
Non-operative orthobiologic use for rotator cuff disorders and glenohumeral osteoarthritis: A systematic review
Abstract
BACKGROUND:
Shoulder pain from rotator cuff pathology and glenohumeral osteoarthritis is a common entity encountered in musculoskeletal practices. Orthobiologic agents are being increasingly used as a treatment option and understanding their safety and efficacy is necessary.
OBJECTIVE:
To systematically evaluate the available evidence for orthobiologic use in rotator cuff and glenohumeral pathology.
METHODS:
A systematic review was undertaken following PRISMA guidelines. Randomized clinical trials (RCTs) and prospective cohort studies evaluating non-operative treatment with prolotherapy, platelet-rich plasma (PRP), or medicinal signaling cells (MSCs) for rotator cuff pathology and glenohumeral osteoarthritis were included. Bias risk assessments used were the Cochrane tool and Newcastle-Ottawa score.
RESULTS:
The search yielded 852 potential articles, of which 20 met the inclusion criteria with a breakdown of 5 prolotherapy, 13 PRP, and 2 MSC. Sixteen studies were RCTs and 4 were cohort studies. Six studies were deemed “low risk of bias or good quality”. Efficacy results were mixed, and no serious adverse events were reported from orthobiologic treatment.
CONCLUSIONS:
Orthobiologics offer a relatively safe management option with inconclusive evidence for or against its use for rotator cuff pathology. No studies on glenohumeral osteoarthritis met the inclusion criteria. Adoption of standardized preparation reporting and consistent use of functional outcome measures is imperative for future studies to consider.
1.Introduction
Shoulder pain is a common debilitating condition with an estimated annual prevalence ranging from 4.7–46.7% [1]. The shoulder is involved in numerous movements required for daily function resulting in significant debilitation when injured. In addition to causing functional limitations, the inability to fully utilize on’s shoulder can contribute to mood disorders such as depression and anxiety [2]. Patients who perform heavy manual labor, athletes, wheelchair users, and hemiplegic individuals are at increased risk of developing shoulder pain. With increasing age, specifically beyond age 50, there is a higher incidence of shoulder pain [2, 3, 4]. The prevalence and incidence of disability due to shoulder pain increase with age and activity level [5, 6]. This has created a large economic burden. In 2000, the direct costs for treatment of shoulder pain in the United States averaged 7 billion dollars [7]. As the general population strives to be more active, physicians will find themselves treating an increasing number of patients with shoulder pathology.
Two of the most common shoulder pathologies encountered are rotator cuff disorders and glenohumeral osteoarthritis. The reported prevalence of rotator cuff pathology varies widely from 9.7–62%. Amongst shoulder pain presentations in the primary care setting, rotator cuff disorders account for 30–70% of visits [8, 9]. Glenohumeral arthritis has a prevalence ranging between 4–26% [10].
Early in the clinical course of shoulder disorders, typical treatments include activity modification, physical therapy, oral anti-inflammatories, and corticosteroid injections. Long term use of corticosteroid is becoming increasingly controversial, as there are concerns regarding tendon and chondral toxicity [11, 12]. For recalcitrant cases, surgical intervention with rotator cuff repair or arthroplasty may be offered. However, not all patients are surgical candidates due to limitations from lengthy post-operative recovery times, multiple or complex shoulder lesions, and other comorbidities. While multiple surgical technique options exist, tendon tear thickness is the most important determinant in the decision to pursue surgical treatment [13]. In the case of partial rotator cuff tears, good to excellent surgical outcomes, as measured by shoulder specific scales have been reported [14]. However, long term results are unclear, with further rotator cuff degeneration reported at 5 years of follow-up [15]. Orthobiologics have recently gained traction as a management option for these disorders. Three of the most commonly used orthobiologic agents are prolotherapy, platelet-rich plasma (PRP) and medicinal signaling cells (MSCs), the latter of which are typically obtained from autologous bone marrow aspirate or adipose tissue [16, 17].
Prolotherapy involves an injection of a solution often including hypertonic dextrose with the goal of repairing connective tissue and ameliorating pain. The mechanism of action is not completely understood. It is thought that the injected proliferant initiates a local inflammatory cascade, thereby triggering release of growth factors and cytokines [18, 19]. For example, dextrose functions as an osmotic agent causing cell dehydration at the injection site which creates local trauma that attracts inflammatory cells. This chemomodulation theoretically leads to connective tissue proliferation and reduction in pain and tissue dysfunction.
Platelet-rich plasma (PRP) consists of an autologous concentration of platelets isolated from whole blood via centrifugation. It is hypothesized that a platelet concentration greater than baseline may contribute to its efficacy. The proposed mechanism is that PRP initiates the bod’s own repair processes, modulates inflammation, delivers growth factors, and attracts and activates MSCs, which promote a healing environment and reduce pain [20]. In vitro studies have shown PRP to induce downregulation of the crucial inflammatory molecules Interleukin 6 and Interleukin 8, which can help attenuate hyperalgesia [21].
MSCs are cells with the perceived capability to proliferate and differentiate into cells that regenerate tissue functionality following injury [19]. They are perivascular in origin and can be isolated from any vascularized tissue [22]. Most commonly, MSCs are harvested from bone marrow, adipose, umbilical or placental tissue sources [23]. In vitro studies have shown these cells to express growth factors such as transforming growth factor beta (TGFB) and vascular endothelial growth factor (VEGF), which are known to stimulate local tissue repair [24]. Additionally, they suppress the proliferation of inflammatory T-cells and inhibit monocyte maturation, creating both immunomodulatory and anti-inflammatory effects [24, 25].
Given the increasing use of these agents, it is necessary to review the available evidence regarding their safety and efficacy. The purpose of this systematic review is to evaluate outcomes of prospective randomized clinical trials (RCTs) and cohort studies on use of non-operative orthobiologics for treatment of rotator cuff pathology and glenohumeral osteoarthritis.
2.Methods
2.1Search strategy and study selection
This systematic eview was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [26]. The following electronic databases were queried: PubMed, Embase and ScienceDirect. References from found articles were additionally reviewed for potential inclusion. All studies from database inception to September 2020 were assessed.
Searches were performed for each selected orthobiologic agent: prolotherapy, PRP, and MSCs. The following search terms were used: (Prolotherapy OR Hypertonic Dextrose OR Proliferative Therapy) AND (Shoulder OR Rotator Cuff OR Shoulder Arthritis OR Glenohumeral Arthritis), (Platelet rich plasma OR PRP OR Autologous Conditioned Serum) AND (Shoulder OR Rotator Cuff OR Shoulder Arthritis OR Glenohumeral Arthritis), (Bone Marrow Aspirate Concentrate OR BMAC OR Adipocyte Signaling Cell OR ASC OR MFAT) AND (Shoulder OR Rotator Cuff OR Shoulder Arthritis OR Glenohumeral Arthritis). PubMed and Embase searches were performed using the main search bar, whereas ScienceDirect searches were performed using the “Title, abstract or author-specified keywords” advanced search tab.
2.2Eligibility
Titles and abstracts from retrieved studies were reviewed for the following inclusion/exclusion criteria. Eligible studies were prospective randomized clinical trials or cohort studies, were written in English, and studied outcomes of either prolotherapy, PRP, or MSCs on patients with rotator cuff pathology or glenohumeral osteoarthritis. Retrospective studies, case series and case reports, animal studies, and studies in which patients had undergone or were undergoing surgical intervention at time of orthobiologic treatment were excluded.
Levels of evidence for each study were determined by the criteria of the American Association of Physical Medicine & Rehabilitation, an adaptation of those proposed by The Journal of Bone and Joint Surgery [27]: Level I – Randomized controlled trials or systemic review of level I randomized controlled trials; Level II – Prospective cohort studies, poor-quality randomized controlled trials, systematic reviews of level II studies or non-homogenous level I studies; Level III – Case-control studies, retrospective cohort studies, systematic reviews of level III studies; Level IV – Case series; and Level V – Expert opinion.
2.3Bias assessment
Quality and bias risk assessment were evaluated using the Cochrane Collaboration risk of bias tool for randomized controlled trials and the Newcastle-Ottawa bias tool for non-randomized cohort studies [28, 29]. Three researchers separately assessed each article (SD, SD, DR). Discrepancies in risk of bias were resolved through discussion with all reviewers.
Regarding randomized clinical trials, studies were considered to have a low risk of bias when all items were scored as “low risk”. If 1 or 2 items were scored as “unclear risk” or “high risk”, the study was considered moderate risk of bias. When more than 2 items were scored as “unclear risk” or “high risk”, the study was considered at high risk of bias [30]. Cohort studies were deemed good, fair, or poor quality using the suggested scoring system within the Newcastle-Ottawa Quality Assessment Form for Cohort Studies.
3.Results
As outlined in Fig. 1, 852 studies were identified through the search with 824 being excluded prior to full review. Twenty-eight articles were read in full and 20 met the eligibility criteria and were included in this review with a breakdown of 5 prolotherapy, 13 PRP, and 2 MSC. Sixteen studies were RCTs and 4 were cohort studies.
Figure 1.
PRISMA flow diagram for included studies.
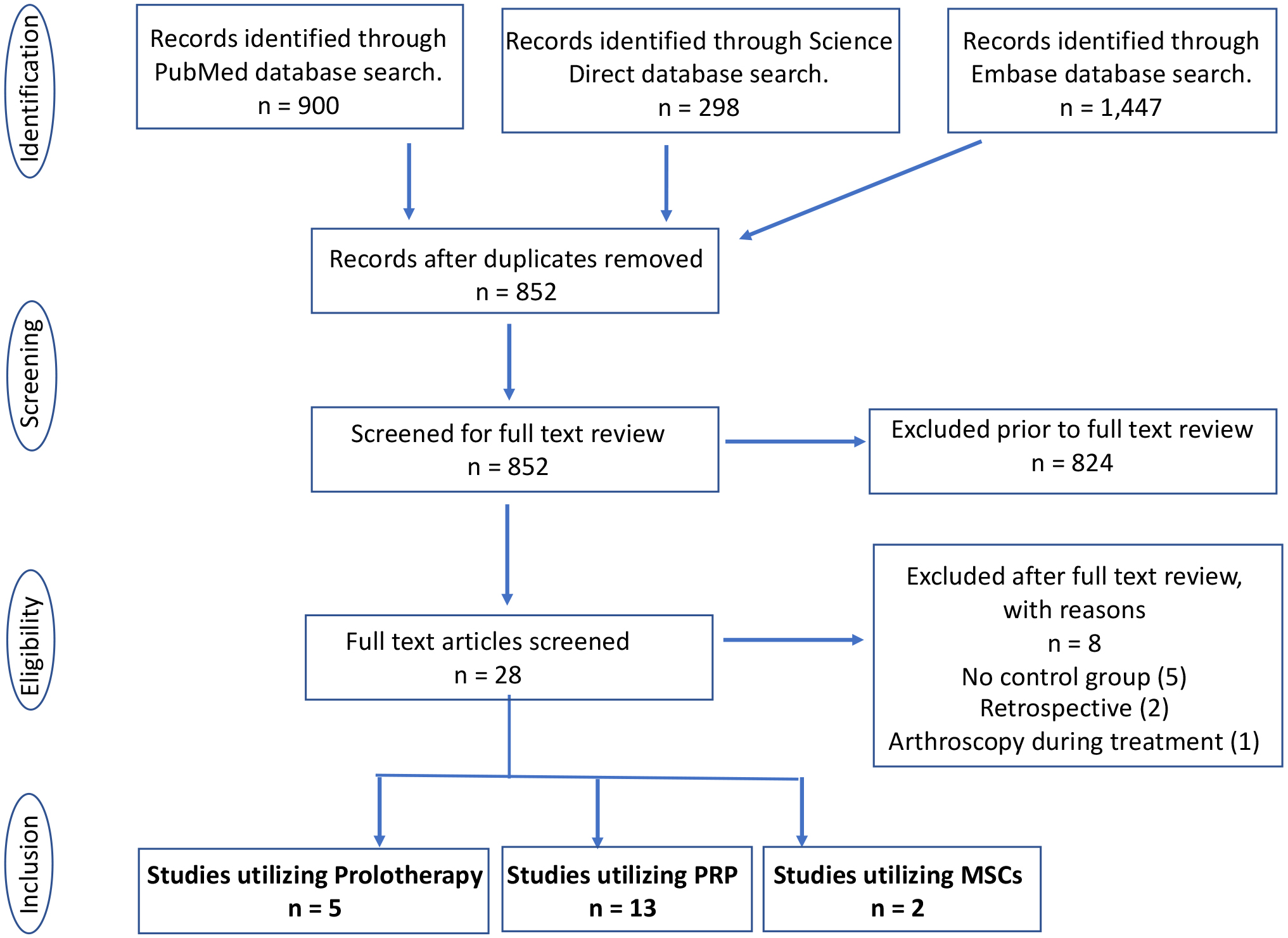
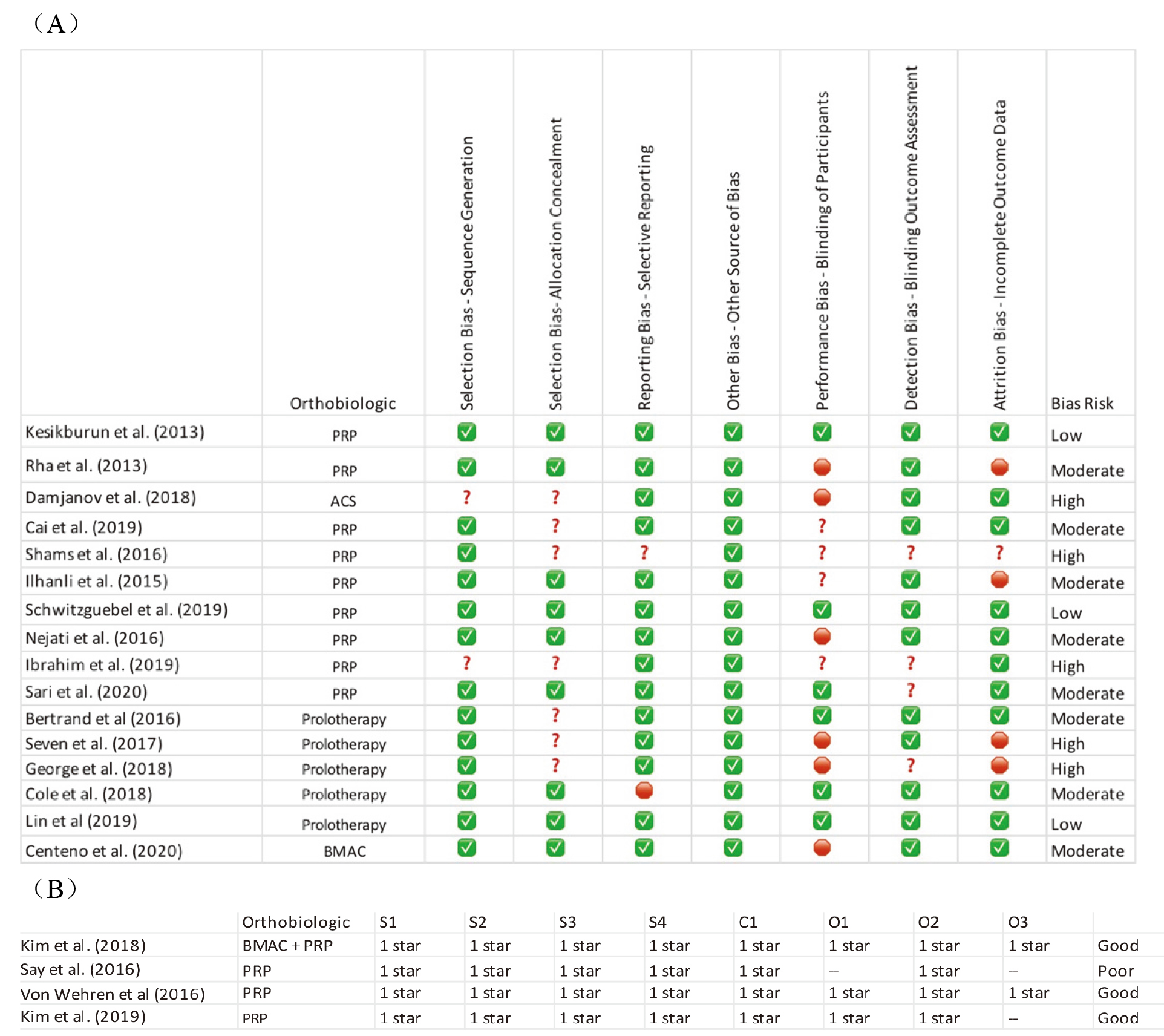
Figure 2.
Bias assessment utilizing (A) the Cochrane Collaboration risk of bias tool for randomized controlled trials and (B) the Newcastle-Ottawa bias tool for non-randomized cohort studies. Checkmark depicts low risk of bias, question mark depicts unclear risk of bias, and the stop sign depicts high risk of bias for each bias-type on the Cochrane tool, respectively.
3.1Studies utilizing prolotherapy
Five studies were analyzed that evaluated the therapeutic effects of prolotherapy, with a total of 253 participants (136 prolotherapy and 117 control). Follow-up times ranged from 6 weeks to 1 year. All five were RCTs and evaluated rotator cuff pathology. Study characteristics are outlined in Table 1. Bias risk was deemed low for one study, moderate for two studies, and high for two studies (Fig. 2). Controls in the studies were as follows: two used saline injection, two used exercise therapy, and one used corticosteroid injection. The most common prolotherapy agent used was dextrose in concentrations ranging from 12.5–25% in four studies, with one study utilizing 25% glucose. Four studies utilized ultrasound image guidance.
Overall, results regarding pain outcomes varied with sustained benefit seen in two studies, short-term benefit seen at 2 weeks but not 6 weeks in one study, and no significant change compared to control in two studies. Number of injections varied from one to six, with three studies using a single injection. Out of the 136 patients treated with prolotherapy, two sustained grade 2 burns from hot water packs used after the injection, one developed hypotension after injection, and three had 48 hours of post-injection soreness; no other complications were reported.
3.1.1Prolotherapy versus saline
Two studies evaluated prolotherapy versus saline. Bertrand et al. evaluated 29 patients treated with three monthly palpationguided injections of prolotherapy into the supraspinatus enthesis against 20 patients treated with saline into the enthesis and 27 patients treated with saline superficial to the enthesis [31]. Primary outcome was achieving at least a 2.8-point change in visual analog scale (VAS) score. At 9 months, significantly more patients in the prolotherapy group maintained a 2.8-point VAS decrease compared to control groups (
Lin et al. compared 16 patients treated with a single ultrasoundguided prolotherapy injection to 15 patients treated with saline into the supraspinatus enthesis [32]. Primary outcomes were Shoulder Pain and Disability Index (SPADI) and VAS scores at 6 weeks follow-up. Secondary outcomes were shoulder active range of motion and ultrasound characteristics via histogram. No significant betweengroup differences were found for any measure at final follow-up. Prolotherapy had superior results at two weeks regarding VAS, SPADI, and shoulder flexion/abduction. Both had significant final withingroup changes for VAS and SPADI.
3.1.2Prolotherapy versus exercise therapy
Two studies evaluated prolotherapy versus exercise therapy. Seven et al. compared 57 patients treated with up to 6 rounds of ultrasound-guided prolotherapy to 44 patients treated with exercise therapy [33]. Prolotherapy patients were given a home exercise program while the exercise group attended supervised therapy sessions three times weekly for 12 weeks in addition to the home exercise program. Outcomes assessed included VAS, Western Ontario Rotator Cuff index (WORC), and SPADI. Final follow-up was one year, and significant improvement was seen for all outcomes in the prolotherapy group (
George et al. compared 7 patients treated with a single ultrasound-guided injection of prolotherapy to 5 patients treated with standard exercise therapy [34]. The Disabilities of the Arm, Shoulder, and Hand (DASH) score was used to evaluate functional outcomes. No significant difference was found between groups at 12-week follow-up.
3.1.3Prolotherapy versus corticosteroid
One study evaluated prolotherapy versus corticosteroid. Cole et al. compared 17 patients injected with ultrasound-guided prolotherapy into the supraspinatus tendon to 18 patients treated with methylprednisolone injected into the subacromial bursa [35]. Patients were followed up at 6 weeks, 3 months, and 6 months with primary outcome measured being pain with overhead activity on a five-point Likert scale. The prolotherapy group had significant pain relief at 3 months and both groups had significant pain relief at 6 months. However, no significant betweengroup differences were found at either time point. Both groups showed significant improvement in secondary outcomes (shoulder satisfaction, pain frequency, ultrasound characteristics, and supraspinatus strength) with no significant differences between groups.
3.2Studies utilizing PRP
Thirteen studies were analyzed that evaluated the therapeutic effects of PRP, with a total of 839 participants (338 PRP and 501 control). All evaluated rotator cuff pathology. Study characteristics are outlined in Table 2. Follow-up periods ranged from 6 weeks to 1 year. Of these 13 studies, ten were RCTs and three were cohort studies. Amongst the RCTs, bias risk was
Table 1
Prolotherapy studies
| Author (year) | Level of evidence | Study design | Pathology | Intervention | Composition of prolotherapy | Outcome measures | Conclusions | Complications |
|---|---|---|---|---|---|---|---|---|
| Bertrand et al. (2016) | I | Design: RC Intervention: Dextrose vs saline Sample size: 73 [29 prolotherapy] Follow-up: 9 months | Ultrasound-confirmed supraspinatus tendinosis/tear | Three monthly injections either (1) onto painful entheses with dextrose (Enthesis-Dextrose), (2) onto entheses with saline (Enthesis-Saline), or (3) above entheses with saline (Superficial-Saline) | 25% Dextrose | VAS, satisfaction, USPRS | Prolotherapy superior to placebo for pain and satisfaction at 9 months | No complications from prolotherapy |
| Seven et al. (2017) | II | Design: RC Intervention: Dextrose vs exercise Sample size: 101 [57 prolotherapy] Follow-up: 1 year | Rotator cuff tendinosis or partial tear | Maximum 6 rounds of ultrasound-guided injections into subacromial bursa and surrounding ligaments/tendons | 25% Dextrose for subacromial bursa and 15% Dextrose for tendon/ligament insertions | VAS, SPADI, WORC | Prolotherapy superior to exercise therapy regarding pain and function at minimum of 1 year | Two patients with grade 2 burns, three with severe post-injection pain for 2 days, one with hypotension |
| George et al. (2018) | II | Design: RC Intervention: Dextrose vs physical therapy Sample size: 12 [7 prolotherapy] Follow-up: 12 weeks | Supraspinatus tendinosis | Ultrasound-guided intra-tendinous injection | 12.5% Dextrose | DASH with pain sub-score | Prolotherapy not superior to physical therapy regarding pain at 12 weeks | None reported |
| Cole et al. (2018) | I | Design: RC Intervention: Glucose vs corticosteroid Sample size: 36 [17 prolotherapy] Follow-up: 6 months | Ultrasound-confirmed supraspinatus tendinopathy | Ultrasound-guided intra-tendinous injection of dextrose or ultrasound-guided methylprednisolone injection into subacromial bursa | 25% Glucos | Five-point Likert scale | Prolotherapy not superior to corticosteroid regarding pain reduction at 3 or 6 months | None reported |
| Lin et al. (2019) | I | Design: RC Intervention: Dextrose vs saline Sample size: 31 [16 prolotherapy] Follow-up: 6 weeks | Supraspinatus tendinopathy | Ultrasound-guided supraspinatus enthesis injection | 20% Dextrose | VAS, SPADI, ROM | Prolotherapy superior to placebo regarding pain and function at 2 weeks but not 6 weeks | No complications |
DASH: Disabilities of the Arm, Shoulder, and Hand; RCT: randomized controlled trial; ROM: range of motion; SPADI: Shoulder Pain and Disability Index; USPRS: Ultrasound Shoulder Pathology Rating Scale; VAS: visual analog scale; WORC: Western Ontario Rotator Cuff index.
Table 2
PRP studies
| Author (year) | Level of evidence | Study design | Pathology | Intervention | Composition of PRP | Outcome measure | Conclusions | Complications |
|---|---|---|---|---|---|---|---|---|
| Kesikburun et al. (2013) | I | Design: RC Intervention: PRP vs. saline Sample size: 40 [20 PRP] Follow-up: 1 year | Rotator cuff tendinosis or partial tendon tear | Ultrasound-guided intra-tendinous injection into the center of the lesion and at 4 sites around the lesion | P: 5 mL (1014.9 | WORC, SPADI, VAS, RO | No significant difference between PRP and placebo groups for any outcomes measured | No major. Self-limited local inflammatory pain after injection |
| Rha et al. (2013) | I | Design: RC Intervention: PRP vs. dryneedling Sample size: 39 [20 PRP] Follow-up: 6 months | Supraspinatus tendon lesion (tendinosis or partial tear | Two dry needling procedures or two PRP injections at 4-week intervals under ultrasound guidance | P: 3 m L: N R: N A: N | SPADI, ROM, physician global rating scale, ultrasound measuremen | PRP superior to dry needling regarding SPADI at 6 months | No major complications reported |
| Damjanov et al. (2018) | II | Design: RC Intervention: ACS vs.betamethasone Sample size: 32 [16 ACS] Follow-up: 24 weeks | Chronic supraspinatus tendinopathy on ultrasound | Four ultrasound-guided ACS injections once weekly over 4 weeks vs. 3 betamethasone injections once weekly over 3 weeks with saline injection at week 4 into the enthesis and para-tenon of the supraspinatus tendon | P: 2 m L: N R: N A: N | VAS, CMS | PRP superior to steroid regarding pain and shoulder function at 24 weeks | No complications reported |
| Cai et al. (2019) | I | Design: RC Intervention: saline vs. sodium hyaluronate vs. PRP vs. SH | Partial thickness rotator cuff tear | Ultrasound-guided subacromial injection of saline, SH, PRP, or SH | P: 4 mL (PRPgroup), 2 mL(SH | Constant, ASES, VAS, MRI | PRP superior to placebo and SH for Constant at 12 months | Not reported |
| Shams et al. (2016) | II | Design: RC Intervention: PRP vs. corticosteroid Sample size: 40 [20 PRP] Follow-up: 6 months | Partial thickness rotator cuff tear | Subacromial injection of PRP or corticosteroid (40 mg triamcinolone) | P: 2.5 m L: – R: N A: NR | ASES, CMS, SST, VAS, MRI | PRP not superior to steroid for any outcomes at 6 months | Not reported |
| Ilhanli et al. (2015) | I | Design: RC Intervention: PRP vs. physical therapy Sample size: 62 [30 PRP] Follow-up: 12 months | Chronic partial supraspinatus tear | Intraarticular PRP once a week for 3 weeks vs. 15 sessions of standard exercise therapy | P: 6 mL (concentration 2.1–2.5 | ROM, VAS, DASH, Neer’s, Hawkins’, drop arm test | PRP superior for functional outcomes but not ROM compared to PT at 1 year | No complications reported |
| Schwitzguebel et al. (2019) | I | Design: RC Intervention: PRP vs. saline Sample size: 80 [41 PRP] Follow-up: 7 months | Isolated interstitial supraspinatus tear | Two ultrasound-guided injections into the lesion at 1-month intervals with PRP or saline | P: 2 m L: – R: N A: – | MRI, VAS, SANE, Constant, ASES, adverse effect | PRP not superior to placebo regarding pain and functional scores at 7 months | More pain |
|
Table 2, continued | ||||||||
|---|---|---|---|---|---|---|---|---|
| Author (year) | Level of evidence | Study design | Pathology | Intervention | Composition of PRP | Outcome measure | Conclusions | Complications |
| Nejati et al. (2016) | I | Design: RC Intervention: PRP vs exercise therapy Sample size: 62 [31 PRP] Follow-up: 6 months | Subacromial impingement syndrome | Injection at baseline and 1 month into tear (ultrasound-guided) and subacromial bursa or weekly exercise therapy for 3 months | P: 4 mL (900,00/ mm | VAS, ROM, DASH, WORC, MR | Not superior to exercise | Not reported |
| Say et al. (2016) | II | Design: Cohort study Intervention: PRP vs steroid Sample size: 60 [30 PRP] Follow-up: 6 months | Subacromial impingement syndrome with MRI confirmed rotator cuff tendinosis or partial tear | One subacromial PRP or methylprednisolone injection | P: 2.5 mL (count 4 | Constant, VAS, ROM | Steroids superior to PRP regarding pain and function at 6 months | None reported |
| Von Wehren et al. (2016) | II | Design: Cohort study Intervention: PRP vs steroid Sample size: 50 [25 PRP] Follow-up: 6 months | Partial thickness supraspinatus tears | Three weekly PRP injections into lateral subacromial space or one cortisone injection | P: 5 m L: NR R: N A: N | VAS, ASES, CMS, SST | PRP superior to steroid regarding pain and function at 12 weeks but not 6 months | None reported |
| Ibrahim et al. (2019) | II | Design: RC Intervention: PRP vs steroid Sample size: 30 [15 PRP] Follow-up: 2 months | Rotator cuff tendinopathy | Single ultrasound-guided PRP or methylprednisolone injection into subacromial space | P: 2 m L: NR R: N A: | VAS, ROM, SDQ | PRP not superior to steroid regarding pain and function at 2 months | None reported |
| Kim et al. (2019) | II | Design: Cohort study Intervention: PRP vs exercise Sample size: 30 [15 PRP] Follow-up: 24 weeks | Rotator cuff tendinopathy | Single ultrasound-guided PRP injection | P: 2 mLL: NRR: NRA: NR | ASES, CMS, NRS | PRP superior to exercise at 6 and 12 weeks regarding pain, and at 24 weeks regarding pain and function | Adhesive capsulitis in 1 PRP patient |
| Sari et al. (2020) | I | Design: RCT Intervention: PRP vs prolotherapy vs steroid vs lidocaineSample size: 120 [30 PRP]Follow-up: 24 weeks | Rotator cuff tendinosis or grade I partial tears | Single ultrasound-guided subacromial injection of PRP, prolotherapy, steroid, or lidocaine | P: 5 mL (count 5 | VAS, ASES, WORC | Steroid superior to PRP, prolotherapy at 3 weeks for VAS, ASES, and WORC. PRP superior to steroid at 24 weeks for VAS and WORC | Not reported |
P: platelet count (milliliters injected, cells per microliter if applicable); L: leukocyte content (
deemed low for two studies, moderate for five studies, and high for three studies. Two cohort studies were deemed high quality and the other low quality (Fig. 2). Nine studies utilized ultrasound image guidance.
Controls in the studies were as follows: five used corticosteroid injection, three used saline injection, two used exercise therapy, one used dry needling, and one used either corticosteroid, prolotherapy, or lidocaine. For each study, PRP composition is reported using the PRLA classification system described by Mautner et al. [36]. All studies reported the volume of PRP injected, 0 reported red blood cell (RBC) concentration, 5 reported leukocyte concentration, and 7 reported if and what type of activation was used. Out of the 338 patients treated with PRP, 11 experienced pain for greater than 48 hours, 8 experienced frozen shoulder, 4 experienced lesion extension, and 1 developed adhesive capsulitis.
3.2.1PRP versus corticosteroid
Five studies evaluated PRP versus corticosteroid. Damjanov et al. compared 16 patients injected with ultrasound-guided autologous conditioned serum (ACS) into the enthesis and paratenon of the supraspinatus to 16 patients injected with betamethasone [37]. At 4 weeks, no betweengroup differences were found for VAS and Constant Shoulder Score (CSS), with both groups showing improvement from baseline. However, at 24 weeks VAS and CSS were significantly improved in the ACS group. Eight adverse events were reported for the steroid group and none for ACS.
Shams et al. compared 20 patients injected with palpation-guided PRP into the subacromial space to 20 patients treated with triamcinolone [38]. There were significantly better outcomes with PRP compared to corticosteroid in VAS, American Shoulder and Elbow Surgeon (ASES) Standardized Shoulder Assessment Form, Constant-Murley Score (CMS), and the Simple Shoulder Test (SST) at 12 weeks. However, at final 6 month follow-up, there was no statistically significant difference between groups. Nonsignificant improvement in grades of tendinopathy and tear was noted in both groups compared to baseline, with no difference between the PRP and corticosteroid groups.
Say et al. compared 30 patients injected with palpation-guided PRP into the subacromial space to 30 patients treated with a mixture of methyprednisolone and prilocaine [39]. Patients were followed up at 6 weeks and 6 months with outcomes measured by the CMS for function, VAS for pain, and range of motion of the shoulder. The steroid group showed significantly more improvement in CMS and VAS at both timepoints compared to the PRP group. No difference was found for range of motion but both groups showed similar improvement over the course of treatment.
Von Wehren et al. compared 25 patients injected three times in 7-day intervals with palpation-guided autologous conditioned serum into the subacromial space to 16 patients treated with a single cortisone injection [40]. Outcomes included the Mental Component Summary, ASES Standardized Shoulder Assessment Form, SST, and VAS. A magnetic resonance image (MRI) was also performed before and 6 months after injection. Both groups showed positive withingroup changes. At 12 weeks, ACS outperformed steroid but this difference was not sustained at 6 months. MRI data showed an improvement in tendinopathy grade for both groups, but there was not a statistically significant difference between groups.
Ibrahim et al. compared 15 patients injected under ultrasoundguidance with PRP into the subacromial subdeltoid space to 15 patients treated with methylprednisolone acetate [41]. There was a significant improvement in pain, Shoulder Disability Questionnaire (SDQ) score, range of motion, and rotator cuff tests in both groups at 8 weeks, with an insignificant difference between groups. Ultrasound findings were notable for significant improvement in the frequency of tendinitis/bursitis in the steroid group and significant improvement in partial tears and effusion in the PRP group.
3.2.2PRP versus saline
Three studies evaluated PRP versus saline. Kesikburun et al. compared 20 patients treated with ultrasound-guided PRP to 20 patients treated with saline [42]. Both groups additionally were prescribed an exercise program. Final follow-up was at one year. The primary outcome was WORC score and secondary outcomes were SPADI, VAS with Neer’s impingement sign, and passive range of motion. No significant change was noted for any outcome measure between groups at any time point.
Cai et al. compared ultrasound-guided injections into the subacromial space once weekly over a period of four weeks for 45 patients treated with PRP only, 47 patients treated with sodium hyaluronate (SH) only, 49 patients treated with PRP and SH combined, and 48 patients treated with normal saline [43]. Ultimately, the SH
Table 3
MSC studies
| Autho (year) | Level of evidence | Study design | Pathology | Intervention | Composition | Outcome measures | Conclusions | Complications |
|---|---|---|---|---|---|---|---|---|
| Centeno et al. (2020) | I | Design: RCT crossover study Intervention: BMAC | Partial to full thickness supraspinatus tears | Ultrasound-guided injection of BMAC | 1–2 mL injectate consisting of 60% by volume of BMAC | DASH, NPS, modified SANE | BMAC | No serious adverse events. Post-procedural pain in two patients |
| Kim et al. (2018) | II | Design: Prospective, non-randomized, comparative, single-blind study Intervention: BMAC | Partial tear of rotator cuff tendon | Ultrasound-guided injection of BMAC | 2 mL BMAC | VAS, MMT, ASES, tear size on ultrasound | BMAC | None reported |
ASES: American Shoulder and Elbow Surgeon Form; BMAC: bone marrow aspirate concentrate; MMT: manual muscle testing; PRP: platelet-rich plasma; PL: platelet lysate; VAS: visual analog scale.
Schwitzguebel et al. compared ultrasound-guided treatment of 41 patients injected with PRP into isolated interstitial supraspinatus tears to 39 patients injected with normal saline [44]. There was no significant difference in lesion volume, VAS score, Single Assessment Numeric Evaluation (SANE) score, CMS, or ASES score between the PRP and normal saline groups at 7 months. At final followup at a minimum of 12 months (average of 19.5 months), there were no significant difference between the PRP and control groups for VAS score or SANE score. Additionally, the authors noted significantly higher incidence of adverse events (pain for greater than 48 hours, frozen shoulder, extension of lesion to bursal or articular surface) in the PRP group compared with the normal saline group.
3.2.3PRP versus exercise therapy
Three studies evaluated PRP versus exercise therapy. Ilhanli et al. compared 30 patients treated with three weekly palpation-guided intra-articular PRP injections to 32 patients treated with exercise therapy [45]. The therapy regimen was performed five times weekly for three weeks followed by continuation in the home setting and included modalities, range of motion, stretching, and strengthening exercises. At 12 months, significant improvement in range of motion, pain, and DASH scores were noted in both groups. Range of motion improved more in the therapy group, while function via DASH score improved more in the PRP group.
Nejati et al. compared 31 patients treated with two monthly ultrasound-guided PRP injections into the injured rotator cuff tendons and subacromial bursa to 31 patients treated with exercise therapy [46]. Therapy utilized a progressive phasic approach focused on the rotator cuff and scapular stabilizers. It was supervised once weekly for three months, with a home exercise program utilized on other days. The home exercise program was continued for months three to six. The exercise therapy group outperformed the PRP group for outcome measures at 1, 3, and 6 months.
Kim et al. compared 30 patients treated with a single ultrasoundguided PRP injection utilizing a peppering technique to 30 patients treated with exercise therapy [47]. Exercises were performed for 20 minutes at least 4 days per week without any supervision. While both groups received education regarding the exercise regimen, the PRP group was not formally instructed to follow the regimen nor was their compliance with it measured. There was no significant difference in the ASES and CMS between the two groups at 6 and 12 weeks. However at 24 weeks the PRP group outperformed the exercise group. The Numeric Rating Scale (NRS) scores significantly improved for the PRP group compared to the control group at 6 weeks, but not at 12 and 24 weeks.
3.2.4PRP versus dry needling
One study evaluated PRP versus dry needling. Rha et al. compared 20 patients treated with two ultrasound-guided PRP injections into the supraspinatus tendon separated by a 4-week interval to 19 patients treated with dry needling. Dry needling was performed under ultrasound-guidance and involved passing a needle through the lesion approximately 40–50 times, in two sessions over a 4 week interval [48]. Both groups showed a significant reduction in the SPADI score and improvement in range of motion at all followup visits compared to baseline. At six months, the SPADI score was significantly better for the PRP group compared to the dry needling group. Notably, in sonographic assessment of the 16 patients in the PRP group who completed the sixmonth follow-up, two patients with partial-thickness tears (1 articular tear and 1 bursal surface tear) of the supraspinatus improved to tendinosis and two patients with tendinosis improved to normal status. In 14 patients in the dry needling group who completed the six-month follow-up, no partial tears of the supraspinatus improved to tendinosis and one case of tendinosis improved to normal status.
3.2.5PRP versus prolotherapy versus corticosteroid versus lidocaine
One study by Sari et al. evaluated 120 patients treated a single ultrasound-guide injection into the subacromial bursa with either PRP, prolotherapy (20% dextrose), triamcinolone, or 1% lidocaine [49]. There were 30 patients in each of the four groups, and all were given a shoulder rehabilitation program to complete for 6 weeks. They found the corticosteroid group had significantly lower VAS and WORC scores at 3 weeks compared to the other groups, while the PRP group outperformed corticosteroid at 24 weeks.
3.3Studies utilizing MSCs
Two studies evaluated the therapeutic effects of bone marrow aspirate concentrate (BMAC) with a total of 49 participants (26 BMAC and 23 control). Study characteristics are outlined in Table 3. Follow-up periods ranged from 3 to 24 months. One was an RCT and one was a cohort study. The RCT was deemed to be of moderate bias risk and the cohort study was deemed to be of good quality (Fig. 2). Out of the 26 patients treated with BMAC, 2 reported post-procedural pain, 2 later developed contralateral shoulder pain, and 1 patient developed hand numbness 12 months after the procedure.
Kim et al. evaluated 12 patients treated with a combination of ultrasoundguided BMAC and PRP against 12 patients treated with a three-month home exercise program [50]. Outcomes included VAS, strength testing, and ASES scores. At 3 months VAS scores (
Centeno et al. evaluated 14 patients treated with ultrasound-guided injections of BMAC
4.Discussion
This systematic review provides an overview of the available evidence regarding outcomes of non-operative orthobiologic use for treatment of shoulder pathology. Twenty studies in total were included with most utilizing PRP and all evaluating rotator cuff pathology. Providers are increasingly using these agents to treat recalcitrant cases of tendon disease and arthritis, and knowledge of the current literature regarding these treatments is imperative to guide clinical decision making. Across studies, there were no major adverse safety events reported, suggesting that orthobiologics provide a relatively safe treatment option. However, data on their efficacy have thus far been conflicting. Consistent with reviews on orthobiologics for treatment of other musculoskeletal conditions, our review found significant heterogeneity between injection protocols, agent composition, outcome measures, and results across studies evaluating their use in conditions affecting the shoulder. Notably, no studies evaluating outcomes for glenohumeral osteoarthritis met the inclusion criteria.
4.1Prolotherapy
Wide variation exists regarding usage patterns of prolotherapy, but one common feature is injection of an irritant agent into a painful tendon/ligament and the adjacent space over a course of one or more treatment sessions [52]. Most commonly, an osmotic agent such as dextrose is utilized. Concentrations over 10% are required to induce the inflammatory mechanisms thought responsible for stimulation of healing [53]. Interestingly, amongst the prolotherapy studies evaluated in this review, the two in which significant pain relief was sustained long-term both utilized multiple injections and the three with either non-significant or non-sustained pain relief used a single injection.
Additionally, higher concentrations of dextrose were used in the positive studies. A trial on temporomandibular joint hypomobility found no changes in outcome based on differing prolotherapy concentration above 10% [54]. They postulated after the threshold concentration for inflammation induction was met, specific concentration was not as critical to outcomes. Whether these results translate to shoulder pathology requires additional study. Imaging guidance improves injection accuracy through direct visualization of the target and was used in four studies, three of which had negative findings.
Taken together, these findings suggest prolotherapy to be a safe treatment option with perhaps greater efficacy for shoulder pathology when provided through a series of injections using higher concentrations of dextrose. Methodologic quality varied in the reviewed studies limiting overall interpretation. Only one study by Lin et al. was deemed low risk of bias. Development of higher-quality study protocols will be important for clarifying the efficacy of prolotherapy for treatment of shoulder injuries.
4.2PRP
PRP is the most wellstudied orthobiologic for shoulder pathology, and this trend persisted in our paper where it comprised the bulk of reviewed studies. Most analyses have focused on PRP use in conjunction with operative intervention, and results have been mixed. Short-term results of improved pain and functional outcomes were found by Wang et al. when PRP was used at the time of rotator cuff repair [55]. Cai et al. found the use of PRP in full-thickness rotator cuff repairs to have no significant benefit regarding clinical outcomes but did show a lower failure-to-heal rate in small and moderately sized tears [56]. The literature regarding non-operative use is more sparse. A systematic review by Hurley et al. evaluated 5 RCTs on non-operative outcomes for PRP in rotator cuff pathology, all of which are included in the present review. Their review concluded PRP may not be beneficial in the short term for chronic rotator cuff pathology [30].
Throughout all reviews, there was a wide range of methodologic variability limiting interpretation of results. Standardization of solution preparation and reporting has repeatedly been called for. Using the PRLA classification system for PRP formulations, we found no studies to report on all components. The amount of PRP used was the only consistently reported parameter. However, total administered platelet counts were reported in only three studies. Three additional studies included in this review reported platelet concentration above baseline, which can drastically differ depending on the donor’s baseline values.
Leukocyte content and use of an activating agent are of particular interest as they may affect treatment response. Chen et al. reviewed 18 studies using PRP and found leukocyte-rich preparations to have worse pain outcomes for rotator cuff tears [57]. Leukocyte content was only reported in 5 studies evaluated here, of which four used leukocyte-poor preparations with positive results in one and negative results in three. The sole study using a leukocyte-rich preparation had positive outcomes [45]. Interestingly, these studies did not specify the types of leukocytes present, leaving it unclear as to whether specific classes of leukocytes monocytes or neutrophils impact the clinical efficacy of PRP. One review defined leukocyte-rich preparations as having a neutrophil concentration above baseline, with below baseline being classified as leukocyte-poor [58]. However, the PRLA classification system defines leukocyte-poor as less than 1% total concentration and leukocyte-rich as greater than 1% total concentration. Adoption of a standardized definitions with precise cutoff values would allow more consistent reporting and reproducibility.
PRP activation refers to using an agent during preparation that activates platelet degranulation and induces a gel formation to confine platelet secretion to the chosen site [59]. A review by Warth et al. found no difference in Constant scores between activated and non-activated preparations in patients undergoing rotator cuff repair [60]. Activation status was reported in 7 studies evaluated here. Four reported using an activating agent, with only two having positive functional outcomes. Amongst the three using non-activated PRP, none found PRP superior to control. This again highlights the need for standardized preparation reporting as it remains unclear if an optimal formulation exists
4.3MSCs
Only two studies evaluating MSCs met the inclusion criteria highlighting the limited literature available for this increasingly popular treatment option. Notably, despite good methodological quality, MSCs alone were not used, but instead a combination of BMAC and PRP. It remains unclear if these positive results were from the MSCs, adjuvant treatment, or the combination of both. In the operative setting, Hernigou et al. found enhanced tendon healing and quality when single-row rotator cuff repair was performed in conjunction with BMAC injection [61]. Notably, patients with a loss of tendon integrity during the ten-year follow-up period received fewer MSCs as compared with those who had maintained a successful repair during the same interval leading the authors to conclude that the number of transplanted MSCs was the most important outcome determinant. Whether these results will translate to improvement in pain and functional outcomes is unclear.
Low evidencelevel studies comprise most of the literature on MSCs use for shoulder pathology. In a large case series, Centeno et al. treated 115 shoulders with rotator cuff tears and glenohumeral arthritis with autologous BMAC. Improvement in pain and disability was observed one month post-treatment and continued for up to 2 years [62]. No serious adverse events were reported. Notably, follow-up functional outcomes were only completely reported for 40 of the original 115 shoulders treated. Striano et al. reported results on 18 patients with chronic shoulder pain treated with micronized adipose fat transfer [63]. Patients were followed for one year and significant improvement was noted for pain reduction and functional improvement using the Numeric Pain Scale and American Shoulder and Elbow Surgeons Score. More well-designed studies are needed to evaluate clinical impact of MSCs use and to provide insight on the role of MSCs source in efficacy.
4.4Limitations
The results of this systematic review are limited by several factors. Inclusion of only English-language studies introduces selection bias. Wide diversity in preparations, injection protocols, outcome measures, and follow-up times inherently limits generalizability. Only three of thirteen PRP studies noted the platelet count delivered, drastically limiting the ability to draw comparative conclusions between studies and between treatment modalities. No meta-analysis was performed within orthobiologic groups which would have allowed for more objective efficacy assessments. Furthermore, only fifteen out of twenty studies performed injections under ultrasound guidance, thereby skewing the potential effectiveness of the orthobiologic.
4.5Conclusions and future directions
The primary finding of this review was that orthobiologics offer a relatively safe management option carrying a low risk of minor complications with inconclusive evidence for or against its use for rotator cuff pathology. No studies met our inclusion criteria that explored the effect of orthobiologic intervention on glenohumeral osteoarthritis, and thus no conclusions could be made regarding orthobioloic safety or efficacy for the treatment of glenohumeral osteoarthritis. Adoption of standardized preparation reporting and consistent use of functional outcome measures is imperative for future studies to consider.
Conflict of interest
None to report.
Funding
None to report.
References
[1] | Luime JJ, Koes BW, Hendriksen IJM, Burdorf A, Verhagen AP, Miedema HS, Verhaar JAN. Prevalence and incidence of shoulder pain in the general population; a systematic review. Vol. 33, Scandinavian Journal of Rheumatology. (2004) . 73–81. |
[2] | Millett PJ, Gobezie R, Boykin RE. Shoulder osteoarthritis: Diagnosis and management. Vol. 78, American Family Physician. American Academy of Family Physicians. (2008) . |
[3] | Ludewig PM, Borstad JD. Effects of a home exercise programme on shoulder pain and functional status in construction workers. Occup Environ Med. (2003) Nov; 60: (11): 841–9. |
[4] | Sawatzky BJ, Slobogean GP, Reilly CW, Chambers CT, Hol AT. Prevalence of shoulder pain in adult-versus childhood-onset wheelchair users: a pilot study. J Rehabil Res Dev. (2005) May; 42: (3 SUPPL. 1): 1–8. |
[5] | Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, Simmons A, Williams G. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis. (1998) ; 57: (11): 649–55. |
[6] | Heuberer PR, Plachel F, Willinger L, Moroder P, Laky B, Pauzenberger L, Lomoschitz F, Anderl W. Critical shoulder angle combined with age predict five shoulder pathologies: a retrospective analysis of 1000 cases. BMC Musculoskelet Disord. (2017) ; 18: (1). |
[7] | Meislin RJ, Sperling JW, Stitik TP. Persistent shoulder pain: epidemiology, pathophysiology, and diagnosis. Am J Orthop (Belle Mead NJ) [Internet]. (2005) Dec [cited 2019 Sep 7]; 34: (12 Suppl): 5–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/16450690. |
[8] | Sambandam SN, Khanna V, Gul A, Mounasamy V. Rotator cuff tears: An evidence based approach. Vol. 6, World Journal of Orthopaedics. Baishideng Publishing Group Co; (2015) . 902–18. |
[9] | Oliva F, Osti L, Padulo J, Maffulli N. Epidemiology of the rotator cuff tears: a new incidence related to thyroid disease. Muscles Ligaments Tendons J. (2014) Jul 1; 4: (3): 309–14. |
[10] | Anderson BC, Curtis MR. Glenohumeral osteoarthritis http:// www.uptodate.com/contents/glenohumeral-osteoarthritis? topicKe… Shoulder Elb [Internet]. (2016) [cited 2019 Nov 9]; 8: (3): 1–20. Available from: doi: 10.1177/1758573216644183. |
[11] | Dean BJF, Lostis E, Oakley T, Rombach I, Morrey ME, Carr AJ. The risks and benefits of glucocorticoid treatment for tendinopathy: A systematic review of the effects of local glucocorticoid on tendon. Vol. 43, Seminars in Arthritis and Rheumatism. (2014) . 570–6. |
[12] | Sherman SL, Khazai RS, James CH, Stoker AM, Flood DL, Cook JL. In vitro toxicity of local anesthetics and corticosteroids on chondrocyte and synoviocyte viability and metabolism. Cartilage. (2015) Jan 1; 6: (4): 233–40. |
[13] | Matthewson G, Beach CJ, Nelson AA, Woodmass JM, Ono Y, Boorman RS, Lo IKY, Thornton GM. Partial Thickness Rotator Cuff Tears: Current Concepts [Internet]. Vol. 2015, Advances in Orthopedics. Hindawi Limited; (2015) [cited 2020 Sep 8]. Available from: https://pubmed.ncbi.nlm.nih.gov/26171251/. |
[14] | Strauss EJ, Salata MJ, Kercher J, Barker JU, McGill K, Bach BR, Romeo AA, Verma NN. The arthroscopic management of partial-thickness rotator cuff tears: A systematic review of the literature [Internet]. Vol. 27, Arthroscopy – Journal of Arthroscopic and Related Surgery. Arthroscopy; (2011) [cited 2020 Sep 8]. 568–80. Available from: https://pubmed.ncbi.nlm.nih.gov/21296545/. |
[15] | Kartus J, Kartus C, Rostgård-Christensen L, Sernert N, Read J, Perko M. Long-term clinical and ultrasound evaluation after arthroscopic acromioplasty in patients with partial rotator cuff tears. Arthrosc – J Arthrosc Relat Surg [Internet]. (2006) Jan [cited 2020 Sep 8]; 22: (1): 44–9. Available from: https://pubmed.ncbi.nlm.nih.gov/16399460/. |
[16] | Borg-Stein J, Osoria HL, Hayano T. Regenerative sports medicine: past, present, and future (adapted from the PASSOR legacy award presentation; AAPMR; October 2016). PM R [Internet]. (2018) [cited 2019 Sep 7]; 10: (10): 1083–105. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30031963. |
[17] | Anz AW, Bapat A, Murrell WD. Concepts in regenerative medicine: Past, present, and future in articular cartilage treatment. Vol. 7, Journal of Clinical Orthopaedics and Trauma. Elsevier B.V.; (2016) . 137–44. |
[18] | Hauser RA, Lackner JB, Steilen-Matias D, Harris DK. A systematic review of dextrose prolotherapy for chronic musculoskeletal pain. Vol. 9, Clinical Medicine Insights: Arthritis and Musculoskeletal Disorders. Libertas Academica Ltd.; (2016) . 139–59. |
[19] | DeChellis DM, Cortazzo MH. Regenerative medicine in the field of pain medicine: prolotherapy, platelet-rich plasma therapy, and stem cell therapy-theory and evidence. Tech Reg Anesth Pain Manag. (2011) Apr; 15: (2): 74–80. |
[20] | Pourcho AM, Smith J, Wisniewski SJ, Sellon JL. Intraarticular platelet-rich plasma injection in the treatment of knee osteoarthritis: review and recommendations. Am J Phys Med Rehabil. (2014) ; 93: (11): S108–21. |
[21] | Andia I, Rubio-Azpeitia E, Maffulli N. Platelet-rich plasma modulates the secretion of inflammatory/angiogenic proteins by inflamed tenocytes. Clin Orthop Relat Res [Internet]. (2015) May [cited 2019 Nov 23]; 473: (5): 1624–34. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25670657. |
[22] | Caplan AI. Mesenchymal stem cells: time to change the name! Stem Cells Transl Med. (2017) ; 6: (6): 1445–51. |
[23] | Maqsood M, Kang M, Wu X, Chen J, Teng L, Qiu L. Adult mesenchymal stem cells and their exosomes: Sources, characteristics, and application in regenerative medicine [Internet]. Vol. 256, Life Sciences. Elsevier Inc.; (2020) [cited 2020 Sep 8]. Available from: https://pubmed.ncbi.nlm.nih.gov/32585248/. |
[24] | Freitag J, Bates D, Boyd R, Shah K, Barnard A, Huguenin L, Tenen A. Mesenchymal stem cell therapy in the treatment of osteoarthritis: Reparative pathways, safety and efficacy – A review. Vol. 17, BMC Musculoskeletal Disorders. BioMed Central Ltd.; (2016) . |
[25] | Djouad F, Bouffi C, Ghannam S, Noël D, Jorgensen C. Mesenchymal stem cells: innovative therapeutic tools for rheumatic diseases. Nat Rev Rheumatol [Internet]. (2009) Jul [cited 2019 Sep 7]; 5: (7): 392–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19568253. |
[26] | Moher D, Liberati A, Tetzlaff J, Altman DG, Altman D, Antes G, et al. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Vol. 6, PLoS Medicine. (2009) . |
[27] | Wright JG, Swiontkowski MF, Heckman JD. Introducing levels of evidence to the journal. Vol. 85, Journal of Bone and Joint Surgery – Series A. Journal of Bone and Joint Surgery Inc.; (2003) . 1–3. |
[28] | Ottawa Hospital Research Institute [Internet]. [cited 2019 Nov 23]. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp. |
[29] | Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. (2019) ; 366: . |
[30] | Hurley ET, Hannon CP, Pauzenberger L, Fat DL, Moran CJ, Mullett H. Nonoperative treatment of rotator cuff disease with platelet-rich plasma: a systematic review of randomized controlled trials. Arthroscopy [Internet]. (2019) May [cited 2019 Nov 23]; 35: (5): 1584–91. Available from: http://www.ncbi.nlm.nih.gov/pubmed/31000394. |
[31] | Bertrand H, Reeves KD, Bennett CJ, Bicknell S, Cheng A-L. Dextrose prolotherapy versus control injections in painful rotator cuff tendinopathy. Arch Phys Med Rehabil [Internet]. (2016) Jan [cited 2019 Aug 28]; 97: (1): 17–25. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26301385. |
[32] | Lin C-L, Huang C-C, Huang S-W. Effects of hypertonic dextrose injection in chronic supraspinatus tendinopathy of the shoulder: a randomized placebo-controlled trial. Eur J Phys Rehabil Med [Internet]. (2019) Aug [cited 2019 Aug 29]; 55: (4): 480–7. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30543266. |
[33] | Seven MM, Ersen O, Akpancar S, Ozkan H, Turkkan S, Yıldız Y, Koca K. Effectiveness of prolotherapy in the treatment of chronic rotator cuff lesions. Orthop Traumatol Surg Res [Internet]. (2017) [cited 2019 Aug 29]; 103: (3): 427–33. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28215611. |
[34] | George J, Li SC, Jaafar Z, Hamid MSA. Comparative effectiveness of ultrasound-guided intratendinous prolotherapy injection with conventional treatment to treat focal supraspinatus tendinosis. Scientifica (Cairo) [Internet]. (2018) [cited 2019 Aug 29]; 2018: : 4384159. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30057849. |
[35] | Cole B, Lam P, Hackett L, Murrell GAC. Ultrasound-guided injections for supraspinatus tendinopathy: corticosteroid versus glucose prolotherapy – a randomized controlled clinical trial. Shoulder Elb [Internet]. (2018) Jul [cited 2019 Aug 29]; 10: (3): 170–8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29796104. |
[36] | Mautner K, Malanga GA, Smith J, Shiple B, Ibrahim V, Sampson S, Bowen JE. A call for a standard classification system for future biologic research: the rationale for new PRP nomenclature. PM R [Internet]. (2015) Apr [cited 2019 Nov 23]; 7: (4 Suppl): S53–9. Available from: http://www.ncbi.nlm.nih.gov/pubmed/25864661. |
[37] | Damjanov N, Barac B, Colic J, Stevanovic V, Zekovic A, Tulic G. The efficacy and safety of autologous conditioned serum (ACS) injections compared with betamethasone and placebo injections in the treatment of chronic shoulder joint pain due to supraspinatus tendinopathy: a prospective, randomized, double-blind, controlled study. Med Ultrason [Internet]. (2018) Aug 30 [cited 2019 Aug 28]; 20: (3): 335–41. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30167587. |
[38] | Shams A, El-Sayed M, Gamal O, Ewes W. Subacromial injection of autologous platelet-rich plasma versus corticosteroid for the treatment of symptomatic partial rotator cuff tears. Eur J Orthop Surg Traumatol [Internet]. (2016) Dec [cited 2019 Aug 28]; 26: (8): 837–42. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27544678. |
[39] | Say F, Gurler D, Bulbul M. Platelet-rich plasma versus steroid injection for subacromial impingement syndrome. J Orthop Surg (Hong Kong) [Internet]. (2016) [cited 2019 Oct 19]; 24: (1): 62–6. Available from: http://www.ncbi.nlm.nih.gov/pubmed/27122515. |
[40] | von Wehren L, Blanke F, Todorov A, Heisterbach P, Sailer J, Majewski M. The effect of subacromial injections of autologous conditioned plasma versus cortisone for the treatment of symptomatic partial rotator cuff tears. Knee Surg Sports Traumatol Arthrosc [Internet]. (2016) Dec [cited 2019 Oct 13]; 24: (12): 3787–92. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26017742. |
[41] | Ibrahim DH, El-Gazzar NM, El-Saadany HM, El-Khouly RM. Ultrasound-guided injection of platelet rich plasma versus corticosteroid for treatment of rotator cuff tendinopathy: effect on shoulder pain, disability, range of motion and ultrasonographic findings. Egypt Rheumatol. (2019) Apr 1; 41: (2): 157–61. |
[42] | Kesikburun S, Tan AK, Yilmaz B, Yaşar E, Yazicioğlu K. Platelet-rich plasma injections in the treatment of chronic rotator cuff tendinopathy: a randomized controlled trial with 1-year follow-up. Am J Sports Med [Internet]. (2013) Nov [cited 2019 Aug 28]; 41: (11): 2609–16. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23893418. |
[43] | Cai YU, Sun Z, Liao B, Song Z, Xiao T, Zhu P. Sodium hyaluronate and platelet-rich plasma for partial-thickness rotator cuff tears. Med Sci Sports Exerc [Internet]. (2019) [cited 2019 Aug 29]; 51: (2): 227–33. Available from: http://www.ncbi.nlm.nih.gov/pubmed/30199423. |
[44] | Schwitzguebel AJ, Kolo FC, Tirefort J, Kourhani A, Nowak A, Gremeaux V, Saffarini M, Lädermann A. Efficacy of platelet-rich plasma for the treatment of interstitial supraspinatus tears: a double-blinded, randomized controlled trial. Am J Sports Med. (2019) Jul 1; 47: (8): 1885–92. |
[45] | Ilhanli I, Guder N, Gul M. Platelet-rich plasma treatment with physical therapy in chronic partial supraspinatus tears. Iran Red Crescent Med J [Internet]. (2015) Sep [cited 2019 Aug 29]; 17: (9): e23732. Available from: http://www.ncbi.nlm.nih.gov/pubmed/26473076. |
[46] | Nejati P, Ghahremaninia A, Naderi F, Gharibzadeh S, Mazaherinezhad A. Treatment of subacromial impingement syndrome: platelet-rich plasma or exercise therapy? A randomized controlled trial. Orthop J Sport Med [Internet]. (2017) May [cited 2019 Oct 19]; 5: (5): 2325967117702366. Available from: http://www.ncbi.nlm.nih.gov/pubmed/28567426. |
[47] | Kim SJ, Yeo SM, Noh SJ, Ha CW, Lee BC, Lee HS, Kim SJ. Effect of platelet-rich plasma on the degenerative rotator cuff tendinopathy according to the compositions. J Orthop Surg Res [Internet]. (2019) Dec 2 [cited 2020 Sep 11]; 14: (1). Available from: https://pubmed.ncbi.nlm.nih.gov/31791360/. |
[48] | Rha D, Park G-Y, Kim Y-K, Kim MT, Lee SC. Comparison of the therapeutic effects of ultrasound-guided platelet-rich plasma injection and dry needling in rotator cuff disease: a randomized controlled trial. Clin Rehabil [Internet]. (2013) Feb [cited 2019 Aug 28]; 27: (2): 113–22. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23035005. |
[49] | Sari A, Eroglu A. Comparison of ultrasound-guided platelet-rich plasma, prolotherapy, and corticosteroid injections in rotator cuff lesions. J Back Musculoskelet Rehabil [Internet]. (2020) [cited 2020 Sep 11]; 33: (3): 387–96. Available from: https://pubmed.ncbi.nlm.nih.gov/31743987/. |
[50] | Kim SJ, Kim EK, Kim SJ, Song DH. Effects of bone marrow aspirate concentrate and platelet-rich plasma on patients with partial tear of the rotator cuff tendon. J Orthop Surg Res [Internet]. (2018) Jan 3 [cited 2019 Aug 28]; 13: (1): 1. Available from: http://www.ncbi.nlm.nih.gov/pubmed/29298726. |
[51] | Centeno C, Fausel Z, Stemper I, Azuike U, Dodson E. A randomized controlled trial of the treatment of rotator cuff tears with bone marrow concentrate and platelet products compared to exercise therapy: a midterm analysis. Stem Cells Int [Internet]. (2020) [cited 2020 Sep 11]; 2020. Available from: https://pubmed.ncbi.nlm.nih.gov/32399045/. |
[52] | Rabago D, Slattengren A, Zgierska A. Prolotherapy in Primary Care Practice. Vol. 37, Primary Care – Clinics in Office Practice. (2010) . 65–80. |
[53] | Jensen KT, Rabago DP, Best TM, Patterson JJ, Vanderby R. Early inflammatory response of knee ligaments to prolotherapy in a rat model. J Orthop Res [Internet]. (2008) Jun [cited 2019 Nov 29]; 26: (6): 816–23. Available from: http://www.ncbi.nlm.nih.gov/pubmed/18240327. |
[54] | Mustafa R, Güngörmüş M, Mollaoglu N. Evaluation of the efficacy of different concentrations of dextrose prolotherapy in temporomandibular joint hypermobility treatment. J Craniofac Surg. (2018) Jul 1; 29: (5): e461–5. |
[55] | Wang C, Xu M, Guo W, Wang Y, Zhao S, Zhong L. Clinical efficacy and safety of platelet-rich plasma in arthroscopic full-thickness rotator cuff repair: a meta-analysis. PLoS One. (2019) ; 14: (7). |
[56] | Cai YZ, Zhang C, Lin XJ. Efficacy of platelet-rich plasma in arthroscopic repair of full-thickness rotator cuff tears: a meta-analysis. J Shoulder Elb Surg. (2015) Dec 1; 24: (12): 1852–9. |
[57] | Chen X, Jones IA, Togashi R, Park C, Vangsness CT. Use of Platelet-Rich Plasma for the Improvement of Pain and Function in Rotator Cuff Tears: A Systematic Review and Meta-analysis With Bias Assessment. Am J Sports Med [Internet]. (2019) Nov 19 [cited 2019 Nov 27]; 036354651988142. Available from: doi: 10.1177/0363546519881423. |
[58] | Le ADK, Enweze L, DeBaun MR, Dragoo JL. Current Clinical Recommendations for Use of Platelet-Rich Plasma. Vol. 11, Current Reviews in Musculoskeletal Medicine. Humana Press Inc.; (2018) . 624–34. |
[59] | Cavallo C, Roffi A, Grigolo B, Mariani E, Pratelli L, Merli G, Kon E, Marcacci M, Filardo G. Platelet-Rich Plasma: The Choice of Activation Method Affects the Release of Bioactive Molecules. Biomed Res Int. 2016; 2016. |
[60] | Warth RJ, Dornan GJ, James EW, Horan MP, Millett PJ. Clinical and structural outcomes after arthroscopic repair of full-thickness rotator cuff tears with and without platelet-rich product supplementation: a meta-analysis and meta-regression. Arthrosc – J Arthrosc Relat Surg. (2015) ; 31: (2): 306–20. |
[61] | Hernigou P, Flouzat Lachaniette CH, Delambre J, Zilber S, Duffiet P, Chevallier N, Rouard H. Biologic augmentation of rotator cuff repair with mesenchymal stem cells during arthroscopy improves healing and prevents further tears: a case-controlled study. Int Orthop. (2014) ; 38: (9): 1811–8. |
[62] | Centeno CJ, Al-Sayegh H, Bashir J, Goodyear SH, D Freeman M. A prospective multi-site registry study of a specific protocol of autologous bone marrow concentrate for the treatment of shoulder rotator cuff tears and osteoarthritis. J Pain Res. (2015) Jun 5; 8: : 269–76. |
[63] | RD Striano GMNBKA. Refractory shoulder pain with osteoarthritis, and rotator cuff tear, treated with micro fragmented adipose tissue. Orthop Spine Sport Med. (2018) ; 2: : 14. |


