
Optimal activation ratio of the scapular muscles in closed kinetic chain shoulder exercises: A systematic review
Abstract
BACKGROUND:
Muscle synergies contribute to scapular position during arm movement. The trapezius and serratus anterior (SA) muscles are the main stabilizers and are therefore the main target muscles of therapeutic exercises.
OBJECTIVE:
To systematically review the current literature investigating the optimal activation ratio of the scapular muscles during a range of closed kinetic chain exercises.
METHODS:
A systematic review search was conducted to identify studies reporting shoulder electromyography (EMG) activity during rehabilitation exercises in healthy participants. The search was conducted in PubMed, Cochrane Library, MEDLINE, CINAHL, Scopus, SPORTDiscus, and ScienceDirect. The included studies reported closed kinetic chain exercises and the muscle activity as a percentage of maximum voluntary isometric contraction (%MVIC) or muscle ratios of the lower trapezius (LT), middle trapezius (MT), and SA with respect to the upper trapezius (UT). Muscle ratios were classified as optimal if they were equal to or lower than 0.6, and the adapted Newcastle-Ottawa Scale (NOS) was used to evaluate the methodological quality of the selected studies.
RESULTS:
Twenty-nine studies were included in this review; 7 main exercises and 30 variations of these were reported. The average electromyographic activity of the concentric and eccentric phase was considered. Half Push Up, Push Up Plus, and Scap Protraction exercises showed optimal SA activity (UT/SA
CONCLUSIONS:
The exercises in higher positions (e.g. exercises with the trunk closest to the vertical line) or unstable surfaces tend to favor UT activity over the MT, LT and SA. The exercises including scapular retraction showed optimal UT/MT and UT/LT ratios, while those including scapular protraction showed optimal UT/SA ratios. This will assist therapists in the correct selection of exercises for shoulder rehabilitation.
1.Introduction
The scapulothoracic joint is part of the shoulder joint complex [1]. In this joint, the action of the muscle force couples contributes to the scapular position during arm movement [2]. The main muscles responsible for this function are the trapezius and serratus anterior (SA) [3], and for this reason, they are the main target muscles of therapeutic exercises in scapular rehabilitation and training programs [4].
The absence of adequate muscle coordination in the shoulder joint complex tends to alter the scapular position and movement. This concept is known as scapular dyskinesis [5]. This dysfunction is considered a predisposing factor in shoulder pathologies, such as rotator cuff tendonitis, rotator cuff tendon rupture, and subacromial impingement syndrome, among others [3]. It has been observed that participants with shoulder pain have muscle imbalances between the scapulothoracic and glenohumeral muscles [6], and because of this, the current rehabilitation and prevention programs of shoulder injuries seek to reestablish adequate muscular activity [4]. These programs are based on therapeutic exercises in open and closed kinetic chain [7, 8]. Currently, there is evidence regarding the positive and negative effects of open kinetic chain exercises on the stabilizing and mobilizing muscles (primary motors) of the shoulder [9, 10]. However, information on the effects of closed kinetic chain shoulder exercises is limited. In this context, a few exercises such as Push Up, Press Up and Pull Up have shown positive effects on scapular joint stability, since they recruit the scapular stabilizing muscles and produce a lower electromyographic (EMG) activation amplitude of the primary motor muscles of the shoulder [7, 11, 12, 13].
Several authors have studied EMG activity in healthy and symptomatic people during shoulder rehabilitation exercises, evidencing alterations in EMG amplitude and latency [2, 14, 15, 16]. For example, an overactivation of the upper trapezius (UT) – expressed through the percentage of maximum voluntary isometric contraction (%MVIC) – and a decreased activation of the lower trapezius (LT) and serratus anterior (SA) have been observed in people with subacromial impingement syndrome [2, 14]. In this context, several reports have considered that the optimal exercises in the shoulder rehabilitation are those that present a low UT activation ratio with respect to the middle trapezius (MT), LT and SA muscles [3, 6, 7, 16, 17]. Specifically, a ratio less than 0.6 between %MVIC of the UT and other scapular muscles (MT, LT and SA) has been considered optimal [3, 16]. There are multiple investigations that compare EMG activation of shoulder muscles during scapular rehabilitation exercises [17, 18, 19]. However, it is difficult to make an accurate comparison between studies due to methodological variability in the acquisition and processing of EMG signals, creating a confusing variable when comparing a certain exercise between studies. Recently, Schory et al. compared the ratios of activation of the scapular muscles in open kinetic chain exercises from several studies, finding higher ratios in exercises in the standing position, and decreasing when changing to prone or lateral positions [10]. However, to date there is no systematic review that provides methodologically comparable information on the activation ratios of scapular muscles in closed kinetic chain exercises. Such information could provide better knowledge of closed kinetic chain exercises and promote an optimal scapular muscle activation, assisting when developing shoulder rehabilitation exercises. The purpose of this manuscript was to systematically review the current literature investigating optimal activation ratio of the scapular muscles during a range of closed kinetic chain exercises.
2.Methods
2.1Study design
This study is a systematic review reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [20].
2.2Database source and search criteria
The search strategy was carried out according to the following electronic databases: MEDLINE, PubMed, Scopus, Cumulative Index to Nursing and Allied Health Literature (CINAHL), ScienceDirect, SPORTDiscus, and Cochrane Library, considering articles from January 1955 to January 2019. The reference lists of the selected articles were also searched to identify additional studies. The search strategy was carried out according to the databases mentioned above. See the Appendix for the detailed search strategy in each database.
Table 1
Characteristics of the included studies
| Authors | Participants | Age (SD) years | Exercises | Muscles evaluated | Outcome |
|---|---|---|---|---|---|
| Andersen (2012) [13] | 17 asymptomatic females | 29 (7.2) | Press Up, Scap Protraction | UT, MT, LT, SA | %MVIC Ratio |
| Ashnagar (2016) [35] | 40 asymptomatic females | 23.9 (1.9) | Plank | UT, SA | %MVIC |
| Batbayar (2015) [11] | 9 asymptomatic males | 25 (2.7) | Push Up Plus | UT, MT, LT, SA | %MVIC Ratio |
| Borms (2017) [38] | 15 asymptomatic females 15 asymptomatic males | 23.2 (1.8) | Half Pull Up | UT, MT, LT, SA | %MVIC |
| Calatayud (2014) [31] | 29 asymptomatic males | 22.6 (2.6) | Push Up, Unstable Push Up (suspended), Resisted Push Up | UT, SA | %MVIC |
| Cools (2014) [32] | 16 asymptomatic females 16 asymptomatic males | 22.3 (1.3) | Knee Push Up Plus | UT, MT, LT, SA | %MVIC |
| De Mey (2014) [7] | 26 asymptomatic males, 21 asymptomatic females | 22 (4.3) | Half Push Up, Knee Push Up, Scap Protraction, Unstable Scap Protraction (suspended), Supine Pull Up, Unstable Pull Up (suspended) | UT, MT, LT, SA | %MVIC Ratio |
| Gioftsos (2016) [12] | 13 asymptomatic males | 20.5 (1) | Push Up, Push Up Plus, Push Up Unstable (balance board) | UT, MT, SA | %MVIC Ratio |
| Huang (2013) [42] | 5 asymptomatic females 7 asymptomatic males | 23.8 (2.9) | Knee Push Up Plus | UT, SA | Ratio |
| Hwang (2017) [45] | 29 asymptomatic males | 24.7 (2.4) | Push Up Plus | UT, SA | %MVIC Ratio |
| Lee (2013) [27] | 20 asymptomatic males | 23.7 (1.2) 23.3 (1.4) | Scap Protraction, Unstable Scap Protraction (suspended) | UT, LT, SA | %MVIC |
| Lee (2014) [33] | 15 asymptomatic males | 22.8 (2.0) | Unstable Scap Protraction (suspended) | UT, SA | %MVIC |
| Lehman (2008) [25] | 10 asymptomatic males | 26.3 (1.1) | Half Push Up, Unstable Half Push Up (ball), Scap Protraction, Unstable Scap Protraction (ball) | UT, LT, SA | %MVIC |
| Martins (2008) [43] | 20 asymptomatic males | 22.8 (3.1) | Wall Press, Unstable Wall Press (ball), One Hand Scap Protraction, Unstable One Hand Scap Protraction (ball) | UT, SA | %MVIC Ratio |
| McCabe (2007) [22] | 15 asymptomatic males | 31.7 (9.5) | Press Up | UT, MT, LT, SA | %MVIC |
| Oliver (2018) [39] | 19 asymptomatic participants | 23.2 (4.2) | Unstable Plan (balance board), One Hand Plank | UT, LT, SA | %MVIC |
| Park (2013) [44] | 16 asymptomatic males | 22–26 | Scap Protraction | UT, SA | %MVIC Ratio |
| Park (2013) [28] | 14 asymptomatic males | 22 (2) | Push Up | UT, LT, SA | %MVIC |
| Park (2013) [29] | 20 asymptomatic males | 21–26 | Push Up, Unstable Push Up (balance board) | UT, LT, SA | %MVIC |
| Park (2015) [34] | 20 asymptomatic males | 23.9 (1.7) | Scap Protraction | UT, SA | %MVIC |
| Pontillo (2007) [23] | 15 asymptomatic males | 30 (6) | One Hand Plank | UT, LT, SA | %MVIC |
| Puhringer (2017) [40] | 14 asymptomatic males | 28.5 (8.1) | Isometric Pull Up | UT, MT, LT, SA | %MVIC |
| Sandhu (2008) [24] | 35 asymptomatic males | 20–30 | Half Push Up, Unstable Push Up (ball), Wall Press, Unstable Knee Push Up (ball) | UT, SA | %MVIC |
| Santos (2018) [41] | 18 asymptomatic males | 18–28 | Push up, One Hand Push Up | UT, MT, LT, SA | %MVIC |
| Seo (2013) [30] | 10 asymptomatic males | 24.6 | Half Push Up Plus, Unstable Push Up Plus (ball), Half Knee Push Up Plus, Unstable Knee Push Up Plus (ball) | UT, MT, LT, SA | %MVIC |
| Tucker (2010) [26] | 13 asymptomatic females 13 asymptomatic males | 22–39 | Push Up, Unstable Push Up (bosu), Unstable Plank (cuff link) | UT, MT, LT, SA | %MVIC |
| Vega (2016) [36] | 20 asymptomatic females 10 asymptomatic males | 23.5 (3.6) | Wall Press, Scap Protraction | UT, MT, LT, SA | %MVIC |
| Youdas (2016) [37] | 13 asymptomatic females 13 asymptomatic males | 24.5 (4.4) 23.4 (0.8) | Supine Pull Up | UT, MT, LT | %MVIC |
| Youdas (2018) [46] | 13 asymptomatic males y 13 asymptomatic females | 24.2 (3.6) | Supine Pull Up, Unstable Pull Up (bosu) | UT, MT, LT, SA | %MVIC Ratio |
SD, standard deviation; SA, serratus anterior; LT, lower trapezius; MT, middle trapezius; UT, upper trapezius; MVIC, maximum voluntary isometric contraction.
2.3Inclusion and exclusion criteria
Articles were included in the systematic review if they met the following inclusion criteria: 1) articles in English language; 2) measurement of EMG amplitude of the UT muscle and at least one of the following muscles: MT, LT and SA; 3) normalization of the electromyographic amplitude as %MVIC; 4) asymptomatic participants; and 5) articles that include at least one exercise in closed kinetic chain. This concept is understood as the exercise in which the most distal segment of the chain is fixed, causing the movement between the most proximal segments [3]. Articles were excluded from the review if they presented any of the following criteria: 1) languages other than English; 2) participants with shoulder pathology; and 3) studies in which the participants were evaluated only after performing any therapeutic intervention.
2.4Study review process and data extraction
The search was completed independently by two authors (OI and MJ) in each of the databases according to the previously mentioned search strategy. The authors reviewed the titles and abstracts retrieved from all databases and determined whether the studies met the inclusion criteria. Then the entire text was read, and the inclusion and exclusion criteria were rigorously applied to determine whether the study would be included in the review. In case of disagreement, some form of consensus was attempted; if no consensus could be reached, the team sought the opinion of a third reviewer (GMR).
Once the exercises and the EMG data were obtained, if the muscle activation ratio in the studies was not specified, the reviewers performed the calculations manually using the %MVIC of the evaluated muscles. An optimal ratio equal to or less than 0.6 was considered between the %MVIC of the UT and that of other scapular muscles: MT, LT and SA [3, 16]. Both reviewers presented the extracted data in a standardized summary table (Table 1), which included the following elements: author and year of publication, number of participants, age, exercises performed, muscles evaluated, %MVIC, and muscle activation ratios.
2.5Evaluation of quality of the studies
The adapted Newcastle-Ottawa Scale (NOS) was used to evaluate the methodological quality of the cross-sectional studies [21]. The adapted NOS consists of 7 items that include sample selection, comparability, and exposure. Each item is rated with 0 to 2 stars, with 10 stars being the maximum total score. The item comparability evaluates whether the participants in different outcomes groups are comparable based on the study design or analysis and the control of confounding factors. Two stars were awarded when the study presented control of the principal confounding factor (electromyography: location of the electrodes and EMG data processing) and one star when presented any other factor (e.g., description of the exercises, anthropometric measures). It was considered that the studies categorized from 0 to 4 stars have a low methodological quality, from 5 to 7 a moderate quality, and from 8 to 10 stars a high quality. Score disagreements were resolved by consensus, and the finally agreed-upon rating was assigned to each study. The agreement between reviewers for the final classification of the studies was a kappa coefficient of 0.90.
3.Results
3.1Study selection
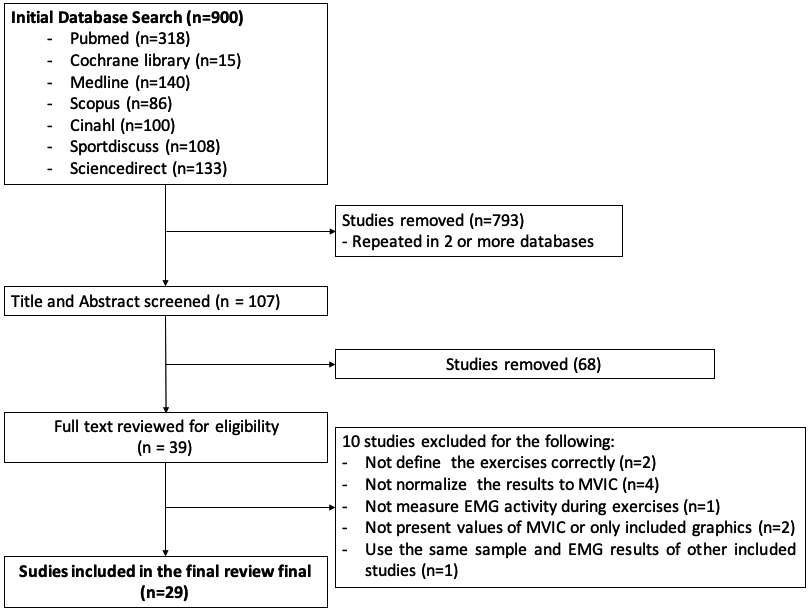
The flowchart detailing the search and selection of studies is presented in Fig. 1. The initial search yielded 900 results. A total of 793 articles were repeated in 2 or more databases. After removing the duplicate articles, the titles and abstracts of 107 articles were reviewed. Thirty-nine articles were selected for the evaluation of eligibility criteria. After the complete reading of these articles, 29 studies were included in the review.
Figure 1.
Flowchart of the search and selection of studies. MVIC, maximus voluntary isometric contraction; EMG, electromyography.
3.2Characteristics of included studies
The 29 articles were considered cross-sectional studies and the muscular electrical activity was evaluated through surface electromyography. A total of 627 healthy participants with an age range of 20 to 31 years was included in the studies. Only data from healthy participants, who had not undergone therapeutic intervention prior to the evaluation, were included. Regarding EMG variables, 20 studies reported only %MVIC [22, 23, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 24, 25, 26, 27, 28, 29, 30, 31], one study reported only muscle activation ratios [42], and eight studies measured both variables [7, 11, 12, 13, 43, 44, 45, 46]. All the investigations evaluated the UT EMG activity, 13 studies measured MT EMG activity [7, 11, 40, 41, 46, 13, 22, 26, 30, 32, 36, 37, 38], and 21 measured the LT EMG activity [7, 11, 29, 30, 32, 36, 37, 38, 39, 40, 41, 44, 12, 46, 13, 22, 23, 25, 26, 27, 28]. Almost all studies measured the EMG activity of SA, except one [37]. The characteristics of each study are summarized in Table 1.
3.3Summary of activation ratios and exercises
The exercises analyzed in the articles were the Push Up, Scap Protraction, Pull Up, Press Up, and Plank and Wall Press, with different variations of each one. Fourteen studies evaluated the Push Up exercise and its variations [7, 11, 32, 41, 42, 45, 12, 24, 25, 26, 28, 29, 30, 31], nine studies evaluated the Scap Protraction exercise and its variations [7, 13, 25, 27, 33, 34, 36, 43, 44], five studies evaluated the Pull Up and its variations [7, 37, 38, 40, 46], two studies evaluated the Press Up [13, 22], four studies evaluated the Plank and its variations [23, 26, 35, 39], and three studies evaluated the Wall Press and its variations [24, 36, 43]. Fourteen studies used unstable surfaces as an exercise variation (e.g. therapeutic ball, bosu, string, etc.), and the therapeutic ball was the variation most used [7, 12, 33, 39, 43, 46, 24, 25, 26, 27, 28, 29, 30, 31]. Figures 2 and 3 show the main exercises with their respective variants and the Table 2 shows the muscle activation ratios UT/MT, UT/LT, and UT/SA according to each author.
Table 2
Exercises in closed kinematic chain and muscle activation ratios
| UT/MT | UT/LT | UT/SA | ||||
| Ratio | Ratio | Ratio | Ratio | Ratio | Ratio | |
| 1.1 Push Up. | ||||||
| Calatayud (2014) [31] | – | – | – | – | 0.22 | – |
| Gioftsos (2016) [12] | – | – | – | 6.40 | 0.48 | – |
| Park (2013) [28] | – | – | – | 0.65 | – | 0.74 |
| Park (2013) [29] | – | – | – | 0.69 | – | 0.80 |
| Tucker (2010) [26] | – | 2.484 | – | 1.66 | – | 0.80 |
| Santos (2018) [41] | 0.538 | – | 0.340 | – | 0.07 | – |
| 1.2 Half Push Up. The participant performed a Push Up with a trunk inclination of 45 | ||||||
| height). | ||||||
| De Mey (2014) [7] | – | 0.73 | 0.48 | – | 0.21 | – |
| Lehman (2008) [25] | – | – | 0.50 | – | 0.21 | – |
| Sandhu (2008) [24] | – | – | – | – | – | 1.47 |
| 1.3 Resisted Push Up. The participants performed a Push Up with an elastic band around the shoulders. | ||||||
| Calatayud (2014) [31] | – | – | – | – | 0.29 | – |
| 1.4 Unstable Push Up. The participants performed a Push Up grasping an elastic sling (suspended) or with the hands on a balance board, | ||||||
| ball, or bosu. | ||||||
| Calatayud (2014) [31] (suspended) | – | – | – | – | – | 0.68 |
| Gioftsos (2016) [12] (balance board) | – | – | – | 5.4 | 0.59 | – |
| Park (2013) [28] (balance board) | – | – | – | 0.72 | – | 0.84 |
| Park (2013) [29] (balance board) | – | – | – | 0.69 | – | 0.90 |
| Sandhu (2008) [24] (ball) | – | – | – | – | – | 1.72 |
| Tucker (2010) [26] (bosu) | – | 3.16 | – | 2.24 | – | 1.28 |
| 1.5 Unstable Half Push Up. The participants performed a Push Up with a trunk inclination of 45 | ||||||
| (suspended) or with the hands on a therapeutic ball. | ||||||
| De Mey (2014) [7] (suspended) | – | 1.11 | – | 0.96 | 0.52 | – |
| Lehman (2008) [25] (ball) | – | – | – | 1.11 | 0.53 | – |
| 1.6 Knee Push Up. The participants performed a Push Up supporting on the knees. | ||||||
| De Mey (2014) [7] | – | 0.77 | – | 0.82 | 0.28 | – |
| Huang (2013) [42] | – | – | – | – | 0.45 | – |
| 1.7 Half Knee Push Up. The participant performed a Knee Push Up with a trunk inclination of 45 | ||||||
| 30 cm of height). | ||||||
| Sandhu (2008) [24] | – | – | – | – | – | 2.61 |
| 1.8 Unstable Knee Push Up. The participants performed a Knee Push Up grasping an elastic sling (suspended) or with the hands on a | ||||||
| therapeutic ball. | ||||||
| De Mey (2014) [7] (suspended) | – | 0.98 | – | 0.73 | 0.44 | – |
| Sandhu (2008) [24] (ball) | – | – | – | – | – | 3.80 |
| 1.9 One Hand Push Up. The participants performed a Push Up supporting only one arm on the floor. | ||||||
| Santos (2018) [41] | 0.59 | – | 0.38 | – | 0.12 | – |
| 2.1 Push Up Plus. | ||||||
| Batbayar (2015) [11] | – | 1.62 | – | 2.37 | 0.09 | – |
| Gioftsos (2016) [12] | – | – | – | 7.20 | 0.36 | – |
| Hwang (2017) [45] | – | – | – | – | 0.17 | – |
| 2.2 Half Push Up Plus. The participants performed a Push Up Plus with a trunk inclination of 45 | ||||||
| 30 cm of height). | ||||||
| Seo (2013) [30] | – | 1.03 | – | 1.17 | – | 0.98 |
| 2.3 Unstable Push Up Plus. The participants performed a Push Up Plus with the hands on a balance board, therapeutic ball, or bosu. | ||||||
| Gioftsos (2016) [12] (balance board) | – | – | – | 6.40 | 0.43 | – |
| Seo (2013) [30] (ball) | – | 0.97 | – | 1.68 | – | 1.25 |
| 2.4 Knee Push Up Plus. The participants performed a Push Up Plus supporting on the knees. | ||||||
| Cools (2014) [32] | – | 1.12 | – | 1.35 | 0.31 | – |
| 2.5 Half Knee Push Up Plus. The participant performed a Knee Push Up Plus with a trunk inclination of 45 | ||||||
| (box of 30 cm). | ||||||
| Seo (2013) [30] | 0.57 | – | – | 1.18 | – | 0.96 |
| 2.6 Unstable Knee Push Up Plus. The participants performed a Knee Push Up Plus with the hands on a Pilates ball. | ||||||
| Seo (2013) [30] (ball) | – | 0.63 | – | 1.51 | – | 0.80 |
| 3.1 Scap Protraction. | ||||||
| Andersen (2012) [13] | – | 1.01 | – | 0.76 | 0.34 | – |
| De Mey (2014) [7] | – | 0.85 | – | 0.72 | 0.33 | – |
| Lee (2013) | – | – | – | 4.27 | 0.40 | – |
|
Table 2, continued | ||||||
| UT/MT | UT/LT | UT/SA | ||||
| Ratio | Ratio | Ratio | Ratio | Ratio | Ratio | |
| Lehman (2008) [25] | – | – | 0.40 | – | 0.11 | – |
| Park (2013) [44] | – | – | – | – | 0.06 | – |
| Park (2015) [34] | – | – | – | – | 0.11 | – |
| Vega (2016) [36] | – | 1.41 | – | 1.50 | 0.54 | – |
| 3.2 Unstable Scap Protraction. The participant performed a Scap Protraction grasping an elastic sling (suspended) or on an exercise ball. | ||||||
| De Mey (2014) [7] (suspended) | – | 1.01 | – | 0.66 | – | 0.64 |
| Lee (2013) [27] (suspended) | – | – | – | 3.42 | 0.45 | – |
| Lee (2014) [33] (suspended) | – | – | – | – | 0.10 | – |
| Lehman (2008) [25] (ball) | – | – | – | 0.97 | 0.17 | – |
| 3.3 One Hand Scap Protraction. The participant performed a Scap Protraction supporting only one arm on the floor. | ||||||
| Martins (2008) [43] | – | – | – | – | 0.39 | – |
| 3.4 Unstable One Hand Scap Protraction. The participant performed a Scap Protraction supporting one arm on the floor. | ||||||
| Martins (2008) [43] | – | – | – | – | 0.32 | – |
| 4.1 Press Up. | ||||||
| McCabe (2007) [22] | – | 0.84 | 0.48 | – | – | 0.61 |
| Andersen (2012) [13] | – | 0.85 | 0.34 | – | 0.42 | – |
| 5.1 Supine Pull Up. | ||||||
| De Mey (2014) [7] | – | 0.65 | – | 0.64 | – | 2.48 |
| Youdas (2016) [37] | – | 1.49 | – | 0.83 | – | – |
| Youdas (2018) [46] | – | 1.00 | – | 2.20 | – | 1.10 |
| 5.2 Resisted Supine Pull Up. The participant performed a Supine Pull Up by wearing a backpack of 10% body mass. | ||||||
| Youdas (2018) [46] | – | 0.93 | – | 1.9 | – | 4.5 |
| 5.3 Half Pull Up. The participant performed a Pull Up from supine plank position, with a trunk inclination of 45 | ||||||
| leaning back with only heels touching the ground. | ||||||
| Borms (2017) [38] | 0.52 | – | 0.58 | – | 0.49 | – |
| 5.4 Isometric Pull Up. From standing position, the participant performed a pull up with both hands on the wall at climbing position | ||||||
| (shoulder at 90 | ||||||
| Puhringer (2017) [40] | 0.15 | – | 0.08 | – | 0.27 | – |
| 5.5 Unstable Supine Pull Up. The participant performed a pull up grasping an elastic sling (suspended) or supporting heels on a bosu. | ||||||
| De Mey (2014) [7] (suspended) | – | 0.77 | – | 0.80 | – | 1.76 |
| Youdas (2018) [46] (bosu) | – | 0.97 | – | 1.90 | – | 4.70 |
| 6.1 Modified Plank. The participant performs a plank with elbows slightly flexed, and with their lower extremities supported on the knees. | ||||||
| Ashnagar (2016) [35] | – | – | – | – | 0.28 | – |
| 6.2 Unstable Plank. The participant performed a plank on an unstable surface. | ||||||
| Oliver (2018) [39] (balance board) | – | – | 0.35 | – | 0.12 | – |
| Tucker (2010) [26] (cuff link) | – | 1.26 | – | 0.88 | 0.15 | – |
| 6.3 One Hand Plank. The participant performed a plank supporting only one hand on the floor. | ||||||
| Oliver (2018) [39] | – | – | 0.48 | – | 0.24 | – |
| Pontillo (2007) [23] | – | – | 0.28 | – | 0.31 | – |
| 7.1 Wall Press. | ||||||
| Martins (2008) [43] | – | – | – | – | – | 0.69 |
| Sandhu (2008) [24] | – | – | – | – | – | 2.14 |
| Vega (2016) [36] | – | 1.68 | – | 1.23 | – | 0.95 |
| 7.2 Unstable One Hand Wall Press. The participant performed the wall press pressing a swiss ball to the wall. | ||||||
| Martins (2008) | – | – | – | – | – | 0.73 |
SA, serratus anterior; LT, lower trapezius; MT, middle trapezius; UT, upper trapezius; MVIC, maximum voluntary isometric contraction.
Figure 2.
Description of Push Up, Push Up Plus, and its variants. For the detailed description of each exercise, see “Summary of Activation Ratios and Exercises” in the “Evidence Synthesis” section. (1.1) Push Up; (1.2) Half Push Up; (1.3) Resisted Push Up; (1.4) Unstable Push Up; (1.5) Unstable Half Push Up; (1.6) Knee Push Up; (1.7) Half Knee Push Up; (1.8) Unstable Knee Push Up; (1.9) One Hand Push Up; (2.1) Push Up Plus; (2.2) Half Push Up Plus; (2.3) Unstable Push Up Plus; (2.4) Knee Push Up Plus; (2.5) Half Knee Push Up Plus; (2.6) Unstable Knee Push Up Plus.
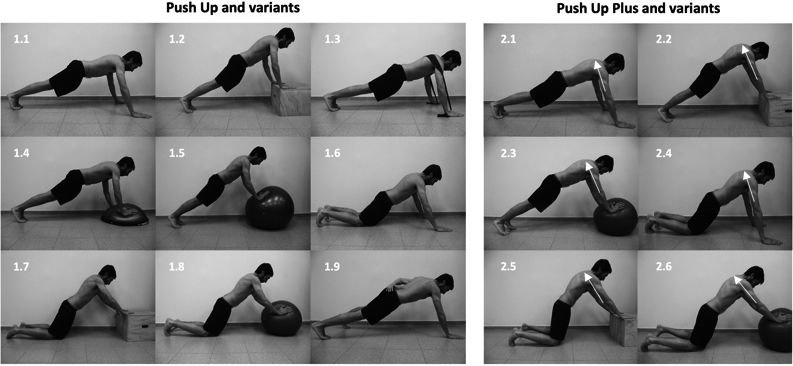
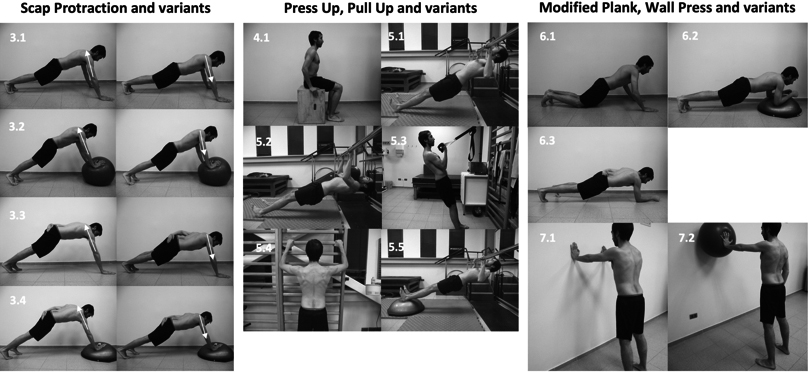
Figure 3.
Description of Scap Protraction, Press Up, Pull Up, Modified Plank, Wall Press, and its variants. For the detailed description of each exercise, see “Summary of Activation Ratios and Exercises” in the “Evidence Synthesis” section. (3.1) Scap Protraction; (3.2) Unstable Scap Protraction; (3.3) One Hand Scap Protraction; (3.4) Unstable One Hand Scap Protraction; (4.1) Press Up; (5.1) Supine Pull Up; (5.2) Resisted Supine Pull Up; (5.3) Half Pull Up; (5.4) Isometric Pull Up; (5.5) Unstable Supine Pull Up; (6.1) Modified Plank; (6.2) Unstable Plank; (6.3) One Hand Plank; (7.1) Wall Press; (7.2) Unstable One Hand Wall Press.
For the UT/MT activation ratio, the exercises that obtained the highest number of optimal ratios in the studies were the One Hand Push Up, Half Pull Up, and Isometric Pull Up. For the UT/LT ratio, the exercises were the Half Push Up, Press Up, Half Pull Up, Isometric Pull Up, and One Hand Plank. For the UT/SA ratio, the exercises were the Half Push Up, Resisted Push Up, Unstable Half Push Up, Knee Push Up, One Hand Push Up, Push Up Plus, Knee Push Up Plus, Scap Protraction, Unstable Scap Protraction, One Hand Scap Protraction, Unstable One Hand Scap Protraction, Half Pull Up, Isometric Pull Up, Modified Plank, Unstable Plank, and One Hand Plank (Table 2).
3.3.1Push Up
The starting position is prone, shoulder at 90
3.3.2Push Up Plus
The starting position is prone, as a Push Up, with the weight distributed over the hands and feet. Then, the participant performs a Push Up, and at the end of the ascending phase the participant pushes his shoulders forward, maintaining a creeping posture (scapular protraction) [11, 12, 45]. Three studies presented an optimal UT/SA ratio (0.09–0.36) [11, 12, 45]. In contrast, two studies showed a non-optimal UT/LT ratio (2.37–7.20) [11, 12]. The Push Up Plus presented five variations (Half Push Up Plus, Unstable Push Up Plus, Knee Push Up Plus, Half Knee Push Up Plus, and Unstable Knee Push Up Plus) (Table 2). Most of these exercises presented non-optimal UT/MT (0.63–1.62) [30, 32] and UT/LT (1.17–7.20) [12, 30, 32] ratios.
3.3.3Scap protraction
The starting position is prone, as in a Push Up, with the weight distributed over the hands and feet. Then, the participant pushes the shoulders forward, without flexing the elbows, and maintains a creeping posture (scapular protraction) [7, 13, 25, 27, 34, 36, 44]. Seven studies showed an optimal UT/SA ratio (0.06–0-54) [7, 13, 25, 27, 34, 36, 44]. Nevertheless, this exercise presented non-optimal UT/LT (0.72–4.27) [7, 13, 27, 36] and UT/MT (0.85–1.41) [7, 13, 36] ratios in three or more studies. The Scap Protraction showed three variations (Unstable Plus, One Hand Scap Protraction, and Unstable One Hand Scap protraction) (Table 2), which presented an optimal UT/SA ratio (0.10–0.45) [25, 27, 33, 43].
3.3.4Press Up
The participant sits straight, with straight arms and supported palms. He then lifts off the bench and descends in front of the seat, just moving the shoulder girdle [13, 22]. Two studies [13, 22] showed an optimal UT/LT ratio (0.34–0.48), but not so for the UT/MT ratio (0.84–0.85).
Table 3
Newcastle-Ottawa Quality Assessment Scale adapted for cross-sectional studies
| Selection | Comparability | Outcomes | ||||||
| Authors | Represent. of the sample | Sample size | Non- respondents | Ascertainment of the exposure | Control confounding factors | Assessment outcome | Statistical test | Methodological quality score |
| Andersen (2012) [13] | – | – | – | – | ** | – | * | 3 (low) |
| Ashnagar (2016) [35] | – | – | – | – | ** | – | * | 3 (low) |
| Batbayar (2015) [11] | – | – | – | – | ** | – | * | 3 (low) |
| Borms (2017) [38] | – | * | – | – | ** | – | * | 4 (moderate) |
| Calatayud (2014) [31] | – | * | – | – | ** | – | * | 4 (moderate) |
| Cools (2014) [32] | – | * | – | – | ** | – | * | 4 (moderate) |
| De Mey (2014) [7] | – | – | – | – | ** | – | * | 3 (low) |
| Gioftsos (2016) [12] | – | – | – | – | ** | – | * | 3 (low) |
| Huang (2013) [42] | – | – | – | * | ** | – | * | 4 (moderate) |
| Hwang (2017) [45] | – | – | – | * | ** | – | * | 4 (moderate) |
| Lee (2013) [27] | – | – | – | – | ** | – | * | 3 (low) |
| Lee (2014) [33] | – | – | – | * | * | – | * | 3 (low) |
| Lehman (2008) [25] | – | – | – | – | ** | – | * | 3 (low) |
| Martins (2008) [43] | – | – | – | * | ** | – | * | 4 (moderate) |
| McCabe (2007) [22] | – | – | – | – | ** | – | * | 3 (low) |
| Oliver (2017) [39] | – | – | – | – | ** | – | * | 3 (low) |
| Park (2013) [44] | – | – | – | * | ** | – | * | 4 (moderate) |
| Park (2013) [28] | – | – | – | – | ** | – | * | 3 (low) |
| Park (2013) [29] | – | – | – | * | ** | – | * | 4 (moderate) |
| Park (2015) [34] | – | – | – | * | ** | – | * | 4 (moderate) |
| Pontillo (2007) [41] | – | – | – | * | ** | – | * | 4 (moderate) |
| Pühringe (2017) [40] | – | – | – | – | ** | – | * | 3 (low) |
| Sandhu (2008) [24] | – | – | – | – | ** | – | * | 3 (low) |
| Santos (2018) [41] | – | * | – | * | ** | – | * | 5 (moderate) |
| Seo (2013) [30] | – | – | – | * | ** | – | * | 4 (moderate) |
| Tucker (2010) [26] | – | – | – | – | ** | – | * | 3 (low) |
| Vega (2016) [36] | – | – | – | * | ** | – | * | 4 (moderate) |
| Youdas (2016) [37] | – | * | – | * | ** | – | * | 5 (moderate) |
| Youdas (2018) [46] | – | * | – | * | ** | – | ** | 5 (moderate) |
This scale has been adapted from the Newcastle-Ottawa Quality Assessment Scale adapted for cross-sectional studies [21].
3.3.5Pull Up
The starting position is supine on the floor underneath a pull-up device, then reaching vertically and grasping the horizontal bar with the hands in supination and slightly wider than shoulder width. Then the participant pulls towards the bar, maintaining supine position [7, 37, 46]. Three studies showed non-optimal UT/MT (0.65–1.00), UT/LT (0.64–2.20), and UT/SA (1.10–2.48) ratios [7, 37, 46]. Four variants of the Pull Up were included (Resisted Pull Up, Half Pull Up, Isometric Pull Up, and Unstable Pull Up) (Table 2). Of these, the Half Pull Up and the Isometric Pull Up revealed optimal UT/MT (0.15–0.52), UT/LT (0.08–0.58), and UT/SA (0.27–0.49) ratios [38, 40]. Two studies [7, 46] showed non-optimal UT/MT (0.77–0.97), UT/LT (0.8–1.9), and UT/SA (1.76–4.7) ratios for the Unstable Pull Up exercise [7, 46].
3.3.6Plank
The results of the review did not show the standard or classical Plank evaluation, but rather three variations, which are described in Table 2. Despite this, we have decided to describe the standard Plank to facilitate understanding of its variations. The participant isometrically maintains the prone position, with the trunk and lower limbs fully extended, the shoulders flexed at 90
3.3.7Wall press
The participant is in standing position with elbows extended, shoulders flexed at 90
3.4Methodological quality evaluation
The scores of each criterion of the adapted Newcastle-Ottawa Scale for cross-sectional studies are shown in Table 3. The scores obtained from the articles fluctuated between 3 and 5 stars. Fourteen studies presented a low methodological quality (3 stars) [7, 11, 33, 35, 39, 40, 12, 13, 22, 24, 25, 26, 27, 28] and 15 studies were classified as moderate quality [23, 29, 42, 43, 44, 45, 46, 30, 32, 32, 34, 36, 37, 38, 41]. No study provided data related to the representativeness of the sample or information about non-respondents. In addition, six studies performed calculations for the sample size [31, 32, 37, 38, 41, 46]and thirteen obtained a star in the item ascertainment of the exposure due to the application of clinical evaluations or validated tools to select the sample [23, 29, 44, 45, 46, 30, 33, 34, 36, 37, 41, 42, 43]. Only one study did not present control of the principal confounding factor (electromyography: location of the electrodes and EMG data processing) [27]. The rest of the studies specifically described the location of electrodes and EMG processing based on the Surface Electromyography for the Non-Invasive Assessment of Muscles recommendations. All the studies controlled at least one additional confounding factor (e.g., weight, height, body mass index, physical condition, level of fatigue prior to evaluation, randomization of the exercises). In addition, all the studies obtained a star in the results item and in the statistical analysis item. None used blind evaluation to obtain the data.
4.Discussion
The results indicate that Scap Protraction and Push Up Plus exercises showed an optimal UT/SA ratio in most studies [7, 11, 12, 13, 25, 27, 34, 36, 45]. Low-position exercises (seated or prone) such as Press Up, Half Push Up, and One Hand Plank showed an optimal UT/LT ratio in most studies [13, 22, 23, 39], while Half Pull Up and Isometric Pull Up showed an optimal UT/ML ratio in a limited number of studies [38, 40].
4.1Upper trapezius
The exercises that presented UT/SA ratios above 1.0 were Supine Pull Up, Unstable Pull Up, Resisted Pull Up, and Half Knee Push Up. These exercises are characterized by a scapular retraction movement in the supine position, starting from a complete scapular protraction, which favors UT activity above SA activity [46, 47, 48]. Youdas et al. explain that during Pull Up variations the SA mainly contributes to posterior scapular tilt and acts as a force couple of external rotation movement [46]. On the other hand, higher UT/SA ratios during Half Knee Push Up may be due to methodological variations such as shoulder flexion angle at the end of the ascending phase [33, 45]. UT relations with the remaining scapular muscles equal to or less than 0.6 have been identified in the following sections of the study.
4.2Middle trapezius and lower trapezius
Exercises with optimal UT/MT ratios were Half Pull Up and Isometric Pull Up. The “Pull” type exercises include scapular retraction and downward rotation, which favor MT muscle activity with respect to the UT muscle [48]. Exercises with optimal UT/LT ratios were Press Up, Half Push Up, and One Hand Plank. UT/LT ratio was one of the most investigated in the selected studies, possibly due to the stabilizing function of the LT muscle, which controls anterior scapular tilt and maintaining an adequate subacromial space [3, 5]. The exercises previously mentioned are characterized by a scapular retraction, downward rotation, and posterior tilt. These imply a higher activity of three portions of the trapezius muscle, according several authors [3, 6, 48]. In the Half Push Up exercise, the “push” force is performed in a lean trunk position, which demands a lower muscle activity compared to a horizontal position [18]. A higher shoulder elevation angle, as a consequence of trunk inclination, favors the mechanical advantage of the LT muscle, which contracts concentrically to generate a scapular downward rotation and posterior tilt [10]. This in turn favors the SA to generate scapular protraction and upward rotation [33, 45, 49]. On the contrary, the UT muscle does not present a proper muscle fiber alignment above 90
4.3Serratus anterior
Exercises with optimal UT/SA ratios were Half Push Up, Unstable Half Push Up, Knee Push Up, Push Up Plus, Knee Push Up Plus, Scap Protraction, Unstable Scap Protraction, One Hand Scap Protraction, Unstable One Hand Scap Protraction, Unstable Plank, and One Hand Plank. The articles that investigated the conventional Push Up exercise presented controversial results in relation to the UT/SA ratio. Three studies showed a ratio less than 0.6 [12, 31, 41] and three studies greater than 0.6 [26, 29, 44]. UT/SA was the most investigated ratio in the articles included in this systematic review, possibly due to the scapulothoracic stabilizing function of the SA muscle and its contribution to scapular protraction and upward rotation [3, 47]. The Push Up exercise and its variants (“half”, “knee”, and “plus”) showed an optimal SA muscle activity, possibly due to the scapular protraction generated in the “pushing phase” in closed kinetic chain [34, 47] and to an eccentric contraction during the “support” and “descending” phases of the trunk [31, 47]. On the other hand, during a scapular protraction in standing or open kinetic chain position, as Scaption or Shrug exercises, a greater UT muscle activity with respect to SA has been observed [10, 50]. The Knee Push Up and Knee Push Up Plus exercises presented a higher SA muscle activity with respect to UT, representing a lower muscle co-contraction and a ratio lower than 0.6. This is possible due to low UT muscle activity related to a lower shoulder load in the “knee” position [24]. Finally, the Scap Protraction and its variants showed optimal UT/SA ratios. During this exercise, a 90–100
Unstable surfaces were the most used variant in the analyzed exercises, which is frequent during training and rehabilitation processes [25, 30]. In general, muscle activity ratio tends to increase with the use of unstable surfaces [7]. According to the selected studies, higher scapular muscle ratios are due to an increase in UT muscle activity [26]. It is possible to attribute this tendency to muscle co-contraction and increased synergies to maintain center of mass stability in the presence of sudden disturbances in multiple directions [31, 43, 51, 52]. Méndez-Rebolledo et al. measured the effect of sudden perturbation of the arm on the SA recruitment pattern and the three portions of the trapezius muscle in healthy participants, observing an increase in muscle co-contraction [52].
4.4Methodological quality
According to the adapted Newcastle-Ottawa Scale, 14 studies were classified as low methodological quality, while 15 studies were classified as moderate methodological quality (see Table 3). Among the scale items, the lower score was obtained in sample selection, which represents 50% of the total score. Considering the study design included in the present review (cross-sectional with EMG measurement), a convenience sample is often used, which doesn’t add score according to the scale. Besides, few studies reported a sample size calculation or a reliable tool for healthy participants’ selection (e.g., clinical test or validated questionnaire). Regarding the comparability item, all studies except one [33] described the main confounding variable, related to the standardized EMG acquisition procedure and data processing methods (e.g., SENIAM recommendations, filter type description and filter frequencies). It is noteworthy that several studies are based on the Hermens recommendations for electrode positioning, nevertheless this document does not provide recommendations for SA electrode positioning [53]. Finally, all studies included in this review performed an appropriate statistical analysis, though it is not described if a blind evaluation, record linkage or self-report was used.
4.5Limitations
In the included studies there is a considerable variability of exercises, such as speed of execution, duration of concentric and eccentric phases, joint position angles, use of stable or unstable surfaces, and others. This complicates exercise and results comparability. As a recommendation, future studies should consider to evaluate the pectoralis minor activation for a better understanding of scapular muscle activity during therapeutic exercises. The pectoralis minor is an important muscle involved in the scapular protraction movement [47] and has an important role in closed chain protraction exercises. Also, these results only apply to healthy participants and may not be representative of patient with shoulder injuries who are performing rehabilitation exercises. The ability of patients to perform these exercises may also be limited. Some of these exercises may also cause increase in pain in certain patient populations. Finally, the studies included in the present systematic review showed a high variability of exercise nomenclature. For this reason, the present review generated a proposal that attempts be made to unify the nomenclature. This will facilitate the analysis and comparison of the results of various investigations.
5.Conclusions
The present review summarizes closed kinetic chain exercises performed in shoulder rehabilitation, classifying them according to stabilizing muscle activity ratios, and proposing a unified nomenclature for them. The main differences among exercises were related to the participant body position, demanded scapular movement, and support surface type, which determined the difficulty level of each variation. The exercises performed in more demanding conditions, such as higher positions or unstable surfaces, tend to favor the UT activity over the MT, LT and SA. The exercises including scapular retraction showed optimal UT/MT ratios (Half Pull Up and Isometric Pull Up) and UT/LT (Press Up, Half Push Up and One Hand Plank), while those including scapular protraction showed optimal UT/SA ratios (Scap Protraction and variants). It is necessary to consider these factors, especially patients’ individual characteristics, considering that the rehabilitation process include a combination of open and closed chain exercises. While knowing the ratios is valuable, it is likely that most of the exercises will be performed at some point during rehabilitation and not just a single exercise.
Conflict of interest
The research is not financed, and the authors have no conflicts of interest to report.
References
[1] | Terry GC, Chopp TM. Functional anatomy of the shoulder. J Athl Train. (2000) ; 35: (3): 248–55. |
[2] | Michener LA, Sharma S, Cools AM, Timmons MK. Relative scapular muscle activity ratios are altered in subacromial pain syndrome. J Shoulder Elb Surg. (2016) ; 25: (11): 1861–7. |
[3] | Kibler W, Sciascia A, Wilkes T. Scapular dyskinesis and its relation to shoulder injury. J Am Acad Orthop Surg. (2012) ; 20: (6): 364–72. |
[4] | Edwards P, Ebert J, Joss B, Bhabra G, Ackland T, Wang A. Exercise rehabilitation in the non-operative management of rotator cuff tears: A review of the literature. Int J Sports Phys Ther. (2016) ; 11: (2): 279–301. |
[5] | Kibler WB, Ludewig PM, McClure PW, Michener LA, Bak K, Sciascia AD. Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the “scapular summit”. Br J Sports Med. (2013) ; 47: (14): 877–85. |
[6] | Phadke V, Camargo P, Ludewig P. Scapular and rotator cuff muscle activity during arm elevation: a review of…: EBSCOhost. Brazilian J Phys Ther. (2009) ; 13: (1): 1–9. |
[7] | De Mey K, Danneels L, Cagnie B, Borms D, T’Jonck Z, Van Damme E, et al. Shoulder muscle activation levels during four closed kinetic chain exercises with and without Redcord slings. J Strength Cond Res. (2014) ; 28: (6): 1626–35. |
[8] | Karandikar N, Vargas OOO. Kinetic chains: A review of the concept and its clinical applications. PM R. (2011) ; 3: (8): 739–45. |
[9] | Kolber M, Beekhuizen K, Cheng M, Hellman M. Shoulder injuries attributed to resistance training: A brief review. J Strength Cond Res Res. (2010) ; 24: (6): 1696–704. |
[10] | Schory A, Bidinger E, Wolf J, Murray L. Systematic review a systematic review of the exercises that produce optimal muscle ratios of the scapular stabilizers in normal shoulders. Int J Sports Phys Ther. (2016) ; 11: (3): 321–36. |
[11] | Batbayar Y, Uga D, Nakazawa R, Sakamoto M. Effect of various hand position widths on scapular stabilizing muscles during the push-up plus exercise in healthy people. J Phys Ther Sci. (2015) ; 27: (8): 2573–6. |
[12] | Gioftsos G, Arvanitidis M, Tsimouris D, Kanellopoulos A, Paras G, Trigkas P, et al. EMG activity of the serratus anterior and trapezius muscles during the different phases of the push-up plus exercise on different support surfaces and different hand positions. J Phys Ther Sci. (2016) ; 28: (7): 2114–8. |
[13] | Andersen C, Zebis M, Saervoll C, Sundstrup E, Jakobsen M, Sjøgaard G, et al. Scapular muscle activity from selected strengthening exercises performed at low and high intensities. J Strength Cond Res. (2012) ; 26: (9): 2408–16. |
[14] | Ludewig P, Cook T. Alterations in shoulder kinematics and associated muscle activity in people with symptoms of shoulder impingement. Phys Ther. (2000) ; 80: (3): 276–91. |
[15] | Cools A, Witvrouw EE, Declercq GA, Danneels LA, Cambier DC. Scapular muscle recruitment patterns: trapezius muscle latency with and without impingement symptoms. J Orthop Sport Phys Ther. (2003) ; 31: (4): 542–9. |
[16] | Phadke V, Ludewig PM. Study of the scapular muscle latency and deactivation time in people with and without shoulder impingement. J Electromyogr Kinesiol. (2013) ; 23: (2): 469–75. |
[17] | Escamilla R, Yamashiro K, Paulos L, Andrews J. Shoulder muscle activity and function in common shoulder rehabilitation exercises. Sport Med. (2009) ; 39: (8): 663–85. |
[18] | Cricchio M, Frazer C. Scapulothoracic and scapulohumeral exercises: A narrative review of electromyographic studies. J Hand Ther. (2011) ; 24: (4): 322–34. |
[19] | Kinsella R, Pizzari T. Electromyographic activity of the shoulder muscles during rehabilitation exercises in subjects with and without subacromial pain syndrome: A systematic review. Shoulder Elb. (2016) ; 9: (2): 112–26. |
[20] | Moher D, Liberati A, Tetzlaff J, Altman DG. Academia and clinic annals of internal medicine preferred reporting items for systematic reviews and meta-analyses: Ann Intern Med. (2009) ; 151: (4): 264–9. |
[21] | Modesti P, Reboldi G, Cappuccio F, Agyemang C, Remuzzi G, Rapi S, et al. Panethnic differences in blood pressure in europe: A systematic review and meta-analysis. PLoS One. (2016) ; 11: (1): e0147601. |
[22] | McCabe RA, Orishimo KF, McHugh MP, Nicholas SJ. Surface electromygraphic analysis of the lower trapezius muscle during exercises performed below ninety degrees of shoulder elevation in healthy subjects. N Am J Sports Phys Ther. (2007) ; 2: (1): 34–43. |
[23] | Pontillo M, Karl Orishimo DF, Ian Kremenic MJ, Malachy McHugh MeP, Mullaney MJ, Timothy Tyler D. Shoulder musculature activity and stabilization during upper extremity weight-bearing activities. North Am J Sport Phys Ther. (2007) ; 2: (2): 90–6. |
[24] | Sandhu J, Mahajan S, Shenoy S. An electromyographic analysis of shoulder muscle activation during push-up variations on stable and labile surfaces. Int J Shoulder Surg. (2008) ; 2: (2): 30. |
[25] | Lehman GJ, Gilas D, Patel U. An unstable support surface does not increase scapulothoracic stabilizing muscle activity during push up and push up plus exercises. Man Ther. (2008) ; 13: (6): 500–6. |
[26] | Tucker WS, Armstrong CW, Gribble PA, Timmons MK, Yeasting RA. Scapular muscle activity in overhead athletes with symptoms of secondary shoulder impingement during closed chain exercises. Arch Phys Med Rehabil. (2010) ; 91: (4): 550–6. |
[27] | Lee S, Lee D, Park J. The effect of hand position changes on electromyographic activity of shoulder stabilizers during push-up plus exercise on stable and unstable surfaces. J Phys Ther Sci. (2013) ; 25: (8): 981–4. |
[28] | Park S, Yoo W. Effects of push-up exercise phase and surface stability on activation of the scapulothoracic musculature. Int J Athl Ther Train. (2013) ; 18: (4): 34–8. |
[29] | Park S, Yoo W, Kwon H, Kim D, Lee S, Park M. Scapulothoracic muscle activation on stable and unstable support surfaces. Int J Athl Ther Train. (2013) ; 18: (1): 25–9. |
[30] | Seo S, Jeon I, Cho Y, Lee H, Hwang Y, Jang J. Surface EMG during the push-up plus exercise on a stable support or swiss ball: Scapular stabilizer muscle exercise. J Phys Ther Sci. (2013) ; 25: (7): 833–7. |
[31] | Calatayud J, Borreani S, Colado JC, Martin F, Rogers ME. Muscle activity levels in upper-body push exercises with different loads and stability conditions. Phys Sportsmed. (2014) ; 42: (4): 106–18. |
[32] | Cools A, Borms D, Cottens S, Himpe M, Meersdom S, Cagnie B. Rehabilitation exercises for athletes with biceps disorders and SLAP lesions: A continuum of exercises with increasing loads on the biceps. Am J Sports Med. (2014) ; 42: (6): 1315–22. |
[33] | Lee S, Lee D, Park J. Effect of the shoulder flexion angle in the sagittal plane on the muscle activities of the upper extremities when performing push-up plus exercises on an unstable surface. J Phys Ther Sci. (2014) ; 26: (10): 1589–91. |
[34] | Park SY, Yoo WG. Activation of the serratus anterior and upper trapezius in a population with winged and tipped scapulae during push-up-plus and diagonal shoulder-elevation. J Back Musculoskelet Rehabil. (2015) ; 28: (1): 7–12. |
[35] | Ashnagar Z, Shadmehr A, Hadian M, Talebian S, Jalaei S. The effects of whole body vibration on EMG activity of the upper extremity muscles in static modified push up position. J Back Musculoskelet Rehabil. (2016) ; 29: (3): 557–63. |
[36] | Vega Toro AS, Cools AMJ, de Oliveira AS. Instruction and feedback for conscious contraction of the abdominal muscles increases the scapular muscles activation during shoulder exercises. Man Ther. (2016) ; 25: : 11–8. |
[37] | Youdas JW, Keith JM, Nonn DE, Squires AC, Hollman JH. Activation of spinal stabilizers and shoulder complex muscles during an inverted row using a portable pull-up device and body weight resistance. J Strength Cond Res. (2016) ; 30: (7): 1933–41. |
[38] | Borms D, Ackerman I, Smets P, Van Den Berge G, Cools AM. Biceps disorder rehabilitation for the athlete. Am J Sports Med. (2017) ; 45: (3): 642–50. |
[39] | Oliver G, Washington J, Barfield J, Gascon S, Gilmer G. Quantitative analysis of proximal and distal kinetic chain musculature during dynamic exercises. J Strength Cond Res. (2018) ; 32: (6): 1545–53. |
[40] | Pühringer M, Strutzenberger G, Leitl D, Holzner K, Schwameder H. Possibilities of altering arm and shoulder muscle activation in a static therapeutic climbing exercise through arm position, hand support and wall inclination. Eur J Sport Sci. (2017) ; 17: (9): 1212–9. |
[41] | Santos MR, Cavalcante BR, Ferreira FLS, Nascimento VYS, Oliveira VMA, Souza FT, et al. Effects of Conscious Abdominal Contraction on Periscapular Muscle Activity. (2018) ; 72: (4): 23–9. |
[42] | Huang H-Y, Lin J-J, Guo YL, Wang WT-J, Chen Y-J. EMG biofeedback effectiveness to alter muscle activity pattern and scapular kinematics in subjects with and without shoulder impingement. J Electromyogr Kinesiol. (2013) ; 23: (1): 267–74. |
[43] | Martins J, Tucci H, Andrade R, Araújo R, Bevilaqua-Grossi D, Oliveira A. Electromyographic amplitude ratio of serratus anterior and upper trapezius muscles during modified push-ups and bench press exercises. (2008) ; 22: (2): 477–84. |
[44] | Park S, Yoo W, Kim M, Oh J, An D. Differences in EMG activity during exercises targeting the scapulothoracic region: A preliminary study. Man Ther. (2013) ; 18: (6): 512–8. |
[45] | Hwang U, Kwon O, Weon J, Jeon I, Kim S. Effect of humeral-elevation angle on electromyographic activity in the serratus anterior during the push-up-plus exercise. J Sport Rehabil. (2017) ; 26: (1): 57–64. |
[46] | Youdas JW, Hubble JW, Johnson PG, McCarthy MM, Saenz MM, Hollman JH. Scapular muscle balance and spinal stabilizer recruitment during an inverted row. Physiother Theory Pract. (2018) ; 00: (00): 1–12. |
[47] | Castelein B, Cagnie B, Parlevliet T, Cools A, Candotti CT, Loss JF, et al. Serratus anterior or pectoralis minor: Which muscle has the upper hand during protraction exercises? Man Ther. (2016) ; 13: (2): 158–64. |
[48] | Contemori S, Panichi R, Biscarini A. Effects of scapular retraction/protraction position and scapular elevation on shoulder girdle muscle activity during glenohumeral abduction. Hum Mov Sci. (2019) ; 64: (December 2018): 55–66. |
[49] | McClure, Tate, Kareha, Irwin, Zlupko. A clinical method for identifying scapular dyskinesis, part 1: Reliability. J Athl Train. (2009) ; 44: (2): 160–4. |
[50] | Oliveira VMA, da Batista LSP, Pirauá ALT, Pitangui ACR, De Araújo R. Electromyographic activity and scapular. Brazilian J Kinanthropometry Hum Perform. (2013) ; (April). |
[51] | Cools A, Witvrouw E, De Clercq G, Danneels L, Willems T, Cambier D, et al. Scapular muscle recruitment pattern: Electromyographic response of the trapezius muscle to sudden shoulder movement before and after a fatiguing exercise. J Orthop Sport Phys Ther. (2002) ; 32: (5): 221–9. |
[52] | Mendez-Rebolledo, Gatica-Rojas, Martinez-Valdes, Xie. The recruitment order of scapular muscles depends on the characteristics of the postural task. J Electromyogr Kinesiol. (2016) ; 31: : 40–7. |
[53] | Hermens HJ, Freriks B, Disselhorst-Klug C, Rau G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol. (2000) ; 10: (5): 361–74. |
Appendices
Appendix
List of combination of keywords and Boolean operators that were used to retrieve the studies.
PubMed and Cochrane Library
Filters PubMed: clinical trial, humans, english, since 01-01-1995 to 31-12-2018.
Filters Cochrane Library: trial, since 01-01-1995 to 31-12-2018.
1. upper trapezius (Text Word)
2. pectoralis minor (Text Word)
3. 1 OR 2
4. scapular muscles (Text Word)
5. middle trapezius (Text Word)
6. lower trapezius (Text Word)
7. serratus anterior (Text Word)
8. 4 OR 5 OR 6 OR 7
9. muscle activation (Text Word)
10. muscle activity (Text word)
11. recruitment (Text Word)
12. 9 OR 10 OR 11
13. electromyography (MeSH Terms)
14. electromyography (Text Word)
15. emg (Text Word)
16. 13 OR 14 OR 15
17. exercise (MeSH Terms)
18. exercise (Text Word)
19. resistance training (MeSH Terms)
20. rehabilitation (MeSH Terms)
21. 17 OR 18 OR 19 OR 20
22. 3 AND 8 AND 12 AND 16 AND 21
Scopus, MEDLINE, SPORTDiscus, and CINAHL
Limit: English, human, article, since 01-01-1995 to 31-12-2018.
1. upper trapezius
2. scapular muscles OR middle trapezius OR lower trapezius OR serratus anterior
3. muscle activation OR muscle activity OR recruitment
4. electromyography OR emg
5. exercise OR training OR rehabilitation
6. 1 AND 2 AND 3 AND 4 AND 5
ScienceDirect
Filters: Nursing and health science, since 1995 to 2018.
1. Upper trapezius OR pectoralis minor
2. Scapular muscles OR middle trapezius OR lower trapezius OR serratus anterior
3. Muscle activation OR muscle activity OR recruitment
4. Electromyography OR emg
5. Exercise OR training OR rehabilitation
6. 1 AND 2 AND 3 AND 4 AND 5


