups were obtained from the included studies and added to RevMan 5.4. Random-effects inverse variance (IV) was used with the measurement of the effect of MD. A random-effects model was incorporated when the assumption is that the data demonstrated effects across studies that are randomly situated around a central value [45]. Forest plots were generated to illustrate the specific differences between the group’s effects on pain intensity and MD within the respective 95% CIs.
3.Results
3.1Study selection
Figure 1.
Flow chart for the systematic review.
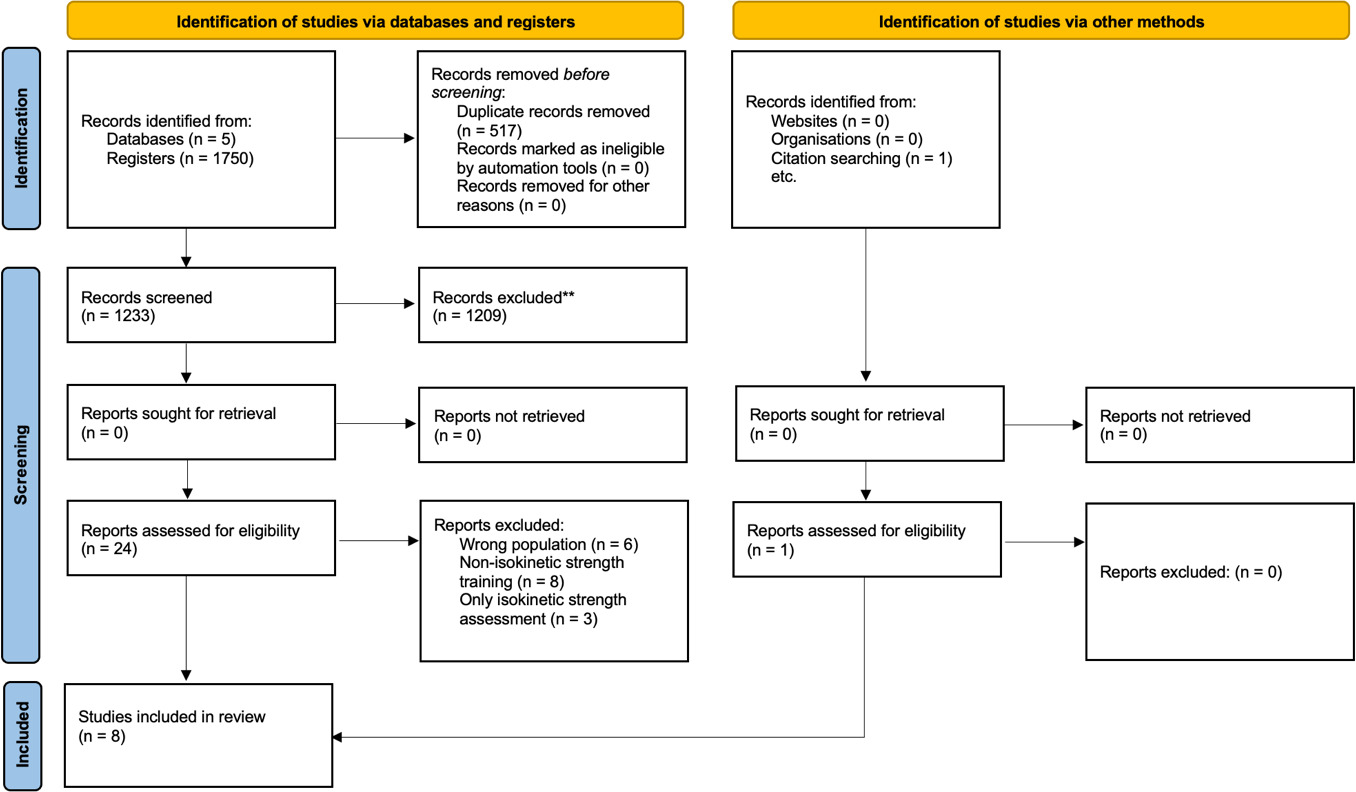
We found no systematic reviews with an objective similar to that of the present study. From the initial search, 1750 articles were retrieved (Fig. 1), of which 517 were eliminated as duplicates. After evaluating titles and abstracts, 1209 articles were excluded as not relevant to this review, leaving 24 articles for full-text reading. One additional article was identified from other sources.
From the 25 articles, six articles were excluded because they did not include patients with NSLBP, eight because they performed strength training but not isokinetic strength training, and three because they only performed isokinetic strength assessment and not isokinetic strength training. Thus, eight articles were selected, seven included in the meta-analysis. The reference list was reviewed without finding new articles. An update of the search was conducted until 17 November 2022; however, no articles met the inclusion criteria.
3.2Study characteristics
The retrieved studies included 361 participants with NSLBP, of whom only 19.66% (71) were women. Of the total sample, 143 received IKT. The number of participants per study ranged from 17 [22] to 60 [46, 47, 48, 49]. The minimum age of participants was 20.23
Table 1
Characteristics of the included studies
| Author | Year/country | Study design | Sample size | Gender | Age (years | LBP classification | Outcomes | Instrument |
|---|---|---|---|---|---|---|---|---|
| Nambi et al.(A) [47] | 2020/Saudi Arabia | RCT | 60 LBP. CG: 20. IKT: 20. CST: 20. | 60 Males | CG: 21.38 | Chronic ( | Pain intensity Player wellness Sprint & Jump performances | VAS Questionnaire Sprint & jump test |
| Nambi et al.(B) [50] | 2020/Saudi Arabia | RCT | 45 LBP. CG: 15. IKT: 15. VRT: 15. | 45 Males | CG: 20.78 | Chronic ( | Pain intensity Player wellness, Sprint & Jump performances | VAS Questionnaire Sprint & jump test |
| Nambi et al.(C) [48] | 2020/Saudi Arabia | RCT | 60 LBP. CG: 20. IKT: 20. CST: 20. | 60 Males | CG: 21.9 | Chronic ( | Pain intensity Paraspinal CSA Multifidus thickness Inflammatory biomarker | VAS MRI Ultrasound Blood analysis |
| Olivier et al.[49] | 2008/France | RCT | 60 LBP. CG: 30. IKT: 30. | 33 Males 27 Females | 39 | Chronic ( | Pain intensity Isokinetic strength Quality of life Flexibility Trunk endurance | VAS Cybex norm Dallas score Finger to floor McGill battery |
| Calmels et al. [22] | 2004/France | RCT | 17 LBP. IKT: 9. CG: 8. | 16 Males 1 Female | 43 | Chronic. | Pain intensity Disability Trunk mobility Muscle extensibility and strength | VAS Quebec scale Schöber index Biering Sorensen and Shirado ito test |
| Sertpoyraz et al. [52] | 2009/Turkey | RCT | 40 LBP. IKT: 20. CG: 20. | 9 Males 31 Females | IKT: 38.75 | Chronic ( | Pain intensity Disability Isokinetic strength Spinal mobility Depressive symptoms | VAS MOLBDQ Cybex norm Finger to floor Questionnaire |
| Nambi et al.[46] | 2021/Saudi Arabia | RCT | 60 LBP. CG: 20. IKT: 20. VRT: 20. | 60 Males | CG: 23.3 | Chronic ( | Pain intensity Kinesiophobia Hormonal values | VAS TSK-17 Blood serum analysis |
| de Freitas et al. [51] | 2008/Brazil | RCT | 19 LBP. CG: 10 IKT: 9. | 7 Males 12 Females | CG: 31.2 | Chronic ( | Pain intensity Disability Isokinetic strength Flexibility and lumbar mobility | VAS RMQ Cybex 6000 Schöber and Finger to floor |
LBP: Low back pain; CG: control group; IKT: isokinetic training; CST: core stability training; VRT: virtual reality training; RCT: randomized controlled trial; SD: standard deviation; VAS: visual analogue scale; CSA: cross-sectional area; MRI: Magnetic resonance imaging; MOLBDQ: Modified Oswestry Low Back Disability Questionnaire; TSK-17: Tampa Scale; RMQ: Roland Morris questionnaire.
Table 2
The characteristics of isokinetic strengthening training of the included studies
| Author/year | Group/intervention | Isokinetic training protocols | Dosage/velocities | Frequency (x per week) | Intervention length (week) | Dynamometer |
|---|---|---|---|---|---|---|
| Nambi et al. 2020(A) [47] | IKT: Isokinetic strengthening CST: Core stability exercise CG: Conventional rehabilitation. | Warm-up: five min. Flexor/extensor stretching. Position: standing ROM: 90 | Training: 15 reps | 5 | 4 | Biodex Corporation, NY, USA. |
| Nambi et al. 2020(B) [50] | IKT: Isokinetic strengthening VRT: Virtual reality training exercise CG: Conventional rehabilitation. | Warm-up: five min. Flexor/extensor stretching. Position: standing ROM: 90 | Training: 15 reps | 5 | 4 | Biodex Corporation, NY, USA. |
| Nambi et al. 2020(C) [48] | IKT: Isokinetic strengthening CST: Core stability exercise CG: Conventional rehabilitation. | Warm-up: five min. Flexor/extensor stretching. Position: standing ROM: 90 | Training: 15 reps | 5 | 4 | Biodex Corporation, NY, USA. |
| Olivier et al.2008 [49] | IKT: Isokinetic strengthening + Conventional rehabilitation CG: Conventional rehabilitation. | Day hospitalization Three phases | Week 1: 8 reps | 5 | 4 | Not reported. |
| Calmels et al.2004 [22] | IKT: Isokinetic strengthening CG: Conventional rehabilitation. | Warm-up: ten min. Position: standing ROM: 70 | Session 1 and 2: 7 reps | 3 | 2 | Cybex 6000 |
| Sertpoyraz et al. 2009 [52] | IKT: Isokinetic strengthening CG: Conventional rehabilitation. | Warm-up: ten min. Position: standing ROM: 90 | Training: 5 reps | 5 | 3 | Cybex Norm Computerized Isokinetic, Cybex Company, New York. |
| Nambi et al.2021 [46] | IKT: Isokinetic strengthening VRT: Virtual reality training exercise CG: Conventional rehabilitation. | Warm-up: five min. Flexor/extensor stretching. Position: standing ROM: 90 | Training: 15 reps | 5 | 4 | Not reported. |
| de Freitaset al. [51] | IKT: Isokinetic strengthening CG: Conventional rehabilitation. | Stretching. ROM: 100 | Month 1: 8 reps | 2 | 12 | Cybex 6000 |
IKT: isokinetic training; CST: core stability training; CG: control group; VRT: virtual reality training; ROM: range of movement; reps: repetitions.
Table 3
Summary of findings (SoF) and quality of evidence (GRADE) for Isokinetic trunk training in NSLBP patients
| Certainty assessment | No. of patients | Effect absolute | Certainty | Importance | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| No. of | Study | RoB | Inconsistency | Indirectness | Imprecision | Other | IKT | CG | (95% CI) | ||
| studies | design | considerations | |||||||||
| Pain intensity immediately post intervention | |||||||||||
| 7 | RCT | Serious | Very serious | Not serious | Serious | None | 123 | 123 | MD | Important | |
| Pain intensity 1 month follow up | |||||||||||
| 3 | RCT | Serious | Very serious | Not serious | Serious | None | 54 | 53 | MD | Important | |
| Pain intensity 3 months follow up | |||||||||||
| 2 | RCT | Serious | Very serious | Not serious | Serious | None | 39 | 38 | MD | Important | |
| Pain Intensity 6 months follow up | |||||||||||
| 2 | RCT | Serious | Very serious | Not serious | Not serious | None | 35 | 34 | MD | Important | |
RoB: Risk of bias; IKT: Isokinetic training; CG: control group; CI: confidence interval; RCT: Randomized controlled trial; MD: mean difference. Explanations: a. Differences in the population assessed; b. The heterogeneity between studies was considerable (I
GRADE: Working Group grades of evidence.
High certainty: We are very confident that the true effect lies close to that of the estimate of the effect.
Moderate certainty: We are moderately confident in the effect estimate: The true effect is likely to be close to the estimate of the effect, but there is a possibility that it is substantially different.
Low certainty: Our confidence in the effect estimate is limited: The true effect may be substantially different from the estimate of the effect.
Very low certainty: We have very little confidence in the effect estimate: The true effect is likely to be substantially different from the estimate of effect.
Regarding training protocols, all studies considered a trunk IKT group compared to a control group (CG). The CG performed conventional exercises such as stretching and isotonic and isometric exercises of the trunk muscles. In addition, Nambi et al. [47, 48] included a core stability training group and Nambi et al. [46, 50] a virtual reality training group. For the analysis, core stability and virtual reality training groups were not included. The total intervention period ranged from two [22] to twelve weeks [51], with total training sessions between six [22] and twenty-four [51]. Concerning the dynamometers, Nambi et al. [47, 48, 50] used Biodex Corporation, NY, USA, Calmels et al. [22] and de Freitas et al. [51] a Cybex 6000
3.3Risk of bias within studies
Figure 2.
Risk of bias summary: review authors’ judgements about each risk of bias item for each included study.
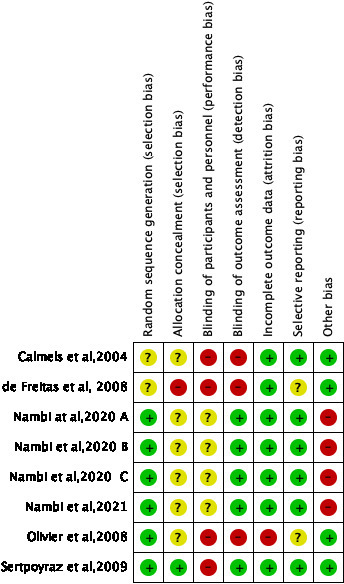
Figures 2 and 3 show the RoB assessment for all articles. For the overall RoB, only one article [52] rated 85.7% of their articles items as low RoB; four [46, 47, 48, 50] ordered 57.1% of their items as low RoB, and three [22, 49, 51] obtained less than 50% of the items classified as low RoB. Of the eight articles, 87.5% were classified as low RoB in the attrition bias [22, 46, 47, 48, 50, 51, 52], 75% were classified as low RoB in the randomization process [46, 47, 48, 49, 50, 52], and reporting bias [22, 46, 47, 48, 50, 52]. Only one article in allocation concealment [52], none in the blinding of participants and personnel, and 62.5% in the blinding of outcome assessment [46, 47, 48, 50, 52]. Four articles [46, 47, 48, 50] were classified as high RoB in “other bias” due to the specific population in which they performed the intervention.
3.4Effect of isokinetic strengthening training
3.4.1Pain intensity
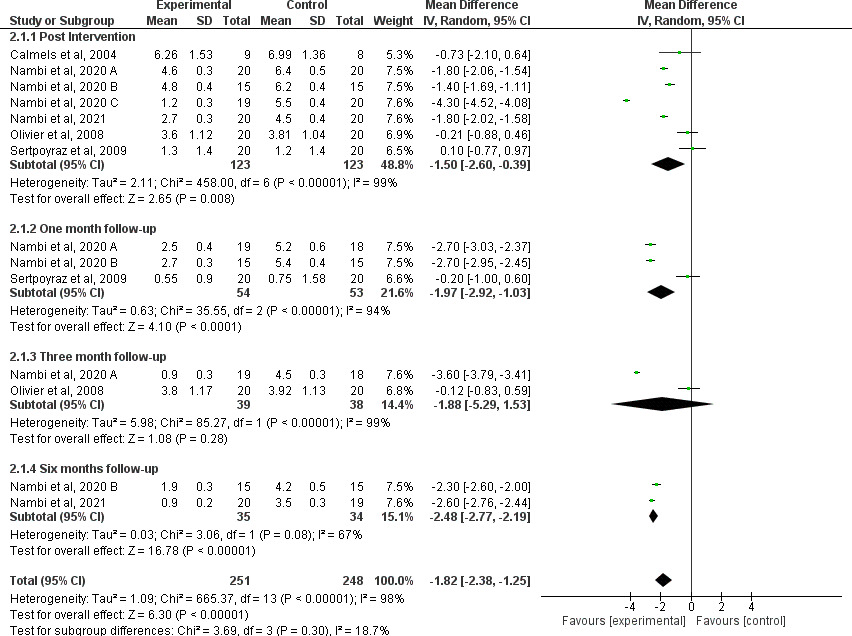
All the retrieved studies in this review evaluated pain intensity using the visual analog scale (VAS). For this reason, we performed a meta-analysis of pain intensity. One article could not be incorporated into the meta-analysis because it reported a significant decrease in pain in both groups (IKT and CG) but only indicated
At one month follow-up, the meta-analysis revealed a significant decrease in pain intensity, in favor of the IKT group of
Figure 3.
Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
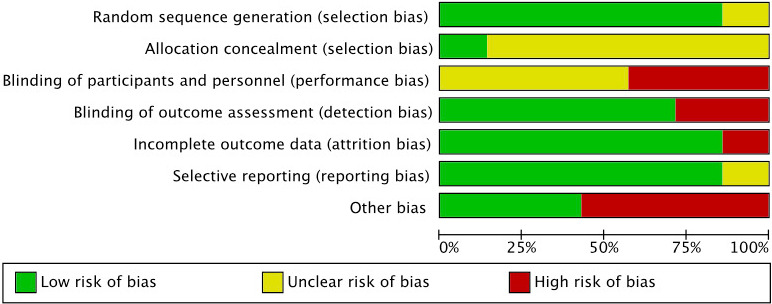
Figure 4.
Forest plot of comparison between IKT (experimental) vs CG articles for changes in pain intensity. SD
3.4.2Disability
Three of the articles retrieved in this review evaluated the effects of an IKT program on disability. Calmels et al. [22] used the Quebec scale to measure functional capacity and found no significant improvements in either the CG (
3.4.3Isokinetic trunk flexor and extensor strength
Only three articles of the retrieved studies evaluated the isokinetic trunk flexor and extensor strength. Olivier et al. [49] found a significant increase between pre-and post-intervention peak torque values in trunk flexor and extensor muscles. However, they only reported statistically significant differences in extensor peak torque between groups at 30
4.Discussion
The objective of this review and meta-analysis was to determine the effects of isokinetic trunk training on pain, disability, and isokinetic trunk strength in NSLBP patients. The main finding of this review is that the trunk IKT could be a clinical tool for pain management in patients with NSLBP, although the evidence is very uncertain. In addition, IKT reduces disability and increases trunk strength in NSLBP patients, although few RCTs exist for IKT on disability or trunk strength in patients with NSLBP.
All the studies included in this review considered patients with cLBP, that is, lasting more than three months. When comparing the clinical manifestations between patients with acute, subacute, or chronic LBP, the latter presents a higher level of pain, greater consumption of analgesics, and greater risk of requiring lumbar surgery than patients with acute and subacute LBP [53]. This review and meta-analysis show decreased pain intensity in the IKT group. The IKT group presents a more significant decrease in pain intensity post-intervention (
The difference in training volumes could explain this high heterogeneity, e.g., the studies conducted by Nambi’s group performed a protocol of 20 sessions, consisting of three sets of 15 repetitions at velocities of 60
A network meta-analysis by Owen et al. [54] attempted to determine the best exercise mode to treat LBP. The results show that Pilates, motor control, and exercise-based or aerobic training decrease pain. However, these results have high heterogeneity and low quality of evidence. Another network meta-analysis conducted by Gianola et al. [55] concluded that pain management in patients with NSLBP should be done with non-pharmacological treatment, in which exercise appears as the best alternative to reduce pain at immediate follow-up. Thus, exercise appears to be a suitable intervention for pain management in LBP.
Although the mechanism by which IKT is effective as an intervention for LBP patients is not known, we postulate that strength training with maximum load throughout the entire range of motion, as in IKT, can contribute to greater spinal stability by training the trunk muscles, which can translate into less pain for patients. However, further research is needed to understand the mechanisms underlying the decrease in pain using IKT.
We know that LBP is the leading cause of disability in the world [56]. In this review, only three studies evaluated the effects of IKT on disability. Calmels et al. report no improvement in disability, whereas de Freitas et al. [51] found a decrease in disability in both groups, with no differences. Sertpoyraz et al. [52], the only one with low RoB, reported decreased disability in the IKT and CG using the MOLBDQ. A reduction of six points in MOLBDQ is considered clinically relevant [57]. Thus, both the IKT and CG groups significantly decreased disability, 7.20 and 8.35 points, respectively, and with clinically meaningful results. Many factors can contribute to disability, such as biophysical, psychological, social, and genetic factors. Therefore, disability is not simply the result of nociceptive inputs [58]. Consequently, different types of interventions can be expected to have positive effects on disability. Thus, isokinetic trunk training could be considered a training option when the goal is to improve the disability of patients with NSLBP. It should not be ignored that these results come from only two study, so they should be interpreted with caution. Thus, further research regarding the effects of IKT on disability is needed.
Trunk muscle strength has been considered a risk factor for developing LBP [14]. In addition, we know that patients with cLBP have a decrease in lumbar extensor isokinetic strength [24]. In this review, although eight studies included a group that trained strength, only three research measured whether the IKT program affects isokinetic trunk strength. Olivier et al. [49], who added only 15 minutes daily IKT to a conventional treatment program, reported a significant increase in both groups, with differences between groups only in extensor strength at 30
Isokinetic muscle strength, a difference of pain intensity and disability, is an objective measure to determine the effects of an intervention. Furthermore, we know that neural adaptations predominate in the first weeks of strength training [60]; we can suggest that further research considering more extended training periods is necessary to observe the chronic effects of strength training in NSLBP patients. In addition, given the questioning regarding the lack of natural movements when using classical isokinetic dynamometers [61], we can further suggest using the new generations of dynamometers with a more functional approach [62, 63]. Functional dynamometers could allow a more significant transfer of these skills to the sports and daily activities of patients with cLBP. Finally, due to the limited evidence regarding disability and trunk strength in NSLBP patients, and limited evidence in non-athletes and women regarding pain intensity, further research is needed to elucidate the role of isokinetic trunk training in subjects with NSLBP.
4.1Study limitations
This review is not exempt from limitations, such as, for example, it only encompasses articles published between 2001 to 2022, which could have excluded some of the evidence from this review. On the other hand, it includes a small number of studies and a small number of participants. In addition, most of the included studies were conducted by the same research group [46, 47, 48, 50], which evaluated only a specific type of young and athletic population, which may make it difficult to generalize the findings of this review to the rest of the patients. Despite being the same research group, the authors clarified that these were different trials with different samples. Moreover, these results should be interpreted with caution due to the high heterogeneity found, probably due to the different samples and training protocols. In addition, we did not perform the publication bias analysis since this analysis requires a minimum of 10 studies, according to the Cochrane handbook [64]. However, we can consider it a strength that there was no language restriction in the retrieved articles. Furthermore, to our knowledge, this is the first review that attempts to determine the potential role of isokinetic trunk strength training in patients with NSLBP.
5.Conclusion
Trunk IKT could be a novel clinical tool for pain management in patients with NSLBP, although evidence is scarce. In addition, few RCTs exist for IKT on disability or trunk strength in patients with NSLBP. Based on the current evidence, it is not possible to provide a clear recommendation on the effects of trunk IKT on pain, disability, and trunk strength. Therefore, further research on this topic is needed.
Ethical approval
Not applicable.
Funding
This study has been partially supported by FEDER/ Junta de Andalucía-Consejería de Transformación Económica, Industria, Conocimiento y Universidades /Proyecto B-CTS-184-UGR20. This work was supported by DGI-University Andres Bello, N
Informed consent
Not applicable.
Author contribution
WR-F Conception of review, database searches, data extraction, risk of bias assessment, statistical analysis, preparation, and revision of manuscript. LC-R Conception of review, reviewed conflicts between investigators, and revision of manuscript. DM-G data extraction, statistical analysis, preparation, and revision of manuscript. AR-P Conception of review, data extraction, preparation, and revision of manuscript. DJ-M Conception of review, database searches, data extraction, risk of bias assessment, preparation, and revision of manuscript. All authors approved the final version.
Supplementary data
The supplementary files are available to download from http://dx.doi.org/10.3233/BMR-220301.
Acknowledgments
This paper will be part of Waleska Reyes-Ferrada Doctoral Thesis performed in the Biomedicine Doctorate Program of the University of Granada, Spain. We appreciate the collaboration in this study of Nicolás Grob-Hernandez, Gonzalo Iturrieta-Correa, Camila Tapia-Brahland, and Geraldine Luengo-Monsalve. The postdoctoral researchers Daniel Jerez-Mayorga, Angela Rodriguez-Perea and Darío Martinez-Garcia has a contract through the programme “Recualificación del Profesorado Universitario. Modalidad Margarita Salas”, Universidad de Granada/Ministerio de Universidades y Fondos Next Generation de la Unión Europea.
Conflict of interest
The authors declare that they have no conflict of interest.
References
[1] | Gatchel RJ. Low Back Pain: Recent Advances and Perspectives. MDPI. Epub ahead of print. (2017) December 29. doi: 10.3390/books978-3-03842-656-1. |
[2] | Hoy D, Brooks P, Blyth F, et al. The Epidemiology of low back pain. Best Pract Res Clin Rheumatol. (2010) ; 24: : 769-781. |
[3] | Buchbinder R, van Tulder M, Öberg B, et al. Low back pain: a call for action. Lancet. (2018) ; 391: : 2384-2388. |
[4] | Wu A, March L, Zheng X, et al. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Ann Transl Med. (2020) ; 8: : 299-299. |
[5] | Vlaeyen JWS, Maher CG, Wiech K, et al. Low back pain. Nat Rev Dis Prim. (2018) ; 4: : 52. |
[6] | Heuch I, Foss IS. Acute low back usually resolves quickly but persistent low back pain often persists. J Physiother. (2013) ; 59: : 127. |
[7] | da Silva T, Mills K, Brown BT, et al. Recurrence of low back pain is common: a prospective inception cohort study. J Physiother. (2019) ; 65: : 159-165. |
[8] | Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. (2017) ; 389: : 736-747. |
[9] | Klyne DM, Hall LM, Nicholas MK, et al. Risk factors for low back pain outcome: Does it matter when they are measured? Eur J Pain. (2022) ; 26: : 835-854. |
[10] | Tagliaferri SD, Ng S, Fitzgibbon BM, et al. Relative contributions of the nervous system, spinal tissue and psychosocial health to non-specific low back pain: Multivariate meta-analysis. Eur J Pain. (2022) ; 26: : 578-599. |
[11] | Catalá MM, Schroll A, Laube G, et al. Muscle Strength and Neuromuscular Control in Low-Back Pain: Elite Athletes Versus General Population. Front Neurosci. (2018) ; 12: : 436. |
[12] | Steele J, Bruce-Low S, Smith D. A reappraisal of the deconditioning hypothesis in low back pain: Review of evidence from a triumvirate of research methods on specific lumbar extensor deconditioning. Curr Med Res Opin. (2014) ; 30: : 865-911. |
[13] | Hori Y, Hoshino M, Inage K, et al. ISSLS PRIZE IN CLINICAL SCIENCE 2019: clinical importance of trunk muscle mass for low back pain, spinal balance, and quality of life – a multicenter cross-sectional study. Eur Spine J. (2019) ; 28: : 914-921. |
[14] | Cho KH, Beom JW, Lee TS, et al. Trunk muscles strength as a risk factor for nonspecific low back pain: a pilot study. Ann Rehabil Med. (2014) ; 38: : 234-240. |
[15] | Lee JH, Hoshino Y, Nakamura K, et al. Trunk muscle weakness as a risk factor for low back pain. A 5-year prospective study. Spine. (1999) ; 24: : 54-57. |
[16] | Tataryn N, Simas V, Catterall T, et al. Posterior-Chain Resistance Training Compared to General Exercise and Walking Programmes for the Treatment of Chronic Low Back Pain in the General Population: A Systematic Review and Meta-Analysis. Sport Med – Open. (2021) ; 7: : 17. |
[17] | Tjøsvoll SO, Mork PJ, Iversen VM, et al. Periodized resistance training for persistent non-specific low back pain: a mixed methods feasibility study. BMC Sports Sci Med Rehabil. (2020) ; 12: : 30. |
[18] | Pedersen BK, Saltin B. Exercise as medicine – evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand J Med Sci Sports. (2015) ; 25: : 1-72. |
[19] | Saragiotto BT, Maher CG, Yamato TP, et al. Motor control exercise for chronic non-specific low-back pain. Cochrane Database Syst Rev. (2016) ; 36: : 301-302. |
[20] | Coulombe BJ, Games KE, Neil ER, et al. Core Stability Exercise Versus General Exercise for Chronic Low Back Pain. J Athl Train. (2017) ; 52: : 71-72. |
[21] | Ozsoy G, Ilcin N, Ozsoy I, et al. The Effects Of Myofascial Release Technique Combined With Core Stabilization Exercise In Elderly With Non-Specific Low Back Pain: A Randomized Controlled, Single-Blind Study. Clin Interv Aging. (2019) ; 14: : 1729-1740. |
[22] | Calmels P, Jacob JF, Fayolle-Minon I, et al. Use of isokinetic techniques vs standard physiotherapy in patients with chronic low back pain. Preliminary results. Ann Readapt Med Phys Rev Sci la Soc Fr Reeduc Fonct Readapt Med Phys. (2004) ; 47: : 20-27. |
[23] | Stark T, Walker B, Phillips JK, et al. Hand-held dynamometry correlation with the gold standard isokinetic dynamometry: A systematic review. PM R. (2011) ; 3: : 472-479. |
[24] | Mueller S, Stoll J, Mueller J, et al. Validity of isokinetic trunk measurements with respect to healthy adults, athletes and low back pain patients. Isokinet Exerc Sci. (2012) ; 20: : 255-266. |
[25] | Reyes-Ferrada W, Chirosa-Rios L, Rodriguez-Perea A, et al. Isokinetic Trunk Strength in Acute Low Back Pain Patients Compared to Healthy Subjects: A Systematic Review. Int J Environ Res Public Health. (2021) ; 18: : 2576. |
[26] | Reyes-Ferrada W, Chirosa-Rios L, Martinez-Garcia D, et al. Reliability of trunk strength measurements with an isokinetic dynamometer in non-specific low back pain patients: A systematic review. J Back Musculoskelet Rehabil. (2022) ; 1: : 1-12. |
[27] | Pontes SS, de Carvalho ALR, de Almeida KO, et al. Effects of isokinetic muscle strengthening on muscle strength, mobility, and gait in post-stroke patients: a systematic review and meta-analysis. Clin Rehabil. (2019) ; 33: : 381-394. |
[28] | Davies GJ, Ellenbecker TS. Application of Isokinetics in Testing and Rehabilitation. In: Physical Rehabilitation of the Injured Athlete. Elsevier; (2012) . pp. 548-570. |
[29] | Park J-H, Chung SW, Lee S-J, et al. Evaluation of the Electromyographic Amplitude-to-Work Ratio in the Infraspinatus Muscle During External Shoulder Rotation Exercises: A Comparison of Concentric Isotonic and Isokinetic Exercises. Orthop J Sport Med. (2020) ; 8: : 232596712093245. |
[30] | Malliou PC. Effective ways of restoring muscular imbalances of the rotator cuff muscle group: a comparative study of various training methods. Br J Sports Med. (2004) ; 38: : 766-772. |
[31] | Keles SB, Sekir U, Gur H, et al. Eccentric/concentric training of ankle evertor and dorsiflexors in recreational athletes: Muscle latency and strength. Scand J Med Sci Sport. (2014) ; 24: : 29-38. |
[32] | Golik-Peric D, Drapsin M, Obradovic B, et al. Short-Term Isokinetic Training Versus Isotonic Training: Effects on Asymmetry in Strength of Thigh Muscles. J Hum Kinet. (2011) ; 30: : 29-35. |
[33] | Lee SEK, Lira CAB de, Nouailhetas VLA, et al. Do isometric, isotonic and/or isokinetic strength trainings produce different strength outcomes? J Bodyw Mov Ther. (2018) ; 22: : 430-437. |
[34] | Vidmar MF, Baroni BM, Michelin AF, et al. Isokinetic eccentric training is more effective than constant load eccentric training on the quadriceps rehabilitation following partial meniscectomy: A randomized clinical trial. Phys Ther Sport. (2019) ; 39: : 120-125. |
[35] | Vidmar MF, Baroni BM, Michelin AF, et al. Isokinetic eccentric training is more effective than constant load eccentric training for quadriceps rehabilitation following anterior cruciate ligament reconstruction: a randomized controlled trial. Brazilian J Phys Ther. (2020) ; 24: : 424-432. |
[36] | Zinke F, Warnke T, Gäbler M, et al. Effects of isokinetic training on trunk muscle fitness and body composition in world-class canoe sprinters. Front Physiol. (2019) ; 10: : 21. |
[37] | Zhang X, Bi X, Shao J, et al. Curative effects on muscle function and proprioception in patients with chronic lumbar disk herniation using isokinetic trunk muscle strength training. Int J Clin Exp Med. (2019) ; 12: : 4311-4320. |
[38] | Ciriello VM, Shaw WS, Rivard AJ, et al. Dynamic training of the lumbar musculature to prevent recurrence of acute low back pain: a randomized controlled trial using a daily pain recall for 1 year. Disabil Rehabil. (2012) ; 34: : 1648-1656. |
[39] | Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) ; 372: : n71. |
[40] | Ouzzani M, Hammady H, Fedorowicz Z, et al. Rayyan – a web and mobile app for systematic reviews. Syst Rev. (2016) ; 5: : 210. |
[41] | Higgins JPT, Altman DG, Sterne JAC. Assessing risk of bias in included studies. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration; (2011) . Available from: https://handbook.cochrane.org. |
[42] | Hartling L, Ospina M, Liang Y, et al. Risk of bias versus quality assessment of randomised controlled trials: cross sectional study. BMJ. (2009) ; 339: : b4012-b4012. |
[43] | Santesso N, Glenton C, Dahm P, et al. GRADE guidelines 26: informative statements to communicate the findings of systematic reviews of interventions. J Clin Epidemiol. (2020) ; 119: : 126-135. |
[44] | Cochran WG. The combination of estimates from different experiments. Biometrics. (1954) ; 10: : 101-129. |
[45] | DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. (1986) ; 7: : 177-188. |
[46] | Nambi G, Abdelbasset WK, Alrawaili SM, et al. Virtual reality or isokinetic training; its effect on pain, kinesiophobia and serum stress hormones in chronic low back pain: A randomized controlled trial. Technol Heal Care. (2021) ; 29: : 155-166. |
[47] | Nambi G, Abdelbasset WK, Alqahtani BA, et al. Isokinetic back training is more effective than core stabilization training on pain intensity and sports performances in football players with chronic low back pain. Medicine (Baltimore). (2020) ; 99: : e20418. |
[48] | Nambi G, Abdelbasset WK, Alsubaie SF, et al. Isokinetic training – its radiographic and inflammatory effects on chronic low back pain. Medicine (Baltimore). (2020) ; 99: : e23555. |
[49] | Olivier N, Lepretre A, Caby I, et al. [Does exercise therapy for chronic lower-back pain require daily isokinetic reinforcement of the trunk muscles?]. Ann Readapt Med Phys Rev Sci la Soc Fr Reeduc Fonct Readapt Med Phys. (2008) ; 51: : 284-291. |
[50] | Nambi G, Abdelbasset WK, Elsayed SH, et al. Comparative Effects of Isokinetic Training and Virtual Reality Training on Sports Performances in University Football Players with Chronic Low Back Pain-Randomized Controlled Study. Evidence-Based Complement Altern Med. (2020) ; 2020: : 1-10. |
[51] | Freitas CD, Greve JMD. Comparison between isokinetic dynamometer and therapeutic ball exercises in chronic low-back pain of mechanical origin. Fisioter e Pesqui. (2008) ; 15: : 380-386. |
[52] | Sertpoyraz F, Eyigor S, Karapolat H, et al. Comparison of isokinetic exercise versus standard exercise training in patients with chronic low back pain: a randomized controlled study. Clin Rehabil. (2009) ; 23: : 238-247. |
[53] | Hüllemann P, Keller T, Kabelitz M, et al. Clinical Manifestation of Acute, Subacute, and Chronic Low Back Pain in Different Age Groups: Low Back Pain in 35,446 Patients. Pain Pract. (2018) ; 18: : 1011-1023. |
[54] | Owen PJ, Miller CT, Mundell NL, et al. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br J Sports Med. (2019) ; 1-12. |
[55] | Gianola S, Bargeri S, Del Castillo G, et al. Effectiveness of treatments for acute and subacute mechanical non-specific low back pain: a systematic review with network meta-analysis. Br J Sports Med. (2022) ; 56: : 41-50. |
[56] | GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. (2018) ; 392: : 1789-1858. |
[57] | Fritz JM, Irrgang JJ. A comparison of a modified Oswestry Low Back Pain Disability Questionnaire and the Quebec Back Pain Disability Scale. Phys Ther. (2001) ; 81: : 776-88. |
[58] | Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. Lancet. (2018) ; 391: : 2356-2367. |
[59] | Schoenfeld BJ, Ogborn D, Krieger JW. Dose-response relationship between weekly resistance training volume and increases in muscle mass: A systematic review and meta-analysis. J Sports Sci. (2017) ; 35: : 1073-1082. |
[60] | Pearcey GEP, Alizedah S, Power KE, et al. Chronic resistance training: is it time to rethink the time course of neural contributions to strength gain? Eur J Appl Physiol. (2021) ; 121: : 2413-2422. |
[61] | Bouilland S, Loslever P, Lepoutre FX. Biomechanical comparison of isokinetic lifting and free lifting when applied to chronic low back pain rehabilitation. Med Biol Eng Comput. (2002) ; 40: : 183-192. |
[62] | Dvir Z, Müller S. Multiple-joint isokinetic dynamometry: a critical review. J Strength Cond Res. (2019) ; 0: : 1-15. |
[63] | Rodriguez-Perea Á, Jerez-Mayorga D, García-Ramos A, et al. Reliability and concurrent validity of a functional electromechanical dynamometer device for the assessment of movement velocity. Proc Inst Mech Eng Part P J Sport Eng Technol. (2021) ; 1-6. |
[64] | Mavridis D, Salanti G. How to assess publication bias: Funnel plot, trim-and-fill method and selection models. Evid Based Ment Health. (2014) ; 17: : 30. |


