
High-intensity laser therapy on pain relief in symptomatic knee osteoarthritis: A systematic review and meta-analysis
Abstract
BACKGROUND:
Osteoarthritis is one of the leading causes of global disability and pain.
OBJECTIVE:
To investigate whether High-Intensity Laser therapy has superior pain-relieving effects in individuals with symptomatic knee osteoarthritis.
METHODS:
Searches were conducted using CENTRAL, MEDLINE, CINAHL, EMBASE, Web of Science, PEDro, and related reference lists with language limed to English. Clinical trials investigating the effectiveness of High-Intensity Laser therapy compared to other laser therapies, conventional therapies or exercises on knee osteoarthritis pain were included. The screening and selection of studies, data extraction, and methodological quality assessment were performed by two independent researchers. Studies were quantitatively integrated using the Review Manager Software and qualitative analysis using the criteria recommended by the Cochrane Collaboration.
RESULTS:
Nine studies meeting the eligibility criteria were identified, among which only one study was identified as excellent methodology quality, six was marked as good quality, and the remaining two studies were regarded as fair or poor quality. All studies reported positive effects of High-Intensity Laser therapy on knee osteoarthritis pain. Two studies (136 people) gave indication that there was moderate evidence that High-Intensity Laser therapy could be a promising new possibility in pain relief among patients with knee osteoarthritis compared with sham laser therapy in a short-term treatment (MD,
CONCLUSION:
High-Intensity Laser therapy could be a promising and recommended modality in alleviating knee osteoarthritis pain, especially when it was implemented in combination with exercises.
1.Introduction
Osteoarthritis is one of the leading causes of global disability and pain [1, 2, 3, 4] and a key symptom of individuals seeking medical care [5, 6] and absenteeism [7, 8] worldwide, especially in an aging [9, 10] and predisposing obese group [11, 12]. Knee osteoarthritis (KOA) is the most common form of osteoarthritis [13], accounting for more than four-fifths overall burden of the disease [14], characterized by structural alternations of the hyaline articular cartilage, subchondral bone, ligaments, capsule, and synovium [2].
Globally, the prevalence of symptomatic KOA was estimated to be 3.8% compared to hip osteoarthritis (0.85%) in 2010, peaking at around 50 years of age [1]. Statistically, knee and hip osteoarthritis were ranked as the 11
There is a wide spectrum of factors associated with KOA, including age [16, 17], gender [2, 6], obesity [11, 12], genetics [18], previous knee trauma [19], BMI [11, 12], knee malalignment [20], and quadriceps muscle strength [21]. Consequently, management of these predisposed or highly risk factor seems to be highly essential, however, among which some features cannot be reversed or ameliorated in a short term, like age, gene, sex, distorted cartilage, or ligaments degeneration. Considering this, attention should be paid to the patient’s pain relief or risk prevention such as balance issues and falls caused by KOA, particularly when pain extremely affects ambulation and sleeping [22].
Clinically, education, individual-specific exercise therapy (ET) as well as weight-loss are identified to be the first-line treatment in the long-term exercise protocol [23]. Nonetheless, therapeutic intensity and its effectiveness possibly be affected as pain initials drastically and the long-term adherence to ET and negative belief in patients with KOA are also barriers [24, 25, 26]. Therefore, the management of pain related to KOA is indispensable.
High-Intensity Laser therapy (HILT), is a promising option of treatment modality, which can penetrate deeper tissues (up to 100 mm) [27, 28] than other laser therapies, playing a role in intraarticular of the knee, and being regarded as a noninvasive, safe, and effective method to treat pain. Previous studies demonstrated that HILT is effective in the management of Patellofemoral Pain Syndrome [29], subacromial syndrome [30], and low back pain [31], mainly because of its accelerating connective tissue repair, affecting fibroblast function, releasing of anti-inflammatory and endogenous mediators [32], as well as stimulating deeper soft tissue metabolism [33]. Recently, several studies utilizing varied protocols, were conducted to investigate the effectiveness of HILT in individuals with KOA. A similar meta-analysis published in 2020 by Hyun-Jin Song [34] did not divide the control group into separate groups and directly integrated quantitatively, which may exaggerate or reduce the effect of HILT on KOA pain. Consequently, the purpose of this study was to update the review related to the effectiveness of HILT on pain in individuals with KOA based on the types of the control group and provides recommendations on the decision-making process of managing KOA pain when choosing laser therapy or other physiotherapies.
2.Methods
2.1Protocol and registration
This study was conducted based on PRISMA [35] (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) statement and registered in PROSPERO (Registration Number: CRD42020175318).
Table 1
Level of evidence
| Level of evidence | Indications |
|---|---|
| Strong evidence | Consistent findings among multiple higher-quality RCTs |
| Moderate evidence | Consistent findings among multiple lower quality RCTs and/or one higher quality RCT |
| Conflicting evidence | One lower quality RCT |
| No evidence | No RCTs |
2.2Eligibility criteria
All eligible and published clinical randomized controlled trials, investigating the effectiveness of HILT on KOA pain, were included with language limited to English. Patients, 45 years of age or older, diagnosed as symptomatic KOA according to the American College of Rheumatology (ACR) classification, orthopedics, or rheumatologists’ opinions, clinical or imaging findings. Studies, comparing all kinds of HILT (parameters including different wavelengths and power) to other treatments including placebo laser therapy (PL), ET, and conventional physiotherapies (CPT) were included. Participants with severe cognitive impairment or combined with other knee joint impairments were excluded.
2.3Search strategy
Eligible articles were identified with key words (“knee osteoarthritis”, “knee degenerative arthritis”, “knee arthrosis”, “knee OA” OR “KOA”) AND (“high intensity laser therapy”, “high power laser therapy”, “HILT” OR “Nd: YAG”), utilizing the following databases. Electronic retrieval: CENTRAL (Cochrane Central Register of Controlled Trials, up to September 2022), MEDLINE (1950 to September 2022), CINAHL (1982 to September 2022), EMBASE (1980 to September 2022), WOS (Web of science, 1900 to September 2022), PEDro (Physiotherapy Evidence Database, 1999 to September 2022), PsycINFO (1806 to September 2022), SCOPUS (2004 to September 2022). Manual retrieval: 1) manually retrieve references from relevant reviews and originally selected articles to include eligible studies; 2) manual search clinical trial registration platform: ClinicalTrials.gov.
2.4Study selection
The screening and selection of studies were conducted by two independent researchers (WWY, CP) with authors and press unblinded. Afterward the studies were excluded if the titles and abstracts did not meet the pre-set standards. The consensus was achieved by discussion when it was unclear whether the controversial studies should be included, if controversy persists, a decision was made by group discussion (WWY, CP, CCX). Afterwards, the full text of studies originally selected was screened. A forward and backward search was conducted on these eligible studies using the Science Citation Index to obtain other relevant RCTs. Reasons for exclusion of the literature from the full text screening were recorded in the screening form.
2.5Data extraction
Two reviewers (CP, WWY) independently extracted usable information, which contained the first author, publication date, participants’ data (sample size, duration of symptom, and average age), interventions, outcome measurements, the term of follow-ups, from eligible studies.
2.6Assessment of methodological quality
PEDro scale was performed by two independent researchers (CP, WWY) to evaluate the methodological quality of each eligible RCT (9–10: excellent, 6–8: good, 4–5: fair, and
2.7Data analysis
Extracted data was processed by Review Manager Software (version 5.30), with continuous variables were analyzed in the form of mean with a 95% confidence interval (CI). I
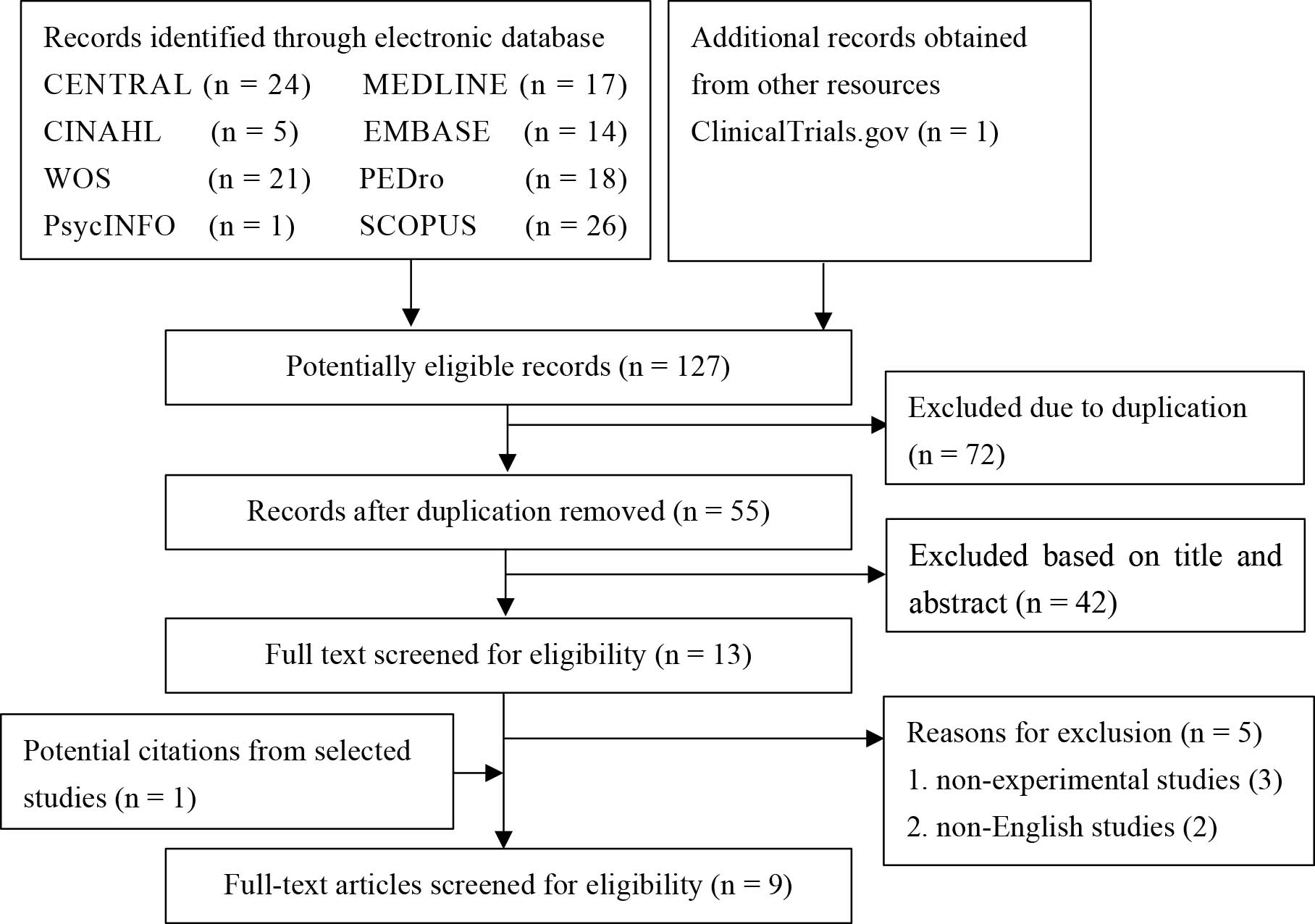
Figure 1.
Flow chart showing the screening process and search results.
3.Results
3.1Literature search
A total of 127 citations were brought into screening (Fig. 1). Then, 55 remained citations were screened for titles and abstracts after duplicate articles were removed with 13 articles remaining for full-text screening. Five articles were excluded after screening the full text among which two articles were in non-English language [38, 39], and three articles [40, 41, 42] were only compared before and after treatment but not with other interventions. Finally, 9 articles [25, 26, 43, 44, 45, 46, 47, 48, 49] meet our selection criteria were included for the current review.
3.2Study characteristics
A total of 9 studies [25, 26, 43, 44, 45, 46, 47, 48, 49] (419 people) meeting the eligibility criteria were identified to further analysis with sample size ranging from 20 to 125 (Table 2). The people included in this review were all diagnosed with KOA, but the diagnostic methods and duration of symptoms were not the same. Alayat et al. [43], and Kheshie et al. [46] diagnosed KOA based on expert opinions (orthopedics or rheumatologists) combined with the imaging findings of the knee joint, while Angelova et al. [44] and Kim et al. [47] mainly based on clinical findings (with or without imaging). The remaining 5 studies [25, 26, 45, 48, 49] were based on the American College of Rheumatology (ACR) classification criteria for the diagnosis of KOA. Regarding the duration of KOA, four studies [25, 26, 45, 46] included people with a disease course of more than 6 months, one study [48] was more than 6 weeks, two [43, 49] was more than 3 months, and the other [44] was more than 4 years. One study [47] included patients whose disease course was unknown. In 7 studies [25, 26, 43, 44, 45, 46, 49], the arthritis classification was at grade II or III (assessed by Kellgren and Lawrence classification), but the KOA classification of the subjects in the study of Gworys et al. [48] and Kim et al. [47] was unclear. The average age of the subjects in all studies was between 50 and 70.
In terms of the type of HILT, the dose, the treatment time, and the operation methods were different in individual studies (details were illustrated in Table 3). There were two studies [44, 48] comparing HILT with other laser treatments (placebo laser, PL, LILT), 4 studies [26, 45, 47, 49] comparing HILT with other therapies (CPT, ET), and 3 studies [25, 44, 46] comparing HILT
For outcome measurements, the visual analog scale (VAS) was used in all 9 studies to evaluate pain intensity before and after operation.
3.3Methodological quality
Of those 9 articles [25, 26, 43, 44, 45, 46, 47, 48, 49], only one study [25] was identified as excellent methodology quality due to the potential biases existed in the process of allocation concealment and assessor operation (Table 4). Six [26, 43, 44, 45, 46, 49] of 9 were considered as having good quality, among which selection bias, attrition bias and performance bias were emerged separately or combined. The remaining studies [47, 48] were regarded as fair or poor quality.
3.4Effects on pain relief
HILT versus other laser therapies (PL, LILT)
There were two studies [44, 48] comparing the effects
Table 2
Characteristics of included studies
| Study ID | Population | Interventions | Outcome measures | Results | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Number Exp/Con | Age M (SD) | BMI Kg/m | X-ray stage | Duration of symptoms | Exp group Con groups | Treatment sessions | |||||
| Alayat 2017 | 23 | 55 | (4.41) | 28.15 | (1.72) | HILT | 12 | VAS | VAS (6 W, 12 W follow-up): | ||
| 22 | 53.64 | (3.54) | 28.91 | (0.49) | ET | 12 | |||||
| 22 | 52.86 | (5.03) | 28.63 | (1.00) | PL | 12 | |||||
| Anna 2016 | 37 | 65.11 | (1.40) | NA | II/III | HILT | 7 | VAS | VAS (7 days): | ||
| 35 | 64.71 | (1.98) | NA | II/III | PL | 7 | |||||
| Nazari 2018 | 30 | 61.5 | (3.9) | 27.7 | (1.4) | II/III | HILT | 12 | VAS | VAS (4 W, 12 W follow-up): | |
| 30 | 62.4 | (3.14) | 27.2 | (1.6) | II/III | CPT | 12 | ||||
| 30 | 62.24 | (3.87) | 27.5 | (1.8) | II/III | ET | 12 | ||||
| Kheshie 2014 | 20 | 52.1 | (6.47) | 29.94 | (3.36) | HILT | 12 | VAS | VAS (6 W): | ||
| 18 | 56.56 | (7.86) | 28.62 | (5.20) | LILT | 12 | |||||
| 15 | 55.6 | (11.02) | 28.51 | (3.35) | PL | 12 | |||||
| Gworys 2012 | 30 | 65.4 | (9.6) | NA | NA | HILT | 10 | VAS | VAS (HILT vs PL): | ||
| 30 | 65.9 | (9.0) | NA | NA | HILT* | 10 | VAS (HILT vs LILL): non-significant | ||||
| 34 | 57.6 | (11.8) | NA | NA | LILT | 10 | |||||
| 31 | 67.7 | (11.3) | NA | NA | PL | 10 | |||||
| Kim 2016 | 10 | 65.3 | (4.2) | NA | NA | NA | HILT | 12 | VAS | VAS: | |
| 10 | 65.5 | (4.0) | NA | NA | CPT | 12 | |||||
| Mazlum 2020 | 20 | 57.85 | (8.06) | 29.94 | (5.49) | II/III | HILT | 10 | VAS | VAS (2 W, 6 W follow-up): | |
| 20 | 58.62 | (11.28) | 31.95 | (4.86) | II/III | PL | 10 | ||||
| Mostafa 2022 | 20 | 46.62 | (8.68) | 29.26 | (2.48) | II | HILT | 12 | VAS | VAS (4 W): | |
| 20 | 40.12 | (9.45) | 28.82 | (5.23) | II | ESWT | 4 | ||||
| Samaan 2022 | 20 | 55.4 | (6.34) | 28.98 | (2.23) | II/III | HILT | 10 | VAS | VAS (4 W): | |
| 20 | 55.2 | (4.77) | 29.1 | (2.42) | II/III | LIPUS | 10 | ||||
| 20 | 57.0 | (6.39) | 29.75 | (2.12) | II/III | ET | 10 | ||||
NA: not available; HILT
Table 3
Types of interventions of included studies
| Study ID | Parameters of high intensity laser | Treatment sites | Application protocols | Comparators | ||
|---|---|---|---|---|---|---|
| Types of HILT | Output power | Total dose | ||||
| Alayat 2017 | Pulsed Nd: YAG laser produced by the HIRO 3.0 device (ASA, Arcugnano, Vicenza, Italy) | Peak powers: 3 kW | 3000 J | Anteromedial and lateral surfaces of the knee with the knee flexed to 90 | Transverse and longitudinal scanning with hand piece being perpendicular to the treated area Anterior or posterior knee surface scanned in two subphases (initial and final) with three fluency levels | ET: range of motion, flexibility, stretching, strengthening exercises |
| Anna 2016 | Semiconductive neodymium laser IV produced by BTL (wavelength 1064 nm) | Peak power: 12 W | 3300J | First three procedures: medial and lateral sides of the knee Next 4 sessions: medial side of the knee | First three procedures: medial and lateral sides of the knee. distant application, 2 minutes, 25 Hz Next 4 sessions: medial side of the knee. Dose 120 J/cm | PL: sham laser treatment, without turning on the light beam |
| Nazari 2018 | Nd: YAG laser with wavelength of 1064 nm (Fysiomed, Belgium) | Peak power: 5 W | 2400 J | The medial and lateral sides of the knee with the patient in a supine position and the knee flexed at 30 | A slow manual scanning in longitudinal and perpendicular direction with a 6-cm probe placed vertically in contact with the joint line | CPT: TENS and US ET: muscle strengthening, flexibility |
| Kheshie 2014 | Pulsed Nd: YAG laser, produced by HIRO 3 device (ASA, Arcugnano, Vicenza, Italy) | Peak powers: 3 kW | 1250 J | Anterior, medial, and lateral aspects of the knee joint in supine lying position with the knee flexed at 30 | The scanning performed transversely and longitudinally in the knee joint with emphasis on the application on the joint line between the tibial and femoral epicondyles | PL |
| Gworys 2012 | Synchronized two-wave laser emitted by an MLS device and one-wave laser/808 nm, 905 nm | HILT 1: 400 mW, energy density 6.21 J/cm | HILT 1: 148.8 J HILT 2: 79.2 J | Three points: medial and lateral of the knee joint gap Two points: superior and inferior aspect of the patellofemoral joint Two points: popliteal fossa | Laser energy administered as contact, single- point, slight pressure irradiation with the use of a laser probe with a lens applicator | PL simulated without actual irradiation |
| Kim 2016 | HILT device (HEALTRON, United Technology Inc., Israel) | No details | No details | Tibia and femoral epicondyle with patient’s knee bent at around 30 | Keep a separation distance of around 1 cm between the handpiece and the skin throughout the treatment | CPT: hot pack treatment, ultrasonic waves |
| Mazlum 2020 | Nd: YAG Laser (BTL-6000) | Peak powers: 12 kW | 300 J | No details | No details | PL |
| Mostafa 2022 | Nd: YAG laser therapy through the HIRO 03 device (ASA, Arcugnano, Vicenza, Italy) with wavelength of 1064 nm | Peak powers: 3 kW | 18 J | The medial side of the knee while the patient lay supine with the knee exed at 30 degree | The HILT handpiece moved transversely and longitudinally in the anterior, medial, and lateral aspects of the knee joint, emphasizing the joint line between the tibial and femoral epicondyles | Extracorporeal shock wave therapy |
| Samaan 2022 | Nd:YAG Laser (BTL-6000 High Intensity Laser 12 W) with wavelength of 1064 nm | Peak powers: 12 kW | 300 J (the analgesic mode) 3000 J (the biostimulation mode) | Both side of the knee | All treatments standardized using a device that placed the participant in a supine position and the semi knee flexion 90 | CPT: low-intensity pulsed ultrasound, active ROM exercises, muscle strengthening, and flexibility exercises |
ET: exercise therapies; PL: placebo laser therapies; CPT: conventional therapies.
Table 4
Methodological quality of included studies
| Study ID | Items of PEDro scale | Total | Level | ||||||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |||
| Alayat 2017 | Yes | Yes | No | Yes | Yes | No | Yes | Yes | No | Yes | Yes | 7/10 | Good |
| Anna 2016 | Yes | No | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 6/10 | Good |
| Nazari 2019 | Yes | Yes | No | Yes | No | No | Yes | Yes | No | Yes | Yes | 6/10 | Good |
| Kheshie 2014 | Yes | Yes | No | Yes | No | No | Yes | Yes | No | Yes | Yes | 6/10 | Good |
| Gworys 2012 | Yes | Yes | No | No | No | No | No | Yes | Yes | No | Yes | 4/10 | Poor |
| Kim 2016 | Yes | Yes | No | No | No | No | No | Yes | Yes | Yes | Yes | 5/10 | Fair |
| Mazlum 2020 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 9/10 | Excellent |
| Mostafa 2022 | Yes | Yes | Yes | Yes | No | Yes | No | Yes | Yes | Yes | Yes | 8/10 | Good |
| Samaan 2022 | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 | Good |
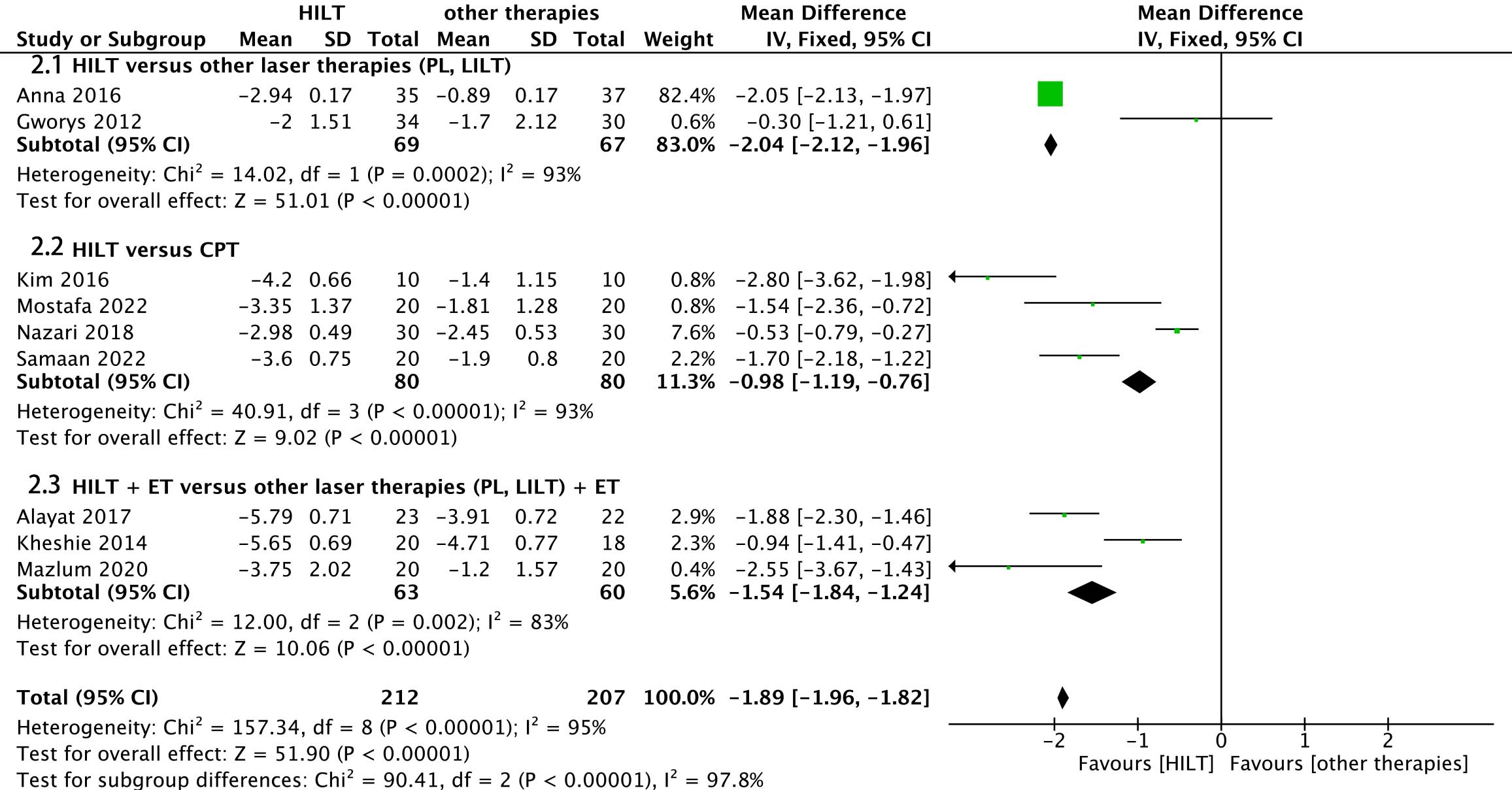
Figure 2.
Forest plot of knee pain VAS scores for HILT versus other therapies.
of HILT and PL in the treatment of KOA pain. A total of 133 subjects in these two studies used VAS to evaluate changes in pain before and after treatment. One study performed by Gworys and colleagues [48] investigated the effectiveness of HILT (dose 12.4 J/point) in contrast to PL therapy on relieving knee pain in patients with KOA, showing that the largest improvement of pain relief was seen in the HILT group after 10 sessions of treatment. In another study, Anna et al. [44] demonstrated that HILT was capable of producing statistically significant immediate (7 days), cumulative, and long lasting (three months) effect on pain in KOA compared to LILT therapy.
The high-intensity laser used in Anna’s research [44] had a wavelength of 1064 nm and an energy density of 12 J/cm
The meta-analysis demonstrated significant pain relief effects of HILT compared to other laser therapies (MD,
3.5HILT versus CPT
Four studies [26, 45, 47, 49] (three [26, 45, 49] with good quality, one [47] with fair quality, 160 people in total) were performed to compare pain relieving effects between HILT and CPT (TENS, Ultrasound, ESWT), showing that HILT was significantly more effective than CPT in decreasing the VAS score after 10 or 12 sessions of treatment, among which one study [45] also demonstrated a long-lasting effect (after 12 weeks) of HILT on pain relief. The populations of the four studies were both 50–75 years old.
The type of high-intensity laser in Nazari’s research [45] was Nd: YAG laser, the wavelength of 1064 nm, the frequency was 30 Hz, the peak power was 5 W, the energy density was 60 J/cm
The meta-analysis demonstrated significant pain relief effects of HILT compared to CPT (MD,
3.6HILT + +
Three studies [25, 43, 46] compared HILT
Alayat [43] used Pulsed Nd:YAG laser therapy, wavelength (1064 nm), very high peak powers (3 kW), average power (10.5 W), high levels of fluency (510–1780 mJ/cm
The meta-analysis demonstrated a significant pain relief effect of HILT
4.Discussion
These nine studies [25, 26, 43, 44, 45, 46, 47, 48, 49] all compared the effects of HILT and other treatments in relieving KOA pain. All studies have shown that HILT was effective in relieving KOA pain, and HILT is not inferior to other treatments in relieving knee pain, including LILT, ET, TENS, ultrasound therapy.
Biologically, KOA is commonly involved not only in the cartilage, subchondral bone, synovial tissue, but also pathoanatomic changes, including insufficient synthesizing extracellular matrix and collagen fibrils of chondrocytes [2, 50]. Therefore, therapies with deeper penetration may be needed to relieve pain in KOA patients.
The biological effects of laser therapies on human tissues may be related to the following main effects: thermal effects (increasing the temperature of the liquid, resulting in changes in intracellular pressure); mechanical effects (cellular mechanical pressure and kinetic changes); electrical effects (causing molecular structure changes of cell membranes and permeability); photochemistry (stimulation of photochemical reactions and selective absorption of certain chemicals in cells); bio-stimulation (providing quantum energy to cells without histological changes) [51]. According to the available evidence [25, 26, 29, 31, 43, 44, 45, 46, 47, 48, 49], the photodynamic and thermodynamics of HILT were the main reasons for the analgesic, anti-edema, anti-inflammatory and repairing effects of HILT. The thermal, photochemical, and mechanical effects of HILT were more obvious than other laser therapies [52]. The main advantage of HILT compared to LILT in pain-relieving effects is that as the power increases, the penetration depth increased (up to 100 mm) and thus worked better in deep structures such as the incomplete cartilage surface inside the knee joint [27, 28, 34, 43, 53]. The stimulation of nerve fiber regeneration by HILT also modulated the “gate control system” to achieve analgesic results [52]. HILT can also block cyclooxygenase and lipoxygenase as well as affect prostaglandins and the synthesis of prostacyclin used to regulate the components of the inflammatory response, exudation, alteration, and proliferation, and to stimulate the body’s re-adaptation response to achieve anti-inflammatory purposes [44]. The effectiveness of HILT is based on laser pulses with a certain frequency and pulse width. Because of this high peak power, a large amount of energy can be delivered in a short period of time, whereas conventional laser treatments that deliver the same amount of energy take longer and work more slowly.
Conventional physical therapies, including TENS [45, 47] (low-frequency electrical stimulation increasing pain threshold), Ultrasound [45] (mechanical stimulation, heat, and cellular massage effects), ESWT [49] (mechanical stimulation promoting subchondral bone repair and increasing the anoxic pain threshold) penetrates less deeply than HILT. However, HILT incorporates all the features of these modalities. When HILT is combined with ET, its pain relief effect may be better. On the one hand, the anti-inflammatory effect induced by HILT probably prompt compliance of exercises and increasing of exercises intensity, and on the other hand, exercise training improving the mechanical load shifts from the joint to the muscle compartments by increasing muscle strength [25, 46]. Through this transfer of mechanics, cartilage regeneration increases, thus the thickness of the cartilage also increases [46], which potentially explains why this combination treatment is superior to other treatments. In a recent meta-analysis, Ahmad et al. [54] investigated that both LILT and HILT are beneficial as adjuncts to ET in the management of KOA pain. However, this meta-analysis did not compare the pain relief effect between HILT
In addition, due to potential bias in the included populations (vary grades of KOA, different duration of onset), intervention methods (different types of HILTs, operating methods, and sites of action) in the included studies, the meta-analysis was highly heterogeneous (heterogeneity greater than 90%). Based on the quality level of the included studies, we also performed qualitative analyses to determine the level of evidence for the three subgroup comparisons.
5.Conclusion
HILT could be a promising modality in alleviating KOA pain, especially when it was implemented in combination with ET. HILT should be recommended for pain relief in patients with KOA over other treatments.
This review limits the age of the eligible population to 45 years and older and does not consider the effect of high-intensity laser on traumatic KOA pain. Due to the limited number of included articles, the current study only provided a qualitative description without conducting a meta-analysis of the effect after follow-up. Therefore, future meta-analysis can consider the use of hierarchical analysis to study the effect of HILT on the pain relief effects of traumatic KOA and explore the long effect of HILT.
Ethical approval
Not applicable.
Funding
The study was supported by the Shenzhen Science and Technology Program (No. GJHZ20190823115412789) and Shenzhen Science and Technology Program (No. JCYJ20210324134401004).
Informed consent
Not applicable.
Author contributions
PC was responsible for the drafting, revising and literature search of the paper. XW registered the paper. WW was responsible for literature search and data extraction. CC was responsible for data extraction of the included studies. HL identified the overall framework and provided statistical support.
Acknowledgments
Thanks to Dr. Li for her valuable advice on the overall framework and statistical support of the paper.
Conflict of interest
None to report.
References
[1] | Cross M, Smith E, Hoy D, et al. The global burden of hip and knee osteoarthritis: Estimates from the global burden of disease 2010 study. Ann Rheum Dis. (2014) ; 73: (7): 1323-30. |
[2] | Hunter DJ, Bierma-Zeinstra S. Osteoarthritis. Lancet. (2019) ; 393: (10182): 1745-1759. |
[3] | Hunter DJ, Schofield D, Callander E. The individual and socioeconomic impact of osteoarthritis. Nat Rev Rheumatol. (2014) ; 10: (7): 437-41. |
[4] | Prieto-Alhambra D, Judge A, Javaid MK, et al. Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: Influences of age, gender and osteoarthritis affecting other joints. Ann Rheum Dis. (2014) ; 73: (9): 1659-64. |
[5] | Hayami T. Osteoarthritis of the knee joint as a cause of musculoskeletal ambulation disability symptom complex (MADS). Clin Calcium. (2008) ; 18: (11): 1574-80. |
[6] | Tang X, Wang S, Zhan S, et al. The Prevalence of Symptomatic Knee Osteoarthritis in China: Results From the China Health and Retirement Longitudinal Study. Arthritis Rheumatol. (2016) ; 68: (3): 648-53. |
[7] | Agaliotis M, Mackey MG, Jan S, et al. Burden of reduced work productivity among people with chronic knee pain: A systematic review. Occup Environ Med. (2014) ; 71: (9): 651-9. |
[8] | Bieleman HJ, Bierma-Zeinstra SM, Oosterveld FG, et al. The effect of osteoarthritis of the hip or knee on work participation. J Rheumatol. (2011) ; 38: (9): 1835-43. |
[9] | Busija L, Bridgett L, Williams SR, et al. Osteoarthritis. Best Pract Res Clin Rheumatol. (2010) ; 24: (6): 757-68. |
[10] | Silverwood V, Blagojevic-Bucknall M, Jinks C, et al. Current evidence on risk factors for knee osteoarthritis in older adults: A systematic review and meta-analysis. Osteoarthritis Cartilage. (2015) ; 23: (4): 507-15. |
[11] | Funck-Brentano T, Nethander M, Moverare-Skrtic S, et al. Causal factors for knee, hip, and hand osteoarthritis: A Mendelian Randomization Study in the UK Biobank. Arthritis Rheumatol. (2019) ; 71: (10): 1634-1641. |
[12] | Lohmander LS, Gerhardsson de Verdier M, Rollof J, et al. Incidence of severe knee and hip osteoarthritis in relation to different measures of body mass: A population-based prospective cohort study. Ann Rheum Dis. (2009) ; 68: (4): 490-6. |
[13] | Turkiewicz A, Petersson IF, Bjork J, et al. Current and future impact of osteoarthritis on health care: A population-based study with projections to year 2032. Osteoarthritis Cartilage. (2014) ; 22: (11): 1826-32. |
[14] | Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. (2012) ; 380: (9859): 2163-96. |
[15] | Fu K, Robbins SR, McDougall JJ. Osteoarthritis: The genesis of pain. Rheumatology (Oxford). (2018) ; 57: (suppl_4): iv43-iv50. |
[16] | Cooper C, Snow S, McAlindon TE, et al. Risk factors for the incidence and progression of radiographic knee osteoarthritis. Arthritis Rheum. (2000) ; 43: (5): 995-1000. |
[17] | Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: An update with relevance for clinical practice. Lancet. (2011) ; 377: (9783): 2115-26. |
[18] | arc OC, arc OC, Zeggini E, et al. Identification of new susceptibility loci for osteoarthritis (arcOGEN): A genome-wide association study. Lancet. (2012) ; 380: (9844): 815-23. |
[19] | von Porat A, Roos EM, Roos H. High prevalence of osteoarthritis 14 years after an anterior cruciate ligament tear in male soccer players: A study of radiographic and patient relevant outcomes. Ann Rheum Dis. (2004) ; 63: (3): 269-73. |
[20] | Xie K, Han X, Jiang X, et al. The effect of varus knee deformities on the ankle alignment in patients with knee osteoarthritis. J Orthop Surg Res. (2019) ; 14: (1): 134. |
[21] | Oiestad BE, Juhl CB, Eitzen I, et al. Knee extensor muscle weakness is a risk factor for development of knee osteoarthritis. A systematic review and meta-analysis. Osteoarthritis Cartilage. (2015) ; 23: (2): 171-7. |
[22] | Riddle DL, Golladay GJ. A longitudinal comparative study of falls in persons with knee arthroplasty and persons with or at high risk for knee osteoarthritis. Age Ageing. (2018) ; 47: (2): 318. |
[23] | Block JA. Osteoarthritis: OA guidelines: Improving care or merely codifying practice? Nat Rev Rheumatol. (2014) ; 10: (6): 324-6. |
[24] | Dobson F, Bennell KL, French SD, et al. Barriers and facilitators to exercise participation in people with hip and/or knee osteoarthritis: Synthesis of the literature using behavior change theory. Am J Phys Med Rehabil. (2016) ; 95: (5): 372-89. |
[25] | Akaltun MS, Altindag O, Turan N, et al. Efficacy of high intensity laser therapy in knee osteoarthritis: A double-blind controlled randomized study. Clin Rheumatol. (2021) ; 40: (5): 1989-1995. |
[26] | Samaan S, Sedhom MG, Grace MO. A randomized comparative study between high-intensity laser vs low-intensity pulsed ultrasound both combined with exercises for the treatment of knee osteoarthritis. Int J Rheum Dis. (2022) ; 25: (8): 877-886. |
[27] | Fan ZW, Qiu JS, Kang ZJ, et al. High beam quality 5 J, 200 Hz Nd: YAG laser system. Light Sci Appl. (2017) ; 6: (3): e17004. |
[28] | Benavides O, De la Cruz May L, Flores A. Experimental study on reflection of high-intensity nanosecond Nd: YAG laser pulses in ablation of metals. Optics and Lasers in Engineering. (2015) ; 68: : 83-86. |
[29] | Nouri F, Raeissadat SA, Eliaspour D, et al. Efficacy of high-power laser in alleviating pain and improving function of patients with patellofemoral pain syndrome: A single-blind randomized controlled trial. J Lasers Med Sci. (2019) ; 10: (1): 37-43. |
[30] | Karaca B. Effectiveness of high-intensity laser therapy in subacromial impingement syndrome. Photomed Laser Surg. (2016) ; 34: (6): 223-8. |
[31] | Alayat MS, Atya AM, Ali MM, et al. Long-term effect of high-intensity laser therapy in the treatment of patients with chronic low back pain: A randomized blinded placebo-controlled trial. Lasers Med Sci. (2014) ; 29: (3): 1065-73. |
[32] | Herman JH, Khosla RC. In vitro effects of Nd: YAG laser radiation on cartilage metabolism. J Rheumatol. (1988) ; 15: (12): 1818-26. |
[33] | Ezzati K, Laakso EL, Salari A, et al. The beneficial effects of high-intensity laser therapy and co-interventions on musculoskeletal pain management: A systematic review. J Lasers Med Sci. (2020) ; 11: (1): 81-90. |
[34] | Song HJ, Seo HJ, Kim D. Effectiveness of high-intensity laser therapy in the management of patients with knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials. J Back Musculoskelet Rehabil. (2020) ; 33: (6): 875-884. |
[35] | Moher D, Shamseer L, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev. (2015) ; 4: : 1. |
[36] | Alam MM, Khan A, Farooq M. Effects of whole-body vibration on muscle strength, balance and functional mobility in patients with multiple sclerosis: A systematic review and Meta-analysis. Journal of Musculoskeletal Research. (2020) ; 23: : 1-16. |
[37] | Furlan AD, Pennick V, Bombardier C, et al. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine (Phila Pa 1976). (2009) ; 34: (18): 1929-41. |
[38] | Štglić-Rogoznica N, Stamenković D, Grubišić-Karavanić V, et al. Evidence based clinical practice of high intensity laser therapy (hilt) effectiveness in elderly patients with knee osteoarthritis. Medicina Fluminensis. (2012) ; 48: : 488-496. |
[39] | Taghizadeh delkhosh C, Fatemi E, Ghorbani R, et al. Comparing the Immediate and Long-term Effects of Low and High Power Laser on the symptoms of Knee Osteoarthritis. Journal of Mazandaran University of Medical Sciences. (2018) . |
[40] | Stiglić-Rogoznica N, Stamenković D, Frlan-Vrgoc L, et al. Analgesic effect of high intensity laser therapy in knee osteoarthritis. Coll Antropol. (2011) ; 35 Suppl 2: 183-5. |
[41] | High intensity laser therapy in knee osteoarthritis: comparison between two different pulsed-laser treatment protocols. |
[42] | Viliani T, Carabba C, Mangone G, et al. High intensity pulsed Nd: YAG laser in painful knee osteoarthritis: The biostimulating protocol. Energy for Health. (2012) ; 9: : 18-22. |
[43] | Alayat MSM, Aly THA, Elsayed AEM, et al. Efficacy of pulsed Nd: YAG laser in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers in Medical Science. (2017) ; 32: (3): 503-511. |
[44] | Angelova A, Ilieva EM. Effectiveness of high intensity laser therapy for reduction of pain in knee osteoarthritis. Pain Res Manag. (2016) ; 2016: : 9163618. |
[45] | Nazari A, Moezy A, Nejati P, et al. Efficacy of high-intensity laser therapy in comparison with conventional physiotherapy and exercise therapy on pain and function of patients with knee osteoarthritis: A randomized controlled trial with 12-week follow up. Lasers Med Sci. (2019) ; 34: (3): 505-516. |
[46] | Kheshie AR, Alayat MS, Ali MM. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers Med Sci. (2014) ; 29: (4): 1371-6. |
[47] | Kim GJ, Choi J, Lee S, et al. The effects of high intensity laser therapy on pain and function in patients with knee osteoarthritis. J Phys Ther Sci. (2016) ; 28: (11): 3197-3199. |
[48] | Gworys K, Gasztych J, Puzder A, et al. Influence of various laser therapy methods on knee joint pain and function in patients with knee osteoarthritis. Ortop Traumatol Rehabil. (2012) ; 14: (3): 269-77. |
[49] | Mostafa M, Hamada HA, Kadry AM, et al. Effect of high-power laser therapy versus shock wave therapy on pain and function in knee osteoarthritis patients: A randomized controlled trial. Photobiomodul Photomed Laser Surg. (2022) ; 40: (3): 198-204. |
[50] | Sinusas K. Osteoarthritis: Diagnosis and treatment. Am Fam Physician. (2012) ; 85: (1): 49-56. |
[51] | Ansari MA, Mohajerani E. Mechanisms of Laser-Tissue Interaction: I. Optical Properties of Tissue. Journal of Lasers in Medical Sciences. (2011) ; 2. |
[52] | Stiglić-Rogoznica N, Stamenković D, Frlan-Vrgoc L, et al. Analgesic effect of high intensity laser therapy in knee osteoarthritis. Collegium Antropologicum. (2011) ; 35 Suppl 2: 183-5. |
[53] | Zati A, Desando G, Cavallo C, et al. Treatment of human cartilage defects by means of Nd: YAG Laser Therapy. J Biol Regul Homeost Agents. (2012) ; 26: (4): 701-11. |
[54] | Ahmad MA, MS AH, Yusof A. Effects of low-level and high-intensity laser therapy as adjunctive to rehabilitation exercise on pain, stiffness and function in knee osteoarthritis: A systematic review and meta-analysis. Physiotherapy. (2022) ; 114: : 85-95. |
[55] | Wyszyńska J, Bal-Bocheńska M. Efficacy of high-intensity laser therapy in treating knee osteoarthritis: A first systematic review. Photomed Laser Surg. (2018) ; 36: (7): 343-353. |


