
Intravesical Bacille Calmette-Guerin (BCG) Vaccine Affects Cognition
Abstract
The Montreal Cognitive Assessment (MoCA) is a valuable assessment of the patient’s awareness of time and place. We show that bacille Calmette-Guerin (BCG) significantly affects MoCA testing when administered by the intravesical route. MoCA scores were lower with increasing age and higher in more formally educated individuals. Patients receiving BCG tended to maintain their MoCA scores, whereas almost half the control cases tended to show reduced scores. This benefit is supported by reduced pre-amyloid biomarkers in BCG-injected healthy volunteers and a favorable effect on neuronal dendritic development in animal models. Our results suggest that BCG has a beneficial impact on the cognitive status of older individuals.
INTRODUCTION
Recently, several vaccines have been cited as lowering the risk of developing dementia [1–7]. Our studies and others have shown that intravesical bacille Calmette-Guerin (BCG) is significantly effective in treating non-invasive muscle superficial bladder cancer and correlates with less dementia in treated patients [1, 4]. In our Israeli institutions, as well as in four other independent medical centers, a reduction of dementia and, more specifically, Alzheimer’s disease (AD) has been in the order of 80% to 19% following BCG treatment [1, 2–7]. Here, we have added an early monitor of cognition, the Montreal Cognitive Assessment (MoCA, https://mocacognition.com) [8] questionnaire to our bladder cancer patients to determine if BCG affects cognition. Early recognition of cognitive impairment would be preferable to awaiting diagnosis of full-fledged AD and may improve the success of an intervention.
MATERIALS AND METHODS
The MoCA test consists of 30 points administered to the patient in about ten minutes. The test measures “short-term memory, visuospatial abilities, executive functions, attention, concentration and working memory, language, and orientation to time and place” [8]. Patients attending the urology clinic with a history of bladder cancer were recruited for this prospective evaluation. After signing an informed consent, they filled out the MoCA questionnaire. The testing person was blind to whether the individual had received BCG. Correct answers to 26 questions is considered normal, whereas below 26, the individual is deemed to have mild cognitive impairment (MCI). A total of 134 patients filled out the MoCA questionnaire at least once. Thirty-four patients performed the test twice; four were tested three times, one four times, and one five times. Almost three-quarters of the tests were repeated within 20 months, scheduled as closely as possible to being repeated within a year of the first test. The primary measurement was the change between the first and last MoCA measurements. A one-tailed Fisher’s Exact Test was used to compare changes in the MoCA score of BCG receivers and non-receivers. The local IRB approved the trial.
RESULTS
Population and the effects of age and schooling
The overall bladder cancer patient population gave a distribution of correct responses above 26 of 73%, with 27% in the area of MCI. Males predominated, with 83% (n = 111). The average age of the population was 71.4 years. Fifty-five percent (n = 74) were treated with BCG; of these, 11 (15%) were women, a ratio of 5.7 males to females, close to the national bladder cancer average of four males to each female [9]. The number of women treated with BCG was about half the total (11 of 23 – 47%). There was no difference in age between the patients receiving BCG and the controls (72 versus 71.4 years).
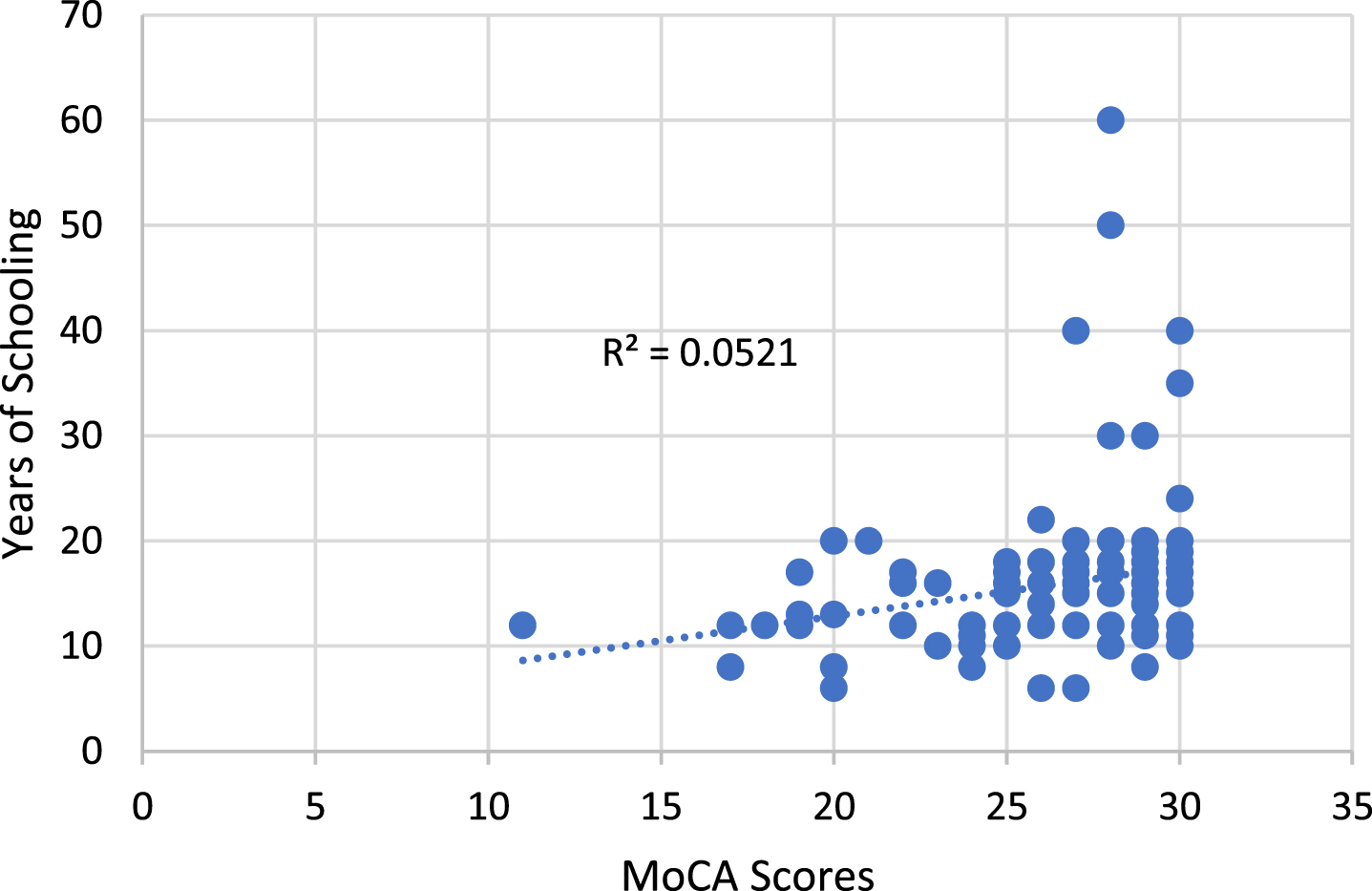
The first MoCA score versus age is plotted in Fig. 1, showing a trend to lower values with increasing age (p = 0.0026; the slope is defined as –0.122 MoCA answer scores per year of age). As illustrated in Fig. 2, years of schooling showed an upward MoCA score trend (p = 0.0099, with a slope of 0.11 per year of education). The very high values of school years were of Yeshiva scholars, who spent most of their lives in traditional Jewish studies.
Fig. 1
Effect of age on MoCA scores.
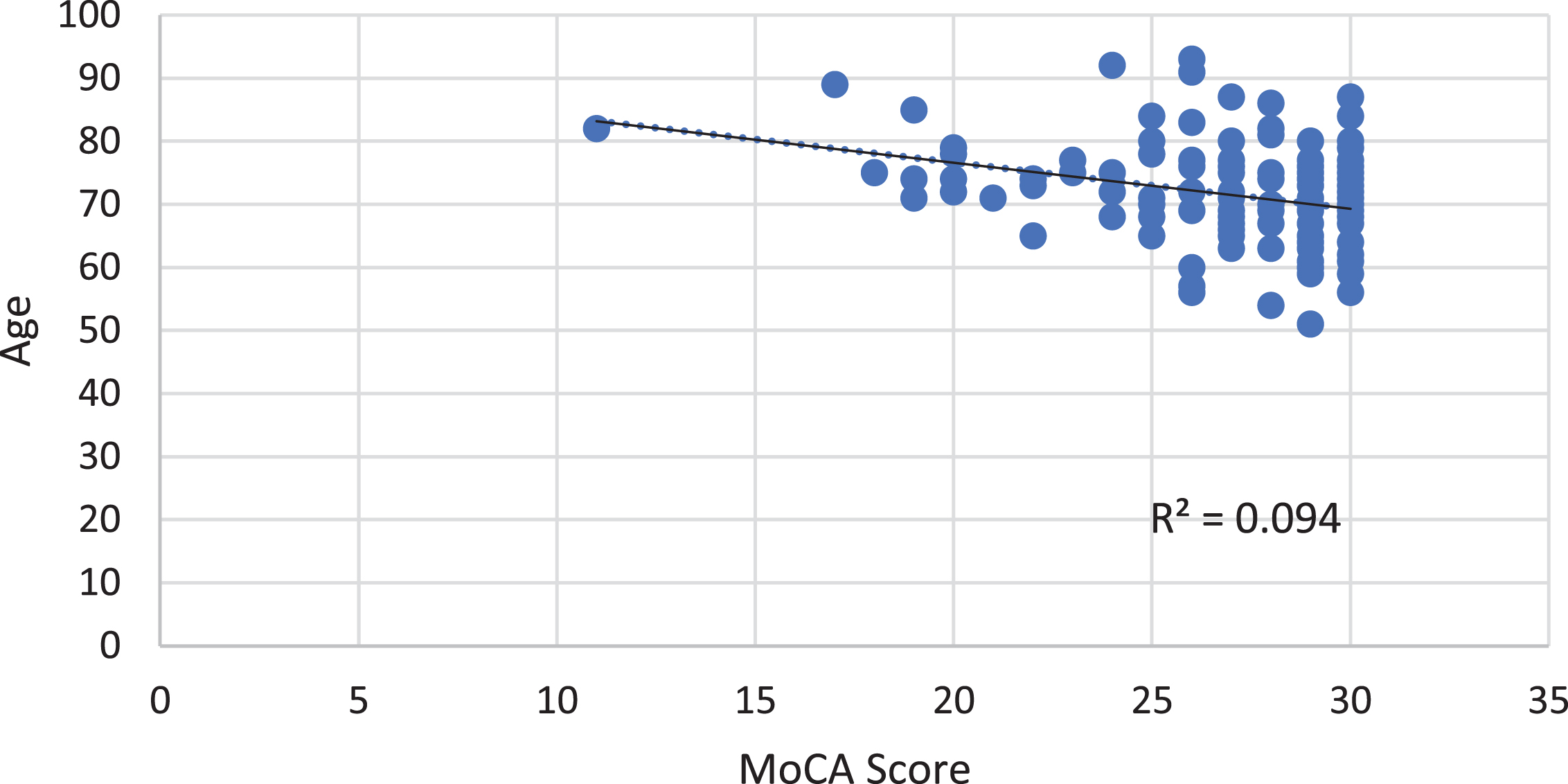
Fig. 2
Effect of schooling years on MoCA scores.
MoCA retesting: the effect of BCG
Of the 34 MoCA-retested individuals, 20 received BCG, and 14 did not (controls). Both groups were predominantly males; those receiving BCG were 18 males and two females, and the controls were 12 males and two females. The average age of the retested individuals was 73 years, slightly above the general average. The average time between the first and second MoCA evaluations in the BCG and control groups was 15 and 20 months, respectively. The percentage of MCI-diagnosed patients did not change upon retesting; in both the first and second tests, it was 25% and 14% respectively. However, more than half of the 34 retested individuals moved upward (1–6 points or more per individual), and one-quarter stayed the same. This increase may have indicated a familiarity with the procedure. Of greater interest was that seven individuals moved downward.
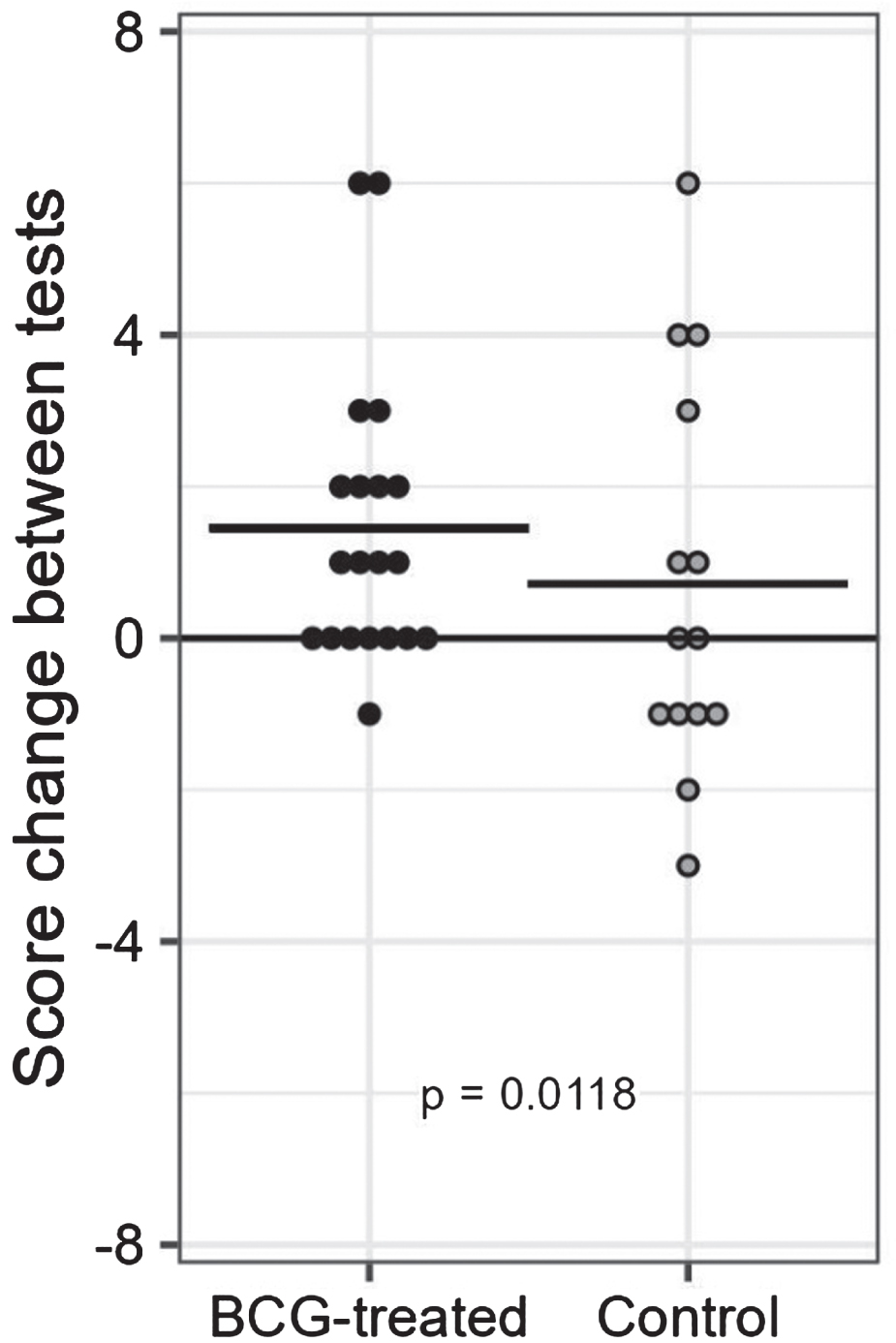
We took advantage of the retesting to determine the effect of BCG on the MoCA score along a timeline. The median score of the first MoCA tests was the same for BCG-treated and control groups (median score 28). Figure 3 presents the change in MoCA scores between the first and the second tests in both groups. One individual immunized with BCG showed a minor decrease; the rest showed either exact repeats (n = 7) or an increased score (n = 12). Notably, six were recorded as lowering their MoCA score among the unvaccinated individuals, and only one in the BCG-treated group. We removed from these considerations two outliers: one in the BCG-treated group, with an increase of 12 points, and one in the controls, with a decrease of 13 points. A one-tailed Fisher’s Exact Test for the two groups’ equal negative results gives a p-value of 0.0118, significant at p < 0.05 but not at p < 0.01. Of the six control individuals whose scores were reduced, the clinical records showed that one was clinically diagnosed with MCI and was being treated.
Fig. 3
Score change between tests in BCG-treated and control patients.
DISCUSSION
Although the number of individuals is small, we believe this study is important for several reasons: 1) urological groups involved in similar research are relying on the dementia endpoint, while the MoCA test may provide insight into an earlier stage in the pathogenesis of AD, 2) several prospective studies applying BCG by injection are underway, with pre-amyloid tests being intermediate, but with AD as an outcome. Results will be years in coming unless changes in early cognition are accounted for, and 3) a pilot study of the robust biomarker of predictive of AD is a mass spectrometry-based plasma amyloid 42/40 ratio [10]. This, combined with age and APOE, can predict brain amyloid status. These parameters are incorporated in an Amyloid Probability Score (APS)—a score that identifies low, intermediate, or high risk of having cerebral amyloid. Results on forty-nine BCG-naïve, immunocompetent individuals nine months after vaccination found reduced risk assessment. Follow-up plasma amyloid testing revealed a reduction in the APS in all the risk groups, especially in the high-risk group of young individuals (p = 0.016). As we do here, the authors argued for skepticism in the “embracement of these results.”
Metabolic studies of BCG support its role in affecting neuronal health. The studies of type 1 diabetes and BCG in activating trained innate immunity have all indicated that the monocyte/macrophage cell line shifts from anaerobic to aerobic glycolysis [11, 12]. Furthermore, it has been suggested that these cells, when passing through the blood-brain barrier, can transfer lactate to glial cells, which, in their cerebral role, can help to maintain neuronal health [12].
4) Three animal studies, with models for AD and Parkinson’s disease [13, 15], have indicated a profound effect of BCG on the brain. Furthermore, one group reported a proliferation of neuronal dendrites [14].
In summary, this study suggests that BCG has a beneficial effect on the cognitive status of bladder cancer patients. In addition, the MoCA test may provide a valuable test for early AD diagnosis.
AUTHOR CONTRIBUTIONS
Charles Leonard Greenblatt, M.D. (Conceptualization; Formal analysis; Investigation; Writing – original draft); Herve Bercovier, D.V.M. (Conceptualization; Formal analysis); Benjamin Y Klein, M.D. (Formal analysis; Writing – review & editing); Ofer N. Gofrit, M.D., Ph.D. (Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Project administration; Validation; Writing – review & editing).
ACKNOWLEDGMENTS
We thank the CureAlz Foundation for its financial support and continuing interest in our research on immunotherapy of Alzheimer’s disease. We thank Dr. Shoshana Frankenburg for carefully reading the manuscript and her suggestions, as well as Shani and Raanan Vaknine for helping with technical editing issues.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article and in the table in its supplementary material.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-240307.
REFERENCES
[1] | Gofrit ON , Klein BY , Cohen IR , Ben-Hur T , Greenblatt CL , Bercovier H ((2019) ) Bacillus Calmette-Guerin (BCG) therapy lowers the incidence of Alzheimer’s disease in bladder cancer patients. PLoS One 14: , e0224433. |
[2] | Kim JI , Zhu D , Barry E , Kovac E , Aboumohamed A , Agalliu I , Sankin A ((2021) ) Intravesical bacillus Calmette-Guerin treatment is inversely associated with the risk of developing Alzheimer disease or other dementia among patients with non-muscle-invasive bladder cancer. Clin Genitourin Cancer 19: , e409–e416. |
[3] | Weinberg MS , Zafar A , Magdamo C , Chung SY , Chou WH , Nayan M , Deodhar M , Frendl DM , Feldman AS , Faustman DL , Arnold SE , Vakulenko-Lagun B , Das S ((2023) ) Association of BCG vaccine treatment with death and dementia in patients with non-muscle-invasive bladder cancer. JAMA Netw Open 6: , e2314336. |
[4] | Klinger D , Hill BL , Barda N , Halperin E , Gofrit ON , Greenblatt CL , Rappoport N , Linial M , Bercovier H ((2021) ) Bladder cancer immunotherapy by BCG is associated with a significantly reduced risk of Alzheimer’s disease and Parkinson’s disease. Vaccines (Basel) 9: , 491. |
[5] | Makrakis D , Holt SK , Bernick C , Grivas P , Gore JL , Wright JL ((2022) ) Intravesical BCG and incidence of Alzheimer disease in patients with bladder cancer: Results from an administrative dataset. Alzheimer Dis Assoc Disord 36: , 307–311. |
[6] | Wu X , Yang H , He S , Xia T , Chen D , Zhou Y , Liu J , Liu M , Sun Z ((2022) ) Adult vaccination as a protective factor for dementia: A meta-analysis and systematic review of population-based observational studies. Front Immunol 13: , 872542. |
[7] | Greenblatt CL , Lathe R ((2024) ) Vaccines and dementia: Part II. Efficacy of BCG and other vaccines against dementia. J Alzheimers Dis 98: , 361–372. |
[8] | MoCA Cognition, https://mocacognition.com |
[9] | Silverman B , Ben Lesan M , Dichtier R , King-Boker L ((2021) ) Cancer of the urinary bladder. Israel Cancer Registry. |
[10] | Dow CT , Greenblatt CL , Chan ED , Dow JF ((2022) ) Evaluation of BCG vaccination and plasma amyloid: A prospective, pilot study with implications for Alzheimer’s disease. Microorganisms 10: , 424. |
[11] | Kuhtreiber WM , Tran L , Kim T , Dybala M , Nguyen B , Plager S , Huang D , Janes S , Defusco A , Baum D , Zheng H , Faustman DL ((2018) ) Long-term reduction in hyperglycemia in advanced type 1 diabetes: The value of induced aerobic glycolysis with BCG vaccinations. NPJ Vaccines 3: , 23. |
[12] | Klein BY , Greenblatt CL , Gofrit ON , Bercovier H ((2022) ) Bacillus Calmette-Guerin in immuno-regulation of Alzheimer’s disease. Front Aging Neurosci 14: , 861956. |
[13] | Zuo Z , Qi F , Yang J , Wang X , Wu Y , Wen Y , Yuan Q , Zou J , Guo K , Yao ZB ((2017) ) Immunization with Bacillus Calmette-Guerin (BCG) alleviates neuroinflammation and cognitive deficits in APP/PS1 mice via the recruitment of inflammation-resolving monocytes to the brain. Neurobiol Dis 101: , 27–39. |
[14] | Li Q , Zhang Y , Zou J , Qi F , Yang J , Yuan Q , Yao Z ((2016) ) Neonatal vaccination with bacille Calmette-Guerin promotes the dendritic development of hippocampal neurons. Hum Vaccin Immunother 12: , 140–149. |
[15] | Yong J , Lacan G , Dang H , Hsieh T , Middleton B , Wasserfall C , Tian J , Melega WP , Kaufman DL ((2011) ) BCG vaccine-induced neuroprotection in a mouse model of Parkinson’s disease. PLoS One 6: , e16610. |


