
Development of a Cognitive Composite for Preclinical Alzheimer’s Disease in Korean Older Adults
Abstract
Background:
As tracking subtle cognitive declines in the preclinical stage of Alzheimer’s disease (AD) is difficult with traditional individual outcome measures, need for cognitive composite for preclinical AD is widely recognized.
Objective:
We aimed to develop culturally appropriate cognitive composite that sensitively identifies subtle cognitive decline of preclinical AD in Korean older adults.
Methods:
A total 225 cognitively normal elderly individuals from the Korean Brain Aging Study for the Early Diagnosis and Prediction of Alzheimer’s Disease, were included. Tests of episodic memory, orientation, and executive function were carefully selected through review of previously established composites. Three candidate composites including Consortium to Establish a Registry for Alzheimer’s Disease Word list recall (WLR), Logical memory (LM) II, and Mini-Mental status examination (MMSE) in common, and Letter fluency test (LF), category fluency test, or Stroop color and word test, were selected.
Results:
Student t-tests demonstrated that only the composite composed of WLR, LM II, MMSE, and LF (Composite 1) showed a significant difference in score decline over two-year follow-up period between Aβ positive and negative group (p = 0.03). Linear mixed model analyses also showed that the Aβ x time interaction effect was significant only for Composite 1 (p = 0.025). Based on the results, Composite 1 was chosen as the final cognitive composite for preclinical Alzheimer’s disease (CPAD).
Conclusions:
CPAD can be used to assess subtle cognitive decline of preclinical AD in clinical research settings, especially in Korean older adults. It also may be used for monitoring progression or treatment benefits in clinical practices.
INTRODUCTION
Preclinical Alzheimer’s disease (AD) describes a disease state without noticeable cognitive impairment but with cerebral accumulation of pathological amyloid-β (Aβ) [1, 2]. As in vivo neuroimaging and cerebrospinal fluid biomarkers for cerebral Aβ deposition are available, diagnosis and research of preclinical AD in living human have become possible.
Measuring subtle cognitive changes in the preclinical AD is important for clinical research and even crucial for drug trials targeting preclinical AD [3]. In this context, the Alzheimer Disease Cooperative Study Preclinical Alzheimer Cognitive Composite (ADCS-PACC) [4] was developed to identify Aβ-related cognitive decline in the preclinical phase of AD in 2014. The ADCS-PACC includes cognitive tests that assess episodic memory, executive function, and orientation, and it has been used as a primary outcome measure in Anti-Amyloid Treatment in Asymptomatic Alzheimer’s study (A4 study) [5]. Several other cognitive composites, such as AD Composite Scores [6], the z-scores of Attention, Verbal fluency, and Episodic memory for Nondemented older adults composite [7], and the Alzheimer’s Prevention Initiative Composite Cognitive Test (APCC) [8], have also been developed to evaluate cognitive change in preclinical AD. While the cognitive composites differ in the tests that they are composed of, the common tests include that of episodic memory, orientation, and executive function in common. Tests for episodic memory, executive function, or orientation are known to be sensitive to identifying cognitive change in the early stage of AD [9–11].
While the previously developed cognitive composites demonstrated the ability to sensitively evaluate subtle cognitive decline in preclinical AD, all of them were developed by using the cohort data that mainly included highly educated non-Hispanic white individuals. Cultural and linguistic background can be a major factor for result and interpretation of cognitive tests [12, 13]. Education levels, which strongly affect the results of most cognitive tests, are also considerably different in Korean older adults compared to western ones. The range of educational levels among Korean old individuals is wider than that of North Americans [14]. The previously developed composites did not consider these cultural, linguistic differences, and local normative data, and it is unknown whether they can be adapted to populations of various cultural backgrounds. We aimed to determine whether the constructs of previously developed composites, that is, tests of episodic memory, orientation, and executive function are valid in Korean individuals despite of these differences in cultural and linguistic backgrounds, and confirm a cognitive composite that can sensitively assess the subtle cognitive decline of preclinical AD in Korean older adults.
METHODS
Participants
This study included cognitively normal subjects from the Korean Brain Aging Study for Early Diagnosis and Prediction of Alzheimer’s Disease (KBASE) [15], which started in 2014.
A total 225 cognitively normal (CN) individuals included in the analyses met the following criteria: 1) age between 55 and 90 at baseline, 2) Clinical Dementia Rating [16] score of 0, 3) no diagnosis of mild cognitive impairment (MCI) or dementia at baseline, 4) completed baseline and 2-year follow-up evaluation including clinical assessments, comprehensive neuropsychological tests, and amyloid positron emission tomography (PET) evaluation at baseline. The exclusion criteria were as follows: 1) presence of a major psychiatric illness including schizophrenia, major depressive disorder, bipolar disorder, and alcohol-related disorders; 2) significant neurological or general medical conditions or diseases that could affect mental function; 3) illiteracy; 4) the presence of significant visual/hearing difficulties and/or severe communication or behavioral problems that would make clinical examinations or brain scans difficult; and 5) taking an investigational drug. The study protocol was approved by the institutional review boards of Seoul National University Hospital (C-1401-027-547) and SNU-SMG Boramae Medical Center (26-2015-60), Seoul, South Korea, and the study was conducted in accordance with the recommendations of the current version of the Declaration of Helsinki. All participants gave written informed consent.
Clinical, neuropsychological, and laboratory assessment
All participants underwent comprehensive clinical assessments by trained board-certified psychiatrists based on the KBASE clinical assessment protocol [15] which incorporated the Koran Version of Consortium to Establish a Registry for Alzheimer’s Disease (CERAD-K) clinical assessment [17] at baseline and at 2-year follow-up. All participants were also given a comprehensive neuropsychological assessment battery, administered by trained clinical neuropsychologist or psychometrists according to the standardized protocol incorporating the CERAD-K neuropsychological battery [14]. The neuropsychological tests included in the KBASE protocol are listed in Table 2.
Table 2
Cognitive tests in the KBASE cohort study
| Cognitive test | Domain |
| Category fluency test (Animal) | Language/ Executive |
| function | |
| Boston Naming Test | Language |
| Korean Adult Reading Test | Language |
| MMSE-KC | Cognitive Status |
| CERAD Word List Memory | Episodic memory |
| CERAD Word List Recall | Episodic memory |
| CERAD Word List Recognition | Episodic memory |
| WMS-K-IV Logical Memory I | Episodic memory |
| WMS-K-IV Logical Memory II | Episodic memory |
| WAIS-IV-K block design | Visuospatial function |
| Clock Drawing Test (CLOX1, CLOX2) | Visuospatial function |
| Constructional Praxis | Visuospatial function |
| Constructional Praxis recall | Visuospatial memory |
| Rey Complex Figure Test | Visuospatial memory |
| Stroop Test (Word, Color, Color-word) | Executive function |
| Letter fluency test | Executive function |
| Trail Making Test (A, B) | Attention |
| Digit Span | Attention |
KBASE, The Korean Brain Aging Study for the Early Diagnosis and Prediction of Alzheimer’s disease; MMSE-KC, Mini-Mental Status Examination in the Korean Version of the CERAD Assessment Packet; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; WMS-K-IV, Korean Wechsler Memory Scale-Fourth Edition; WAIS-IV-K, Wechsler Adult Intelligence Scale-Fourth edition Korean version.
Measurement of cerebral Aβ deposition
Details were described previously [15]. Briefly, participants underwent simultaneous three-dimensional (3D) [11C] Pittsburgh compound B (PiB) PET (PiB-PET) and 3D T1-weighted MRI using the 3.0T PET-MR scanner (mMR Biograph, Siemens) according to the manufacturer’s guidelines. The automatic anatomic labeling algorithm and a region-combining method [18] were used to determine regions of interest (ROIs), to characterize the PiB retention levels in the frontal, lateral parietal, posterior cingulate/precuneus, and lateral temporal regions. The standardized uptake value ratio (SUVr) values for each ROI were generated by dividing the mean value for all voxels within each ROI by the mean cerebellar uptake value in the same image. Each participant was classified as Aβ positive (Aβ+) if the SUVr value was > 1.21, and Aβ negative (Aβ-) if SUVr was ≤1.21 [19].
Selection of candidate cognitive composites
Most of the previously developed cognitive composites for preclinical AD [4, 6, 8, 20–22] include tests covering episodic memory, orientation, and executive function, which are sensitive to identify cognitive change in the early stage of AD (Table 3) [9–11]. Based on the previously developed composites, therefore, we first selected cognitive tests for the three cognitive domains, with consideration of the comparability to the previously developed ones, the PACC in particular [4]. The following tests were included in the composite of the current study: (a) CERAD word list recall (WLR) [17] and delayed recall score of the WMS-K-IV Logical Memory II (LM-DR) [23] were selected as the candidate tests for episodic memory, (b) Mini-Mental State Examination (MMSE) in the Korean version of the CERAD assessment packet [14] for cognitive status, and (c) the fluency tests (both FAS (LF) and Animals (CF)) [24] and Stroop Color and Word test (Stroop CW) [25] for executive function. After the selection of the tests for the cognitive domains, three different candidate composites were derived based on different combination of the tests. Each candidate composite consists of 4 cognitive tests, including two tests from the episodic memory domain, a test from executive function, and MMSE for cognitive status. The candidate composites examined in the study are presented in Table 4. Z-scores based on age-, sex-, education-adjusted normative data were used in the analyses [14]. Of note, no weights were applied.
Table 3
Assessments in the previously developed cognitive composites for preclinical AD
| Cognitive Composites | Cognitive domains | |||
| Memory | Orientation | Executive function | Others | |
| ADCS-PACC [4] | FCSRT, LM-DR | MMSE total | DSST | |
| modified-PACC [21] | ADAS-cog, LM-DR | MMSE total | TMT-B | |
| PACC5 [20] | FCSRT LM-DR | MMSE total | DSST CF | |
| ADCOMS [6] | 4 items of ADAS-cog | 2 items of MMSE | CDR-SB | |
| API ADAD composite [22] | CERAD WLR | MMSE Orientation to time | CERAD BNT CERAD constructional praxis Raven’s Progressive Matrices | |
| APCC [8] | CERAD WLR, LM-DR | Orientation items of MMSE Judgement of Line Orientation | Symbol digit modalities | Raven’s Progressive Matrices |
| ZAVEN [7] | CVLT-II total recall, LM-DR | DSST Letter fluency | ||
ADCS-PACC, the Alzheimer Disease Cooperative Study Preclinical Alzheimer Cognitive Composite; ADCOMS, AD Composite Scores; API, the Alzheimer’s Prevention Initiative; APCC, the Alzheimer’s Prevention Initiative Composite Cognitive Test; ZAVEN, the Z-scores of Attention, Verbal fluency, and Episodic memory for Nondemented older adults composite; FCSRT, Free and Cued Selective Reminding Test; LM-DR, Logical memory delayed recall on Wechsler Memory Scale; ADAS-cog, the Alzheimer’s Disease Assessment Scale–Cognitive subscale; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; WLR, Word List Recall, CVLT-II, the California Verbal Learning Test, Second Edition; MMSE, Mini-Mental Status Examination; DSST, Digit Symbol Substitution Test; CF, Category fluency test; TMT-B, Trail Making Test-B; CDR-SB, the Clinical Dementia Rating-sum of boxes; BNT, Boston Naming Test.
Table 4
Components of the three candidate composites
| Composite | Cognitive tests included in each candidate composite | ||||
| Composite 1 | CERAD WLR | LM-DR | MMSE | LF | |
| Composite 2 | CERAD WLR | LM-DR | MMSE | CF | |
| Composite 3 | CERAD WLR | LM-DR | MMSE | Stroop CW | |
MMSE, Mini-Mental Status Examination; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; WLR, Word List Recall; LM-DR, delayed recall score of the WMS-K-IV Logical Memory II; LF, Letter fluency Test; CF, Category fluency Test; Stroop CW, Stroop Color and Word test.
Determination of the final cognitive composite for preclinical AD
To determine the final cognitive composite for preclinical AD (CPAD), (a) we first compared baseline and 2-year follow-up scores of each of the three candidate composites between the Aβ+ and Aβ- groups. CPAD score changes over two years were also compared between the groups using student t-test; and (b) we analyzed the longitudinal effect of Aβ positivity on the score change over two years for each candidate composite using linear mixed models. The models included each candidate composite score at baseline or 2-year follow-up as a dependent variable, and included Aβ positivity, interval between the tests (Time), and Aβ positivity × Time interaction term as independent variables. In addition, the slope between the visits was examined. We assumed random effects as random intercepts for each individual only. The reference group was the Aβ negative group. Aβ positivity was based on baseline visit. To ensure the robustness of our results, we implemented a bootstrap analysis for each composite model. This analysis was performed using the R statistical software (version 4.0.2, R Development Core Team, 2020) and leveraged the “lme4” and “boot” packages. We conducted 1,000 bootstrap iterations to derive stable estimates and confidence intervals. The best composite was chosen based on the results of the analysis (a) and (b)—the composite that showed greater decline of the score in Aβ positive group compared to Aβ negative group.
Validation of the CPAD
We additionally validated the CPAD, the finally selected composite, by comparing it between the groups divided based on clinical progression (i.e., progressed versus non-progressed) using linear mixed model analysis. Clinically progressed group included those who progressed to MCI or dementia from CN. Individuals who remain clinically normal were included in non-progressed group. The model included CPAD scores of each visit as a dependent variable, and included clinical progression status, time, and clinical progression x time interaction term as independent variables. We assumed random effects as random intercepts for each individual only. The reference group was the non-progressed group.
RESULTS
Baseline characteristics
Baseline characteristics for each of the groups by Aβ status are described in Table 1. Aβ+ group is significantly older than Aβ- group. There are no differences between the groups in sex or education. Aβ+ group has significantly higher percentages of APOE ɛ4 carriers, and those who progressed to MCI or AD dementia at the 2-year follow-up. The baseline cognitive scores were not significantly different between Aβ groups.
Table 1
Baseline Characteristics of Participants by Aβ status
| Aβ-negative | Aβ-positive | All | ||
| participants | participants | participants | ||
| Characteristics | (n = 182) | (n = 43) | (n = 225) | pa |
| Age, y | 67.7 (8.0) | 73.7 (5.9) | 68.9 (8.0) | < 0.001*** |
| Sex, n (%) | ||||
| Female | 93 (51) | 22 (51) | 115 (51) | 0.994 |
| Male | 89 (49) | 21 (49) | 110 (49) | |
| Education, y | 11.9 (4.9) | 12.8 (4.0) | 12.1 (4.7) | 0.175 |
| APOE ɛ4 status, n (%) | ||||
| Non-carriers | 158 (87) | 28 (65) | 186 (83) | 0.001** |
| Carriers | 24 (13) | 15 (35) | 39 (17) | |
| Progressors, n (%) | ||||
| Progressors | 10 (5) | 7 (16) | 17 (8) | 0.016 |
| Non-progressors | 172 (95) | 36 (84) | 208 (92) | |
| MMSE scoreb | 0.29 (0.87) | 0.27 (0.91) | 0.28 (0.87) | 0.895 |
| CERAD WLR scoreb | 0.46 (0.80) | 0.21 (0.87) | 0.41 (0.82) | 0.083 |
| LM-DR scoreb | 0.36 (0.94) | 0.20 (0.84) | 0.32 (0.92) | 0.276 |
| CF scoreb | 0.34 (1.20) | 0.19 (1.01) | 0.10 (0.99) | 0.410 |
| LF scoreb | 0.05 (0.94) | 0.30 (1.16) | 0.31 (1.17) | 0.220 |
| Stroop CW scoreb | 0.28 (0.96) | 0.02 (0.90) | 0.23 (0.95) | 0.097 |
Aβ, amyloid-β; MMSE, Mini-Mental Status Examination; CERAD, Consortium to Establish a Registry for Alzheimer’s Disease; WLR, Word List Recall; LM-DR, delayed recall score of the WMS-K-IV Logical Memory II; CF, Category fluency Test; LF, Letter fluency Test; Stroop CW, Stroop Color and Word test; All values are given as mean (SD) values or number (%) of participants. aDetermined by use of Student T-test for continuous variables and the Pearson χ2 -test for categorical variables. bThe values are z-scores using normative data for Korean elderly by age, sex, and education. (*p < 0.05, **p < 0.01, ***p < 0.001).
Difference of three candidate composites at each time point between Aβ+ and Aβ- group
All three candidate composites did not significantly differ between Aβ+ and Aβ- groups at baseline (Table 5), whereas all three candidate composites showed significant differences by Aβ status at 2-year follow-up (Composite 1, p = 0.03; Composite 2, p = 0.02; Composite 3, p = 0.01).
Table 5
Composite scores of Aβ-positive and Aβ-negative groups at baseline, 2-year follow-up, and differences of two time points in each candidate composite
| Baseline | 2 year f/u | Difference | |||||||
| Aβ- | Aβ+ | pa | Aβ- | Aβ+ | pa | Aβ- | Aβ+ | pa | |
| Composite 1 | 0.30 (0.57) | 0.24 (0.62) | 0.600 | 0.31 (0.65) | 0.05 (0.68) | 0.030* | 0.01 (0.54) | –0.21 (0.56) | 0.030* |
| Composite 2 | 0.37 (0.60) | 0.22 (0.62) | 0.140 | 0.35 (0.64) | 0.08 (0.66) | 0.020* | –0.01 (0.50) | –0.12 (0.52) | 0.240 |
| Composite 3 | 0.36 (0.56) | 0.17 (0.60) | 0.070 | 0.50 (0.68) | 0.19 (0.68) | 0.010* | 0.16 (0.50) | 0.03 (0.51) | 0.150 |
Data are shown as mean (SD). a Determined by use of Student t-test. *p < 0.05.
Effect of Aβ positivity on the longitudinal change of candidate composites
Student t-tests demonstrated that only the composite 1 showed a significant difference in the score change over two years between Aβ groups (Composite 1, p = 0.03; Composite 2, p = 0.24; Composite 3, p = 0.15) (Table 5). Linear mixed model analyses showed that the fixed effect of the interaction of time and Aβ status was significant only for Composite 1 (p = 0.025, 95% confidence interval (CI) [–0.397, –0.028]) but not statistically significant in Composites 2 and 3 (p = 0.216, 95% CI[–0.280, 0.063).; p = 0.106, 95% CI[–0.264, 0.024], respectively). The fixed effect of time reflecting the reference group (Aβ negative) was significant for Composite 3 (p < 0.001, 95% CI[0.071, 0.198]) but not significant for Composite 1 and 2 (p = 0.773, 95% CI[–0.068, 0.091).; p = 0.633, 95% CI[–0.092, 0.056], respectively) (Table 6 and Fig. 1). In the bootstrap analysis, Composite 1 and 2 showed results comparable to those of the original models. The fixed effect of the interaction of time and Aβ status remained significant for Composite 1 (95% CI [–0.350, –0.070]) but not for Composite 2 (95% CI [–0.249, 0.026]). In contrast, the fixed effect of the interaction of time and Aβ status for Composite 3 was significant in the bootstrap analysis (95% CI [–0.229, –0.014]), whereas not in the original model (Table 7).
Fig. 1
The results of the linear mixed models of time and Aβ interaction for each candidate composites. (A) Composite 1. (B) Composite 2. (C) Composite 3. The bars indicate 95% confidence intervals. The fixed effect of the interaction of time and Aβ status was significant only for Composite 1(A).
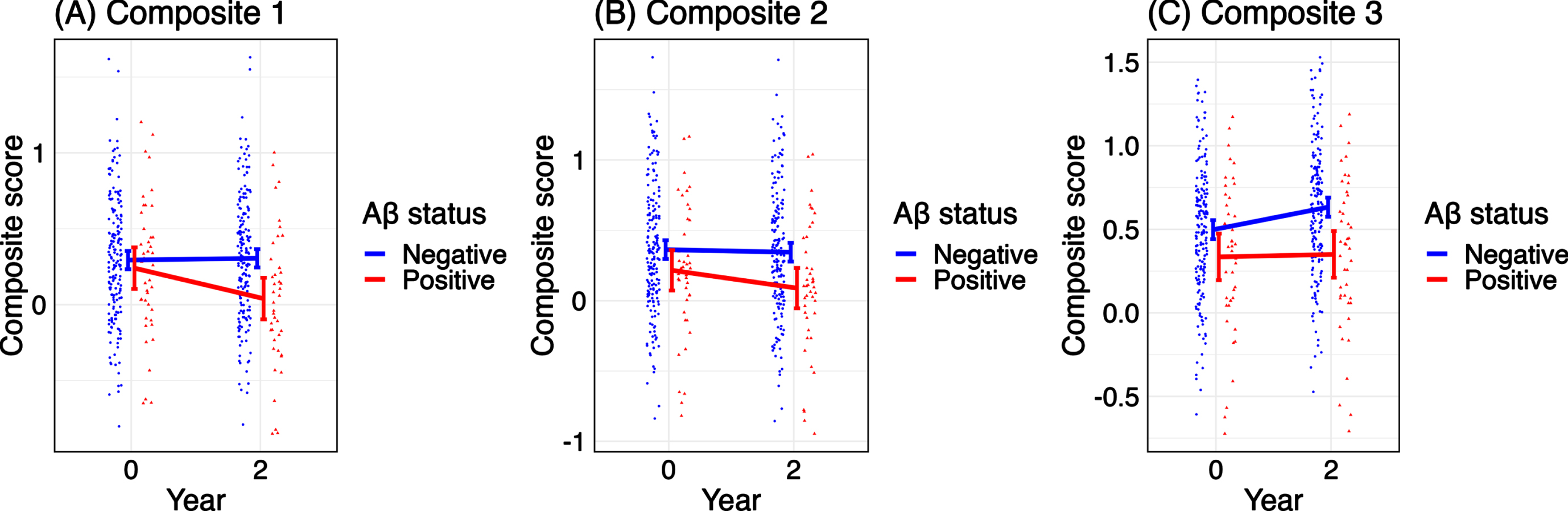
Table 6
The results of linear mixed model analysis of time and interaction between time and Aβ status for 3 candidate composites
| Variables | Composite 1 | Composite 2 | Composite 3 | |||
| Estimate | p | Estimate | p | Estimate | p | |
| [95% CI] | [95% CI] | [95% CI] | ||||
| Time | 0.011 [–0.068, 0.091] | 0.773 | –0.018 [–0.092, 0.056] | 0.633 | 0.135 [0.071, 0.198] | <0.001*** |
| Aβ status (Aβ+) | –0.053 [–0.257, 0.151] | 0.611 | –0.146 [–0.354, 0.061] | 0.168 | –0.163 [–0.342, 0.016] | 0.077 |
| Time x Aβ status | –0.212 [–0.397, –0.028] | 0.025* | –0.108 [–0.280, 0.063] | 0.216 | –0.120 [–0.264, 0.024] | 0.106 |
| (Intercept) | 0.293 [0.203, 0.383] | <0.001*** | 0.363 [0.271, 0.454] | <0.001*** | 0.497 [0.418, 0.577] | <0.001*** |
CI, confidence interval. The reference group was Aβ negative group. Composite 1 only showed a significant p-value of both Time and Time x Aβ status interaction. (*p < 0.05, **p < 0.01, ***p < 0.001).
Table 7
The Bootstrap results of linear mixed model analysis of time and interaction between time and Aβ status for 3 candidate composites
| Variables | Composite 1 | Composite 2 | Composite 3 | |||
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | |
| Time | –0.010 | –0.050, 0.077 | –0.019 | –0.075, 0.040 | 0.134 | 0.084, 0.185 |
| Aβ status (Aβ+) | –0.056 | –0.214, 0.095 | –0.148 | –0.302, 0.006 | –0.165 | –0.298, –0.035 |
| Time x Aβ status | –0.212 | –0.350, –0.070 | –0.110 | –0.249, 0.026 | –0.121 | –0.229, –0.014 |
| (Intercept) | 0.294 | 0.209, 0.667 | 0.364 | 0.293, 0.433 | 0.498 | 0.169, 0.493 |
The reference group was Aβ negative group.
Determination of the final CPAD
Given the abovementioned findings, Composite 1 was selected as the final composite that best identifies the amyloid–related subtle cognitive decline in preclinical AD. The final selected composite is:
Final composite (CPAD) score = CERAD WLR + LM-DR + MMSE total + LF
Relationship between clinical progression and CPAD score
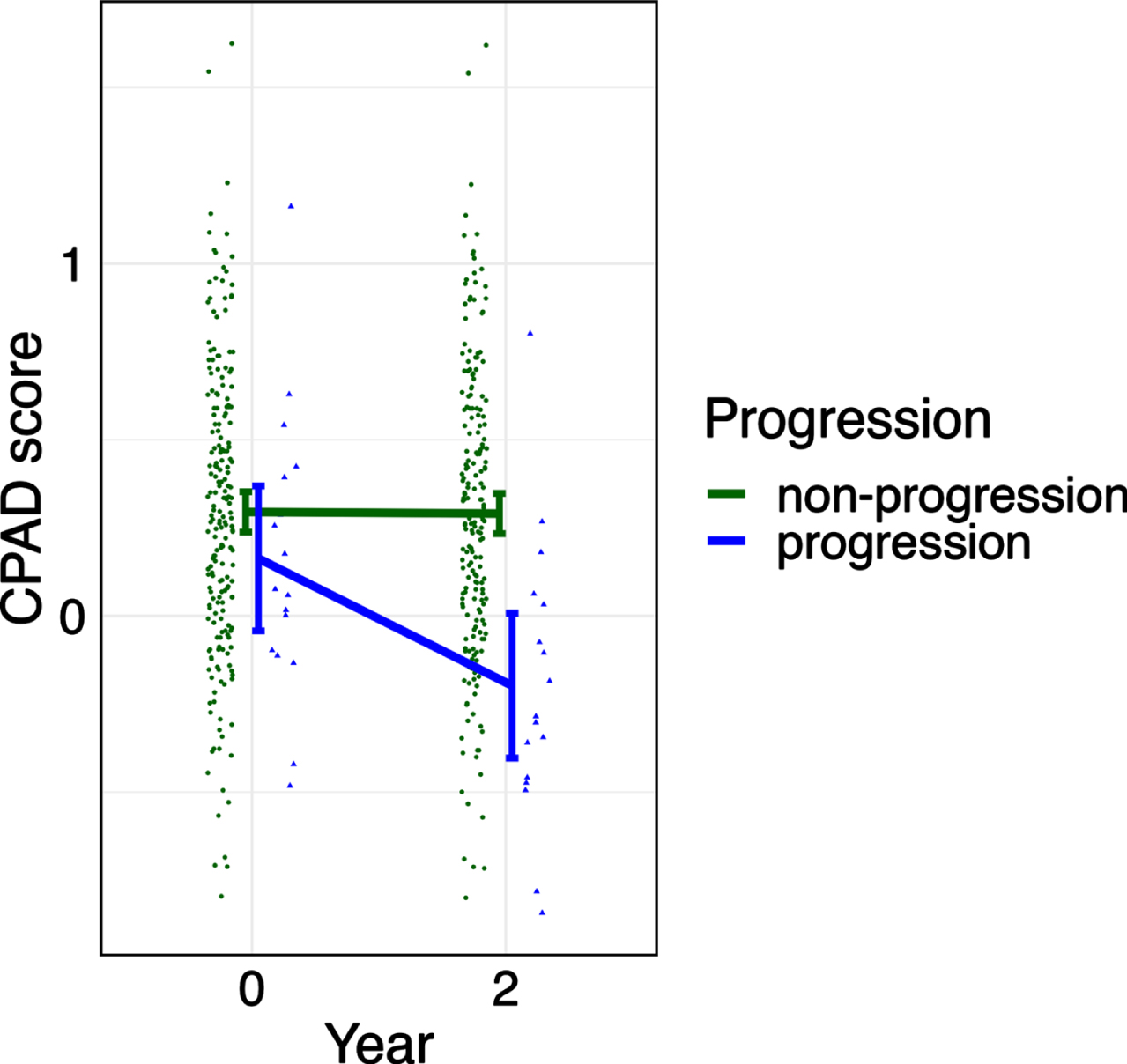
A linear mixed model was performed to determine whether the final selected composite was related to clinical progression to MCI or dementia. At the 2-year follow-up, 17 participants (8%) had progressed to MCI and no subjects who progressed to dementia. 208 participants (92%) remained clinically normal. In a linear mixed model with the CPAD score as the independent variable, a fixed effect of the interaction between time and progression was significant (p = 0.018, 95% CI [–0.650, –0.062]) (Table 8 and Fig. 2).
Table 8
The results of linear mixed model analysis of time and interaction between time and progression for final selected Composite (CPAD)
| Variables | CPAD | ||
| Estimate | 95% CI | p | |
| Time | –0.004 | –0.079, 0.070 | 0.905 |
| Progression (progressors) | –0.132 | –0.446, 0.183 | 0.412 |
| Time x Progression | –0.356 | –0.650, –0.062 | 0.018* |
| (Intercept) | 0.295 | 0.212, 0.378 | <0.001*** |
The reference group was non-progression group. (*p < 0.05, **p < 0.01, ***p < 0.001).
Fig. 2
The result of the linear mixed model of time and progression interaction for CPAD. The bars indicate 95% confidence intervals. The fixed effect of the interaction of time and progression was significant.
DISCUSSION
We developed CPAD, a cognitive composite to measure subtle cognitive changes of the preclinical AD, suitable for Korean older adults. We carefully selected tests to be included in the candidate composites, to parallel previously established composite scores developed largely with non-Hispanic White individuals. We selected a composite that best identified the amyloid–related subtle cognitive decline in preclinical AD as the final one. CPAD includes the CERAD WLR, LM-DR, MMSE total, and LF.
Similar to previous developed composite scores, CPAD covers the cognitive domains of episodic memory, executive function, and orientation. However, there are some differences in the individual items. Comparing with the PACC, the Free and Cued Selective Reminding Test (FCSRT) [26], which is not included in the KBASE protocol was substituted by the CERAD WLR. The CERAD WLR differs from the FCSRT in that it does not provide selective reminders. Nevertheless, the WLR test is considered a sensitive test to detect subtle cognitive changes in preclinical AD and is included in the API composite [22] and APCC [8]. For executive functions domain, the LF test was included instead of frequently used the Digit Symbol Substitution Test (DSST) [27], given that the current data do not have the DSST included in the battery. Evidence for the LF test as a strong predictor of progression to premorbid AD or MCI from normal cognition provides support inclusion of the LF instead of the DSST [28–30].
A major consideration for the difference from previously developed composites is cultural and linguistic factors. CPAD was developed based on data from Korean adult, and therefore a better option to use to detect or evaluate cognitive changes in preclinical AD in the Korean population. Demographic factors such as education and literacy lead to inequality in subsequent cognitive or occupational activities, and they affect cognitive reserve [31]. In addition, linguistic differences can produce biases due to translation or altered items in cognitive tests [32]. In our study, we confirmed that the CPAD could detect cognitive changes in preclinical AD in the Korean population, even though it was developed considering comparability with previously developed composites, especially PACC. However, unlike previous composites, we used demographically adjusted z-scores based on local normative data, considering the characteristics of Korean older adults whose cognitive performance varies greatly depending on their age, sex, and level of educational attainment, as well as their interactions. This point can be considered in future global studies with various cultural backgrounds.
We additionally tried to determine whether the longitudinal change of this composite score is related to the clinical progression of preclinical AD to MCI or dementia using a linear mixed model. The result showed that the change of CPAD score is significantly greater in the progression group than in the non-progression group, supporting the validity of CPAD.
There are some limitations of this study. First, a 2-year follow-up period also may not be long enough to track the cognitive change of participants. Additional validation with a longer follow-up period in the future may be helpful. Nevertheless, the final composite from the current study is meaningful because the significance was detected despite relatively short interval between the assessments. Second, although the cognitive domains of CPAD are very similar to those of the previously reported composites including PACC, there are differences in the individual tests included in each domain. Therefore, CPAD cannot be considered as a direct equivalent or counterpart to any of the previously reported cognitive composites for preclinical AD in a global study or trial. Third, generalizing the CPAD to other ethnic groups should be done with caution. Fourth, there are no alternate versions in both the development and final stages of the CPAD. Cognitively normal elderly may generate a significant practice effect, which can influence results in longitudinal studies. Future studies need to consider and strive to overcome this factor. Finally, the CPAD was developed using only observational study data and has not been validated using actual clinical trial data. Recent criticisms have pointed out that composite scores based on observational datasets may lead to overfitting and it remains unclear that these composites have adequate sensitivity to detect a clinically meaningful treatment effect in trials [33, 34].
CPAD can be used to assess subtle cognitive decline of preclinical AD in clinical research settings, especially in clinical trials with Korean older adults with preclinical AD. It also may be used for monitoring progression or treatment benefits in clinical practices.
ACKNOWLEDGMENTS
We thank all members of the KBASE Research Group for their contribution. Members of the KBASE Research Group are listed elsewhere (http://kbase.kr). We sincerely thank the patients for their participation in this study.
FUNDING
This study was supported by a grant from the Ministry of Science and ICT, Republic of Korea (NRF2014M3C7A1046042), a grant from the Ministry of Health and Welfare, Republic of Korea (HI18C0630 and HI19C0149), a grant from the Seoul National University Hospital, Republic of Korea (number 3020200030), and a grant from the National Institute of Aging (U01AG072177). The funding source had no role in the study design, data collection, data analysis, data interpretation, writing of the manuscript, or decision to submit it for publication.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
REFERENCES
[1] | Sperling RA , Aisen PS , Beckett LA , Bennett DA , Craft S , Fagan AM , Iwatsubo T , Jack CR Jr. , Kaye J , Montine TJ , Park DC , Reiman EM , Rowe CC , Siemers E , Stern Y , Yaffe K , Carrillo MC , Thies B , Morrison-Bogorad M , Wagster MV , Phelps CH ((2011) ) Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the National Institute on Aging-Alzheimer’s Association workgroups on diagnostic guidelines for Alzheimer’s disease. Alzheimers Dement 7: , 280–292. |
[2] | Jack CR Jr. , Bennett DA , Blennow K , Carrillo MC , Dunn B , Haeberlein SB , Holtzman DM , Jagust W , Jessen F , Karlawish J , Liu E , Molinuevo JL , Montine T , Phelps C , Rankin KP , Rowe CC , Scheltens P , Siemers E , Snyder HM , Sperling R , Contributors ((2018) ) NIA-AA Research Framework: Toward a biological definition of Alzheimer’s disease. Alzheimers Dement 14: , 535–562. |
[3] | Vellas B , Bateman R , Blennow K , Frisoni G , Johnson K , Katz R , Langbaum J , Marson D , Sperling R , Wessels A , Salloway S , Doody R , Aisen P , Task Force M ((2015) ) Endpoints for pre-dementia AD trials: A report from the EU/US/CTAD Task Force. J Prev Alzheimers Dis 2: , 128–135. |
[4] | Donohue MC , Sperling RA , Salmon DP , Rentz DM , Raman R , Thomas RG , Weiner M , Aisen PS Australian Imaging Biomarkers and Lifestyle Flagship Study of Ageing; Alzheimer’s Disease Neuroimaging Initiative; Alzheimer’s Disease Cooperative Study ((2014) ) The preclinical Alzheimer cognitive composite: Measuring amyloid-related decline. JAMA Neurol 71: , 961–970. |
[5] | Sperling RA , Rentz DM , Johnson KA , Karlawish J , Donohue M , Salmon DP , Aisen P ((2014) ) The A4 study: Stopping AD before symptoms begin? , 228fs. Sci Transl Med 6: , 213. |
[6] | Wang J , Logovinsky V , Hendrix SB , Stanworth SH , Perdomo C , Xu L , Dhadda S , Do I , Rabe M , Luthman J , Cummings J , Satlin A ((2016) ) ADCOMS: A composite clinical outcome for prodromal Alzheimer’s disease trials. J Neurol Neurosurg Psychiatry 87: , 993–999. |
[7] | Lim YY , Snyder PJ , Pietrzak RH , Ukiqi A , Villemagne VL , Ames D , Salvado O , Bourgeat P , Martins RN , Masters CL , Rowe CC , Maruff P ((2016) ) Sensitivity of composite scores to amyloid burden in preclinical Alzheimer’s disease: Introducing the Z-scores of Attention, Verbal fluency, and Episodic memory for Nondemented older adults composite score. Alzheimers Dement (Amst) 2: , 19–26. |
[8] | Langbaum JB , Ellison NN , Caputo A , Thomas RG , Langlois C , Riviere ME , Graf A , Lopez Lopez C , Reiman EM , Tariot PN , Hendrix SB ((2020) ) The Alzheimer’s Prevention Initiative Composite Cognitive Test: A practical measure for tracking cognitive decline in preclinical Alzheimer’s disease. Alzheimers Res Ther 12: , 66. |
[9] | Grober E , Hall CB , Lipton RB , Zonderman AB , Resnick SM , Kawas C ((2008) ) Memory impairment, executive dysfunction, and intellectual decline in preclinical Alzheimer’s disease. J Int Neuropsychol Soc 14: , 266–278. |
[10] | Elias MF , Beiser A , Wolf PA , Au R , White RF , D’Agostino RB ((2000) ) The preclinical phase of alzheimer disease: A 22-year prospective study of the Framingham Cohort. Arch Neurol 57: , 808–813. |
[11] | Derby CA , Burns LC , Wang C , Katz MJ , Zimmerman ME , L’Italien G , Guo Z , Berman RM , Lipton RB ((2013) ) Screening for predementia AD: Time-dependent operating characteristics of episodic memory tests. Neurology 80: , 1307–1314. |
[12] | Kittner SJ , White LR , Farmer ME , Wolz M , Kaplan E , Moes E , Brody JA , Feinleib M ((1986) ) Methodological issues in screening for dementia: The problem of education adjustment. J Chronic Dis 39: , 163–170. |
[13] | Escobar JI , Burnam A , Karno M , Forsythe A , Landsverk J , Golding JM ((1986) ) Use of the Mini-Mental State Examination (MMSE) in a community population of mixed ethnicity. Cultural and linguistic artifacts. J Nerv Ment Dis 174: , 607–614. |
[14] | Lee DY , Lee KU , Lee JH , Kim KW , Jhoo JH , Kim SY , Yoon JC , Woo SI , Ha J , Woo JI ((2004) ) A normative study of the CERAD neuropsychological assessment battery in the Korean elderly. J Int Neuropsychol Soc 10: , 72–81. |
[15] | Byun MS , Yi D , Lee JH , Choe YM , Sohn BK , Lee JY , Choi HJ , Baek H , Kim YK , Lee YS , Sohn CH , Mook-Jung I , Choi M , Lee YJ , Lee DW , Ryu SH , Kim SG , Kim JW , Woo JI , Lee DY , Group KR ((2017) ) Korean Brain Aging Study for the Early Diagnosis and Prediction of Alzheimer’s Disease: Methodology and baseline sample characteristics. Psychiatry Investig 14: , 851–863. |
[16] | Morris JC ((1993) ) The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 43: , 2412–2414. |
[17] | Lee JH , Lee KU , Lee DY , Kim KW , Jhoo JH , Kim JH , Lee KH , Kim SY , Han SH , Woo JI ((2002) ) Development of the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment Packet (CERAD-K): Clinical and neuropsychological assessment batteries. J Gerontol B Psychol Sci Soc Sci 57: , P47–53. |
[18] | Reiman EM , Chen K , Liu X , Bandy D , Yu M , Lee W , Ayutyanont N , Keppler J , Reeder SA , Langbaum JB , Alexander GE , Klunk WE , Mathis CA , Price JC , Aizenstein HJ , DeKosky ST , Caselli RJ ((2009) ) Fibrillar amyloid-beta burden in cognitively normal people at 3 levels of genetic risk for Alzheimer’s disease. Proc Natl Acad Sci U S A 106: , 6820–6825. |
[19] | Villeneuve S , Rabinovici GD , Cohn-Sheehy BI , Madison C , Ayakta N , Ghosh PM , La Joie R , Arthur-Bentil SK , Vogel JW , Marks SM , Lehmann M , Rosen HJ , Reed B , Olichney J , Boxer AL , Miller BL , Borys E , Jin LW , Huang EJ , Grinberg LT , DeCarli C , Seeley WW , Jagust W ((2015) ) Existing Pittsburgh Compound-B positron emission tomography thresholds are too high: Statistical and pathological evaluation. Brain 138: , 2020–2033. |
[20] | Papp KV , Rentz DM , Orlovsky I , Sperling RA , Mormino EC ((2017) ) Optimizing the preclinical Alzheimer’s cognitive composite with semantic processing: The PACC5. Alzheimers Dement (N Y) 3: , 668–677. |
[21] | Mormino EC , Papp KV , Rentz DM , Donohue MC , Amariglio R , Quiroz YT , Chhatwal J , Marshall GA , Donovan N , Jackson J , Gatchel JR , Hanseeuw BJ , Schultz AP , Aisen PS , Johnson KA , Sperling RA ((2017) ) Early and late change on the preclinical Alzheimer’s cognitive composite in clinically normal older individuals with elevated amyloid beta. Alzheimers Dement 13: , 1004–1012. |
[22] | Ayutyanont N , Langbaum JB , Hendrix SB , Chen K , Fleisher AS , Friesenhahn M , Ward M , Aguirre C , Acosta-Baena N , Madrigal L , Munoz C , Tirado V , Moreno S , Tariot PN , Lopera F , Reiman EM ((2014) ) The Alzheimer’s prevention initiative composite cognitive test score: Sample size estimates for the evaluation of preclinical Alzheimer’s disease treatments in presenilin 1 E280A mutation carriers. J Clin Psychiatry 75: , 652–660. |
[23] | Chey J , Kim J , Park K , Hwang S , Hong S (2012) Korean Wechsler Memory Scale-IV., Korea Psychology, Daegu. |
[24] | Ryu SH , Kim KW , Kim S , Park JH , Kim TH , Jeong HG , Kim JL , Moon SW , Bae JN , Yoon JC , Choo IH , Lee DW , Chang SM , Jhoo JH , Kim SK , Cho MJ ((2012) ) Normative study of the category fluency test (CFT) from nationwide data on community-dwelling elderly in Korea. Arch Gerontol Geriatr 54: , 305–309. |
[25] | Seo EH , Lee DY , Choo IH , Kim SG , Kim KW , Youn JC , Jhoo JH , Woo JI ((2008) ) Normative study of the Stroop Color and Word Test in an educationally diverse elderly population. Int J Geriatr Psychiatry 23: , 1020–1027. |
[26] | Buschke H ((1984) ) Cued recall in amnesia. J Clin Neuropsychol 6: , 433–440. |
[27] | Wechsler D (1981) Wechsler Adult Intelligence Scale Revised, Psychological Corporation, San Antonio, TX. |
[28] | Papp KV , Mormino EC , Amariglio RE , Munro C , Dagley A , Schultz AP , Johnson KA , Sperling RA , Rentz DM ((2016) ) Biomarker validation of a decline in semantic processing in preclinical Alzheimer’s disease. Neuropsychology 30: , 624–630. |
[29] | Clark LJ , Gatz M , Zheng L , Chen YL , McCleary C , Mack WJ ((2009) ) Longitudinal verbal fluency in normal aging, preclinical, and prevalent Alzheimer’s disease. Am J Alzheimers Dis Other Demen 24: , 461–468. |
[30] | Blacker D , Lee H , Muzikansky A , Martin E , Tanzi R , McArdle J , Moss M , Albert M ((2007) ) Neuropsychological measures in normal individuals that predict subsequent cognitive decline. Arch Neurol 64: , 862–871. |
[31] | Roe CM , Xiong C , Miller JP , Morris JC ((2007) ) Education and Alzheimer disease without dementia. Support for the cognitive reserve hypothesis. Neurology 68: , 223–228. |
[32] | Ng KP , Chiew HJ , Lim L , Rosa-Neto P , Kandiah N , Gauthier S ((2018) ) The influence of language and culture on cognitive assessment tools in the diagnosis of early cognitive impairment and dementia. Expert Rev Neurother 18: , 859–869. |
[33] | Borland E , Edgar C , Stomrud E , Cullen N , Hansson O , Palmqvist S ((2022) ) Clinically relevant changes for cognitive outcomes in preclinical and prodromal cognitive stages: Implications for clinical Alzheimer trials. Neurology 99: , e1142–e1153. |
[34] | Jutten RJ , Papp KV , Hendrix S , Ellison N , Langbaum JB , Donohue MC , Hassenstab J , Maruff P , Rentz DM , Harrison J , Cummings J , Scheltens P , Sikkes SAM ((2023) ) Why a clinical trial is as good as its outcome measure: A framework for the selection and use of cognitive outcome measures for clinical trials of Alzheimer’s disease. Alzheimers Dement 19: , 708–720. |


