
Long-term effects of rehabilitation and prevention of further chronification of pain among patients with non-specific low back pain
Abstract
BACKGROUND:
Psychological factors influence the development and persistence of chronic low back pain (CLBP) and may impair the psychosocial rehabilitation success.
OBJECTIVE:
To examine the effects of a combined pain competence and depression prevention training compared to the pain competence training alone and as well as the patients’ stages of pain on the long-term psychosocial rehabilitation success.
METHODS:
In this controlled multicentre study with cluster-block randomization, patients with CLBP in different stages of pain (I–III) received either pain competence training (control group, CG;
RESULTS:
Patients in stage of pain I and II showed significant improvements in depressive symptoms, anxiety, mental health, and average pain intensity at the 12-month follow-up, irrespective from treatment condition.
CONCLUSIONS:
Multidisciplinary rehabilitation seems to be appropriate for patients with CLBP in stage of pain I and II. However, patients in stage of pain III need more psychological treatments to manage their mental comorbidities.

1.Introduction
Non-specific low back pain is a leading health problem, especially in Western industrial countries [1]. Previous research has provided evidence that psychosocial factors influence the transition from acute to chronic low back pain (CLBP) and the exacerbation of low back pain [2]. Psychosocial risk factors (yellow flags) are especially emotional responses (e.g., depressive symptoms) and dysfunctional cognitive (e.g., catastrophizing) and behavioural pain coping strategies (avoidance/endurance behaviour) [3, 4, 5]. Consequently, there is a need to better understand the relationship between psychosocial and physical aspects to increase knowledge about the process of pain chronification. Therefore, interdisciplinary and multimodal pain management treatments with cognitive-behavioural components were developed, and a biopsychosocial approach was applied to these treatments [6, 7]. Their short- and mid-term treatment effectiveness among patients with CLBP was demonstrated, showing decreased pain intensity, disability, and pain catastrophizing and increased quality of life (e.g., [8, 9, 10]). Furthermore, first long-term improvements in quality of life and daily functioning [11] as well as intake of medication and use of the health care system were reported [12].
With regard to German multidisciplinary orthopaedic rehabilitation, different long-term treatment effects among patients with CLBP have been reported [13, 14, 15]. For example, a standardized back school programme [14] and an integrative pain management training without cognitive-behavioural elements [15] could not evoke significant long-term improvements in psychological parameters (e.g., mental quality of life, depression, anxiety), but in somatic outcomes [15]. However, cognitive-behavioural pain management training with an additional depression prevention module showed beneficial long-term effects in depressive symptoms and anxiety [16, 17]. For further research, our former treatment was modified to integrate current didactic methods and newly developed psychological treatment elements. Thus, in this modified cognitive-behavioural pain management and depression prevention training, called Debora [18], elements of mindfulness-based interventions as well as group workshops without educators were included. The results showed that Debora significantly improved depressive symptoms and pain self-efficacy among patients with high levels of depressive symptoms at a 12-month-follow-up assessment [19].
Finally, stage of pain among patients with CLBP has been proven to be a significant moderator for rehabilitation outcomes [20]. Thus, subgroups with different stages of pain should be taken into consideration, which have to be evaluated by an objective measure of the chronification process (cf. [21, 22]). In German-speaking countries, the Mainz Pain Staging System (MPSS) has been established as a valid and reliable measurement for pain chronification [23]. The MPSS is a diagnosis-independent staging model and comprises a total of four axes that investigate different dimensions of pain based on anamnestic patient data. Hence, the MPSS differentiates three stages of pain (I–III); patients in stage of pain I demonstrate a low level of chronification, and patients in stage of pain III show a high level of chronification. In German studies, psychological symptoms (e.g., depressive symptoms, anxiety), pain-specific parameters (e.g., impairment in daily activities) and inability to work were enhanced with an increasing stage of pain [24]. In addition, former results suggest that higher stages of pain may interfere with the psychosocial rehabilitation success [20, 25, 26]. Our combined training Debora is aimed to improve long-term psychosocial rehabilitation outcome among patients in stages of pain I and II but without co-existing mental disorders.
The aim of this study was to examine the 1-year longitudinal effects of Debora and stages of pain on depressive symptoms (primary outcome) as well as anxiety, somatization, health status and average pain intensity (secondary outcomes) in German inpatient multidisciplinary rehabilitation centres. It is expected that patients with CLBP will differ in their long-term psychosocial rehabilitation success dependent on the treatment conditions and stages of pain.
2.Methods
2.1Design and procedure
The present study was a randomized controlled trial with cluster-block randomization. Block randomization was realized by having two multidisciplinary orthopaedic clinics perform the control condition and two other clinics simultaneously perform the intervention condition to control seasonal effects. In the context of cluster randomization, each clinic had the same number of control and intervention groups according to an a priori fixed alternating rhythm [27]. Patients were assigned to the clinics by the German Pension Insurance. The project management therefore had no influence on how many patients were assigned to which clinic at which time. In addition, all patients from one week of arrival formed a closed psychological group who participated in either the control or the intervention condition. All psychological interventions and thus also the pain competence and depression prevention training, were conducted by clinical psychologists working on site in the respective cooperation clinic. Additionally, a documentation assistant was employed in each clinic to coordinate the study.
To investigate the long-term rehabilitation outcomes, a 2
Recruitment consecutively occurred during the initial physical consultation in four inpatient multidisciplinary clinics in Germany: ‘Paracelsus-Klinik an der Gande’ in Bad Gandersheim, ‘Reha-Zentrum Bad Sooden-Allendorf Klinik Werra’ in Bad Sooden-Allendorf, ‘Rehabilitationsklinik Auental’ in Bad Steben and ‘Rehabilitationsklinik Göhren’ in Göhren. The patients were informed about the aims, contents and data protection process of the study. Referring to the week of arrival, voluntary patients were allocated to treatment conditions. Allocation was achieved by a randomized Latin square design to control for seasonal effects; the four allocation plans were assigned to the clinics by an independent doctoral student at the Europa-Universität of Flensburg. While the physician determined the stage of pain during an initial consultation, the other data were collected with questionnaires. Data collection pre- and post-assessment occurred before (
Although physicians and nursing staff were blinded to the patients’ group assignment, patients and responsible therapists who conducted the pain competence training or the combined training with depression prevention were not. The documentation assistants in the clinics who organised and accompanied the data collections had also knowledge of the assignment of the treatment conditions and were therefore not blinded. In addition, the study management and thus the evaluators of the analyses had the pseudonymised data and the list for linking the ID numbers with the plain names. However, the study data were entered pseudonymously and subsequently analysed. The statistical variable intervention group/control group was noted in the data sets. The evaluators were therefore not blinded.
This study was approved by the ethical review board of the German Psychological Society (DGPs) and was conducted in accordance with the 1964 Declaration of Helsinki and its later amendments. Written consent was obtained from all individual participants included. Furthermore, the trial was registered with the German Clinical Trial Register DRKS (DRKS00015465). The present study is a secondary analysis within the evaluation of the registered, controlled trial Debora. Therefore, no additional sample size calculation and power analysis was performed for the present analysis, as it is a continuing evaluation within the overall trial Debora. The sample size calculation was calculated before starting the study for the primary outcome ‘depression’. Please see the published sample size calculation and power analysis in Linton and Kienbacher [22].
2.2Participants
A total of 526 patients with CLBP were included in the per protocol (PP) analyses. The patients had a mean age of 53.22 years (
Table 1
Participant’s baseline characteristics for all stages of pain according to the Mainz Pain Staging System
| Variable | Stage of pain I ( | Stage of pain II ( | Stage of pain III ( | Total sample ( | |
|---|---|---|---|---|---|
| Socio-demographic data | |||||
| Age [in years] (mean | 52.79 | 53. 18 | 53.74 | 53.22 | |
| Gender, female no. (%) | 96 (76.2%) | 235 (87.0%) | 101 (77.7%) | 432 (82.1%) | |
| Family status, married no. (%) | 71 (56.4%) | 173 (64.1%) | 87 (66.9%) | 331 (62.9%) | |
| Educational level no. (%) | |||||
| Low | 24 (19.1%) | 51 (18.9%) | 28 (21.5%) | 103 (19.6%) | |
| Middle | 50 (39.7%) | 135 (50.0%) | 68 (52.3%) | 253 (48.1%) | |
| High | 50 (39.7%) | 80 (29.6%) | 31 (23.9%) | 161 (30.6%) | |
| Other school-leaving qualification | 2 (1.5%) | 4 (1.5%) | 2 (1.5%) | 8 (1.5%) | |
| Work-related data | |||||
| Employed no. (%) | 113 (89.7%) | 237 (87.8%) | 108 (83.1%) | 458 (87.1%) | |
| Days of sick leave due to pain in the last 3 months, | 26 (20.6%) | 74 (27.4%) | 47 (36.2%) | 147 (28.0%) | |
| more than 2 weeks no. (%) | |||||
| Pain history | |||||
| Pain duration [in years] (mean | 13.57 | 14.80 | 17.14 | 15.11 | |
| Pain locations no. (mean | 4.30 | 5.21 | 6.48 | 5.31 | |
| Average pain intensity (mean | 4.23 | 4.93 | 5.57 | 4.92 | |
| Psychological status | |||||
| Depressive symptoms (CES-D; mean | 20.18 | 23. 35 | 26.30 | 23.32 | |
| Health status (SF-12; mean | |||||
| Physical | 41.35 | 37.36 | 32.98 | 37.25 | |
| Mental | 39.27 | 38.75 | 36.91 | 38.43 |
2.3Treatment conditions
In the context of a German inpatient multidisciplinary orthopaedic rehabilitation programme lasting 3 to 4 weeks, the combined pain competence and depression prevention training ‘Debora’ was implemented and followed a biopsychosocial approach of CLBP [18]. The aim of the cognitive-behavioural patient training is to reduce biopsychosocial dysfunction among patients with somatic-psychic comorbidity of CLBP and depressive symptoms. Furthermore, long-term attitude and behaviour change through the promotion of patients’ self-management skills and empowerment are further aims of the training. To conduct patient training, clinics were a priori provided with prepared presentations and materials (worksheets, printed cards, videos, package string, ball) for the exercises in each session. In addition, different participant booklets with information und worksheets were made and handed out for CG and IG patients. In general, each session of the training addressed a key topic and was equally structured by the following building blocks: Homework feedback (except 1st session), psychoeducation, practical relevance (self-reflection, exercise, video examples, role play or discussion), homework and feedback on each session.
The pain competence training included four sessions and discussed the interactions between behaviour and pain (1), emotions and pain (2), cognitions and pain (3) and stress and pain (4) [18, 19]. While the first session discusses the basics of the biopsychosocial model and distinguishes positive from negative behaviour, the second session focuses on pain-reducing and pain-enhancing emotions. In the third session, cognitive restructuring is practiced, and the role of attention on pain perception is explained. The combined influences of behaviour and emotions on pain are highlighted and put together to form the vicious circle. In the fourth session, it is explained how stress arises, and personal stressful situations, stress responses and coping strategies are explored. Patients in the CG and IG participated in the pain competence training.
In addition, only patients in the IG received four sessions of cognitive-behavioural depression prevention training. In the first session (1a), the effects of dysfunctional behaviour such as avoidance or social isolation and functional behaviour such as relaxation or social interaction are discussed. The Activities-Emotions-Pain Protocol as an instrument for the promotion of the activity level is presented for patients to complete regularly during training. In the second session, especially nonverbal communication of pain is discussed (2a). The patients’ own pain communication is reflected upon. In the third session (3a), automatic thoughts are discussed, and the phenomena of thought suppression and catastrophizing are worked out. The formulation of alternative positive self-instructions is practiced using the ABC-scheme. Finally, the distinction between adaptive and maladaptive coping strategies is practiced (4a). A psychotherapist guided all four to eight closed group sessions. Each group session lasted 75 minutes. After each session, the patients participated in a 25-minute group workshop without a psychotherapist to complete cognitive-behavioural exercises and promote participants’ empowerment and a social exchange of experiences within the group [18].
2.4Outcome measures
For the present analysis, the primary outcome (depressive symptoms) and four secondary outcomes (anxiety, somatization, health status, average pain intensity) were selected and measured at each time of assessment. Depressive symptoms were measured with the German version of the CES-D (ADS, [28]). The 20 items of the ADS assess the severity of depressive symptoms over the past two weeks on a four-point scale (0
Anxiety was measured using the 7-item anxiety subscale of the German version of the Hospital Anxiety and Depression Scale (HADS-D, [29]), which is rated on a four-point scale (0
To measure somatization, the somatization subscale of the German short version of the Brief-Symptom-Checklist (Mini-SCL, [30]) was used. The 6-item questionnaire rates items on a five-point scale (0
Health status was measured with the 6-item physical health and mental health subscales of the German version of the Short-Form-12 (SF-12, [31]). The standard score is from 0 to 100, and higher scores represent better physical and mental quality of life.
To measure the average pain intensity, the single-item average pain intensity of the German Questionnaire of Pain (DSF, [32]) was applied. The single item was rated on an 11-point scale with reference to the past two weeks.
2.5Statistical analysis
For depressive symptoms, anxiety, somatization and average pain intensity, univariate two-way measures analyses of variance (ANOVA) were performed with treatment condition (CG, IG) and stage of pain (I–III) as between-subjects factors and time of assessment (
3.Results
3.1Dropout analyses
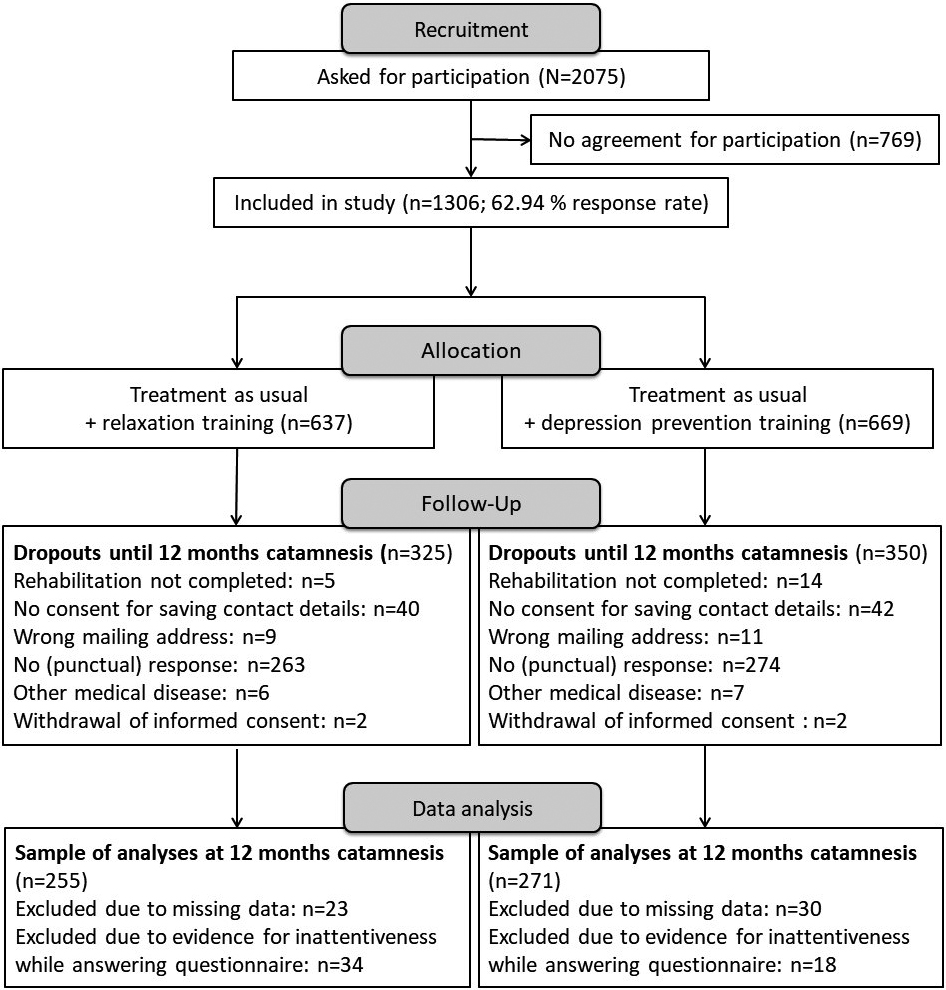
A total of 2075 patients with CLBP were approached for the study, and 769 patients did not agree to participate. Thus, 1306 patients with CLBP were randomized and participated in the study at pre-assessment. During the 12-month follow-up, 675 patients dropped out due to different reasons (dropout rate: 51.68%; Fig. 1). Figure 1 shows that not returning the questionnaire on time or at all is the most common reason for dropping out. Other reasons are no consent for saving contact details, wrong mailing address, rehabilitation not completed, withdrawal of informed consent or other medical disease. Filter variables were also used during data analyses to examine the same patients. These filter variables were the ADS scores and the evidence of response bias at all assessment points [23], stage of pain (MPSS, [23]) and gender at pre-assessment. As a result, the sample size decreased to 526 patients, who were included in the PP. Furthermore, analyses after MI were conducted. The MI sample comprised all patients who agreed to participate in the study. The same filter variables as in PP analyses were used. Thus, the sample size was finally
Figure 1.
Flowchart of sample sizes for control and intervention group (CONSORT).
Chi
3.2Rehabilitation outcome
None of the multi- and univariate repeated measures ANOVAs showed significant two-way interactions. However, a one-way interaction of treatment condition and time of assessment was significant for somatization. Furthermore, a significant one-way interaction of stage of pain and time of assessment was found for depressive symptoms, anxiety, mental health and average pain intensity (Table 2). The following description of rehabilitation outcomes is focused on the interaction effects of time. Moreover, all presented main and interaction effects were confirmed by ITT analyses, except for the one-way interaction treatment condition by time in somatization.
Table 2
Results (ANOVA) for treatment condition (TC), stage of pain (MPSS), and time of assessment (T)
| Variable | Factors | |||||||
|---|---|---|---|---|---|---|---|---|
| TC | MPSS | TC x MPSS | T | TC x T | MPSS x T | TC x MPSS x T | ||
| Depressive symptoms |
| 1, 520 | 2, 520 | 2, 520 | 2.7, 1398.8 | 2.7, 1398.8 | 5.4, 1398.8 | 5.4, 1398.8 |
| F | 0.20 | 23.88 | 0.99 | 171.76 | 0.56 | 2.96 | 1.44 | |
| p | 0.659 |
| 0.371 |
| 0.623 | 0.010 | 0.202 | |
|
| 0.000 | 0.084 | 0.004 | 0.248 | 0.001 | 0.011 | 0.006 | |
| Anxiety |
| 1, 518 | 2, 518 | 2, 518 | 2.8, 1472.1 | 2.8, 1472.1 | 5.7, 1472.1 | 5.7, 1472.1 |
| F | 0.41 | 19.44 | 0.42 | 176.76 | 1.39 | 2.63 | 1.40 | |
| p | 0.522 |
| 0.659 |
| 0.247 | 0.017 | 0.215 | |
|
| 0.001 | 0.070 | 0.002 | 0.254 | 0.003 | 0.010 | 0.005 | |
| Somatization |
| 1, 518 | 2, 518 | 2, 518 | 2.9, 1481.7 | 2.9, 1481.7 | 5.7, 1481.7 | 5.7, 1481.7 |
| F | 0.04 | 30.05 | 1.01 | 65.41 | 2.68 | 0.95 | 0.47 | |
| p | 0.843 |
| 0.367 |
| 0.048 | 0.453 | 0.822 | |
|
| 0.000 | 0.104 | 0.004 | 0.112 | 0.005 | 0.004 | 0.002 | |
| Health status (multivariate) |
| 2, 455 | 4, 910 | 4, 910 | 6, 2734 | 6, 2734 | 12, 2734 | 12, 2734 |
| F | 0.35 | 22.43 | 0.99 | 78.09 | 0.50 | 2.59 | 0.96 | |
| p | 0.702 |
| 0.413 |
| 0.813 | 0.002 | 0.483 | |
|
| 0.002 | 0.090 | 0.004 | 0.146 | 0.001 | 0.011 | 0.004 | |
| Physical health |
| 1, 456 | 2, 456 | 2, 456 | 2.7, 1250.1 | 2.7, 1250.1 | 5.5, 1250.1 | 5.5, 1250.1 |
| F | 0.49 | 42.30 | 0.83 | 40.54 | 0.71 | 0.51 | 0.92 | |
| p | 0.484 |
| 0.438 |
| 0.533 | 0.784 | 0.477 | |
|
| 0.001 | 0.156 | 0.004 | 0.082 | 0.002 | 0.002 | 0.004 | |
| Mental health |
| 1, 456 | 2, 456 | 2, 456 | 2.8, 1309.9 | 2.8, 1309.9 | 5.8, 1309.9 | 5.8, 1309.9 |
| F | 0.07 | 13.50 | 0.87 | 118.19 | 0.27 | 4.61 | 1.13 | |
| p | 0.789 |
| 0.422 |
| 0.839 |
| 0.345 | |
|
| 0.000 | 0.056 | 0.004 | 0.206 | 0.001 | 0.020 | 0.005 | |
| Average pain intensity |
| 1, 473 | 2, 473 | 2, 473 | 2.9, 1357.1 | 2.9, 1357.1 | 5.7, 1357.1 | 5.7, 1357.1 |
| F | 0.05 | 39.50 | 1.16 | 61.42 | 0.58 | 3.24 | 0.81 | |
| p | 0.819 |
| 0.314 |
| 0.618 | 0.004 | 0.556 | |
|
| 0.000 | 0.143 | 0.005 | 0.115 | 0.001 | 0.014 | 0.003 | |
Legend.
3.2.1Effects of treatment condition by time
As depicted in Table 3, only the IG improved significantly in somatization with a small effect size 6 months after rehabilitation (
Table 3
Means (
| Variable | Control group (1) | Intervention group (2) | Dependent comparisons | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
| ||||||||||
| Somatization |
| 6.73 | 4.63 | 5.69 | 6.01 | 6.77 | 4.20 | 6.23 | 6.14 | 1 |
| 0.49 | 0.47 | ||||
|
|
| 0.040 | 0.019 |
|
| 0.691 | |||||||||||
|
| 0.31 | 0.26 | 0.30 | 0.31 | 0.31 | 0.26 | 0.31 | 0.31 | 2 |
| 0.25 | 0.33 | 0.07 | ||||
|
|
|
| 0.007 |
|
| 0.143 | |||||||||||
Legend.
3.2.2Effects of stage of pain by time
Univariate repeated measures ANOVA yielded a simple interaction for depressive symptoms and anxiety (Table 2). First, patients in stage of pain I (
The average pain intensity significantly decreased among patients in stage of pain I (
Table 4a
Means (
| Variable | Stage of pain 1 | Stage of pain 2 | Stage of pain 3 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
|
|
|
|
|
|
|
|
|
| ||
| Depressive symptoms | M | 20.32 | 9.57 | 14.42 | 15.44 | 23.40 | 12.51 | 18.30 | 18.21 | 26.41 | 16.30 | 23.30 | 25.19 |
| SE | 0.98 | 0.85 | 1.06 | 1.07 | 0.67 | 0.58 | 0.72 | 0.73 | 0.96 | 0.84 | 1.04 | 1.05 | |
| Anxiety | M | 9.23 | 4.59 | 6.36 | 6.81 | 10.30 | 6.17 | 7.87 | 7.74 | 11.19 | 8.05 | 9.40 | 9.78 |
| SE | 0.38 | 0.38 | 0.39 | 0.40 | 0.26 | 0.26 | 0.27 | 0.27 | 0.37 | 0.37 | 0.38 | 0.39 | |
| Mental health | M | 38.80 | 51.36 | 45.66 | 45.37 | 38.35 | 48.45 | 44.46 | 44.22 | 36.73 | 45.08 | 39.91 | 37.05 |
| SE | 1.05 | 1.00 | 1.12 | 1.09 | 0.71 | 0.67 | 0.75 | 0.74 | 1.00 | 0.96 | 1.06 | 1.04 | |
| Average pain intensity | M | 4.27 | 3.06 | 2.95 | 3.15 | 4.98 | 3.66 | 3.99 | 3.96 | 5.54 | 4.78 | 4.82 | 5.22 |
| SE | 0.17 | 0.18 | 0.19 | 0.18 | 0.11 | 0.12 | 0.13 | 0.12 | 0.16 | 0.17 | 0.18 | 0.17 | |
Legend.
Table 4b
Effect sizes (ES), and pairwise comparisons (
| Variable | Independent comparisons | Dependent comparisons | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MPSS |
|
|
|
| MPSS | |||||||||
| Depressive | 1-2 | ES | 0.28 | 0.31 | 0.33 | 0.23 | 1 | ES | 0.51 | 0.62 | 0.09 | |||
| symptoms | p | 0.009 | 0.004 | 0.003 | 0.032 | p |
|
|
|
|
| 0.197 | ||
| 1-3 | ES | 0.56 | 0.71 | 0.75 | 0.81 | 2 | ES | 0.61 | 0.60 | |||||
| p |
|
|
|
| p |
|
|
|
|
| 0.860 | |||
| 2-3 | ES | 0.28 | 0.40 | 0.42 | 0.58 | 3 | ES | 0.74 | 0.93 | 0.16 | ||||
| p | 0.010 |
|
|
| p |
| 0.001 | 0.222 |
|
| 0.015 | |||
| Anxiety | 1-2 | ES | 0.25 | 0.37 | 0.35 | 0.21 | 1 | ES | 0.42 | 0.52 | 0.10 | |||
| p | 0.020 | 0.001 | 0.002 | 0.053 | p |
|
|
|
|
| 0.121 | |||
| 1-3 | ES | 0.46 | 0.81 | 0.70 | 0.67 | 2 | ES | 0.40 | 0.37 | |||||
| p |
|
|
|
| p |
|
|
|
|
| 0.522 | |||
| 2-3 | ES | 0.21 | 0.44 | 0.35 | 0.46 | 3 | ES | 0.75 | 0.43 | 0.33 | ||||
| p | 0.048 |
| 0.001 |
| p |
|
|
|
|
| 0.171 | |||
| Mental health | 1-2 | ES | 0.04 | 0.28 | 0.10 | 0.10 | 1 | ES | 1.16 | 0.63 | 0.60 | |||
| p | 0.721 | 0.016 | 0.373 | 0.387 | p |
|
|
|
|
| 0.758 | |||
| 1-3 | ES | 0.19 | 0.60 | 0.50 | 0.73 | 2 | ES | 0.93 | 0.56 | 0.54 | ||||
| p | 0.154 |
|
|
| p |
|
|
|
|
| 0.713 | |||
| 2-3 | ES | 0.15 | 0.32 | 0.39 | 0.63 | 3 | ES | 0.76 | 0.29 | 0.03 | ||||
| p | 0.187 | 0.004 | 0.001 |
| p |
| 0.003 | 0.775 |
|
| 0.002 | |||
| Average pain | 1-2 | ES | 0.40 | 0.32 | 0.52 | 0.43 | 1 | ES | 0.05 | 0.10 | ||||
| intensity | p | 0.001 | 0.005 |
|
| p |
|
|
| 0.548 | 0.622 | 0.227 | ||
| 1-3 | ES | 0.71 | 0.92 | 0.95 | 10.10 | 2 | ES | 0.18 | 0.16 | |||||
| p |
|
|
|
| p |
|
|
| 0.007 | 0.014 | 0.803 | |||
| 2-3 | ES | 0.32 | 0.60 | 0.42 | 0.67 | 3 | ES | 0.02 | 0.24 | 0.20 | ||||
| p | 0.005 |
|
|
| p |
|
| 0.082 | 0.791 | 0.011 | 0.012 | |||
Legend.
4.Discussion
In this multicentre study, the long-term rehabilitation outcomes of a German pain management and depression prevention training among patients with CLBP were examined. Additionally, the stages of pain were considered.
4.1Rehabilitation outcome
The PP analyses revealed a significant interaction between treatment condition and time of assessment in somatization only; patients in the IG benefited in somatization at the 6-month follow-up assessments, showing a small effect size. However, the treatment conditions did not significantly differ at any assessment point. Moreover, the analyses after MI could not validate this interaction effect. Thus, no additional influence of depression prevention training on somatization could be assumed. Overall, the missing interaction effects between treatment condition and time of assessment on the other outcomes must be discussed. In contrast to the current findings, results of our previous pain management training showed significant improvements in psychological parameters (e.g., depressive symptoms), especially for the IG at a 12-month follow-up [16]. The different clinical settings have to be considered. While the present study involved multidisciplinary rehabilitation, patients with CLBP in the previous study were treated in two orthopaedic clinics with less psychological elements [17]. The missing superiority of the current depression prevention training could have been due to the biopsychosocial approach of the whole multidisciplinary rehabilitation and to the modified concept of the current pain management training [18]. In contrast to the earlier pain management training, more interactive methods, mindfulness-based interventions, and additional group workshops were included. Thus, patients in the CG could have already strengthened biopsychological aspects in the multidisciplinary rehabilitation.
Furthermore, patients in stages of pain I and II improved in depressive symptoms, anxiety, mental health, and average pain intensity in the medium- and long-term, with small to medium effect sizes. It can be assumed that patients in stage of pain I benefit from participation in pain management training alone and are oversupplied by the additional depression prevention training, even though no negative effects were observed in the present results. According to higher psychological impairments among patients in stage of pain II, treatment with the combined pain management and depression prevention training seemed appropriate for this subgroup. However, the present effects contradict earlier results, which did not demonstrate a significant long-term influence of the stages of pain on depressive symptoms, mental health, or average pain intensity [20]. Thus, it can be assumed that our modified depression prevention training is better adapted to the psychological and pain-related needs among patients with CLBP in stage of pain II. In contrast to the previous training, for example, the ABC scheme to reconstruct dysfunctional cognitions as well as more psychological elements to develop problem and emotion-focused coping strategies and to improve social support were included [18]. Moreover, recent studies demonstrated only a reduction in anxiety for patients in stage of pain I 24 months after treatment [20]. This finding supports our assumption that the modified group training with modern didactics and methods (e.g., mindfulness-based interventions) should be addressed in patients in stage of pain II. However, patients in stage of pain I would not be over-treated by participation in Debora.
Mixed results have been provided regarding the link between the stage of pain and the average pain intensity. In contrast to our non-significant results, Pfingsten et al. [24] found an improved pain intensity 6 months after rehabilitation. However, in agreement with the present findings, patients in a lower stage of pain had a greater long-term therapeutic success in average pain intensity [25]. Finally, similar results for depressive symptoms were found; patients in stage of pain I benefited most from reduced depressive symptoms [26]. Thus, the findings of Gerrits et al. [35] can support that pain is a risk indicator for the development of depressive symptoms and anxiety. The present results add more evidence to the research on the relationship between chronic pain and mental disorders [35].
The rehabilitation success of patients in stage of pain III was lower than in the upper stages of pain and was not sustainable; this subgroup showed significant improvements in depressive symptoms, anxiety, mental health and average pain intensity at the 6-month follow-up, favourable effects could only be maintained in anxiety at the 12-month follow-up. These findings are in line with the unfavourable prognosis of Gerbershagen [23] regarding stage-specific treatment outcomes. Additionally, these recurrent effects lend support to the assumption that the multidisciplinary rehabilitation was likely to be insufficient to meet the need for psychological treatment in this subgroup. Therefore, treatment in psychosomatic rehabilitation is necessary.
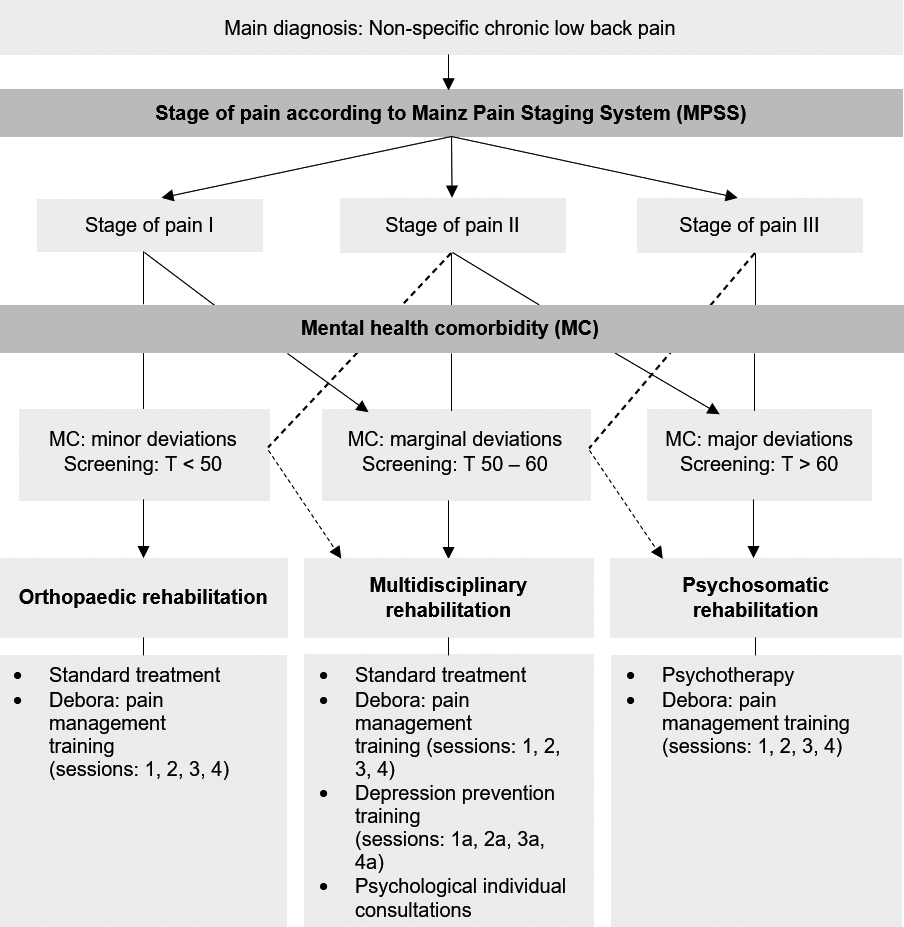
Figure 2.
Stepped care model.
4.2Limitations
The strengths of the present multicentre study, apart from the study design with cluster block randomisation and the sample size of 526 patients with CLBP, are above all the additional consideration of the stage of pain in the longitudinal section. Nevertheless, the study also has limitations, which are listed below.
First, the present study showed a high dropout rate until the 12-month follow-up assessment. However, dropout analyses revealed an equal distribution of patients who dropped out across the treatment condition. Thus, systematic effects can be excluded. Additionally, no significant differences between patients who dropped out and participants who stayed in the study depending on the treatment condition were detected. This means that participants in the intervention group did not drop out significantly more often than participants in the control group. Nevertheless, patients who dropped out and participants who stayed in the study significantly differed in terms of age, pain duration, gender, family status and net household income. However, analyses after MI confirmed almost all significant results of the PP analyses. Therefore, neither systematic effects nor an overestimation of the long-term effects from the PP analyses were supported. Due to the high dropout rate, it can be suspected that Little’s MCAR-test for MI [34] became significant (2 (5302)
Second, the majority of patients in the present sample indicated a higher level of education. The results are limited to patients with similar sample characteristics. However, former studies ascertained unfavourable effects of cognitive-behavioural pain management trainings for patients with CLBP and a lower educational level (cf. [17, 36]).
4.3Clinical implications
Overall, the current results confirm that pain management trainings with cognitive-behavioural elements such as Debora and previous programmes [11, 12] are effective in the long-term. Moreover, a high stage of pain had a negative influence on the long-term success of rehabilitation. Therefore, early identification of psychosocial risk factors (yellow flags) and of the stage of pain among patients with CLBP are important (cf. [37]).
Based on the current results, a stepped care model for patients with CLBP was developed to adequately supply each subgroup [21, 26, 38] (Fig. 2). According to this allocation model, i) orthopaedic rehabilitation is recommended if patients with CLBP are in stage of pain I and a screening of mental comorbidities shows subclinical scores (
In contrast, ii) multidisciplinary rehabilitation should be chosen if patients are in stage of pain I or II and borderline mental health is diagnosed (T 50–60). In this subgroup, additional psychological treatment elements in multidisciplinary rehabilitation could address the moderate psychosocial impairments of patients with CLBP and may prevent further persistence. A multidisciplinary rehabilitation is also recommended for patients who do not yet have a mental comorbidity (
Finally, iii) psychosomatic rehabilitation is recommended for patients with CLBP in stage of pain II and III and mental comorbidities (screening result:
5.Conclusions
In summary, the present results show that patients in stage of pain I and II benefited from rehabilitation at the 6- and 12-month follow-up assessments in depressive symptoms, anxiety, mental health, and the average pain intensity, both statistically and clinically. Patients in stage of pain III showed lower beneficial effects in the mid-term and were able to maintain significant improvements only in anxiety 12 months after rehabilitation. Accordingly, the presented stepped care model for CLBP is necessary to prevent the development of mental disorders and the persistence of CLBP in stage of pain I and II. Simultaneously, there is a high need for more psychological treatments among patients in stage of pain III. Thus, the present study further elucidated the important role of the stages of pain and co-existing psychological symptoms for the treatment of patients with CLBP and contributes to the improvement of subgroup-specific treatment success and the prevention of further chronification of pain.
Conflict of interest
None declared.
Funding
This work was supported by the Deutsche Rentenversicherung Bund (German Pension Insurance) under grant 8011–106–31/31.115.
References
[1] | Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Genevay S, Hoy D, et al. What low back pain is and why we need to pay attention. Lancet. (2018) ; 391: : 2356–67. doi: 10.1016/S0140-6736(18)30480-X. |
[2] | Pincus T, McCracken LM. Psychological factors and treatment opportunities in low back pain. Best Pract Res Clin Rheumatol. (2013) ; 27: : 625–35. doi: 10.1016/j.berh.2013.09.010. |
[3] | Hasenbring M, Chehadi O, Titze C, Kreddig N. Fear and anxiety in the transition from acute to chronic pain: There is evidence for endurance besides avoidance. Pain Management. (2014) ; 4: : 363–74. |
[4] | Puschmann A-K, Drießlein D, Beck H, Arampatzis A, Moreno Catalá M, Schiltenwolf M, et al. Stress and self-efficacy as long-term predictors for chronic low back pain: A prospective longitudinal study. J Pain Res. (2020) ; 13: : 613–21. doi: 10.2147/JPR.S223893. |
[5] | Martinez-Calderon J, Flores-Cortes M, Morales-Asencio JM, Luque-Suarez A. Which psychological factors are involved in the onset and/or persistence of musculoskeletal pain? An umbrella review of systematic reviews and meta-analyses of prospective cohort studies. Clin J Pain. (2020) ; 36: : 626–37. doi: 10.1097/AJP.0000000000000838. |
[6] | Foster NE, Anema JR, Cherkin D, Chou R, Cohen SP, Gross DP, et al. Prevention and treatment of low back pain: Evidence, challenges, and promising directions. Lancet. (2018) ; 391: : 2368–83. doi: 10.1016/S0140-6736(18)30489-6. |
[7] | McParland JL, Andrews P, Kidd L, Williams L, Flowers P. A scoping review to ascertain the parameters for an evidence synthesis of psychological interventions to improve work and wellbeing outcomes among employees with chronic pain. Health Psychology and Behavioral Medicine. (2021) ; 9: : 25–47. doi: 10.1080/21642850.2020.1863809. |
[8] | Kamper SJ, Apeldoorn AT, Chiarotto A, Smeets RJ, Ostelo RWJG, Guzman J, van Tulder MW. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ. (2015) ; 350: : 1–11. doi: 10.1136/bmj.h444. |
[9] | Linton SJ, Nordin E. A 5-year follow-up evaluation of the health and economic consequences of an early cognitive behavioral intervention for back pain: A randomized, controlled trial. Spine. (2006) ; 31: : 853–8. |
[10] | You DS, Ziadni MS, Cooley CE, Talavera DC, Mackey SC, Poupore-King H. Effectiveness of a multidisciplinary rehabilitation program in real-world patients with chronic back pain: A pilot cohort data analysis. J Back Musculoskelet Rehabil. (2021) . doi: 10.3233/BMR-200305. |
[11] | van Hooff ML, van der Merwe, Johannes D, O’Dowd JK, Pavlov PW, Spruit M, de Kleuver M, van Limbeek J. Daily functioning and self-management in patients with chronic low back pain after an intensive cognitive behavioral programme for pain management. Eur Spine J. (2010) ; 19: : 1517–26. doi: 10.1007/s00586-010-1435-5. |
[12] | van Hooff ML, ter Avest W, Horsting PP, O’Dowd JK, de Kleuver M, van Lankveld W, van Limbeek J. A short, intensive cognitive behavioral pain management program reduces health-care use in patients with chronic low back pain. Eur Spine J. (2012) ; 21: : 1257–64. doi: 10.1007/s00586-011-2091-0. |
[13] | Mangels M, Schwarz S, Worringen U, Holme M, Rief W. Evaluation of a behavioral-medical inpatient rehabilitation treatment including booster sessions. Clinical Journal of Pain. (2009) ; 25: : 356–64. doi: 10.1097/AJP.0b013e3181925791. |
[14] | Meng K, Peters S, Faller H. Effectiveness of a standardized back school program for patients with chronic low back pain after implementation in routine rehabilitation care. Patient Educ Couns. (2017) ; 100: : 1161–8. doi: 10.1016/j.pec.2017.01.011. |
[15] | Semrau J, Hentschke C, Buchmann J, Meng K, Vogel H, Faller H, et al. Long-term effects of interprofessional biopsychosocial rehabilitation for adults with chronic non-specific low back pain: A multicentre, quasi-experimental study. PLoS One. (2015) ; 10: : e0118609. doi: 10.1371/journal.pone.0118609. |
[16] | Hampel P, Tlach L. Cognitive-behavioral management training of depressive symptoms among inpatient orthopedic patients with chronic low back pain and depressive symptoms: A 2-year longitudinal study. J Back Musculoskelet Rehabil. (2015) ; 28: : 49–60. doi: 10.3233/BMR-140489. |
[17] | Tlach L, Hampel P. Long-term effects of a cognitive-behavioral training program for the management of depressive symptoms among patients in orthopedic inpatient rehabilitation of chronic low back pain: A 2-year follow-up. Eur Spine J. (2011) ; 20: : 2143–51. doi: 10.1007/s00586-011-1810-x. |
[18] | Mohr B, Korsch S, Roch S, Hampel P. Debora – Trainingsmanual Rückenschmerzkompetenz und Depressionsprävention [Debora – manual of pain competence and depression prevention training]. Berlin: Springer; (2017) . |
[19] | Hampel P, Köpnick A, Roch S. Psychological and work-related outcomes after inpatient multidisciplinary rehabilitation of chronic low back pain: A prospective randomized controlled trial. BMC Psychology. (2019) ; 7: : 6. doi: 10.1186/s40359-019-0282-3. |
[20] | Mohr B, Krohn-Grimberghe B, Gräf T, Schulze J, Petermann F, Hampel P. Patienten mit chronisch unspezifischem Rückenschmerz: Zur Bedeutung psychosozialer Merkmale. [Patients with chronic low back pain: The impact of psychosocial features]. Rehabilitation. (2009) ; 48: : 288–97. doi: 10.1055/s-0029-1239551. |
[21] | van Tulder MW, Ostelo R, Vlaeyen JW, Linton SJ, Morley SJ, Assendelft WJ. Behavioral treatment for chronic low back pain: A systematic review within the framework of the Cochrane Back Review Group. Spine. (2000) ; 25: : 2688–99. doi: 10.1097/00007632-200010150-00024. |
[22] | Linton SJ, Kienbacher T. Psychological subgrouping to assess the risk for the development or maintenance of chronic musculoskeletal pain: Is this the way forward? Clin J Pain. (2020) ; 36: : 172–7. doi: 10.1097/AJP.0000000000000787. |
[23] | Gerbershagen HU. Konzept einer multidisziplinären Schmerzklinik [Concept of a multidisciplinary pain clinic]. Anasthesiol Intensivmed Notfallmed Schmerzther. (1992) ; 27: : 377–80. |
[24] | Pfingsten M, Schöps P, Wille T, Terp L, Hildebrandt J. Chronifizierungsausmaß von Schmerzerkrankungen: Quantifizierung und Graduierung anhand des Mainzer Stadienmodells [Chronification extent of pain diseases: Quantification and graduation using the Mainz Pain Staging Model]. Schmerz. (2000) ; 14: : 10–7. |
[25] | Zhuk A, Schiltenwolf M, Neubauer E. Langfristige Wirksamkeit einer multimodalen Schmerztherapie bei chronischen Rückenschmerzen. [Long-term efficacy of multimodal pain therapy for chronic back pain]. Nervenarzt. (2018) ; 89: : 546–51. doi: 10.1007/s00115-017-0391-2. |
[26] | Ljutow A, Nagel B. Wie schätze ich die Rückenschmerzsituation meines Patienten ein? Die Mainzer Chronifizierungsstadien und ihre prognostische Bedeutung. [How can I assess the back pain status in my patients? The Mainz chronic disease staging method and its prognostic value]. Z Orthop Ihre Grenzgeb. (2005) ; 143: : 311–5. doi: 10.1055/s-2005-836634. |
[27] | Campbell MK, Piaggio G, Elbourne DR, Altman DG. Consort 2010 statement: Extension to cluster randomised trials. BMJ. (2012) ; 345: : e5661. doi: 10.1136/bmj.e5661. |
[28] | Hautzinger M, Bailer M, Hofmeister D, Keller F. Allgemeine Depressionsskala [Center for Epidemiological Studies Depression Scale (CES-D)]. 2nd ed. Göttingen: Hogrefe; (2012) . |
[29] | Herrmann-Lingen C, Buss U, Snaith RP. HADS-D Hospital Anxiety and Depression Scale – Deutsche Version Deutsche Adaptation der Hospital Anxiety and Depression Scale German Version. 3rd ed. Bern: Hans Huber; (2011) . |
[30] | Franke GH. Mini-SCL: Mini-Symptom-Checklist. Göttingen: Hogrefe; (2017) . |
[31] | Morfeld M, Kirchberger I, Bullinger M. SF-36 Fragebogen zum Gesundheitszustand: Deutsche Version des Short Form-36 Health Survey [SF-36 Health Status Questionnaire: German Version of the Short Form-36 Health Survey]. 2nd ed. G?ttingen: Hogrefe; (2011) . |
[32] | Nagel B, Pfingsten M, Lindena G, Kohlmann T. Deutscher Schmerz-Fragebogen: Handbuch [German Pain Questionnaire: Manual]. Berlin: Deutsche Schmerzgesellschaft e.V.; (2015) . |
[33] | Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. New York: Academic Press; (1988) . |
[34] | Little RJA. A test of missing completely at random for multivariate data with missing values. Journal of the American Statistical Association. (1988) ; 84: : 1198–202. |
[35] | Gerrits MMJG, van Oppen P, van Marwijk HWJ, Penninx BWJH, van der Horst HE. Pain and the onset of depressive and anxiety disorders. Pain. (2014) ; 155: : 53–9. doi: 10.1016/j.pain.2013.09.005. |
[36] | Dhondt E, van Oosterwijck J, Cagnie B, Adnan R, Schouppe S, van Akeleyen J, et al. Predicting treatment adherence and outcome to outpatient multimodal rehabilitation in chronic low back pain. J Back Musculoskelet Rehabil. (2020) ; 33: : 277–93. doi: 10.3233/BMR-181125. |
[37] | Nicholas MK, Linton SJ, Watson PJ, Main CJ. Early identification and management of psychological risk factors (“yellow flags”) in patients with low back pain: A reappraisal. Phys Ther. (2011) ; 91: : 737–53. doi: 10.2522/ptj.20100224. |
[38] | van Wambeke P, Desomer A, Jonckheer P, Depreitere B. The Belgian national guideline on low back pain and radicular pain: Key roles for rehabilitation, assessment of rehabilitation potential and the PRM specialist. Eur J Phys Rehabil Med. (2020) ; 56: : 220–7. doi: 10.23736/S1973-9087.19.05983-5. |


