
Current Status and Challenges in Dementia Care in the Philippines: A Scoping Review
Abstract
Background:
Dementia prevalence is increasing in low- and middle-income countries such as the Philippines.
Objective:
This study aimed to give an overview of dementia care in the Philippines and to identify gaps in terms of local epidemiology, research, financial coverage, diagnostics, pharmacotherapy, manpower, and caregiver support.
Methods:
This scoping review was conducted using the Preferred Reporting Items for Systematic reviews and Meta-analysis guidelines extension for scoping reviews. Six international and two local databases, and government and non-government websites were searched. Data published in the English or Filipino language on dementia epidemiology, research, diagnostics, management, manpower, and training were extracted from the earliest indexed record until June 2022.
Results:
The prevalence of dementia in the Philippines is high and research output on all aspects of dementia is low. Cost is a major barrier as health care coverage is limited, with reliance mainly on out-of-pocket payments, leading to challenges in the proper diagnosis and treatment of dementia. There is a low specialist-to-population ratio, with shortages beyond manpower and training.
Conclusions:
Gaps in dementia care include limited published local data, high healthcare costs, inadequate health financing, and limited manpower.
INTRODUCTION
Dementia is a neurocognitive disorder presenting with deterioration in cognitive function beyond what is expected from the consequences of biological aging, significantly interfering with activities of daily living and social autonomy [1]. Approximately 60% of people with dementia currently reside in low- and middle-income countries (LMIC) including the Philippines [2]. Filipinos aged 60 and older comprised 7.5% of the total Philippine population as of 2020 [3], and this proportion is expected to increase to 12.8% by 2035 [4].
The Philippines is an archipelago with 7,641 islands subdivided into 17 administrative regions, 81 provinces, 145 cities, 1,489 municipalities, and 42,044 barangays, each with their own local governing bodies [5, 6]. With the enactment of the Local Government Code of 1991 or Republic Act (RA) 7160, the autonomy and responsibility of providing basic health services have been transferred to the local government units [5, 7]. While this devolution was implemented to encourage self-reliance and ensure efficiency in the allocation and distribution of resources, difficulties in coordination between national and local governments, poor health prioritization, lack of facilities and skilled health workers, and poorly functioning referral systems have led to a fragmented system delivering inadequate services to vulnerable groups such as older adult Filipinos [5, 7].
Earlier scoping reviews have explored the status and challenges in the care of people with various neurological disorders such as bacterial meningitis, autoimmune encephalitis, brain tumors, epilepsy, multiple sclerosis, and Parkinson’s disease in the Philippines [8–13], but comprehensive local data on dementia remains lacking. This scoping review aimed to give an overview of dementia care in the Philippines and to identify challenges and gaps in the provision of dementia care in terms of local epidemiology, research, financial coverage, diagnostics, pharmacotherapy, manpower, and caregiver support.
METHODS
Protocol
Our study adhered to the Preferred Reporting Items for Systematic reviews and Meta-analysis (PRISMA) extension for scoping reviews [14]. This article does not contain any studies involving human or animal participants performed by any of the authors.
Eligibility criteria
We considered published systematic reviews, review articles, cohort studies, conference proceedings, clinical practice guidelines, and local government data on the local epidemiology, research output, health financing, diagnostics, pharmacotherapy, manpower availability, and caregiver training for dementia in the Philippines. Case reports, abstracts only, and animal and plant studies were excluded. Articles not in English or Filipino were excluded. Only human studies set in the Philippines were included, with studies on Filipinos or healthcare workers living abroad excluded. No restrictions were set in terms of the date of publication.
Information sources
We searched international databases including PubMed, Scopus, EMBASE, EBSCO, Web of Science, and ClinicalTrials.gov. We also searched local medical databases such as the Health Research and Development Information Network (HERDIN) and Philippine E-Journals for relevant studies. We accessed pertinent and available literature via official websites of international organizations (i.e., World Health Organization, World Bank), government and non-government agencies [i.e., Philippine Department of Health (DOH), Philippine Health Insurance Corporation (PhilHealth), Philippine Statistics Authority (PSA), National Institutes of Health-Institute of Aging, and local professional organizations (i.e., Philippine Neurological Association (PNA), Alzheimer’s Disease Association of the Philippines (ADAP), Dementia Society of the Philippines (DSP), Philippine College of Geriatric Medicine (PCGM), and the Philippine Society of Geriatrics and Gerontology (PSGG)]. Data on the cost of diagnostics and medications were identified through relevant laboratories and institutions via website and phone queries. Due to paucity of data on some categories, grey literature was explored through links and secondary searches.
Search and selection of sources
We conducted a scoping review of the available literature from the earliest indexed record until June 2022 using “(dementia OR Alzheimer* OR vascular dementia OR Lewy body disease OR frontotemporal dementia) AND Philippines” as our search string. Duplicates were excluded. Authors PDL, AAS, and VMA separately screened all titles and abstracts based on the eligibility criteria; author RDJ was consulted for disagreements. We then retrieved the full text of eligible articles for data extraction.
We also searched the websites of international and local organizations as previously mentioned using the terms “incidence, prevalence, research, cost, laboratory, medication, neurologist, psychiatrist, geriatrician, caregiver,” “dementia,” AND “Philippines.”
RESULTS
The search of studies
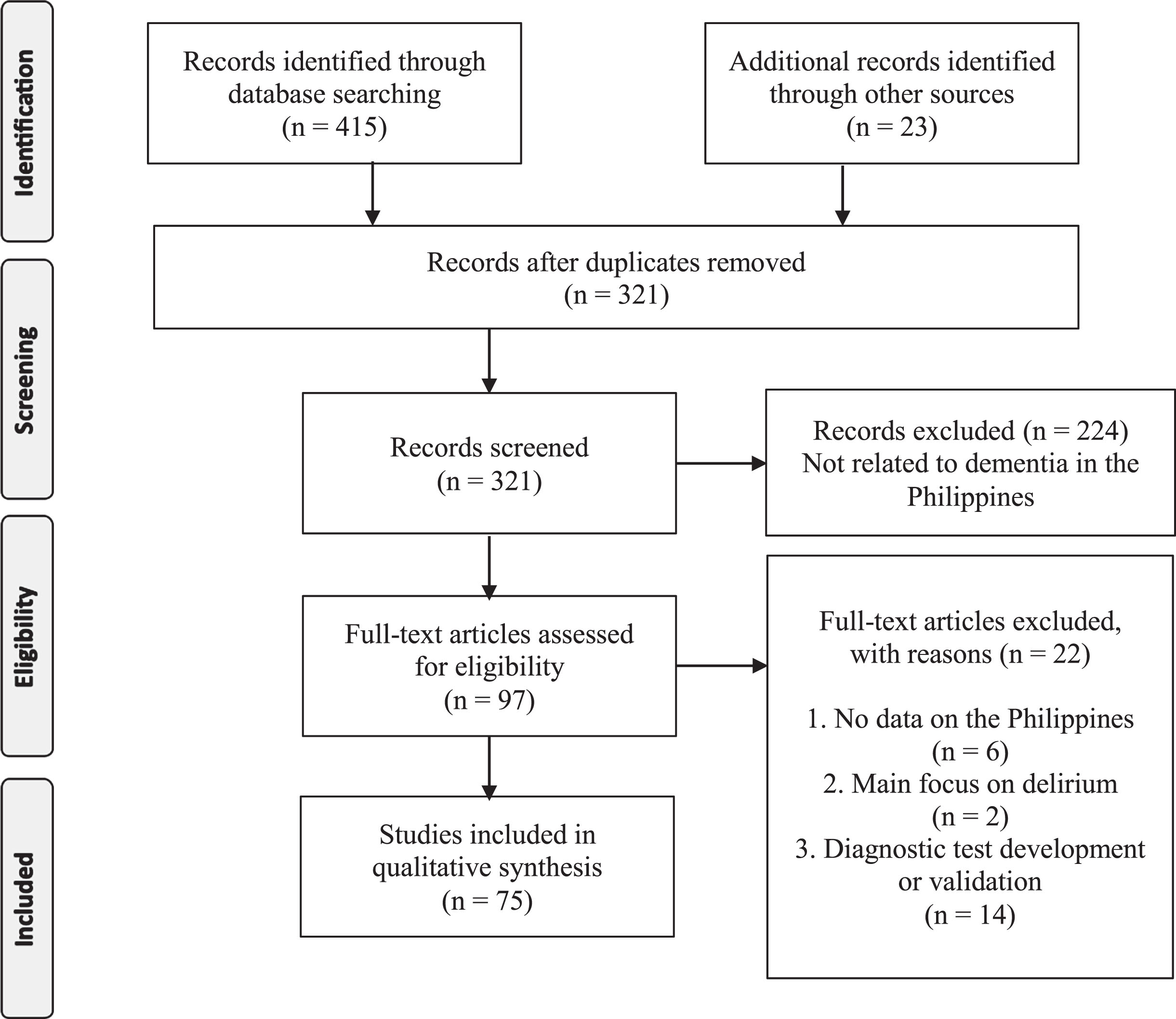
The search yielded a total of 438 articles (see Fig. 1). We then screened 321 articles after duplicates were removed. A total of 97 full-text articles were assessed for eligibility, out of which we excluded 22 articles which did not have data on the Philippines, and which focused on delirium, test construction, and validation for their main topic. Thus, a total of 75 articles were included for synthesis. Of the 75 articles, 10 focused on epidemiology, 3 on research, 23 on health service delivery and financing, 5 on diagnostics, 18 on management, 8 on manpower resources, 8 on caregiver support.
Fig. 1
Flow diagram adapted from PRISMA extension for scoping reviews.
The local epidemiology of dementia
As of 2015, the prevalence of dementia in the Philippines was 10.6% for those 60 years and over, with an age-standardized prevalence of 14.2%, equating to an estimated 726,864 people living with dementia [15]. As of 2021, the estimated dementia incidence in the Philippines was at 16 per 1,000, with an estimated increase in dementia cases to 1,474,588 by 2030, 1,972,067 by 2040, and 2,529,436 by 2050 [16]. The most common subtype of dementia was AD (85.5%), followed by vascular dementia (11.7%), and other dementias (2.7%). Increasing age was associated with an increased risk for dementia, while educational attainment was associated with a reduced risk. Sex and civil status were not associated with dementia risk [15]. The mean total disease duration was 3.84 years, with an estimated disability-adjusted life years of 2,876 years per 100,000 persons [16]. In order to address the lack of updated data on dementia incidence and prevalence, the PNA is in the process of creating a multi-center, prospective database on Filipinos diagnosed with cognitive impairment and dementia, targeted to be completed by 2024 [17].
Dementia research in the Philippines
Dementia research and innovation has been identified as an action area in the WHO’s global action plan on the public health response to dementia for 2017-2025, with the global target of doubling the output of global research between 2017 and 2025 [2]. Research productivity in the field of dementia has been noted to be growing rapidly over the recent years; however, research output on dementia in the Philippines has remained low. In a previously conducted systematic search of published articles on dementia in Southeast Asia by Sy, et al. (2020), only 11 out of 1,006 (1.1%) publications were from the Philippines, comprising only 8 of the 687 (1.2%) publications found in journals with impact factor [18]. This signifies the need for adequate resources and government support in order to advance dementia research in the country.
Financial coverage of costs
The Philippines’ current health expenditure (CHE) has increased by 12.6%, from USD 14.34 billion in 2019 to USD 16.14 billion in 2020. Its total health expenditure (THE), considering the health capital formation expenditure, has also increased by 10.4%, from USD 16.39 billion in 2019 to USD 18.02 billion in 2020; now accounting for 5.6% of the country’s gross domestic product (GDP). Consequently, per capita health spending has also increased by 10.7%, from USD 133.74 in 2019 to USD 148.04 in 2020. However, despite these improvements in health financing, the Philippines still only ranks 6th out of 11 countries in Southeast Asia, with its THE per capita equating to only 5.4% of that of Singapore [19]. Over the past decades, out-of-pocket spending has been the leading source of health expenditure in the country. In 2020, government schemes and compulsory contributory health care financing schemes contributed the largest percentage to health expenditure (45.7%), but household out-of-pocket payments still came in at a close second place (44.7%) [20]. As per the latest PSA data, the average annual family income is USD 5,640 (USD 1.00 = PhP 55.5 as of May 1, 2023), with an average annual family expenditure of USD 4,306, of which only 2.7% is being allocated for health [21].
In order to provide some financial risk protection, PhilHealth was established through the National Health Insurance Act of 1995, with the goals of providing health insurance coverage and ensuring affordable, acceptable, available, and accessible healthcare services for all Filipinos [22]. Through RA 10645, all senior citizens are automatically covered by the National Health Insurance Program [23]. Some of the common causes for hospital admissions in older adults, including pneumonia, osteoporosis, osteoarthritis, and dementia are covered by PhilHealth; in particular, case rates for dementia ranged from USD 141-180 [24]. However, despite its high coverage (92%), benefit utilization is low, likely due to poor awareness of members and maldistribution of health services and facilities [5, 6]. Social insurance programs such as the Social Security System for the private sector and the Government Service Insurance System for the public sector also aim to provide financial protection for their members, but they remain poorly utilized. Based on the 2014 Consumer Finance Survey, only 1 in every 4 economically dominant household members aged 60 and above were covered by social security, with 1 in every 4 pensioners receiving a monthly pension of below USD 36, and 3 in every 5 pensioners receiving a monthly pension of below USD 90 [25]. Another means of alleviating financial burden on older adults was the passage and implementation of the Senior Citizens Act (RA 7432), further amended by the Expanded Senior Citizens Act of 2003 (RA 9257) and 2010 (RA 9994). Through these legislations, older adults are now entitled to a twenty percent discount and exemption from the value-added tax (VAT) in the purchase of medicines, vaccines, medical and dental services, and diagnostic and laboratory fees in all private facilities, as well as free medical and dental services, and diagnostic and laboratory fees in all government facilities [26]. In 2017, the DOH has issued policy guidelines on the standards of care for older persons in the acute and sub-acute care, rehabilitation facility, continuing care retirement community and long-term care settings; enumerating guidelines on the creation of safe and secure environments and strengthening collaborative effort among various stakeholders [27]. Lastly, the National Commission of Senior Citizens Act (RA 11350) was also created in 2019 to ensure the full implementation of government laws, policies, and programs on senior citizens, as well as to formulate policies geared towards the promotion and protection of the rights and well-being of senior citizens [28]. This legislation, however, effectively misses out on the population of young-onset dementia and also does not provide additional benefits to older adults living with dementia who require higher levels and costs of care.
Challenges in the diagnosis of dementia
Initial assessment of dementia heavily relies on the patient’s clinical history, with emphasis on the cognitive, behavioral, and psychological symptoms, and the impact of these symptoms on the patient’s daily activities. A complete physical examination, including a neurologic examination, should be performed to exclude possible visual and auditory problems and to check for focal neurologic deficits. Several cognitive assessment tools in the form of validated questionnaires are available to evaluate the patient’s cognition, mood, behavior, and functional performance. Laboratory tests and neuroimaging studies are also necessary to rule out reversible (i.e., toxic, metabolic, infectious) causes of cognitive decline (see Table 1) [29].
Table 1
Cost of laboratory and neuroimaging tests in government and private hospitals
| Test | Cost, in USD | Cost, in USD | Cost, in USD |
| (Government – | (Government –Full) | (Private)** | |
| Subsidized)* | |||
| Basic work-up | |||
| Complete blood count | 0–3 | 5 | 12 |
| Basic electrolytes | 0–14 | 30 | 105 |
| Thyroid function test | 0–12 | 21 | 105 |
| Rapid plasma reagin | 0–3 | 8 | 14 |
| Serum B12 | Not available | Not available | 117 |
| Additional work-up | |||
| Serum amyloid | Not available | Not available | 400 |
| ApoE4 | Not available | Not available | 101 |
| Cranial CT scan plain | 0–27 | 67 | 168 |
| Cranial MRI plain | 0–78 | 99 | 296 |
| Cranial FDG PET*** plain | Not available | Not available | 1,100 |
| Cranial FDG PET with contrast | Not available | Not available | 1,255 |
| Cranial amyloid PET | Not available | Not available | 2,672 |
| Electroencephalogram | 0–20 | 49 | 46 |
*Diagnostic test prices from the Philippine General Hospital listed as of May 1, 2023 [30]. **Diagnostic test prices from St. Luke’s Medical Center listed as of May 1, 2023 [31]. ***Fully or partially subsidized, irrespective of insurance coverage. FDG, F-fluorodeoxyglucose; PET, positron emission tomography; CT, computed tomography; MRI, magnetic resonance imaging.
Diagnostic tests are primarily funded out-of-pocket, as PhilHealth only covers in-hospital admissions and coverage is based on predetermined case rates (see Table 2). Dementia has a case rate of USD 180, with USD 54 as professional fee and USD 126 as hospital fee. Given the nature of the disease, most people with dementia are seen in outpatient clinics. Consultation fees with neurologists in private clinics typically range from USD 15 to USD 45, while consultation fees with dementia specialists in memory clinics typically range from USD 36 to USD 90 [30, 31]. These are not yet covered by PhilHealth and may only be partially covered by private health maintenance organizations or insurance.
Table 2
PhilHealth case rates for dementia as of May 1, 2023
| ICD 10 | Description | Case Rate | Professional | Health Care |
| Code | (USD) | Fee (USD) | Institution | |
| Fee (USD) | ||||
| F01.0 | Vascular dementia of acute onset | 148 | 44 | 103 |
| G30.9 + F00.9** | Dementia in Alzheimer’s disease, unspecified | 180 | 54 | 126 |
| G31.8 | Lewy body dementia | 180 | 54 | 126 |
| B22.0 | HIV dementia | 400 | 120 | 280 |
| F01.1 | Multi-infarct dementia, predominantly | 141 | 42 | 98 |
| cortical dementia | ||||
| F01.8 | Other vascular dementia | 141 | 42 | 98 |
| F01.9 | Vascular dementia, unspecified | 141 | 42 | 98 |
| F03 | Unspecified dementia, presenile dementia | 141 | 42 | 98 |
**HIV –human immunodeficiency virus, USD –United States dollar.
Challenges in the treatment of dementia
Management of dementia involves both pharmacologic and non-pharmacologic treatment strategies. Medications used in the treatment of dementia include acetylcholinesterase inhibitors (donepezil, galantamine, and rivastigmine) and N-methyl-D-aspartate antagonist (memantine). Galantamine is no longer available in the Philippines as of May 1, 2023. Comparing the cost, availability, and affordability of these AD drugs among 21 countries across 6 continents, these drugs have been noted to be more expensive in LMIC compared to high-income countries. In addition, most high-income countries subsidize the cost of these medications through health insurance, while patients spend for these medications from their own pockets in LMICs [32].
The Philippine government’s response to the inaccessibility of essential medications over the past years was the legislation of the Generics Act of 1988, and consequently, the development of the Philippine National Formulary (PNF). The PNF contains the list of essential medicines that can be procured by the government and serves as the basis for PhilHealth reimbursement for public and private health facilities. However, only donepezil (5 mg and 10 mg tablets) and rivastigmine (1.5 mg, 3 mg, and 6 mg capsules) are included in the PNF [33]. Noticeably absent on the PNF are higher doses of donepezil (23 mg tablet), rivastigmine (4.6 mg/24 h patch 5, 9.5 mg/24 h patch 10, 13.3 mg/24 h patch 15), and memantine 20 mg tablet. The Drug Price Reference Index (DPRI) enumerates the ceiling prices of essential medicines for government bidding and procurement. The recommended cost of the following drugs as per the DPRI are USD 0.30 for donepezil 5 mg tablet, USD 0.28 for donepezil 10 mg tablet, and USD 0.77 for memantine 10 mg tablet [34]. However, locally available memantine 10 mg costs USD 0.41–2.54, memantine 20 mg costs USD 4.54, donepezil 5 mg costs USD 0.45–2.03, donepezil 10 mg costs USD 0.68–2.64, and donepezil 23 mg costs USD 2.57 (see Table 3). The wide price range is accounted for by the unavailability of generic versions for memantine 20 mg and donepezil 23 mg. As of June 2022, the minimum wage is USD 10 per day, with the average Filipino family spending 42.6% on food, 12.2% on house rental, 8.2% on utilities, 6.61% on transportation, and only 2.7% on healthcare [21, 35].
Table 3
Cost of available dementia medications in the Philippines* as of May 1, 2023
| Drug | Formulation | Price (USD) |
| Donepezil | Donepezil 5 mg tab | 0.45–2.03 |
| Donepezil 10 mg tab | 0.68–2.64 | |
| Donepezil 23 mg tab | 2.57 | |
| Rivastigmine | Rivastigmine 4.6 mg/24 h patch 5 | 1.95 |
| Rivastigmine 9.5 mg/24 h patch 10 | 2.38 | |
| Rivastigmine 13.3 mg/24 h patch 15 | 2.38 | |
| Memantine | Memantine 10 mg tab | 0.41–2.54 |
| Memantine 20 mg tab | 4.54 |
*Drug prices from Mercury Drug Corporation listed as of May 1, 2023 [36].
In addition to laboratory tests, neuroimaging studies, and medications, other direct medical costs include consultation and hospitalization fees, and caregiver salaries. Direct non-medical costs include nursing home fees, transportation costs to healthcare providers, and costs of home safety modifications. Lastly, indirect costs include the potential earning capacity of unpaid caregivers. In a Filipino community-based study done in 2016, the median direct medical cost was computed at USD 237.40, while direct non-medical cost was at USD 6.57, with the total median indirect cost at USD 229.03. Adding up the annual indirect costs due to unpaid caregiving, the median direct cost was USD 3,650, making the overall total annual per capita cost at USD 3,916.47 [16].
Manpower density
Although the Philippines can educate and develop numerous healthcare professionals, a significant number is lost due to migration to higher income countries. In a 2017 study, the desire to migrate in the next 2 years was noted in 29% of doctors, 51% of nurses, 61% of physical therapists, and 24% of midwives, contributing to the gap in the available manpower especially in rural areas [37]. From 1990 to 2017, a total of 350,361 healthcare professionals have left the country: 95% of which are nurses, 3% are doctors, and 2% are midwives [38]. To stem the tide of migration and ensure a steady supply of doctors, the University of the Philippines College of Medicine started requiring their graduates in 2011 to sign contracts of return service, which entails residing and working in the Philippines for the next 5 years after graduation [39].
At the emergence of dementia symptoms, people and caregivers often turn to their primary care physician for a diagnosis. However, in a local study done in 2000, 64% of primary care physicians expressed their doubt in their ability to diagnose dementia clinically and 92% will opt to refer their patients to specialists such as neurologists, psychiatrists and geriatricians for diagnosis and treatment [40]. There are 664 active fellows of the Philippine Neurological Association, nearly half practice in the National Capital Region (NCR), and a nationwide a ratio of 1 neurologist per 164,156 Filipinos. There are only eleven dementia specialists in the country, and all but one practice in NCR. There are twelve accredited training institutions for Adult Neurology in the Philippines, nine of which are in NCR. Fellowship training in dementia is offered in only three institutions in NCR [41]. There are only ten memory clinic sites in the country mostly staffed by neurologists, with a few clinics under geriatrics and wellness offering similar services. There are two university hospital-based memory centers: University of Santo Tomas Hospital (private) and the Philippine General Hospital (government). The only DOH-funded hospital with a memory center is the National Center for Mental Health; all other memory clinics are in private hospitals [42]. There are only 591 psychiatrists and 140 geriatricians in the country, with a ratio of 1 : 184,433 and 1 : 778,571 respectively (Table 4) [43, 44]. Lastly, there are 133 psychologists (0.1 : 100,000), 516 psychiatric nurses (0.5 : 100,000), and 1,241 mental health social workers (1.2 : 100,000) in the Philippines [45]. These data highlight the lack of healthcare professionals trained in providing care for persons with dementia.
Table 4
Number of neurologists, psychiatrists, and geriatricians in the Philippines*
| Regions | Neurologists | Psychiatrists | Geriatricians | Total |
| TOTAL | 664 | 591 | 140 | 1,395 |
| Ratio to Population | 1 : 164,000 | 1 : 184,000 | 1 : 779,000 | 1 : 78,000 |
| (109 million) |
*According to the PNA, PPA and PCGM [41, 43, 44].
Caregiver training and support
Rooted in the Filipino concept of utang na loob (debt of gratitude) and giving back to one’s parents, co-residence with family members remains to be the most common living arrangement for older Filipinos. The primary caregiver is often a female family member, who is either the patient’s spouse or daughter [46]. However, the majority of caregivers taking care of older adult Filipinos have never received formal training on dementia care [47]. At present, government organizations and specialty medical societies conduct caregiver training programs for both family caregivers and rural health workers on basic dementia care. The Philippine Technical Education and Skills Development Authority offers a caregiving training program which includes provision of care and support to older adults as one of its core competencies; however, there are no specific modules on caring for people with dementia [48]. In 2018, the WHO has created a dementia toolkit for community workers in low-and middle-income countries which aims to assist community workers in identifying people at risk for dementia, providing support to people with dementia and their families, and engaging local communities in dementia-related activities [49].
DISCUSSION
The Philippines has an aging population, with a high dementia prevalence projected to be twice the crude estimated prevalence for the entire Southeast Asia in 2015 [50]. Despite the total number of older persons being large in absolute numbers, the relative numbers remain small, hence they do not receive much attention from government agencies. With projections for these numbers to increase in the next thirty years, the discrepancy in terms of the amount of attention older Filipinos receive also continues to widen. Local research on dementia remains limited, potentially due to paucity of financial and human resources and institutional support. However, the increase in research productivity on dementia in recent years within the region, has encouraged researchers in the country to contribute to local data which could be useful in the development of a more culturally appropriate plan of care [18]. And although the national government has enacted laws and policies which aim to protect and improve the quality of life of older adults, the devolution of management to local government units who do not imbibe the same priorities results in fragmented care.
Cost is one of the major barriers preventing Filipino persons with dementia from getting high quality of care. Despite increasing health expenditures by the government, the Philippines still lags behind its neighboring countries in Southeast Asia in terms of THE per capita; ranking at 6th place behind Singapore, Brunei, Malaysia, Thailand, and Vietnam. The Philippines’ THE equates to only 5.4% of that of Singapore and is only twice that of Myanmar [51]. Efforts by the national government to provide financial risk protection in the form of social insurance programs are inadequate to cover both direct and indirect expenses from the diagnosis of dementia up to long-term home care. The national health insurance is poorly utilized, and at best, only partially covers in-patient admissions, while social insurance in the form of monthly pensions is barely enough to shoulder the cost of dementia medications. This forces persons with dementia and their families to rely on out-of-pocket payments to shoulder their expenses; a formidable challenge when the minimum wage is USD 10 per day and may even be less, depending on the region of residence [35].
This study further emphasizes the disparity between the availability, accessibility, and affordability of diagnostics and therapeutics between public and private health systems. Laboratory and neuroimaging tests typically cost 2–10 times more in private compared to that of government facilities that offer full coverage. More sophisticated tests such as serum amyloid and cranial amyloid positron emission topography scans are only available in private institutions. Consultation fees with private neurologists and dementia specialists roughly cost 2–6 times the minimum wage. In terms of treatment, not all medications for dementia are included in the national formulary, with most pharmacies dispensing branded medications which cost higher than the ceiling prices noted in the DPRI. The costs of dementia care present an economic burden per patient of roughly USD 3,916.47 annually, which is over half of the average family annual income in the Philippines [16].
In terms of manpower, there is a low ratio of specialists to the general population. There are only 0.05 neurologists, 0.04 psychiatrists, and 0.01 geriatricians for every 10,000 population, with more than half practicing in the NCR, and the rest unevenly distributed into the 16 other regions. This is half the ideal doctor-to-patient ratio prescribed by WHO, although there is no set specialist-to-population target ratio. Nursing homes remain underutilized due to the stigma attached to institutionalizing relatives into these homes, erroneously equating it to abandonment and lack of debt of gratitude. Consequently, most older persons are left under the care of untrained caregivers who are left with the responsibility of providing long-term care.
As of 2022, Singapore is the only country in Southeast Asia with a funded National Dementia Strategy ensuring that programs and other improvements regarding dementia care are implemented [52] Currently, dementia is only mentioned as one of the outputs and key indicators in the 2019–2023 Philippines’ Mental Health Strategic Plans, with efforts to integrate a dementia plan in the succeeding plan for 2024–2028 [53, 54]. With the lack of a national dementia plan and limited implementation of the healthy and productive aging program [55], non-government organizations have tried to fill the gaps by embarking on numerous programs in accordance with the WHO global action plan on dementia [2]. These programs range from yearly dementia awareness campaigns culminating in World Alzheimer’s Month every September, lay fora, prevention and risk reduction infographics and materials, requests for further government subsidy and insurance coverage, running support groups for families caring for persons with dementia, ensuring availability of free dementia screening tools, and translating the WHO iSupport Manual for Dementia for free download [56–58]. In addition, these organizations leverage their network and resources to liaise the academe, clinicians, families, and persons living with dementia to relevant clinical trials that may benefit them. These organizations like the ADAP, DSP, PCGM, and PSGG to name a few, also constitute the stakeholders who participate in consultative workshops initiated by the government for programs or laws relevant to providing care for persons with dementia.
Despite the extensive search done using international and local databases as well as gray literature, this review may have missed relevant published and unpublished literature. Other relevant articles published in the non-English or non-Filipino language may also have been missed. Lastly, given the intrinsic nature of scoping reviews, the lack of critical appraisal of included studies can also be a potential source of bias.
Conclusion and future perspectives
This scoping review explores the current status and gaps in dementia care in the Philippines. Our findings have been consistent with the findings of earlier reviews on the status of various neurological disorders in the country. A multi-pronged approach on enhancing research on nationwide dementia epidemiology, improving government financial support spanning the different levels of dementia care, improving access to dementia diagnostics and medications as well as increasing the number of dedicated manpower for dementia would be important in filling the gaps in dementia care in the Philippines. Acknowledging these gaps and challenges is a good initial step in developing plans and health policies to improve the quality of life of Filipinos with dementia but eventually, a national dementia plan will be necessary for systematic and cost effective delivery of care.
ACKNOWLEDGMENTS
The authors have no acknowledgements to report.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available within the article.
REFERENCES
[1] | World Health Organization (2020) Dementia.https://www.who.int/news-room/fact-sheets/detail/dementiaLast updated March 15, 2023, Accessed on September 6, 2023. |
[2] | World Health Organization (2017) Global action plan on the public health response to dementia 2017-2025. |
[3] | National QuickStat for 2022 https://psa.gov.ph/statistics/quickstat/nationalLast updated 2022, Accessed on August 23, 2022. |
[4] | Abalos JB ((2020) ) Older persons in the Philippines: A demographic,socioeconomic and health profile. Ageing Int 45: , 230–254. |
[5] | Dayrit M , Lagrada L , Picazo O , Pons M , Villaverde M (2018) The Philippines health system review. In Health Systems in Transition, PatcharanarumolW,Tangcharoensathien V, eds. WHO Press, Geneva, p. 1–316. |
[6] | Department of Health (2017) National Objectives for Health Philippines 2017–2022. |
[7] | Alliance for Improving Health Outcomes. The Philippine Health System at a glance,https://www.aiho.org.ph/2017/05/08/philippine-health-system/Last updated 2017, Accessed on August 2, 2022. |
[8] | Ocampo FF , Espiritu AI , Jamora RDG ((2022) ) Current status and challenges in the care of patients with bacterial meningitis in the Philippines: A scoping review. Trop Med Int Health 27: , 38–48. |
[9] | Pagaling GT , Turalde CWR , Jamora RDG ((2022) ) Autoimmune encephalitis in the Philippines: A scoping review on the treatment gaps, challenges, and current state of care. Front Neurol 13: , 788309. |
[10] | Mondia MWL , Espiritu AI , Batara JMF , Jamora RDG ((2021) ) Neuro-oncology in the Philippines: A scoping review on the state of medical practice, deterrents to care and therapeutic gaps. Ecancermedicalscience 15: , 1238. |
[11] | Moalong KMC , Espiritu AI , Fernandez MLL , Jamora RDG ((2021) ) Treatment gaps and challenges in epilepsy care in the Philippines. Epilepsy Behav 115: , 107491. |
[12] | Ignacio KHD , Espiritu AI , Jamora RDG ((2020) ) The current status and challenges in multiple sclerosis management in the Philippines. Mult Scler Relat Disord 46: , 102510. |
[13] | Jamora RDG , Miyasaki JM ((2017) ) Treatment gaps in Parkinson’s disease care in the Philippines. Neurodegener Dis Manag 7: , 245–251. |
[14] | Tricco AC , Lillie E , Zarin W , O’Brien KK , Colquhoun H , Levac D , Moher D , Peters MDJ , Horsley T , Weeks L , Hempel S , Akl EA , Chang C , McGowan J , Stewart L , Hartling L , Aldcroft A , Wilson MG , Garritty C , Lewin S , Godfrey CM , MacDonald MT , Langlois E V. , Soares-Weiser K , Moriarty J , Clifford T , Tunçalp Ö , Straus SE ((2018) ) PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann Intern Med 169: , 467–473. |
[15] | Dominguez J , Fe De Guzman M , Reandelar M , Thi Phung TK ((2018) ) Prevalence of dementia and associated risk factors:A population-based study in the Philippines. J Alzheimers Dis 63: , 1065–1073. |
[16] | Dominguez J , Jiloca L , Fowler KC , De Guzman MF , Dominguez-Awao JK , Natividad B , Domingo J , Dominguez JD , Reandelar M , Ligsay A , Yu JR , Aichele S , Phung TKT ((2021) ) Dementia incidence, burden and cost ofcare: A Filipino community-based study.. Front Public Health 9: , 628700. |
[17] | The Philippine Neurological Association One Database-Dementia (PNA1DB-Dem),https://clinicaltrials.gov/study/NCT05484960Last updated August 2, 2022, Accessed on August 10. |
[18] | Sy MCC , Espiritu AI , Sy MSC , Jamora RDG , Anlacan VMM ((2020) ) Dementia research productivity and associations with socioeconomic factors and burden of disease in Southeast Asia. J Alzheimers Dis 76: , 1151–1160. |
[19] | Total health expenditure per capita in Southeast Asia 2019 (in U.S. dollars), by country, Last updated March 3, 2022, Accessed on August 2, 2022. |
[20] | Philippine Statistics Authority (2021) Health Spending Registered 12.6 Percent Growth, Share of Health to Economy Went Up to 5.6 Percent in 2020.https://www.psa.gov.ph/content/health-spending-registered-126-percent-growth-share-health-economy-went-56-percent-2020. |
[21] | Philippine Statistics Authority (2018) 2018 Family Income and Expenditure Survey.https://psada.psa.gov.ph/catalog/FIES/about. |
[22] | Philippine Health Insurance Corporation (2014) Agency’s mandate and functions,https://www.philhealth.gov.ph/about_us/mandate.phpLast updated 2014, Accessed on September 6, 2022. |
[23] | The LAWPHiL Project (2014) Republic Act No. 10645,https://lawphil.net/statutes/repacts/ra2014/ra_10645_2014.htmlLast updated November 5, 2014, Accessed September 6, 2022. |
[24] | Philippine Health Insurance Corporation (2017) List of Medical Case Rates.https://www.philhealth.gov.ph/circulars/2017/annexes/0019/AnnexA-MedicalCaseRates.pdfLast updated February 2017, Accessed May 1, 2023. |
[25] | Mina CD , Cacnio FCQ (2019) Are Filipino senior citizens financially protected?: Evidence from Consumer Finance Survey.https://www.isi-next.org/abstracts/submission/793/view/Last updated 2022, Accessed September 6, 2022. |
[26] | Fourteenth Congress of the Republic of the Philippines (2003) Senate S.B. No. 2154.https://legacy.senate.gov.ph/lis/bill_res.aspx?congress=14&q=SBN-2154Accessed September 6, 2022. |
[27] | Department of Health (2017) Policy Guidelines on the Standards of Care for Older Persons in All Healthcare Settings,https://extranet.who.int/mindbank/item/7178Last updated January 30, 2017, Accessed September 6, 2022. |
[28] | Official Gazette (2018) Republic Act No. 11350.https://www.officialgazette.gov.ph/2019/07/25/republic-act-no-11350/Last updated July 25, 2019, Accessed September 6, 2022. |
[29] | Pink J , O’Brien J , Robinson L , Longson D ((2018) ) Dementia: Assessment, management and support: Summary of updated NICE guidance. BMJ (Online) 361: , k2438. |
[30] | Philippine General Hospital Radish (Computerized Registry of Admissions and Discharges),http://172.16.187.118/radishLast updated April 2023, Accessed on May 1, 2023. |
[31] | St. Luke’s Medical Center,https://www.stlukes.com.phLast updated April 2023, Accessed on May 1, 2023. |
[32] | Suh G-H , Wimo A , Gauthier S , O’Connor D , Ikeda M , Homma A , Dominguez J , Yang B-M ((2009) ) International price comparisons of Alzheimer’s drugs: A way to close the affordability gap. Int Psychogeriatr 21: , 1116–1126. |
[33] | The Philippine National Formulary,https://pharma.doh.gov.ph/the-philippine-national-formularyLast updated 2019, Accessed on September 6, 2022. |
[34] | Drug Price Reference Index (10th edition),https://dpri.doh.gov.phLast updated August 23, 2022, Accessed on September 6, 2022. |
[35] | Department of Labor and Employment NationalWages and Productivity Commission (2022) National Capital Region,https://nwpc.dole.gov.ph/regionandwages/national-capital-regionLast updated 2022, Accessed on September 6, 2022. |
[36] | Mercury Drug Corporation,https://www.mercurydrug.comLast updated 2023, Accessed on May 1, 2023. |
[37] | Castro-Palaganas E , Spitzer DL , Kabamalan MMM , Sanchez MC , Caricativo R , Runnels V , Labontć R , Murphy GT , Bourgeault IL ((2017) ) An examination of the causes, consequences, and policy responses to the migration of highly trained health personnel from the Philippines: The high cost of living/leaving –a mixed method study. Hum Resour Health 15: , 1–14. |
[38] | Robredo JP , Ong B , Eala MA , Naguit RJ ((2022) ) Outmigration and unequal distribution of Filipino physicians and nurses: An urgent call for investment in health human resource and systemic reform. Lancet Reg Health West Pac 25: , 100512. |
[39] | University of the Philippines Manila College of Medicine (2022) Return Service Obligation Program & Regionalization Program.https://cm.upm.edu.ph/p/unified-handbook-rsop-rp/Last updated 2022, Accessed on February 19, 2023. |
[40] | Capino P , Ramos M Jr. , Gatchalian E ((2000) ) Beliefs and attitudes of general practitioners on Alzheimer’s disease dementia. Philipp J Intern Med 38: , 183–187. |
[41] | Philippine Neurological Association (2022) PNA Fellows,https://www.philippineneurologicalassociation.com/pna-fellowsLast updated 2022, Accessed on September 6, 2022. |
[42] | Dementia Society Philippines (2021) Memory Clinic Sites,https://www.dementia.org.ph/memory-clinic-sitesLast updated 2021, Accessed on September 6, 2022. |
[43] | Philippine Psychiatric Association (2022) Philippine Psychiatric Association: Search a Psychiatrist,https://philippinepsychiatricassociation.org/psychiatristLast updated 2023, Accessed on October 8, 2023. |
[44] | Senate of the Philippines, 19th Congress (2019) Angara: PH needs more medical students to specialize in treating elderly,https://legacy.senate.gov.ph/press_release/2019/0505_angara1.aspLast updated 2019, Accessed on October 8, 2023. |
[45] | World Health Organization, Department of Health (2020) Philippines WHO Special Initiative for Mental Health Situational Assessment, Last updated March 2020, Accessed on February 19, 2023. |
[46] | Cruz GT , Cruz CJP , Saito Y eds. (2019) Ageing and Health in the Philippines, Economic Research Institute for ASEAN and East Asia (ERIA), Jakarta. |
[47] | Dela Vega SF , Cordero CP , Palapar LA , Garcia AP , Agapito JD ((2018) ) Mixed-methods research revealed the need for dementia services and Human Resource Master Plan in an aging Philippines. J Clin Epidemiol 102: , 115–122. |
[48] | Technical Education and Skills Development Authority (2020) Training Regulations CaregivingNCII, Last updated 2020, Accessed on September 6, 2022. |
[49] | World Health Organization Regional Office for theWestern Pacific (2018) Dementia Toolkit for Community Workers in Low- and Middle-Income Countries: Guide for communitybased management and care of people with dementia, World Health Organization Regional Office for theWestern Pacific, Manila. |
[50] | Prince MJ , Wimo A , Guerchet MM , Ali GC , Wu Y-T , Prina M (2015)World Alzheimer Report 2015. The Global Impact of Dementia: An analysis of prevalence, incidence, cost and trends. Alzheimer&s Disease International, London. |
[51] | TheGlobalEconomy.com (2020) Health spending per capita in South East Asia,https://www.theglobaleconomy.com/rankings/health_spending_per_capita/South-East-AsiaLast updated 2020, Accessed on May 28, 2023. |
[52] | World Health Organization (2023) Global Dementia Observatory –Dementia Plan,https://www.who.int/data/gho/data/themes/global-dementia-observatory-gdoLast updated 2023, Accessed on May 28, 2023. |
[53] | Philippine Council for Mental Health (2019) Mental Health Strategic Plan, World Health Organization Philippines, Manila. |
[54] | Electronic Freedom of Information –Request for National Dementia Plan of the Philippines #DOH-454113927358,https://www.foi.gov.ph/requestsLast updated May 4, 2023, Accessed on October 11, 2023 |
[55] | Department of Health (2023) Healthy and Productive Ageing Program,https://doh.gov.ph/health-programs/healthy-and-productive-ageing-programLast updated 2023, Accessed on May 28, 2023. |
[56] | Alzheimer’s Disease International (2022) World Alzheimer’s Monthhttps://www.alzint.org/get-involved/world-alzheimers-monthLast updated 2023, Accessed on May 28, 2023. |
[57] | Dementia Society of the Philippines (2019) Dementia Screening Tools,https://www.dementia.org.ph/dementia-screening-toolsLast updated 2019, Accessed on May 28, 2023. |
[58] | Alzheimer’s Disease Association of the Philippines (2022) iSupport Para Sa Dementia: Pagsasanay at gabay para sa mga tagapag-alaga ng taong may dementia, Alzheimer’s Disease Association of the Philippines, Manila. |


