
The effects of short foot exercises to treat flat foot deformity: A systematic review
Abstract
BACKGROUND:
Studies on the effects of performing short foot exercises (SFEs) on the medial longitudinal arch (MLA) have been inconclusive.
OBJECTIVE:
This study aimed to conduct a systematic review of the effects of SFEs.
METHODS:
‘SFE’ and ‘intrinsic foot muscle’ were keywords used to search for randomized controlled trials. One researcher screened relevant articles based on their titles and abstracts, and two independent researchers closely read the texts, accepting nine studies for inclusion. Outcomes, intervention duration, frequency, and the number of interventions were investigated.
RESULTS:
Of 299 potential studies identified, the titles and abstracts of 211 studies were reviewed, and 192 were excluded. The full texts of 21 studies were obtained and evaluated according to inclusion and exclusion criteria. Nine studies met the inclusion criteria. Six studies concerning the MLA were identified, with four reporting MLA improvement. There was no consensus concerning the number and frequency of SFEs performed, and the mechanism of MLA improvement was unclear. MLA improvement was observed in participants who undertook
CONCLUSIONS:
The results suggest that performing SFEs for
1.Introduction
1.1Flat foot deformity
Flat foot deformity is a chronic foot condition that includes flattening of the medial longitudinal arch (MLA), hindfoot valgus, and midfoot abduction [1], with a reported prevalence of 2–23% in adults [2]. The following factors have been associated with flat feet: occupation [2], obesity [3], and age [4]. Recently, injuries to foot ligaments [5] and a decreased muscle cross-sectional area of the intrinsic foot muscles (IFMs) [6] have also been reported in flat feet, suggesting that foot function is impaired. Studies comparing flat feet with normal alignment have reported that flat feet involve a higher incidence of plantar tendinitis [7]. Furthermore, flat feet have been cited as an important etiology of several lower extremity overuse injuries, including low back pain [8] and shin splints [9, 10]. Therefore, treating a flat foot deformity may potentially prevent overuse injuries.
1.2Treatment for flat foot deformity
Flat feet have previously been classified as flexible or rigid [11]. For rigid flat feet, surgical treatment to correct the bony structure is common [12]. For flexible flat feet, clinically asymptomatic cases do not require intervention [13]. For symptomatic cases, conservative therapy such as nonsteroidal anti-inflammatory drugs, weight loss, functional foot orthoses, physical therapy, and exercise therapy remain treatments of choice to relieve pain and prevent progression of the deformity [14, 15]. Exercise therapy for flat feet includes extrinsic muscle and IFM strengthening to maintain the MLA [16, 17]. The effects of toe flexion exercises, such as the toe curl exercise (TCE), have also been reported [18]. However, the TCE involves the use of both IFMs and extrinsic foot muscles, and recent studies have focused on the IFMs alone [19, 20, 21]. It has been reported that patients with flat feet have higher incidence rates of IFM atrophy compared with patients with a normal MLA [7] and there is a correlation between cross-sectional areas of atrophied IFMs, such as the abductor hallucis longus and flexor digitorum brevis muscles, and the severity of flat feet [22]. Short foot exercises (SFEs) have been used as exercise therapy for IFMs.
1.3Short foot exercises
SFEs shorten the length of the foot through contracting the plantar muscles of the foot to pull the first metatarsal towards the heel and heighten the MLA without flexing the toes [23]. In flatfoot deformity, SFEs are used to strengthen the IFMs, which maintain the MLA [24, 25]. Okamura reported that this exercise decreased foot posture index (FPI) values [26]. In chronic ankle instability, an eight-week SFE intervention was shown to increase Cumberland Ankle Instability Tool (CAIT) values [27].
Prior studies have reported that some patients cannot perform SFEs satisfactorily, even after two weeks of practice [28], and that this is one of the most difficult exercise therapies to implement. In addition, studies on the effect of SFEs on MLA improvement in patients with flat feet have reported differing outcomes [29] and this area remains contentious. Furthermore, the number and frequency of SFEs performed, the duration of the intervention, and the types of outcomes evaluated have not been fully investigated.
1.4Study purpose
The purpose of this study was to conduct a systematic review of studies that provided full details concerning the number and frequency of SFEs undertaken, the duration of the intervention, and the types of outcomes, along with the effects of SFEs.
2.Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) statement and was registered in the PROSPERO database under the identification number CRDCRD42020183467.
2.1Search method
A combination of the following keywords and their variation were used: (short foot exercise OR (short or foot or exercise) OR SFE) AND (intrinsic muscle OR (intrinsic or muscle) OR IFM) to search for randomized controlled trials (RCTs) up to October 2021. We used PubMed, Physiotherapy Evidence Database (PEDro), and the Cochrane Library (including Cochrane Central Register of Controlled Trials, CENTRAL) as search databases. Two reviewers independently conducted the search.
2.2Inclusion and exclusion criteria
The target studies were selected in terms of the abstracts of related articles identified during the database search. The retrieved studies were screened to determine their relevance. Inclusion criteria comprised: (i) RCTs, (ii) studies that included at least one group using an SFE as an intervention, and (iii) articles published in English. Exclusion criteria comprised: (i) animal experiments, and (ii) abstracts, letters, reviews, systematic reviews, meta-analyses, or case reports.
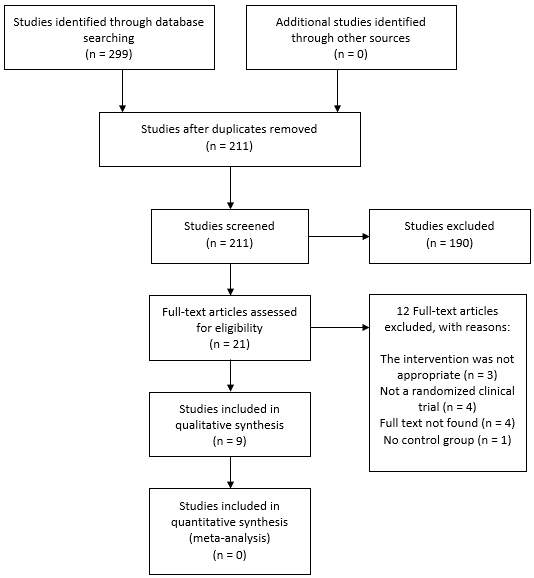
Figure 1.
Flowchart for the selection of included trials.
2.3Quality assessment
The selected studies were independently and critically reviewed and evaluated by two reviewers using the Cochrane risk of bias tool for randomised trials (RoB 2.0), to assess the methodological quality of the included studies for risk of bias across five domains: (i) the randomization process, (ii) deviations from intended interventions, (iii) missing outcome data, (iv) measurement of the outcomes, and (v) selection of the reported results. Studies with a low risk of bias in all five domains were considered to have a low risk of overall bias, studies with some concerns in at least one domain were considered to have some concerns overall, and studies with a high risk of bias overall or a high risk of bias in at least one domain were considered to have a high risk of bias. Studies with at least one domain of some concern were considered to have a concern overall, whereas those with at least one domain of a high risk of bias or studies with multiple domains of some concern were considered to have a high risk of bias. Disagreements among the reviewers were resolved through discussion [30].
Figure 2.
Risk of bias graph: a review of authors’ evaluations concerning each risk of bias item presented as percentages across all included studies.
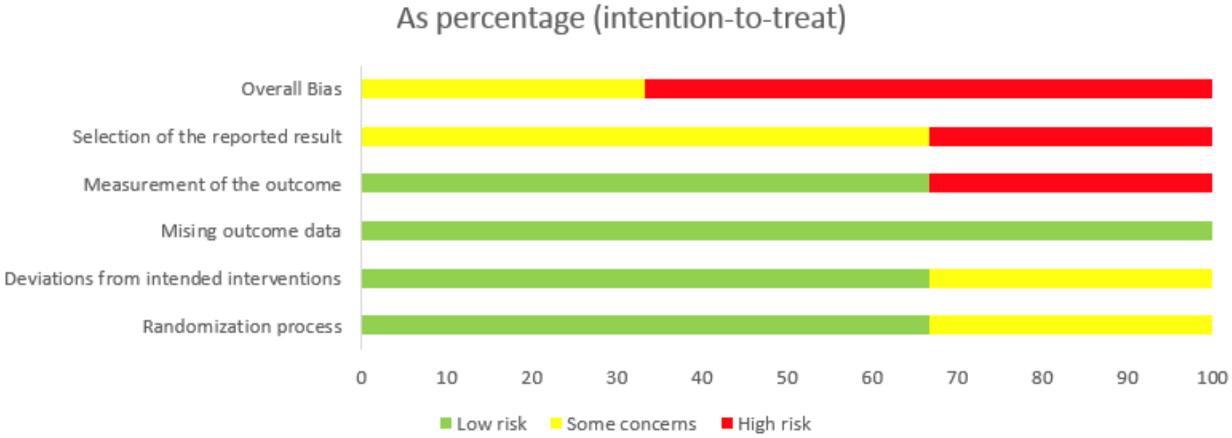
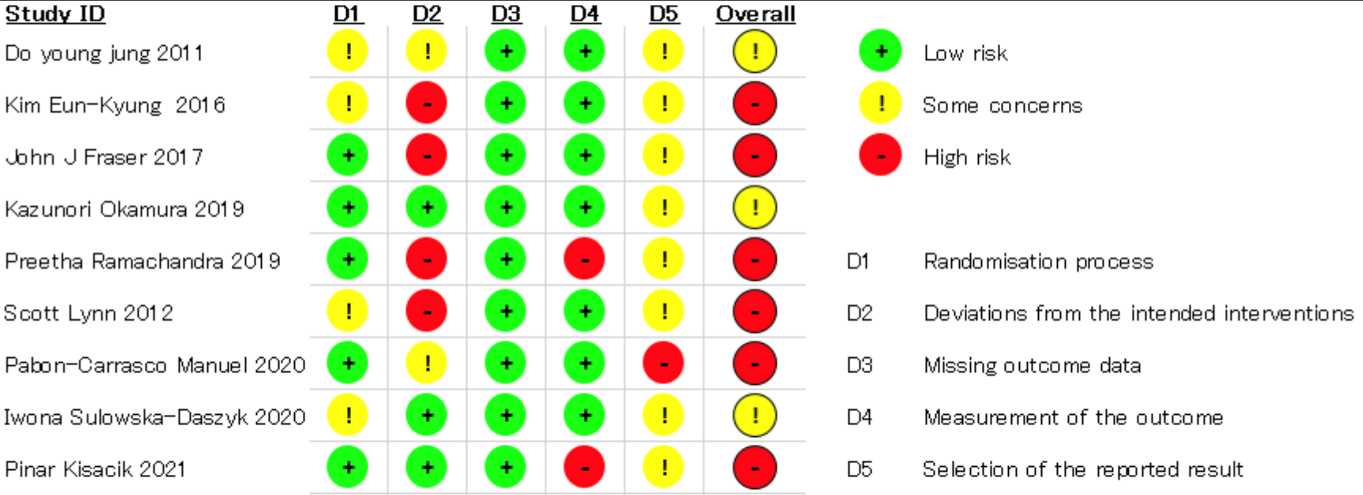
Figure 3.
Risk of bias summary: a review of the authors’ evaluations concerning each risk of bias item for each included study.
2.4Data extraction
A meta-analysis was conducted on dynamic balance, specifically the Y-balance test. One reviewer extracted all the relevant data separately. The extracted and tabulated data included the lead author, year of publication, the number of participants, total score (number of SFEs, frequency of intervention, duration of intervention), type of muscle contraction, posture of execution, duration of muscle contraction, and type of outcome.
Total score
The amount of load was also compared.
2.5Statistical analysis
This meta-analysis was performed using Review Manager Version 5.4 software. Statistical calculations were performed for all included studies using detailed data for SFE alone, SFE combined with other exercise therapies, and exercise therapies alone. An SFE group (SFE combined with exercise therapy) and an exercise therapy group (exercise therapy only) were compared using a random-effects model. Statistical reliability was calculated using 95% confidence intervals (CIs). Statistical heterogeneity was assessed using
3.Results
3.1Study selection
A database search identified 291 potential studies, and 211 abstracts remained after duplicate studies had been removed. The abstracts were then reviewed, and a preliminary evaluation was conducted to assess the eligibility of 21 full-text articles. Nine studies met our inclusion criteria and 12 were excluded, as the interventions in those studies were deemed inappropriate (Fig. 1).
3.2Study characteristics
3.2.1SFE setting
The basic characteristics of the nine selected studies are shown in Tables 1 and 2. Concerning the number of times a single SFE intervention was conducted, the minimum was five times and the maximum was 104 times. Interventions were provided 2–7 days per week, and the intervention period ranged from 4–14 weeks. The total score ranged from 120 to 6552. One study did not provide details concerning the number of repetitions; therefore, the total score could not be calculated.
3.2.2The MLA
Navicular height, the navicular drop test (ND), and the FPI were used to measure the MLA. Six reports concerning the MLA were identified, of which four reported an improvement in the MLA. Kim et al. conducted a five-week SFE study among university students with flat feet and reported a significant decrease in ND post-intervention [33]. Okamura et al. conducted SFEs with electromyographic biofeedback in university students with flat feet and reported a significant post-intervention improvement in the FPI at eight
Table 1
Characteristics of the selected studies
| Author | Year | Patient | Number of patients | Group | Introduction practice | Intervention |
| Outcome for conditions other than MLA | ||
|---|---|---|---|---|---|---|---|---|---|---|
| Jung et al. | 2011 | University students with flexible flat foot | 28 M: NR F: NR | (1) FO | FOSF group were also instructed in a short-foot exercise protocol. | (1) wear FO | None |
| ||
| Fraser et al. | 2017 | Healthy adult | 24 M: 12 F: 12 | (1) intervention (2) control | All participants were verbally instructed, provided demonstration, and guided through a single practice trial of the toe-spread-out, hallux-extension, and lesser-toe-extension exercises prior to baseline assessment. | (1) SFE | None |
| ||
| Iwona et al. | 2020 | Amateur runners | 80 M: 57 F: 23 | (1) SFE (2) control | NR | (1) SFE, Reverse Tandem Gait exercise Vele’s Forward Lean Exercises with band loops strengthening Stability disc exercises (2) No intervention | None |
| ||
| Kim et al. | 2016 | University students with flexible flat foot | 14 M: 10 F: 4 | (1) SFE (2) ASI | Before the intervention, the researcher demonstrated the short foot exercises while giving verbal instructions. | (1) SFE (2) Walking wth ASI | ND | Y-balance tests | ||
| Kısacık et al. | 2021 | Patients with PFP | 30 M: 5 F: 25 drop out: 5 | (1) SFE (2) control | NR | (1) SFE (2) Hip and knee strengthening and stretching exercises |
|
| ||
| Lynn et al. | 2012 | Healthy adult | 24 M: 15 F: 15 drop out: 6 | (1) SFE (2) TCE (3) control | The SFE and TCE groups were instructed to return to the laboratory 1 week after initial testing to receive training on exercises that were to be performed during the training phase of the study. | (1) SFE (2) TCE (3) No intervention | ND |
|
|
Table 1, continued | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Patient | Number of patients | Group | Introduction practice | Intervention |
| Outcome for conditions other than MLA | ||
| Okamura et al. | 2020 | University students with flexible flat foot | 20 M: 3 F: 17 | (1) SFE (2) control | Participants received verbal instruction and a demonstration of the correct technique to perform the short-foot exercise. | (1) SFE |
|
| ||
| Manuel et al. | 2020 | University students with flexible flat foot | 85 M: 42 F: 48 drop out: 5 | (1) SFE (2) NBFE | NR | (1) SFE (2) NBFE |
| None | ||
| Ramachandra et al. | 2019 | Pregnant women | 86 M: F: 86 | (1) Study group (2) Control | NR | (1) Regulr antenatal exercise |
|
| ||
SFE: short foot exercise, ASI: ancle support insole, NR: not reported, EMG: electromyogram, ES: electrical stimulation, PFP: patellofemoral pain, TCE: toe curl exercise, NBFE: non-biomechanical function exercise, FO: foot orthosis.
Table 2
Total score of selected studies
| Author | Year | Patient | Number of patients | Group | Introduction practice | Intervention | Total score | Period [week] | Nsumber of exercise interventons/day or week | Time of intervention | Number of repetitions | Number of sets |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Jung et al. | 2011 | University students with flexible flat foot | 28 M: R F: NR | (1) FO | FOSF group were also instructed in a short-foot exercise protocol. | (1) wear FO | 1680 | 8 | (1) 2/day | (1) NR (2) none | (1) 5 (2) none | (1) 3 (2) none |
| Fraser et al. | 2017 | Healthy adult | 24 M: 12 F: 12 | (1) intervention (2) control | All participants were verbally instructed, provided demonstration, and guided through a single practice trial of the toe-spread-out, hallux-extension, and lesser-toe-extension exercises prior to baseline assessment. | (1) SFE | 6552 | 4 | (1) 3/day | (1) NR (2) none | (1) 15 | (1) 3 (2) none |
| Iwona et al. | 2020 | Amateur runners | 80 M: 57 F: 23 | (1) SFE (2) control | NR | (1) SFE, Reverse Tandem Gait exercise Vele’s Forward Lean Exercises with band loops strengthening Stability disc exercises (2) No intervention | 1260 | 6 | (1) 1/day | (1) 30 minutes (2) none | (1) 30 (2) none | (1) 1 (2) none |
| Kim et al. | 2016 | University students with flexible flat foot | 14 M: 10 F: 4 | (1) SFE (2) ASI | Before the intervention, the researcher demonstrated the short foot exercises while giving verbal instructions. | (1) SFE (2) Walking wth ASI | Not repetitions but time | 5 | (1) 1/day | (1) 30 minutes (2) 30 minutes | (1) NR (2) NR | (1) 1 (2) 1 |
|
Table 2, continued | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Patient | Number of patients | Group | Introduction practice | Intervention | Total score | Period [week] | Nsumber of exercise interventons/day or week | Time of intervention | Number of repetitions | Number of sets |
| Kısacık et al. | 2021 | Patients with PFP | 30 M: 5 F: 25 drop out: 5 | (1) SFE (2) control | NR | (1) SFE (2) Hip and knee strengthening and stretching exercises | 120 | 6 | (1) 1/day | (1) NR (2) NR | (1) 10 (2) 10 | (1) 1 (2) 1 |
| Lynn et al. | 2012 | Healthy adult | 24 M: 15 F: 15 drop out: 6 | (1) SFE (2) TCE (3) control | The SFE and TCE groups were instructed to return to the laboratory 1 week after initial testing to receive training on exercises that were to be performed during the training phase of the study. | (1) SFE (2) TCE (3) No intervention | 2800 | 4 | (1) 1/day | (1) NR (2) NR (3) none | (1) 100 (2) 100 (3) none | (1) 1 (2) 1 (3) none |
| Okamura et al. | 2020 | University students with flexible flat foot | 20 M: 3 F: 17 | (1) SFE (2) control | Participants received verbal instruction and a demonstration of the correct technique to perform the short-foot exercise. | (1) SFE | 720 | 8 | (1) 1/day | (1) 5 sec/time (2) none | (1) 10 (2) none | (1) 3 (2) none |
| Manuel et al. | 2020 | University students with flexible flat foot | 85 M: 42 F: 48 drop out :5 | (1) SFE (2) NBFE | NR | (1) SFE (2) NBFE | 140 | 4 | (1) 1/day | (1) 30 sec/time (2) 30 sec/time | (1) 5 (2) 5 | (1) 1 (2) 1 |
|
Table 2, continued | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Author | Year | Patient | Number of patients | Group | Introduction practice | Intervention | Total score | Period [week] | Nsumber of exercise interventons/day or week | Time of intervention | Number of repetitions | Number of sets |
| Ramachandra et al. | 2019 | Pregnant women | 86 M: 0 F: 86 | (1) Study group (2) Control | NR | (1) Regulr antenatal exercise | 4320 | 14 | (1) 1/day | (1) NR (2) NR | (1) 20 (each) | (1) 3 (2) NR |
SFE: short foot exercise, ASI: ancle support insole, NR: not reported, EMG: electromyogram, ES: electrical stimulation, PFP: patellofemoral pain, TCE: toe curl exercise, NBFE: non-biomechanical function exercise, FO: foot orthosis.
weeks [26]. Ramachandra et al. conducted 14 weeks of SFEs in pregnant women and reported a significant post-intervention increase in navicular height [34]. Kısacık et al. conducted a six-week SFE study of patients with patellofemoral pain (PFP) and reported a significant decrease in ND and FPI scores post-intervention [35].
3.2.3Other outcomes
The outcomes for conditions other than the MLA were IFM function and morphology, balance, foot morphology, and the dynamic navicular drop (DND) test. In three studies, IFM function and morphology were used as outcomes, and both IFM thickness and muscle activity were reported to have improved [23, 26, 36]. Of two studies that used balance as an outcome, all patients showed an improvement in dynamic balance [33, 38]. One study used foot morphology as an outcome in pregnant women and reported that foot length and width increased with advancing gestational weeks in the control group, but foot length and width did not change with advancing gestational weeks in the SFE group [34]. One study used the DND test as an outcome, and reported no change in DND test results [26]. Another study used a visual analogue scale and the Kujala patellofemoral scale as outcomes in patients with PFP, and reported that values in both scales reduced post-intervention [35]. However, another study used functional movement screen test results as a study outcome and reported that scores increased post-intervention [37].
3.2.4Risk of bias
Figures 2 and 3 show risk of bias ratings for each included study. All studies had an increased risk due to the impossibility of blinding the participants. The risk of bias was also increased for studies that did not describe the randomization process, deviations from the intended intervention, missing outcomes, outcome measures, or selection of outcomes to report.
4.Discussion
4.1Summary
A systematic review of the number and frequency of SFEs, the duration of the intervention, and the types of outcomes, was undertaken to determine the effects of SFEs Four studies showed MLA improvement compared with two studies that showed no improvement in the MLA. For outcomes other than the MLA, IFM function and morphology, balance, foot morphology, and DND tests were used, showing the effect of SFEs on IFM thickness and activity, and improvement in balance.
4.2Effects of the intervention on the MLA
Recently, several systematic reviews have focused on IFMs. Willems et al. examined the effects of a plantar IFM strengthening intervention on dynamic balance control and foot function during gait in adults [38] and Erin et al. reported the effects of an intervention on functional mobility [39]; however, neither intervention method was limited to performing SFEs. In a systematic review, Cameron et al. focused on SFEs but limited their investigation to ND as the outcome [40]. Our study provided a review of studies reporting the effectiveness, frequency, and duration of SFE interventions.
Four of six included studies found improvement in the MLA with SFEs. MLA improvement was observed for interventions of
The plantar fascia is reported to be a major contributor to MLA retention [43, 44, 45]. The plantar fascia overlaps the IFMs and attaches to the flexor digitorum brevis. Therefore, IFM strengthening plays an important role in maintaining the foot’s medial longitudinal arch [21, 46]. Three studies described the use of IFM function and morphology as study outcomes and reported improvements in both muscle thickness and muscle activity. However, no study reported changes to the structure of the IFM in relation to the height of the MLA. Furthermore, one study reported no significant change in IFM thickness but improvement in the MLA [26]. Additionally, one study showed an increase in the muscle cross-sectional area of the abductor hallucis muscle, but no change to navicular height [47]. That study did not find an association between IFM hypertrophy and the MLA. Therefore, the effect of SFEs on the MLA require further investigation of morphological changes from an IFM perspective as well as from multiple other perspectives.
4.3Effects on balance
Two studies showed an improvement in balance function [33, 41]. Kim et al. used the Y-balance test as an outcome measure of balance [33]. Lynn et al. used a force plate and found a decrease in center of pressure movements during the Y-balance test [44]. It has been reported that patients with flat feet are more unstable in a static standing position than those without flat feet [48] and, in a study that evaluated dynamic stability during closed-eye standing using a force plate, participants with flat feet were reported to have significantly lower dynamic stability than those with normally arched feet [49]. Lee et al. reported that eight weeks of SFE intervention improved joint position, sense of the ankle joint, and dynamic balance in patients after ankle sprain [50]. In a systematic review of balance training, the most effective intervention period for improving balance ability was 11–12 weeks, and many reports indicate interventions of 5 weeks or longer [51]. From these reports, a period of more than 5 weeks is required for the prompting of the proprioceptive sensation, which is consistent with the period required for the improvement of MLA by SFE. In other words, SFE may have stimulated proprioceptive sensation in the foot, leading to an improvement in MLA. However, none of the RCTs selected in this study targeted proprioceptive sensation. We hypothesized that SFE had an influence with central nervous systems factors that affect muscle strength is the change in the firing rate of alpha motor neurons (rate coding). When the CNS instructs a muscle to contract, both alpha and gamma motor neurons are activated. Gamma motor neurons to contract the intrafusal fibers appropriately. Thus, IFM with SFE altered the firing rate of gamma motor neurons, resulting in altered proprioception.
4.4Clinical significance of Neues
Five weeks of continuous SFE for flat feet may improve morphology and proprioception in the IFMs and improve the MLA. In addition, SFEs have been shown to be more effective than functional orthotic therapy in improving the MLA [33].
4.5Study limitations
This study had several limitations. First, we did not perform a meta-analysis of three studies that reported efficacy in improving the MLA because those studies included a wide range of participants, such as pregnant women, patients with PFP, and college students Second, it was not possible to determine whether the participants were able to learn how to correctly perform the SFEs. In previous studies, SFE requires an hour to two weeks of practice to master, and there are reports of failure to master this exercise even after practice [29]. One included study explained how to perform the SFE but did not mention the time taken to practice or an assessment of whether it had been performed correctly. Okamura et al. used electromyography as feedback, whereas no feedback was provided in other studies [26].
5.Conclusions
The results of this study suggested that SFEs were effective in improving the MLA in participants with flat feet with an intervention period of
Ethical approval
No individual patient data was used for the meta-analysis. Ethical approval was thus not required.
Funding
None to report.
Acknowledgments
The authors would like to thank Editage (www.editage.com) for English language editing.
Conflict of interest
The authors have no conflicts of interest to declare.
References
[1] | Toullec E. Adult flatfoot. Orthop & Traumatol: SurgRes. (2015) ; 101: (1): 11-17. doi: 10.1016/j.otsr.2014.07.030. |
[2] | Shibuya N, Jupiter DC, Ciliberti LJ, Vanburen V, La Fontaine J. Characteristics of Adult Flatfoot in the United States. J Foot Ankle Surg. (2010) ; 49: (4): 363-368. doi: 10.1053/j.jfas.2010.04.001. |
[3] | Jankowicz-Szymańska A, Wódka K, Kołpa M, Mikołajczyk E. Foot longitudinal arches in obese, overweight and normal weight females who differ in age. Homo. (2018) ; 69: (1-2): 37-42. doi: 10.1016/j.jchb.2018.03.001. |
[4] | Troiano G, Nante N, Citarelli GL. Pes planus and pes cavus in Southern Italy: a 5 year study. Ann Ist Super Sanita. (2017) ; 53: (2): 142-145. doi: 10.4415/ANN_17_02_10. |
[5] | Mansour R, Teh J, Sharp RJ, Ostlere S. Ultrasound assessment of the spring ligament complex. Eur Radiol. (2008) ; 18: (11): 2670-2675. doi: 10.1007/s00330-008-1047-1. |
[6] | Angin S, Crofts G, Mickle KJ, Nester CJ. Ultrasound evaluation of foot muscles and plantar fascia in pes planus. Gait Posture. (2014) ; 40: (1): 48-52. doi: 10.1016/j.gaitpost.2014.02.008. |
[7] | Yu-Chi H, Lin-Yi W, Her-Cherng W, Kai-Lan C, Chau-Peng L. The Relationship between the Flexible Flatfoot and Plantar Fasciitis: Ultrasonographic Evaluation. Chang Gung Med J. (2004) ; 27: (6): 443-448. |
[8] | Menz HB, Dufour AB, Riskowski JL, Hillstrom HJ, Hannan MT. Foot posture, foot function and low back pain: the Framingham Foot Study. Rheumatology. (2013) ; 52: (12): 2275-2282. doi: 10.1093/rheumatology/ket298. |
[9] | Newman P, Witchalls J, Waddington G, Adams R. Risk factors associated with medial tibial stress syndrome in runners: a systematic review and meta-analysis. Open Access J Sports Med. (2013) ; 4: : 229-241. doi: 10.2147/oajsm.s39331. |
[10] | Reshef N, Guelich DR. Medial tibial stress syndrome. Clin Sports Med. (2012) ; 31: (2): 273-290. doi: 10.1016/j.csm.2011.09.008. |
[11] | Francisco R, Chiodo CP, Wilson MG. Management of the Rigid Adult Acquired Flatfoot Deformity. Foot Ankle Clin. (2007) ; 12: : 317-327. doi: 10.1016/j.fcl.2007.03.013. |
[12] | Deland JT. Adult-acquired Flatfoot Deformity. J Am Acad Orthop Surg. (2008) ; 16: (7): 399-406. doi: 10.5435/00124635-200807000-00005. |
[13] | Taha AMS, Feldman DS. Painful Flexible Flatfoot. Foot Ankle Clin. (2015) ; 20: (4): 693-704. doi: 10.1016/j.fcl.2015.07.011. |
[14] | Miniaci-Coxhead SL, Flemister AS. Office-based management of adult-acquired flatfoot deformity. Med Clin North Am. (2014) ; 98: (2): 291-299. doi: 10.1016/j.mcna.2013.10.006. |
[15] | Crevoisier X, Assal M, Stanekova K. Hallux valgus, ankle osteoarthrosis and adult acquired flatfoot deformity: a review of three common foot and ankle pathologies and their treatments. EFORT Open Rev. (2016) ; 1: (3): 58-64. doi: 10.1302/2058-5241.1.000015. |
[16] | McKeon PO, Hertel J, Bramble D, Davis I. The foot core system: a new paradigm for understanding intrinsic foot muscle function. Br J Sports Med. (2015) ; 49: (5): 290-290. doi: 10.1136/bjsports-2013-092690. |
[17] | Mckeon PO, Hertel J, Bramble D, Davis I. Freeing the foot: integrating the foot core system into rehabilitation for lower extremity injuries. Clin Sports Med. (2015) ; 34: (2): 347-361. doi: 10.1016/j.csm.2014.12.002. |
[18] | David TB, Hans S, Jae C, John P. Dynamic support of the human longitudinal arch. A biomechanical evaluation. Clin orthop Related Res. (1995) ; (316): 165-172. |
[19] | Fiolkowski P, Brunt D, Bishop M, Woo R, Horodyski M. Intrinsic pedal musculature support of the medial longitudinal arch: an electromyography study. J Foot Ankle Surg. (2003) ; 42: (6): 327-333. doi: 10.1053/j.jfas.2003.10.003. |
[20] | Headlee DL, Leonard JL, Hart JM, Ingersoll CD, Hertel J. Fatigue of the plantar intrinsic foot muscles increases navicular drop. J Electromyogr Kinesiol. (2008) ; 18: (3): 420-425. doi: 10.1016/j.jelekin.2006.11.004. |
[21] | Kelly LA, Cresswell AG, Racinais S, Whiteley R, Lichtwark G. Intrinsic foot muscles have the capacity to control deformation of the longitudinal arch. J R Soc Interface. (2014) ; 11: (93): 20131188. doi: 10.1098/rsif.2013.1188. |
[22] | Angin S, Mickle KJ, Nester CJ. Contributions of foot muscles and plantar fascia morphology to foot posture. Gait Posture. (2018) ; 61: : 238-242. doi: 10.1016/j.gaitpost.2018.01.022. |
[23] | Do-Young J, Monn-Hwan K, Oh-Yun K, Heon-Seock C, Won-Hwee L. A comparison in the muscle activity of the abductor hallucis and the medial longitudinal arch angle during toe curl and short foot exercises. Phys Ther Sport. (2011) ; 12: (1): 30-35. doi: 10.1098/rsif.2013.1188. |
[24] | Do-Young J, Eun-Kyung K, Oh-Yun K. Effect of foot orthoses and short-foot exercise on the cross-sectional area of the abductor hallucis muscle in subjects with pes planus: a randomized controlled trial. J Back Musculoskelet Rehabil. (2011) ; 24: (4): 225-231. doi: 10.3233/BMR-2011-0299. |
[25] | Jihyun L, Jangwhon Y, Heonseock C. Foot exercise and taping in patients with patellofemoral pain and pronated foot. J Bodyw Mov Ther. (2017) ; 21: (1): 216-222. doi: 10.1016/j.jbmt.2016.07.010. |
[26] | Okamura K, Fukuda K, Oki S, Ono T, Tanaka S, Kanai S. Effects of plantar intrinsic foot muscle strengthening exercise on static and dynamic foot kinematics: A pilot randomized controlled single-blind trial in individuals with pes planus. Gait Posture. (2020) ; 75: : 40-45. doi: 10.1016/j.gaitpost.2019.09.030. |
[27] | Lee E, Cho J, Lee S. Short-Foot Exercise Promotes Quantitative Somatosensory Function in Ankle Instability: A Randomized Controlled Trial. Med Sci Monit. (2019) ; 25: : 618-626. doi: 10.12659/msm.912785. |
[28] | Edward MP, Patrick CG. Effect of plantar intrinsic muscle training on medial longitudinal arch morphology and dynamic function. Man Ther. (2013) ; 18: (5): 425-430. doi: 10.1016/j.math.2013.02.007. |
[29] | Haun C, Brown CN, Hannigan K, Johnson ST. The Effects of the Short Foot Exercise on Navicular Drop: A Critically Appraised Topic. J Sport Rehabil. (2021) ; 30: (1): 152-157. doi: 10.1123/jsr.2019-0437. |
[30] | Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) ; l4898: . doi: 10.1136/bmj.l4898. |
[31] | Higgins JPT. Measuring inconsistency in meta-analyses. BMJ. (2003) ; 327: (7414): 557-560. doi: 10.1136/bmj.327.7414.557. |
[32] | Deeks JJ, Higgings JP, Altman D. Analysing Data and Undertaking Meta-Analyses. Cochrane Handbook for Systematic Reviews of Interventions. 2008: : 243-296. |
[33] | Kim E-K, Kim JS. The effects of short foot exercises and arch support insoles on improvement in the medial longitudinal arch and dynamic balance of flexible flatfoot patients. J Phys Sci. (2016) ; 28: (11): 3136-3139. doi: 10.1589/jpts.28.3136. |
[34] | Ramachandra P, Kumar P, Kamath A, Maiya AG. Effect of intrinsic and extrinsic foot muscle strengthening exercises on foot parameters and foot dysfunctions in pregnant women: a randomised controlled trial. Int J Ther Rehabil. (2019) ; 26: (2): 1-11. doi: 10.12968/ijtr.2018.0027. |
[35] | Kısacık P, Tunay VB, Bek N, Atay ÖA, Selfe J, Karaduman AA. Short foot exercises have additional effects on knee pain, foot biomechanics, and lower extremity muscle strength in patients with patellofemoral pain. Journal of Back and Musculoskeletal Rehabilitation. (2021) : 1-12. doi: 10.3233/bmr-200255. |
[36] | John FJ, Jay H. Effects of a 4-Week Intrinsic Foot Muscle Exercise Program on Motor Function: A Preliminary Randomized Control Trial. J Sport Rehabil. (2019) ; 28: : 339-349. doi: 10.1123/jsr.2017-0150. |
[37] | Sulowska-Daszyk I, Mika A, Oleksy Ł. Impact of Short Foot Muscle Exercises on Quality of Movement and Flexibility in Amateur Runners. Int J Environ Res Public Health. (2020) ; 17: (18): 6534. doi: 10.3390/ijerph17186534. |
[38] | Willemse L, Wouters EJM, Bronts HM, Pisters MF, Vanwanseele B. The effect of interventions anticipated to improve plantar intrinsic foot muscle strength on fall-related dynamic function in adults: a systematic review. Journal of Foot and Ankle Research. (2022) ; 15: (1). doi: 10.1186/s13047-021-00509-0. |
[39] | Futrell EE, Roberts D, Toole E. The effects of intrinsic foot muscle strengthening on functional mobility in older adults: A systematic review. (2022) ; 70: (2): 531-40. doi: 10.1111/jgs.17541. |
[40] | Haun C, Brown CN, Hannigan K, Johnson ST. The Effects of the Short Foot Exercise on Navicular Drop: A Critically Appraised Topic. Journal of Sport Rehabilitation. (2021) ; 30: (1): 152-7. doi: 10.1123/jsr.2019-0437. |
[41] | Lynn SK, Padilla RA, Tsang KKW. Differences in static- and dynamic-balance task performance after 4 weeks of intrinsic-foot-muscle training: the short-foot exercise versus the towel-curl exercise. J Sport Rehabil. (2012) ; 21: (4): 327-333. doi: 10.1123/jsr.21.4.327. |
[42] | Pabón-Carrasco M, Castro-Méndez A, Vilar-Palomo S, Jiménez-Cebrián AM, García-Paya I, Palomo-Toucedo IC. Randomized Clinical Trial: The Effect of Exercise of the Intrinsic Muscle on Foot Pronation. Int J Environ Res Public Health. (2020) ; 17: (13): 4882. doi: 10.3390/ijerph17134882. |
[43] | Onahue SW, Sharkey NA. Strains in the metatarsals during the stance phase of gait: implications for stress fractures. J Bone Joint Surg Am. (1999) ; 81: (9): 1236-1244. doi: 10.2106/00004623-199909000-00005. |
[44] | Ijun W. Nonlinear finite element analysis for musculoskeletal biomechanics of medial and lateral plantar longitudinal arch of Virtual Chinese Human after plantar ligamentous structure failures. Clin Biomech. (2007) ; 22: (2): 221-229. doi: 10.1016/j.clinbiomech.2006.09.009. |
[45] | Iaquinto JM, Wayne JS. Computational model of the lower leg and foot/ankle complex: application to arch stability. J Biomech Eng. (2010) ; 132: (2): 021009.1-021009.6. doi: 10.1115/1.4000939. |
[46] | Wong YS. Influence of the abductor hallucis muscle on the medial arch of the foot: a kinematic and anatomical cadaver study. Foot Ankle Int. (2007) ; 28: (5): 617-620. doi: 10.3113/FAI.. |
[47] | Namsawang J, Eungpinichpong W, Vichiansiri R, Rattanathongkom S. Effects of the Short Foot Exercise With Neuromuscular Electrical Stimulation on Navicular Height in Flexible Flatfoot in Thailand: A Randomized Controlled Trial. J Prev Med Public Health. (2019) ; 52: (4): 250-257. doi: 10.3961/jpmph.19.072. |
[48] | Ahmasebi R, Karimi M, Satvati B, Fatoya F. Evaluation of Standing Stability in Individuals with Flatfeet. Foot Ankle Spec. (2014) ; 8: (3): 168-174. doi: 10.1177/1938640014557075. |
[49] | Sung PS, Zipple JT, Andraka JM, Danial P. The kinetic and kinematic stability measures in healthy adult subjects with and without flat foot. Foot. (2017) ; 30: : 21-26. doi: 10.1016/j.foot.2017.01.010. |
[50] | Lee E, Cho J, Lee S. Short-Foot Exercise Promotes Quantitative Somatosensory Function in Ankle Instability: A Randomized Controlled Trial. Med Sci Monit (2019) ; 25: : 618-626. doi: 10.12659/msm.912785. |
[51] | Lesinski M, Hortobágyi T, Muehlbauer T, Gollhofer A, Granacher U. Effects of Balance Training on Balance Performance in Healthy Older Adults: A Systematic Review and Meta-analysis. Sports Med. (2015) ; 45: (12): 1721-1738. doi: 10.1007/s40279-015-0375-y. |


