
The effect of sleep hygiene and physiotherapy on bruxism, sleep, and oral habits in children with sleep bruxism during the COVID-19 pandemic
Abstract
BACKGROUND:
Sleep bruxism has been associated with temporomandibular dysfunction, pain, fatigue, and poor sleep quality.
OBJECTIVE:
The aim of this study was to determine the gender and age distribution of sleep and oral habits of children with sleep bruxism and to examine the effect of a sleep hygiene and physiotherapy program.
METHODS:
In this cross-sectional study, 82 children aged 6–13 years with sleep bruxism were initially screened between March 2020 and June 2021, from which 37 of them voluntarily attended an 8-week sleep hygiene and physiotherapy program. Evaluations were made using a Visual Analogue Scale (VAS), the Children’s Sleep Habits Questionnaire (CSHQ), and the Oral Habits Questionnaire (OHQ) at the beginning and at the end of the 8-week program.
RESULTS:
Statistically significant differences were determined between the 6–9 years and 10–13-year age groups in respect of the sleep habits subcategories of resistance to bedtime (
CONCLUSION:
There was no relationship between sleep bruxism and gender, but a relationship was found with age. The rate of bruxism was seen to decrease with an increase in age. It was determined that oral, sleep habits, and bruxism are closely related, and the rates at which bruxism is seen are affected by the oral habits. Sleep hygiene and physiotherapy have been effective in children with sleep bruxism.
1.Introduction
The relationship between temporomandibular disorder (TMD) and sleep bruxism has long been a subject of interest but has not yet been fully clarified. There are many risk factors forming and triggering TMDs, and although these remain a matter of current debate, the most important risk factor has been reported to be bruxism [1, 2]. Bruxism is defined as repetitive jaw-muscle activity characterized by clenching or grinding of the teeth and/or bracing or thrusting of the mandible with circadian manifestations [1]. This behavior in individuals has been associated with TMD, fatigue, pain in the face, head, and neck, sleep apnea, and reduced sleep quality [3, 4, 5].
Although bruxism is known to increase with stress, the etiology has not yet been fully explained, and the formation and pathogenesis of bruxism are thought to be multifactorial. Researchers have determined that dental, systemic, genetic, and psychological factors play a role in bruxism, but which of these factors is predominant is still under debate [6, 7]. The prevalence of bruxism in children has been reported to be in a wide range between 6% and 58% depending on different evaluations, and it has been shown to decrease in adolescence with increasing age [8, 9, 10]. It has been emphasized that sleep bruxism (SB) can cause pathological dental erosion, pain, and loss of function in the temporomandibular joint (TMJ) and chewing muscles, limitations in mandibular movement, and headaches and neck problems. Morning pain in the jaw and surrounding muscles, headache, fatigue, difficulty in waking up, and mood changes have been reported to be signs of sleep bruxism [4, 5, 6].
The inability to sleep and poor sleep quality in children can cause daytime fatigue, lack of attention, and poor academic performance [11]. Sleep is of great importance in the development of children. In addition to sleep being an important factor in physical and emotional development and behavior, links have been found to cognitive functions, learning, and attention. It is thought that insufficient sleep in childhood and adolescence, when the brain is developing, has a negative effect on various brain functions and structures. Negative outcomes such as daytime sleepiness, aggressiveness, behavioral problems, learning difficulties, and poor academic performance can be prevented with early identification of sleep problems [11, 12].
Previous research has emphasized that sleep habits can affect sleep quality [4, 5], and SB can lead to sleep respiratory problems [13]. Manfredini et al. stated that bruxism should not be thought of as a disorder, but as a behavior with clinical outcomes [8]. Some studies have been conducted related to the opinion that there could be a relationship between this parafunctional behavior and other oral parafunctional habits [14, 15, 16], and these habits have been reported to be a risk factor for the development of bruxism. Examples of oral parafunctional activities include mouth breathing, chewing the lips and inside of the cheeks, nail biting, chewing pens, and tongue thrusting. These oral habits in children can lay the ground for bruxism. According to the results of a study by Serra Negra et al., in which the relationship between SB and other parafunctional habits were examined, there was determined to be a relationship between SB and daytime teeth clenching, nail biting, pen chewing, and breathing through the mouth [5].
In the treatment of bruxism, it is necessary to eliminate the factors causing the disease. However, as the etiology is multifactorial, a single treatment option may not be sufficient. Therefore, the factors causing the key points of the disease must be determined for an effective, high-quality treatment. Diagnosis in the early stage and taking preventative steps is important for children to be able to avoid TMDs that may develop at a later age. When bruxism continues, TMD symptoms increase, thereby creating higher costs and the need for time-consuming treatments. Several treatment modalities for the treatment of SB have been explained in the literature, including pharmacological, psychological, and dental approaches [17, 18, 19, 20, 21]. Educating children and parents about bruxism, sleep, and oral habits and increasing awareness are essential in early-stage preventative rehabilitation. However, treatment approaches in this regard are seen to be lacking in the literature. There are no studies in the literature that evaluated education on sleep hygiene and therapeutic exercises on SB in children. Educational practices are an essential part of preventative treatment. Providing information about primarly bruxism parafunctional oral and sleep habits is vital in creating awareness in children and parents. Our aims of this study were to determine the gender and age distribution of oral habits and sleep habits of children with SB and to examine the effect of an physiotherapy program on SB, oral, and sleep habits.
2.Materials and methods
2.1Subjects
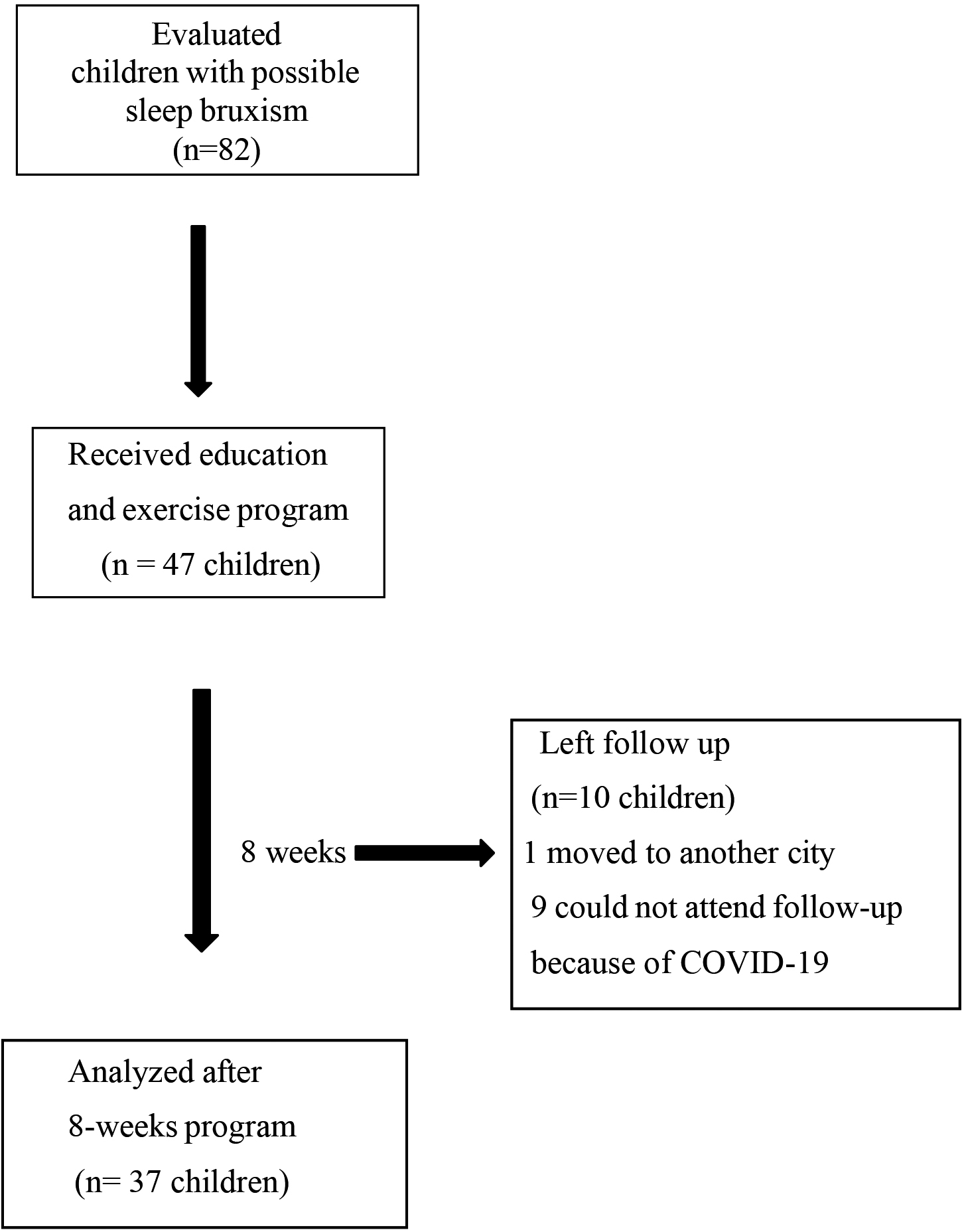
In this cross-sectional study, initial screening was made of 217 children at Cukurova University Clinics of Pediatric Dentistry, Adana, Turkey. 82 children aged 6–13 years diagnosed with SB were evaluated. Among those, a convenience sample of 37 children who agreed to volunteer attended and completed an 8-week education and therapeutic exercise program (Fig. 1).
Figure 1.
Study flow chart.
Approval for the study was granted by the Human Research Ethics Committee of Hasan Kalyoncu University, Turkey (protocol number: 2019/92). The study was registered on the WHO International Clinical Trials Registry Platform (NCT05323942). All procedures conform to the provisions of the Declaration of Helsinki. All children and their parents provided oral and written informed consent. The study was conducted between March 2020 and June 2021.
The study inclusion criteria were defined as age between 6 and 13 years, having a diagnosis of possible sleep bruxism (parental reported), and a signed parental informed consent form for participation in the study. Exclusion criteria were as follows: a history of TMJ surgery, ongoing maxillary orthopedic or orthodontic treatment, the presence of dentofacial anomalies, a medical history of neurological or psychiatric disease, received drugs and interventions and those who would receive them during the program, and inability to co-operate during the study.
2.2Methods
2.2.1Evaluation
Bruxism evaluation
Lobbezoo et al. proposed a system for grading bruxism assessments [1]. In our study, the international consensus on the assessment of bruxism was used in the evaluation of bruxism. The possible bruxism in the child was evaluated in detail through a face-to-face interview with the parents. The mothers of the children in the study were given information about the bruxism and were then asked, “During the past 3–6 months, have you noticed noises of your child clenching or grinding their teeth either when awake or at least 3–5 nights a week when sleeping?” The responses were recorded as parental-reported bruxism present or absent [1, 22].
In this cross-sectional study design, children with SB were recruited. To participate in this study, volunteers provided verbal consent to an oral examination, including dental impressions, and their guardians/parents provided oral and written consent. Of the 217 children, 135 were excluded from the study due to unsigned consent forms, or because they had ongoing maxillary orthopedic or orthodontic treatment or other exclusion criteria. Finally, the study group included 82 children with possible SB aged between 6 and 13 years. The evaluation was made by a pediatric dentist (I.Y). No dental treatment was offered or carried out as part of the invitation to participate.
Demographic information of the study participants was recorded. A TMJ examination was performed before and after the exercise program, and the children and parents were questioned about joint noises, crepitation, pain, and other symptoms. Information about the children was gathered through the application of the Oral Habits Questionnaire (OHQ) to the children, and the Children’s Sleep Habits Questionnaire (CSHQ) to the parents. The children received the education and home exercise program and were instructed to follow for 8 weeks by a physiotherapist (E.K). Throughout the 8-week program, a reminder message was sent once a week to the parents.
Pain evaluation
Pain severity was measured with a Visual Analog Scale (VAS) and the degree of pain was questioned in various circumstances. The children were instructed to mark the degree of pain felt on a scale marked from 0
![Sleep hygiene education [27, 28].](https://ip.ios.semcs.net:443/media/bmr/2023/36-5/bmr-36-5-bmr220235/bmr-36-bmr220235-g002.jpg)
![5x5 therapeutic exercise program [29].](https://ip.ios.semcs.net:443/media/bmr/2023/36-5/bmr-36-5-bmr220235/bmr-36-bmr220235-g003.jpg)
Evaluation of the Children’s Sleep Habits
The Children’s Sleep Habits Questionnaire (CSHQ) was used in this study. The original scale was developed by Owen et al. [24] to investigate the sleep habits of children and sleep-related problems. Validity and reliability studies of the Turkish version were conducted by Fiş et al. [25]. The CSHQ has satisfactory psychometric properties in children and has been used in previous investigations of sleep in children. The parents were given the necessary information about the questionnaire and were then instructed to complete it. The form has a total of 33 items in 8 subscales of resistance to bedtime, sleep latency, sleep duration, sleep anxiety, nocturnal waking, parasomnia, sleep respiratory disorder, and daytime sleepiness. A total of 41 points is accepted as the threshold and values above this are evaluated as “significant at a clinical level”, showing that the child experiences clinically significant sleep problems.
Evaluation of oral habits
The Oral Habits Questionnaire comprises 21 items with 5-point Likert-type responses of 4
2.2.2Education and physiotherapy
From the 82 children initially evaluated, 37 volunteer children received education about bruxism and parafunctional oral habits, sleep habits, sleep hygiene education [27, 28] (Fig. 2), and 5 x 5 therapeutic exercises [29] (Fig. 3). By explaining parafunctional oral habits individually, it was aimed to raise awareness in the children and their parents, and for the children to be conscious of these activities and not to perform them. In the OHQ, it was questioned whether or not they performed each of these oral parafunctional activities and how aware are of them they were. The parents were given education on the subject of sleep hygiene.
The therapeutic exercises given included diaphragmatic breathing training, relaxation, and head-neck stretching and strengthening exercises. The effects of the education were examined after the 8-week program. After ensuring that the children had learned the exercises correctly, an exercise brochure was given and the children were instructed to perform 5 repetitions of each exercise 5 times a day for 8 weeks. The parents were instructed to monitor the home program and a reminder message was sent once a week. Evaluations and measurements were made before and after the 8-week program.
2.3Statistical analysis
A total sample size of 34 was required to detect a moderate effect size (Cohen’s d
Table 1
Demographic characteristics of the children
| Minimum | Maximum |
| SD | |
| Evaluated children ( | ||||
| Age (years) | 6.00 | 13.00 | 9.22 | 1.80 |
| Height (cm) | 117.00 | 164.00 | 134.26 | 9.46 |
| Weight (kg) | 19.00 | 62.00 | 30.87 | 8.13 |
| BMI (kg/cm | 11.10 | 25.10 | 16.88 | 2.56 |
| Children who received exercise and education program ( | ||||
| Age (years) | 6.00 | 13.00 | 8.93 | 1.80 |
| Height (cm) | 117.00 | 164.00 | 133.72 | 10.02 |
| Weight (kg) | 19.00 | 62.00 | 29.22 | 8.25 |
| BMI (kg/cm | 11.10 | 23.10 | 16.11 | 2.63 |
X: mean; SD: standard deviation.
Table 2
Comparisons of the oral habits questionnaire and children’s sleep habits questionnaire values of the children according to the age groups
|
| Min | Max |
| SD |
|
| |
|---|---|---|---|---|---|---|---|
| OHQ | |||||||
| 6–9 years | 53 | 12.00 | 30.00 | 20.75 | 4.64 | 0.531 | |
| 10–13 years | 29 | 12.00 | 42.00 | 23.10 | 8.24 | ||
| CSHQ | |||||||
| 6–9 years | 53 | 37.00 | 65.00 | 47.26 | 7.42 | 0.313 | |
| 10–13 years | 29 | 34.00 | 60.00 | 45.07 | 6.72 | ||
| Bedtime resistance | |||||||
| 6–9 years | 53 | 6.00 | 17.00 | 9.70 | 2.98 |
0.001 | |
| 10–13 years | 29 | 6.00 | 12.00 | 7.59 | 1.97 | ||
| Sleep onset | |||||||
| 6–9 years | 53 | 1.00 | 2.00 | 1.21 | 0.41 | 0.822 | |
| 10–13 years | 29 | 1.00 | 3.00 | 1.24 | 0.58 | ||
| Sleep anxiety | |||||||
| 6–9 years | 53 | 4.00 | 12.00 | 6.62 | 2.08 |
0.043 | |
| 10–13 years | 29 | 4.00 | 10.00 | 5.69 | 1.81 | ||
| Sleep duration | |||||||
| 6–9 years | 53 | 3.00 | 7.00 | 3.64 | 1.08 | 0.885 | |
| 10–13 years | 29 | 3.00 | 8.00 | 3.72 | 1.28 | ||
| Night wakings | |||||||
| 6–9 years | 53 | 3.00 | 8.00 | 4.09 | 1.30 | 0.885 | |
| 10–13 years | 29 | 3.00 | 6.00 | 3.93 | 0.92 | ||
| Parasomnias | |||||||
| 6–9 years | 53 | 7.00 | 15.00 | 9.92 | 1.80 |
0.040 | |
| 10–13 years | 29 | 7.00 | 19.00 | 10.86 | 2.40 | ||
| Sleep disordered breathing | |||||||
| 6–9 years | 53 | 3.00 | 9.00 | 3.68 | 1.52 |
0.041 | |
| 10–13 years | 29 | 3.00 | 5.00 | 3.83 | 0.89 | ||
| Daytime sleepiness | |||||||
| 6–9 years | 53 | 7.00 | 22.00 | 11.91 | 3.00 | 0.112 | |
| 10–13 years | 29 | 6.00 | 22.00 | 10.90 | 3.50 |
Table 3
Comparisons of the oral habits questionnaire and children’s sleep habits questionnaire values of the children according to gender
|
| Min | Max |
| SD |
|
| |
|---|---|---|---|---|---|---|---|
| OHQ | |||||||
| Female | 38 | 13.00 | 35.00 | 21.63 | 5.56 | 0.665 | |
| Male | 44 | 12.00 | 42.00 | 21.55 | 6.79 | ||
| CCSHQ | |||||||
| Female | 38 | 36.00 | 65.00 | 46.13 | 8.09 | 0.326 | |
| Male | 44 | 34.00 | 62.00 | 46.80 | 6.44 | ||
| Bedtime resistance | |||||||
| Female | 38 | 6.00 | 13.00 | 8.74 | 2.45 | 0.825 | |
| Male | 44 | 6.00 | 17.00 | 9.14 | 3.16 | ||
| Sleep onset | |||||||
| Female | 38 | 1.00 | 3.00 | 1.13 | 0.41 | 0.066 | |
| Male | 44 | 1.00 | 3.00 | 1.30 | 0.51 | ||
| Sleep anxiety | |||||||
| Female | 38 | 4.00 | 12.00 | 6.13 | 2.24 | 0.276 | |
| Male | 44 | 4.00 | 10.00 | 6.43 | 1.84 | ||
| Sleep duration | |||||||
| Female | 38 | 3.00 | 8.00 | 3.47 | 0.95 | 0.150 | |
| Male | 44 | 3.00 | 8.00 | 3.84 | 1.27 | ||
| Night wakings | |||||||
| Female | 38 | 3.00 | 6.00 | 4.11 | 1.11 | 0.438 | |
| Male | 44 | 3.00 | 8.00 | 3.98 | 1.25 | ||
| Parasomnias | |||||||
| Female | 38 | 7.00 | 19.00 | 10.29 | 2.47 | 0.733 | |
| Male | 44 | 7.00 | 15.00 | 10.23 | 1.67 | ||
| Sleep disordered breathing | |||||||
| Female | 38 | 3.00 | 8.00 | 3.55 | 1.22 | 0.104 | |
| Male | 44 | 3.00 | 9.00 | 3.89 | 1.40 | ||
| Daytime sleepiness | |||||||
| Female | 38 | 7.00 | 22.00 | 11.95 | 3.38 | 0.483 | |
| Male | 44 | 6.00 | 17.00 | 11.20 | 3.03 |
Table 4
Comparisons of the pain severity values before and after the education program
| VAS (0–10 cm) |
| Min | Max |
| SD |
|
| |
|---|---|---|---|---|---|---|---|---|
| Headache on waking in the morning | BE | 37 | 0.00 | 4.00 | 0.36 | 0.97 |
0.027 | |
| AE | 37 | 0.00 | 3.00 | 0.19 | 0.67 | |||
| Jaw pain on waking in the morning | BE | 37 | 0.00 | 8.00 | 0.85 | 1.94 |
0.027 | |
| AE | 37 | 0.00 | 5.00 | 0.50 | 1.26 | |||
| Jaw pain when eating | BE | 37 | 0.00 | 5.00 | 0.70 | 1.45 |
0.026 | |
| AE | 37 | 0.00 | 3.00 | 0.39 | 0.88 | |||
| Jaw pain after eating | BE | 37 | 0.00 | 4.50 | 0.31 | 1.00 | 0.180 | |
| AE | 37 | 0.00 | 3.00 | 0.22 | 0.67 | |||
| Jaw pain before going to sleep at night | BE | 37 | 0.00 | 5.00 | 0.61 | 1.24 |
0.007 | |
| AE | 37 | 0.00 | 2.50 | 0.28 | 0.65 |
Table 5
Comparisons of the oral habits questionnaire and children’s sleep habits questionnaire values of the children before and after the education program
|
| Min | Max |
| SD |
|
| ||
|---|---|---|---|---|---|---|---|---|
| OHQ | BE | 37 | 12.00 | 40.00 | 22.14 | 6.42 | 5.595 |
0.000 |
| AE | 37 | 11.00 | 36.00 | 19.76 | 5.65 | |||
| CSHQ | BE | 37 | 34.00 | 65.00 | 47.35 | 7.03 | 0.405 | |
| AE | 37 | 35.00 | 68.00 | 47.11 | 7.61 | |||
| Bedtime resistance | BE | 37 | 6.00 | 17.00 | 9.22 | 2.91 |
0.001 | |
| AE | 37 | 6.00 | 16.00 | 8.73 | 2.62 | |||
| Sleep onset | BE | 37 | 1.00 | 3.00 | 1.24 | 0.49 | 0.157 | |
| AE | 37 | 1.00 | 2.00 | 1.19 | 0.40 | |||
| Sleep anxiety | BE | 37 | 4.00 | 12.00 | 6.46 | 2.05 | 0.655 | |
| AE | 37 | 4.00 | 12.00 | 6.49 | 2.06 | |||
| Sleep duration | BE | 37 | 3.00 | 8.00 | 3.78 | 1.25 |
0.008 | |
| AE | 37 | 3.00 | 8.00 | 3.59 | 1.07 | |||
| Night wakings | BE | 37 | 3.00 | 8.00 | 4.14 | 1.21 | 0.157 | |
| AE | 37 | 3.00 | 8.00 | 4.08 | 1.14 | |||
| Parasomnias | BE | 37 | 7.00 | 19.00 | 10.43 | 2.35 |
0.000 | |
| AE | 37 | 7.00 | 18.00 | 11.49 | 2.02 | |||
| Sleep disordered breathing | BE | 37 | 3.00 | 9.00 | 3.78 | 1.38 | 0.317 | |
| AE | 37 | 3.00 | 9.00 | 3.76 | 1.36 | |||
| Daytime sleepiness | BE | 37 | 6.00 | 22.00 | 11.38 | 3.36 | 0.000 | 1.000 |
| AE | 37 | 6.00 | 22.00 | 11.38 | 3.41 |
Mean; SD: standard deviation;
3.Results
From the initial screening of 217 children aged 6–13 years, 82 with SB were identified (37.8% SB). The demographic variables of the 82 children with SB first evaluated (44 males, 38 females). Among those, 37 children (19 males, 18 females) who received the education program are shown in Table 1. Mouth breathing was determined in 3 children, the presence of an allergy in 15 children, and the presence of primary dentition in 71 children. Among children having SB reported by the parents, ringing in the ears in 6.1%, earache in 3.7%, dizziness in 1.2%, headache in 9.8%, facial pain in 2.4%, difficulty swallowing in 3.7%, and neck pain in 1.2% were determined. According to the parental reports following the education and exercise program, SB was not seen in 7 children but continued in 30 children. A reduction of approximately 20% in SB was obtained following the 8-week education and exercise program.
The comparisons of the oral and sleep habits of the 82 children according to the age groups of 6–9 years and 10–13 years are shown in Table 2. A statistically significant difference was determined between the 6–9 years and 10–13 years age groups in respect of the CSHQ subcategories of resistance to bedtime 95% CI: mean (min-max) 9.70 (6.00–17.00) to 7.59 (6.00–12.00),
No statistically significant difference was determined between the children according to gender in respect of the OHQ, CSHQ, and subscale mean points (
The comparisons of the OHQ and CSHQ values of the children before and after the 8-week program are shown in Table 5. A statistically significant decrease was determined in OHQ, 95% CI: mean (min-max) 22.14 (12.00–40.00), to 19.76 (11.00–36.00),
4.Discussion
There are few studies in the literature that have shown a relationship between therapeutic exercises and bruxism [35, 36]. However, there are still no guidelines for the treatment of bruxism in children and adolescents, and the need for multidisciplinary approaches has been emphasized [6, 10, 31]. In this study, the effects of children’s sleep and oral habits on sleep bruxism as well as an 8-week education and exercise program were evaluated to establish subsequent protective and preventative approaches. Of 82 children initially evaluated, 37 children and their parents volunteered to receive education about bruxism, parafunctional oral and sleep habits, and sleep hygiene and then received an exercise program. The children were shown how to perform the therapeutic exercises. Parafunctional oral habits were explained separately to create awareness in the children and parents, and the children were instructed to be conscious of these activities and not to engage in these habits. At the end of the 8-week program, a close relationship between oral and sleep habits and sleep bruxism was determined.
The prevalence of bruxism seen in children has a very wide range in literature because of the differences in evaluation methods [7, 8, 9, 19]. SB in children was determined at the rate of 38% in this study and 32% in a previous prevalence study in Turkey [32]. It was thought that the higher rate in the current study could have been due to the effect of conducting the study during the COVID-19 pandemic.
Although previous studies in the literature have shown bruxism at equal rates in both genders [8, 13], it has also been stated that girls aged 3–7 years are more predisposed to bruxism than boys [14]. Results in the literature on this subject differ greatly. In the current study, bruxism was observed more in boys (54%) than girls (46%), but no difference was determined between the genders in respect of oral habits and sleep habits.
It has been reported that SB is seen at higher rates in childhood and the prevalence decreases together with age in adolescence [8, 22, 33]. The high prevalence of bruxism in childhood has been suggested to be due to tighter control of younger children by parents and therefore, the prevalence is affected by the parents noticing SB [22]. Most studies have recorded the presence of bruxism according to reports taken from parents and this has been defined as possible SB [22, 32]. In parallel with findings in the literature, the possible SB rate in the current study was seen to decrease together with aging. Of the 82 children with SB, 53 (65%) were in the 6–9 years age group and 29 (35%) in the 10–13 years age group. Although the reliability of parental reports is discussed in the literature, parents are an important source for the collection of findings in children. It is also thought that as the parents notice the regularity of sleep and sleep problems and bruxism, there is increased awareness of SB and its effects.
The etiology of SB is multifactorial, and several treatment modalities have been described, including pharmacological, psychological, and dental approaches [20, 31, 32, 33, 34]. For the treatment of bruxism in adults, stretching exercises, electrotherapy, massage, muscle relaxation, and manual therapies have been used as physiotherapeutic approaches [21, 30, 35, 37]. Several non-invasive methods are applied for the treatment of bruxism in children, including oral appliances, biofeedback, cognitive-behavioral approaches, and pharmacological approaches [17, 18, 19, 20, 33]. Although discussions and different approaches are ongoing in the treatment of SB in children, the approach that has come to prominence is that it must be considered that the maxillary structures are at the growth and development stage in every intervention applied [19]. It has also been reported that physiological wear in the teeth is required for the development of the jaw structure in children aged 3–5 years [38]. The approach taken to other treatments considers the fact that the rate of bruxism decreases with increasing age, and adults do not perform these activities [8, 22, 38]. It has been recommended that researchers follow up on the signs and symptoms of bruxism, such as tooth wear, craniofacial pain, headache, and TMD or restricted mouth opening [6, 20]. The collaboration of the child, parents, and clinician has been emphasized as important in the treatment of bruxism in children and adolescents. Therefore, increasing children’s and parents’ awareness is a critical approach to establishing collaboration. Learning about parafunctional oral habits, being aware of these, and awareness of and avoiding incorrect postural behavior in daily activities and when lying in bed is an important stage. Behavioral strategies include biofeedback, relaxation, and sleep hygiene [27, 28, 29]. Sleep hygiene precautions include ensuring that the bedroom is quiet and well-ventilated, that the child is relaxed before going to bed, and that fluid intake is avoided before bedtime [27, 28]. These precautions aim to reduce the effect of mental stress on SB.
In a previous study of 54 university students, the 5 x 5 therapeutic exercises used in the current study were effective on the head and neck posture, increased sleep quality, and reduced neck disability and fatigue [29]. Educational practices are an important part of preventative treatment. In the current study, the 37 children with SB who volunteered to participate in the education and 5 x 5 therapeutic exercises were taught how to apply these exercises and received sleep hygiene education. According to the parental report, after the 8-week program, 7 children no longer had SB, and SB persisted in 30 children. This showed a decrease of approximately 20% in a period of 2 months.
Pain severity
Although myofascial, jaw, and facial pain have been suggested to be triggering or maintaining factors of bruxism, the fundamental role of these is not known [1, 2, 3]. Length and frequent contractions in the chewing muscles, which trigger pain, bruxism, and clenching and/or grinding of the teeth, which are among the mechanically accelerating factors of bruxism, are known to cause pain [10]. Bruxism is generally first reflected clinically as pain associated with chewing muscle irregularities. Baad-Hansen et al. [3] reported that there could be a relationship between bruxism and musculoskeletal system problems, while Andreucci et al. [39] stated that the development of musculoskeletal problems in children and adolescents was a risk factor for sleep problems. Serra-Negra et al. reported that in the relationship between SB and sleep, there was a 19-fold greater possibility of SB in children with pain in the mouth region [40]. In the current study, the highest pain severity was found to be jaw pain upon waking in the morning. Worse pain in the mornings in the chewing muscles and/or the TMJ suggests SB as the etiology of the pain. Following the 8-week education and therapeutic exercise program, a significant decrease in the pain values of the children was determined. Comparing the VAS values before and after the education program, a significant decrease in the points of headache on waking, jaw pain on waking, jaw pain when eating, and jaw pain when going to bed was observed. The significant decrease in headache and jaw pain on waking in the mornings indicates a decrease in SB. It was seen that regularly applied exercises and attention to sleep hygiene before going to bed were effective approaches in lowering the pain severity values of the children. The combination of the program of breathing, relaxation, stretching, and strengthening exercises for the jaw and neck muscles with behavioral therapy in this study can be considered important in this respect.
Sleep habits
In previous studies, it has been emphasized that sleep habits affect sleep quality [4, 5, 11], and respiratory disorders in sleep are risk factors for bruxism [13]. Snoring, mouth breathing, restless sleep, drooling, lying prone, and insufficient duration of sleep have been found to be associated with bruxism in children [4]. In a study of 496 children by Ferreira et al. [13], SB was determined at the rate of 25.6%, and obstructive sleep apnea (OSA) was diagnosed in 4.83%. A significant correlation was found between children with SB and OSA. In a recent study, which examined the relationship between sleep disorders and SB, sleep disorders were determined in 61.4% of 160 children with SB [32]. Children with SB were found to have 3-fold worse sleep quality [7]. It was also reported that there was a tendency to release tension accumulated during the day through bruxism when asleep. Children who snore or have nightmares have been found to have a greater probability of developing SB [3, 4] and thus it has been reported that some sleep quality characteristics can serve as signs for the early diagnosis of bruxism by parents and healthcare specialists, and thereby the negative outcomes can be reduced.
SB treatment for children generally starts with patient education related to sleep hygiene. This includes providing good conditions in the bedroom and restricting eating, drinking, and physical activity before going to bed. In a study that combined relaxation techniques with sleep hygiene precautions for 4 weeks, it was determined that although no significant differences were found [41], it may be important in clinical practice to recommend sleep hygiene with other approaches to sleep habits for the prevention of SB [9, 27, 28].
As a result of the evaluations in the current study, it was determined that the mean total CSHQ values of both age groups and both genders were above 41, which is accepted as significant at a clinical level [24]. This finding showed that the vast majority of the children, irrespective of age and gender, experienced sleep problems at a clinically significant level. In the CSHQ subscales, the mean resistance to bedtime, sleep anxiety, and sleep respiratory disorder values were found to be higher in the 6–9 years age group, and the parasomnia values were higher in the 10–13 years age group. When the effect of the 8-week program of education and therapeutic exercises was evaluated after the program, there was found to be a significant decrease in the resistance to bedtime values and a significant increase in the sleep duration values.
The results of the current study showed that after education, SB was eliminated in approximately one in five children. Parents were taught as much as the children about sleep hygiene. The education of the children and parents and increasing their awareness of sleep habits were thought to be related to the decrease in bruxism. However, there was seen to be a need for longer-term and more comprehensive education programs to be given about sleep habits.
Oral habits
Examples of oral parafunctional habits include mouth breathing, chewing the lips and inside of the cheeks, long-term use of a pacifier, and tongue thrusting. Previous studies have shown that there could be a relationship between oral habits and bruxism, and parafunctional oral habits have been reported to be a risk factor for the development of bruxism [14, 15, 16].
Lamenha Lins [15] stated that SB was seen 2.71-fold more in children who breathed through their mouth, and Yazıcıoğlu [16] reported that bruxism with sleeping with the mouth open was a risk factor for TMD. Serra-Negra examined the relationship between SB and other parafunctional oral habits in Brazilian children, and the results of that study showed that SB was associated with daytime teeth clenching, nail biting, pen chewing, and mouth breathing [5], and in another study, a high level of stress and responsibility was reported to be among the key factors in the development of SB in children [40].
Consistent with the findings in the literature, a significant association was determined in the current study between SB and the oral habits of the children. No differences were determined in the oral habits according to age and gender. There was found to be a statistically significant decrease in the oral habits of the children following the 8-week education program compared to before the program. The change of OHQ value of 22.14 before the program to 19.76 after the program was found to be statistically significant. The decrease in oral habits was seen to be effective on bruxism activity. When the presence of a relationship between SB and oral parafunction and sleep behaviors is considered, interventions for the elimination of these types of behaviors are vital. In the current study, the attention of the children included in the education and exercise program was drawn to parafunctional oral, tongue, and lip habits and posture in daily living activities, and they were educated on following routine bedtime programs and awareness of these elements. Through individual interviews with the parents, they were requested to remind, help, and monitor the children throughout the 8-week program.
There were limitations to this study, primarily that there was no control group of children with TMD and no bruxism to compare with the children with bruxism. A questionnaire-based assessment was used to evaluate parafunctional activities, and there could have been recalling bias from the parents. In addition, as the study was conducted during the COVID-19 pandemic, it was thought that the sleep habits of the children could have been affected by the quarantine restrictions on social life and the disruptions to schooling with home education. Moreover, as it was not feasible to ask parents to bring the children for follow-up during this period or for reasons such as having moved away from the city, only children who volunteered and were able to attend at the end of the program were included in the education and exercise program, and thus the study was completed with 37 children at the end of the 8-week period. There is a need for further studies with a control group and longer educational sessions. Despite these limitations, it was observed that the sleep hygiene and parafunctional activity training and exercise program given to the children provided a positive change in their oral and sleep habits. It was determined that the pain severity values of the children decreased significantly after the training program. The results of our study in a restrictive period such as the pandemic made this study strong. The strengths of this study recommend consideration of the education and exercise programs during a similar pandemic condition and/or access to care issues at the clinics arise.
Providing information about bruxism and other parafunctional oral and sleep habits is vital in creating awareness in children and parents. Sleep hygiene education and therapeutic exercises should be integrated with the treatment approaches recommended in the literature for children with bruxism. In patient care management, education and exercise programs may provide close interactions with the patients resulting in an increase in patients’ awareness of their health and oral health-related quality of life.
5.Conclusion
The results of the study demonstrated that there was no relationship between SB and gender, but a relationship was found with age. The rate of bruxism was seen to decrease with an increase in age. The resistance to bedtime, sleep anxiety and sleep respiratory disorder values were found to be higher in the 6–9 years age group, and parasomnia values were higher in the 10–13 years age group. It was determined that oral and sleep habits and bruxism are closely related, and the rates at which bruxism is seen are affected by oral habits. 8-week education and physiotherapy program increased the parents’ and children’s awareness of SB, oral, and sleep habits.
In the future, we recommend a randomized controlled trial for longer-term and more comprehensive programs with a control group to prove the efficacy of education and exercises in children with bruxism.
Funding
The authors did not receive any financial support for this study.
Author contributions
All listed authors made valuable contributions to the development of this manuscript. Conception and design: AT; Collection and assembly of data: EK; Analysis and interpretation of the data: AT; Drafting of the article: AT, IY; Critical revision of the article for important intellectual content: AHT; Final edition of the manuscript: AT, İY.
Acknowledgments
The authors would like to thank the children and their parents who participated in the study. Additional thanks to Çukurova University Clinic of Pediatric Dentistry.
Conflict of interest
The authors declare that they have no conflict of interest that pertain to this work.
References
[1] | Lobbezoo F, Ahlberg J, Raphael KG, et al. International consensus on the assessment of bruxism: Report of a work in progress. J Oral Rehabil. (2018) Nov; 45: (11): 837-844. doi: 10.1111/joor.12663. |
[2] | de Oliveira Reis L, Ribeiro RA, Martins CC, et al. Association between bruxism and temporomandibular disorders in children: A systematic review and metaanalysis. Int J Paediatr Dent. (2019) ; 29: (5): 585–595.ipd.12496. doi: 10.1111/ipd.12496. |
[3] | Baad-Hansen L, Thymi M, Lobbezoo F, et al. To what extent is bruxism associated with musculoskeletal signs and symptoms? A systematic review. J Oral Rehabil. (2019) ; 46: (9): 845-861. doi: 10.1111/joor.12821. |
[4] | Guo H, Wang T, Li X, et al. What sleep behaviors are associated with bruxism in children? A systematic review and meta-analysis. Sleep Breath. (2017) ; 21: (4): 1013-1023. doi: 10.1007/s11325-017-1496-3. |
[5] | Serra-Negra JM, Ribeiro MB, Prado IM, et al. Association between possible sleep bruxism and sleep characteristics in children. Cranio. (2017) ; 35: (5): 315-320. doi: 10.1080/08869634.2016.1239894. |
[6] | Bulanda S, Ilczuk-Rypuła D, Nitecka-Buchta A, et al. Sleep Bruxism in Children: Etiology, Diagnosis, and Treatment-A Literature Review. Int J Environ Res Public Health. (2021) ; 10: (18): 9544. doi: 10.3390/ijerph18189544. |
[7] | Gomes MC, Neves ET, Perazzo MF, et al. Evaluation of the association of bruxism, psychosocial and sociodemographic factors in preschoolers. Braz Oral Res. (2018) ; 32: : e009. doi: 10.1590/1807-3107bor-2018.vol32.0009. |
[8] | Manfredini D, Restrepo C, Diaz-Serrano K, et al. Prevalence of sleep bruxism in children: A systematic review of the literature. J Oral Rehabil. (2013) ; 40: (8): 631-642. doi: 10.1111/joor.12069. |
[9] | Leal TR, de Lima LCM, Perazzo MF, et al. Influence of the practice of sports, sleep disorders, and habits on probable sleep bruxism in children with mixed dentition. Oral Dis. (2021) ; 10.1111/odi.13917. doi: 10.1111/odi.13917. |
[10] | Christidis N, Lindström Ndanshau E, Sandberg A, et al. Prevalence and treatment strategies regarding temporomandibular disorders in children and adolescents-A systematic review. J Oral Rehabil. (2019) ; 46: (3): 291-301. doi: 10.1111/joor.12759. |
[11] | Herrera M, Valencia I, Grant M, et al. Bruxism in children: Effect on sleep architecture and daytime cognitive performance and behavior. Sleep. (2006) ; 29: (9): 1143-1148. doi: 10.1093/sleep/29.9.1143. |
[12] | Massignan C, de Alencar NA, Soares JP, et al. Poor sleep quality and prevalence of probable sleep bruxism in primary and mixed dentitions: A cross-sectional study. Sleep Breath. (2019) ; 23: (3): 935-941. doi: 10.1007/s11325-018-1771-y. |
[13] | Ferreira NMR, Dos Santos JFF, Dos Santos MBF, et al. Sleep bruxism associated with obstructive sleep apnea syndrome in children. Cranio. (2015) ; 33: (4): 251-255. doi: 10.1179/2151090314Y.0000000025. |
[14] | Tosato JP, Biasotto-Gonzalez DA. Symptomatology of the temporomandibular dysfunction related to parafunctional habits in children. Braz J Oral Sci. (2005) ; 4: (14): 787-790. |
[15] | Lamenha Lins RM, Cavalcanti Campêlo MC, Mello Figueiredo L, et al. Probable sleep bruxism in children and its relationship with harmful oral habits, type of crossbite and oral breathing. J Clin Pediatr Dent. (2020) ; 44: (1): 66-69. doi: 10.17796/1053-4625-44.1.12. |
[16] | Yazıcıoğlu İ, Çiftçi V. Evaluation of signs and symptoms of temporomandibular disorders and incisal relationships among 7-10-year-old Turkish children with sleep bruxism: A cross-sectional study [published online ahead of print, 2021 Jun 26]. Cranio. (2021) ; 1-7. doi: 10.1080/08869634.2021.1939932. |
[17] | Tavares-Silva C, Holandino C, Homsani F, et al. Homeopathic medicine of Melissa officinalis combined or not with Phytolacca decandra in the treatment of possible sleep bruxism in children: A crossover randomized triple-blinded controlled clinical trial. Phytomedicine. (2019) ; 58: : 152869. doi: 10.1016/j.phymed.2019.152869. |
[18] | Mostafavi SM, Jafari A, Hoseini SG, et al. The efficacy of low and moderate dosage of diazepam on sleep bruxism in children: A randomized placebo-controlled clinical trial. J Res Med Sci. (2019) ; 24-28. doi: 10.4103/jrms.JRMS_131_18. |
[19] | Chisini LA, San Martin AS, Cademartori MG, et al. Interventions to reduce bruxism in children and adolescents: A systematic scoping review and critical reflection. Eur J Pediatr. (2020) ; 179: (2): 177-189. doi: 10.1007/s00431-019-03549-8. |
[20] | lerardo G, Mazur M, Luzzi V, et al. Treatments of sleep bruxism in children: A systematic review and meta-analysis. Cranio. (2021) ; 39: (1): 58-64. doi: 10.1080/08869634.2019.1581470. |
[21] | Damar Örenler S, Tuncer A, Najafov E. A comparison of manual therapy and splint therapy in patients diagnosed with myofascial temporomandibular dysfunction with sleep bruxism. Turk J Physiother Rehabil. (2022) ; 33: (2): 89-97. doi: tjpr1027272. |
[22] | Bulanda S, Ilczuk-Rypuła D, Nitecka-Buchta A, et al. Sleep Bruxism in Children: Etiology, Diagnosis, and Treatment-A Literature Review. Int J Environ Res Public Health. (2021) Sep 10; 18: (18): 9544. doi: 10.3390/ijerph18189544. |
[23] | Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement of acute pain. Acad Emerg Med. (2001) ; 8: (12): 1153-7. doi: 10.1111/j.1553-2712.2001.tb01132.x. |
[24] | Owens JA, Spirito A, McGuinn M. The Children’s. Sleep Habits Questionnaire (CSHQ): Psychometric properties of a survey instrument for school-aged children. Sleep. (2000) ; 23: (8): 1043-1051. |
[25] | Fiş PN, Arman A, Ay P, et al. The validity and the reliability of Turkish version of Children’s Sleep Habits Questionnaire. Anatolian J Psychiatry. (2010) ; 11: : 151-160. |
[26] | Markiewicz MR, Ohrbach R, McCall Jr W. Oral behaviors checklist: reliability of performance in targeted waking-state behaviors. J Orofac Pain. (2006) ; 20: (4): 306-316. |
[27] | Hall WA, Nethery E. What does sleep hygiene have to offer children’s sleep problems? Paediatr Respir Rev. (2019) ; 31: : 64-74. doi: 10.1016/j.prrv.2018.10.005. |
[28] | Tan E, Healey D, Gray AR, et al. Sleep hygiene intervention for youth aged 10 to 18 years with problematic sleep: A before-after pilot study. BMC Pediatr. (2012) ; 12: : 189. doi: 10.1186/1471-2431-12-189. |
[29] | Tuncer A, Maden T, Badat T, et al. The effects of 5x5 exercises on a quality of life of university students, who use smartphones during long periods. Physical Education of Students. (2020) ; 24: (5): 271-277. doi: 10.15561/20755279.2020.003. |
[30] | Gouw S, de Wijer A, Kalaykova SI, et al. Masticatory muscle stretching for the management of sleep bruxism: A randomised controlled trial. J Oral Rehabil. (2018) ; 45: (10): 770-776. doi: 10.1111/joor.12694. |
[31] | Ferrillo M, Ammendolia A, Paduano S, et al. Efficacy of rehabilitation on reducing pain in muscle-related temporomandibular disorders: A systematic review and meta-analysis of randomized controlled trials [published online ahead of print, 2022 Feb 18]. J Back Musculoskelet Rehabil. (2022) ; 10.3233/BMR-210236. doi: 10.3233/BMR-210236. |
[32] | Us MC, Us YO. Evaluation of the relationship between sleep bruxism and sleeping habits in school-aged children [published online ahead of print, 2021 Feb 21]. Cranio. (2021) ; 1-9. doi: 10.1080/08869634.2021.1890454. |
[33] | Casazza E, Giraudeau A, Payet A, et al. Management of idiopathic sleep bruxism in children and adolescents: A systematic review of the literature. Arch Pediatr. (2022) ; 29: (1): 12-20. doi: 10.1016/j.arcped.2021.11.014. |
[34] | Coskun Benlidayi I, Salimov F, Kurkcu M, Guzel R. Kinesio Taping for temporomandibular disorders: Single-blind, randomized, controlled trial of effectiveness. J Back Musculoskelet Rehabil. (2016) ; 29: (2): 373-380. doi: 10.3233/BMR-160683. |
[35] | Amorim CSM, Espirito Santo AS, Sommer M, et al. Effect of physical therapy in bruxism treatment: A systematic review. J Manipulative Physiol Ther. (2018) ; 41: (5): 389-404. doi: 10.1016/j.jmpt.2017.10.014. PMID: 30041736. |
[36] | Makino I, Arai YC, Aono S, et al. The effects of exercise therapy for the improvement of jaw movement and psychological intervention to reduce parafunctional activities on chronic pain in the craniocervical region. Pain Pract. (2014) ; 14: (5): 413-8. doi: 10.1111/papr.12075. |
[37] | Gomes CAFP, El-Hage Y, Amaral AP, et al. Effects of Massage Therapy and Occlusal Splint Usage on Quality of Life and Pain in Individuals with Sleep Bruxism: A Randomized Controlled Trial. J Jpn Phys Ther Assoc. (2015) ; 18: (1): 1-6. doi: 10.1298/jjpta.Vol18_001. |
[38] | Firmani M, Reyes M, Becerra N, et al. Bruxismo de sueño en niños y adolescentes [Sleep bruxism in children and adolescents]. Rev Chil Pediatr. (2015) ; 86: (5): 373-379. doi: 10.1016/j.rchipe.2015.05.001. |
[39] | Andreucci MSc A, Campbell P, Dunn KM. Are Sleep Problems a Risk Factor for the Onset of Musculoskeletal Pain in Children and Adolescents? A Systematic Review. Sleep. (2017) ; 40: (7): 10.1093/sleep/zsx093. doi: 10.1093/sleep/zsx093. |
[40] | Serra-Negra JM, Paiva SM, Flores-Mendoza CE, et al. Association among stress, personality traits, and sleep bruxism in children. Pediatr Dent. (2012) ; 34: (2): e30-4. PMID: 22583874. |
[41] | Valiente López M, van Selms MK, van der Zaag J, et al. Do sleep hygiene measures and progressive muscle relaxation influence sleep bruxism? Report of a randomised controlled trial. J Oral Rehabil. (2015) ; 42: (4): 259-265. doi: 10.1111/joor.12252. |


