
Lumbar instability as an etiology of low back pain and its treatment by prolotherapy: A review
Abstract
BACKGROUND:
Low back pain is a significant spinal disorder that affects much of the population at some point during their lives.
OBJECTIVE:
While proper diagnosis is key, diagnosing the underlying cause of low back pain may often be unclear.
METHOD:
In this review article, we discuss lumbar instability as an etiology of low back pain and its treatment by prolotherapy.
RESULTS:
Spinal ligaments may be an underlying culprit in the development of lumbar instability with resultant low back pain and associated disorders.
CONCLUSION:
In these cases, adequate treatment consisting of non-biologic prolotherapy or cellular prolotherapy, including platelet rich plasma (PRP), can be beneficial in restoring spinal stability and resolving chronic low back pain.
1.Introduction
1.1Background
Low back pain is the most common spinal disorder, with more than one-half of the U.S. population living with chronic pain, and approximately 80% affected by chronic pain at some point in their lives [1, 2]. In the most recent Global Burden of Disease Study, low back pain was the leading cause of years lived with disability [1]. Those with acute low back pain who lack proper diagnosis and treatment are at risk for developing chronic pain, which predisposes them to high rates of disability, limiting their ability to participate in everyday activities and reducing their quality of life. About 20% of people who have had acute low back pain develop chronic low back pain when symptoms continue to persist at one year [3]. Low back pain is typically associated with spondylosis, an umbrella term that refers to the progressive degeneration of the spine and affects the joints, discs, and bones therein. Most low back pain is mechanical in nature and can be caused by any of the following conditions: sprains and strains, intervertebral disc degeneration, herniated or ruptured discs, radiculopathy, sciatica, spinal stenosis, spondylolisthesis, trauma, and scoliosis, as well as an abnormal lordotic curve [4].
In the United States, spinal problems of the back and neck are the most common musculoskeletal conditions to cause limitations in activities of daily living (ADL) in young adults [5]. The number of all-age years lived with disability (YLDs) attributable to low back pain has increased 17.5% since 2007. Low back pain was the leading cause of YLDs in 126 of the 195 countries and territories surveyed [6]. Such a high and sustained YLD figure for low back pain is becoming a cause of concern since it represents the potential loss of a functioning workforce and a greater population of non-wage earners [7]. Previously, the United States Bone and Joint Initiative had reported that nearly 26% of those adults (age 18 or older) who said they were unable to work due to a health condition also attributed it to chronic back or neck problems. In 2013, low back pain was the diagnosis recorded in nearly 62 million healthcare visits [8].
Although 3 out of 4 of these visits were to a physician’s office, more than 2.3 million patients with low back pain were hospitalized and almost 10 million were treated in the emergency department [ibid]. For the years 2012-2014, the annual direct medical costs for all persons with a back-related condition was estimated at $315 billion per year (in 2014 dollars), but this figure does not include costs associated with chiropractic care, physical therapy, alternative therapy (e.g., prolotherapy), or outpatient clinics, and is therefore grossly underestimated [1]. Globally, low back pain is ranked #1 as the leading cause of YLDs for both males and females, and has been so for the past 27 years, reflecting the lack of progress in addressing this type of pain [9, 10].
1.2Stabilizers of the lumbar spine
The spine acquires its stability from the intervertebral discs (IVDs), and the surrounding ligaments and muscles, with the discs and ligaments providing intrinsic stability, and the muscles, extrinsic support. In the lumbar spine, there are 5 vertebrae (L1–L5); rarely, some people have 6. The lower back is formed by the lumbar spine and the beginning of the sacral spine (S1), which is why it is important to examine the sacroiliac joints when a patient complains of persistent low back pain.
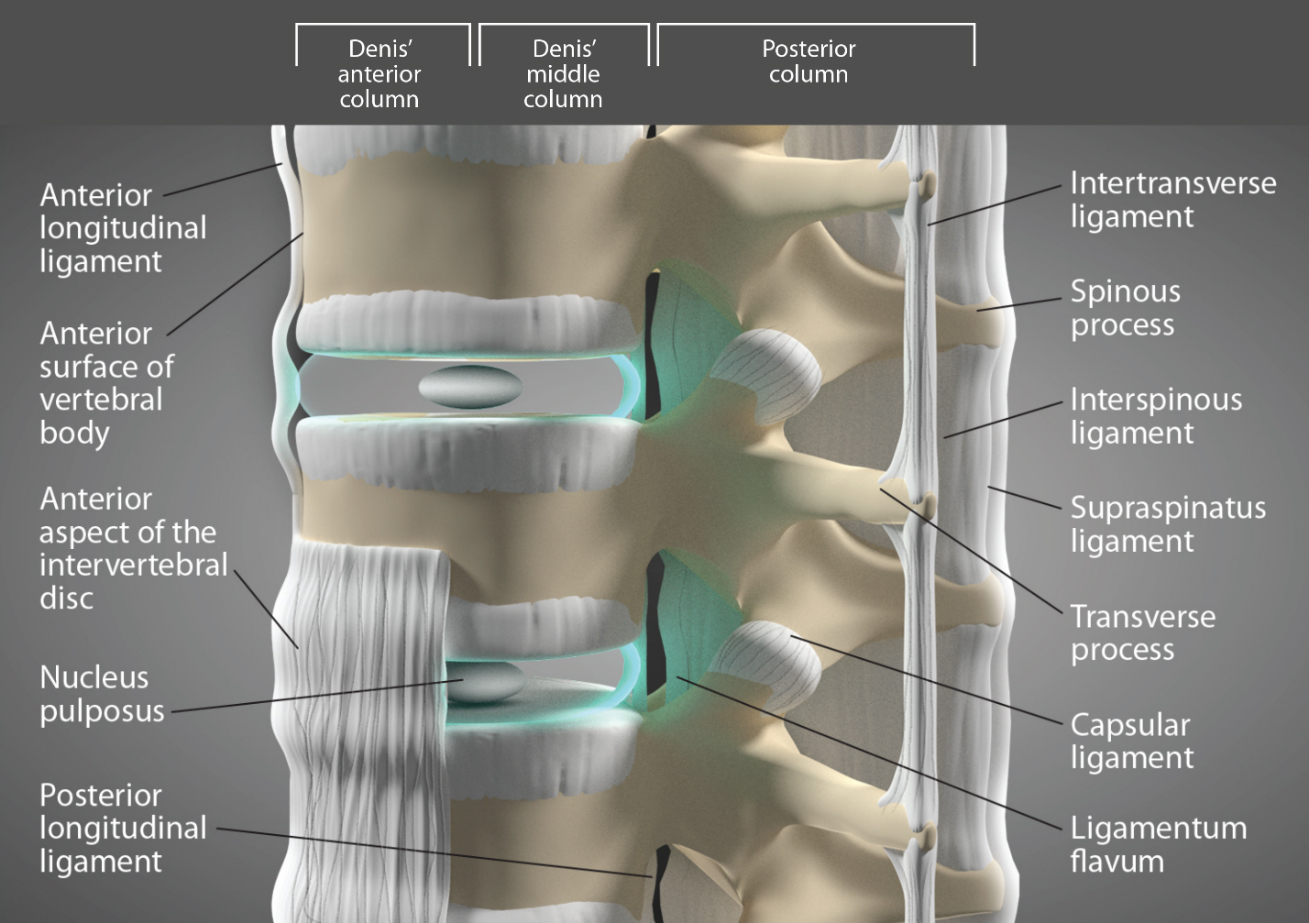
The Denis model divides the spine into 3 columns. The first column is made up of the anterior longitudinal ligament and the front half of the vertebral body and disc; the middle column consists of the back half of the vertebral body and disc, plus the posterior longitudinal ligament; and the third (posterior) column is made up of the facet joints, the ligamentum flavum, and the interconnecting ligaments of the posterior elements (see Fig. 1). The sacrum and its surrounding ligaments form a foundation of structural integrity for both the lumbar spine and posterior pelvic ring, allowing a seamless transition of force from the upper body to the lower extremities [11]. Although the spine is still usually considered stable when only one of the columns has been disrupted, this may not remain so because any looseness of the ligaments in the posterior column can act as a springboard for degeneration of a second column.
Figure 1.
The Denis model of the lumbar spine divides the spine into 3 columns.
Activity- and age-related low back problems do not typically arise immediately after a traumatic event, but instead begin to develop once ligaments start to creep (tendency to slowly elongate) after prolonged stretching. This creeping behavior is the result of the forward motions engrained in the human lifestyle. Our days are spent bending to tie our shoes or pick items up, lifting to carry objects or hold our children, twisting to play sports or go skiing, and sitting (or slouching) to drive, read, talk, or text on cell phones, and use computers at work and home. We all either perform or assume these everyday motions and stationary postures without giving them a second thought, but they can lead to gradual loosening of the posterior ligamentous complex (PLC) over time.
What then are the overriding effects of gradual loosening of the ligaments in the lower back? Our bodies are remarkably intuitive in sensing when something has gone awry, especially when it concerns a vital structure like the spine, and responds by adopting other measures to maintain the spine’s stability. Muscle spasms may develop along the spine generated by the ligamento-muscular reflex, whereby the stretched ligaments rapidly react by signaling the muscles over top of them to squeeze and spasm to prevent the spine from destabilizing. The body also responds to joint instability by causing joint swelling, paraspinal muscle tightening or osteophytes (bone spurs), all of which may help to decrease the force per unit area on the (facet) joints. By doing so, the body temporarily stabilizes the joints. With this said, the body’s overall reaction to the worsening of ligament laxity and instability in the lower spine is to initiate both degenerative and growth mechanisms (balance of anabolic and catabolic events) as protective measures.
1.3Causes of low back pain
Non-specific low back pain is a leading contributor to disease burden worldwide and affects people of all ages [12]. When the etiology of the pain is unknown, or a person is given an inaccurate diagnosis, unnecessary spinal surgeries or other invasive procedures are more likely to occur, and the overuse of opioids and imaging will continue to be a widespread problem. Cost analyses over the last decade have born this out with monumental figures, indicating a 629% increase in Medicare expenditures for epidural steroid injections; a 423% increase in expenditures for opioids related to back pain; a 307% increase in the number of lumbar MRIs among Medicare beneficiaries; and a 220% increase in spinal fusion surgery rates [13]. Diagnosing a person’s low back pain can be difficult to determine since the lumbar spine, like the body itself, consists of many components capable of generating pain and does so via a set of complex pain patterns [14].
Figure 2.
Ligament referral pain patterns from structures in the lower back and hip.
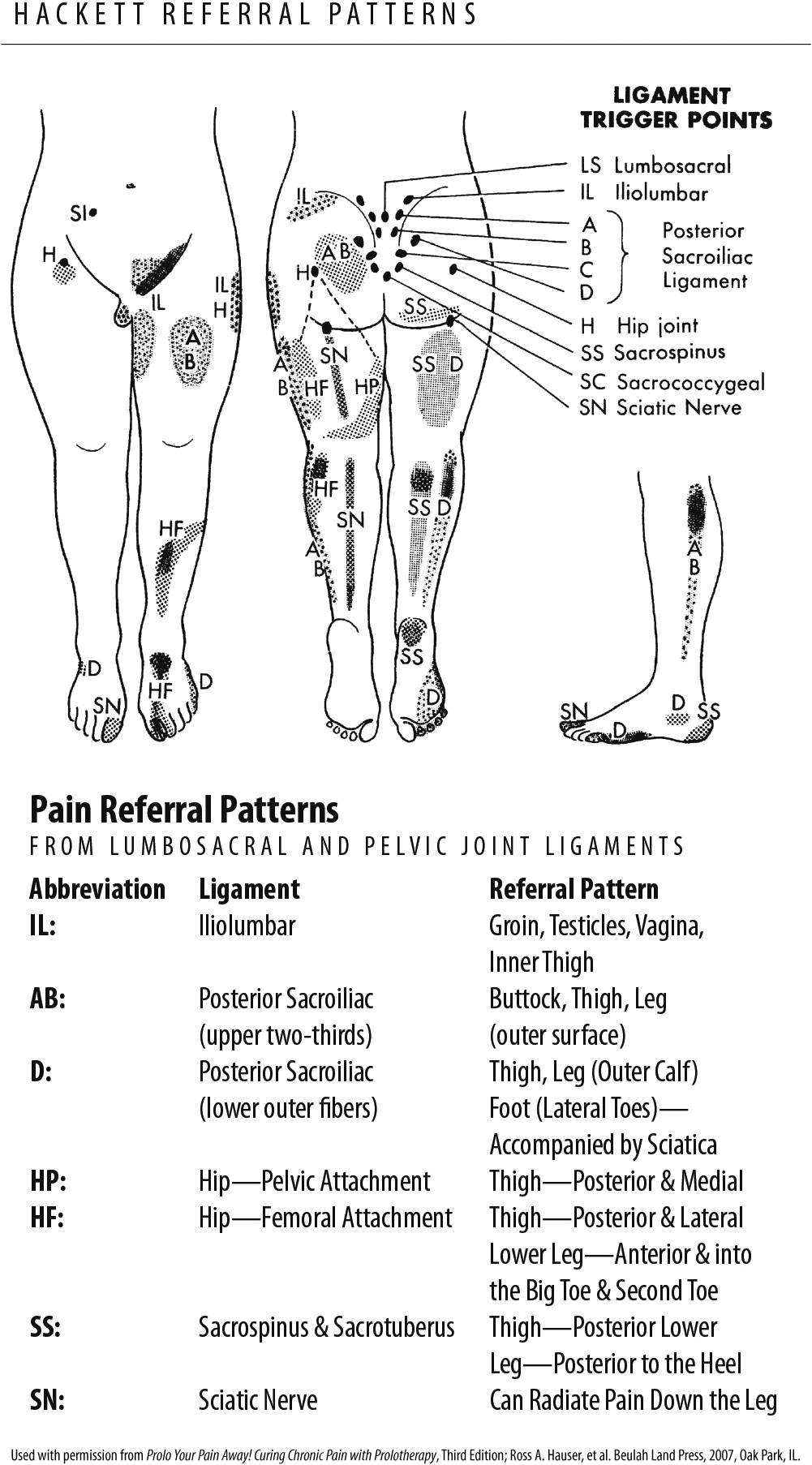
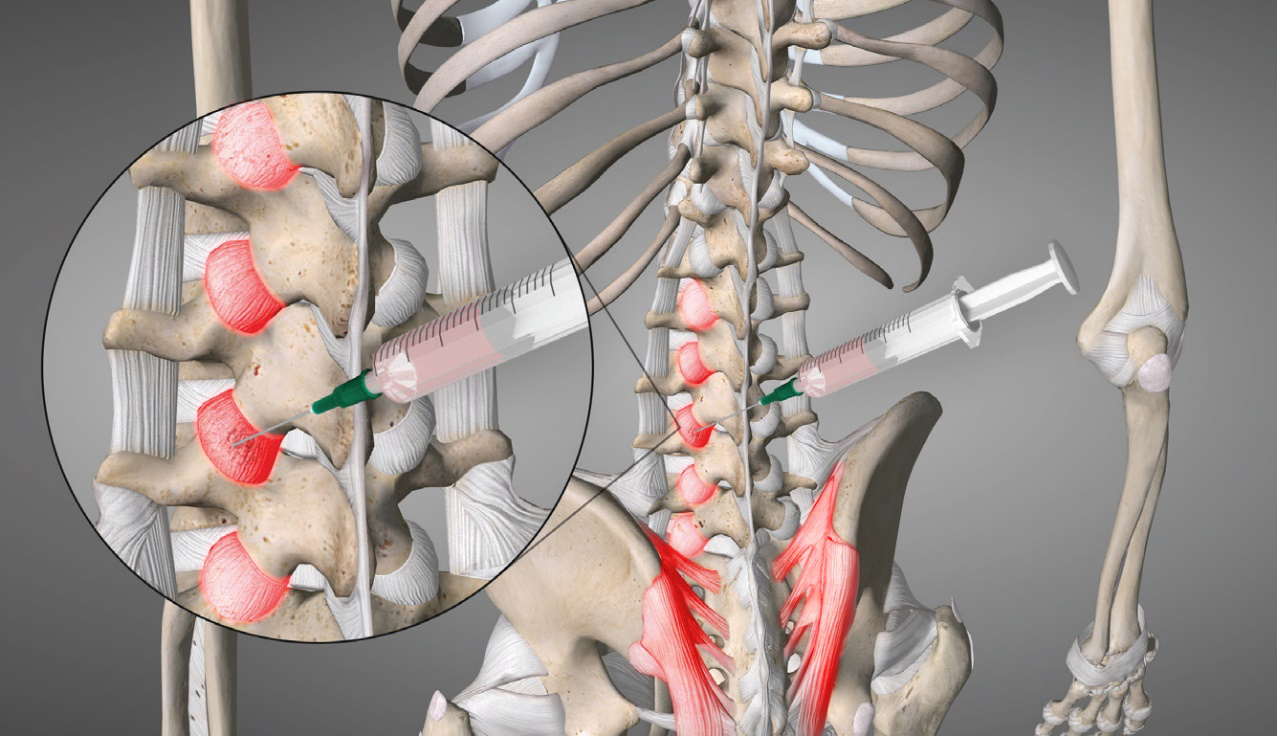
Figure 3.
Prolotherapy treatment for the low back may involve injections to the capsular, sacroiliac, and/or other ligaments and entheses.
George Hackett, MD, who coined the term prolotherapy, was the first to describe the referral pain patterns of injury to the sacroiliac ligaments, which mimicked those of sciatica (see Fig. 2). Stabilization of the sacroiliac joints is one of the successful ways that prolotherapy treats chronic low back pain. Modern medicine typically prescribes medications for chronic back ailments that only serve to mask the pain instead. In a systematic review of disc degeneration, Phillips and colleagues have questioned this tactic, countering back by stating, “The causes of lower back pain are rarely addressed” [15]. We believe the authors were right on target and contend that when a spinal vertebral motion segment becomes dysfunctional and chronic pain develops, it is almost always due to instability caused by ligament laxity, which could be resolved with either comprehensive or cellular prolotherapy.
2.Method
2.1Prolotherapy
Prolotherapy is a regenerative injection treatment that uses various biological substances to initiate an inflammatory healing cascade, mimicking the body’s own response to repairing musculoskeletal injuries. Prolotherapy treatments can be either non-cellular based (d-glucose/hypertonic dextrose) or cellular-based (platelet rich plasma [PRP] and mesenchymal signaling cells/stem cells), the former of which is obtained via a venous blood draw, and the latter via a small volume liposuction or bone marrow harvesting. In the United States, the practice of regenerative medicine, including prolotherapy, is currently limited to using autologous mesenchymal stem cells, which must be obtained and used during the same procedure with little manipulation [16]. Generally, cellular-based prolotherapy is reserved for more severe cases of ligament damage/instability and spinal joint degeneration.
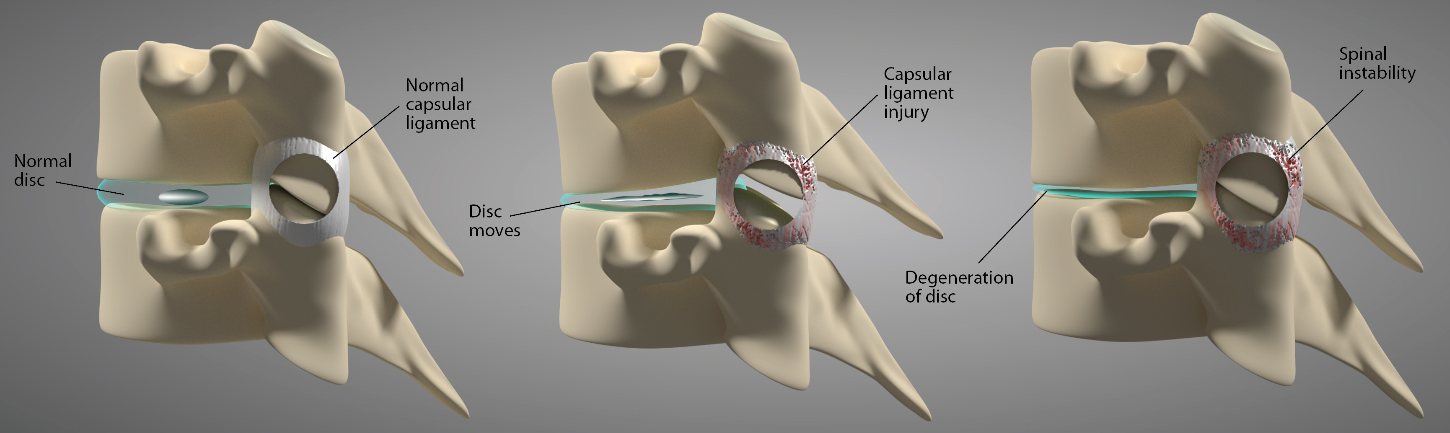
Figure 4.
Capsular ligament injury leads to the development of spinal instability, which can give rise to disc protrusions and eventual disc degeneration in the process.
Various methods of prolotherapy can be used to treat lumbar instability and its consequent pain syndromes; to provide relief expeditiously, however, the administered treatment should be tailored to each individual patient, depending upon confirmation of their diagnosis and primary pain generator. Pain sources include the lumbar facet joints and their capsular ligaments, over-pressured or deranged intervertebral discs resulting from lumbar instability, and sacroiliac and iliolumbar ligaments (see Fig. 3).
2.2Facet joints and their contribution to lumbar instability and low back pain
The facet joints are considered a crucial anatomic region and stabilizer of the spine because they play an important role in load transmission, acting as the posterior load-bearing component for stabilizing the motion segment in flexion and extension while restricting axial rotation. Together with the intervertebral disc, the facet joints transfer loads and guide and constrain motions in the spine. This mechanical behavior and its specialized geometry and biomechanics are meant to ensure the normal health and function of the spine during physiologic loading, but this behavior can lead to joint dysfunction if the tissues within the facet joints are altered by injury, degeneration, or spinal surgery (e.g., disc repair or replacement), which can disrupt facet responses [17]. Typical degenerative changes that occur in response to ligament injuries in the facet joints include cartilage degradation followed by joint space narrowing and sclerosis of the subchondral bone [18].
The lumbar spine is considered unstable if abnormal strains or excessive motion develop in the functional spinal unit, a structure that contains the bodies of the upper and lower vertebrae and the IVD between them, as well as the facet joints, which join the vertebrae together. The functional spinal unit is surrounded by ligaments, including the PLC, which are crucial for maintaining spinal stability. The PLC is made up of the supraspinous ligament, interspinous ligament, ligamentum flavum, and the facet capsule ligaments. The roles of the PLC are to limit excess motion and resist bending and compressive forces. This second function is particularly important, as demonstrated in a study that found intradiscal pressure increases greatly during sitting, lifting, or forward leaning, alone or with twisting, the latter of which involves shear forces that the PLC is ill-equipped to handle. All these motions were found to trigger the loading of such forces onto the PLC [19]. Should the PLC become injured or unable to resist those forces, the lumbar disc would become a pain generator. Other important ligaments surrounding the functional spinal unit are the intertransverse ligament, the anterior longitudinal ligament, and the posterior longitudinal ligament.
Studies have evaluated the effects when various ligaments of the PLC become dysfunctional. For instance, the removal of the facet joint capsular ligaments in the lower lumbar spine causes a large increase in pressure within an otherwise healthy lumbar disc, [20] and cutting these ligaments in the upper lumbar spine causes an increase in side-to-side bending motion [21]. While the lumbar disc and the facet joints are both common pain generators, the facet joint capsular ligaments are arguably the most critical starting point in the development of lower back disorders. This is so because their injury would result in increases in shear forces (side-to-side motion), thereby increasing the likelihood that instability would occur, along with subsequent facet joints and lumbar disc degeneration. It should be noted that the facet joints and interspinous ligaments are the first to be injured under degenerative conditions (see Fig. 4). While the entire PLC is treated in comprehensive prolotherapy, it is the lumbar facet joint capsular ligaments that are targeted.
Although facet joint pain can account for up to 45% of low back pain [18], there are few randomized controlled studies in the literature on the use of comprehensive or cellular prolotherapy for treating this type of pain. Narrative and systematic reviews, as well as meta-analysis, noted overall positive results, especially with cellular prolotherapy, but mixed with noncellular prolotherapy for chronic low back pain [22, 23, 24, 25]. Currently, standard medical care remains focused on masking facet joint pain instead of diagnosing and treating the real cause, which is joint instability. Historically, treatment options have included oral NSAIDs and physical therapy, as well as more invasive interventions such as facet joint corticosteroid injections, diagnostic nerve blocks to the facet joints, and radiofrequency ablation of the sensory nerves supplying the joints if the diagnostic block is positive.
3.Results
3.1Prolotherapy and PRP for facet joint pain
A single-blind, randomized, crossover study evaluated the effectiveness of injection therapy in 35 patients diagnosed as having painful enthesopathies as a major pain generator. Of the patients studied, 86% had undergone prior spinal surgery, and all had been referred to a neurosurgeon to see if more surgery was needed. Patients were injected with either anesthetics alone or with anesthetics combined with a phenol-glycerol proliferant (prolotherapy), for a total of 86 injections. Out of this group, 39 patients were treated with local anesthetics alone, and 47 with prolotherapy. Outcomes were done clinically at regular follow-ups, and subjectively by a series of questionnaires. Clinical assessment revealed 80% of patients had excellent to good relief of pain and tenderness when prolotherapy injections were given, but only 47% of patients given anesthetics alone had the same amount of pain relief. Of the questionnaire responses, 66% reported excellent to good pain relief after prolotherapy vs. 34% after anesthetics alone. Patients in both groups reported improvements in work capacity and social functioning, but patients who received prolotherapy injections had a greater reduction in focal pain intensity than those with anesthetics alone. In the crossover portion of the study, patients who had been in the anesthetics alone group reported they had much better pain relief after getting prolotherapy injections. Those who had been in the initial prolotherapy group said the anesthetic-only injections failed to provide as much pain relief. The authors concluded that prolotherapy injections to painful enthesopathies provide substantial relief from axial pain and tenderness along with functional improvement, even in cases of “failed back [surgery] syndrome” [26].
A study into the use of PRP for facet joint pain examined the results of guided injections of PRP into the lumbar facet joints of 19 patients. The study found that PRP had beneficial effects which improved over time, with 15 of the 19 patients experiencing significant pain reduction by 3 months [21]. In a subsequent randomized prospective study with a larger cohort of 46 subjects, the same lead author compared the results of facet joint injections using either PRP or anesthetic and corticosteroid. At the 1-month mark, 80% of subjects in the corticosteroid group were satisfied with the results of the procedure, but this declined to between 20% and 50% after 6 months. Conversely, the subjects in the PRP group had an increase in satisfaction over time, leading the authors to conclude that PRP was the superior treatment [22]. As the facet joint capsular ligaments loosen, the spinal segments begin to flex (bend forward) more, though imperceptibly to us, when a person leans forward, sits, or lifts. Over time, this results in several possible adaptations, the first of which is disc degeneration (see Fig. 5).
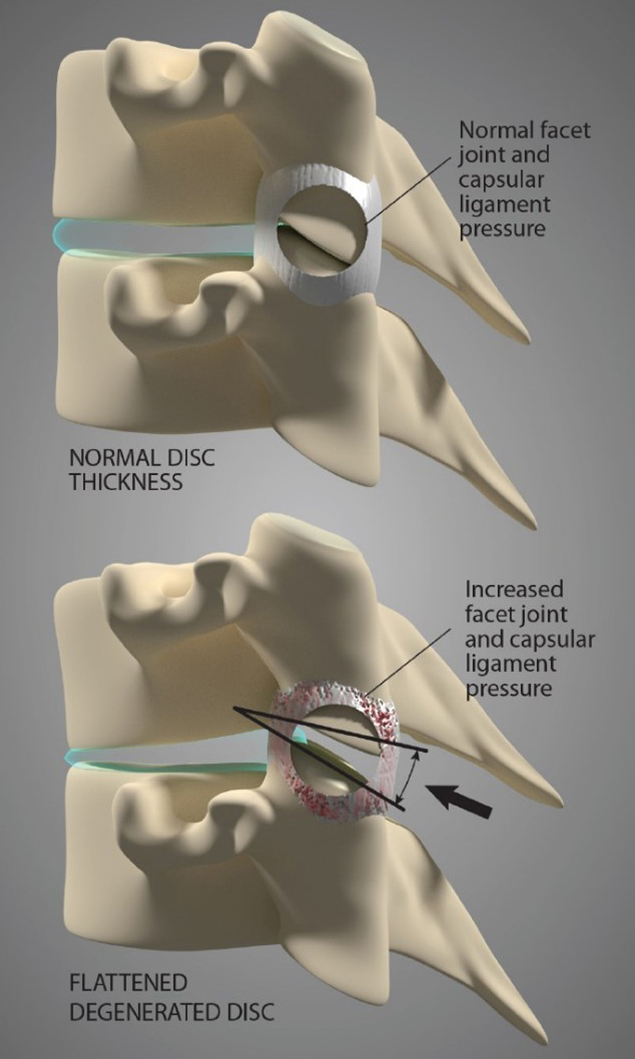
Figure 5.
As the facet joint capsular ligaments loosen, the spinal segments begin to flex more during normal motions. Over time, this will increase pressure in the facet joint(s), as well as accelerate degeneration of the intervertebral disc(s).
3.1.1Disc degeneration as a consequence of lumbar instability
According to the National Institutes of Health (NIH), disc degeneration remains a key cause of chronic low back pain [3] and is thought to be the initiator of degeneration in the spine. This process is believed to result in segmental instability, which in turn increases the load on the facet joints and leads to cartilage alterations. On the reverse, when there is too much motion (due to joint hypermobility or instability from ligament laxity) in the posterior pillar at the facet joints, undue pressure will be exerted on the disc, potentially leading to disc herniation or degeneration.
When the spine is axially loaded, the exterior rim of the IVD can bulge at the periphery. If a person is bending forward, the disc normally bulges posteriorly, but if the person is leaning toward the right, the disc bulges laterally to the left. In other words, the disc bulges normally with movement and thus is not painful. When an MRI shows bulging discs as the main finding, it usually has no clinical significance. If the axial forces are applied over too long a period, however, the disc will not regain its original length and width, even when accounting for recovery time. This could happen, should the PLC become loose due to creep. Every time the person bends or sits thereafter, the loosened ligaments will cause the bony vertebrae to slip or tilt forward and squeeze the front of the lumbar disc more than usual, resulting in a backward bulge [27]. It should therefore be unsurprising that disc pressures are higher when spinal instability is present. When the disc degeneration is long-standing and severe, it can put even more stress on the facet joints, worsening the spinal instability, and ultimately becoming a causative factor in the development of spinal osteoarthritis (see Fig. 6).
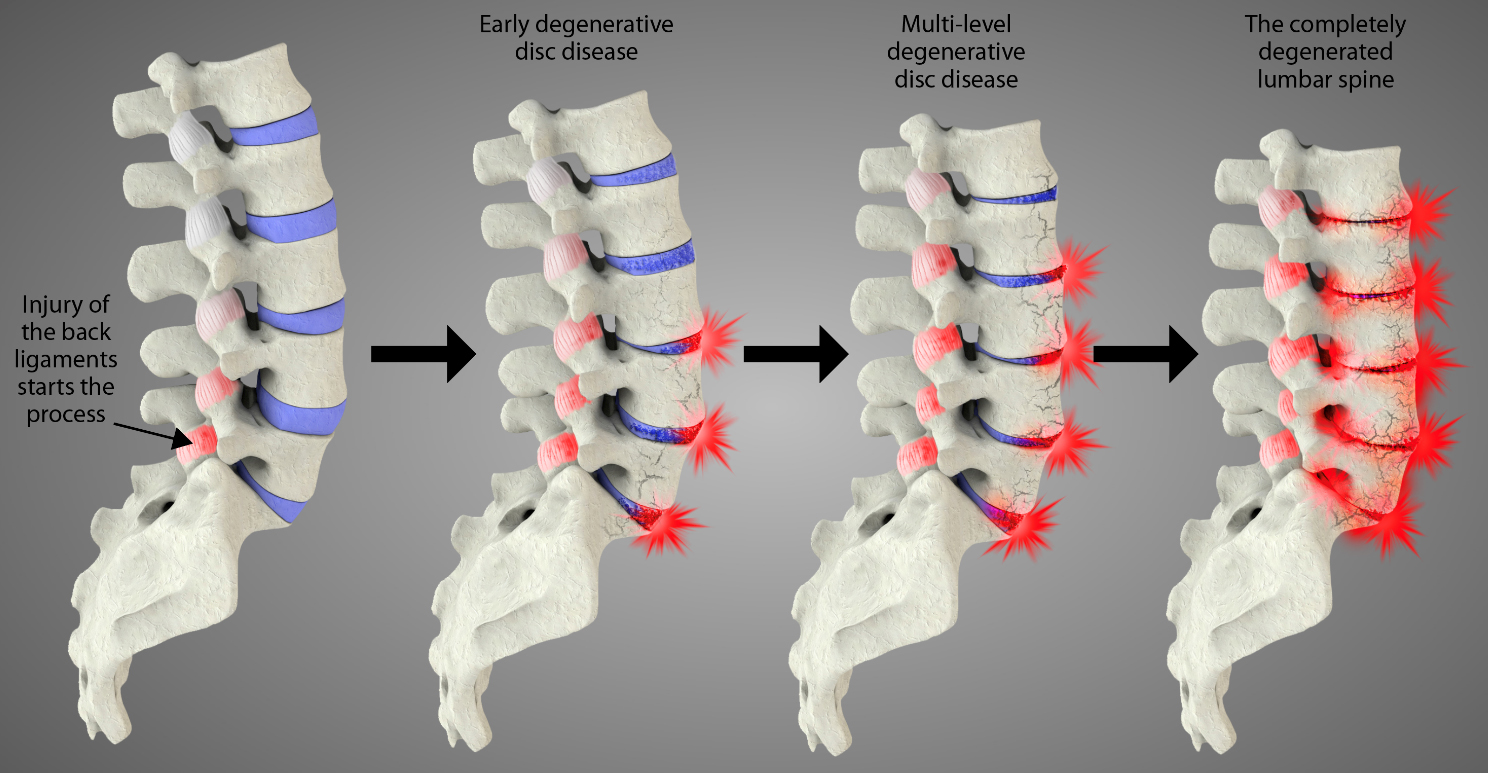
Figure 6.
The progression of degeneration in the lower back starts with an initial injury to one or more spinal ligaments. Over time, the process progresses to involve more spinal segments. Eventually, unresolved spinal instability can cause multi-level degeneration of the lumbar spine.
Discogenic back pain is without a clear source, although it is thought to originate from the intravertebral disc and the associated structures of the motion segment (i.e., facet joints, ligaments, and spinal muscles). The degenerative changes that occur in the disc and the structural defects that ensue in surrounding tissues result in biomechanical instability and inflammation.
Although many treatments and interventions have been explored for disc degeneration, all have had drawbacks. Treatment options such as pain medications, steroid injections, discectomies, and spinal fusion surgeries only address symptoms but do little to stop the degeneration process. Regenerative medicine, including cellular therapies, focuses instead on the biological repair or regeneration of the IVD and surrounding facet joints, posterior ligaments, etc. This has many advantages over current therapies and regenerative treatments that are coming of age in the treatment of discogenic back pain. These therapies include non-cellular and cellular prolotherapy (mesenchymal stem cells or bone marrow aspirate, PRP) and offer the most promise, as they have the potential to provide meaningful pain relief and functional restoration to the spinal ligaments and IVD [28].
3.2Dextrose and cellular prolotherapy for disc degeneration and pain
Degenerated discs are believed to produce nerve root pain either mechanically or chemically. In the case of advanced disc degeneration, this type of pain has a history of being symptomatically resistant to peridural steroids, intra-discal electrothermoplasty, and direct surgical intervention, while also being difficult to resolve. However, exposure of irritated nerves to hypertonic dextrose prolotherapy is thought to have chemoneuromodulatory potential. Sustained pain reduction has been demonstrated in a prospective consecutive patient series in which the effects of disc space injections of hypertonic dextrose were assessed in patients with chronic advanced degenerative discogenic leg pain, with or without low back pain, including those with moderate to severe disc degeneration and concordant pain reproduction with CT discography. Patients underwent bi-weekly disc space injections of a solution consisting of 50% dextrose and 0.25% bupivacaine in the affected disc(s). Each patient was injected an average of 3.5 times. Overall, 43.4% of patients achieved sustained improvement as shown by average changes in numeric pain scores of 71% between pretreatment and 18-month measurements. The authors concluded that intradiscal injection of hypertonic dextrose has promise as a treatment for managing the pain of advanced lumbar disc degeneration [29].
In a retrospective case series of 21 patients with MRI-confirmed lumbar disc degeneration and refractory low back pain/non-radicular low back pain, 18 (86%) of patients experienced 70% or greater improvements in pain and function [30] at 1-year follow up. Patients underwent 3 prolotherapy treatment sessions at 1–3 weeks apart, which included injections at the ligamento-periosteal junctions at the origin and insertion of the posterior sacroiliac ligaments, iliolumbar ligaments, facet joint capsules, and supraspinous and interspinous ligaments (all bilaterally). Injections were done under fluoroscopic guidance.
A small case series of 4 patients [31] with low back pain also proved successful in treating those with disc herniations with prolotherapy. Patients underwent 3–9 prolotherapy sessions to the ligaments of the low back (almost all 1 month apart) with all patients experiencing 95–100% pain relief and increase in function, including the ability to return to work.
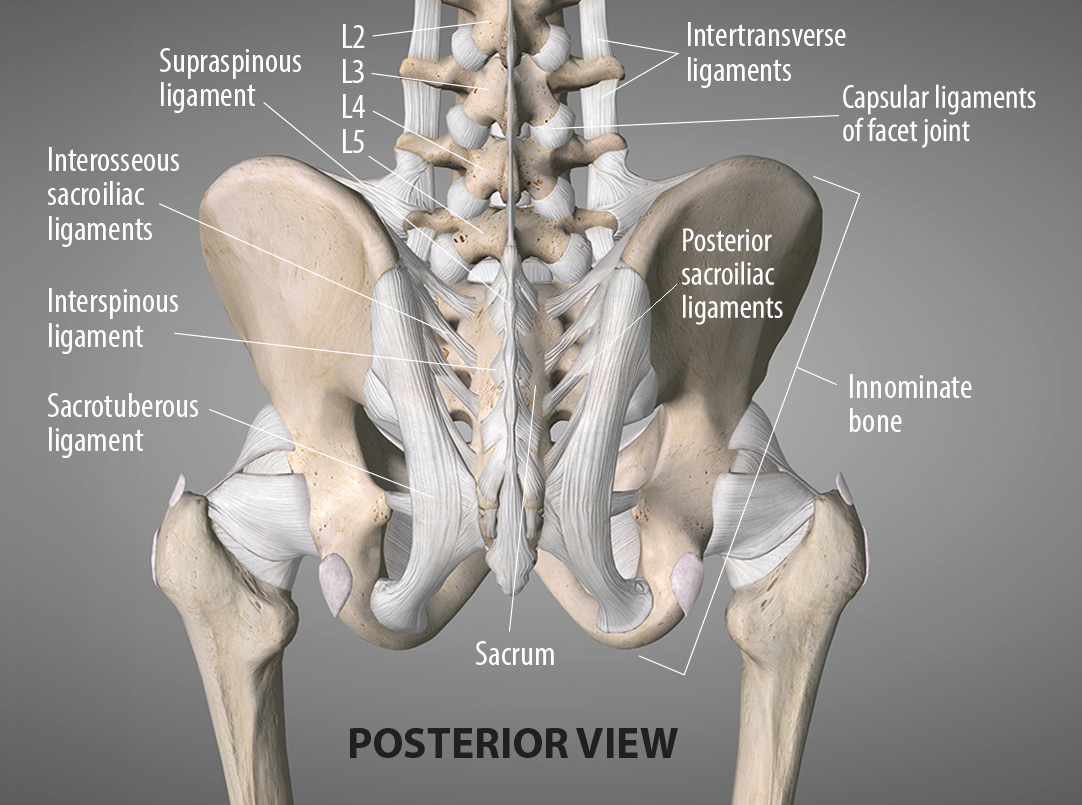
Figure 7.
Ligaments of the low back, including those of the sacroiliac joint.
Intervertebral discs can, to a limited extent, exhibit regenerative properties themselves. While some interventions focus on controlling pain intensity, other more invasive interventions try to stabilize the disc through fusion surgery, which permanently “freezes” that level of the spine and often leads to adjacent segment disease. Cellular prolotherapy, however, focuses on both resolving the pain and stabilizing the disc. Ligamentous and disc regenerative approaches aim at halting or reversing spinal degeneration. As Huang, et al. state, “Existing treatment options…only address symptoms whilst doing little to halt the degeneration process…new therapies focus on the biological repair or regeneration of the nucleus pulposus (NP) and annulus fibrosus (AF) and can be especially promising when applied to an early stage of disc degeneration” [32].
3.2.1Sacroiliac joint-mediated pain
The sacroiliac joint is often described as a large, auricular-shaped synovial joint. Only one-third of the joint, however, is a true synovial joint; the remainder of the sacroiliac joint is made up of an intricate set of ligamentous connections [33]. This strong ligamentous architecture provides stability to the sacroiliac joints. Loss of ligamentous integrity to these joints can result in sacroiliac joint instability and chronic pain (see Fig. 7).
A prospective, randomized, controlled trial was conducted to evaluate the efficacy and long-term effectiveness of intra-articular prolotherapy in relieving sacroiliac joint pain, compared with intra-articular steroid injection. At 15 months, 58% of the patients treated with prolotherapy reported that more than half of their pain was relieved, which was statistically significant (log-rank
Another randomized clinical trial evaluated the efficacy of injections of a dextrose-glycerin-phenol proliferant in treating 79 patients with chronic low back pain who had failed to respond to previous conservative care. Patients were randomly assigned to receive a double-blind series of 6 injections at weekly intervals of either a xylocaine/proliferant or a xylocaine/saline solution into the posterior sacroiliac and interspinous ligaments, fascia, and joint capsules of the lower back from L4 to the sacrum. Of the 39 patients assigned to the proliferant group, 30 achieved a 50% or greater reduction in both pain and disability scores at 6 months compared with 21 of 40 in the group receiving the saline solution (
A prospective study was conducted to determine whether prolotherapy is effective in the treatment of deficient load transfer of the sacroiliac joint in 25 patients. In this study, 3 injections at 6-week intervals of a hypertonic dextrose solution were given into the dorsal interosseous ligament of the affected sacroiliac joint of each patient. Outcome measures included the Quebec Back Pain Disability Scale, Roland-Morris 24, and Roland-Morris 24 Multiform questionnaires, and independent clinical examination by 2 authors. Clinical scores were obtained using the t-test for matched pairs and showed there were significant improvements from baseline to follow-ups at 3, 12, and 24 months (
In an audit of conservative treatments for low back pain, patients who were diagnosed with sacroiliac pain via diagnostic block were treated either by corticosteroid injection to the sacroiliac joint or by prolotherapy to the sacroiliac ligaments. Long-term improvement was assessed at 6 months, after which 63% of the prolotherapy group reported a substantial drop in pain severity compared with only 33% in the corticosteroid group [37].
The use of PRP for treating musculoskeletal conditions is growing, and studies specific to sacroiliac mediated pain have found that PRP provides favorable outcomes. In one randomized, controlled trial of PRP vs. corticosteroid injection, 90% of subjects treated with PRP to the sacroiliac joint were satisfied at the 3-month follow-up compared with only 25% of those who were treated with the steroid [38]. In 2 small case series, PRP was used to treat a total of 14 patients with chronic sacroiliac joint pain, the first of which involved administering a fluoroscopically guided single injection of 4 ml autologous PRP into the sacroiliac joint of 10 patients who had failed other conservative treatments. After 4 follow-up sessions at 3-month intervals, verbal analog scale scores for pain of all 10 patients had decreased more than 50% by the 12
3.2.2Spinal osteoarthritis
Spinal OA (also known as lumbar spine OA) has a complex association with chronic low back pain and affects approximately 80% of the population aged 40 and over, according to 2013–2015 statistics. The authors further reported that low back pain was self-reported at the highest rate (35%) by people in the 45- to 64-year age group, and that this group also underwent the most spinal procedures (47%). Self-reported limitations in performing ADL affect about 10% of people who have OA in their back or neck [41].
Spinal OA is characterized by facet OA, disc space narrowing (DSN), and osteophyte formation (OST) at the same vertebral level and belongs to a group of spinal disorders called spondylosis. In one study, evidence of DSN and OST in the lumbar spine was obtained radiographically from a community-based population, indicating that the prevalence of spinal OA may be as high as 50% to 64% for DSN and 75% to 94% for OST [42].
An important orthopedic principle to consider regarding osteophyte formation is Wolff’s Law, which states that, in humans, any bone will adapt to the stresses put upon it. In the case of instability, those stressors are the loosened ligaments that have been repeatedly pulling on their bony attachments, causing the bone to adapt itself so it can resist this force. This typically results in what is known as bony hypertrophy (bony growth). In the spine, this can be referred to as spurring (osteophyte formation) or facet arthrosis (arthritis) but is more generally known as spondylosis. As the bone grows out further and reaches the area where the ligament(s) is pulling, it can cause a compressive effect and squash the nerve coming through the foramina. In advanced cases, nerve root compression may require treatment with decompression surgery (foraminotomy). In cases of intermittent radiculopathy (meaning the radicular symptoms are not constant), lumbar instability with or without spurring may be a culprit due to excess motion of the vertebrae and IVD narrowing the neural foramina. In cases of back pain with numbness down the leg, prompt medical attention should be sought out so that the instability causing damage to a nerve can be rectified. This even applies to younger people who usually have thick and healthy discs, because they would experience the same type of pain signal should a segment of their spines become injured. A medical practitioner (ideally, a Prolotherapist) can determine at which level that injury occurred and then address the instability before the pain becomes chronic. All too often, patients who feel pain due to unstable facet joints are given passive treatments and told the pain will subside. These conventional treatments (e.g., NSAIDs, cortisone shots, ice, rest), however, are short-lived and put patients at risk for further instability issues and more intense chronic pain as they age.
4.Discussion
4.1Diagnostic clues to utilize prolotherapy in a patient with chronic low back pain
In an editorial, a board-certified physician in family medicine whose specialty is pain management made several points about treatment of low back pain with prolotherapy [43]:
• When patients have weakness of the sacroiliac ligament, it generates pain similar to that of spinal stenosis – that is, pain on ambulation and standing.
• Such patients will respond to ligament prolotherapy.
• Patients with clearly unilateral symptoms often respond to ligament prolotherapy on the painful side of the body.
• Patients who have listhesis and/or disc disease contributing to the stenosis often respond to prolotherapy at that level in the spine.
• Decompressive surgery can worsen instability of the spine. The sciatic pain often improves, but the lower back pain often worsens.
4.1.1Adverse effects
The current status of the literature suggests that non-cellular (including dextrose) and cellular prolotherapy are well tolerated, safe, and reasonably effective. The most frequent adverse events are the expected short-term increase in pain from the interventions and increased risk of infection. Pain and swelling at the injection site(s) are typically short-lived, with patients recovering within several days. Dextrose, a common ingredient in non-cellular prolotherapy, is extremely safe (even in intravenous use) and in 1998, the FDA documented that no adverse outcomes had been reported for 25% intravenous dextrose solution in 60 years [44, 45].
Adverse events with spinal prolotherapy exist and include spinal headache, nerve damage, non-severe spinal cord insult, and disc injury. Prolotherapy performed by an experienced Prolotherapist can mitigate these risks [46] and these events are no more common in prolotherapy procedures than for other spinal injection interventions [47].
Throughout the literature, complications of PRP injections, including infections, are extremely rare. Additionally, PRP has been thought to have anti-microbial properties, thus further lowering risk of infection [48, 49]. It also may have a role in preventing infection, given a recent study that found antimicrobial activity was greatest when a leukocyte-rich PRP was used in conjunction with a mixed antibiotic [50]. As PRP involves the use of the patient’s own blood product, the chance of allergic reaction is quite low.
5.Conclusion
Given the widespread prevalence of spinal disorders, clinicians should understand ligaments as a causative factor for lumbar spinal instability resulting in chronic and worsening low back pain. Degenerative spine conditions are initiated by the development of instability within the PLC, most notably the facet joint capsular ligaments. In response, the body makes adaptations trying to stabilize the spine, which are initially protective but eventually become harmful (e.g., bone spurs). Without addressing the instability, progression of degenerative spinal conditions with low back pain will continue.
Clinically speaking, spinal stability is the ability of the spine to maintain its alignment during loading, and to protect the neural structures it encloses without causing pain. It is the collective job of the bones, muscles, discs, and ligaments to maintain their alignment of the spinal column so the spinal cord and nerves remain protected. If the spine no longer has properly functioning biomechanical properties, however, clinical stability is lost, giving rise to spinal instability and pain.
Prolotherapy is a regenerative treatment option for those suffering from low back pain and associated conditions related to joint and spinal instability. Regenerative treatment to injured ligaments has the potential and ability to strengthen the PLC, and thus relieve both chronic and acute low back pain.
Conflict of interest
None to report.
Ethical declaration
Ethical review was not necessary for this study, as no human subjects were included, and only publicly available data were used.
References
[1] | Weinstein SI, Yelin EH, Watkins-Castillo SI. The big picture. United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States (BMUS), 4 |
[2] | Chaib F. Musculoskeletal conditions affect millions. World Health Organization (WHO) (Internet). (2003) ; Oct 27. [Accessed 2021 July 26]. Available from: https//www.who.int/news/item/27-10-2003-musculoskeletal-conditions-affect-millions. |
[3] | National Institutes of Health (NIH), National Institute of Neurological Disorders and Stroke. Low back pain fact sheet (Internet). (2020) Mar. [Accessed 2021 July 26]. Available from: https//www.ninds.nih.gov/Disorders/Patient-Caregiver-Education/Fact-Sheets/Low-Back-Pain-Fact-Sheet. |
[4] | Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira M, Genevay S. Low back pain series: what low back pain is and why we need to pay attention. Lancet (Internet). (2018) ; [Accessed 2021 July 26]; 391: (10137): 2356-2367. doi: 10.1016/S0140-6736(18)30480-X. |
[5] | Singh K, Andersson G, Watkins-Castillo SI. Low back and neck pain. In: The Burden of Musculoskeletal Diseases in the United States: Prevalence, Societal and Economic Costs (BMUS), 4th ed. United States Bone and Joint Initiative (USBJI) (Internet). [Accessed 2021 July 26]. Available from: https//www.boneandjointburden.org/fourth-edition/iia0/low-back-and-neck-pain.s |
[6] | Wu A, March L, Zheng X, Huang J, Wang X, Zhao J. Global low back pain prevalence and years lived with disability from 1990 to 2017: estimates from the Global Burden of Disease Study 2017. Ann Transl Med (Internet). (2020) [Accessed 2021 July 26]; 8: (6): 299. Available from: https://pubmed.ncbi.nlm.nih.gov/32355743/. doi: 10.21037/atm.2020.02.175. |
[7] | GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017 (published correction appears in Lancet. 2019 Jun 22; 393(10190): e44). Lancet (Internet). (2018) [Accessed 2021 July 26]; 392: (10159): 1789-1858. Available from: https://pubmed.ncbi.nlm.nih.gov/30496104/. doi: 10.1016/S0140-6736(18)32279-7. |
[8] | Weinstein SI, Yelin EH, Watkins-Castillo SI. The big picture. United States Bone and Joint Initiative: The Burden of Musculoskeletal Diseases in the United States (BMUS), 4th ed. United States Bone and Joint Initiative (USBJI) (Internet). [Accessed July 19, 2021] https//www.boneandjointburden.org/fourth-edition/iiaa0/low-back-pain. |
[9] | GBD 2017 DALYs and HALE Collaborators. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Published correction appeared in Lancet. (2019) Jun 22 [Accessed May 1, 2020]; 393: (10190): e44. |
[10] | Deyo RA, Dworkin SF, Amtmann D, Andersson G, Borenstein D, Carragee E. Focus article report of the NIH task force on research standards for chronic low back pain. Clin J Pain. (2014) ; 30: (8): 701-712. |
[11] | Rizkalla JM, Tanner MS, Nimmons S. Classifications in brief: the Denis classification of sacral fractures. Clin Orthop Relat Res. Sep (2019) [Accessed 2021 July 26]; 477: (9): 2178-81. doi: 10.1097/CORR.0000000000000861. |
[12] | Maher C, Underwood M, Buchbinder R. Non-specific low back pain. Lancet. (2017) [Accessed 2021 July 26]; 389: (10070): 736-747. doi: 10.1016/S0140-6736(16)30970-9. |
[13] | Deyo RA, Mirza SK, Turner JA, Martin BI. Overtreating chronic back pain: time to back off? JABFM. (2009) ; 22: : 62-6. |
[14] | Hackett G. Referred pain and sciatica in diagnosis of low back disability. JAMA. (1957) ; 163: (3): 183-5. |
[15] | Phillips FM, Slosar PJ, Youssef JA, Andersson G, Papatheofanis F. Lumbar spine fusion for chronic low back pain due to degenerative disc disease: a systematic review. Spine. (2013) ; 38: (7): E409-22. |
[16] | Rigotti G, Marchi A, Sbarbati A. Adipose-derived mesenchymal stem cells: past, present, and future. Aesthetic Plast Surg. (2009) ; 33: (3): 271-3. |
[17] | Jaumard NV, Welch WC, Winkelstein BA. Spinal facet joint biomechanics and mechanotransduction in normal, injury and degenerative conditions. J Biomech Eng. (2011) ; 133: (7): 071010. doi: 10.1115/1.4004493. |
[18] | Perolat R, Kastler A, Nicot B, Pellat JM, Tahon F, Attye A. Facet joint syndrome: from diagnosis to interventional management. Insights Imaging. (2018) ; 9: (5): 773-89. doi: 10.1007/s13244-018-0638-x. |
[19] | Nachemson AL. Disc pressure measurements. Spine. (1981) Jan-Feb; 6: (1): 93-7. doi: 10.1097/00007632-198101000-00020. |
[20] | Heuer F, Schmidt H, Claes L, Hans-Joachim W. Stepwise reduction of functional spinal structures increase vertebral translation and intradiscal pressure. J Biomech. (2007) ; 40: (4): 795-803. doi: 10.1016/j.jbiomech.2006.03.016. |
[21] | Li Y, Shen Z, Huang M, Wang X. Stepwise resection of the posterior ligamentous complex for stability of a thoracolumbar compression fracture: An in vitro biomechanical investigation. Medicine (Baltimore). (2017) Sep; 96: (35): e7873. doi: 10.1097/MD.0000000000007873. |
[22] | Wu J, Zhou J, Liu C, Zhang J, Xiong W, Lv Y. A prospective study comparing platelet-rich plasma and local anesthetic (LA)/ corticosteroid in intra-articular injection for the treatment of lumbar facet joint syndrome. Pain Pract. (2017) ; 17: : 914-24. |
[23] | Desai MJ, Mansfield JT, Robinson DM, Miller BC, Borg-Stein J. Regenerative medicine for axial and radicular spine-related pain: a narrative review. Pain Pract. (2020) ; 20: : 437-53. |
[24] | Dagenais S, Yelland MJ, Del Mar C, Schoene M. Prolotherapy injections for chronic low back pain. Cochrane Database Systematic Review. (2007) (2): CD004059. doi: 10.1002/14651858.CD004059.pub3. |
[25] | Xuan Z, Yu W, Dou Y, Wang T. Efficacy of platelet-rich plasma for low back pain: a systematic review and meta-analysis. Journal of Neurol Surg A Cent Eur Neurosurg. (2020) ; 81: ; 529-34. |
[26] | Wilkinson HA. Injection therapy for enthesopathies causing axial spine pain and the “failed back syndrome”: a single blinded, randomized, and cross-over study. Pain Physician. (2005) ; 8: (2): 167-73. |
[27] | Cunningham BW, Kotani Y, McNulty PS, Cappuccino A, McAfee PC. The effect of spinal destabilization and instrumentation on lumbar intradiscal pressure: an in vitro biomechanical analysis. Spine (Phila Pa 1976). (1997) Nov 15; 22: (22): 2655-63. |
[28] | Fujii K, Yamazaki M, Kang JD, Risbud MV, Cho SK, Qureshi SA. Discogenic back pain: literature review of definition, diagnosis, and treatment. JBMR Plus. (2019) ; 3: (5): e10180. doi: 10.1002/jbm4.10180. |
[29] | Miller MR, Mathews RS, Reeves KD. Treatment of painful advanced internal lumbar disc derangement with intradiscal injection of hypertonic dextrose. Pain Physician. (2006) ; 9: : 115-21. |
[30] | Inklebarger J, Petrides S. Prolotherapy for lumbar segmental instability associated with degenerative disc disease. Journal of Prolotherapy. (2016) ; 8: : e971-7. |
[31] | Alderman D. Prolotherapy for Low Back Pain: A reasonable and conservative approach to musculoskeletal low back pain, disc disease, and sciatica. Pain Manag. (2007) ; 7: (4). |
[32] | Huang S, Tam V, Cheung KM, Long D, Lv M, Wang T. Stem cell-based approaches for intervertebral disc regeneration. Curr Stem Cell Res Ther. (2011) ; 6: (4): 317-26. doi: 10.2174/157488811797904335. |
[33] | Cohen SP. Sacroiliac Joint Pain: A Comprehensive Review of Anatomy, Diagnosis, and Treatment. Anesth Analg. (2005) ; 101: : 1440-53. doi: 10.1213/01.ANE.0000180831.60169.EA. |
[34] | Kim WM, Lee HG, Jeong CW, Kim CM, Yoon MH. A randomized controlled trial of intra-articular Prolotherapy versus steroid injection for sacroiliac joint pain. J Altern Complement Med. (2010) Dec; 16: (12): 1285-90. doi: 10.1089/acm.2010.0031. |
[35] | Klein RG, Eek BC, DeLong WB, Mooney V. A randomized double-blind trial of dextrose-glycerine-phenol injections for chronic, low back pain. J Spinal Disord. (1993) ; 6: (1): 23-33. |
[36] | Cusi M, Saunders J, Hungerford B, Wisbey-Roth T, Lucas P, Wilson S. The use of Prolotherapy in the sacroiliac joint. Br J Sports Med. (2010) Feb; 44: (2): 100-4. Epub 2008 Apr 9. doi: 10.1136/bjsm.2007.042044. |
[37] | Chakraverty R, Dias R. Audit of conservative management of chronic low back pain in a secondary care setting – part I: facet joint and sacroiliac joint interventions. Acupunct Med. (2004) ; 22: (4): 207-13. |
[38] | Singla V, Batra YK, Bharti N, Goni VG, Marwaha N. Steroid vs. platelet-rich plasma in ultrasound-guided sacroiliac joint injection for chronic low back pain. Pain Pract. (2017) ; 17: : 782-91. |
[39] | Navani A, Gupta D. Role of intra-articular platelet-rich plasma in sacroiliac joint pain. Reg Anesth Pain Med. (2015) ; 19: : 54-9. |
[40] | Ko GD, Mindra S, Lawson GE, Whitmore S, Arseneau L. Case series of ultrasound-guided platelet-rich plasma injections for sacroiliac joint dysfunction. J Back Musculoskelet Rehabil. (2017) ; 30: : 363-70. |
[41] | Hootman JM, Helmick CG. Updated projections of US prevalence of arthritis and associated activity limitations. Arthritis Rheum. (2016) ; 68: (7): 1582-7. |
[42] | Goode AP, Carey TS, Jordan JM. Low back pain and lumbar spine osteoarthritis: how are they related? Curr Rheumatol Rep. (2013) ; 15: (2): 305. doi: 10.1007/s11926-012-0305-z. |
[43] | Matthews JH. Nonsurgical treatment of pain in lumbar spine stenosis. Am Fam Physician. Letters to the Editor. (1999) ; 59: (2): 280-4. |
[44] | [Abbott Labs FDA Indications for 50% Dextrose.] 2004. [Accessed 2014 Nov 12]. Available at http//www.fda.gov/cder/foi/nda/98/19445-s4-s6.htm. |
[45] | Abbott Labs. Approval Documentation for 25% Dextrose Submitted to FDA. Online Documentation. Chicago, IL: Abbott Laboratories, (1998) . |
[46] | Nair LS. Prolotherapy for tissue repair. Transl Res. (2011) ; 158: (3): 129-31. |
[47] | Dagenais S, Ogunseitan O, Haldeman S, Wooley JR, Newcomb RL. Side effects and adverse events related to intraligamentous injection of sclerosing solutions (prolotherapy) for back and neck pain: A survey of practitioners. Arch Phys Med Rehabil. (2006) Jul; 87: (7): 909. |
[48] | Bielecki TM, Gazdzik TS, Arendt J, Szczepanski T, Król W, Wielkoszynski T. Antibacterial effect of autologous platelet gel enriched with growth factors and other active substances: an in vitro study. J Bone Joint Surg Br. (2007) ; 89: : 417-20. doi: 10.1302/0301-620X.89B3.18491. |
[49] | Fabbro MD, Bortolin M, Taschieri S, Ceci C, Weinstein RL. Antimicrobial properties of platelet-rich preparations. A systematic review of the current pre-clinical evidence. Platelets. (2016) ; 27: : 276-85. doi: 10.3109/09537104.2015.1116686. |
[50] | Prysak MH, Lutz CG, Zukofsky TA, Katz JM, Everts PA, Lutz GE. Optimizing the safety of intradiscal platelet-rich plasma: an in vitro study with Cutibacterium acnes. Regen Med. (2019) Oct; 14: (10): 955-67. doi: 10.2217/rme-2019-0098. Epub 2019 Oct. |


