
Observation of the therapeutic effect of auricular bean pressing on early knee osteoarthritis pain: A randomized controlled trial
Abstract
BACKGROUND:
In the treatment of knee osteoarthritis (KOA), there is a need for the long-term use of therapeutic drugs that reduce joint pain and have fewer adverse effects.
OBJECTIVE:
This study aimed to investigate the therapeutic effect of bean pressing on ear points on early KOA pain.
METHODS:
One hundred patients with KOA recruited at the Wenzhou Hospital of Traditional Chinese Medicine between February 2019 and May 2022 were divided randomly into a treatment group (
RESULTS:
On day 5 following the start of treatment, the visual analog scale (VAS) and WOMAC scores of the treatment group were significantly lower than those of the control group (
CONCLUSIONS:
Auricular bean-pressing therapy had an analgesic effect and could also alleviate mild to moderate KOA swelling, joint stiffness, and other symptoms, effectively reducing the demand for NSAIDs and improving both knee function and quality of life. The results suggested that auricular bean-pressing therapy has promising prospects in the treatment of early KOA pain.
1.Introduction
Knee osteoarthritis (KOA) is pathologically characterized by cartilage destruction, degeneration, bone hyperplasia, aseptic synovitis, and ligament degeneration. Its clinical manifestations include pain, swelling, and limited mobility, and in severe cases, it may lead to knee disability, which more frequently occurs in middle-aged and elderly people [1]. The main goal of treating KOA is to reduce pain and improve function [2]. Several options are available to treat KOA, including weight loss, lifestyle advice, exercise therapy, nonsteroidal anti-inflammatory drugs (NSAIDs), corticosteroid injections, and glucosamine supplements. The most commonly used pain treatment drugs are NSAIDs, but their long-term use increases the risk of gastrointestinal bleeding and vascular adverse events [3]. Therefore, there is a need for the long-term use of therapeutic drugs that reduce joint pain and have fewer adverse effects.
Auricular point bean pressing involves pressing and fixing cowherb seed on the auricular points to continuously stimulate them and create a therapeutic effect [4]. The method of pressing auricular points to prevent and treat diseases as a treatment method in China has a history of over 2,000 years. In recent decades, its application has increased considerably, particularly for conditions characterized by pain. According to previous literature [5, 6], auricular point bean pressing (on knee acupoints, for example) has a beneficial effect on relieving pain in patients with KOA who have been treated conservatively or surgically. Other acupoints, such as the adrenal, subcortical, and endocrinal acupoints, are closely associated with sedative and analgesic effects, which are beneficial for relieving the symptoms of KOA. However, there are few studies on the application of auricular point bean pressing to treat early KOA. The present study intervened in early KOA cases using auricular point bean pressing and studied its effect on the Western Ontario and McMaster Universities Osteoarthritis (WOMAC) indexes of function, pain, and stiffness to determine whether acupressure on four pre-selected specific auricular points could relieve joint pain, reduce NSAID consumption, relieve symptoms, and improve functioning. The results provide an evidence-based foundation for clinical treatment.
2.Materials and methods
2.1Clinical data
This was a randomized controlled trial. One hundred participants were selected from patients with KOA who were treated at the Department of Orthopedics of Wenzhou Hospital of Traditional Chinese Medicine between February 2019 and May 2022. The standard follow-up for all treated patients lasted 4 weeks. The study was approved by the ethics committee of the Wenzhou Hospital of Traditional Chinese Medicine Affiliated to Zhejiang University of Traditional Chinese Medicine (approval no. WTCM-H-KT-2019047), and all patients provided signed informed consent for their inclusion in the research. The study met the requirements of the Declaration of Helsinki.
One hundred patients with KOA enrolled in this study were divided into control and study groups (
The inclusion criteria were: (1) patients
The exclusion criteria were: (1) patients who had undergone knee surgery, (2) patients who had undergone intra-articular injection treatment within 3 months before the study treatment, (3) patients who could not complete the data collection form, and (4) patients with ear eczema or a history of any ear surgery.
2.2Therapeutic methods
Figure 1.
Auricular bean-pressing process. (A) Disinfection; (B) Selected auricular acupoints; (C) Fixed Cowherb seeds: (D) Finished.

The control group received routine rehabilitation treatment. In both groups, the patients required NSAIDs during treatment and follow-up; this was prescribed as oral celecoxib (Pfizer Inc., USA) as an anti-inflammatory and for pain relief, one tablet twice a day. Functional exercises were prescribed: isometric training, e.g., straight leg raising and plantar dorsiflexion as the main methods for enhancing muscle strength when the pain was severe or in the acute stage. Joint loosening training included femoral-tibial and proximal tibiofibular joint long-axis traction, patellofemoral lateral and up-down sliding, patellofemoral joint separation, lateral horizontal pushing of the femorotibial joint, patella sliding, and knee extension swings [8]. Each of the above movements was held for 30 s, and 30 training exercises were completed each day. Following pain relief, resistance training for the quadriceps and other muscles around the knee was performed. The patient’s legs were fixed, and the knees could sag naturally; then, the affected limbs were actively extended, and the knees were flexed 50 times/d [9].
The treatment group received auricular point bean-pressing therapy based on the rehabilitation treatment. For auricular disinfection, a cotton swab was pressed onto the acupoints (Fig. 1A). Four auricular acupoints on the same side as the affected knee were selected; these corresponded to the knee and to adrenal, subcortical, and endocrinal [10] functions (Fig. 1B). Cowherb seeds (Tai Cheng Company) were fixed and pressed in an alternative press–release pattern, moving from light to heavy pressure (Fig. 1C). Each acupoint was pressed 20 times, for 5 s each time, to strengthen the stimulation. The pressing strength was sufficient for turning the auricle red, warm, or sore while remaining tolerable. The acupoints on both ears were pressed alternately for 3 min/acupoint, 3 times/d. The cowherb seeds were changed every 3 d, and the course of treatment was 4 weeks [11] (Fig. 1D). The cowherb seeds were fixed to the side where the KOA was observed and were pressed daily in the morning, at noon, and in the evening, with each time lasting approximately 3 min. Pressing was stopped when the patient experienced soreness, numbness, or fever. Patients received the guidance of professional traditional Chinese medicine (TCM) clinical staff to maintain their compliance and ensure accurate acupoint pressure performance.
2.3Treatment indexes
To assess the efficacy of treatment on knee function and pain, the WOMAC index scores [12], the pain visual analog scale (VAS) [13], and serum C-reactive protein (CRP) before and 1 month after treatment were employed as the primary outcomes to evaluate patients. Additionally, the patients’ dependence on celecoxib was a secondary outcome in this study.
The WOMAC is used mainly to evaluate the degree of KOA in patients. The scale includes three dimensions: pain, stiffness, and joint function, with 24 evaluation items. A five-grade scoring method was adopted, and each item was scored from 0 to 4 points according to severity (maximum score: 96 points). The higher the score, the more serious the condition.
The VAS scale comprised a 100-mm-long line with anchoring descriptors. The patient marked the line to indicate their pain perception, and the result was expressed as the distance from the left end point to the marked point (in mm). The maximum score was 10 points. The lower the score, the better the pain relief effect.
The CRP level with high sensitivity can provide effective information for many types of chronic diseases, and its value greatly increases in the early stage of inflammation. In the present study, 5 mL of fasting venous blood was collected from the patient in the morning and centrifuged at high speed. Serum was obtained, and the CRP value was detected by radioimmunoassay.
2.4Statistical analysis
We used SPSS™ Statistics v25.0 software (IBM, Chicago, USA) for all data processing. The data with normal or approximately normal distribution were expressed as mean
3.Results
3.1General information statistics
Table 1
Comparison of general data of patients between two groups
| Group | Treatment group | Control group | |
|---|---|---|---|
| Number of cases | 50 | 50 | |
| Gender (male/female) | 21/29 | 23/27 | 0.687 |
| Age | 69.30 | 67.24 | 0.050 |
| WOMAC total score | 71.30 | 70.00 | 0.181 |
| Kellgren grade (number) (II/III) | 23/27 | 24/26 | 0.841 |
Figure 2.
Sample size determination. Notes: The map summarizes the number of the retrospectively selected patients, patients excluded, and the final sample size obtained.
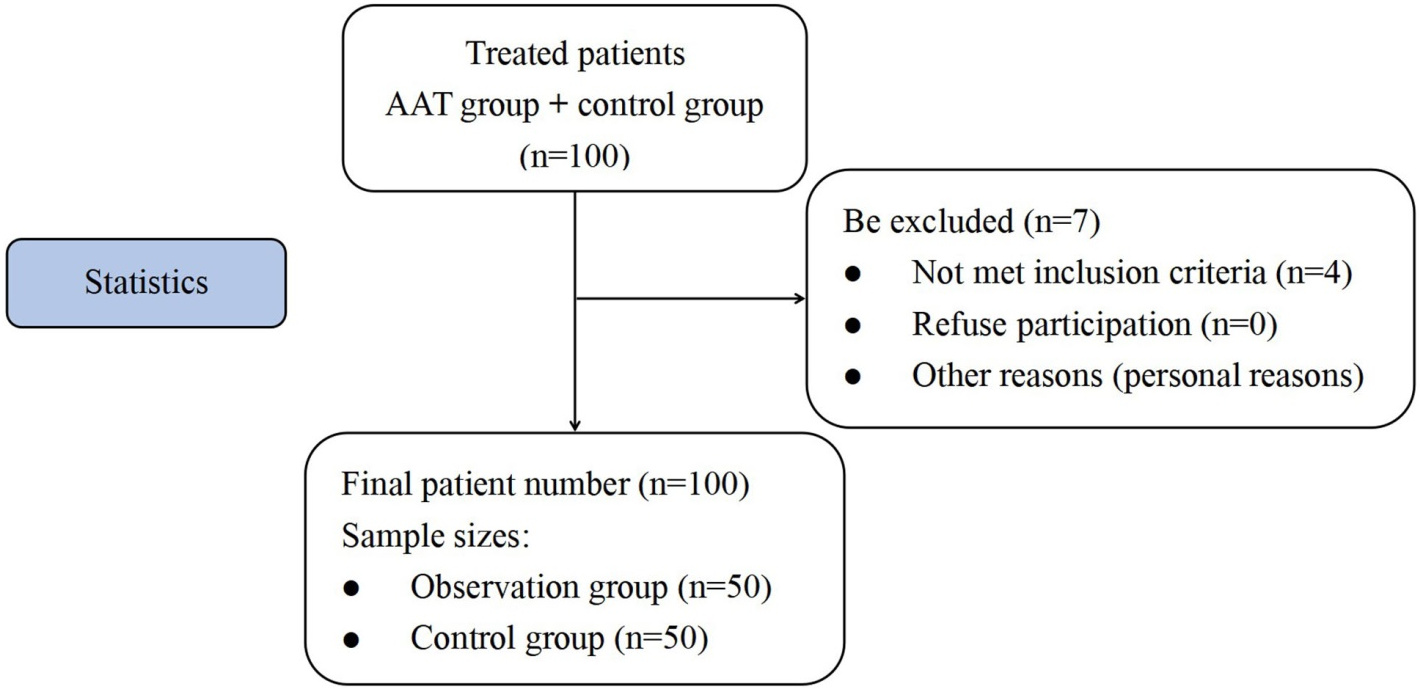
Of the 107 patients sampled in this study, 7 did not meet the inclusion criteria, and 3 were excluded based on the above clinical criteria. None of the patients refused to provide informed consent or undergo continued treatment. Follow-up was discontinued for 4 patients for personal reasons (Fig. 2). Of the 100 patients with KOA who were finally included, 50 received auricular plaster and 50 did not. None of the patients in the statistical analysis were found to have experienced complications. Among the 100 patients, 56 (56%) were women, 44 (44%) were men, 35 (35%) had Class-II KL, and 65 patients (65%) had Class-III KL. The differences in gender, age, body mass index, and KOA classification (KL type) between the two groups were not statistically significant (
3.2Comparison of the knee sign scores and C-reactive protein levels between the two groups before and after treatment
Table 2
Comparison of swelling, tenderness, range of motion, and CRP between the two groups (
| Treatment group | Control group | |||
|---|---|---|---|---|
| SQ swelling | Before treatment | 2.92 | 2.90 | 0.730 |
| After treatment | 1.42 | 2.64 | ||
| Tenderness | Before treatment | 1.94 | 1.96 | 0.650 |
| After treatment | 0.80 | 1.24 | ||
| ROM | Before treatment | 2.90 | 2.84 | 0.377 |
| After treatment | 1.06 | 2.40 | ||
| CRP | Before treatment | 18.41 | 17.82 | 0.243 |
| After treatment | 4.94 | 10.65 |
Compared with the same group before treatment,
Table 3
Comparison of WOMAC scores between the two groups (
| Treatment group | Control group | |||
|---|---|---|---|---|
| Function | Before treatment | 46.58 | 45.48 | 0.204 |
| After treatment | 18.52 | 24.78 | ||
| Pain | Before treatment | 19.48 | 19.36 | 0.604 |
| After treatment | 7.40 | 14.14 | ||
| Stiffness | Before treatment | 5.24 | 5.16 | 0.750 |
| After treatment | 2.20 | 3.70 | ||
| Total score | Before treatment | 71.30 | 70.00 | 0.181 |
| After treatment | 28.12 | 42.62 |
Compared with the same group before treatment,
After 4 weeks of treatment, the swelling, pain, mobility score, and CRP of the knee joints in the treatment group were significantly lower than those in the control group (all
3.3Comparison of the Western Ontario and McMaster Universities osteoarthritis scores between the two groups before and after treatment
The comparison of the total WOMAC scores between the two groups before treatment was not statistically significant (
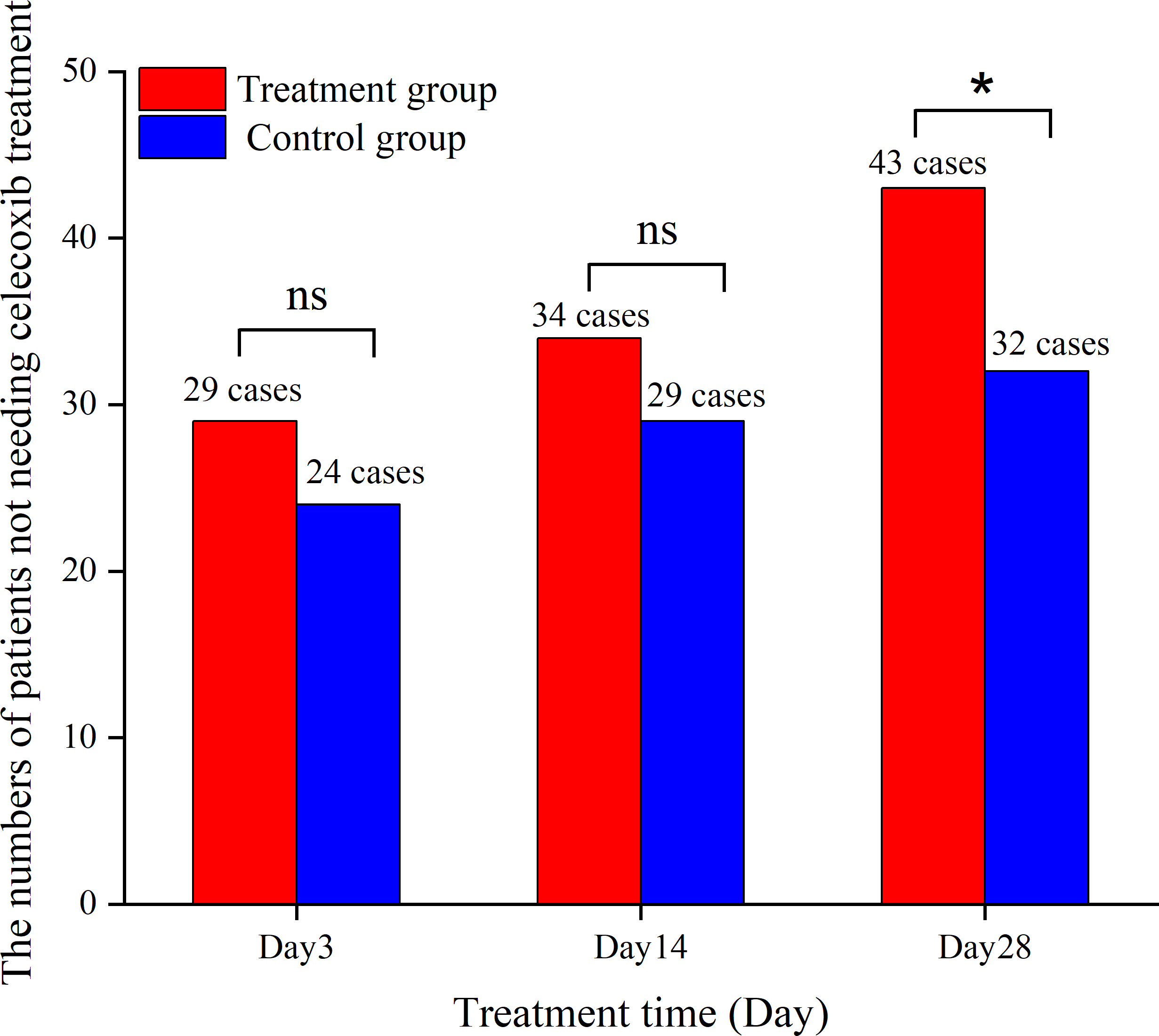
After 4 weeks of treatment, the NSAID requirement of the treatment group was significantly lower than that of the control group (Fig. 3).
Figure 3.
The numbers of patients not requiring celecoxib treatment in both treatment group and control group.
4.Discussion
In the present study, the VAS and WOMAC scores of the treatment group were significantly lower than those of the control group, demonstrating that auricular bean-pressing therapy possessed analgesic and discomfort relief effects, for example, relieving mild- to moderate-degree KOA swelling, joint stiffness, and other symptoms. Considerable evidence has demonstrated the analgesic effect of auricular point bean-pressing therapy [14]. A modern study suggests that the ear is rich in nerves and blood vessels, and stimulating ear acupoints can relieve pain by increasing nerve pain thresholds and regulating the metabolism of pain-causing substances in the body [15].
The pathogenesis of KOA, a degenerative joint disease, remains unclear. It may be related to age, obesity, genetics, and other factors and can be secondary to joint injuries or joint diseases, such as meniscus rupture, joint deformity, and periarticular fractures [16]. The main pathological features of KOA are the degeneration and destruction of articular cartilage, subchondral bone sclerosis, and the formation of osteophytes at the joint edge [17]. The main causes of cartilage destruction are synovial hyperplasia, fibrosis changes, the release of cytokines, and inflammatory factors activating chondrocyte matrix metalloenzymes [18] and degrading extracellular matrix, which chondrocytes depend on for survival [19]. Another study revealed that KOA may also be related to intraosseous hypertension [20]. Here, intraosseous blood circulation in the knee joint is impaired, and intraosseous arterial perfusion is reduced, resulting in insufficient oxygen supply, which damages the nutrient and blood supply environment of the joints and ultimately accelerates the degeneration of articular cartilage. Therefore, inhibiting inflammatory response, improving intraosseous circulation, and delaying the degeneration of articular cartilage are key to preventing and treating KOA [21].
Of note, the results of the present study showed that after 28 days of intervention, the number of people in the treatment group who needed to take celecoxib was significantly lower than that of the control group, and the difference was statistically significant. The dependence on NSAIDs and related complications was also effectively improved after auricular bean-pressing therapy.
A slow, progressive, and chronic disease, osteoarthritis is the leading cause of disability among elderly people. Existing studies showed that many cytokines, growth factors [22], and signaling pathways are involved in regulating osteoarthritis [23, 24]. While NSAIDs can reduce the pain brought on by KOA, their long-term use may cause adverse effects. Auricular point bean-pressing therapy is a method based on the theory of acupuncture and moxibustion in TCM; it regulates the qi and blood of the internal organs by stimulating the acupuncture points on the ear to treat a range of diseases [25, 26]. The effect can be remarkable, particularly for patients with existing pain.
Auricular point bean-pressing therapy has the potential to treat KOA [27]. In the present study, four auricular points on the side where KOA was present, corresponding to the knee and subcortical, adrenal, and endocrinal functioning received acupoint massage. The knee acupoints corresponded to pressure points that relieved knee pain, while the adrenal, subcortical, and endocrinal acupoints were linked to sedative and analgesic effects [24]. The knee and subcortical acupoints present in the ear are holographic targets for delivering therapy to the human body; when stimulated, the feedback information derived from these points is delivered immediately to the location of the disease to mobilize the meridians and stimulate the analgesic structures in the brain to release endorphins and enkephalin analgesic substances [28, 29]. Additionally, these stimulation feedback signals can antagonize pulses emanating from the pain site to reduce pain [30]. Auricular adrenal and endocrinal acupoints can dredge meridians, regulate viscera, relieve spasm and pain, balance yin and yang, and regulate the excitation and inhibition of the cerebral cortex and disorder in the autonomic nervous center; they can also relieve cerebral cortex tension and stimulate the body to secrete pain-relieving substances, thereby inhibiting pain [31]. Tong [32] showed that the auricular adrenal and endocrinal acupoints, which were also selected in the current study, could regulate inflammatory factors and treat inflammatory lesions. These two acupoints play key roles in inhibiting the inflammatory response of the knee joint, improving intraosseous circulation, and reducing knee joint pain. Additionally, Zhang et al. [33] demonstrated that auricular acupressure on the acupoints, such as the knee joint and subcortex, plays a part in relieving analgesia and effectively decreasing NSAID requirements without inducing adverse effects when treating KOA.
Cowherb seed is a well-known TCM herb and is listed in the Chinese Pharmacopoeia, which is widely used in auricular point therapy in China. The seeds have no intrinsic therapeutic value but simply provide physical stimulation to the acupoints and are thus suitable for clinical auricular point bean-pressing therapy.
The small sample size of the present single-center study may have led to some error in the experimental results. Additionally, the short follow-up period in the present study made it difficult to determine the long-term effects of auricular bean pressing on patients with KOA. Further research should be undertaken without these limitations.
5.Conclusion
The present study demonstrated that compared with conventional rehabilitation, auricular point bean-pressing therapy combined with conventional rehabilitation treatment can further relieve knee pain, improve patients’ knee function, and reduce the demand for NSAIDs. This reduces adverse reactions caused by taking drugs, indicating that auricular point bean-pressing therapy combined with conventional rehabilitation treatment could be an effective strategy in treating KOA pain.
Ethical approval
The study was conducted in accordance with the Declaration of Helsinki (as was revised in 2013). The study was approved by the ethics committee of the Wenzhou Hospital of Traditional Chinese Medicine Affiliated to Zhejiang University of Traditional Chinese Medicine (approval no. WTCM-H-KT-2019047).
Funding
The study was supported by Wenzhou Basic Scientific Research Projects (No. Y20190732).
Informed consent
All patients provided signed informed consent for their inclusion in the research.
Author contributions
Conception and design of the research: Yeyan Lin, Xuelai Zhou.
Acquisition of data: Yeyan Lin, Bin Shen.
Analysis and interpretation of the data: Yeyan Lin, Cunxian Lv.
Statistical analysis: Yeyan Lin, Yongqin Wu.
Obtaining financing: Xuelai Zhou.
Writing of the manuscript: Yeyan Lin.
Critical revision of the manuscript for intellectual content: Yeyan Lin.
All authors read and approved the final draft.
Acknowledgments
The authors are particularly grateful to everyone who helped them with the article.
Conflict of interest
The authors declare that they have no competing interests.
References
[1] | Giwnewer U, Rubin G, Orbach H, Rozen N. Treatment for Osteoarthritis of the Knee. Harefuah. (2016) Jul; 155: (7): 403-406. Hebrew. PMID: 28514128. |
[2] | Guidelines for diagnosis and treatment of osteoarthritis (2018 edition). Chinese Journal of Orthopaedics. (2018) ; 38: (12): 705-715. |
[3] | Blandizzi C, Tuccori M, Colucci R, Fornai M, Antonioli L, Ghisu N, DelTacca M. Role of coxibs in the strategies for gastrointestinal protection inpatients requiring chronic non-steroidal anti-inflammatory therapy. Pharmacol Res. (2009) Feb; 59: (2): 90-100. doi: 10.1016/j.phrs.2008.11.004. Epub 2008 Nov 27. PMID: 19073262. |
[4] | Huang LG, Xiao LW. Clinical observation of auricular acupoint therapy inalleviating pain of knee osteoarthritis. Heilongjiang Journal of Traditional Chinese Medicine. (2015) ; 44: (1): 43. doi: CNKI:SUN:HLZY.0.2015-01-029. |
[5] | Liu MM, Tong YG, Chai L, Lei S, Chen JJ. Auricular acupressure therapyfor mild or moderate chronic non-cancer pain: a systematic review. ChineseJournal of Modern Nursing. (2019) ; 25: (16): 2079-2084. doi: 10.3760/cma.j.issn.1674-2907.2019.16.025. |
[6] | He BJ, Tong PJ, Li J, Jing HT, Yao XM. Auricular acupressure foranalgesia in perioperative period of total knee arthroplasty. Pain Med. (2013) Oct; 14: (10): 1608-13. doi: 10.1111/pme.12197. Epub 2013 Jul 18. PMID: 23865512. |
[7] | Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. (1957) Dec; 16: (4): 494-502. doi: 10.1136/ard.16.4.494. PMID: 13498604; PMCID: PMC100 6995. |
[8] | Willingly, Jin R, Yang Y, Kou Y. Analysis of kneeosteoarthritis from the biomechanics of lower limbs. Chinese Journal ofRehabilitation Theory & Practice. (2013) ; 19: (6): 505-509. |
[9] | Wang J, Wang S, Wang YJ. Clinical observation of auricular acupointpressing beans combined with traditional Chinese medicine prescription andacupuncture in the treatment of knee osteoarthritis. Guangming Journal ofChinese Medicine. (2019) ; 34: (6): 917-919. doi: CNKI:SUN:GMZY.0.2019-06-043. |
[10] | Wang Z. Illustrated Auricular Acupoints – Diagnosis, Treatment and Cosmetology. Beijing: China Medical and Technology Press; (2015) . vol. 23. |
[11] | Guan XF, Yang YJ, Lv SW, Qiao L, Luo J, Zhang J, Wang X. Therapeutic effect of comprehensive rehabilitation therapy combined with traditional Chinese and western medicine on knee osteoarthritis. Chinese Archives of Traditional Chinese Medicine. (2016) ; 34: (8): 1980-1982. doi: 10.13193/j.issn.1673-7717.2016.08.054. |
[12] | Gandek B. Measurement properties of the Western Ontario and McMaster Universities Osteoarthritis Index: a systematic review. Arthritis Care Res (Hoboken). (2015) Feb; 67: (2): 216-29. doi: 10.1002/acr.22415. PMID: 25048451. |
[13] | He L, Yue J, Yang L, Wu B, Cao G, Guo Y, Lai G, Tang Y, Ni J. Cervicogenic headache alleviation after cervical coblation nucleoplasty: Aprospective cohort study. Medicine (Baltimore). (2016) Sep; 95: (39): e4786. doi: 10.1097/MD.00000000. PMID: 27684803; PMCID: PMC 5265896. |
[14] | Yu XH, Zhang CP, Zhang YW. Literature study on the rule of auricular point analgesia. Shandong Journal of Traditional Chinese Medicine. (2015) ; 34: (2): 112-113. doi: 10.16295/j.cnki.0257-358x.2015.02.009. |
[15] | Wang FC. Subject of Acupuncture and Moxibustion Technique. Shanghai:Shanghai Science and Technology Press; (2009) . vol. 141. |
[16] | Shen YQ, Liu FX, Cao H, Ma AG. Clinical manifestation and influencefactors in patients with knee osteoarthritis. Chinese Journal of Tissue Engineering Research. (2011) ; 15: (9): 1643-1646. doi: 10.3969/j.issn.1673-8225.2011.09.030. |
[17] | Clinical diagnosis and treatment guidelines of TCM orthopedics andtraumatology: knee paralysis (knee osteoarthritis). Journal of Rehabilitation. (2019) ; 29: (3): 1-7. |
[18] | Yuan Q, Kan WB, Song PF, Zhao J, Yu WG, Wang YJ. Influence of Bushen Huoxue decoction on β-catenin, MMP-7 of synoviocytes in rats withknee osteoarthritis. China Journal of Orthopaedics and Traumatology. (2012) ; 25: (9): 761-765. doi: 10.3969/j.issn.1003-0034.2012.09.014. |
[19] | He BJ, Fang Z, Xie GY, Xu SY. The effect of steaming and washing with Chinese medicine on the level of MMP-3 and MMP-13 in joint synovia ofpatients with osteoarthritis. Acta Chinese Medicine and Pharmacology. (2011) ; 39: (4): 61-64. doi: 10.19664/j.cnki.1002-2392.2011.04.025. |
[20] | Dai QY, Qin XL, Yuan JY, Lin GQ, Liu J, Ruan P, Teng JZ, Rong XB, Han J, Qin J, Wu ZP, Wang X. Construction of a high intraosseous pressure typerabbit osteoarthritis model. Chinese Journal of Tissue Engineering Research. (2011) ; 15: (20): 3645-3648. doi: 10.3969/j.issn.1673-8225.2011.20.009. |
[21] | Zaimreh Y. Correlation between subchondral bone blood supply and osteoarthritis of knee joint. Xinjiang Medical University; (2019) . |
[22] | Chen G, Yao Y, Xu G, Zhang X. Regional difference in microRNA regulation in the skull vault. Dev Dyn. (2019) Oct; 248: (10): 1009-1019. doi: 10.1002/dvdy.97. Epub 2019 Aug 20. PMID: 31397024. |
[23] | Juma SN, Gong X, Hu S, Lv Z, Shao J, Liu L, Chen G. Shark new antigenreceptor (IgNAR): structure, characteristics and potential biomedic alapplications. Cells. (2021) May 8; 10: (5): 1140. doi: 10.3390/cells10051140. PMID: 34066890; PMCID: PMC8151367. |
[24] | Zhang X, Sun X, Chen G. Effect of the combinative use of acupotomy therapy and ultrasonic drug penetration in treating knee joint osteoarthritis. QJM. (2022) Jan 21; 115: (1): 12-16. doi: 10.1093/qjmed/hcaa278. PMID: 33010179. |
[25] | Li YX, Zhao YS, Liu YH. Effects of mindfulness training combined with auricular acupressure on sleep quality and negative emotion in patients with stroke. Chinese Journal of Modern Nursing. (2020) ; 26: (3): 386-389. doi: 10.3760/cma.j.issn.1674-2907.2020.03.020. |
[26] | Chu QQ, Huai SL, Yang J. Effects of point massage combined withpressing ear acupoints with beans on enteral nutritional diarrhea in severepatients. Chinese Journal of Modern Nursing. (2020) ; 26: (35): 4873-4876. doi: 10.3760/cma.j.cn115682-20200714-04369. |
[27] | Kligler B, Nielsen A, Kohrherr C, Schmid T, Waltermaurer E, Perez E, Merrell W. Acupuncture therapy in a group setting for chronic pain. PainMed. (2018) Feb 1; 19: (2): 393-403. doi: 10.1093/pm/pnx134. Erratum in: Pain Med. 2017 Sep 1;18(9):1830. PMID: 28595273. |
[28] | Wang L, Zhao B, Zhou L. Research progress of auricular pointsin the United States. In: Proceedings of the 14th National Symposium on Auricular Diagnosis and Treatment and the Inaugural Meeting of the Auricular Auriculation Professional Committee of Guangdong Acupuncture Association. Foshan: Guangdong Acupuncture and Moxibustion Society; (2012) . |
[29] | Xiang D, Situ Y, Deng S. Experimental study on the effectof electroacupuncture on β-endorphins and uterine activity inendometriosis model animals. Chinese Medical Forum. (2005) ; 4: : 46-47. |
[30] | Zhang Q, Yue J, Golianu B, Sun Z, Lu Y. Updated systematic review andmeta-analysis of acupuncture for chronic knee pain. Acupunct Med. (2017) Dec; 35: (6): 392-403. doi: 10.1136/acupmed-2016-011306. Epub 2017 Nov 8. PMID: 29117967. |
[31] | Agosta C, Laugier J, Guyon L, Denis J, Bertherat J, Libé R, Boisson B, Sturm N, Feige JJ, Chabre O, Cherradi N. MiR-483-5p and miR-139-5ppromote aggressiveness by targeting N-myc downstream-regulated gene familymembers in adrenocortical cancer. Int J Cancer. (2018) Aug 15; 143: (4): 944-957. doi: 10.1002/ijc.31363. Epub 2018 Mar 30. PMID: 29516499. |
[32] | Tong PJ, Wang HD, Ma ZC, Ji WF, Li J, Pan T. Application and effect ofauricular acupoint pressing for analgesia in perioperative period of totalknee joint replacement. Chinese Journal of Integrated Traditional andWestern Medicine. (2010) ; 30: (9): 931-934. doi: CNKI:SUN:ZZXJ.0.2010-09-011. |
[33] | Zhang X, He B, Wang H, Sun X. Auricular acupressure for treating earlystage of knee osteoarthritis: a randomized, sham-controlled prospectivestudy. Randomized Controlled Trial. (2022) Aug 13; 115: (8): 525-529. doi: 10.1093/qjmed/hcab230. |

