
Efficacy of a Mobile-Based Multidomain Intervention to Improve Cognitive Function and Health-Related Outcomes Among Older Korean Adults with Subjective Cognitive Decline
Abstract
Background:
Subjective cognitive decline (SCD) is a self-reported experience of declining cognitive function showing normal performance in cognitive assessments, which is a known risk factor for dementia. Recent studies highlight the importance of nonpharmacological multidomain interventions that can target multiple risk factors of dementia in older adults.
Objective:
This study investigated the efficacy of the Silvia program, a mobile-based multidomain intervention, to improve cognitive function and health-related outcomes of older adults with SCD. We compare its effects to a conventional paper-based multidomain program on various health indicators related to risk factors of dementia.
Methods:
This prospective randomized controlled trial involved 77 older adults with SCD recruited from the Dementia Prevention and Management Center in Gwangju, South Korea during May to October 2022. Participants were randomly assigned to either the mobile- or paper-based group. Interventions were administered for 12 weeks, where pre- and post-assessments were conducted.
Results:
The K-RBANS total score did not show significant differences between groups. The mobile group showed better improvement in K-PRMQ scores and PSS scores than the paper group. Differences within groups showed that mobile-based interventions significantly improved K-PRMQ, STAI-X-1, PSS, and EQ-5D-5 L scores, while paper-based interventions significantly improved PSS, and EQ-5D-5 L scores. Patient adherence rate was 76.6%.
Conclusion:
Overall, the Silvia program was effective for improving self-reported memory failures, stress, anxiety, and health-related quality of life in older adults with SCD. However, longer periods of administration for more than 12 weeks may be needed to achieve significant improvements in cognitive function by objective measures.
INTRODUCTION
Dementia has been significantly associated with functional deterioration of daily activities, behavioral/psychological problems, and high healthcare costs, resulting in disability and dependency among older adults that diminishes quality of life and increases family/caregiver burden [1]. Prevalence is on the rise, where more than 55 million people were living with dementia worldwide in 2020, a number projected to double every 20 years [2]. To decrease the burden of this debilitating disorder, early detection and preventive measures are becoming imperative, according to recent epidemiologic research [3, 4]. Additionally, systematic reviews and meta-analysis have indicated that cognitive decline can be reversed by interventions such as cognitive training [5] or physical exercise [6], showing small to moderate positive effects in global cognitive function. This phenomenon is explained by the concepts of cognitive reserve and neuroplasticity, whereby deterioration of the brain’s function can be delayed by effective cognitive training [7]. Accordingly, the South Korean government and healthcare professionals have sought to design and implement strategies to reverse this trend by providing interventions to help older adults maintain or increase their cognitive function [8].
Subjective cognitive decline (SCD) refers to a self-reported experience of declining cognitive function compared to one’s past, although standardized cognitive tests show normal performance [9]. Although the literature on SCD has been inconsistent due to poor definition of the condition [10], systematic reviews and meta-analysis have shown that older adults with SCD are more than twice as likely to progress to dementia compared to normal [11–13]. Therefore, individuals with SCD would be appropriate candidates for early interventional studies to improve cognitive function and health-related outcomes, which may help delay the onset of dementia.
A growing body of clinical studies highlight the importance of nonpharmacological multidomain interventions which can target multiple risk factors for dementia development [14]. The Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) reported the first clinical trial to test the efficacy of a multidomain lifestyle program for older adults at high risk for dementia [15], which demonstrated its strategic value to promote cognitive function and improve overall health. This approach involves attention to multiple lifestyle components such as cognitive activities, nutrition/diet, exercise, and quality of sleep [15]. Subsequent studies have adopted the FINGER study as a platform to investigate the effectiveness of multidomain interventions for the prevention of cognitive decline, including national studies such as the Multidomain Alzheimer Preventive Trial (MAPT study) [16] and the Prevention of Dementia by Intensive Vascular Care (PreDIVA) study [17]. In addition, a recent meta-analysis of cognitive interventions showed that older adults with mild cognitive impairment participating in programs that incorporated two or more nonpharmacological components, such as cognitive training and aerobic exercise, showed better performance in improving cognitive function than participants in single interventions [18]. Hence, it is important to emphasize the multidomain lifestyle approach as a strategy to protect brain health and promote overall health. However, more research is needed to ensure that they are tailored to meet the needs of diverse populations, as factors such as geography, culture, and economic status can influence its efficacy [19].
With the help of technological advances, cognitive interventions have been going through rapid digitalization in recent years, especially during the COVID-19 pandemic [20, 21]. Computerized cognitive training (CCT) involves various computerized or digital tools including virtual reality, interactive video gaming, and mobile technology [22]. Advanced mobile technologies provide enhanced accessibility, cost-effectiveness, and personalized experiences, which is effective for increasing cognitive health and overall quality of life among people at high risk for developing dementia [22]. Indeed, a recent meta-analysis has shown promising results for the effectiveness of CCT interventions in improving cognitive function in individuals with MCI [5]. CCT can overcome the primary drawbacks of conventional interventions in clinical settings, which are mostly face-to-face interactions using pen-and-paper exercises or oral tasks [23] that require intensive monetary, time, and space resources and the challenge of monitoring patient adherence [24]. In addition, CCT can accommodate variations in task levels according to the individuals’ competency, unlike paper-based exercises [25]. However, despite its potential, the impact of digital health platforms and similar clinical programs have been limited by a lack of scientific evidence concerning 1) the impact of mobile-based multidomain programs on cognitive function and health-related outcomes; 2) the comparative efficacy of mobile-based programs compared to paper-based programs; and 3) ways to develop personalized approaches within multidomain programs for people with high risk of dementia.
In this study, we adopted the Silvia Program, which is a mobile-based multidomain health platform designed for the prevention of dementia. The primary purpose of this study was to assess the efficacy of the Silvia Program to improve the cognitive function and health-related outcomes of older Korean adults with SCD. In addition, we compared any differences in health indicators related to cognitive functions and risk factors of dementia between the Silvia Program and a conventional paper-based multidomain program proposed by the World Health Organization (WHO) [26].
MATERIALS AND METHODS
Study design
This study was a prospective randomized controlled trial with pre-post assessments. Participants were randomly assigned to the mobile-based group or the paper-based group in a 1 : 1 ratio, using a computer-generated allocation system. Data were collected at baseline and after a period of 12 weeks by the evaluators who were blinded as to participants’ group assignments.
Sample and recruitment
Inclusion criteria targeted participants aged 60 to 75 years who 1) were experiencing subjective cognitive decline, 2) had a smart phone and could use it, and 3) understood the purpose and process of this study. Participants were excluded if they had experienced or were experiencing one of the following seven conditions: 1) major psychiatric disorders, 2) dementia, 3) degenerative brain diseases, 4) severe or unstable heart diseases, 5) neurological or psychological diseases that affected cognitive functioning, 5) severe vision or hearing impairment, 6) current participation in a cognitive training program; 7) does not know how to use mobile devices.
Participants were recruited from the Dementia Prevention and Management Center in Gwangju, South Korea, a community-based public institution that provides integrated care for dementia such as early screening, preventive activities, disease education, and patient/family support, during the period May to October 2022. The research team distributed recruitment materials to the list of potential participants. Verbal informed consent was obtained upon contact to the research team by those interested in the study. Potential participants were initially screened for eligibility based on the inclusion and exclusion criteria, and individuals who were eligible for participation were scheduled for baseline measurements. One week before starting the intervention, our research team visited each potential participant to verify eligibility and provide 1–2 hours of orientation to the study.
The intake procedure took place at either the center or the participants’ homes. At intake, the research team (i.e., a clinical psychologist and trained research staff) obtained written informed consent, conducted the orientation sessions, and administered questionnaires for baseline measurements with each participant individually along with the facility staff.
The sample size was calculated using the G*power 3.1.9.7 program (number of groups = 2, α= 0.05, power = 0.95, effect size = 0.63), and the effect size was estimated based on relevant studies [27]. The minimum number of participants was 70 (35 for each group), but considering an approximately 10% dropout rate, at least 77 participants were needed. Based on these calculations, we enrolled 80 participants. This study was approved by the institutional review board of Chosun University Hospital (IRB approval number: 2022-03-013).
Mobile-based multidomain intervention (Silvia Program)
Participants who were randomly assigned to the mobile-based intervention group were first provided access to the Silvia mobile application (Silvia Health Inc., South Korea) and received a 50-minute individual, face-to-face training session on how to use it. The Silvia Program is an mHealth application comprising multidomain programs based on scientific evidence of ways to improve brain health and reduce dementia risk, which consists of seven modules: 1) cognitive training, 2) video-assisted exercise, 3) mindfulness and relaxation, 4) daily diary, 5) educational content, 6) cognitive assessment, and 7) online counseling. Figure 1 shows representative images of the mobile application.
Fig. 1
Representative images of the Silvia mobile application.

1) Cognitive training: Over 20 types of gamified programs stimulating all domains of cognitive functioning (memory, visuo-spatial, language, executive function, attention) were provided. Participants were allowed to choose a program type and level of difficulty and use the training program on a personalized mobile device. Participants were recommended to engage in cognitive training for 10 minutes per day and 5 times per week.
2) Video-assisted exercise: Over 10 different video instructions designed by an exercise therapist were provided, the contents of which included strengthening major muscles, moving joints and tendons to develop balance, etc. Participants could easily follow the movements demonstrated on the Silvia app and were recommended to engage in exercise activities for 15 minutes per day and 5 times per week.
3) Mindfulness and relaxation: Effective relaxation techniques, such as deep breathing and meditation, were provided with video- and audio-guidance. No specific recommendations were given for frequency of use.
4) Daily diary: A self-reportable program where participants could input their lifelog data, such as what they had eaten, what kinds of exercise they had performed, or how many hours of sleep they had, was provided. No specific recommendations were given for frequency of use.
5) Educational content: Articles on various health-related topics were provided in the Silvia app, such as scientific facts about dementia, how to manage stress and anxiety, a list of healthy foods for preventing dementia, exercises beneficial for counteracting dementia, etc. No specific recommendations were given for frequency of use.
6) Cognitive assessment: Voice-based cognitive assessments led by artificial intelligence (AI) were accessible at any time of convenience. The assessments measured the difficulties participants experienced with each cognitive exercise or task, the time they spent completing it, and the scores they achieved. No specific recommendations were given for frequency of use.
7) Online counseling: Based on the personalized data accumulated in the Silvia app, weekly coaching sessions were provided to each of the participants by a professional psychological counselor through online video calls. Participants could ask questions about their health and receive the counselor’s recommendations. Each session lasted 10 20 minutes.
Paper-based multidomain intervention
Participants who were randomly assigned to the paper-based intervention group were provided with the Korean version of the dementia prevention booklet published by the WHO [26], which contained information and advice on various topics, such as cognitive training exercises, physical activity for brain health, smoking cessation, foods for preventing dementia, social activities, weight management, chronic disease management, and depression management. The booklet consisted of 12 chapters, which were delivered consecutively each week via post mail to the participants’ home throughout the study period. Each chapter provided 1) science-based educational content relevant to improving brain health and reducing dementia risk, 2) quizzes for reviewing previously learned contents, and 3) formats for setting personal health goals and recording daily lifestyle information.
Outcome measures
During the first visit, the participants completed baseline assessments on demographic features, overall health status, cognitive function, and various health-related outcomes. Participants completed the same set of assessments after the 12-week intervention.
Demographic features
The demographic and health status information included age, gender, educational level, body mass index, chronic disease status (e.g., diabetes, hyperlipidemia), lifestyle information (e.g., smoking, drinking, physical activity), and living arrangements.
Cognitive function
Cognitive function was measured using two assessment tools. The primary outcome was the Korean version of the Repeatable Battery for the Assessment of Neuropsychological status (K-RBANS). The Korean version of the mini-mental state examination, 2nd edition (K-MMSE-2), was used as a secondary outcome. The reliability and validity of both instruments had been statistically demonstrated in numerous studies involving community-dwelling older adults [28, 29].
The K-RBANS consisted of 5 domains (immediate memory, visuospatial capacity, language, attention, and delayed memory). The index scores for each domain (ranging from 40 to 160) were summed and converted into a total index score (also ranging from 40 to 160), with higher scores representing superior cognitive function. All participants received form A of the K-RBANS at baseline and form B after the 12-week intervention to prevent content practice effects. The K-MMSE-2 measured cognitive function with a total score ranging from 0 to 30, where scores of 24 or higher indicated normal cognitive function.
Self-reported memory failures
The Korean version of the prospective and retrospective memory questionnaire (K-PRMQ) [30] was used to determine the degree of memory failures in daily life as a secondary outcome. The questionnaire consists of 16 items with a total score ranging from 16 to 80. The higher the overall score, the more memory failures were reported.
Depression
Depression was assessed as a secondary outcome using the Center for Epidemiological Studies-Depression (CES-D) questionnaire [31], which comprises 20 items with a total score ranging from 0 to 60. Higher scores indicate rising levels of depression, where scores below 16 indicate normal status.
Anxiety
Anxiety was assessed as a secondary outcome using the State-Trait Anxiety Inventory-X-1(STAI-X-1) [32], which consists of 20 items with a total score ranging from 20 to 80. Higher scores indicate increasing levels of anxiety, where scores of 51 or less indicate normal status [33].
Stress
Stress was assessed as a secondary outcome using the Perceived Stress Scale (PSS) [34], which comprises 10 items with a total score ranging from 0 to 40. Higher scores indicate increasing levels of stress, where scores of 12 or less indicate normal status.
Sleep quality
Sleep quality was assessed as a secondary outcome using the Pittsburgh Sleep Quality Index (PSQI) [35], which consists of 19 items with a total score ranging from 0 to 21. Higher scores indicate rising levels of sleep dysfunction, where scores of 5 or less indicate normal status.
Health-related quality of life
Health-related quality of life was measured as a secondary outcome using the EuroQoL 5-Dimension 5-Level(EQ-5D-5 L) [36], which comprises five items with scores ranging from 5 to 25. Higher overall scores indicate lower quality of the participant’s health status.
Patient adherence
Patient adherence to the Silvia Program was measured for the cognitive training and video-assisted exercise modules by counting the number of days each module was completed, which was defined as fulfilling the time recommendations for each module. Overall adherence was calculated by averaging the day counts for the two modules. Engagement to the remaining 5 modules were not assessed.
Statistical analysis
Data were analyzed using the SPSS 29.0 (IBM Corp, Armonk, NY, USA). Baseline characteristics were described with frequencies, percentages, means, and standard deviations. Independent chi-square tests and t-tests were conducted to compare categorical and continuous variables between groups, respectively. The differences of dependent variables between groups were analyzed using analysis of covariance (ANCOVA), with post-test scores as the dependent variables, group as the independent variable, and pre-test scores as covariates for adjusting baseline differences. Differences with a probability of less than 0.05 were considered significant with two-tailed tests. A paired t-test was used to compare changes in the mean scores of pre and post-test in each group.
Bivariate correlations between patient adherence and cognitive function scores were analyzed using Pearson’s correlation coefficient.
RESULTS
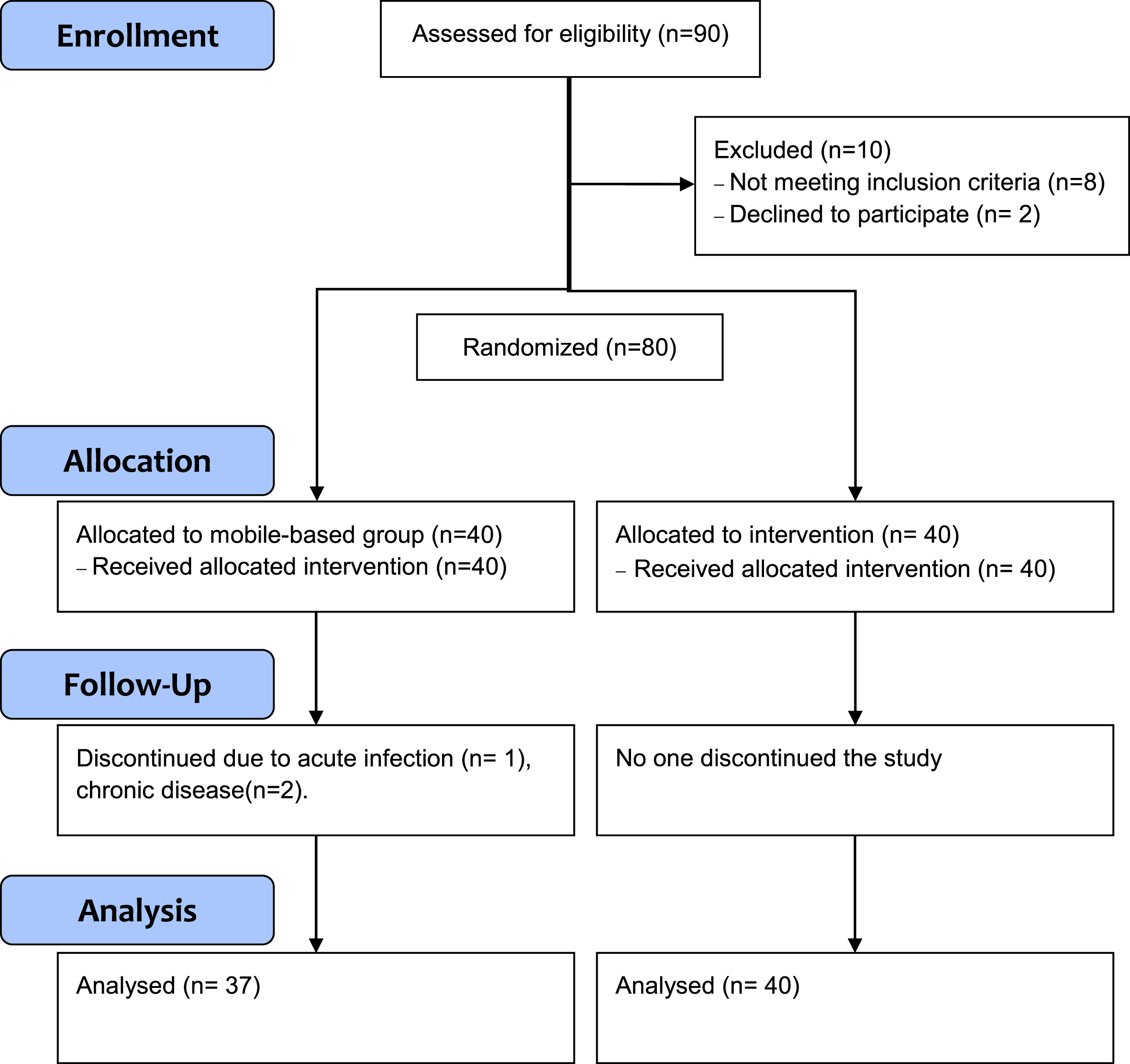
Figure 2 shows the CONSORT flow diagram of this study. A total of 90 participants were initially screened for eligibility, where eight people did not meet the inclusion criteria and two declined to participate. Of the remaining 80 participants enrolled, 77 completed the 12-week program. Three withdrew from the study because of their health conditions. The final numbers of participants were 37 in the mobile-based group and 40 in the paper-based group.
Fig. 2
CONSORT flow diagram of the present study.
Demographic features
Table 1 shows the demographic features of the study participants. The mean age was 70.08 years, and 75.3% of the total participants were female. The mean BMI was 24.42, and 81.8% had at least a high school level education. Regarding health status, 15.6% had diabetes and 48.1% had hyperlipidemia. In addition, 3.9% of participants smoked and 22.1% drank alcohol. Most of the participants (94.8%) said they worked out more than three days a week, and 83.1% lived with a partner. There were no significant differences in demographic features between the two groups.
Table 1
Baseline characteristics and homogeneity tests between groups (N = 77)
| Characteristics | Total (N = 77) | Mobile (n = 37) | Paper (n = 40) | t or χ2 | p |
| Age, mean (SD) | 70.08 (4.17) | 70.3 (4.21) | 69.88 (4.19) | T = 0.44 | 0.66 |
| Gender | |||||
| Male, n (%) | 19 (24.7) | 10 (27.0) | 9 (22.5) | χ2 = 0.21 | 0.64 |
| Female, n (%) | 58 (75.3) | 27 (73.0) | 31 (77.5) | ||
| Education | ∼ | ∼ | χ2 = 0.18 | 0.66 | |
| <High school, n (%) | 14 (18.2) | 6 (16.2) | 8 (20.0) | ||
| High school or higher, n (%) | 63 (81.8) | 31 (83.8) | 32 (80.0) | ||
| Living arrangement | χ2 = 0.21 | 0.65 | |||
| Single, n (%) | 64 (83.1) | 30 (81.1) | 34 (85.0) | ||
| With partner, n (%) | 13 (16.9) | 7 (18.9) | 6 (15.0) | ||
| BMI, mean (SD) | 24.42 (3.38) | 23.87 (3.52) | 24.92 (3.2) | T = –1.37 | 0.17 |
| Diabetes mellitus, n (%) | 12 (15.6) | 3 (8.1) | 9 (22.5) | χ2 = 3.02 | 0.08 |
| Hyperlipidemia, n (%) | 37 (48.1) | 17 (45.9) | 20 (50.0) | χ2 = 0.12 | 0.72 |
| Smoking, n (%) | 3 (3.9) | 1 (2.7) | 2 (5.0) | χ2 = 0.27 | 0.6 |
| Drinking, n (%) | 17 (22.1) | 8 (21.6) | 9 (22.5) | χ2 = 0.009 | 0.92 |
| Physical activity, n (%) | 73 (94.8) | 36 (97.3) | 37 (92.5) | χ2 = 0.89 | 0.34 |
Differences of outcome variables within groups and between groups
Table 2 and Fig. 3 shows the differences of outcome variables between groups and within groups.
Fig. 3
Differences of pre- and post-test scores of outcome variables within groups. *p < 0.05, **p < 0.01.
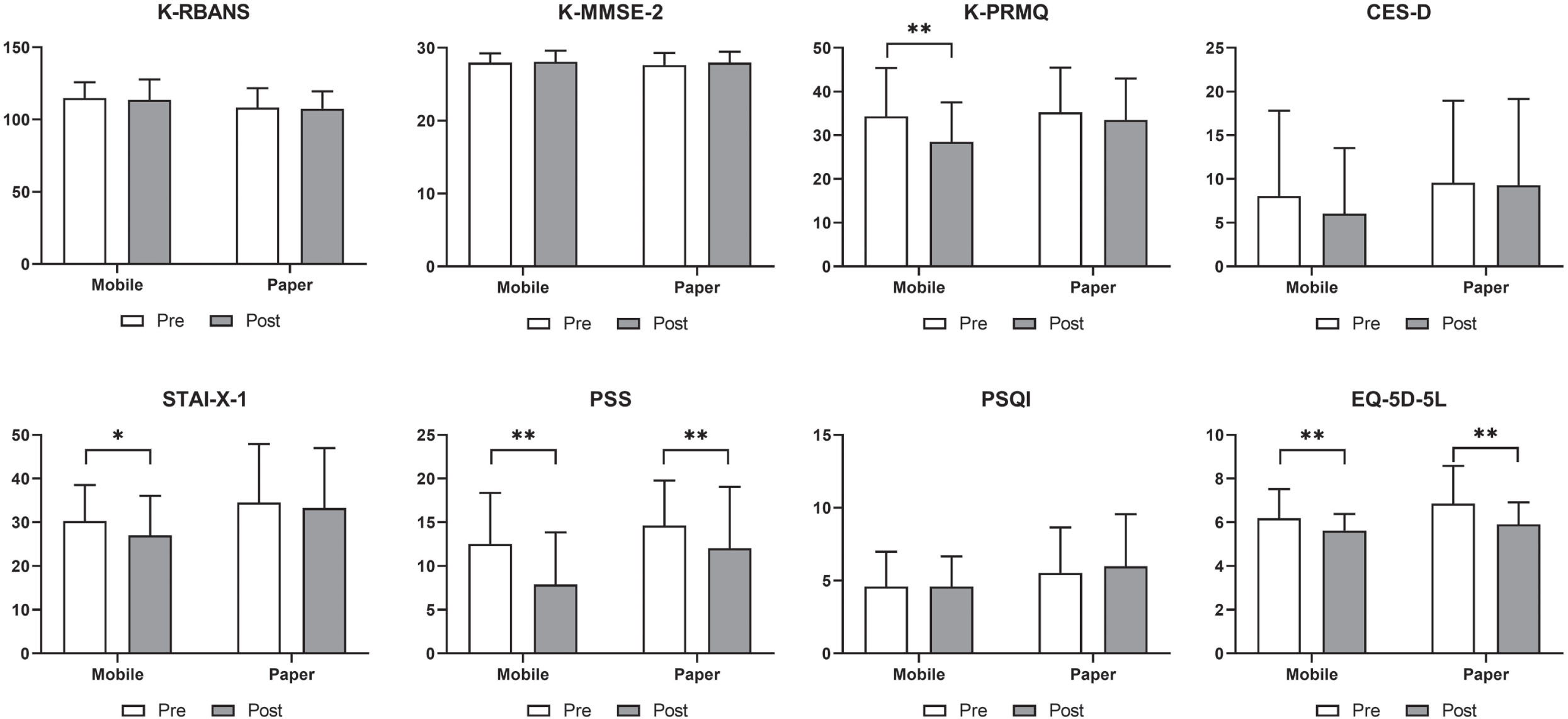
Table 2
Differences of outcome variables within groups and between groups
| Within groups (Paired t-test) | Between groups (ANCOVA) | |||||||
| Variables | Group | n | Pre-test, Mean±SD | Post-test, Mean±SD | t | p | F | p |
| K-RBANS | Mobile | 37 | 114.92±10.94 | 113.68±14.08 | –0.91 | 0.37 | 0.13 | 0.71 |
| Paper | 40 | 108.35±13.36 | 107.55±12.05 | –0.56 | 0.57 | |||
| Immediate memory | Mobile | 37 | 110.03±10.25 | 107.76±15.78 | –1.17 | 0.24 | 0.02 | 0.87 |
| Paper | 40 | 103.78±10.56 | 103.33±10.86 | –0.27 | 0.78 | |||
| Visuospatial capacity | Mobile | 37 | 105.76±8.38 | 106.49±7.69 | 0.55 | 0.58 | 0.48 | 0.48 |
| Paper | 40 | 106.15±9.13 | 105.40±8.73 | –0.44 | 0.66 | |||
| Language | Mobile | 37 | 109.08±13.51 | 103.43±14.94 | –2.60 | 0.01 | 2.13 | 0.14 |
| Paper | 40 | 105.43±13.44 | 97.35±13.26 | –3.86 | <0.001 | |||
| Attention | Mobile | 37 | 111.97±10.48 | 113.27±12.96 | 0.89 | 0.37 | 0.01 | 0.92 |
| Paper | 40 | 105.28±12.31 | 107.43±12.86 | 2.00 | 0.05 | |||
| Delayed memory | Mobile | 37 | 106.49±14.16 | 108.30±15.34 | 1.07 | 0.29 | 0.17 | 0.67 |
| Paper | 40 | 101.8±15.12 | 105.85±12.91 | 2.48 | 0.01 | |||
| K-MMSE-2 | Mobile | 37 | 27.95±1.29 | 28.08±1.53 | 0.57 | 0.57 | 0.001 | 0.97 |
| Paper | 40 | 27.63±1.65 | 27.95±1.51 | 1.18 | 0.12 | |||
| K-PRMQ | Mobile | 37 | 34.35±11.06 | 28.49±9.01 | –3.67 | <0.001 | 8.74 | 0.004 |
| Paper | 40 | 35.25±10.24 | 33.53±9.44 | –1.96 | 0.24 | |||
| CES-D | Mobile | 37 | 8.05±9.75 | 6.03±7.50 | –1.41 | 0.16 | 2.12 | 0.14 |
| Paper | 40 | 9.58±9.37 | 9.28±9.87 | –0.21 | 0.83 | |||
| STAI-X-1 | Mobile | 37 | 30.27±8.26 | 27±9.06 | –2.22 | 0.03 | 2.86 | 0.09 |
| Paper | 40 | 34.5±13.39 | 33.28±13.67 | –0.61 | 0.54 | |||
| PSS | Mobile | 37 | 12.54±5.81 | 7.89±5.94 | –5.28 | <0.001 | 4.68 | 0.03 |
| Paper | 40 | 14.63±5.15 | 12.03±7.02 | –3.04 | 0.004 | |||
| PSQI | Mobile | 37 | 4.59±2.39 | 4.59±2.06 | 0.0 | 1.0 | 1.98 | 0.16 |
| Paper | 40 | 5.53±3.10 | 5.98±3.58 | 1.09 | 0.27 | |||
| EQ-5D-5L | Mobile | 37 | 6.19±1.33 | 5.62±0.75 | –3.81 | <0.001 | 0.01 | 0.89 |
| Paper | 40 | 6.85±1.73 | 5.9±1.0 | –5.31 | <0.001 | |||
Differences between groups were analyzed with ANCOVA, which compared post-test scores between the two groups with pre-test scores as covariates. The K-RBANS total score did not show significant differences between groups. K-PRMQ scores, indicating self-reported memory failures, significantly decreased in the mobile group compared to those of the paper group (F = 8.74, p = 0.004). PSS scores, indicating perceived levels of stress, also significantly improved in the mobile group compared to those of the paper group (F = 4.68, p = 0.03).
Differences within groups were analyzed with paired t-tests. The K-RBANS total score showed no significant differences within groups, although some sub-domains of K-RBANS showed changes after the intervention: language scores were significantly decreased in both groups (p = 0.01 for mobile group, p < 0.001 for paper group), and delayed memory scores significantly increased only in the paper group (p = 0.01). Additionally, mobile-based interventions significantly improved memory failures by K-PRMQ (p < 0.001), anxiety by STAI-X-1 (p = 0.03), stress by PSS (p < 0.001), and health-related quality of life by EQ-5D-5 L scores (p < 0.001), and paper-based interventions significantly improved stress by PSS (p = 0.004) and health-related quality of life by EQ-5D-5 L scores (p < 0.001).
Patient adherence to the Silvia Program
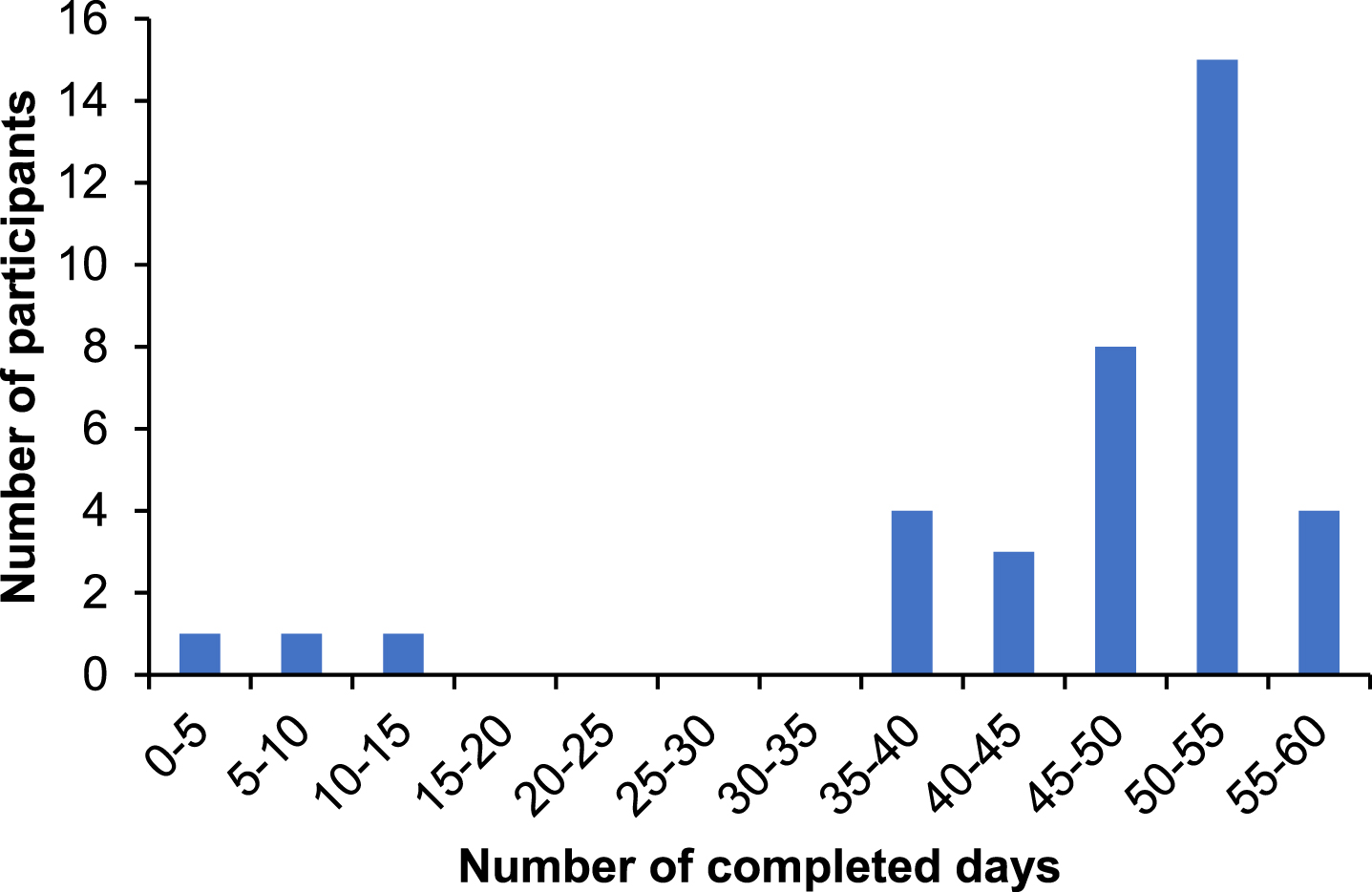
Figure 4 shows patient adherence to the Silvia Program in this study. During the 12-week intervention, the average number of completed days was 46.0 (SD = 13.0) days. As the recommendation of use was 5 days a week, or 60 days for 12 weeks, this amounts to a 76.6% adherence to the program. When we calculated bivariate correlations between patient adherence and pre-post changes for cognitive function scores, we did not find any significant correlations for the K-RBANS total score (r = 0.146, p = 0.388) and MMSE score (r = –0.156, p = 0.358).
Fig. 4
Adherence to the Silvia Program in the mobile group (n = 37).
DISCUSSION
This comparative clinical trial investigated the efficacy of the Silvia Program, a mobile-based multidomain intervention, to improve the cognitive function and health-related outcomes among older Korean adults with a high risk of developing dementia. Overall, our results showed that the mobile-based intervention was superior to the paper-based intervention in improving self-reported memory failures and stress, and both interventions improved stress levels and health-related quality of life. In particular, PRMQ scores were reduced only in the mobile group, which is an accurate tool for identifying self-experiences of memory deficits [37] that has been psychometrically validated unlike most subjective memory measurements included in dementia studies [38]. Therefore, the Silvia Program may be an effective method to prevent cognitive decline before the manifestation of pathologic impairment.
Regarding the primary outcome, our results showed no difference between the mobile-based and the paper-based programs in their effects on overall cognitive function. As both programs were implemented for only 12 weeks, the duration of the intervention may have been insufficient to reveal differences, as most multidomain cognitive interventions were conducted for 19.8 weeks on average and ranged up to 2 years [18, 19]. A recent systematic review and meta-analysis indicated that computerized cognitive training interventions with more sessions and longer durations were more effective in improving global cognitive function [39], and another systematic review reported that significant changes in cognitive function were rarely reported with interventions of fewer than 24 sessions [23]. Although some studies have reported improvements in cognitive function within short periods of less than 12 weeks, most were empirical studies using single domain interventions that targeted specific cognitive functions [40–42], for which the effects were shown to decrease over time [43]. In contrast, most multidomain interventions have shown a steady improvement of cognitive function throughout the intervention period [43].
Previous studies have demonstrated that stress and anxiety serve as possible risk factors for the progression of cognitive decline in older adults [44–46]. Recently, the COVID-19 pandemic brought many restrictive changes into people’s lives, such as social distancing and self-quarantine, which often caused high levels of stress [47]. Notably, research has shown that older adults experiencing cognitive decline registered higher scores on anxiety and stress issues during these situations, suggesting that designing and implementing effective strategies to reduce anxiety and stress are also important for dementia prevention [47]. Our results showed that the Silvia Program effectively reduced levels of stress and anxiety, which may contribute to delaying the progression of cognitive decline.
Prior studies have demonstrated that cognitive decline is negatively associated with health-related quality of life [48, 49]. While there was no statistical difference between the Silvia Program and the paper-based program, both groups showed some improvements in health-related quality of life. As previous studies have mainly focused on the cognitive benefits of multidomain programs for older adults with high risk for dementia [18, 50], this finding extends the literature by showing that the mobile-based multidomain program can improve the quality of life as well as the cognitive health of this population.
Engagement and attrition rates can greatly influence therapeutic efficacy, and the WHO has emphasized the need for testing the feasibility and efficacy of multidomain lifestyle interventions in different geographical and cultural settings [26]. A recent review on mobile-based interventions showed engagement rates of 58 to 83% and attrition rates of 6 to 61% [51], and a meta-analysis showed a pooled dropout rate of 26.2% [52]. In this study, the Silvia Program showed high and persistent engagement rates of 76.6% and a low dropout rate of 7.5%, which proves its feasibility. In addition, we focused on older Korean adults with SCD, which expands the geographical and cultural range of documentation for the efficacy of multidomain lifestyle interventions. Little information exists on the feasibility and efficacy of mobile-based multidomain approaches tested in different settings, where this study contributes to the existing body of knowledge about the benefits of digital health.
Limitations
This study has some limitations to be addressed. First, a 12-week program was provided, and as indicated, that duration may be insufficient to demonstrate cognitive changes among older adults. Future studies are needed that monitor the cognitive health benefits of mobile technology over longer periods. Second, this study focused on older adults with SCD. Further research is needed to address the broad range of cognitive function in older adults, such as subgroup analysis according to MMSE scores (normal versus abnormal) or comparative analysis between participants with or without subjective symptoms. Third, other health comorbidities and variables such as quality of family/social relationships, level of exercises, and technology acceptance may also affect health outcomes. The inclusion of additional factors might provide insights to researchers and practitioners. Finally, in the present study, two programs (mobile versus paper) were compared to investigate any differences in their effects on the cognitive function and mental health among older Korean adults with SCD. Future studies including an additional control group, which does not participate in a multidomain program (e.g., usual care or social conversation as alternatives), is needed to further validate the clinical effects of the Silvia Program.
Overall, the Silvia Program, a mobile-based multidomain intervention, was found to be effective in reducing self-reported memory failures, anxiety, and stress, and improving health-related quality of life. Given the many benefits of digital health, the Silvia Program can allow users to easily access the multidomain program, monitor their progress through AI assessment, and avoid the physical and structural barriers of face-to-face participation. Thus, the present study supports the potential health benefits of mobile health technology for the prevention of dementia and improvement of health-related quality of life in older adults with SCD.
ACKNOWLEDGMENTS
This study was supported by Gwangju Technopark, Gwangju, South Korea.
FUNDING
This research was financially supported by the Ministry of Trade, Industry, and Energy (MOTIE), South Korea, under the “Infrastructure program for industrial innovation” supervised by the Korea Institute for Advancement of Technology (KIAT).
CONFLICT OF INTEREST
J. Lee, A. Park, and R. Hong are employees of Silvia Health Inc. and M. Ko is the CEO of Silvia Health Inc.
DATA AVAILABILITY
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
REFERENCES
[1] | Gale SA , Acar D , Daffner KR ((2018) ) Dementia. Am J Med 131: , 1161–1169. |
[2] | Livingston G , Huntley J , Sommerlad A , Ames D , Ballard C , Banerjee S , Brayne C , Burns A , Cohen-Mansfield J , Cooper C , Costafreda SG , Dias A , Fox N , Gitlin LN , Howard R , Kales HC , Kivimaki M , Larson EB , Ogunniyi A , Orgeta V , Ritchie K , Rockwood K , Sampson EL , Samus Q , Schneider LS , Selbaek G , Teri L , Mukadam N ((2020) ) Dementiaprevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 396: , 413–446. |
[3] | Borson S , Frank L , Bayley PJ , Boustani M , Dean M , Lin PJ , McCarten JR , Morris JC , Salmon DP , Schmitt FA , Stefanacci RG , Mendiondo MS , Peschin S , Hall EJ , Fillit H , Ashford JW ((2013) ) Improving dementia care: The role ofscreening and detection of cognitive impairment. Alzheimers Dement 9: , 151–159. |
[4] | Rasmussen J , Langerman H ((2019) ) Alzheimer’s disease – why we need early diagnosis. Degener NeurolNeuromuscul Dis 9: , 123–130. |
[5] | Zhang H , Huntley J , Bhome R , Holmes B , Cahill J , Gould RL , Wang H , Yu X , Howard R ((2019) ) Effect of computerisedcognitive training on cognitive outcomes in mild cognitive impairment: A systematic review and meta-analysis. BMJ Open 9: , e027062. |
[6] | Biazus-Sehn LF , Schuch FB , Firth J , Stigger FS ((2020) ) Effects of physical exercise on cognitive function of olderadults with mild cognitive impairment: A systematic review and meta-analysis. Arch Gerontol Geriatr 89: , 104048. |
[7] | Soldan A , Pettigrew C , Cai Q , Wang J , Wang MC , Moghekar A , Miller MI , Albert M , Team BR ((2017) ) Cognitive reserveand long-term change in cognition in aging and preclinical Alzheimer’s disease. Neurobiol Aging 60: , 164–172. |
[8] | Choi H , Kim SH ((2018) ) Policy of national responsibility and dementia care. J Korean Med Assoc 61: , 309–313. |
[9] | Parnetti L , Chipi E , Salvadori N , D’Andrea K , Eusebi P ((2019) ) Prevalence and risk of progression of preclinicalAlzheimer’s disease stages: A systematic review and meta-analysis. Alzheimers Res Ther 11: , 7. |
[10] | Roheger M , Hennersdorf XS , Riemann S , Floel A , Meinzer M ((2021) ) A systematic review and network meta-analysis ofinterventions for subjective cognitive decline. Alzheimers Dement (N Y) 7: , e12180. |
[11] | Parfenov VA , Zakharov VV , Kabaeva AR , Vakhnina NV ((2020) ) Subjective cognitive decline as a predictor of futurecognitive decline: A systematic review. Dement Neuropsychol 14: , 248–257. |
[12] | Buckley RF , Maruff P , Ames D , Bourgeat P , Martins RN , Masters CL , Rainey-Smith S , Lautenschlager N , Rowe CC , Savage G , Villemagne VL , Ellis KA , study A ((2016) ) Subjective memory decline predicts greater rates of clinicalprogression in preclinical Alzheimer’s disease. Alzheimers Dement 12: , 796–804. |
[13] | Mitchell AJ , Beaumont H , Ferguson D , Yadegarfar M , Stubbs B ((2014) ) Risk of dementia and mild cognitive impairmentin older people with subjective memory complaints: Meta-analysis. Acta Psychiatr Scand 130: , 439–451. |
[14] | Solomon A , Stephen R , Altomare D , Carrera E , Frisoni GB , Kulmala J , Molinuevo JL , Nilsson P , Ngandu T , Ribaldi F , Vellas B , Scheltens P , Kivipelto M , European Task Force for Brain Health Services ((2021) ) Multidomain interventions: State-of-the-art and future directions for protocols to implement precision dementia risk reduction. A user manual for Brain Health Services-part 4 of 6. Alzheimers Res Ther 13: , 171. |
[15] | Ngandu T , Lehtisalo J , Solomon A , Levalahti E , Ahtiluoto S , Antikainen R , Backman L , Hanninen T , Jula A , Laatikainen T , Lindstrom J , Mangialasche F , Paajanen T , Pajala S , Peltonen M , Rauramaa R , Stigsdotter-Neely A , Strandberg T , Tuomilehto J , Soininen H , Kivipelto M ((2015) ) A 2 year multidomain intervention of diet, exercise,cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderlypeople (FINGER): A randomised controlled trial. Lancet 385: , 2255–2263. |
[16] | Gillette-Guyonnet S , Andrieu S , Dantoine T , Dartigues JF , Touchon J , Vellas B , Group MS ((2009) ) Commentary on “A roadmap for the prevention of dementia II. Leon Thal Symposium 2008.” The Multidomain Alzheimer Preventive Trial(MAPT): A new approach to the prevention of Alzheimer’s disease. Alzheimers Dement 5: , 114–121. |
[17] | Richard E , Van den Heuvel E , Moll van Charante EP , Achthoven L , Vermeulen M , Bindels PJ , Van Gool WA ((2009) ) Prevention of dementia by intensive vascular care (PreDIVA): A cluster-randomized trial in progress. Alzheimer Dis Assoc Disord 23: , 198–204. |
[18] | Salzman T , Sarquis-Adamson Y , Son S , Montero-Odasso M , Fraser S ((2022) ) Associations of multidomain interventionswith improvements in cognition in mild cognitive impairment: A systematic review and meta-analysis. JAMA Netw Open 5: , e226744. |
[19] | Bott NT , Hall A , Madero EN , Glenn JM , Fuseya N , Gills JL , Gray M ((2019) ) Face-to-face and digital multidomainlifestyle interventions to enhance cognitive reserve and reduce risk of Alzheimer’s disease and relateddementias: A review of completed and prospective studies. Nutrients 11: , 2258. |
[20] | Bernini S , Stasolla F , Panzarasa S , Quaglini S , Sinforiani E , Sandrini G , Vecchi T , Tassorelli C , Bottiroli S ((2020) ) Cognitive telerehabilitation for older adults with neurodegenerative diseases in the COVID-19 era: Aperspective study. Front Neurol 11: , 623933. |
[21] | Ammar A , Bouaziz B , Trabelsi K , Glenn JM , Zmijewski P , Muller P , Chtourou H , Jmaiel M , Chamari K , Driss T , Hokelmann A ((2021) ) Applying digital technology to promote active and healthy confinement lifestyle duringpandemics in the elderly. Biol Sport 38: , 391–396. |
[22] | Ge S , Zhu Z , Wu B , McConnell ES ((2018) ) Technology-based cognitive training and rehabilitation interventions forindividuals with mild cognitive impairment: A systematic review. BMC Geriatr 18: , 213. |
[23] | Kallio EL , Ohman H , Kautiainen H , Hietanen M , Pitkala K ((2017) ) Cognitive training interventions for patients withAlzheimer’s disease: A systematic review. J Alzheimers Dis 56: , 1349–1372. |
[24] | Koch T , Iliffe S , project E-E ((2010) ) Rapid appraisal of barriers to the diagnosis and management of patients withdementia in primary care: A systematic review. BMC Fam Pract 11: , 52. |
[25] | Gaitan A , Garolera M , Cerulla N , Chico G , Rodriguez-Querol M , Canela-Soler J ((2013) ) Efficacy of an adjunctivecomputer-based cognitive training program in amnestic mild cognitive impairment and Alzheimer’s disease: Asingle-blind, randomized clinical trial. Int J Geriatr Psychiatry 28: , 91–99. |
[26] | World Health Organization ((2019) ) Risk reduction of cognitive decline and dementia: WHO guidelines. |
[27] | Moon SY , Hong CH , Jeong JH , Park YK , Na HR , Song HS , Kim BC , Park KW , Park HK , Choi M , Lee SM , Chun BO , Koh SH , Park SA , Park HH , Jin JH , Lee EH , Kim SM , Han SM , Kim JS , Ha J , Choi SH ((2021) ) Facility-based and home-basedmultidomain interventions including cognitive training, exercise, diet, vascular risk management, and motivationfor older adults: A randomized controlled feasibility trial. Aging (Albany NY) 13: , 15898–15916. |
[28] | Park JO , Koo BH , Kim JY , Bai DS , Chang MS , Kim OL ((2021) ) The Korean Repeatable Battery for the Assessment of Neuropsychological Status-Update: Psychiatric and neurosurgery patient sample validity. J Korean NeurosurgSoc 64: , 125–135. |
[29] | Baek MJ , Kim K , Park YH , Kim S ((2016) ) The validity and reliability of the Mini-Mental State Examination-2 fordetecting mild cognitive impairment and Alzheimer’s disease in a Korean population. PLoS One 11: , e0163792. |
[30] | Lee W ((2008) ) A study on episodic memory features and everyday memory enhancement of healthy older adults [dissertation]. Unpublished doctoral dissertation, Korea University, Seoul. |
[31] | Radloff LS ((1977) ) The CES-D scale: A self-report depression scale for research in the general population. Appl Psychol Measure 1: , 385–401. |
[32] | Speilberger CD , Gorsuch R , Lushene R , Vagg P , Jacobs G ((1983) ) Manual for the state-trait anxiety inventory. Consulting Psychologists. |
[33] | Kim JT , and D. K. Shin. ((1978) ) A study based on the standardization of the STAI for Korea. New Med J 21: , 69–75. |
[34] | Cohen S ((1988) ) Perceived stress in a probability sample of the United States. The Social Psychology of Health, Spacapan S, Oskamp S, eds. Sage Publications, Inc., pp. 31–67. |
[35] | Sohn SI , Kim DH , Lee MY , Cho YW ((2012) ) The reliability and validity of the Korean version of the Pittsburgh SleepQuality Index. Sleep Breath 16: , 803–812. |
[36] | Herdman M , Gudex C , Lloyd A , Janssen M , Kind P , Parkin D , Bonsel G , Badia X ((2011) ) Development and preliminarytesting of the new five-level version of EQ-5D (EQ-5D-5L). Qual Life Res 20: , 1727–1736. |
[37] | Ronnlund M , Sundstrom A , Adolfsson R , Nilsson LG ((2015) ) Self-reported memory failures: Associations with futuredementia in a population-based study with long-term follow-up. J Am Geriatr Soc 63: , 1766–1773. |
[38] | Crawford JR , Smith G , Maylor EA , Della Sala S , Logie RH ((2003) ) The Prospective and Retrospective MemoryQuestionnaire (PRMQ): Normative data and latent structure in a large non-clinical sample. Memory 11: , 261–275. |
[39] | Li R , Geng J , Yang R , Ge Y , Hesketh T ((2022) ) Effectiveness of computerized cognitive training in delayingcognitive function decline in people with mild cognitive impairment: Systematic review and meta-analysis. JMed Internet Res 24: , e38624. |
[40] | Hyer L , Scott C , Atkinson MM , Mullen CM , Lee A , Johnson A , McKenzie LC ((2016) ) Cognitive training program toimprove working memory in older adults with MCI. Clin Gerontol 39: , 410–427. |
[41] | Vermeij A , Claassen JA , Dautzenberg PL , Kessels RP ((2016) ) Transfer and maintenance effects of onlineworking-memory training in normal ageing and mild cognitive impairment. Neuropsychol Rehabil 26: , 783–809. |
[42] | Manera V , Petit PD , Derreumaux A , Orvieto I , Romagnoli M , Lyttle G , David R , Robert PH ((2015) ) ‘Kitchen andcooking,’ a serious game for mild cognitive impairment and Alzheimer’s disease: A pilot study. Front AgingNeurosci 7: , 24. |
[43] | Cheng Y , Wu W , Feng W , Wang J , Chen Y , Shen Y , Li Q , Zhang X , Li C ((2012) ) The effects of multi-domain versussingle-domain cognitive training in non-demented older people: A randomized controlled trial. BMC Med 10: , 30. |
[44] | Gulpers B , Ramakers I , Hamel R , Kohler S , Oude Voshaar R , Verhey F ((2016) ) Anxiety as a predictor for cognitivedecline and dementia: A systematic review and meta-analysis. Am J Geriatr Psychiatry 24: , 823–842. |
[45] | Comijs HC , van den Kommer TN , Minnaar RW , Penninx BW , Deeg DJ ((2011) ) Accumulated and differential effects of lifeevents on cognitive decline in older persons: Depending on depression, baseline cognition, or ApoE epsilon4status? J Gerontol B Psychol Sci Soc Sci 66: Suppl 1, 111–120. |
[46] | Tschanz JT , Pfister R , Wanzek J , Corcoran C , Smith K , Tschanz BT , Steffens DC , Ostbye T , Welsh-Bohmer KA , Norton MC ((2013) ) Stressful life events and cognitive decline in late life: Moderation by education and age. The Cache County Study. Int J Geriatr Psychiatry 28: , 821–830. |
[47] | Jiloha RC ((2020) ) COVID-19 and Mental Health. Epidem Int 5: , 7–9. |
[48] | Roehr S , Luck T , Pabst A , Bickel H , Konig HH , Luhmann D , Fuchs A , Wolfsgruber S , Wiese B , Weyerer S , Mosch E , Brettschneider C , Mallon T , Pentzek M , Wagner M , Mamone S , Werle J , Scherer M , Maier W , Jessen F , Riedel-Heller SG , AgeCoDe study group ((2017) ) Subjective cognitive decline is longitudinally associatedwith lower health-related quality of life. Int Psychogeriatr 29: , 1939–1950. |
[49] | Konigsberg A , Belau MH , Ascone L , Gallinat J , Kuhn S , Jensen M , Gerloff C , Cheng B , Thomalla G ((2023) ) Subjectivecognitive decline is associated with health-related quality of life in the middle-aged to elderly population. J Alzheimers Dis 91: , 427–436. |
[50] | Meng X , Fang S , Zhang S , Li H , Ma D , Ye Y , Su J , Sun J ((2022) ) Multidomain lifestyle interventions for cognitionand the risk of dementia: A systematic review and meta-analysis. Int J Nurs Stud 130: , 104236. |
[51] | Nwosu A , Boardman S , Husain MM , Doraiswamy PM ((2022) ) Digital therapeutics for mental health: Is attrition theAchilles heel? Front Psychiatry 13: , 900615. |
[52] | Torous J , Lipschitz J , Ng M , Firth J ((2020) ) Dropout rates in clinical trials of smartphone apps for depressivesymptoms: A systematic review and meta-analysis. J Affect Disord 263: , 413–419. |


