Effectiveness of high-intensity laser therapy in the management of patients with knee osteoarthritis: A systematic review and meta-analysis of randomized controlled trials
Abstract
OBJECTIVES:
High-intensity laser therapy (HILT) has recently been used to control pain and symptom improvement in knee osteoarthritis. We performed a systematic review and meta-analysis of randomized controlled trials to assess the effectiveness of HILT in patients with knee osteoarthritis.
METHODS:
We conducted a search of articles in the MEDLINE, EMBASE, Cochrane CENTRAL, and Web of Science databases up to March 2020 for randomized controlled trials investigating HILT intervention, placebo, or active intervention as comparator groups for alleviating pain in knee osteoarthritis. Two independent reviewers evaluated the methodological quality and extracted pain and functional outcomes using a pre-specified form. A meta-analysis was performed using an inverse-variance random effect model. Heterogeneity was assessed using Higgins I
RESULTS:
Six randomized controlled trials (RCTs) were included in this meta-analysis. For VAS pain, 334 patients from four studies showed that HILT significantly decreased pain compared to the control (MD,
CONCLUSION:
The effectiveness of HILT on pain, stiffness, and function in patients with knee osteoarthritis is promising. However, due to the limited number of studies, further randomized controlled trials with large, well-designed samples are needed.
1.Introduction
Knee osteoarthritis is a difficult to cure, yet common disease accompanied by disability in the elderly [1]. The most common symptoms are pain and functional limitations [2]. The main aims of the treatment are symptom improvement and prevention of disease progression.
Treatment methods include medication, physiotherapy, exercise, and surgery. Laser therapy has low adverse reactions and is noninvasive and painless. In particular, low-level laser therapy (LLLT) is a known physical modality in patients with osteoarthritis. However, literature shows that the results of this method may vary. One systematic review showed that LLLT did not significantly improve the pain, stiffness, and function, when compared with a placebo in patients with knee osteoarthritis [3]. However, a significant improvement in the pain, stiffness, and function in LLLT versus placebo was recently reported in an update [4].
High-intensity laser therapy (HILT) has recently been used for pain control. Although it was first applied to destroy tissues, it is now being used to treat joint pain [5, 6]. It can stimulate larger and deeper targets than the LLLT [7]. Due to its higher power than low-level lasers, HILT has a shorter laser emission time and a longer laser emission interval [8]. This new type of HILT has been shown to have a positive effect on pain reduction in various types of musculoskeletal pain, including chronic low back pain, carpal tunnel syndrome, and lateral epicondylitis [9, 10, 11].
A systematic review of the effectiveness of HILT in patients with knee osteoarthritis was conducted until August 2017 [12]; however, a well-designed randomized controlled trial was published in 2018 [13]. In addition, a previous systematic review did not report the pooled estimate of the effectiveness of HILT. Thus, we sought to perform a systematic review and meta-analysis of randomized controlled trials to investigate the effectiveness of HILT on pain in patients with knee osteoarthritis.
2.Methods
2.1Literature search
We searched for articles in the MEDLINE, EMBASE, Cochrane CENTRAL, and Web of Science databases from inception to March 14, 2020. Only HILT-related terms were used and disease-related terms were not included for a higher sensitivity of the search strategy (Supplementary Table 1). In Web of Science, the word ‘pain’ was added to the search. MeSH terms and text words such as “high-intensity laser” and “HILT” were used as part of the search strategy.
2.2Study selection
Two independent reviewers selected the studies. In the scenario of a difference of opinion between the two reviewers, the selection was discussed with a third reviewer. The inclusion criteria were adult patients with knee osteoarthritis, HILT intervention (power 500 mW or more) [14], placebo or active intervention such as LLLT as comparator groups, those who reported pain relief as the primary outcome, randomized controlled trials (RCT) regardless of double-blindness, and peer-reviewed original articles. Studies were excluded if they did not include humans, pain associated with disease, or were reviews or abstracts.
2.3Quality assessment
The risk of bias (ROB) was used for the quality assessment of the RCT study design [15]. We estimated seven criteria including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, incomplete outcome data, selective reporting, and funding source. Low, unclear, and high levels were assessed for each criterion. Two reviewers conducted the quality assessment and another person joined the discussion if there was a difference in opinion.
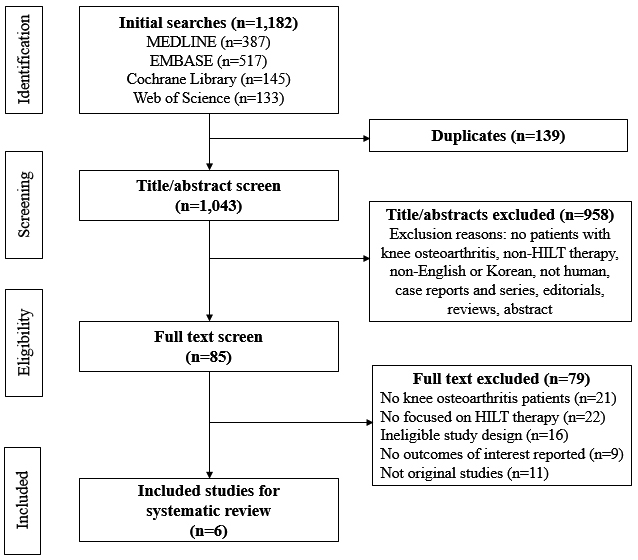
Figure 1.
PRISMA flow diagram of study selections.
2.4Data extraction
Two independent reviewers conducted the data extraction using a pre-specified data extraction form. Data on diagnosis, sample size, interventions, co-interventions, mean age and standard deviation (SD), the percentage of men, Kellgren-Lawrence (K-L) radiological stage [16], evaluation point, country, and outcomes were extracted. The primary outcome of interest was pain and secondary outcomes were stiffness and function using a disease-specific instrument. For the HILT intervention, we collected data on the laser type, wavelength, average output, energy density, J per point, total dose, application time, frequency of treatment, and number of repetitions.
2.5Data analyses
The primary outcome of our study was pain; additionally, knee stiffness and function were secondary outcomes. The pooled estimate was analyzed using an inverse-variance random effect model for continuous variables considering high heterogeneity. Mean difference (MD) for visual analogue scale (VAS) pain was conducted due to the same unit, and standardized mean difference (SMD) was utilized for the measurement of different units. To combine outcomes, we used mean, SD, and the number of patients. If standard error (SE) or
Heterogeneity was assessed visually using a forest plot and Higgins I
3.Results
3.1Literature search
A total of 1,182 articles were identified during the initial search (Fig. 1). After excluding duplicate articles, the title or abstract was screened for 1,043 articles. We reviewed 85 full-text articles and 80 articles were excluded because they did not include patients with knee osteoarthritis or a HILT therapy group, contained ineligible study designs, no interest outcomes reported, or were not original peer-reviewed studies. Finally, six articles were included in this meta- analysis [13, 20, 21, 22, 23, 24].
Table 1
Study characteristics of randomized controlled trials for high-intensity laser therapy in patients with knee osteoarthritis
| Study | Diagnosis | Sample size and intervention | Co- interventions | Mean age (SD) | Male | K-L radiological stage | Evaluation | Country | Outcome measure |
|---|---|---|---|---|---|---|---|---|---|
| Alayat et al. 2017 | Knee osteoarthritis | HILT | NR | 53.85 (4.39) | 100.0% | – Grade I: 15% – Grade II: 39% – Grade III: 46% | – 6 weeks – 3 months | Saudi Arabia | Pain assessment – VAS – WOMAC pain Stiffness/function assessment – WOMAC stiffness – WOMAC function |
| Angelova et al. 2016 | Knee osteoarthritis | HILT 35 PL 37 | NR | HILT 65.11 (1.40), PL 64.71 (1.98) | 31.4% | NR | – 1 week – 1 month – 3 months | Bulgaria | Pain assessment – VAS at rest |
| Gworys et al. 2012 | Knee osteoarthritis | HILT 30 LLLT 34 | NR | HILT 65.4 (9.6), PL 57.6 (11.8) | NR | – 2 weeks | Poland | Pain assessment – VAS – Modified Latinen pain index – Lequesne’s scale | |
| Kheshie et al. 2014 | Knee osteoarthritis | HILT | NR | 54.6 (8.49) | 100.0% | – Grade II: 75% – Grade III: 25% | – 6 weeks | Saudi Arabia | Pain assessment – VAS – WOMAC pain Stiffness/function assessment – WOMAC stiffness – WOMAC function |
| Kim et al. 2009 | Knee osteoarthritis | HILT 14 PL 14 | NSAIDs | HILT 60.6, PL 61.6 | 0% | – Grade II: 100% | – 6 months | South Korea | Pain assessment – VAS – KSCRS pain Stiffness/function assessment – KSCRS stiffness – WOMAC function |
| Nazari et al. 2018 | Knee osteoarthritis | HILT | Acetaminophen (if necessary) | HILT | 45.6% | – Grade II: 60% – Grade III: 40% | – 4 weeks – 12 weeks | Iran | Pain assessment – VAS – WOMAC pain Stiffness/function assessment – WOMAC stiffness – WOMAC function |
K-L: Kellgren and Lawrence, HILT: high-intensity laser therapy, GCS: glucosamine/chondroitin sulfate, Ex: exercise, NR: not reported, VAS: visual analogue scale, WOMAC: Western Ontario and McMaster Universities Osteoarthritis Index, PL: placebo laser, NSAIDs: non-steroidal anti-inflammatory drugs, KRCRS: Knee Society Clinical Rating System, CPT: conventional physical therapy.
Table 2
Study protocols of randomized controlled trials for high-intensity laser therapy in patients with knee osteoarthritis
| Study | Type of laser/ wavelength | Output power/ energy density | Total dose (energy) per session | Application time/no. of total session/ no. of | ||
| sessions | ||||||
| per week | Application sites | Method of application | ||||
| Alayat et al. 2017 | Pulsed Nd:YAG laser/1,064 nm | Very high peak power 3 kW, average power 10.5 W, average energy density 15 J/cm | 3000 J | 7 minutes/ 12/2 | Anterior and posterior knee surface (anteromedial and lateral surfaces, posteromedial and lateral surface) |
|
| Angelova et al. 2016 | Semiconductive neodymium laser IV/1,064 nm | Maximal power 12 W | 3300 J | 12 minutes/ 7/7 | Medial and lateral sides of the knee (intraarticular and periarticular tissues) |
|
| Gworys et al. 2012 | Synchronised two-wave laser emitted by an MLS device and one-wave laser/ 808 nm, 905 mn | HILT 1: power 1100 mW, energy density 6.21 J/cm | HILT 1: 148.8 J | NR/5/2 | Medial and lateral aspect of the knee joint gap, patellofemoral joint on the superior and inferior aspect of the joint, and popliteal fossa | 12 points of knee joint
|
| Kheshie et al. 2014 | Pulsed Nd:YAG laser | NR | 1250 J | 15 minutes/ 12/2 | Anterior, medial, and lateral aspects of the knee joint between tibial and femoral epicondyles |
|
| Kim et al. 2009 | Nd:YAG laser | NR | 3000 J | 6 minutes/ 15/5 | 6 sites of femur and patella | 500 J per 60 seconds for 6 sites
|
| Nazari et al. 2018 | Pulsed mode of E20780 Nd:YAG laser/1,064 nm | Peak power 5 W, energy density 60 J/cm | 2400 J | 8 minutes/ 12/3 | Medial and lateral sides of the knee |
|
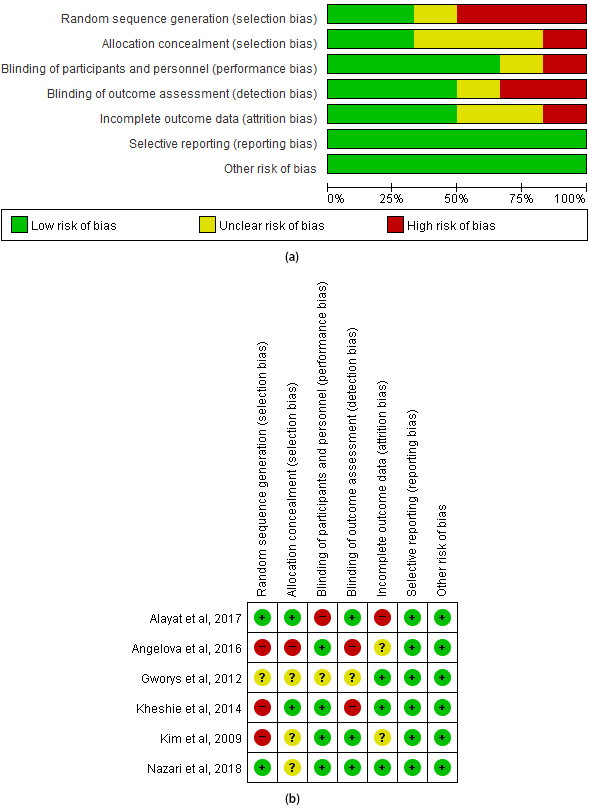
Table 3
Quality assessment of included studies using Risk of Bias Assessment tool for Non-randomized Studies (ROBANS). (a) ROBANS graph, (b) ROBANS summary
3.2General characteristics of the included studies
Table 4
Subgroup analysis of HILT versus control in VAS pain for knee osteoarthritis
| Subgroup | Studies, | Patients, | Random effects, MD [95% CI] | Effect | I | Heterogeneity |
|---|---|---|---|---|---|---|
| Exercise co-intervention | ||||||
| With exercise | 3 | 140 | 0% | 0.38 | ||
| Without exercise | 3 | 194 | 0.003 | 40% | 0.19 | |
| Follow up period | ||||||
| 2 weeks | 1 | 94 | 0.53 | – | – | |
| 4 weeks (1 month) | 2 | 105 | 90% | 0.002 | ||
| 6 weeks | 2 | 107 | 0.08 | 96% | ||
| 12 weeks (3 months) | 3 | 177 | 93% | |||
| 6 months | 1 | 28 | 0.005 | – | – | |
| Comparator | ||||||
| HILT versus active comparator | 3 | 193 | 48% | 0.14 |
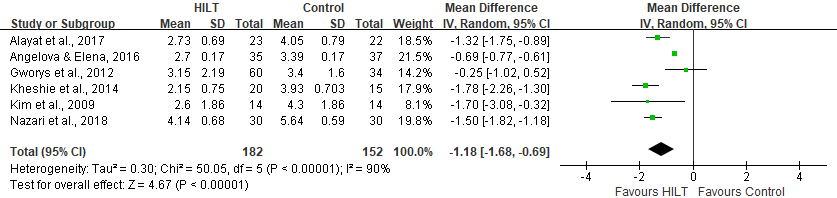
Figure 2.
Mean difference in visual analogue scale (VAS) pain between HILT and control.
The mean age of the study populations ranged from 54 to 65 years (Table 1). Two studies included only men and one study included only women. The percentage of men in the remaining studies ranged from 31.4% to 45.6%. The Kellgren-Lawrence (KL) radiological grade was mostly grades II and III. The countries where the studies were conducted were Saudi Arabia, Bulgaria, South Korea, Iran, and Poland. The final evaluation time points ranged from 2 weeks to 6 months. Pain was assessed using the VAS and/or the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), while stiffness and function were assessed using the WOMAC and the Knee Society Clinical Rating Score (KSCRS). VAS pain with a score ranging from 0 (no pain) to 10 (unbearable pain) was the primary outcome [25]. WOMAC is an arthritis-specific instrument with four levels (none, low, moderate, and severe) and three subscales (pain, stiffness, and physical function) [26, 27]; wherein higher scores indicate higher disability. The Knee Society developed the KSCRS [28], which includes pain, range-of-motion, and function. High scores were 50, 25, and 50, respectively, with high scores indicating severe problems. None of the studies reported adverse events. The modified Latinen pain index (mLPI) includes four dimensions of intensity, frequency, analgesics, and social/professional activities and graded the pain into three groups: slight pain (0–4 points), considerable pain (5–8 points), and severe pain (9–12 points) [29]. Table 2 shows the characteristics of the HILT.
3.3Quality assessment
The ROB results are presented in Fig. 3. Among the included studies, 50% or more studies were estimated to have a low risk for bias regarding the blinding of participants or assessment, selective reporting, and funding source. The method of random sequence generation in four studies was estimated to potentially be at risk for bias. The proportion of low risk for bias in allocation concealment and incomplete outcome data was approximately 30%. The overall quality across studies was fair, despite being vulnerable to selection bias and detection bias of the included studies in this review.
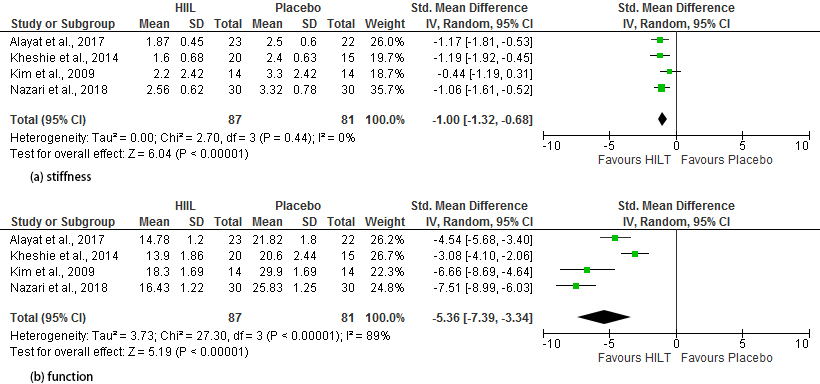
Figure 3.
Mean difference in disease-specific measurement between HILT and control. (a) Stiffness, (b) function.
3.4Clinical outcome: Pain
A total of six studies that evaluated pain using the VAS, including 334 patients, were included in the meta-analysis. We used the combined mean and SD from two HILT groups in Gwory et al.’s study. HILT was observed to significantly decrease the knee pain compared to the control (MD,
No significant difference was observed in the random effect model between the HILT and placebo for disease-specific pain measures such as WOMAC, KSCRS, or mLPI in five studies including 262 patients (SMD,
3.5Clinical outcome: Stiffness
In four studies, 168 patients were included to determine the pooling effectiveness of stiffness using disease-specific measures. The SMD of HILT versus placebo was
3.6Clinical outcome: Function
Four studies, including 87 patients who received HILT and 81 placebos, had pooled results using the disease-specific function. Upon statistical analysis, it was observed that HILT significantly improved function, compared with placebo (SMD,
4.Discussion
Altogether, our meta-analysis showed that knee pain in the HILT group was significantly lower than that in the control group. HILT also significantly positively affected stiffness and function.
These results are in agreement with those from a previous systematic review on LLLT versus placebo in patients with knee osteoarthritis [4, 12]. A systematic review evaluated the effectiveness of HILT and concluded that HILT seemed to be efficient in the alleviation of pain and improved function in knee osteoarthritis. However, the included studies were described narratively and the pooled estimate with meta-analysis was not reported [12]. Rayegani et al. found that VAS pain significantly decreased in the LLLT group (
We observed significant heterogeneity for VAS pain and WOMAC function. Also, Rayegani et al. showed significant heterogeneity for these two factors (I
This study has several strengths. To the best of our knowledge, this is the first systematic review of pooled estimates of HILT in patients with knee osteoarthritis. Although previous systematic reviews have reported on HILT in knee pain and its effectiveness has been reported, the pooled effectiveness of HILT in knee pain has not been estimated [12]. We could identify quantitative estimates using a meta-analysis of HILT versus control in patients with knee osteoarthritis.
We acknowledge that this study has several limitations. First, the sample size of the studies included in the meta-analysis was small. However, this review could use the best available evidence supporting HILT in patients with knee osteoarthritis. Second, we could not compare the different types of laser therapy used for optimal treatment. The laser therapy was diverse according to the included studies. This is due to the fact that standardized therapy has not yet been established. Therefore, further studies are needed to confirm these results. Third, significant heterogeneity was observed in some outcomes. This may be due to the diversity of the study populations, HILT application methods, and co-interventions. Fourth, we only used HILT-related terms in the search strategy. However, the sensitivity of capturing plausible included studies can be heightened.
5.Conclusions
Through this meta-analysis, it is promising that the HILT was effective for pain, stiffness, and function in patients with knee osteoarthritis. The results need to be confirmed with further studies due to the heterogeneity of the data and various laser application methods. Further well-designed randomized control trials with large sample sizes are needed to determine the standardized use of HILT.
Conflict of interest
The authors declare that they have no competing interests.
Abbreviations
| HILT | High-Intensity Level Laser |
| Therapy | |
| CENTRAL | Cochrane Controlled Register of |
| Trials | |
| VAS | Visual Analogue Scale |
| WOMAC | Western Ontario and McMaster |
| Universities Osteoarthritis Index | |
| MD | Mean Difference |
| SMD | Standardized Mean Difference |
| LLLT | Low-Level Laser Therapy |
| RCT | Randomized Controlled Trials |
| ROB | Risk of Bias |
| KSCRS | Knee Society Clinical Rating Score |
| mLPI | modified Laitinen Patin Indicator |
References
[1] | Felson DT, Zhang Y, Hannan MT, Naimark A, Weissman BN, Aliabadi P, et al. The incidence and natural history of knee osteoarthritis in the elderly. The framingham osteoarthritis study. Arthritis Rheum. (1995) ; 38: (10): 1500-5. |
[2] | National Institute of Arthritis and Musculoskeletal and Skin Disease. https://web.archive.org/web/20150518090102/http://www.niams.nih.gov/health_info/Osteoarthritis/default.asp. |
[3] | Huang Z, Chen J, Ma J, Shen B, Pei F, Kraus VB. Effectiveness of low-level laser therapy in patients with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthritis Cartilage. (2015) ; 23: (9): 1437-44. |
[4] | Rayegani SM, Raeissadat SA, Heidari S, Moradi-Joo M. Safety and effectiveness of low-level laser therapy in patients with knee osteoarthritis: A systematic review and meta-analysis. J Lasers Med Sci. (2017) ; 8: (Suppl 1): S12-S19. |
[5] | Viliani C, Martini G, Mangone G, Pasquetti P. High intensive laser therapy in knee osteoarthritis: Comparison between two different pulsed-laser treatment protocol. Energy for Health. (2010) ; 5: : 26-29. |
[6] | Grazio S. Non-pharmacological treatment of musculoskeletal pain. Reumatizam. (2007) ; 54: (2): 37-48. |
[7] | Zati A, Valent A. Physical therapy: New technologies in rehabilitation medicine. (translated to English). Edizioni Minerva Medica. (2006) ; 2006: : 162-85. |
[8] | Kim SH, Kim YH, Lee HR, Choi YE. Short-term effects of high-intensity laser therapy on frozen shoulder: A prospective randomized control study. Man Ther. (2015) ; 20: (6): 751-7. |
[9] | Alayat MS, Atya AM, Ali MM, Shosha TM. Long-term effect of high-intensity laser therapy in the treatment of patients with chronic low back pain: A randomized blinded placebo-controlled trial. Lasers Med Sci. (2014) ; 29: (3): 1065-73. |
[10] | Casale R, Damiani C, Maestri R, Wells CD. Pain and electrophysiological parameters are improved by combined 830–1064 high-intensity LASER in symptomatic carpal tunnel syndrome versus Transcutaneous Electrical Nerve Stimulation. A randomized controlled study. Eur J Phys Rehabil Med. (2013) ; 49: (2): 205-11. |
[11] | Akkurt E, Kucuksen S, Yılmaz H, Parlak S, Sallı A, Karaca G. Long term effects of high intensity laser therapy in lateral epicondylitis patients. Lasers Med Sci. (2016) ; 31: (2): 249-53. |
[12] | Wyszyńska J, Bal-Bocheńska M. Efficacy of high-intensity laser therapy in treating knee osteoarthritis: A first systematic review. Photomed Laser Surg. (2018) ; 36: (7): 343-353. |
[13] | Nazari A, Moezy A, Nejati P, Mazaherinezhad A. Efficacy of high-intensity laser therapy in comparison with conventional physiotherapy and exercise therapy on pain and function of patients with knee osteoarthritis: A randomized controlled trial with 12-week follow up. Lasers Med Sci. (2019) ; 34: (3): 505-516. |
[14] | Painless and non-surgical treatment. High Intensity Laser. https://www.high-intensity-laser.com/subpage. |
[15] | Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions: The Cochrane Collaboration, version 5.1.0. (2011) . https://handbook-5-1.cochrane.org/. |
[16] | Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Ann Rheum Dis. (1957) ; 16: (4): 494-502. |
[17] | Cochrane Training, RevMan Calculator. Finding standard deviations. The Cochrane Collaboration. 2018. http://training.cochrane.org/resource/revman-calculator. |
[18] | Higgins JPT, Green S. (eds). Cochrane handbook for systematic reviews of interventions: The Cochrane Collaboration, version 5.1.0. (2011) . http://handbook.cochrane.org/v5.0.2/. |
[19] | Rücker G, Cates CJ, Schwarzer G. Methods for including information from multi-arm trials in pairwise meta-analysis. Res Synth Methods. (2017) ; 8: (4): 392-403. |
[20] | Alayat MS, Aly TH, Elsayed AE, Fadil AS. Efficacy of pulsed Nd: YAG laser in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers Med Sci. (2017) ; 32: (3): 503-511. |
[21] | Angelova A, Ilieva EM. Effectiveness of high intensity laser therapy for reduction of pain in knee osteoarthritis. Pain Res Manag. (2016) ; 2016: : 9163618. |
[22] | Kheshie AR, Alayat MS, Ali MM. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers Med Sci. (2014) ; 29: (4): 1371-6. |
[23] | Kim JH, Lee S, Kim KS, Yoo CW, Chun TH. Efficacy of high intensity laser therapy in the mild osteoarthritis of the knee: A randomized double-blind controlled trial. J Korean Orthop Res Soc. (2009) ; 12: (2): 53-59. Korean. |
[24] | Gworys K, Gasztych J, Puzder A, Gworys P, Kujawa J. Influence of various laser therapy methods on knee joint pain and function in patients with knee osteoarthritis. Ortop Traumatol Rehabil. (2012) ; 14: (3): 269-77. |
[25] | Revill SI, Robinson JO, Rosen M, Hogg MI. The reliability of a linear analogue for evaluating pain. Anaesthesia. (1976) ; 31: (9): 1191-8. |
[26] | Faik A, Benbouazza K, Amine B, Maaroufi H, Bahiri R, Lazrak N, et al. Translation and validation of Moroccan Western Ontario and McMaster Universities (WOMAC) osteoarthritis index in knee osteoarthritis. Rheumatol Int. (2008) ; 28: (7): 677-83. |
[27] | Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. (1988) ; 15: (12): 1833-40. |
[28] | Insall JN, Dorr LD, Scott RD, Scott WN. Rationale of the Knee Society clinical rating system. Clin Orthop Relat Res. (1989) ; (248): 13-4. |
[29] | Zyznawska J, Mańko G, Kulesa-Mrowiecka M, Brzostek M, Stach DB. The impact of rehabilitation and preventive programmes on the quality of life and pain threshold of patients suffering from lower spinal cord pain. J Pub Health Nursing Med Res. (2013) ; 2: : 30-41. |
[30] | Clijsen R, Brunner A, Barbero M, Clarys P, Taeymans J. Effects of low-level laser therapy on pain in patients with musculoskeletal disorders: A systematic review and meta-analysis. Eur J Phys Rehabil Med. (2017) ; 53: (4): 603-610. |
[31] | Huang Z, Ma J, Chen J, Shen B, Pei F, Kraus VB. The effectiveness of low-level laser therapy for nonspecific chronic low back pain: A systematic review and meta-analysis. Arthritis Res Ther. (2015) ; 17: : 360. |
[32] | Chow RT, Johnson MI, Lopes-Martins RA, Bjordal JM. Efficacy of low-level laser therapy in the management of neck pain: A systematic review and meta-analysis of randomised placebo or active-treatment controlled trials. Lancet. (2009) ; 374: (9705): 1897-90. |
Appendices
Supplementary data
Supplementary Table 1
Strategy for literature search
| Search strategy |
|---|
| MEDLINE |
| 1. HILT.mp. |
| 2. High-intensity laser |
| 3. (high-intensity adj5 laser therap |
| 4. 1 or 2 or 3 |
| EMBASE |
| 1. HILT.mp. |
| 2. High-intensity laser |
| 3. (high-intensity adj5 laser therap |
| 4. 1 or 2 or 3 |
| Cochrane CENTRAL |
| 1. High-intensity laser |
| 2. High-intensity near/5 laser therap |
| 3. HILT |
| 4. #1 or #2 or #3 |
| Web of Science |
| 1. TI |
| 2. TS |
| 3. TS |
| 4. #2 AND #3 |
| 5. #1 OR #4 |
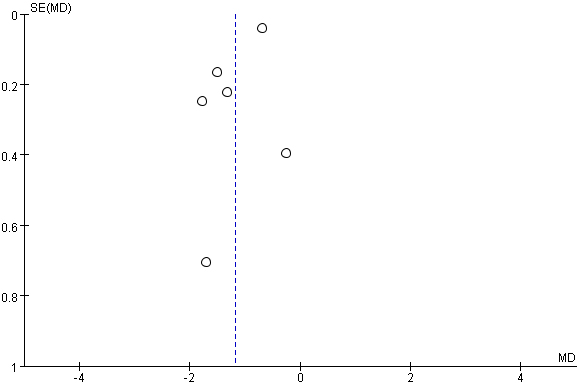
Supplementary Fig. 1.
Funnel plot in visual analogue scale (VAS) pain between HILT and control.