
Prevalence and Determinants of Diagnosed Dementia: A Registry Linkage Study Linking Diagnosis of Dementia in the Population-Based HUNT Study to Registry Diagnosis of Dementia in Primary Care and Hospitals in Norway
Abstract
Background:
A timely diagnosis of dementia can be beneficial for providing good support, treatment, and care, but the diagnostic rate remains unknown and is probably low.
Objective:
To determine the dementia diagnostic rate and to describe factors associated with diagnosed dementia.
Methods:
This registry linkage study linked information on research-based study diagnoses of all-cause dementia and subtypes of dementias, Alzheimer’s disease, and related dementias, in 1,525 participants from a cross-sectional population-based study (HUNT4 70+) to dementia registry diagnoses in both primary-care and hospital registries. Factors associated with dementia were analyzed with multiple logistic regression.
Results:
Among those with research-based dementia study diagnoses in HUNT4 70+, 35.6% had a dementia registry diagnosis in the health registries. The diagnostic rate in registry diagnoses was 19.8% among home-dwellers and 66.0% among nursing home residents. Of those with a study diagnosis of Alzheimer’s disease, 35.8% (95% confidence interval (CI) 32.6–39.0) had a registry diagnosis; for those with a study diagnosis of vascular dementia, the rate was 25.8% (95% CI 19.2–33.3) and for Lewy body dementias and frontotemporal dementia, the diagnosis rate was 63.0% (95% CI 48.7–75.7) and 60.0% (95% CI 43.3–75.1), respectively. Factors associated with having a registry diagnosis included dementia in the family, not being in the youngest or oldest age group, higher education, more severe cognitive decline, and greater need for help with activities of daily living.
Conclusions:
Undiagnosed dementia is common, as only one-third of those with dementia are diagnosed. Diagnoses appear to be made at a late stage of dementia.
INTRODUCTION
Dementia is a major public health concern which affects both the person with dementia and their family [1]. Due to population aging, the prevalence of dementia will increase considerably in the coming years [1]. A recent study found that dementia already accounts for the highest health spending in Norway, at approximately 32 billion a year and 10% of the total health costs [2], in addition to the informal care which forms a large part of dementia care [3].
If dementia is present, a timely diagnosis and post-diagnostic follow-up can facilitate early interventions, including providing persons with dementia and their next of kin with information about the disease and the opportunity to plan for the future. While the follow-up should include proper help and care, early interventions may also contribute to delaying the need for more advanced health services, such as nursing home placement [4]. A timely diagnosis also benefits the health and social care systems by providing the best opportunity to make an appropriate plan for the entire course of the disease [5]. However, when a person develops dementia, it is unlikely that they will be assessed and diagnosed before some time has passed [6]. Some of the people who come to assessment have potentially treatable conditions [6], and some seek assessment due to concerns about their own cognition without having cognitive impairment [7]. These patients may need both assessment and follow-up but should not receive a dementia diagnosis.
In a review of six studies conducted in high-income countries in 2000–2010 the median proportion of persons with diagnosed dementia was 39%, with a range of 20–50% [8]. The diagnostic rate in studies published after 2010 have not increased much, showing a median proportion of 42% and the even wider range of 15–58% [9–15]. On a global scale the rate of undiagnosed dementia can be as high as 75% [6].
Stigma related to dementia is one likely cause of not seeking cognitive assessment [16]. Little knowledge about dementia and a belief that cognitive decline is a normal part of ageing are other reasons for not seeking assessment [17]. Possible reasons for why health care providers do not diagnose dementia can be a lack of knowledge about dementia, a lack of capacity to establish a timely diagnosis, or a fear of the patient’s reaction towards a diagnosis, like suicidal behavior [18]. A reluctance from family physicians to diagnose dementia can also stem from a lack of access to proper post-diagnostic follow-up [5]. Several studies have found more undiagnosed dementia in the early phase of the illness [9–11, 13, 19]. Furthermore, a systematic review of 23 studies described more undetected dementia in the general community (compared to nursing homes), in people younger than 70 years old, and in men [20]. To our knowledge, no study has looked at dementia in the family and its impact on dementia diagnostic rates.
The objective of this study is to determine the dementia diagnostic rate and to describe factors associated with diagnosed dementia.
MATERIALS AND METHODS
Participants, study design, and assessment
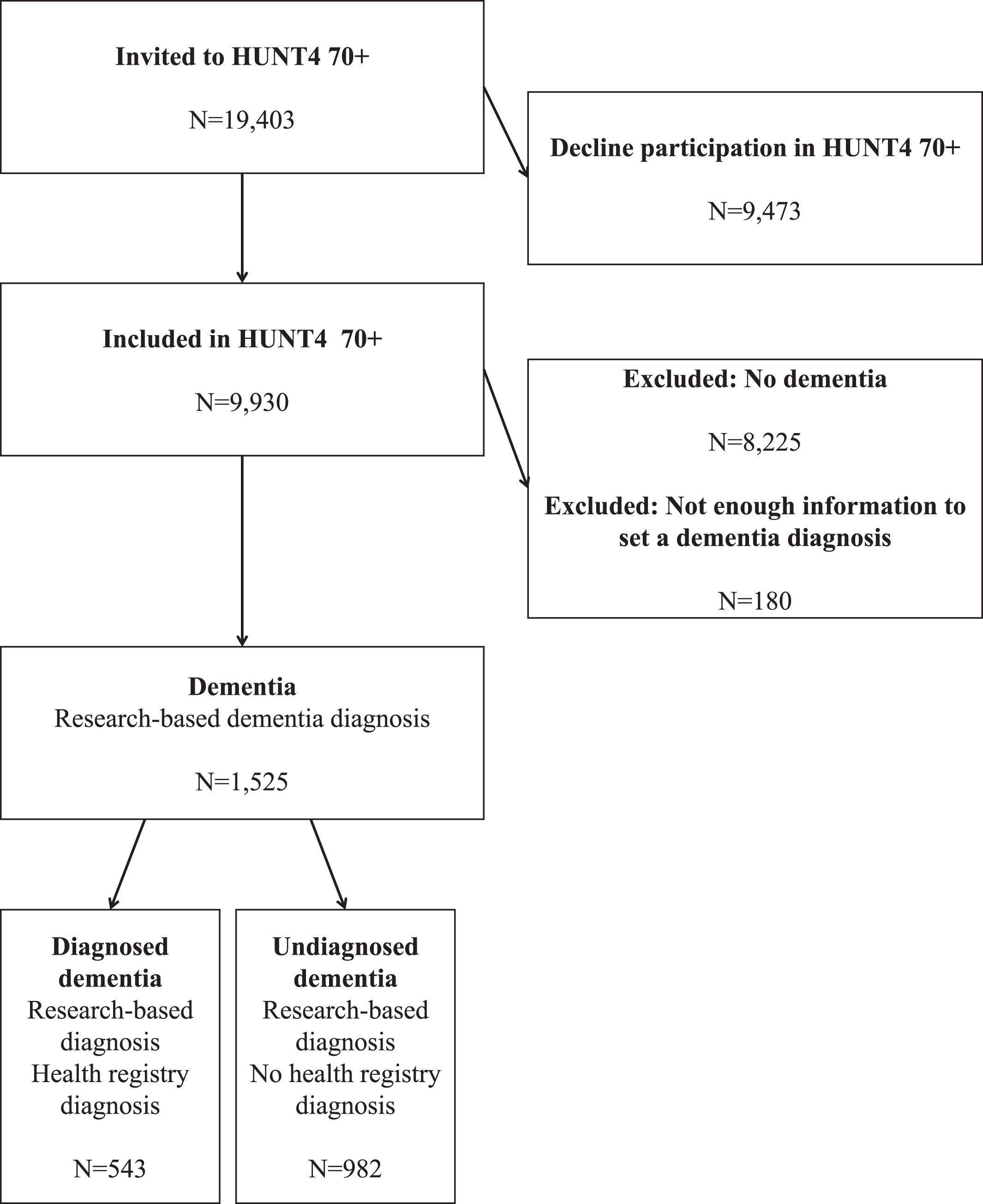
Our sample was recruited from the 9,930 participants in the fourth wave of the population-based Trøndelag Health Study (HUNT), specifically those who were 70 years or older, and who were clinically assessed for dementia (HUNT4 70+, 2017–2019) [21]. A total of 180 cases were excluded due to insufficient information to diagnose dementia, and 8,225 cases were classified with no dementia. This led to a sample comprising 1,525 participants who had received a research-based dementia diagnosis, called study diagnosis. In this registry linkage study, these participants were linked to data in primary care and hospital registries (registry diagnosis) using their personal identification numbers (Fig. 1).
Fig. 1
Flow chart.
Assessments were performed in accordance with the participant’s choice, either at a field station or in the participant’s home. For nursing home participants, the assessment was performed in the nursing home. The cognitive assessment included the Montreal Cognitive Assessment scale (MoCA). For the analyses in this paper, MoCA scores were divided into three groups according to severity: ≥18 for those with mild cognitive impairment (MCI): 10–17 for those with moderate cognitive impairment and: <10 for those with severe cognitive impairment [22, 23]. The assessment included information on subjective cognitive decline, core symptoms, symptom debut, and course of cognitive symptoms. Information on whether they lived with others and on instrumental activities of daily living (I-ADL) was collected through a questionnaire. For I-ADL, the Instrumental Activities of Daily Living Scale, in which the participants answered whether they needed help in nine different I-ADL items (i.e., cooking, light housework, heavy housework, laundry, shopping, paying bills, taking medications, going outdoors, and travel with public transport) was used [24]. Needing help with 0–3 I-ADL items was graded as little need for help, needing help with 4–6 I-ADL items was graded as some need for help, needing help with 7–9 I-ADL items was graded as extensive need for help. In addition, the depression subscale of the Hospital Anxiety and Depression Scale (HADS-D) was used to measure depression, and scores were divided into four groups: 0–7 indicated no depression, 8–10 indicated mild symptoms, 11–14 indicated moderate symptoms, and 15–21 indicated severe symptoms of depression [25, 26]. A caregiver interview was conducted for participants with subjective cognitive decline or scores below a defined threshold on cognitive tests, as well as for all nursing home participants. The home-dwelling participants and the participants’ next of kin were asked if a first-degree and/or a second-degree relative of the participant had dementia. In addition, the care staff in the nursing homes completed the Clinical Dementia Rating (CDR) scale, used to assess stage of dementia [27]. CDR scores range from 0–3, with 0 and 0.5 indicating no or questionable dementia, 1 indicating mild dementia, 2 indicating moderate dementia, and 3 indicating severe dementia. For 46 of the participants from nursing home, the CDR score was below 1; however, since these participants had a dementia study diagnosis, their CDR score was adjusted to 1 in the analysis.
Applying all available information, a team of medical doctors with expertise in old age psychiatry, geriatrics, and neurology diagnosed all participants with study diagnoses according to the DSM-5 criteria for cognitive decline, dementia, and subtypes of dementia [28]. The dementia subtypes included in the study diagnoses were Alzheimer’s disease (AD), vascular dementia (VaD), Lewy body dementias (LBD), frontotemporal dementia (FTD), mixed dementia (defined as major neurocognitive disorder due to multiple etiologies), other specified dementia, and unspecified dementia [28]. The methods of the cognitive assessment in HUNT4 70+ and of the diagnostic process leading to the dementia study diagnoses have been described in detail elsewhere [29].
Participants’ registry-based education level was retrieved from the National Education Database and participants were divided into three groups using the Norwegian standard classification of education (NUS2000), where 0–2 represents elementary, 3–5 secondary, and 6–8 tertiary education [30].
The Norwegian Patient Registry (NPR) is a national administrative health registry; it includes data on the use of specialist health care services and gathers information on the registry diagnoses given to an individual in hospitals, both inpatient and outpatient [31, 32]. In the NPR, the International Classification of Diseases (ICD-10) is used to diagnose MCI, dementia, and dementia subtypes. All ICD-10 codes describing dementia diseases were included, specifically, AD: G30 with all subcodes and F00 with all subcodes; VaD: F01 with all subcodes; LBD: G31.8, F02.3, and F02.8; FTD: G31.0 and F02.0; mixed dementia: G30.8 and F00.2; other specified dementias: G31.2, F02.1, F02.2, and F02.4; and unspecified dementia: F03 and all subcodes [33]. A dementia registry diagnosis was excluded if the consultation consisted of a dementia registry diagnosis combined with one of the codes for MCI (F06.7 or F07.8), e.g., G30 and F07.8, describing AD at an MCI level.
The Control and Payment of Reimbursement to Health Service Providers (KUHR) is part of the Norwegian Registry of Primary Health Care (NRPHC) [34]. KUHR gathers information on an individual’s registry diagnoses provided in primary care, including registry diagnoses from the family physician [31]. The International Classification of Primary Care (ICPC-2) is used by family physicians in their diagnostic work-up, wherein dementia is coded as P70 [35]. In addition, the codes P05 (“Senility, feeling/behaving old”) and P20 (“Memory disturbance”) were added in a sensitivity analysis.
All dementia registry diagnoses in the KUHR and NPR given to participants in the 10 years prior to participation in HUNT4 70+ were retrieved and linked to the study sample. Since some participants might have sought a dementia assessment after participating in HUNT4 70+, only registry diagnoses documented in the registries before the individual’s date of participation were included. In combination, the KUHR and NPR provide information on participants’ dementia registry diagnoses from both primary care and specialist care in hospitals, but they do not gather information about dementia registry diagnoses given in nursing homes.
Statistical analysis
The dementia diagnostic rate was defined as the proportion of people with a dementia registry diagnosis in one or both health registries among those who had a dementia study diagnosis in HUNT4 70 + . To handle missing data, multiple imputations (MI) with chained equations was applied [36]; in total 20 datasets were imputed. Even with a large proportion of missing data, MI can be beneficial to reducing bias [37]. Since a dementia registry diagnosis can be a requirement for admission to a nursing home, we conducted separate analyses for home-dwellers and nursing home residents.
Multiple logistic regression was used to investigate which factors were related to having a dementia registry diagnosis among those with a dementia study diagnosis in HUNT, controlling for covariates. The covariates included in analyses on home-dwellers (with percentage missing in parenthesis) were sex (0), age (0), education (0.2), dementia in the family (5.7), MoCA (0.6), HADS-D (35.1), I-ADL (29.1), and whether they lived with others (17.0). In analyses on nursing home residents, the covariates were sex (0), age (0), education (0.4), dementia in the family (55.6), and CDR (16.1). Significance was set to 5%. Imputed data were used in the main analyses, and complete case data was used in the sensitivity analyses (Supplementary Material). Stata version 18 [38] was used for analyses.
Ethics
The study was approved by the Regional Committee for Medical and Health Research Ethics in Norway (REK South East D 82985) as well as according to the General Data Protection Regulation by the Norwegian Centre for Research Data (NSD 791342). Participation was required informed consent, which was provided after receiving oral and written information about the study. In participants with reduced capacity to consent, their next of kin were informed and gave consent. Participants in HUNT can at any time withdraw their consent for data storage and use in the research; should a participant withdraw their consent, all data about them is then deleted.
RESULTS
Of the 1,525 participants with a dementia study diagnosis, 543 (35.6%) had a dementia registry diagnosis in one or more of the health registries, 393 in NPR, 470 in KUHR and 320 in both NPR and KUHR. The diagnostic rate was 29.9% in men and 39.6% in women. The diagnostic rate increased with age, from 16.9% at 70–74 years to 37.7% at 90+ years. The diagnostic rate among nursing home residents was 66.0%, while among home-dwellers it was 19.8%. The mean MoCA scores in those with a dementia registry diagnosis compared to those without a dementia registry diagnosis were 11.3 (SD 5.5) and 14.6 (SD 4.3), respectively. See Table 1 for descriptive statistics.
Table 1
Sociodemographic and cognitive characteristics
| Total | Undiagnosed | Diagnosed | % diagnosed | |||||
| n = 1,525 | n = 982 | n = 543 | 35.6 | |||||
| All | HD | NH | All | HD | NH | |||
| Sex | ||||||||
| male | 625 | 438 | 374 | 64 | 187 | 74 | 113 | 29.9 |
| female | 900 | 544 | 430 | 114 | 356 | 124 | 232 | 39.6 |
| Age | ||||||||
| 70–74 y | 236 | 196 | 183 | 13 | 40 | 13 | 27 | 16.9 |
| 75–79 y | 275 | 178 | 169 | 9 | 97 | 40 | 57 | 35.3 |
| 80–84 y | 321 | 187 | 166 | 21 | 134 | 56 | 78 | 41.7 |
| 85–89 y | 343 | 203 | 157 | 46 | 140 | 62 | 78 | 40.8 |
| 90+ y | 350 | 218 | 129 | 89 | 132 | 27 | 105 | 37.7 |
| Home-dwellers | 1 002 | 804 | 198 | 19.8 | ||||
| HD living with others | 434 | 364 | 70 | 16.1 | ||||
| Place of participation | ||||||||
| field station | 624 | 544 | 80 | 12.8 | ||||
| home visit | 378 | 260 | 118 | 31.2 | ||||
| nursing home | 523 | 178 | 345 | 66.0 | ||||
| Education | ||||||||
| elementary | 674 | 427 | 334 | 93 | 247 | 86 | 161 | 36.6 |
| secondary | 688 | 461 | 390 | 71 | 227 | 83 | 144 | 33.0 |
| tertiary | 159 | 92 | 79 | 13 | 67 | 28 | 39 | 42.1 |
| Dementia in the family | 446 | 261 | 242 | 19 | 185 | 92 | 93 | 41.5 |
| MoCA mean (SD) | 14.2 (4.6) | 14.8 (4.2) | 11.8 (5.4) | |||||
| HD HADS-D | ||||||||
| score 1–7 | 489 | 413 | 76 | 15.5 | ||||
| score 8–10 | 117 | 94 | 23 | 19.7 | ||||
| score 11–14 | 30 | 20 | 10 | 33.3 | ||||
| score 15–21 | 14 | 10 | 4 | 28.6 | ||||
| HD I-ADL | ||||||||
| needs little help | 418 | 379 | 39 | 9.3 | ||||
| needs some help | 127 | 90 | 37 | 29.1 | ||||
| needs a lot of help | 166 | 114 | 52 | 31.3 | ||||
| NH CDR | ||||||||
| score 1 | 141 | 73 | 68 | 48.2 | ||||
| score 2 | 114 | 36 | 78 | 68.4 | ||||
| score 3 | 184 | 31 | 153 | 83.2 | ||||
HD, Home-dwellers; NH, nursing home residents; MoCA, Montreal Cognitive Assessment was not applied to nursing home participants with known severe dementia; HADS-D, Hospital Anxiety and Depression Scale-Depression; I-ADL, Instrumental activities of daily living; CDR, Clinical Dementia Rating Scale.
Of the 8,225 persons in the HUNT4 70+ who were classified with no dementia, 54 (0.7%) had a dementia registry diagnosis in one or more of the two health registries. The diagnostic rate increased from 35.6% to 45.2% with a registry diagnosis when the codes P05 and P20 were added, along with the P70 code for dementia from ICPC-2; however, at the same time, the diagnostic rate in the group with no dementia increased from 0.7% to 4.1%.
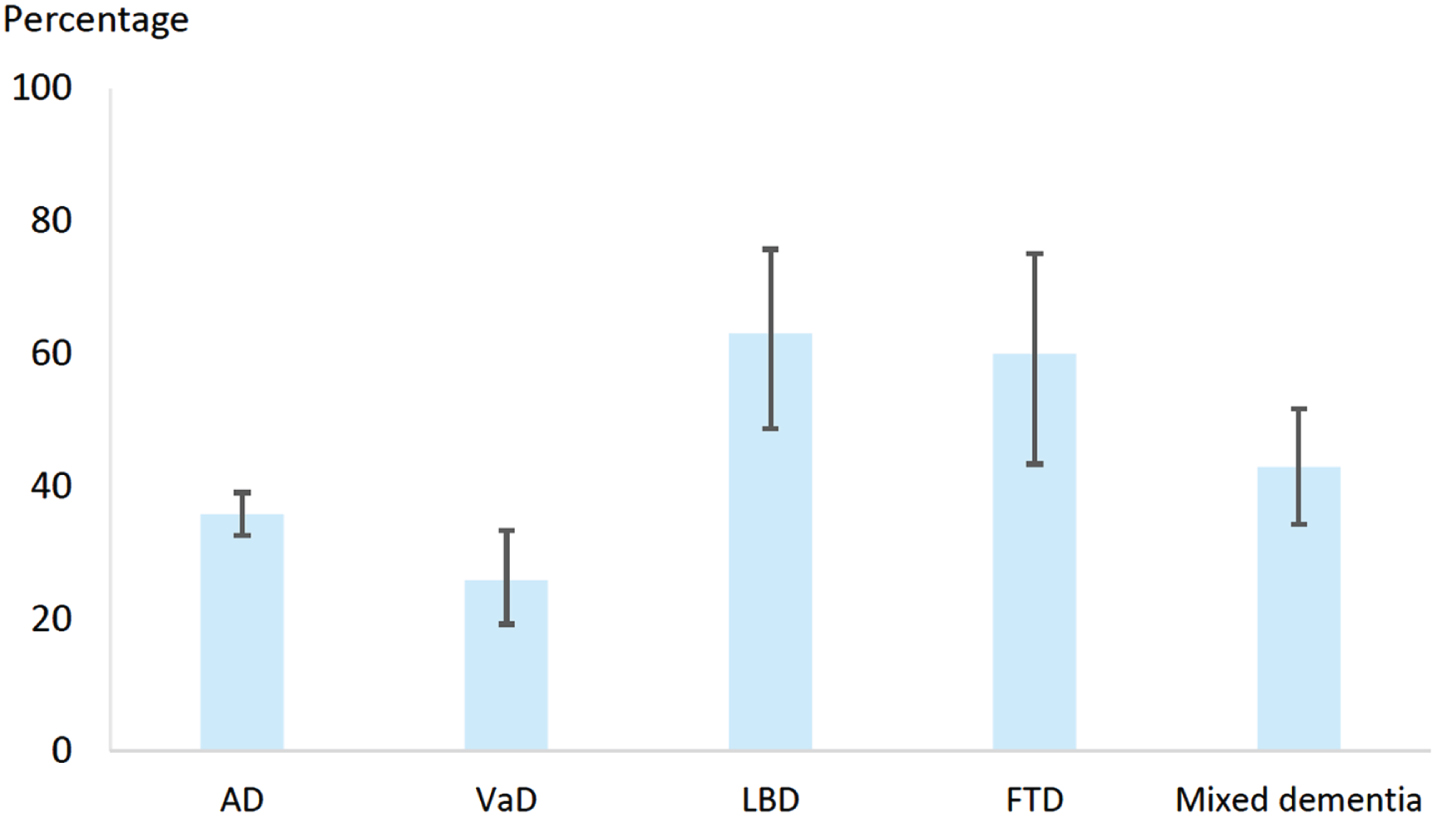
In the 1,525 participants with a HUNT dementia study diagnosis, the diagnostic rate across the different subtypes of dementia is shown in Fig. 2. For those with a research-based LBD study diagnosis, 63.0% (95% Confidence Interval (CI) 48.7–75.7) had a registry diagnosis; for those with a FTD study diagnosis, the diagnostic rate was 60.0% (95% CI 43.3–75.1); for those with a study diagnosis of mixed dementia, the rate was 42.9% (95% CI 34.3–51.7); for those with a study diagnosis of AD, the rate was 35.8% (95% CI 32.6–39.0), and for those with a study diagnosis of VaD, the rate was 25.8% (95% CI 19.2–33.3).
Fig. 2
Diagnostic rate across dementia subtypes. Percentages with 95% confidence interval.
The odds of having a registry diagnosis among home-dwelling participants was higher for participants in the age group 75–89 years compared to those aged 70–74 years, those with tertiary education compared to those with primary education, those with dementia in the family, those with the lowest MoCA scores, and those with more I-ADL help needs (Table 2). The odds of having a registry diagnosis among nursing home residents was higher for participants in the age group 75–79 years compared to those aged 70–74 years, those with dementia in the family, and those with more severe dementia (described as a score of 2 or 3 on the CDR) (Table 3).
Table 2
Diagnosed dementia and the association with sociodemographic and health related factors. Odds ratios (OR) with 95% confidence interval (CI). Sample restricted to home-dwellers, n = 1,002 and performed on the MI sample
| Crude | Sex and age adjusted | Fully adjusted* | |||||||
| Factor | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Female sex (versus male) | 1.46 | 1.06–2.01 | 0.021 | 1.35 | 0.97–1.88 | 0.073 | 1.43 | 0.95–2.14 | 0.086 |
| Age (ref 70–74 y) | 1 | Ref | 1 | Ref | 1 | Ref | |||
| 75–79 y | 3.33 | 1.72–6.44 | <0.001 | 3.34 | 1.72–6.47 | <0.001 | 3.15 | 1.57–6.31 | 0.001 |
| 80–84 y | 4.75 | 2.51–9.00 | <0.001 | 4.63 | 2.44–8.78 | <0.001 | 3.43 | 1.70–6.89 | 0.001 |
| 85–89 y | 5.56 | 2.95–10.49 | <0.001 | 5.30 | 2.80–10.02 | <0.001 | 3.39 | 1.66–6.94 | 0.001 |
| 90+ y | 2.95 | 1.46–5.93 | 0.002 | 2.77 | 2.80–10.02 | 0.004 | 1.20 | 0.53–2.70 | 0.664 |
| Education (ref elementary) | 1 | Ref | 1 | Ref | 1 | Ref | |||
| secondary | 0.83 | 0.59–1.16 | 0.272 | 0.97 | 0.69–1.38 | 0.871 | 1.15 | 0.78–1.69 | 0.490 |
| tertiary | 1.37 | 0.84–2.25 | 0.206 | 1.58 | 0.94–2.64 | 0.082 | 2.05 | 1.15–3.67 | 0.016 |
| Dementia in the family | 2.23 | 1.62–3.08 | <0.001 | 2.37 | 1.70–3.30 | <0.001 | 2.66 | 1.84–3.85 | <0.001 |
| Live with (versus living alone) | 0.85 | 0.61–1.19 | 0.332 | 1.13 | 0.76–1.67 | 0.543 | 0.99 | 0.65–1.51 | 0.966 |
| HADS-D (ref score≤7) | 1 | Ref | 1 | Ref | 1 | Ref | |||
| score 8–10 | 1.44 | 0.86–2.41 | 0.169 | 1.35 | 0.78–2.35 | 0.278 | 0.89 | 0.45–1.75 | 0.729 |
| score 11–14 | 2.30 | 1.09–4.78 | 0.029 | 2.07 | 0.95–4.50 | 0.066 | 0.90 | 0.38–2.10 | 0.803 |
| score 15–21 | 2.09 | 0.69–6.39 | 0.192 | 1.82 | 0.58–5.74 | 0.305 | 0.85 | 0.24–2.98 | 0.799 |
| MoCA (ref score≥18) | 1 | Ref | 1 | Ref | 1 | Ref | |||
| score 17–10 | 0.97 | 0.63–1.49 | 0.880 | 0.79 | 0.50–1.24 | 0.303 | 0.82 | 0.5–1.34 | 0.431 |
| score≤9 | 4.48 | 2.75–7.32 | <0.001 | 3.88 | 2.28–6.60 | <0.001 | 3.23 | 1.72–6.07 | <0.001 |
| I-ADL (ref needs little help) | 1 | Ref | 1 | Ref | 1 | Ref | |||
| needs some help | 3.11 | 1.86–5.16 | <0.001 | 3.00 | 1.75–5.14 | <0.001 | 2.82 | 1.58–5.02 | 0.001 |
| needs a lot of help | 4.05 | 2.79–6.12 | <0.001 | 4.39 | 2.76–6.99 | <0.001 | 3.55 | 2.03–6.20 | <0.001 |
*In the fully adjusted analyses, all factors listed in the first column are included. MI, multiple imputations; HADS-D, Hospital Anxiety and Depression Rating Scale-Depression; MoCA, Montreal Cognitive Assessment; I-ADL, Instrumental activities of daily living.
Table 3
Diagnosed dementia and the association with sociodemographic and health related factors. Odds ratios (OR) with 95% confidence interval (CI). Sample restricted to nursing home residents, n = 523 and performed on the MI sample
| Crude | Sex and age adjusted | Fully adjusted* | |||||||
| Factor | OR | 95% CI | p | OR | 95% CI | p | OR | 95% CI | p |
| Female sex (versus male) | 1.15 | 0.79–1.69 | 0.464 | 1.37 | 0.92–2.05 | 0.120 | 1 | 0.63–1.59 | 0.994 |
| Age (ref 70–74 y) | 1 | Ref | 1 | Ref | 1 | Ref | |||
| 75–79 y | 3.05 | 1.16–8.01 | 0.024 | 3.00 | 1.14–7.89 | 0.026 | 4.81 | 1.58–14.58 | 0.006 |
| 80–84 y | 1.79 | 0.79–4.05 | 0.164 | 1.76 | 0.77–4.00 | 0.178 | 2.08 | 0.81–5.31 | 0.127 |
| 85–89 y | 0.82 | 0.39–1.74 | 0.599 | 0.77 | 0.36–1.66 | 0.510 | 0.95 | 0.39–2.3 | 0.914 |
| 90+ y | 0.57 | 0.28–1.17 | 0.123 | 0.53 | 0.26–1.09 | 0.086 | 0.75 | 0.32–1.78 | 0.512 |
| Education (ref elementary) | 1 | Ref | 1 | Ref | 1 | Ref | |||
| secondary | 1.16 | 0.79–1.70 | 0.435 | 1.02 | 0.68–1.52 | 0.933 | 0.87 | 0.55–1.38 | 0.566 |
| tertiary | 1.71 | 0.87–3.35 | 0.121 | 1.51 | 0.75–3.04 | 0.246 | 1.32 | 0.61–2.86 | 0.486 |
| Dementia in the family | 3.64 | 1.89–6.98 | <0.001 | 3.64 | 1.79–7.41 | 0.001 | 3.06 | 1.39–6.76 | 0.007 |
| CDR (ref score 1) | 1 | Ref | 1 | Ref | 1 | Ref | |||
| score 2 | 2.37 | 1.41–4.00 | 0.001 | 2.35 | 1.36–4.04 | 0.002 | 1.89 | 1.01–3.52 | 0.045 |
| score 3 | 5.14 | 3.03–8.73 | <0.001 | 5.29 | 3.08–9.11 | <0.001 | 4.38 | 2.36–8.14 | <0.001 |
*In the fully adjusted analyses, all factors listed in the first column are included. MI, multiple imputations; CDR, Clinical Dementia Rating scale.
In the complete case analysis for home-dwellers (n = 552), the point estimates were similar, but the significance levels differed (Supplementary Table 1). In the complete case analysis for nursing home residents (n = 154), the age group 75–79 years was empty and could not be included in the analysis; otherwise, point estimates were similar, but the significance levels differed (Supplementary Table 2).
DISCUSSION
This study provides information on the proportion of diagnosed dementia, taken from a large population-based sample of Norwegian older adults. Only 35.6% of the persons with a dementia study diagnosis had a health registry diagnosis from a hospital (NPR) or from primary care (KUHR), and approximately 59% of those with a registry diagnosis were registered in both hospital and primary care. The home-dwellers with a dementia registry diagnosis were more often in the age group 75–89 years, had more advanced dementia, had higher education, and had more often dementia in the family. The nursing home residents with a dementia registry diagnosis were more often in the age group 75–79 years, had more advanced dementia, and had more often dementia in the family. Of the persons in HUNT4 70+ without a dementia study diagnosis, 0.7% had a dementia registry diagnosis recorded in the health registries.
The diagnostic rate in the present study was low, but still clearly within the earlier reported range of diagnostic rates of 20–50% [8]. As Southern et al. describes, a timely diagnosis can be understood as a diagnosis at a point where the symptoms of dementia are starting to have an impact on daily life [5]. Given that this is a population-based study, persons with dementia in the mild phase were included in the dementia study diagnosis, i.e., where most still manage their I-ADL with little help, and it is in this group that the rate of undiagnosed dementia is highest. Previous studies have shown that it might take some time from noticing symptoms to seeking cognitive assessment: in Norway, the median time from symptom detection to assessment in specialist healthcare has been estimated to be 24 months [39, 40]. To achieve high efficacy of initiatives in conserving resources and delaying more advanced care needs, we need to diagnose dementia in the early phases, whereby diagnoses can be timely [18].
Additionally, a cognitive assessment which leads to a dementia diagnosis should provide information about the disease to the person with dementia and their next of kin, along with a plan for dementia follow-up [41]. Family physicians might avoid disclosing the diagnosis to the patient or the family, due to the former’s concerns about consequences for the patient-physician relationship [42]. Family physicians’ reluctance to both diagnose and disclose dementia can be understandable, if a diagnosis does not lead to support and help, one may wonder whether it is beneficial [5, 43].
When we looked at the ICPC-2, we checked for other possible codes of dementia than the P70. The dementia diagnostic rate increased when we included the codes P05 and P20, but the diagnostic rate in people without dementia also increased. Still, it is possible that some family physicians use P05 and P20 as a diagnosis of dementia, since the ICPC-2 is a funding system and family physicians only need to submit one code in their refund claim to the KUHR [2]. If the family physician has not completed or is unsure about performing a dementia assessment, this can lead to reporting a lower code than P70 (such as P05 or P20), since these codes describe symptoms rather than a formal dementia diagnosis. At the same time, people with dementia may get support and help regardless of the diagnosis. As Aldus et al. points out, undiagnosed dementia does not necessary mean that the dementia goes unnoticed by the family physicians or the affected person and their next of kin [10].
In crude and sex- and age-adjusted analyses, the diagnostic rates were almost equal in all age groups above 75 years for home-dwellers, but in fully adjusted analyses, the diagnostic rate in the youngest (70–74 years) and the oldest (90+ years) age groups were lower, which concurs with a previous study finding lower diagnostic rates in people younger than 70 years old and those 90+ years [10]. In nursing home residents, the age group 75–79 years was more likely to be diagnosed compared to both the younger (70–74 years) and the older (80+ years) age groups. The reasons for more undiagnosed dementia in the youngest and the oldest age groups may differ from each other. For the former, the mean time from symptom debut to diagnosis for a person with young-onset AD in our study’s catchment area has recently been described as 5.5 years; both a lack of awareness of young-onset dementia and the health care system taking a long time to set a diagnosis after referral (mean 2.1 years) are possible reasons for this delay [44]. Some of the participants in the youngest age groups in the present study may have young-onset dementia. In Norway, renewal of driving license after 80 years requires a medical certificate [45] and an examination carried out by the family physician; this context can lead to more assessments of dementia in older age groups. Since the prevalence of dementia increases with age, it is understandable that the younger the person with cognitive symptoms is, the longer it takes before someone thinks of assessing dementia; however, for people over 90 years (where almost half have dementia) this should not be the case [29]. Comorbidities, fatigue, frailty, and sensory loss are higher in the oldest old, and expectation concerning their engagement in activities are often lower; all of these can make diagnosing dementia more difficult and explain why persons with dementia in this age group more often go undiagnosed [46]. Another possible reason which has been suggested for the lower diagnostic rate in this age group is that family physicians may think diagnosis may have fewer consequences for treatment and care in the oldest old [47]. Several studies have found that men more often are undiagnosed than women [10, 13, 20], but we did not find such a difference, and there are also others who have not found a sex difference [11, 48], and both culture differences and which variables that have been included in the analyses can have influenced this.
Two studies from the United Kingdom (UK) found a higher diagnostic rate in those with more education [11, 13], and one study which looked at associations between socioeconomic status and dementia diagnosis in patients referred to memory clinics in Denmark found that patients with higher incomes tended to receive an earlier diagnosis [49]. Education has a strong influence on socioeconomic status [50], and in the present study, those with higher education were more likely to be diagnosed. Inequalities in health are socially determined, and given that a higher proportion of those with the highest socioeconomic status are diagnosed, and probably more often receive follow-up, this must be addressed, in order to attain greater health equality for people with lower socioeconomic status and to reduce the diagnostic inequalities [20, 51].
Health literacy can be defined as “the cognitive and social skills which determine the motivation and ability to gain access to, understand and use information in ways which promote and maintain good health” [52]. People with dementia in the family were more likely to be diagnosed. One possible explanation for this can be that this group had more knowledge about dementia, described as cognitive skills in health literacy, and therefore more often sought a dementia assessment. If this in-depth knowledge about dementia has such an effect, it may indicate that more information targeting people at risk can contribute to more people seeking dementia assessment and being diagnosed.
The Norwegian National Dementia Guideline state that family physicians are responsible for dementia assessments in older adults, but more complex cases and rare dementia diseases should be referred to a specialist in old age psychiatry, geriatrics, or neurology in hospitals [41].
In our data, participants with research-based LBD and FTD study diagnoses had a registry diagnosis in approximately 60% of the cases, whereas participants with a study diagnosis of AD and VaD had a recorded health registry diagnoses in 36% and 26% of the cases, respectively. Those with rarer dementia diseases being diagnosed to a greater extent may indicate that family physicians assess these patients and refer them to a hospital, in accordance with the guideline.
A considerable 59% of those with a registry diagnosis had a diagnosis in both the primary care and hospital registries. This can include patients whom family physicians refer to the hospital for other conditions than dementia, but the family physician gives information about the dementia diagnosis because they consider it to be important information for the hospital. However, it is likely that many of these patients are referred to the hospital for a dementia assessment. Given that AD and VaD constitute 67% of all the dementia study diagnoses [29], and that these conditions (in many cases) should be assessed by the family physician [41], the 59% with a dementia registry diagnosis in both the primary care and hospital registries seems a bit high. However, a high degree of referrals to the hospital can also reflect the difficulties family physicians may face in making these diagnoses, since it is complex and time-consuming to assess dementia [4]. In addition, the ICPC-2 does not offer coding for the different etiological dementias, and information about which dementia disease the patient has can be important in the treatment, this may be another reason for sending the patient for a hospital assessment.
In the UK, raising the dementia diagnosis rates has been a national priority for the last 15 years, with many initiatives aimed at family physicians, the health care sector, and the general population [53]. When these initiatives first launched in 2009, the diagnostic rate in England was about 37%; by 2023, it had increased to 63% [54], and there is support that these national initiatives have contributed to the increase [55]. In the same time-frame, Norway has had three national dementia plans; the current one is Dementia Plan 2025 [56], with one of its goals being timely diagnosis. The Norwegian Directorate of Health has studied the diagnostic rate in Norway, where they applied a similar approach to the one the UK used [57], and they found the diagnostic rate in 2016–2017 to be 45%, which increased to 51% in 2022. In Norway, the diagnoses were derived from primary care and hospitals, while in the UK they were derived from primary care and also included information about nursing home residents without a dementia diagnosis who had received medication to alleviate the symptoms of dementia. In both of these studies, the dementia registry diagnoses over a one-year period was divided by the dementia prevalence derived from a population-based sample; in the UK, this was first based on a consensus view of an expert group in the Dementia UK study and the CFAS II study since 2015, while in Norway the HUNT study has been the basis of this calculation [29, 58, 59]. This comparison should be interpreted with caution, as there might be differences in help-seeking behavior between the countries as well as differences in methodology.
The present study uses the registry diagnoses given to the population-based sample from HUNT in 2017–2019, but the diagnostic rate is 10% lower than the rate for 2016–2017 provided by The Norwegian Directorate of Health. The present study did not include diagnoses given to people without a dementia study diagnosis, as well as dementia disease registry diagnoses given together with an MCI code. The present study also excluded registry diagnoses recorded in the registries after participation in HUNT. In HUNT, the collection of data within each municipality lasted only for a few weeks, and the retrieval of diagnoses of a whole year might lead to more diagnoses. The present study took place in one county, but the diagnostic rate may vary across the different counties in Norway.
Meeting the needs of the sheer numbers of people seeking assessment, treatment, and care in the coming years, at an affordable cost, will be a tremendous challenge.
Strengths and limitations
This study has a large population-based sample, comprising both home-dwellers and nursing home residents and encompassing all severity levels of dementia. The linking of the participants to the health registries resulted in no missing data, since the HUNT participants consented to connection with official records upon inclusion. In a large study from the Netherlands, the median time from dementia diagnosis to death was 5.0 years [43], and in a study from Norway, the average life expectancy from dementia symptom debut to death was 8.1 years [3]. Therefore, by retrieving all dementia diagnoses from the health registries for the last 10 years we probably have at least one registration for most of all the diagnosed patients.
We used MI to avoid loss of power and to reduce the risk of bias, which could have been a problem in our complete case analysis [36]. The results from the complete case analyses confirm the findings in our MI analyses. With complete case analyses, approximately 45% of the home-dwellers and 71% of the nursing home residents would have been left out due to missing data on one or more variables.
The diagnostic procedure for the study diagnosis (described in detail elsewhere) was based on a clinical consensus method [29]. This method was chosen to reflect the current diagnostic practice in the study’s catchment area, and it was deemed to be the best way to utilize all available information from the participants; however, no imaging or biomarker data were available.
The health registries did not contain information about dementia diagnoses given to participants at the nursing home, which means that some diagnoses may have been missed. However, most nursing homes demand a diagnosis before nursing home placement if the person has dementia; and furthermore, since the prevalence rate of dementia in Norwegian nursing homes is 84.3% [29] and the average stay in a nursing home is 2 years [60], the number of people that develop dementia and receive a dementia diagnosis during their nursing home stay is probably quite low.
The catchment area in our study consists of small towns and rural areas; the diagnostic rate might be different in city populations. The participants, for the most part, come from an ethnically homogeneous group, which may limit the generalizability to other populations with greater ethnic diversity [21].
Conclusion
Undiagnosed dementia in Norway is common, as only one-third of those with dementia are diagnosed. The diagnosis often comes in a late stage of the dementia, when the person with dementia might be unable to take an active part in planning the future and making legal decisions. This highlights the need to find new ways to promote and achieve timely diagnosis for this condition. Special effort should be made to ensure that people with lower socio-economic status are offered assessment and diagnostic work-up. Since people with a family history of dementia are more often diagnosed, raising public knowledge about dementia may help raise the diagnostic rate.
Knowledge on the extent of undiagnosed dementia can offer important information about the resources needed in diagnostic assessment and follow-up. This will be of great importance in the years to come, which will see growing numbers of people with dementia. At the same time, new diagnostic opportunities, and treatment in an early phase of AD, are on the rise. With these changes, the current assessment and diagnostic practices will be challenged, and we will need to assess how to organize diagnostic services in the future. The capacity to assess more dementia in hospitals is not likely to increase, and there is a need to enable primary care to take on a bigger responsibility in the diagnostic work-up of dementia.
AUTHORS CONTRIBUTIONS
Linda Gjøra (Data curation; Formal analysis; Investigation; Methodology; Writing – original draft; Writing – review & editing); Bjørn Heine Strand (Formal analysis; Methodology; Writing – original draft; Writing – review & editing); Sverre Bergh (Data curation; Writing – review & editing); Ingunn Bosnes (Writing – review & editing); Aud Johannessen (Writing – review & editing); Gill Livingston (Writing – review & editing); Håvard Kjesbu Skjellegrind (Data curation; Investigation; Writing – review & editing); Geir Selbæk (Conceptualization; Data curation; Methodology; Project administration; Supervision; Writing – original draft; Writing – review & editing).
ACKNOWLEDGMENTS
The data collection took part in the fourth wave of the Trøndelag Health Study (HUNT). HUNT is a collaboration between HUNT Research Centre (Faculty of Medicine and Health Sciences, Norwegian University of Science and Technology NTNU), Trøndelag County Council, Central Norway Regional Health Authority, and the Norwegian Institute of Public Health.
FUNDING
The study was financed by the Norwegian Health Association. There were no restrictions regarding the research conduct.
CONFLICT OF INTEREST
Håvard Kjesbu Skjellegrind is a board member for NOEN AS, a company that provides counselling and activity services for persons with dementia and their families. The other authors have no conflicts of interest regarding the publication of this article.
DATA AVAILABILITY
The Trøndelag Health Study (HUNT) has invited persons aged 13 - 100 years to four surveys between 1984 and 2019. Comprehensive data from more than 140,000 persons having participated at least once and biological material from 78,000 persons are collected. The data are stored in HUNT databank and biological material in HUNT biobank. HUNT Research Centre has permission from the Norwegian Data Inspectorate to store and handle these data. The key identification in the data base is the personal identification number given to all Norwegians at birth or immigration, whilst de-identified data are sent to researchers upon approval of a research protocol by the Regional Ethical Committee and HUNT Research Centre. To protect participants’ privacy, HUNT Research Centre aims to limit storage of data outside HUNT databank, and cannot deposit data in open repositories. HUNT databank has precise information on all data exported to different projects and are able to reproduce these on request. There are no restrictions regarding data export given approval of applications to HUNT Research Centre. For more information see: http://www.ntnu.edu/hunt/data.
SUPPLEMENTARY MATERIAL
[1] The supplementary material is available in the electronic version of this article: https://dx.doi.org/10.3233/JAD-240037.
REFERENCES
[1] | GBD 2019 Dementia Forecasting Collaborators ((2022) ) Estimation of the global prevalence of dementia in 2019 and forecasted prevalence in 2050: An analysis for the Global Burden of Disease Study 2019. Lancet Public Health 7: , 105–125. |
[2] | Kinge JM , Dieleman JL , Karlstad Ø , Knudsen AK , Klitkou ST , Hay SI , Vos T , Murray CJL , Vollset SE ((2023) ) Disease-specific health spending by age, sex, and type of care in Norway: A national health registry study. BMC Med 21: , 201. |
[3] | Vossius C , Selbæk G , Ydstebø AE , Benth JS , Godager G , Lurås H , Bergh S ((2015) ) Ressursbruk og sykdomsforløp ved demens (REDIC), Alderspsykiatrisk forskningssenter, Sykehuset Innlandet. |
[4] | World Health Organization, A blueprint for dementia research, https://www.who.int/publications/i/item/9789240058248, Last updated October 04, 2022, Accessed on July 07, 2023. |
[5] | Southern A ((2015) ) Diagnose or disempower? Receiving a diagnosis of dementia in Wales. https://www.alzheimers.org.uk/sites/default/files/migrate/downloads/diagnose_or_disempower.pdf, Alzheimer’s Society, Accessed on February 9, 2024. |
[6] | Gauthier S , Rosa-Neto P , Morais J , Webster C ((2021) ) Journey through the diagnosis of dementia. Alzheimer’s Disease International, London, UK. |
[7] | Frisoni GB , Altomare D , Ribaldi F , Villain N , Brayne C , Mukadam N , Abramowicz M , Barkhof F , Berthier M , Bieler-Aeschlimann M , Blennow K , Brioschi Guevara A , Carrera E , Chételat G , Csajka C , Demonet JF , Dodich A , Garibotto V , Georges J , Hurst S , Jessen F , Kivipelto M , Llewellyn DJ , McWhirter L , Milne R , Minguillón C , Miniussi C , Molinuevo JL , Nilsson PM , Noyce A , Ranson JM , Grau-Rivera O , Schott JM , Solomon A , Stephen R , van der Flier W , van Duijn C , Vellas B , Visser LNC , Cummings JL , Scheltens P , Ritchie C , Dubois B ((2023) ) Dementia prevention in memory clinics: Recommendations from the European task force for brain health services. Lancet Reg Health Eur 26: , 100576. |
[8] | Prince M , Bryce R , Ferri C ((2011) ) World Alzheimer Report 2011. The benefits of early diagnosis and intervention. Alzheimer’s Disease International, London, UK. |
[9] | Gamble LD , Matthews FE , Jones IR , Hillman AE , Woods B , Macleod CA , Martyr A , Collins R , Pentecost C , Rusted JM , Clare L ((2022) ) Characteristics of people living with undiagnosed dementia: Findings from the CFAS Wales study. BMC Geriatr 22: , 409. |
[10] | Aldus CF , Arthur A , Dennington-Price A , Millac P , Richmond P , Dening T , Fox C , Matthews FE , Robinson L , Stephan BCM , Brayne C , Savva GM ((2020) ) Health Services and Delivery Research. In Undiagnosed dementia in primary care: A record linkage study, NIHR Journals Library, Southampton, UK. |
[11] | Amjad H , Roth DL , Sheehan OC , Lyketsos CG , Wolff JL , Samus QM ((2018) ) Underdiagnosis of dementia: An observational study of patterns in diagnosis and awareness in US older adults. J Gen Intern Med 33: , 1131–1138. |
[12] | Eichler T , Thyrian JR , Hertel J , Köhler L , Wucherer D , Dreier A , Michalowsky B , Teipel S , Hoffmann W ((2014) ) Rates of formal diagnosis in people screened positive for dementia in primary care: Results of the DelpHi-Trial. J Alzheimers Dis 42: , 451–458. |
[13] | Savva GM , Arthur A ((2015) ) Who has undiagnosed dementia? A cross-sectional analysis of participants of the Aging, Demographics and Memory Study. Age Ageing 44: , 642–647. |
[14] | Lee SJ , Larson EB , Dublin S , Walker R , Marcum Z , Barnes D ((2018) ) A cohort study of healthcare utilization in older adults with undiagnosed dementia. J Gen Intern Med 33: , 13–15. |
[15] | Rizzuto D , Feldman AL , Karlsson IK , Dahl Aslan AK , Gatz M , Pedersen NL ((2018) ) Detection of dementia cases in two Swedish health registers: A validation study. J Alzheimers Dis 61: , 1301–1310. |
[16] | Nguyen T , Li X ((2020) ) Understanding public-stigma and self-stigma in the context of dementia: A systematic review of the global literature. Dementia (London) 19: , 148–181. |
[17] | Cations M , Radisic G , Crotty M , Laver KE ((2018) ) What does the general public understand about prevention and treatment of dementia? A systematic review of population-based surveys. PLoS One 13: , e0196085. |
[18] | Dubois B , Padovani A , Scheltens P , Rossi A , Dell’Agnello G ((2016) ) Timely diagnosis for Alzheimer’s disease: A literature review on benefits and challenges. J Alzheimers Dis 49: , 617–631. |
[19] | Wilkins CH , Wilkins KL , Meisel M , Depke M , Williams J , Edwards DF ((2007) ) Dementia undiagnosed in poor older adults with functional impairment. J Am Geriatr Soc 55: , 1771–1776. |
[20] | Lang L , Clifford A , Wei L , Zhang D , Leung D , Augustine G , Danat IM , Zhou W , Copeland JR , Anstey KJ , Chen R ((2017) ) Prevalence and determinants of undetected dementia in the community: A systematic literature review and a meta-analysis. BMJ Open 7: , e011146. |
[21] | Åsvold BO , Langhammer A , Rehn TA , Kjelvik G , Grøntvedt TV , Sørgjerd EP , Fenstad JS , Heggland J , Holmen O , Stuifbergen MC , Vikjord SAA , Brumpton BM , Skjellegrind HK , Thingstad P , Sund ER , Selbæk G , Mork PJ , Rangul V , Hveem K , Næss M , Krokstad S ((2023) ) Cohort profile update: The HUNT Study, Norway. Int J Epidemiol 52: , e80–e91. |
[22] | Nasreddine Z, MoCA Cognition, https://mocacognition.com/faq/, Last updated, 2023. Accessed on July 18, 2023. |
[23] | Nasreddine ZS , Phillips NA , Bedirian V , Charbonneau S , Whitehead V , Collin I , Cummings JL , Chertkow H ((2005) ) The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J Am Geriatr Soc 53: , 695–699. |
[24] | Lawton MP , Brody EM ((1969) ) Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 9: , 179–186. |
[25] | Zigmond AS , Snaith RP ((1983) ) The hospital anxiety and depression scale. Acta Psychiatr Scand 67: , 361–370. |
[26] | Bjelland I , Dahl AA , Haug TT , Neckelmann D ((2002) ) The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res 52: , 69–77. |
[27] | Hughes CP , Berg L , Danziger WL , Coben LA , Martin RL ((1982) ) A new clinical scale for the staging of dementia. Br J Psychiatry 140: , 566–572. |
[28] | American Psychiatric Association ((2013) ) Diagnostic and statistical manual of mental disorders (5th ed.), American Psychiatric Publishing, Arlington. |
[29] | Gjøra L , Strand BH , Bergh S , Borza T , Brækhus A , Engedal K , Johannessen A , Kvello-Alme M , Krokstad S , Livingston G , Matthews FE , Myrstad C , Skjellegrind H , Thingstad P , Aakhus E , Aam S , Selbæk G ((2021) ) Current and future prevalence estimates of mild cognitive impairment, dementia, and its subtypes in a population-based sample of people 70 years and older in Norway: The HUNT Study. J Alzheimers Dis 79: , 1213–1226. |
[30] | Statistics Norway, Classification of education (NUS), https://www.ssb.no/en/klass/klassifikasjoner/36,SSB, Last updated October 2023, Accessed on November 23, 2023. |
[31] | Bakken IJ , Ariansen AMS , Knudsen GP , Johansen KI , Vollset SE ((2020) ) The Norwegian Patient Registry and the Norwegian Registry for Primary Health Care: Research potential of two nationwide health-care registries. Scand J Public Health 48: , 49–55. |
[32] | The Norwegian Directorate of Health, Norsk pasientregister (NPR), https://www.helsedirektoratet.no/tema/statistikk-registre-og-rapporter/helsedata-og-helseregistre/norsk-pasientregister-npr/innhold-og-kvalitet-i-npr,Helsedirektoratet, Last updated April 26, 2023, Accessed on July 20, 2023. |
[33] | World Health Organization ((1992) ) The ICD-10 classification of mental and behavioural disorders: Clinical descriptions and clinical guidelines. World Health Organization, Geneva. |
[34] | The Norwegian Directorate of Health, KUHR-databasen, https://www.helsedirektoratet.no/tema/statistikk-registre-og-rapporter/helsedata-og-helseregistre/kuhr, Helsedirektoratet, Last updated July 03, 2023, Accessed on July 20, 2023. |
[35] | World Health Organization, International Classification of Primary Care, 2nd edition (ICPC-2) https://www.who.int/standards/classifications/other-classifications/international-classification-of-primary-care, World Health Organization 2023, Accessed on July 20, 2023. |
[36] | Sterne JA , White IR , Carlin JB , Spratt M , Royston P , Kenward MG , Wood AM , Carpenter JR ((2009) ) Multiple imputation for missing data in epidemiological and clinical research: Potential and pitfalls. BMJ 338: , b2393. |
[37] | Madley-Dowd P , Hughes R , Tilling K , Heron J ((2019) ) The proportion of missing data should not be used to guide decisions on multiple imputation. J Clin Epidemiol 110: , 63–73. |
[38] | StataCorp LLC (2023), College Station, TX, USA. |
[39] | Wackerbarth SB , Johnson MMS ((2002) ) The carrot and the stick: Benefits and barriers in getting a diagnosis. Alzheimer Dis Assoc Disord 16: , 213–220. |
[40] | Helvik AS , Engedal K , Śaltytėq Benth J , Selbæk G ((2018) ) Time from symptom debut to dementia assessment by the specialist healthcare service in Norway. Dement Geriatr Cogn Dis Extra 8: , 117–127. |
[41] | The Norwegian Directorate of Health, Demens - nasjonal faglig retningslinje https://www.helsedirektoratet.no/retningslinjer/demens,Helsedirektoratet, Last updated October 31, 2022, Accessed on August 21, 2023. |
[42] | Koch T , Iliffe S ((2010) ) Rapid appraisal of barriers to the diagnosis and management of patients with dementia in primary care: A systematic review. BMC Fam Pract 11: , 52. |
[43] | Joling KJ , Janssen O , Francke AL , Verheij RA , Lissenberg-Witte BI , Visser PJ , van Hout HPJ ((2020) ) Time from diagnosis to institutionalization and death in people with dementia. Alzheimers Dement 16: , 662–671. |
[44] | Kvello-Alme M , Bråthen G , White LR , Sando SB ((2021) ) Time to diagnosis in young onset Alzheimer’s disease: A population-based study from Central Norway. J Alzheimers Dis 82: , 965–974. |
[45] | The Norwegian Directorate of Health, Driving licence and health requirements, https://www.helsenorge.no/en/health-rights-in-norway/driving-licence-and-health-requirements/, Last updated January 29, 2023, Accessed on December 08, 2023. |
[46] | Brumback-Peltz C , Balasubramanian AB , Corrada MM , Kawas CH ((2011) ) Diagnosing dementia in the oldest-old. Maturitas 70: , 164–168. |
[47] | Prins A , Hemke F , Pols J , Moll van Charante EP ((2016) ) Diagnosing dementia in Dutch general practice: A qualitative study of GPs’ practices and views. Br J Gen Pract 66: , e416–422. |
[48] | Sternberg SA , Wolfson C , Baumgarten M ((2000) ) Undetected dementia in community-dwelling older people: The Canadian Study of Health and Aging. J Am Geriatr 48: , 1430–1434. |
[49] | Petersen JD , Wehberg S , Packness A , Svensson NH , Hyldig N , Raunsgaard S , Andersen MK , Ryg J , Mercer SW , Sondergaard J , Waldorff FB ((2021) ) Association of socioeconomic status with dementia diagnosis among older adults in Denmark. JAMA Netw Open 4: , e2110432. |
[50] | Lindberg MH , Chen G , Olsen JA , Abelsen B ((2022) ) Combining education and income into a socioeconomic position score for use in studies of health inequalities. BMC Public Health 22: , 969. |
[51] | World Health Organization, Social determinants of health, https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1, Last updated 2023, Accessed on July 19, 2023. |
[52] | World Health Organization ((1998) ) Health Promotion Glossary, World Health Organization, Geneva. |
[53] | NHS England, New plans to improve dementia diagnosis rates, https://www.england.nhs.uk/2013/05/dementia-targets/, Last updated March 21, 2017, Accessed on December 12, 2023. |
[54] | NHS Digital, Primary Care Dementia Data. May 2023, https://digital.nhs.uk/data-and-information/publications/statistical/primary-care-dementia-data/may-2023#related-links, Last updated June 15, 2023, Accessed on December 12, 2023. |
[55] | Donegan K , Fox N , Black N , Livingston G , Banerjee S , Burns A ((2017) ) Trends in diagnosis and treatment for people with dementia in the UK from 2005 to 2015: A longitudinal retrospective cohort study. Lancet Public Health 2: , e149–e156. |
[56] | Norwegian Ministry of Health and Care Services ((2022) ) Dementia Plan 2025, Norwegian Ministry of Health and Care Services, Oslo. |
[57] | The Norwegian Directorate of Health, Nasjonal kartlegging av kommunenes tilrettelagte tjenestetilbud for personer med demens 2022, https://www.helsedirektoratet.no/rapporter/nasjonal-kartlegging-av-kommunenes-tilrettelagte-tjenestetilbud-for-personer-med-demens-2022, Last updated June 14, 2023, Accessed on December 14, 2023. |
[58] | Knapp M, Black N, Dixon J, Damant J, Rehill A, Tan S, Independent assessment of improvements in dementia care and support since 2009. Report from the Policy Innovation Research Unit and the NIHR School for Social Care Research. https://researchonline.lshtm.ac.uk/id/eprint/2391582/1/2014-9%20Assessing%20Dementia%20Report.pdf, Policy Innovation Research Unit and NIHR School for Social Care Research, LSE and LSHTM, Last updated October, 2014, Accessed on December 15, 2023. |
[59] | Matthews FE , Arthur A , Barnes LE , Bond J , Jagger C , Robinson L , Brayne C , Medical Research Council Cognitive Function and Ageing Collaboration ((2013) ) A two-decade comparison of prevalence of dementia in individuals aged 65 years and older from three geographical areas of England: Results of the Cognitive Function and Ageing Study I and II. Lancet 382: , 1405–1412. |
[60] | Kjelvik J , Jønsberg E ((2017) ) Botid i sykehjem og varighet av tjenester til hjemmeboende, The Norwegian Directorate of Health, Oslo. |

