
Shadowing Behavior May Be Associated with an Inability to Recognize the External World: A Case Report of Shadowing in a Patient with Posterior Cortical Atrophy
Abstract
Although shadowing behavior— when one individual closely follows another— is routinely documented among patients with dementia, its mechanisms have yet to be elucidated. In particular, there have been no detailed descriptions of patients with shadowing behavior. To propose its potential backgrounds, we describe a patient with posterior cortical atrophy who exhibited prominent shadowing behavior. He also experienced severe difficulties recognizing external stimuli, including visuospatial dysfunction, several types of agnosia, difficulties in verbal comprehension, disorientation, and its associated depression. This shadowing behavior may be adaptive relative to his extreme difficulty with recognizing the world around him.
INTRODUCTION
Some patients with degenerative diseases exhibit person-following behavior. Several terms have been used to describe this behavior, i.e., shadowing [1], clinging [2], stalking, and trailing [3, 4], and it has sometimes been included among wandering behaviors and even among anxiety-based behaviors [5]. Shadowing is not rare: its frequency was reported to be 8.5% among dementia patients based on a questionnaire given to their caregivers [6]. According to Hope et al., the frequency of trailing among patients with moderate to severe dementia is as high as 32% [4]. Surprisingly, almost no research has been performed on mechanisms underlying this intriguing and relatively common behavior. To date, it has been investigated from two aspects, i.e., psychological and cognitive ones, although researchers who have studied its potential mechanisms have often included shadowing among wandering behaviors and did not necessarily focus on this particular behavior. In a psychological context, Hope et al. indicated that trailing, an effort to avoid being alone, is similar to separation anxiety observed in infants [7]. Cognitive-wise, Hope et al., related this behavior to severe cognitive dysfunction and reported that trailing is significantly more prominent among individuals with severe cognitive decline and a score of 7 or less on the Mini-Mental State Examination (MMSE), the maximum score of which is 30 [4, 8]. Given these past findings, shadowing may result from a combination of severe cognitive dysfunction and its related psychological effects. Funayama et al. described a patient who had experienced carbon monoxide poisoning and subsequently kept following any person who came into his sight [9]. The authors concluded that this stimulus-bound behavior resulted from frontal lobe dysfunction and severe difficulties in recognizing the patient’s surroundings, including visuospatial deficits, sensory aphasia, and semantic memory deficits, which were associated with damage to posterior brain regions, such as the temporal and parietal cortices. This individual did not have a degenerative disease but had a diagnosis of hypoxic encephalopathy.
What is needed to further our understanding is a detailed case report of an individual with a degenerative disease who exhibits this behavior— such an individual is described herein. In this case report, we have utilized the term ‘shadowing’ to describe this behavior. We consider it the most appropriate term to describe the phenomenon since it is commonly used to refer to the behavior of individuals with dementia symptoms. Conversely, terms like ‘clinging’ and ‘stalking’ possess strong psychological connotations, ‘trailing’ carries the additional meaning of walking slowly, and ‘wandering behavior’ essentially denotes walking without any clear purpose or direction.
CASE DESCRIPTION
The patient was a right-handed man with 12 years of education who had been the president of a family-owned steel company since his early 50 s. He had no medical history, and his family members had no history of neurological or psychiatric disease. By the age of 59 years, he often became lost and had lost his sense of direction. At the age of 60, the patient no longer remembered how to use the press manufacturing machine or what the work process entailed, both of which he had been working with for 40 years. As a result, he was blamed by his relatives and became depressed. At the age of 61, he began to have difficulties naming his relatives and familiar objects. At the age of 62, he visited the local clinic, where he scored 21 of 30 points on the Japanese version of the Mini-Mental State Examination (MMSE-J) [10], the cut-off point of which is 24. Magnetic resonance imaging of his head demonstrated diffuse atrophy with predominance in the right parietal lobe (Fig. 1A). The same region was found to have relative hypoperfusion based on single-photon emission computerized tomography (SPECT) (Fig. 1B), leading to a diagnosis of Alzheimer’s disease. At the age of 63, he had difficulty using most electric appliances and would complain of not knowing where he was. He became unable to read an analog clock and manifested agraphia for Kanji, which are Chinese ideogram characters and constitute one of the writing systems used in the Japanese language. He missed a part of a Kanji character or was unable to remember an entire Kanji character.
Under these circumstances, he grew increasingly anxious, agitated, and depressed and would not leave the side of his wife, his main caregiver, on whom he depended heavily. He was administered an antidepressant, sertraline, to treat depression. From the age of 66, he was not able to consistently recognize the faces of his family members or understand everyday conversations with them. He was admitted to a nursing home for the elderly when it became impossible for his wife to care for him. In the nursing home, however, he would suddenly get angry and hit his housemates. In addition, he exhibited shadowing behavior, in which he frequently followed certain staff members and his housemates, which annoyed or irritated them. Administration of a psychotropic drug such as quetiapine or bromazepam did not improve his shadowing behavior, making it impossible for him to stay at the facility. He then was admitted to the neuropsychiatry unit in our hospital, where he continuously manifested the shadowing behavior (Fig. 2). Based on his symptoms, i.e., visuospatial dysfunction, agraphia, and prosopagnosia, we diagnosed him as posterior cortical atrophy according to Crutch’s diagnostic criteria [11]. He stayed in our unit for 70 days before he was transferred to a sanatorium. His psychotropic medications were discontinued upon admission.
Informed consent was obtained from the patient and his wife to perform this study.
Examination
We performed neurological and neuropsychological examinations as well as brain imaging. To assess general cognitive function, the MMSE-J was used. Visuospatial function was evaluated using the Japanese version of the Trail Making Test A (TMT-A) [12]. The span tests, i.e., Tapping Span Forward and Digit Span Forward in the Clinical Assessment for Attention [13], which have been used to assess visuospatial function in patients with posterior cortical atrophy [14], were also administered. Patients with posterior cortical atrophy typically show differences between these span tests, with a markedly short span on the Tapping Span Forward test despite a relatively preserved span on the Digit Span Forward test. To assess linguistic function, we administered the Standard Language Test of Aphasia (SLTA) [15], which has been widely used in Japan. Besides, we recorded cognitive dysfunction observed during the daily life of the patient while in the unit to assess his Clinical Dementia Rating [16].
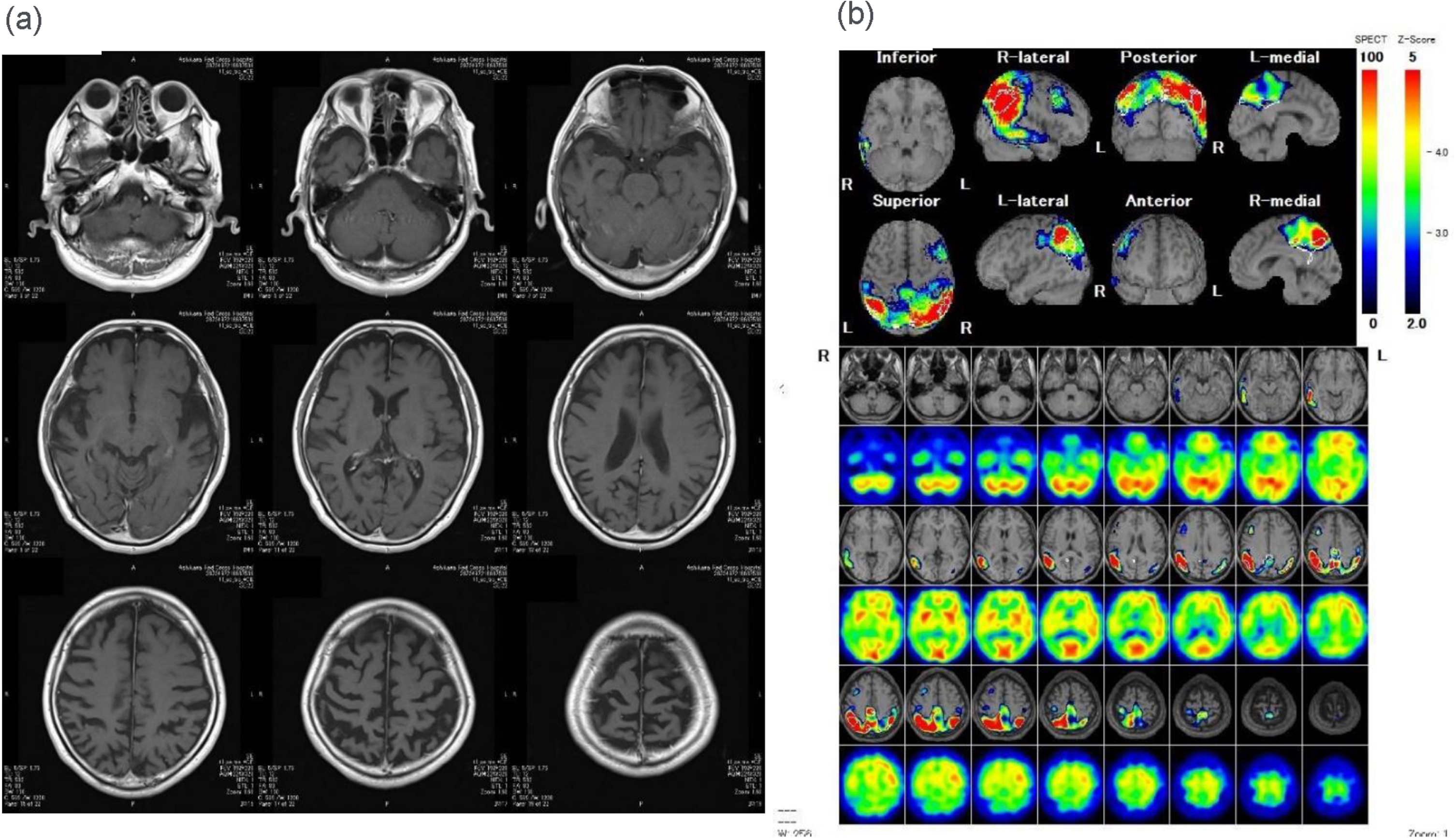
Fig. 1
Brain images at 62 years. (a) Fluid-attenuated inversion recovery (FLAIR) magnetic resonance imaging of the individual’s head shows diffuse atrophy with a predominance in the right parietal lobe. (b) Brain 99mTc-ethyl cysteinate dimer (99mTc-ECD) single-photon emission computed tomography (SPECT) imaging of the head and the eZIS analysis shows relative hypoperfusion in the right parietal lobe.
To better evaluate the severity of his shadowing behavior, we followed the method developed by Funayama et al., [9] in which the frequency of shadowing behavior was scored as 0, never; 1, occasionally; 2, moderately often; and 3, most of the time, and the severity was scored as 0, none; 1, mild; 2, moderate; and 3, severe. Severity was determined based on the presence or absence of changes in shadowing behavior in response to external stimuli, such as prompts from the therapist or the presence of other patients. For example, if shadowing behavior remained unchanged even with such external stimuli, it was classified as severe. If shadowing behavior easily disappeared in response to prompts from the therapist or stimuli from other patients, it was classified as mild. The total score was expressed as the product of the frequency and severity scores. MADRS-J [17] was used to assess his depression and was administered both at admission and at discharge. For brain imaging, magnetic resonance imaging and Brain 99mTc-ethyl cysteinate dimer (99mTc-ECD) single-photon emission computerized tomography with easy Z-score imaging system (eZIS) analysis [18] were used.
RESULTS
Upon neurological examination, the individual never showed paresis, parkinsonian signs, involuntary movements, ataxia, sensory disturbance, and primitive reflexes. He did not present with any stimulus-bound behaviors, i.e., instinctive grasp reaction [19] or incidental utilization behavior [20, 21]. The results of the neuropsychological tests are presented in Table 1. In simple terms, the patient exhibited severe cognitive impairments, with visuospatial dysfunction being the most prominent, followed by aphasia and disorientation. Notably, the Trail Making Test (TMT) revealed severe visuospatial dysfunction as the patient was unable to connect circles, indicating a limitation in simultaneously identifying multiple targets, which is consistent with simultanagnosia [22]. Similarly, the patient displayed a restricted span of one unit on the Tapping Span Forward task, while managing to repeat three digits on the Digit Span Forward task. Regarding speech, the patient’s fluency remained intact; however, he experienced frequent word finding difficulties, repetition difficulties, and phonological paraphasias. These characteristics align with the logopenic subtype, which can occur in conjunction with posterior cortical atrophy [23]. It is important to note that the patient’s verbal comprehension abilities were also disrupted, highlighting the broader impairment that extends beyond the typical features of logopenic subtype aphasia.
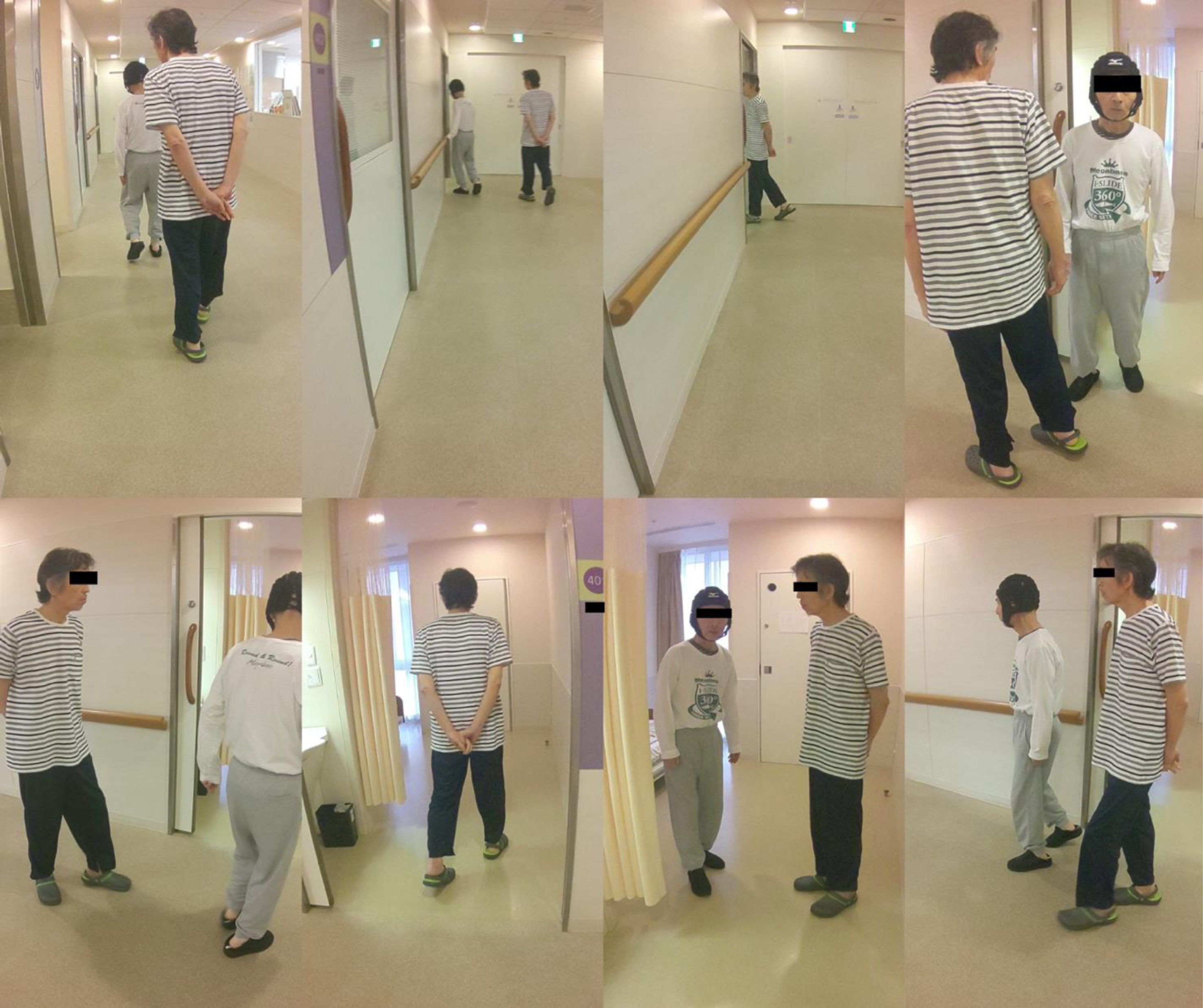
Fig. 2
Shadowing behavior. The patient wearing a striped shirt shows shadowing behavior. He follows another patient into that room. When another patient leaves the room, he follows him out of the room again.
Observation of his daily living in the unit revealed severe cognitive dysfunction, particularly severe visuospatial dysfunction. He had difficulty positioning himself to sit in a chair and would attempt to lie down on his bed to sleep, only to miss the bed completely. He also had dressing apraxia in which he put his clothes on backwards. During a meal, he was able to see and grasp only one dish at a time that was in front of him and could not see the other dishes. He became lost even in this unit, suggesting he had severe topographical disorientation, an inability in navigating through environments [24]. In addition, he often wandered into the rooms of female patients, suggesting he had also landmark agnosia, an inability to recognize surroundings, such as rooms, buildings, and landscapes [25, 26]. Although he could use everyday tools, such as a toothbrush, he could not remember how to flush the toilet or even how to open the door in his own room, suggesting that he had apraxia for some tools. He also manifested mirror agnosia [27], in which he sometimes misidentified his own image when reflected in a mirror as a different person and tried to talk to his image. Given these difficulties, his Clinical Dementia Rating was rated at 3 (severe).
Table 1
Results of the patient’s neuropsychological tests
| Attribute | Examination | Patient Score | Normal Population Score for the 60s |
| Dementia severity | Clinical Dementia Rating (0, normal; 3 severe) | 3 | 0 |
| General cognitive function | Mini-Mental State Examination (MMSE) | 3/30 | Cutoff point: 24 |
| Short-term memory | Tapping Span Forward Test | 1 digit | 4.7±0.54 digits |
| Digit Span Forward Test Visuospatial function | 3 digits Trail Making Test A(TMT-A) | 4.9±0.86 digits unable to perform (due to his simultanagnosia) | Cutoff point: 49 seconds and/or 3 errors |
| Linguistic function | Standard Language Test of Aphasia (SLTA) | Word comprehension 9/10 Short-sentence comprehension 0/10 Object naming 5/20 Sentence repetition 2/5 phrases | A perfect score on all four items |
Regarding the shadowing behavior assessment, the patient had a maximum score of 9, with a frequency score of 3 (most of the time) and a severity score of 3 (severe). When the person he was following almost fell over, the patient prevented his fall. When a male patient with dementia whom he was following entered the women’s restroom, he also went in there. He followed only certain people, and his facial expression was relatively calm and relaxed when he was following one of those people, as if he felt safe and enjoyed being with that individual. We never stopped him from doing this shadowing behavior during his stay in our unit, and he never got angry, anxious, or depressed during the whole stay, even though his psychotropic medications were discontinued. His score on the MADRS-J at admission and discharge was 3 and 2, respectively, both of which were within the normal range of < 7 [23].
Figure 3A and 3B shows the follow-up brain images at 65 and 66 years old. These images demonstrated that this patient’s atrophy and hypoperfusion developed as the disease progressed, with marked atrophy and hypoperfusion in the right parietal lobe as well as the contralateral left parietal lobe.
To sum up, this patient, with his posterior cortical atrophy, exhibited remarkable shadowing behavior, in conjunction with severe difficulties recognizing his surroundings, including visuospatial dysfunction, agnosia (prosopagnosia, mirror agnosia, and landmark agnosia), difficulties in verbal comprehension, and disorientation, all of which substantially reduced his ability to perform activities of daily living and lead to dependency on others.
DISCUSSION
Here we describe in detail a degenerative patient who had posterior cortical atrophy and exhibited shadowing behavior. While we did not conduct any pathological investigations, the patient’s neurological and neuropsychological symptoms, combined with the high prevalence of Alzheimer’s pathology in posterior cortical atrophy [11, 28], support his clinical diagnosis of early-onset Alzheimer’s disease with posterior cortical atrophy.
In contrast to the previous case involving carbon monoxide poisoning, where shadowing behavior was observed [9], our patient did not exhibit stimulus-bound behaviors or primitive reflexes. This suggests that such behaviors may not always be essential for the development of shadowing behavior. However, both cases shared common features, including severe visuospatial dysfunction, agnosia or semantic memory deficits, difficulties in verbal comprehension, and disorientation. These observations imply that profound challenges in recognizing surroundings, both visually and auditorily, could potentially contribute to the manifestation of shadowing behavior.
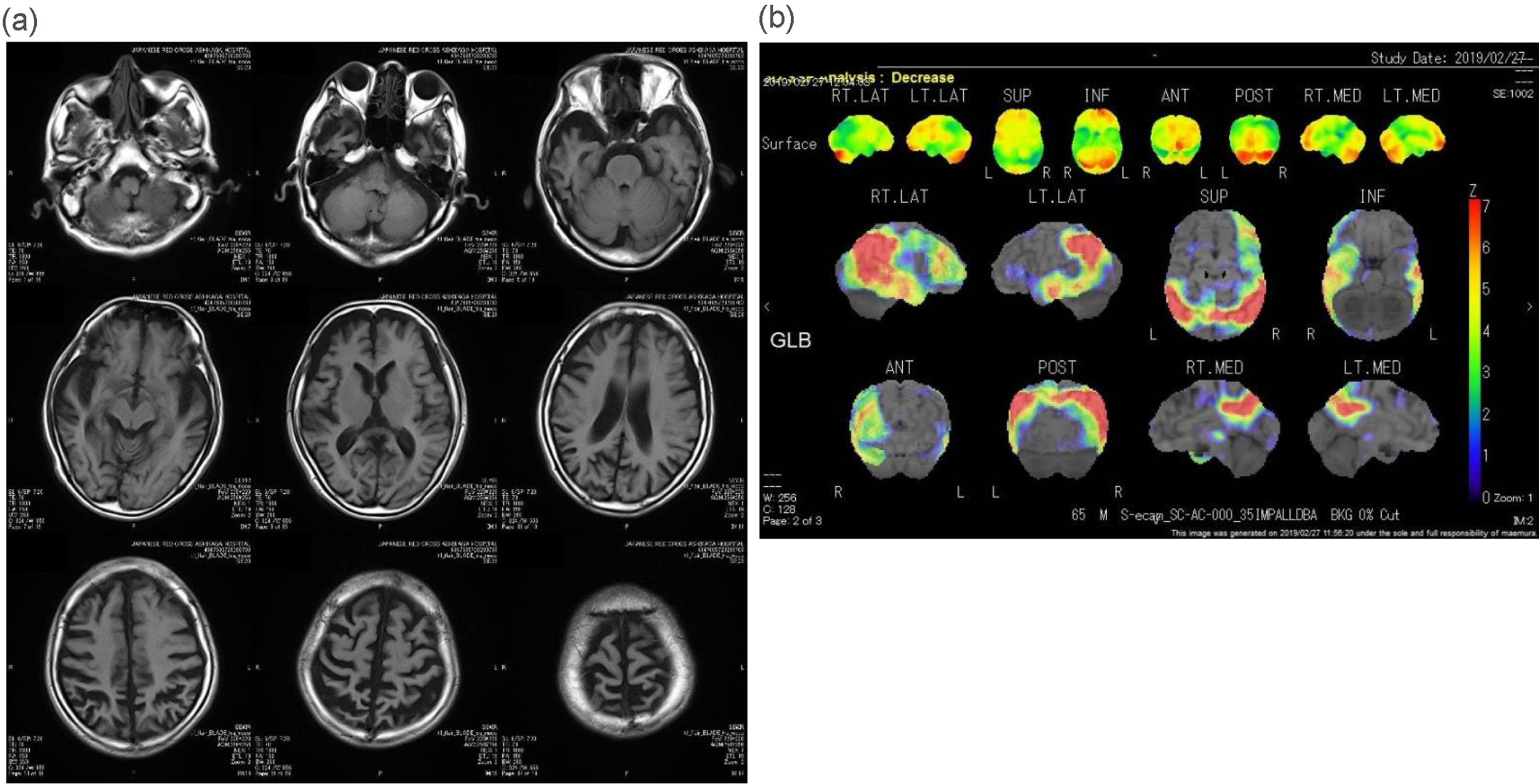
Fig. 3
Follow-up brain images. (a) Fluid-attenuated inversion recovery (FLAIR) magnetic resonance imaging of the head of the patient at 66 years of age shows progressive atrophy of the right lateral temporal and parietal lobes as well as the left parietal lobe. (b) 123I-labeled N-isopropyl-p-iodo-amphetamine (123I-IMP) single-photon emission computed tomography (SPECT) imaging of the head of the same individual at 65 years of age and subsequent three-dimensional stereotactic surface projections (3D-SSP) analysis show that the relative hypoperfusion of both parietal lobes has progressed.
This case involved posterior cortical atrophy, which is a rare form of degenerative disease with visuospatial dysfunction. However, because shadowing is a relatively common symptom in dementia [4, 6], it may occur not only in cases of posterior cortical atrophy but also in some cases of dementia, particularly typical Alzheimer’s disease [2]. Compared to the behavioral symptoms observed in behavioral variant frontotemporal dementia, which are associated with frontal and anterior temporal atrophy, Alzheimer’s disease is characterized by a broader range of cognitive dysfunctions, including deficits in episodic memory, visuospatial abilities, visual perception, and receptive language skills [29, 30]. The cognitive impairments observed in Alzheimer’s disease are associated with atrophy in posterior brain regions, such as the medial temporal, parietal, parieto-temporal, and temporo-occipital regions, which play a role in recognizing stimuli from the external world and contribute to visuospatial and visual perception, as well as verbal comprehension [31]. Consistent with this perspective, the present case experienced severe visuospatial deficits, visual perception dysfunction (several types of agnosia), disorientation, and difficulties in verbal comprehension, collectively resulting in challenges in perceiving the external stimuli. These difficulties significantly impede the patient’s ability to recognize external world as a whole. In such circumstances, patients often become reliant on others, leading to a fear of being left alone in some cases [7]. This fear may contribute to the development of shadowing behavior, which is considered an adaptive response to mitigate excessive anxiety in these individuals [7]. This perspective aligns with the previous understanding that shadowing behavior can arise from both cognitive and psychological factors [4, 7]. Moreover, in the present case, we provide more detailed and specific information about dysfunctions that may be associated with this shadowing behavior. It is important to note that these dysfunctions are not limited to a single domain, but rather encompass several aspects of recognition functions.
Drawing definitive conclusions from this single case is challenging, especially given the severity of this patient’s deficits (MMSE 3/30). However, the profound cognitive dysfunctions observed, particularly the severe difficulties in recognizing the surroundings, could potentially contribute to the development of shadowing behavior. To confirm these proposed mechanisms, larger studies involving an adequate number of degenerative patients specifically focusing on shadowing behavior are needed.
ACKNOWLEDGMENTS
We thank the patient and his wife for allowing us to report the results of this case study.
FUNDING
The authors have no funding to report.
CONFLICT OF INTEREST
The authors have no conflict of interest to report.
DATA AVAILABILITY STATEMENT
The datasets generated and/or analyzed during the current study are available from the corresponding author (S. Kudo) upon request.
REFERENCES
[1] | Algase DL , Beattie ERA , Bogue EL , Yao L ((2001) ) The Algase wandering scale: Initial psychometrics of a new caregiver reporting tool. Am J Alzheimers Dis Other Demen 16: , 141–152. |
[2] | Asada T , Kinoshita T , Kakuma T ((2000) ) Analysis of behavioral disturbances among community-dwelling elderly with Alzheimer disease. Alzheimer Dis Assoc Disord 14: , 160–167. |
[3] | The International Psychogeriatric Association Behavioral and Psychological Symptoms of Dementia (BPSD) Educational Pack. http://www.ipa-online.org/ipaonlinev3/ipaprograms/bpsdarchives/bpsdrev/1BPSDfinal.pdf. |
[4] | Hope T , Keene J , McShane RH , Fairburn CG , Gedling K , Jacoby R ((2001) ) Wandering in dementia: A longitudinal study. Int Psychogeriatr 13: , 137–147. |
[5] | Kales HC , Gitlin LN , Lyketsos CG ((2015) ) Assessment and management of behavioral and psychological symptoms of dementia. BMJ 350: , h369. |
[6] | Nichols LO , Edd JM , Greene WA , Burns R , Graney MJ , Lummus A , Nichols LO , Edd JM , Alex W , Burns R , Graney MJ , Lummus A , Greene WA ((2009) ) Dementia caregivers ’ most pressing concerns. Clin Gerontol 32: , 1–14. |
[7] | Hope RA , Fairburn CG ((1990) ) The nature of wandering in dementia: A community-based study. Int J Geriatr Psychiatry 5: , 239–245. |
[8] | Folstein MF , Folstein SE , McHugh PR ((1975) ) “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res 12: , 189–198. |
[9] | Funayama M , Takata T ((2019) ) Forced person-following: A new type of stimulus-bound behavior. Neurocase 25: , 75–79. |
[10] | Sugishita MHI ((2010) ) Validity and reliability of mini mental state examination-japanese (MMSE-J): A preliminary report. Japan J Cogn Neurosci 12: , 186–190. |
[11] | Crutch SJ , Schott JM , Lehmann M , Primativo S , Rossor MN , Ryan NS , Shakespeare TJ , Suárez González A , Yong KXX , Fox NC , Rabinovici GD , Lehmann M , Murray M , Snowden JS , Snowden JS , van der Flier WM , Pijnenburg Y , Scheltens P , van der Flier WM , Dickerson BC , Vandenberghe R , Ahmed S , Butler C , Bak TH , Boeve BF , Graff-Radford J , Cappa SF , Ceccaldi M , de Souza LC , Dubois B , Felician O , Felician O , Galasko D , Graff-Radford NR , Hof PR , Hof PR , Krolak-Salmon P , Magnin E , Mendez MF , Nestor PJ , Onyike CU , Pelak VS , Pelak VS , Suárez González A , Tang-Wai DF , Carrillo M ((2017) ) Consensus classification of posterior cortical atrophy. Alzheimers Dement 13: , 870–884. |
[12] | Brain Function Test Committee, Japan Society for Higher Brain Dysfunction ((2019) ) Trail Making Test, Japanese edition (TMT-J). Shinkoigakushuppankai, Tokyo. |
[13] | Kato M ((2006) ) Clinical assessment of attention. Shinkoigakushuppankai, Tokyo. |
[14] | Funayama M , Takata T , Nakagawa Y , Sunagawa K , Nakajima A , Kawashima H , Mimura M ((2021) ) Visuospatial working memory dysfunction from tapping span test as a diagnostic tool for patients with mild posterior cortical atrophy. Sci Rep 11: , 10580. |
[15] | Nakagawa Y , Sano Y , Funayama M , Kato M ((2019) ) Prognostic factors for long-term improvement from stroke-related aphasia with adequate linguistic rehabilitation. Neurol Sci 40: , 2141–2146. |
[16] | Morris JC ((1993) ) The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 43: , 2412–2414. |
[17] | Inada T ((2004) ) Clinical evaluation of depressive disorders by the MADRS Japanese version using the SIGMA. Jiho, Tokyo. |
[18] | Matsuda H , Mizumura S , Nagao T , Ota T , Iizuka T , Nemoto K , Kimura M , Tateno A , Ishiwata A , Kuji I , Arai H , Homma A ((2007) ) An easy Z-score imaging system for discrimination between very early Alzheimer’s disease and controls using brain perfusion SPECT in a multicentre study. Nucl Med Commun 28: , 199–205. |
[19] | Seyffarth H , Denny-brown D ((1948) ) The grasp reflex and the instinctive grasp reaction. Brain 71: , 109–183. |
[20] | Kertesz A , Davidson W , Fox H ((1997) ) Frontal behavioral inventory: Diagnostic criteria for frontal lobe dementia. Can J Neurol Sci 24: , 29–36. |
[21] | Shallice T , Burgess PW , Schon F , Baxter DM ((1989) ) The origins of utilization behaviour. Brain 112 (Pt 6): , 1587–1598. |
[22] | Rizzo M , Vecera SP ((2002) ) Psychoanatomical substrates of Bálint’s syndrome. J Neurol Neurosurg Psychiatry 72: , 162–178. |
[23] | Fitzpatrick D , Blanco-Campal A , Kyne L ((2019) ) A case of overlap posterior cortical atrophy and logopenic variant primary progressive aphasia. Neurologist 24: , 62–65. |
[24] | Aguirre GK , D’Esposito M ((1999) ) Topographical disorientation: A synthesis and taxonomy. Brain 122 (Pt 9): , 1613–1628. |
[25] | Takahashi N , Kawamura M ((2002) ) Pure topographical disorientation–the anatomical basis of landmark agnosia. Cortex 38: , 717–725. |
[26] | Van Der Ham IJM , Martens MAG , Claessen MHG , Van Den Berg E ((2017) ) Landmark agnosia: Evaluating the definition of landmark-based navigation impairment. Arch Clin Neuropsychol 32: , 472–482. |
[27] | Connors MH , Coltheart M ((2011) ) On the behaviour of senile dementia patients vis-à-vis the mirror: Ajuriaguerra, Strejilevitch and Tissot (1963). Neuropsychologia 49: , 1679–1692. |
[28] | Cipriano L , Oliva M , Puoti G , Signoriello E , Bonavita S , Coppola C ((2022) ) Is the pathology of posterior cortical atrophy clinically predictable? Rev Neurosci 33: , 849–858. |
[29] | Silveri MC ((2007) ) Frontotemporal dementia to Alzheimer’s disease. Dialogues Clin Neurosci 9: , 153–160. |
[30] | Musa G , Slachevsky A , Muñoz-Neira C , Méndez-Orellana C , Villagra R , González-Billault C , Ibáñez A , Hornberger M , Lillo P ((2020) ) Alzheimer’s disease or behavioral variant frontotemporal dementia? Review of key points toward an accurate clinical and neuropsychological diagnosis. J Alzheimers Dis 73: , 833–848. |
[31] | Mesulam MM ((1998) ) From sensation to cognition. Brain 121 (Pt 6): , 1013–1052. |


